")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Effect of Omega-3 Fatty Acids on Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Authors Yu H , Su X, Lei T, Zhang C, Zhang M, Wang Y, Zhu L, Liu J
Received 27 July 2021
Accepted for publication 13 September 2021
Published 23 September 2021 Volume 2021:16 Pages 2677—2686
DOI https://doi.org/10.2147/COPD.S331154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Haichuan Yu,1,2 Xiaojie Su,1,2 Ting Lei,1,2 Chuchu Zhang,1,2 Meng Zhang,1,2 Yalei Wang,1,2 Lei Zhu,1,2 Jian Liu1,2
1Department of Intensive Care Unit, The First Hospital of Lanzhou University, Lanzhou, People’s Republic of China; 2The First Clinical Medical College of the First Hospital of Lanzhou University, Lanzhou City, People’s Republic of China
Correspondence: Jian Liu
Department of Intensive Care Unit, The First Hospital of Lanzhou University, No. 1, Donggang West Road, Chengguan District, Lanzhou City, Gansu Province, People’s Republic of China
Tel +86 136 0935 4197
Email [email protected]
Purpose: Omega-3 fatty acid is an emerging hotspot on anti-inflammation and chronic obstructive pulmonary disease (COPD) is known as a chronic inflammatory disease. The effect of Omega-3 fatty acid supplement on patients with COPD remains mixed for insufficient evidence. This systematic review and meta-analysis is based on neat randomized controlled trials trying to give a clearer impression on the effect of Omega-3 on patients with COPD.
Methods: This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) statements. Randomized clinical trials (RCTs) published in electronic databases including Medline, Embase, Cochrane Library, ClinicalTrials.gov and China National Knowledge Infrastructure (CNKI) by May 10, 2021 were searched. Data extracted from 6 predetermined domains (nutritional condition, lipid composition, inflammatory biomarker, lung function, physical endurance and quality of life [QoL]) were reviewed and analyzed.
Results: A total of 8 RCTs evaluating 418 patients (age, mean [SD] = 67.3 [10.2] years) were included. Statistical differences were found in 3 parameters of 3 domains – weight (Wt) (0.25 [95% CI, 0.02 to 0.48], P = 0.03) in nutritional condition, low-density lipoprotein (LDL) (0.70 [95% CI, 0.30 to 1.10], P = 0.00) in lipid composition and interleukin-6 (IL-6) level (− 0.32 [95% CI, − 0.60 to − 0.05], P = 0.02) in inflammatory biomarker – while no significant difference was found in lung function, physical endurance or QoL.
Conclusion: Comparing with placebo, Omega-3 intake was associated with more weight-gaining, LDL increase and IL-6 reduction. These results should be interpreted cautiously for the quality and quantity of available evidence are limited.
Keywords: COPD, omega-3 fatty acids, systematic review and meta-analysis
Introduction
Around the globe, COPD is now a tremendous social and medical burden with a point prevalence of 3.92% and the third highest mortality of 41.9 deaths per 100,000 a year.1,2 COPD is characterized by incompletely reversible limitation and chronic inflammation of the airway.2 Chronic inflammation locally causes reconstruction of the airway and systematically leads to weight loss. Moreover, weight loss was confirmed as an independent risk factor of mortality in COPD patients.3,4 Therefore, exerting intervention on COPD patients’ nutritional and inflammatory condition is vital to improve patients’ life quality and lighten the relative social burden.
Omega-3 fatty acids, also named n-3 poly-unsaturated fatty acids (n-3 PUFAs), are a special kind of lipid found to be a weight promoter in cachexia cancer patients.5,6 It is widely discussed as a potential anti-inflammatory factor,7 and has become a potential therapy method on anti-acute/chronic inflammation. It has lots of pathways that Omega-3 may have to function as an anti-inflammation factor mainly including competitively inhibiting Omega-6’s metabolism,8 directly or indirectly downregulating nuclear factor kappa-B (NF-ϰB).9 Theoretically, Omega-3 can reduce local or systemic inflammation to furthermore improve patients’ body weight, muscle volume and responses of other medical interventions and finally promote QoL through these pathways.7,10
Omega-3 has been discussed in many studies but its reported results on several respiratory diseases were inconsistent. A 2019 meta-analysis about Omega-3 and acute respiratory distress syndrome (ARDS) indicates that Omega-3 enteral supplement may be associated with an improvement in partial arterial O2 pressure (PaO2) to fraction of inspiration O2 (FiO2) ratio (PaO2/FiO2).11 While results of a 2006 systematic review and a 2009 meta-analysis about Omega-3 and asthma show unignorable inconsistency to aforementioned theoretical deductions.12,13
Based on previous practices on other respiratory diseases and its theoretical potential, a hypothesis presented that Omega-3 intake may be beneficial in COPD patients.14 Even though lots of observational studies reported results that seems to support the beneficial effect of Omega-3 on COPD patients, almost the same number of reports exist with contrary results, and a 2015 meta-analysis based on such studies concluded these evidences as “paucity”.15
Recently, more randomized controlled trials (RCTs) about COPD have been published, but just as former observational studies, contradictions among them are still not able to be diminished. For instance, on body weight, a study indicates that Omega-3 intake can cause weight-gaining,16 while another shows that no between-group differences can be observed in the Omega-3 group and the comparator group;17 on QoL, Kim et al found that Omega-3 intake may somehow improve patients’ QoL,18 but other studies show that Omega-3 intake is ineffective on such domain.17,19
Hence, it is now of great necessity to re-evaluate the effect of Omega-3 on patients with COPD to provide a clearer and more comprehensive understanding.
