")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Effect of Repeated Intranasal Administration of Different Doses of Insulin on Postoperative Delirium, Serum τ and Aβ Protein in Elderly Patients Undergoing Radical Esophageal Cancer Surgery
Authors Huang Q, Shi Q, Yi X, Zeng J, Dai X, Lin L, Yang Y, Wu X , Gong G
Received 28 January 2023
Accepted for publication 21 April 2023
Published 28 April 2023 Volume 2023:19 Pages 1017—1026
DOI https://doi.org/10.2147/NDT.S405426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yuping Ning
Qingqing Huang,1 Qin Shi,2 Xiaobo Yi,1 Jingzheng Zeng,2 Xuemei Dai,1 Lu Lin,1 Yanling Yang,1 Xiao Wu,2 Gu Gong1
1Department of Anesthesiology, The General Hospital of Western Theater Command, Chengdu, People’s Republic of China; 2Department of Anesthesiology, North Sichuan Medical College, Nanchong, People’s Republic of China
Correspondence: Gu Gong, Department of Anesthesiology, The General Hospital of Western Theater Command, 270 Tianhui Road, Rongdu Avenue, Jinniu District, Chengdu, Sichuan, 610083, People’s Republic of China, Tel +8617360137572, Fax +86 28570423, Email [email protected]
Objective: Postoperative delirium is common after general anesthesia in older patients. However, there are currently no effective preventive measures. This study investigated the effect of repeated intranasal administration of different insulin doses before surgery on postoperative delirium in older patients with esophageal cancer, and the possible mechanism for its efficacy.
Methods: In this randomized, placebo-controlled, double-blind, parallel-group study, 90 older patients were randomly assigned to either a Control (normal saline), Insulin 1 (20 U/0.5 mL intranasal insulin), or Insulin 2 (30 U/0.75 mL intranasal insulin) group. Delirium was assessed on postoperative days 1 (T2), 2 (T3), and 3 (T4) using the Confusion Assessment Method for the Intensive Care Unit. Serum τ and Aβ protein levels were measured at T0 (before insulin/saline administration), T1 (end of surgery), T2, T3 and T4.
Results: The Insulin 2 group had a significantly lower prevalence of delirium compared to the Control and Insulin 1 groups three days after surgery. Compared to baseline, τ and Aβ protein levels increased significantly at T1–T4. Compared to the Control group, the Insulin 1 and 2 groups had significantly lower τ and Aβ protein levels at T1–T4, and the Insulin 2 group had significantly lower levels than the Insulin 1 group at T1–T2.
Conclusion: The administration of 30 U of intranasal insulin twice daily, from 2 days preoperatively until 10 minutes preanesthesia on the day of surgery, can significantly reduce postoperative delirium in older patients undergoing radical esophagectomy. It can also decrease postoperative τ and Aβ protein expression without causing hypoglycemia.
Clinical Trial Registration: This study was registered at the Chinese Clinical Trial Registry (www.chictr.org.cn, with the unique identifier: ChiCTR2100054245; December 11, 2021).
Keywords: postoperative delirium, intranasal insulin, τ protein, Aβ protein, aged
Introduction
Postoperative delirium (POD) is a common postoperative complication in older patients undergoing surgery, and its prevalence can reach 50% after esophageal cancer surgery.1 Its main manifestations are disordered thinking, disorientation, inattention, day and night reversal, and altered consciousness. POD can lead to increased postoperative complications and perioperative mortality.2 Currently, the pathogenesis of POD is unclear and there is no safe and effective method for its prevention and treatment. Intranasal insulin administration is an important treatment for the cognitive impairment associated with abnormal brain energy metabolism, and has received extensive attention recently.3–5 Following its intranasal administration, insulin can quickly reach the central cerebrospinal fluid through the cerebral ventricular system around the olfactory nerve in the nasal cavity. This method allows insulin to bypass the blood–brain barrier, leading to higher levels in the brain. Thus, intranasal administration can effectively prevent the adverse effects of peripheral administration, such as hypoglycemia.6 Shpakov et al7 showed that insulin has a unique effect after binding to different insulin receptors in the brain, and could be used for treatment of cerebral ischemia, traumatic brain injuries, and postoperative delirium (after anesthesia), as well as diabetes mellitus and its complications such as dysfunctions in the gonadal and thyroid axes.
Our previous study indicated that repeated administration of intranasal insulin could reduce the prevalence of POD and tumor necrosis factor-α, interleukin-1β, and interleukin-6 levels in elderly patients after laparoscopic radical gastrointestinal tumor resection.8 Meanwhile, existing studies suggest that total τ protein and Aβ protein may be potential biomarkers for postoperative delirium.9,10 However, there are no studies on the effect of repeated intranasal administration of different insulin doses on POD. This study investigated the effect of repeated intranasal administration of different insulin doses on POD, serum τ protein, and serum Aβ protein in older patients undergoing a radical esophagectomy. We proposed the hypothesis that repeated intranasal administration of different insulin doses can reduce postoperative delirium in older patients and decrease postoperative τ and Aβ protein expression. Present trial was performed to verify this hypothesis.