Methods
This systematic review and meta-analysis follows the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) statements (full checklist in Supplementary Table S1: PRISMA 2009 checklist).20 Protocol of this study was registered and artificially censored in the International Prospective Register of Systematic Reviews (PROSPERO #CRD42021249933).21
Search Strategy
Five databases including Medline, Embase, Cochrane Library, ClinicalTrials.gov and CNKI were searched for literatures published by May 10, 2021. To define the population, “chronic obstructive pulmonary disease” was combined by the Boolean operator “AND” with terms that potentially evaluated Omega-3 fatty acid supplementation such as “n-3 polyunsaturated fatty acid”, “fish oil”, etc. To limit the study design, the term “randomized controlled trials” was added to the search strategy with “AND” respectively. See detailed search strategy in Supplementary Data S2.
Study Selection
Only articles reporting RCTs written in English or Chinese were included. RCTs included must focus on the effect of Omega-3 intake (no matter how it was administered) on patients with spirometrically diagnosed COPD. All relevant publications were assessed separately by two researchers, and a third researcher re-assessed when there are different opinions about articles.
Data Extraction and Quality Assessment
A standardized data extraction chart was developed in advance. Two reviewers extracted the data separately and a third reviewer integrated if differences appeared. Risk of bias was evaluated by data-extractors utilizing Cochrane Collaboration risk of bias tool for RCTs.22
Outcome Measurements
At the stage of conception, we reviewed the hypothesis of the role Omega-3 may play in COPD, and roughly separated it into 2 groups: intrinsic one indicates the change that Omega-3 supplementation might cause in biochemical or pathophysiological aspects, including inflammation biomarker, lipid composition, lung function; extrinsic one presents the difference of clinical manifestation, including nutritional status, physical endurance, QoL. All of 6 domains in the 2 groups were considered as primary outcomes. In the actual data extraction stage, firstly we summarized parameters provided by included studies, and a parameter would be meta-analyzed only when it had been reported by at least 3 studies. If no parameter in a domain could be statistically synthesized, such domain would be analyzed only in the manner of systematic review.