Patients and Methods
Study Population
This study was approved by the ethics committee of the General Hospital of Western Theater Command (Ethics Approval No. 2019ky64) before beginning and was conducted in accordance with the principles in the Helsinki Declaration, the chairperson of the ethics committee, Haiwei Yang. The date of approval by the ethics committee was July 30, 2019. Written informed consent was obtained from all participants. The study was registered with the Chinese Clinical Trial Registry, at www.chictr.org.cn with the unique identifier, ChiCTR2100054245 on December 11, 2021. The study was conducted and reported using CONSORT reporting guidelines (Supplementary CONSORT 2010).11 On this prospective, double-blind, single-center, randomized, parallel-group study we enrolled 90 patients (age ≥65 years, American Society of Anesthesiologists (ASA) physical status I to III, body mass index (BMI) ≤28 kg/m²) who were undergoing radical resection for esophageal cancer with a combined thoracoscopy and laparoscopy under general anesthesia between January 2022 and May 2022 at the General Hospital of Western Theater Command. The primary exclusion criteria were, (1) contraindications to the nasal administration of therapeutics (such as nasal defects or lesions) (2) history of hypertension or diabetes (3) history of insulin allergy (4) history of alcoholism (5) inability to communicate preoperatively (eg, coma, severe dementia, speech impairment, or severe visual or hearing impairments) (6) low preoperative Mini-Mental Status Examination score pre-elementary school <17 points, elementary school <20 points, and middle school (including technical secondary) <24 points (7) severe heart, liver, or kidney disease and (8) history of neurological or psychiatric disease. Primary withdrawal criteria included (1) insulin use via a non-nasal route during the trial (2) operation time of <3 hours or >6 hours (3) reoperation within 3 days after the initial operation (4) unpredicted adverse events (eg, drug allergies, anesthesia-related adverse events, or surgical accidents), and (5) loss to follow-up (patient discharge within 3 days postoperatively).
Sample Size Calculation and Randomization
A literature review found that the prevalence of POD was up to 50% in older patients undergoing radical resection for esophageal cancer.1 After the intranasal administration of 20 U insulin,8 the prevalence of POD was 13.5%. In the pre-experiment, there was a 10% prevalence of POD after intranasal 30 U insulin administration. We set α=0.05 (two-tailed), 1-β=0.9, effect size (W) =0.4206, and we used Power Analysis and Sample Size (PASS), version 11.0 (NCSS Statistical Software, Kaysville, UT, USA) to calculate the sample size of 74. We have used a sample size of 90 cases to account for a loss to follow-up rate of 20%.
Participants were randomly classified into the Control, Insulin 1, and Insulin 2 groups in a 1:1:1 ratio (30 patients in each group). Ninety sealed envelopes with test solutions (normal saline, 20 U/0.5 mL of insulin and 30 U/0.75 mL of insulin; 30 each) were prepared. We used SPSS version 25.0 (IBM Corp., Armonk, NY, USA) to generate a random number list to number the sealed envelopes. The envelopes were arranged in ascending order by a researcher who did not participate in the trial. When a patient was enrolled in the study, the researcher opened the envelope and prepared the specified dosage on the nasal mucosal atomization device with a syringe (Wuxi Nice Life Technology Co., Ltd., Jiangsu, China), wrote the random number in the patient’s file and discarded the envelope. Anesthesiologists, patients, and surgeons were blinded to the assignment of the patient groups. Jiangsu Wanbang Biochemical Pharmaceutical Co. Ltd. (Jiangsu, China) supplied rapid-acting insulin (10 mL: 400 U).
Administration Method
Patients in the Control, Insulin 1, and Insulin 2 groups received 0.5 mL of intranasal saline, 20 U (0.5 mL) insulin, and 30 U (0.75 mL) insulin, respectively, using the nasal mucosal atomization device with a syringe starting 2 days preoperatively, twice daily at 0900 and 1900 hours. The final dose was administered 10 minutes before induction of anesthesia on the operative day, for five administrations. Detailed operation of nasal administration: put the patient in the supine position, tilt the head back, clean the nasal secretions with a cotton swab, and then drop the solvent that has been configured in the nasal mucosal physicochemical device into the nose. Alternatively administered on both sides of the nasal passage. Gently pinch the nose to make sufficient contact with the nasal mucosa and reduce the entry into the throat. The patients were instructed to restore his position after 5–10 minutes. This procedure was performed by a researcher who was not involved in the postoperative evaluation.
Anesthetic Management
Patients received an ECG, oxygen saturation, bispectral index (BIS), and invasive blood pressure monitoring. They also had oxygen therapy and were cannulated with a central venous pressure infusion device (CVP) and an arterial blood gas-sampling device (ABG) under local anesthesia. Etomidate (0.3 mg/kg), sufentanil (0.4 μg/kg), and atracurium (0.2 mg/kg) were used to induce general anesthesia. Following muscle relaxation, tracheal intubation was performed under laryngoscopic guidance, and mechanical ventilation was performed. Intraoperatively, the tidal volume was maintained at 8–10 mL / kg, the respiratory rate at 12 times / min, the inspiratory ratio at 1: 1 and the end tidal CO2 at 35–45 mmHg. Remifentanil and propofol were continuously infused at 0.2 to 0.4 ug / kg / min and 4 to 8 mg / kg / h, respectively, and sevoflurane was inhaled to maintain a BIS value of 40 to 60. Sevoflurane, propofol, and remifentanil were stopped 5 minutes before the end of surgery. Intraoperative vasoactive drugs were administered to stabilize blood pressure and heart rate if necessary. A heating blanket was applied to keep the body warm and the body temperature was monitored. All patients received postoperative analgesia. During the first 48 hours after surgery, they received 100 mL of normal saline solution containing butorphanol (5 mg), tropisetron (10 mg), and sufentanil (100 μg) via patient-controlled intravenous analgesia at an infusion rate of 2 mL / h and a lockout time of 15 min with doses of 0.5 mL of bolus.