Statistical Analysis
Given that the sample size of relative studies is generally too small to ignore the influence of baseline deviation, we conducted data synthesis and analysis procedure based on the principle of “change from baseline”. All data we extracted for pooling are continuous, so standardized mean difference (SMD) with 95% CI was utilized. The pooled effect size was calculated by the fixed-effects method in this study, but random-effects method would be chosen instead if the heterogeneity cannot be ignored. I2 test was conducted to quantify the heterogeneity among studies. Sensitivity analysis would be exerted if substantive heterogeneity existed. Publication bias would be tested by Egger’s test if the number of included studies is more than 10.23 Only when two-tailed P values were smaller than 0.05 could it be deemed as statistically significant.
We used R (version 4.0.4, meta package [version 4.18-1]) to do all statistical analysis.
The Engauge Digitizer (version 4.1) graphical data extraction software was used to extract data that were only provided by images.
Results
The literature search identified 217 studies, from which we finally included 8 studies with a total population of 418 (age, mean [SD], 67.3 [10.2]) (see Figure 1). Administrations of Omega-3 vary, but all of the studies administered standardized mixture of Omega-3 (some with vitamin D or other components). Baseline characteristics of population and details of administration are managed in Table 1.
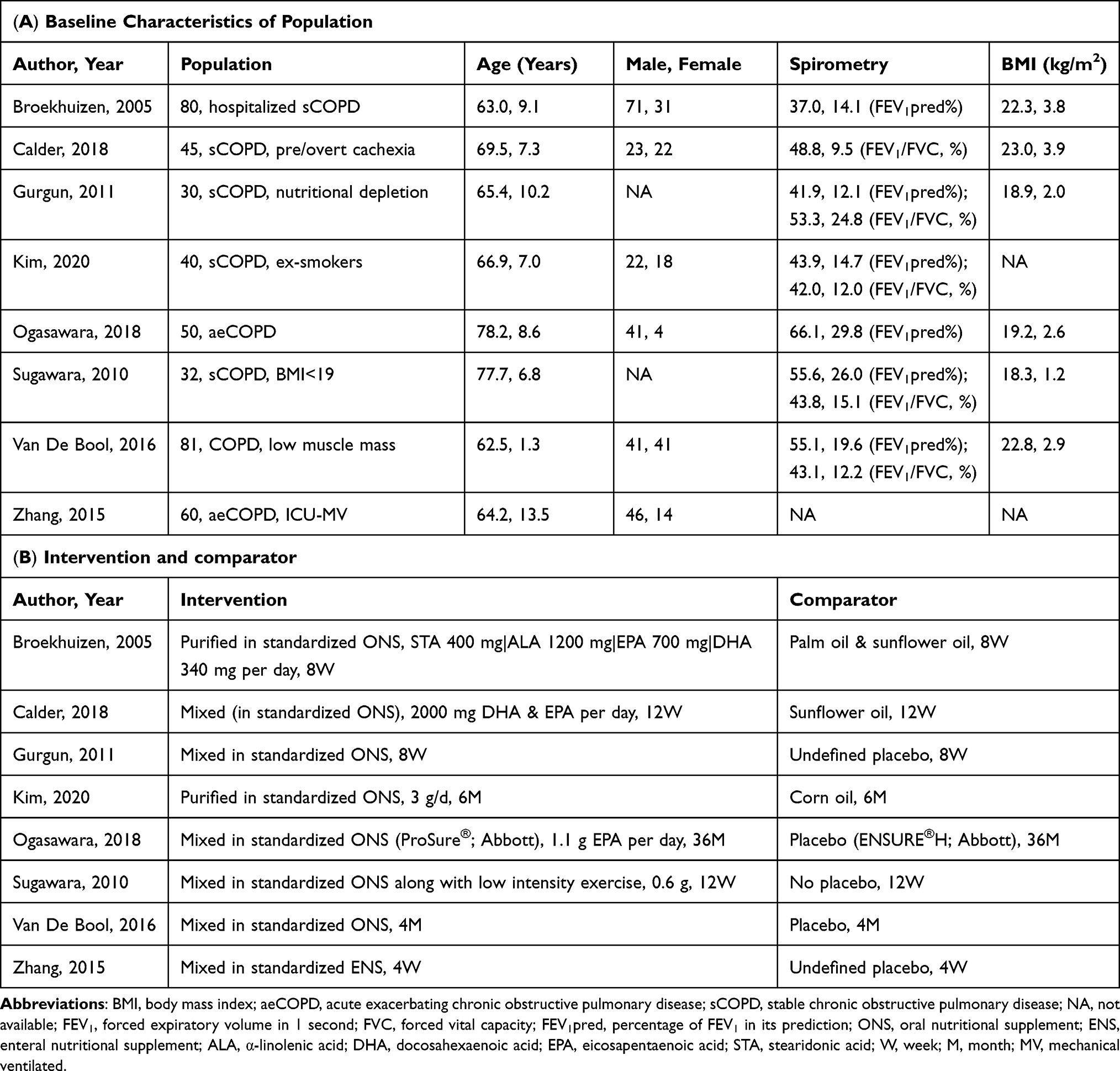 |
Table 1 Characteristics of Included Studies |
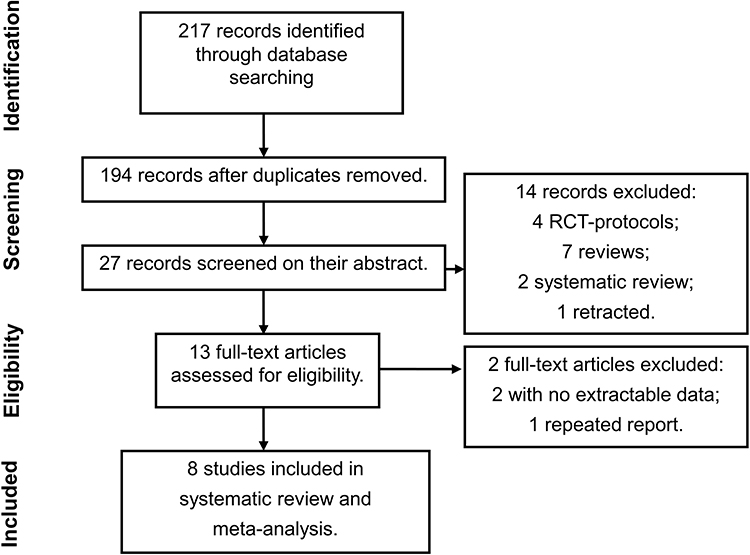 |
Figure 1 PRISMA flowchart. Notes: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. Creative Commons. |
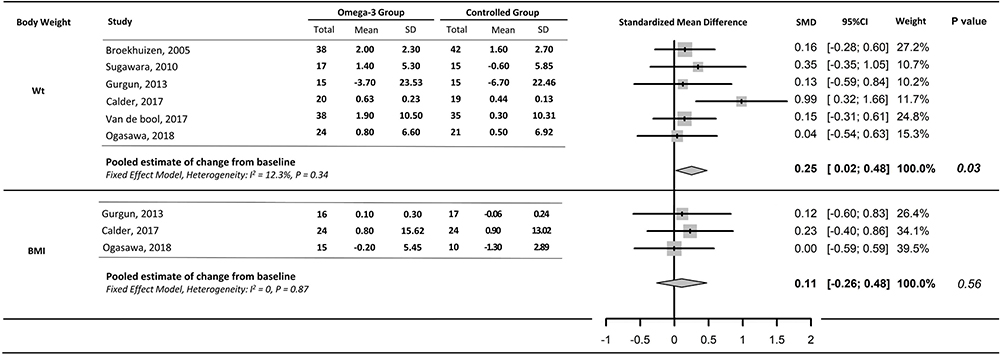 |
Figure 2 Pooled estimation of nutritional condition. |
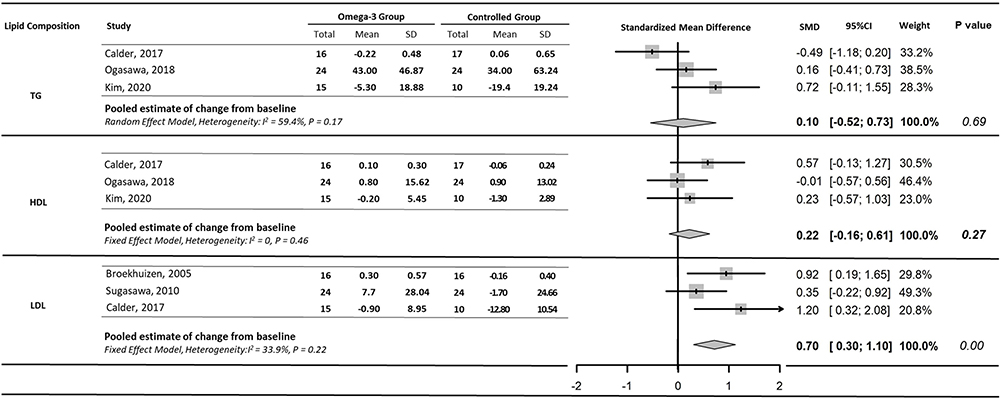 |
Figure 3 Pooled estimation of lipid composition. |
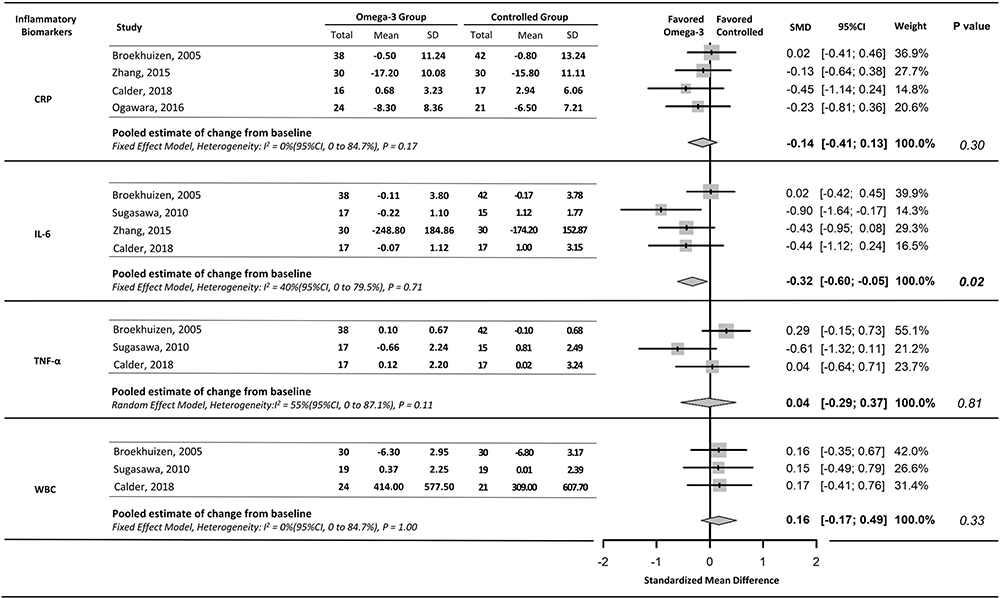 |
Figure 4 Pooled estimation of inflammatory biomarkers. |
Overall risk of bias was graded moderate to low mainly because uncertainty of randomization and sequence allocation (see full assessment in Supplementary Figure S3: Risk of bias across studies and Supplementary Table S4: Risk of bias in individual studies). It is unavailable to evaluate the publication bias for the quantity of included studies is too small (<10).23
For 6 pre-decided domains, we analyzed every parameter to decide those synthesizable ones. The criterion of inclusion for meta-analysis is that the data were reported by at least 3 studies and at the meantime extractable. Based on this criterion, we finally decided body weight and body mass index (BMI) in nutritional condition; blood concentrations of triglyceride (TG), high-density lipoprotein (HDL), LDL in lipid composition; blood concentration of C-reactive protein (CRP), IL-6, tumor necrosis factor-α (TNF-α) and white blood cell (WBC) in inflammatory biomarker; 6-minute walking distance (6MWD) in physical endurance; 2 scales including COPD assessment test (CAT) and St Georges’ respiratory questionnaire (SGRQ) in QoL. Lung function relating parameters would be presented in a manner of systematic review for the insufficiency and inconsistency of reports.
Sensitivity analysis was performed to exclude possible influence of heterogeneity on pooling results in each domain one by one. Results remain stable in those parameters with significant differences (see in Supplementary Figure S7: Sensitivity analysis results).
Nutritional Condition
Six studies are available for meta-analysis of body weight,17,19,24–27 and 3 for BMI.17,19,25 In the body weight group, 5 studies provided the body weight of participants,17,19,24,26,27 while the other LBM (Figure 2).25 Before pooling estimating, only 1 study indicated that Omega-3 could increase the body weight of the COPD population with statistical significance.17 Meta-analysis shows no statistical difference between Omega-3 supplemented population and controlled population in BMI (SMD, I2 = 0%, fixed effects model, 0.11 [95% CI, −0.26 to 0.59]). However statistical significance can be found when it comes to the body weight (SMD, I2 = 12.3%, fixed effects model, 0.25 [95% CI, 0.02 to 0.48], P = 0.03).