Data Collection
The demographics and medical histories of the patients were recorded, including age, sex, BMI, MMSE score, operation time, ASA classification, hemoglobin concentration, total intraoperative infusion, blood transfusion volume, blood loss and the numerical rating scale (NRS) score during the first 3 postoperative days.
Primary Endpoint
The patients were followed twice daily from 0800 to 1000 and 1800 to 2000 hours during the first 3 days after surgery, days using the Confusion Assessment Method for the intensive care unit (CAM-ICU) by an investigator (Jingzheng ZENG), who was not involved in anaesthesia and perioperative care, and was not allowed to exchange patients’information with anaesthesiologists who take care of patients in the operating room. The feasibility of the Chinese version of CAM-ICU has been established in studies reported by our group and others.8,12 The CAM-ICU was carried out in two steps.13,14 Patient sedation/agitation levels were first evaluated using the Richmond Agitation Sedation Scale (RASS).15 If the patient was not responsive to verbal stimuli (ie, RASS score ≤ −4), we stopped assessing delirium and the patient was considered comatose. When the RASS score was ≥ −3, a delirium assessment was performed using CAM-ICU. Diagnostic criteria for a positive outcome in the CAM ICU included: (1) acute delirium attack and fluctuating disease status; (2) inattention; (3) disorganized thinking; and (4) change in consciousness.16 Delirium was diagnosed when the patient showed the first and second features, plus the third or fourth feature. POD was defined as a positive CAM-ICU in the first 3 days after the operation.
Secondary Endpoints
Biochemical Tests
Venous blood (3 mL) was collected in procoagulant tubes at five time points, before insulin/saline administration (T0), at the end of surgery (T1), and on postoperative days 1, 2, and 3 (T2, T3, and T4, respectively). After centrifugation at 3000 xg for 15 minutes, the supernatant was removed, placed in a cryopreservation tube, and stored in a freezer at −80 °C until further assay. Enzyme-linked immunosorbent assay kits determined the τ protein and Aβ protein concentrations according to the manufacturer’s instructions (Thermo Fisher, United States). The trained research personnel performing the assays were blinded to group assignment.
Adverse Events
The main predicted adverse event related to using insulin was hypoglycemia. Hypoglycemia was defined as a blood glucose concentration <2.77 mmol/L.17 A continuous glucose monitoring system (Shenzhen Silicon-based Sensing Technology Co., Ltd., Shenzhen, China) was used to dynamically track the patient’s blood glucose levels during the trial. Serum insulin concentration at T0 and T1 was determined using enzyme-linked immunosorbent assay kits according to the manufacturer’s instructions (Thermo Fisher, United States). A total nasal symptom score (TNSS) was performed by an investigator (Lu LIN), who was blinded to the group assignment after dosing, which included assessing nasal congestion, runny nose, nasal itching, and sneezing. Each symptom was scored on a four-point scale: 0=no symptoms, 1=mild symptoms, 2 = moderate symptoms and 3=severe symptoms for a total score of 12 points. The higher the score, the more severe the nasal irritation symptoms.18
Statistical Analysis
The collected data were entered into EpiData version 3.1 (The EpiData Association, Odense, Denmark), exported to Microsoft Excel 2016 (Redmond, WA, USA), and analyzed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Outcome analyzes were based on intent-to-treat; that is, all patients were analyzed in the group to which they were randomized.19,20 Continuous data were first tested using the Shapiro–Wilk test to verify a normal distribution. Continuous data with normal distributions are expressed as mean ± SD. A one-way analysis of variance was used to analyze the data, and the Tukey’s test was applied to post hoc pairwise comparisons. P <0 .05 was considered statistically significant. Continuous data with nonnormal distributions are expressed as median (interquartile range) and were analyzed with the Kruskal–Wallis test. If the results were statistically significant, comparisons between groups were made using the Mann–Whitney U-test. Categorical variables are expressed as frequencies or percentages and analyzed with the Pearson chi-square or Fisher exact test. Repeated-measures analysis of variance was used to compare τ protein and Aβ protein levels between groups at each time point. If the results were statistically significant, comparisons between groups were made using the Mann–Whitney U-test. The Bonferroni method was used to control for type I error for multiple comparisons between the Control, Insulin 1, and Insulin 2 groups.
Quality Control
Data were monitored by the Quality Control Division of the Clinical Research Ethics Committee of the General Hospital of the Western Theater Command.