Lipid Composition
In this domain, TG, HDL and LDL were finally decided to be meta-analyzed for each of them was reported in 3 studies (Figure 3).17,18,25 There is no difference in TG (SMD, I2 = 59.4%, random effects model, 0.10 [95% CI, −0.52 to 0.73], P = 0.69) and HDL (SMD, I2 = 0, fixed effects model, 0.22 [95% CI, −0.16 to 0.61], P = 0.27) between 2 groups, but we found Omega-3 may be associated with higher concentration of blood LDL (SMD, I2 = 33.9%, fixed effects model, 0.70 [95% CI, 0.30 to 1.10], P = 0.00).
Inflammatory Biomarkers
CRP and IL-6 were separately reported in 4 studies,17,24–26,28 meanwhile white blood cell count (WBC) and TNF-α were separately reported in 3 studies (Figure 4).17,24–26,28 Between 2 groups of patients, no statistically significant difference was found in CRP (SMD, I2 = 12.6%, fixed effects model, −0.14 [95% CI, −0.41 to 0.13], P = 0.30), TNF-α (SMD, I2 = 55%, random effects model, 0.04 [95% CI, −0.29 to 0.37], P = 0.81) and WBC (SMD, I2 = 0, fixed effects model, 0.16 [95% CI, −0.17 to 0.49], P = 0.33). However, it was found that comparing with the placebo intaking group, the Omega-3 intaking group had statistically significant reduction on IL-6 level (SMD, I2 = 40%, fixed effects model, −0.32 [95% CI, −0.60 to −0.05], P = 0.02).
Physical Endurance
Five studies evaluated the 6MWD and were included in the evaluation of this domain (see Supplementary Figure S5: Pooled estimation of physical endurance). Although other data like 6-minute walking test BORG scale17–19 and steps per day16,25 were also reported by other included studies, we considered 6MWD sufficient and respective for pooling. No significant statistical difference can be found in the pooled results between the Omega-3 supplement group and the control group (SMD, I2 = 0%, fixed effects model, −0.02 [95% CI, −0.29 to 0.26], P = 0.90).
QoL
Four studies with a total population of 203 were included in this domain for meta-analysis (see Supplementary Figure S6: Pooled estimation of Quality of Life),17–19,25 all of them report no difference in both groups but Kim et al reports a 35% superiority (P = 0.01) of Omega-3 on the population of decreased SGRQ points more than 4.18 No significant difference can be found between the Omega-3 supplement group and the control group (SMD, I2 = 83%, random effect model, −0.31 [95% CI, −1.15 to 0.53], P = 0.47) in this domain.
Lung Function
Three studies mentioned the change of lung function before and after the intervention,17,18,24 but only 2 reported extractable data of different measurements,18,24 so we can do only systematic review rather than meta-analysis in this domain. Broekhuizen et al reported that no effect was observed on FEV1 and inspiratory strength without data shown in their article.24 Calder et al reported that no effect was observed on forced expiratory volume in 1 second (FEV1) (P = 0.37), while the intervention group exacerbated less than the controlled group (4.5% [n = 1] vs 13.6% [n = 3]).17 Kim et al reported the change of spirometry, but no statistical difference between groups was found also (FEV1, 0.002 [95% CI, −0.14 to 0.18]; FEV1%pred, 0.8 [95% CI, –4.8 to 6.4]; forced vital capacity (FVC), 0.1 [95% CI, −0.2 to 0.5]; FEV1/FVC, −0.01 [95% CI, −0.06, 0.04]; carbon monoxide diffusing capacity (DLCO), 0.2 [95% CI, −0.8 to 1.1], DLCO/VA (alveolar ventilation), 0.1 [95% CI, −0.1 to 0.3]).18 Overall, up to now there is no sufficient evidence that can support that Omega-3 may have positive effect on lung function of patients with COPD.
Discussion
Results show that Omega-3 intake does have some effects on weight-gaining, LDL increase and IL-6 reduction. No more significant difference can be found in physical endurance, QoL. In the domain of lung function, a small number of studies existed and the disparity of their results disenabled us to analyze its relationship with Omega-3.
In the domain of nutritional condition, we found that Omega-3 may have weight-gaining effect on patients with COPD. Nutritional condition is an important factor influencing the quality of life and prognosis in patients with COPD. Unhealthy nutritional condition can impair the QoL of patients with COPD.29 A Cochrane systematic review by Ferreira et al found that low BMI and fat-free mass index (FFMI) condition in a COPD population are related to a poor prognosis.30 And the weight-losing process of COPD patients is caused multifactorially by chronic inflammation and oxidant stress.10 It is shown in a study by Grimble et al that Omega-3 intake can inhibit the inflammatory process.31 And a series of studies showed that the metabolism of Omega-3 can produce anti-oxidative derivatives.32,33 The weight-gaining effect of Omega-3 on COPD patients found in our study indicates that the hypothesis that Omega-3 may improve COPD patients’ nutritional condition is tenable.