Results
Patient Inclusion
There were 90 patients were included in the final intention-to-treat analysis (Figure 1). The three groups had similar demographic characteristics. There were no significant differences in age, sex, BMI, MMSE score, operation time, ASA classification, hemoglobin concentration, total intraoperative infusion, blood transfusion volume, blood loss and NRS score during the first 3 postoperative days (Table 1).
 |
Table 1 Patient Demographics and Clinical Data |
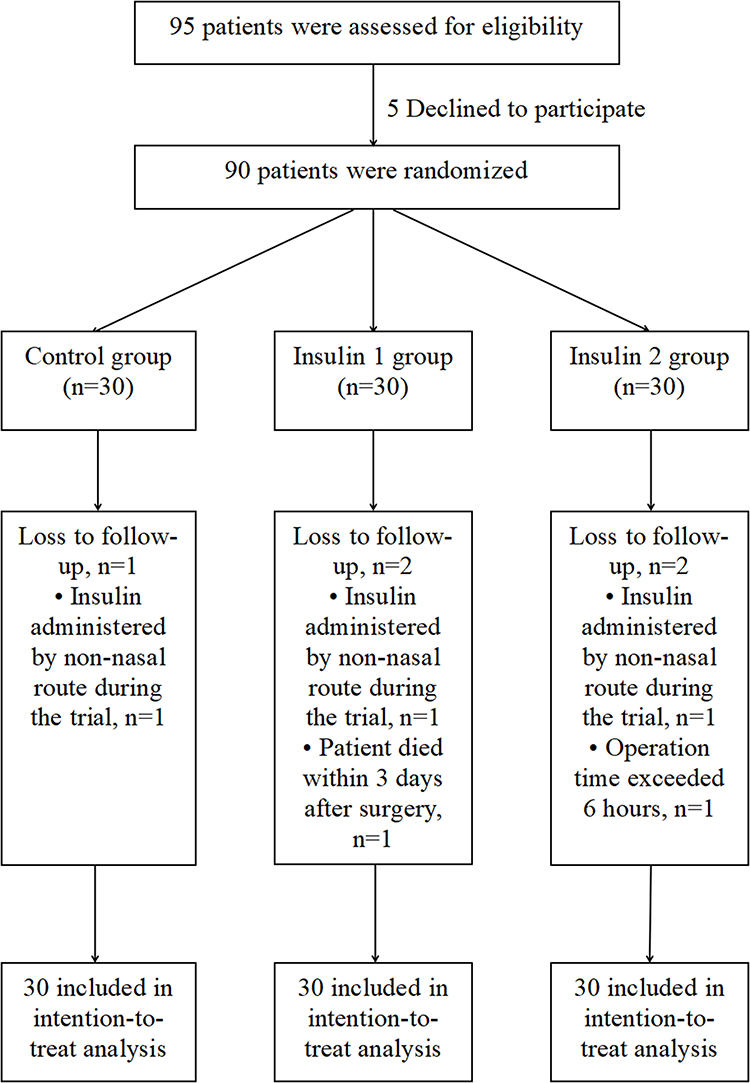 |
Figure 1 Flow diagram of the study. |
RASS Scores and the Prevalence of POD
None of the patients was comatose (as measured by the RASS) throughout the trial. Compared to the Control group, the Insulin 1 (63.3% vs 30%, P=0.019) and Insulin 2 (63.3% vs 3.3%, P<0.001) groups demonstrated a decreased prevalence of POD within 3 days postoperatively. Compared to the Insulin 1 group, the Insulin 2 group (30% vs 3.3%, P=0.012) demonstrated a decreased POD prevalence within 3 days postoperatively (Table 2).