In the domain of lipid composition, we found that Omega-3 supplementation may cause LDL increase in COPD population. An overall increasing tendency of lipid can be observed in our study, but only the increase of LDL is statistically significant. First reason of this phenomenon may be that even though existing studies about the relationship of Omega-3, LDL, and health remain mixed,34 not few of them concluded the same result as us. For instance, Phillipson et al found that LDL decreased after 4 weeks of Omega-3 enriched diet.35 However, Gries et al found that Omega-3 supplement did not make any difference to participants’ concentration of blood lipid.36 Harris et al found that though very low-density lipoprotein (VLDL) decrease is positively related to the dose of Omega-3 intake, but LDL increased no matter what the dose is.37 The second reason may be the designs of included studies vary. For instance, Simopoulos suggests that LDL after Omega-3 supplement may increase if the intake of saturated fatty acids was not controlled,38 and none of the studies we reviewed did control the intake of saturated fatty acids. The third reason may be that the analysis was based on a limited number of included studies and small population. In a word, it is well proved that lipid metabolism was closely associated with inflammation,39 and HDL/LDL ratio may matter on COPD patients’ comorbidity (pulmonary hypertension, for example) and prognosis.40 Relationships of Omega-3 intake, different lipids and COPD are still confusing. More attention is needed on such problems.
In the domain of inflammatory biomarkers, our meta-analysis indicates that Omega-3 intake is significantly related to IL-6 reduction. COPD is characterized as a disease of chronic inflammation, and many studies strongly connect Omega-3 intake with lowering of inflammatory level.7 High IL-6, TNF-α level was found related to cachexia in cancer patients,41,42 and cachexia is not an uncommon condition in COPD patients. CRP and WBC are also confirmed as indicators of systemic inflammation in COPD patients.43 IL-6 is widely seen as a hub of various inflammatory pathways. As we comprehensively investigated series of inflammatory biomarkers including IL-6, CRP, WBC, and TNF-α, only IL-6 shows significance. Hence, albeit we found IL-6 reduction in our pooled results, it is insufficient to conclude that Omega-3 is capable of downregulating the COPD patients’ inflammatory level. More studies are needed to confirm the still-mixed Omega-3’s anti-inflammatory effect on COPD.
In the left domains, including patients’ physical endurance, lung function and QoL, although all of which were highly associated with the aforementioned 3 domains, we did not get enough evidence to support the relationship between Omega-3 and COPD.44 In our study, no significant effect was observed based on the pooling results of physical endurance and QoL. However, in the study by Kim et al, the effect that the Omega-3 group has significantly more SGRQ score-decreasing cases is still unignorable for our statistical pooling results were based on limited studies and small population.18 Future studies ought to pay extra attention to checking Omega-3’s effect on QoL closely. As for lung function, no parameter is available of statistical synthetization, and it seems no superiority of Omega-3 exhibited based on the results of our systematic review.
The results of this systematic review and meta-analysis should be interpreted quite cautiously for the limited quality and quantity of available evidence. Existing RCTs were limited by incomplete control (for instance, used regular vegetable oil instead of refined Omega-3 free oil to be the placebo), lacking detailed description of concealment approach (for example, Omega-3 and placebo ought to be encapsulated in the same nontransparent capsules), unbalanced follow-up, high dropout rates and the potential bias because of industrial funding. Additionally, most studies ignored to measure some fundamental clinical outcomes, such as change of lipid composition (especially the concentration if Omega-3, Omega-6 in the blood). Future studies may benefit from inclusion of clearly described concealment approach and comprehensive observation. More well-conducted RCTs are required to determine the comparative effectiveness of specific Omega-3 kinds (EPA vs DHA, for example) along with other treatment.
It ought to be noticed that a few limitations in this meta-analysis and systematic review itself can also impair the strength of evidence of our findings. The first point is that pooled results are all imprecise for the limited sample size and the majority of results did not show statistical significance. Second, though we excluded the potential effect by sensitivity analysis, heterogeneity related to outcome definitions, measurement tools (eg, different questionnaires to measure QoL) and administrations is still unignorable and therefore weakened the strength of evidence. Third, publication bias assessment was unable to be conducted for the small number of finally included studies.
Conclusion
In this systematic review and meta-analysis, we found that compared with placebo, Omega-3 intake was associated with weight-gaining, LDL increase and IL-6 reduction, while no significant difference in physical endurance, QoL or lung function was found. It should be emphasized that any interpretation based on the results of this study should be quite cautious for the quality of available evidence is limited, and the majority of outcomes was based on small numbers of studies.
Abbreviations
ARDS, acute respiratory distress syndrome; BMI, body mass index; CI, confidence interval; CNKI, China National Knowledge Infrastructure; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; DLCO, carbon monoxide diffusing capacity; FEV1, forced expiratory volume in 1 second; FFMI, fat-free mass index; FVC, forced vital capacity; HDL, high density lipoprotein; IL-6, interleukin-6; LDL, low density lipoprotein; MV, mechanical ventilated; NF-ϰB, nuclear factor kappa B; PRISMA, Preferred Reporting Items for Systematic Review and Meta-analyses; QoL, quality of life; RCT, randomized controlled trial; SD, standard difference; SMD, standardized mean difference; TG, triglycerides; TNF-α, tumor necrosis factor-α; VA, alveolar ventilation; VLDL, very low-density lipoprotein; Wt, weight.
Consent for Publication
All details of any images, videos, recordings, etc presented in this article can be published, and all authors agree with the article contents to be published. All authors are able to provide copies of signed consent forms to the journal editorial office if requested.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Projects of Gansu Province (grant number 18JR3RA344). Funder had no role in the design of the study, the collection and analysis of the data, or the preparation of the manuscript.