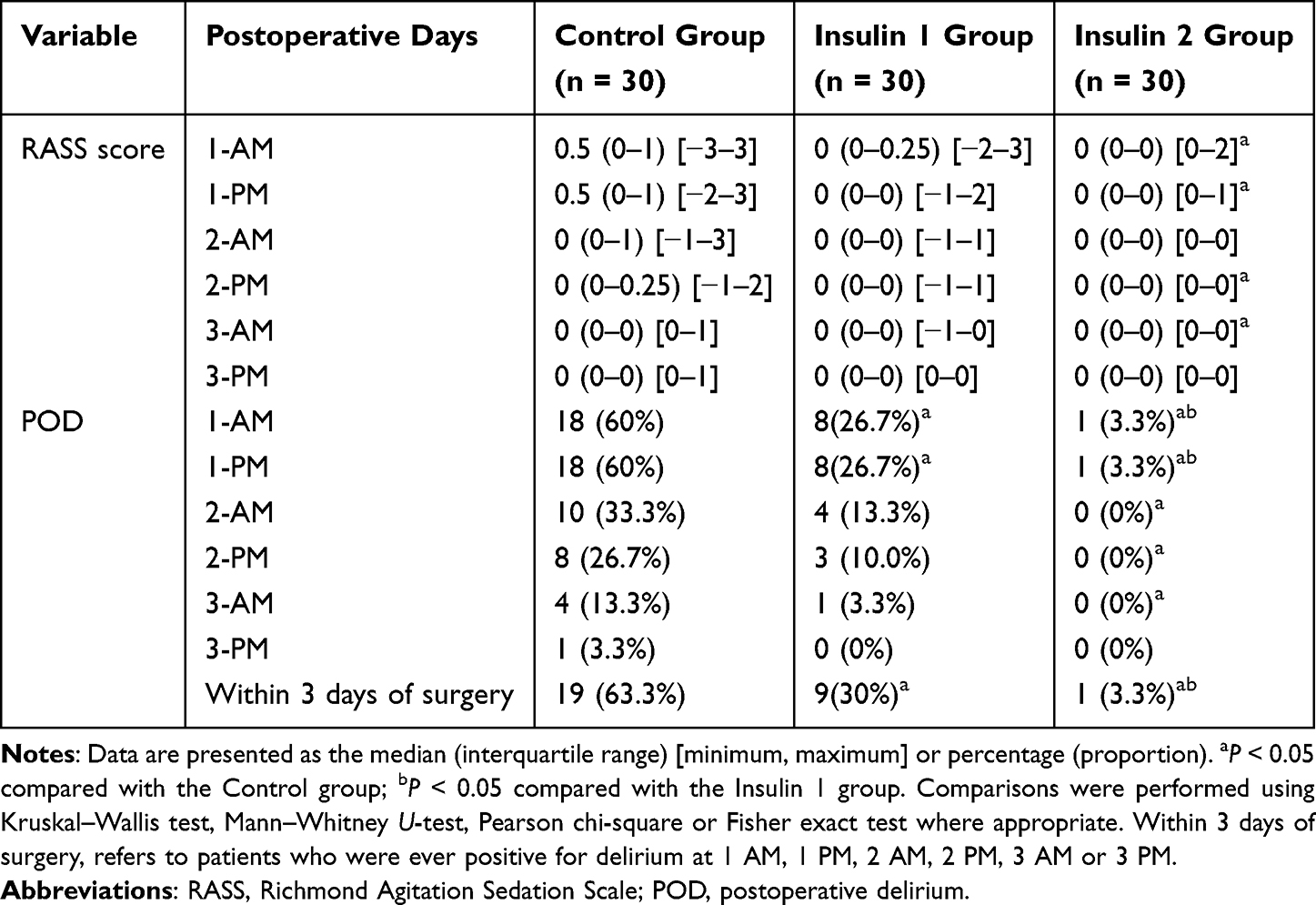 |
Table 2 RASS Scores and Incidence of Postoperative Delirium During the First Three Postoperative Days |
τ Protein and Aβ Protein
Compared to the baseline value at T0, serum τ protein and Aβ protein concentrations increased significantly at T1–T4 (P<0.05). Compared to the Control group, the τ and Aβ protein levels in the Insulin 1 and Insulin 2 groups at T1–T4 were significantly reduced (P<0.05). Compared to the Insulin 1 group at the same time, the τ and Aβ protein levels in the Insulin 2 group at T1–T2 were significantly reduced (P<0.05) (Table 3).
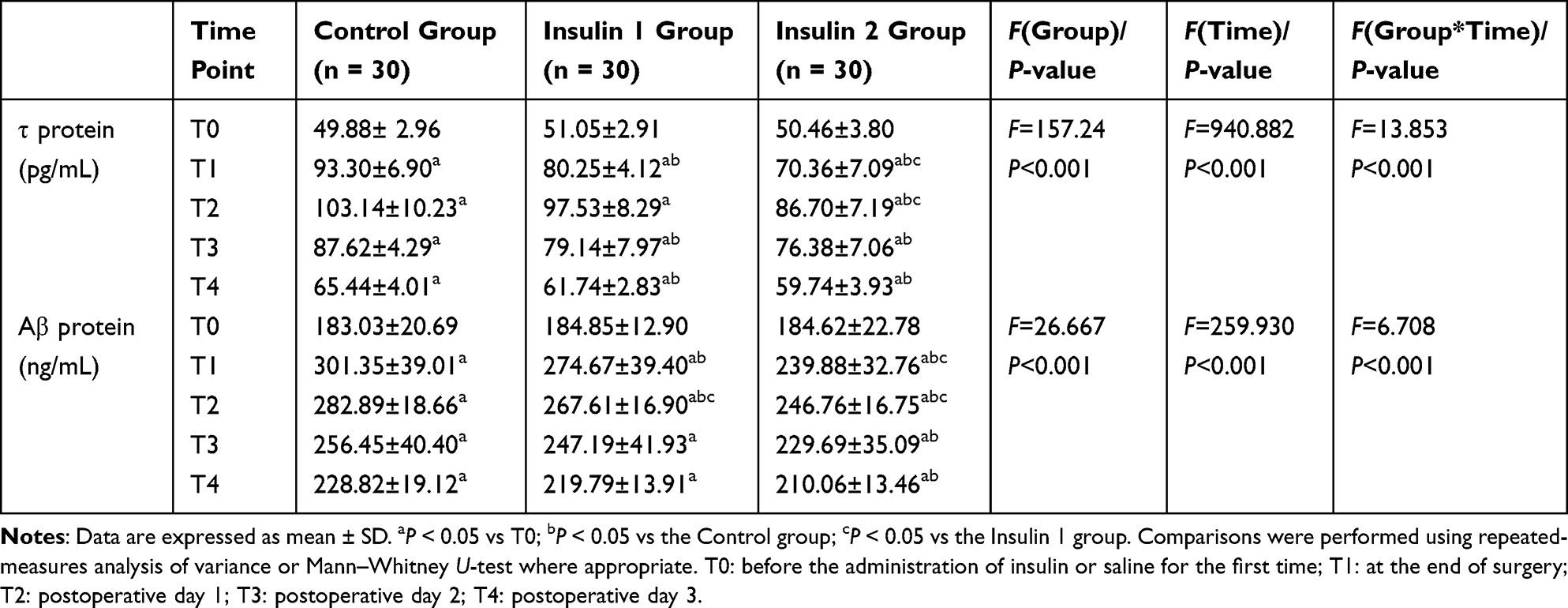 |
Table 3 Comparison of TAU Protein and Aβ Protein Expression in Three Groups of Patients at Different Time Points |
Adverse Events
None of the participants experienced defined hypoglycemic reactions, as assessed by continuous glucose monitoring. Furthermore, all patients had a TNSS of 0. There were no significant differences in serum insulin concentrations between the three groups in T0 and T1 (Table 4).
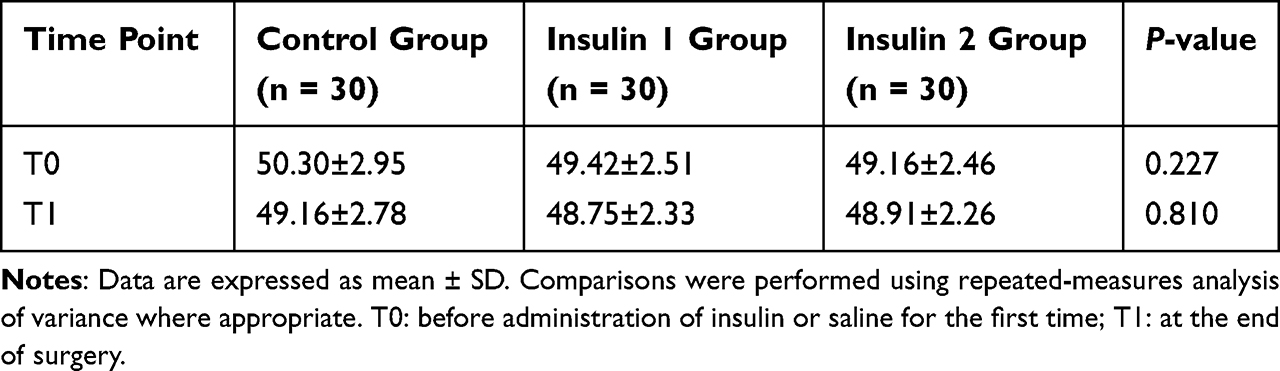 |
Table 4 Comparison of Insulin Level in Serum (pmol/L) at T0 and T1 Among the Three Groups |
Discussion
POD is a mental illness syndrome with confusion as the primary clinical manifestation that often appears as attention, memory, psychomotor, and sleep-wake cycle disorders.21 Currently, the exact mechanism of POD is unclear. However, most studies have indicated it is related to various promoting factors, such as primary nervous system diseases, drugs, history of organic encephalopathy (eg, dementia, Parkinson disease, preoperative cognitive impairment, and other cerebrovascular diseases), metabolic disorders, surgical procedures, anesthesia, and the environment.21 At present, studies have shown that delirium is associated with amyloid-tau-neurodegeneration pathophysiology.22 Aβ protein is the main component of senile plaques, consisting of a short peptide of 39–42 amino acids produced and released by β and γ secretases during the formation of the amyloid precursor protein.23 The τ protein is an axonal microtubule-associated protein whose main function is to bind and stabilize microtubules and promote microtubule polymerization. Existing studies have shown that general anesthetics (such as isoflurane and propofol) can enhance Aβ protein oligomerization and synthesis and τ protein phosphorylation.24 Extracellular aggregation of Aβ into oligomers can increase its neurotoxicity and induce neuronal degeneration and even apoptosis.25 Multiple kinases hyperphosphorylate the τ protein. Hyperphosphorylated τ protein forms oligomeric aggregates and neurofibrillary tangles, losing its function to maintain insulin signaling in the brain, which leads to insulin resistance. This process not only impairs hippocampal plasticity and enhances cognitive deficits, but also leads to the accumulation of Aβ.26 Furthermore, phosphorylated τ protein has reduced microtubule binding affinity and axonal localization ability. It is induced to be released into dendrites by Aβ, leading to early synaptic toxicity and progressive dendritic spine damage.27 Ultimately, Aβ and τ proteins synergistically block neuronal function, damage the brain, affect cognitive function, and lead to POD. τ and Aβ proteins are released into the extracellular fluid only after cranial nerve injury. This release changes the permeability of the blood-brain barrier, and the τ and Aβ proteins enter the bloodstream. The results of the present study support this pattern, as the three groups had different POD rates at 1–3 days postoperatively, and τ and Aβ protein levels increased significantly compared to preoperative levels.
Xie et al28 and Cunningham et al29 found that the Aβ-42, phosphorylated τ protein, and total τ protein levels; τ/Aβ-40 ratio; and τ/Aβ-42 ratio in preoperative cerebrospinal fluid can be used as predictors of POD during joint replacement surgery. Moreover, Ballweg et al30 evaluated the association between the biomarkers glial fibrillary acidic protein and τ protein, and the prevalence and severity of delirium in 114 surgical patients. They found that changes in plasma τ protein were associated with prevalence and severity of delirium. When insulin is administered intranasally, the nonamyloidogenic processing of the amyloid precursor protein is enhanced, while amyloidogenic processing is compromised. Furthermore, the involvement of apolipoprotein E in Aβ metabolism is reduced, which improves cognitive deficits and brain insulin signaling disorders. This greatly reduces Aβ production and plaque formation,31 thereby treating and preventing AD.