Disclosure
The authors report grants from Science and Technology Projects of Gansu Province, during the conduct of the study. There are no other conflicts of interest in this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. 2021 GLOBAL STRATEGY FOR PREVENTION, DIAGNOSIS AND MANAGEMENT OF COPD; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
3. Schols AM, Slangen J, Volovics L, Wouters EF. Weight loss is a reversible factor in the prognosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1791–1797. doi:10.1164/ajrccm.157.6.9705017
4. Saetta M, Turato G, Baraldo S, et al. Goblet cell hyperplasia and epithelial inflammation in peripheral airways of smokers with both symptoms of chronic bronchitis and chronic airflow limitation. Am J Respir Crit Care Med. 2000;161(3 Pt 1):1016–1021. doi:10.1164/ajrccm.161.3.9907080
5. Wigmore SJ, Ross JA, Falconer JS, et al. The effect of polyunsaturated fatty acids on the progress of cachexia in patients with pancreatic cancer. Nutrition. 1996;12(1 Suppl):S27–30. doi:10.1016/0899-9007(95)00078-X
6. Fearon KC, Von Meyenfeldt MF, Moses AG, et al. Effect of a protein and energy dense N-3 fatty acid enriched oral supplement on loss of weight and lean tissue in cancer cachexia: a randomised double blind trial. Gut. 2003;52(10):1479–1486. doi:10.1136/gut.52.10.1479
7. Calder PC. Polyunsaturated fatty acids, inflammation, and immunity. Lipids. 2001;36(9):1007–1024. doi:10.1007/s11745-001-0812-7
8. Lands WE, Libelt B, Morris A, et al. Maintenance of lower proportions of (n - 6) eicosanoid precursors in phospholipids of human plasma in response to added dietary (n - 3) fatty acids. Biochim Biophys Acta. 1992;1180(2):147–162. doi:10.1016/0925-4439(92)90063-S
9. Culp BR, Titus BG, Lands WE. Inhibition of prostaglandin biosynthesis by eicosapentaenoic acid. Prostaglandins Med. 1979;3(5):269–278. doi:10.1016/0161-4630(79)90068-5
10. Eid AA, Ionescu AA, Nixon LS, et al. Inflammatory response and body composition in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(8 Pt 1):1414–1418. doi:10.1164/ajrccm.164.8.2008109
11. Langlois PL, D’Aragon F, Hardy G, Manzanares W. Omega-3 polyunsaturated fatty acids in critically ill patients with acute respiratory distress syndrome: a systematic review and meta-analysis. Nutrition. 2019;61:84–92. doi:10.1016/j.nut.2018.10.026
12. Anandan C, Nurmatov U, Sheikh A. Omega 3 and 6 oils for primary prevention of allergic disease: systematic review and meta-analysis. Allergy. 2009;64(6):840–848. doi:10.1111/j.1398-9995.2009.02042.x
13. Reisman J, Schachter HM, Dales RE, et al. Treating asthma with omega-3 fatty acids: where is the evidence? A systematic review. BMC Complement Altern Med. 2006;6(1):26. doi:10.1186/1472-6882-6-26
14. Schols AM. Nutritional and metabolic modulation in chronic obstructive pulmonary disease management. Eur Respir J Suppl. 2003;46:81s–86s. doi:10.1183/09031936.03.00004611
15. Fulton AS, Hill AM, Williams MT, Howe PR, Coates AM. Paucity of evidence for a relationship between long-chain omega-3 fatty acid intake and chronic obstructive pulmonary disease: a systematic review. Nutr Rev. 2015;73(9):612–623. doi:10.1093/nutrit/nuv017
16. Van De Bool C, Ruten E, Van Helvoort A, Franssen F, Wouters E, Schols A. Physiological effects of nutritional supplementation as adjunct to exercise training in COPD patients with low muscle mass. The double blind, placebo controlled multi-centre NUTRAIN-trial. Eur Respir j Conf. 2016;48:nopagination.
17. Calder PC, Laviano A, Lonnqvist F, Muscaritoli M, Öhlander M, Schols A. Targeted medical nutrition for cachexia in chronic obstructive pulmonary disease: a randomized, controlled trial. J Cachexia Sarcopenia Muscle. 2018;9(1):28–40. doi:10.1002/jcsm.12228
18. Kim JS, Thomashow MA, Yip NH, et al. Randomization to omega-3 fatty acid supplementation and endothelial function in COPD: the COD-Fish randomized controlled trial. Chronic Obstruct Pulmonary Dis. 2020;8:1.
19. Gurgun A, Deniz S, Argin M, Karapolat H. The effects of nutritional supplementation added to pulmonary rehabilitation in muscle wasted chronic obstructive pulmonary disease: a randomised, controlled, prospective study. Am J Respir Crit Care Med. 2011;183:1.
20. Preferred Reporting VM. Items for systematic reviews and meta-analyses: the PRISMA statement. Revista Espanola De Nutrición Humana Y Dietética. 2009;18(3):e123.
21. Yu Haichuan SX, Ting L. Omega-3 fatty acids administration effects on chronic obstructive pulmonary disease patients: a systematic review and meta-analysis of randomized controlled trials. PROSPERO 2021 #CRD42021249933; 2021. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021249933.
22. Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane, 2021. Available fromwww.training.cochrane.org/handbook.
23. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
24. Broekhuizen R, Wouters EF, Creutzberg EC, Weling-Scheepers CA, Schols AM. Polyunsaturated fatty acids improve exercise capacity in chronic obstructive pulmonary disease. Thorax. 2005;60(5):376–382. doi:10.1136/thx.2004.030858
25. Ogasawara T, Marui S, Miura E, et al. Effect of eicosapentaenoic acid on prevention of lean body mass depletion in patients with exacerbation of chronic obstructive pulmonary disease: a prospective randomized controlled trial. Clin Nutr ESPEN. 2018;28:67–73. doi:10.1016/j.clnesp.2018.09.076
26. Sugawara K, Takahashi H, Kasai C, et al. Effects of nutritional supplementation combined with low-intensity exercise in malnourished patients with COPD. Respir Med. 2010;104(12):1883–1889. doi:10.1016/j.rmed.2010.05.008
27. van de Bool C, Rutten EPA, van Helvoort A, Franssen FME, Wouters EFM, Schols A. A randomized clinical trial investigating the efficacy of targeted nutrition as adjunct to exercise training in COPD. J Cachexia Sarcopenia Muscle. 2017;8(5):748–758. doi:10.1002/jcsm.12219
28. Zhang G, Zou J. [Clinical application of enteral immune nutrition for chronic obstructive pulmonary disease patients]. Zhonghua Yi Xue Za Zhi. 2015;95(19):1501–1504. Chinese.
29. Goris AHC, Schols AMWJ, Capm W-S, Wouters EFM. P.62 Tissue depletion in relation to physical function and quality of life in patients with severe chronic obstructive pulmonary disease. Clinical Nutrition. 1997;16:39. doi:10.1016/S0261-5614(97)80186-0
30. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;12:Cd000998.
31. Grimble RF, Howell WM, O’Reilly G, et al. The ability of fish oil to suppress tumor necrosis factor alpha production by peripheral blood mononuclear cells in healthy men is associated with polymorphisms in genes that influence tumor necrosis factor alpha production. Am J Clin Nutr. 2002;76(2):454–459. doi:10.1093/ajcn/76.2.454
32. Hong S, Gronert K, Devchand PR, Moussignac RL, Serhan CN. Novel docosatrienes and 17S-resolvins generated from docosahexaenoic acid in murine brain, human blood, and glial cells. Autacoids in anti-inflammation. J Biol Chem. 2003;278(17):14677–14687. doi:10.1074/jbc.M300218200
33. Serhan CN, Clish CB, Brannon J, Colgan SP, Chiang N, Gronert K. Novel functional sets of lipid-derived mediators with antiinflammatory actions generated from omega-3 fatty acids via cyclooxygenase 2-nonsteroidal antiinflammatory drugs and transcellular processing. J Exp Med. 2000;192(8):1197–1204. doi:10.1084/jem.192.8.1197
34. Ravnskov U, Diamond DM, Hama R, et al. Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review. BMJ Open. 2016;6(6):e010401. doi:10.1136/bmjopen-2015-010401
35. Phillipson BE, Rothrock DW, Connor WE, Harris WS, Illingworth DR. Reduction of plasma lipids, lipoproteins, and apoproteins by dietary fish oils in patients with hypertriglyceridemia. N Engl J Med. 1985;312(19):1210–1216. doi:10.1056/NEJM198505093121902
36. Gries A, Malle E, Wurm H, Kostner GM. Influence of dietary fish oils on plasma Lp(a) levels. Thromb Res. 1990;58(6):667–668. doi:10.1016/0049-3848(90)90314-3
37. Harris WS, Rothrock DW, Fanning A, et al. Fish oils in hypertriglyceridemia: a dose-response study. Am J Clin Nutr. 1990;51(3):399–406. doi:10.1093/ajcn/51.3.399
38. Simopoulos AP. Omega-3 fatty acids in health and disease and in growth and development. Am J Clin Nutr. 1991;54(3):438–463. doi:10.1093/ajcn/54.3.438
39. Ghoshal S, Witta J, Zhong J, de Villiers W, Eckhardt E. Chylomicrons promote intestinal absorption of lipopolysaccharides. J Lipid Res. 2009;50(1):90–97. doi:10.1194/jlr.M800156-JLR200
40. Li C, Yan L, Xu J. [Correlations between lipid ratio/oxidative stress status in COPD patients and pulmonary hypertension as well as prognosis]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2016;41(11):1168–1174. Chinese.
41. Brenner DA, O’Hara M, Angel P, Chojkier M, Karin M. Prolonged activation of jun and collagenase genes by tumour necrosis factor-alpha. Nature. 1989;337(6208):661–663. doi:10.1038/337661a0
42. Black K, Garrett IR, Mundy GR. Chinese hamster ovarian cells transfected with the murine interleukin-6 gene cause hypercalcemia as well as cachexia, leukocytosis and thrombocytosis in tumor-bearing nude mice. Endocrinology. 1991;128(5):2657–2659. doi:10.1210/endo-128-5-2657
43. Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59(7):574–580. doi:10.1136/thx.2003.019588
44. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.