Regarding intranasal insulin as a non-invasive strategy, Guo et al32 found its long-term administration improved cognitive impairment, τ protein hyperphosphorylation, and microglia activation in a streptozotocin-induced AD rat model. In cases of POD with pathogenesis similar to AD, studies33 indicate that intranasal insulin attenuates propofol-induced hyperphosphorylation of τ protein, promotes insulin signaling in the brain, and leads to upregulation of protein phosphatase 2A (the major τ phosphatase in the brain). Zhang et al34 pretreated mice with daily intranasal insulin (1.75 U/day) for 1 week, and then induced anesthesia by injecting intraperitoneal propofol, which was maintained by sevoflurane inhalation for 1 hour. Intranasal insulin was found to treat anesthesia-induced spatial learning and memory deficits using the Morris water maze test 1 to 5 days after anesthesia, in addition to attenuating anesthesia-induced τ protein hyperphosphorylation and promoting synaptic protein expression in the brain. In this study, the prevalence of POD and the expression of τ and Aβ proteins in the serum of the patients in the Insulin 1 and 2 groups were significantly lower than in the Control group 1 to 3 days postoperatively. This finding suggests that insulin intranasal administration can reduce τ protein hyperphosphorylation and Aβ, thus reducing the prevalence of POD. Additionally, the prevalence of POD and the expression of τ protein and Aβ protein in the serum of the patients were significantly lower in the Insulin 2 group than in the Insulin 1 group on days 1 to 3 postoperatively. These results suggest that insulin 30 U/time (administered 2 days preoperatively, twice daily, until 10 min before anesthesia on the day of surgery) can significantly reduce the prevalence of POD in elderly patients scheduled for radical esophagectomy, as well as reduce the expression of serum τ protein and Aβ protein postoperatively. In this study, the preventive effect of different doses of intranasal insulin on POD was explored to find a suitable dose and provide a reliable basis for widespread clinical use.
The present study had some limitations. First, we did not collect data on motor subtypes of delirium, the number of delirium episodes, or the duration of delirium. Second, according to preliminary experiments, a single nasal administration of 40 U insulin caused hypoglycemia in some patients. We did not evaluate whether the benefits of the dose outweighed the adverse effects. Third, different types of insulin were not studied.
Conclusion
Our trial results suggest that in elderly patients who undergo radical resection for esophageal cancer under combined thoracoscopy and laparoscopy, repeated intranasal injections of 30 U insulin may significantly reduce the prevalence of POD and the expression of τ and Aβ proteins at 3 days postoperatively. It should be emphasized that these results should be further confirmed in large multicenter trials, and intranasal insulin should be tested at more time points during the perioperative period.
Data Sharing Statement
The raw data for this study have been uploaded to www.medresman.org.cn and are also available from the corresponding author on reasonable request.
Acknowledgments
We would like to thank the medical staff at the Department of Anesthesiology for their support in this clinical trial. We would also like to thank Editage (www.editage.com) for English language editing.
Funding
This study was supported by the hospital management project of the General Hospital of the Western Theater Command (2021-XZYG-C25).
Disclosure
The authors certify that there are no conflicts of interest with any financial organization regarding the material discussed in the manuscript.
References
1. Takeuchi M, Takeuchi H, Fujisawa D, et al. Incidence and risk factors of postoperative delirium in patients with esophageal cancer. Ann Surg Oncol. 2012;19(12):3963–3970. doi:10.1245/s10434-012-2432-1
2. Ren A, Zhang N, Zhu H, et al. Effects of preoperative anxiety on postoperative delirium in elderly patients undergoing elective orthopedic surgery: a prospective observational cohort study. Clin Interv Aging. 2021;16:549–557. doi:10.2147/CIA.S300639
3. Shemesh E, Rudich A, Harman-Boehm I, et al. Effect of intranasal insulin on cognitive function: a systematic review. J Clin Endocrinol Metab. 2012;97(2):366–376. doi:10.1210/jc.2011-1802
4. Gaddam M, Singh A, Jain N. A comprehensive review of intranasal insulin and its effect on the cognitive function of diabetics. Cureus. 2021;13(8):e17219. doi:10.7759/cureus.17219
5. Hallschmid M. Intranasal insulin for alzheimer’s disease. CNS Drugs. 2021;35(1):21–37. doi:10.1007/s40263-020-00781-x
6. Renner DB, Svitak AL, Gallus NJ, et al. Intranasal delivery of insulin via the olfactory nerve pathway. J Pharm Pharmacol. 2012;64(12):1709–1714. doi:10.1111/j.2042-7158.2012.01555.x
7. Shpakov AO, Zorina II, Derkach KV. Hot spots for the use of intranasal insulin: cerebral ischemia, brain injury, diabetes mellitus, endocrine disorders and postoperative delirium. Int J Mol Sci. 2023;24(4):3278. doi:10.3390/ijms24043278
8. Huang Q, Li Q, Qin F, et al. Repeated preoperative intranasal administration of insulin decreases the incidence of postoperative delirium in elderly patients undergoing laparoscopic radical gastrointestinal surgery: a randomized, placebo-controlled, double-blinded clinical study. Am J Geriatr Psychiatry. 2021;29(12):1202–1211. doi:10.1016/j.jagp.2021.02.043
9. Tang X, Yv H, Wang F, et al. The relationship between suboptimal social networks and postoperative delirium: the PNDABLE study. Front Aging Neurosci. 2022;14:851368. doi:10.3389/fnagi.2022.851368
10. Chan CK, Sieber FE, Blennow K, et al. Association of depressive symptoms with postoperative delirium and CSF biomarkers for alzheimer’s disease among hip fracture patients. Am J Geriatr Psychiatry. 2021;29(12):1212–1221. doi:10.1016/j.jagp.2021.02.001
11. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J Pharmacol Pharmacother. 2010;1(2):100–107. doi:10.4103/0976-500X.72352
12. Su X, Meng ZT, Wu XH, et al. Dexmedetomidine for prevention of delirium in elderly patients after non-cardiac surgery: a randomised, double-blind, placebo-controlled trial. Lancet. 2016;388(10054):1893–1902. doi:10.1016/S0140-6736(16)30580-3
13. Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703–2710. doi:10.1001/jama.286.21.2703
14. Ely EW, Margolin R, Francis J, et al. Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Crit Care Med. 2001;29(7):1370–1379. doi:10.1097/00003246-200107000-00012
15. Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166(10):1338–1344. doi:10.1164/rccm.2107138
16. Wang C, Wu Y, Yue P, et al. Delirium assessment using Confusion Assessment Method for the Intensive Care Unit in Chinese critically ill patients. J Crit Care. 2013;28(3):223–229. doi:10.1016/j.jcrc.2012.10.004
17. Jinwu Q. Diagnosis and clinical management of hypoglycemia. J Clin Internal Med. 1990;23(02):12–14.
18. Tamasauskiene L, Gasiuniene E, Sitkauskiene B. Translation, adaption and validation of the total nasal symptom score (TNSS) for Lithuanian population. Health Qual Life Outcomes. 2021;19(1):54. doi:10.1186/s12955-020-01659-8
19. Yan T, Liang XQ, Wang GJ, et al. Prophylactic penehyclidine inhalation for prevention of postoperative pulmonary complications in high-risk patients: a double-blind randomized trial. Anesthesiology. 2022;136(4):551–566. doi:10.1097/ALN.0000000000004159
20. Li YW, Li HJ, Li HJ, et al. Delirium in older patients after combined epidural-general anesthesia or general anesthesia for major surgery: a randomized trial. Anesthesiology. 2021;135(2):218–232. doi:10.1097/ALN.0000000000003834
21. Allen SR, Frankel HL. Postoperative complications: delirium. Surg Clin North Am. 2012;92(2):409–31, x. doi:10.1016/j.suc.2012.01.012
22. Parker M, White M, Casey C, et al. Cohort analysis of the association of delirium severity with cerebrospinal fluid amyloid-tau-neurodegeneration pathologies. J Gerontol a Biol Sci Med Sci. 2022;77(3):494–501. doi:10.1093/gerona/glab203
23. Chen GF, Xu TH, Yan Y, et al. Amyloid beta: structure, biology and structure-based therapeutic development. Acta Pharmacol Sin. 2017;38(9):1205–1235. doi:10.1038/aps.2017.28
24. Sun ZD, Hu JX, Wu JR, et al. Toxicities of amyloid-beta and tau protein are reciprocally enhanced in the Drosophila model. Neural Regen Res. 2022;17(10):2286–2292. doi:10.4103/1673-5374.336872
25. Hoover BR, Reed MN, Su J, et al. Tau mislocalization to dendritic spines mediates synaptic dysfunction independently of neurodegeneration. Neuron. 2010;68(6):1067–1081. doi:10.1016/j.neuron.2010.11.030
26. Sayas CL, Medina M, Cuadros R, et al. Role of tau N-terminal motif in the secretion of human tau by end binding proteins. PLoS One. 2019;14(1):e0210864. doi:10.1371/journal.pone.0210864
27. Miller EC, Teravskis PJ, Dummer BW, et al. Tau phosphorylation and tau mislocalization mediate soluble Aβoligomer-induced AMPA glutamate receptor signaling deficits. Eur J Neurosci. 2014;39(7):1214–1224. doi:10.1111/ejn.12507
28. Xie Z, Swain CA, Ward SA, et al. Preoperative cerebrospinal fluid β-Amyloid/Tau ratio and postoperative delirium. Ann Clin Transl Neurol. 2014;1(5):319–328. doi:10.1002/acn3.58
29. Cunningham EL, McGuinness B, McAuley DF, et al. CSF beta-amyloid 1-42 concentration predicts delirium following elective arthroplasty surgery in an observational cohort study. Ann Surg. 2019;269(6):1200–1205. doi:10.1097/SLA.0000000000002684
30. Ballweg T, White M, Parker M, et al. Association between plasma tau and postoperative delirium incidence and severity: a prospective observational study. Br J Anaesth. 2021;126(2):458–466. doi:10.1016/j.bja.2020.08.061
31. Mao YF, Guo Z, Zheng T, et al. Intranasal insulin alleviates cognitive deficits and amyloid pathology in young adult APPswe/PS1dE9 mice. Aging Cell. 2016;15(5):893–902. doi:10.1111/acel.12498
32. Guo Z, Chen Y, Mao YF, et al. Long-term treatment with intranasal insulin ameliorates cognitive impairment, tau hyperphosphorylation, and microglial activation in a streptozotocin-induced Alzheimer’s rat model. Sci Rep. 2017;7:45971. doi:10.1038/srep45971
33. Chen Y, Run X, Liang Z, et al. Intranasal insulin prevents anesthesia-induced hyperphosphorylation of tau in 3xTg-AD mice. Front Aging Neurosci. 2014;6:100. doi:10.3389/fnagi.2014.00100
34. Zhang Y, Dai CL, Chen Y, et al. Intranasal insulin prevents anesthesia-induced spatial learning and memory deficit in mice. Sci Rep. 2016;6:21186. doi:10.1038/srep21186
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.