")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Effect of Microbial Quality of Washing Water on Hand Hygiene Status of Food Handlers in Jimma Town: Implication for Food Hygiene and Safety
Authors Berhanu L , Mereta ST, Gume B, Kassa T , Berihun G , Dadi LS , Suleman S , Tegegne D, Getaneh A, Bedru H
Received 19 February 2021
Accepted for publication 29 April 2021
Published 19 May 2021 Volume 2021:14 Pages 1129—1134
DOI https://doi.org/10.2147/JMDH.S306359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Leykun Berhanu,1 Seid Tiku Mereta,2 Beje Gume,2 Tesfaye Kassa,3 Gete Berihun,1 Lelisa Sena Dadi,4 Sultan Suleman,5 Dechassa Tegegne,6 Assegid Getaneh,6 Habib Bedru7
1Department of Environmental Health Science, Wollo University, Dessie, Ethiopia; 2Department of Environmental Health Science and Technology, Jimma University, Jimma, Ethiopia; 3School of Medical Laboratory Science, Jimma, Ethiopia; 4Department of Epidemiology, Jimma University, Jimma, Ethiopia; 5Department of Pharmacy, Jimma University, Jimma, Ethiopia; 6Department of Veterinary Medicine, Jimma University, Jimma, Ethiopia; 7Jimma Zone Livestock and Fishery Development Office, Jimma, Ethiopia
Correspondence: Leykun Berhanu Email [email protected]
Background: In most cases, people pay more attention to the microbial quality of drinking water than the quality of water they used to wash hands. This may lead to the occurrence of various foodborne illnesses through the introduction of pathogenic microbes during preparation and serving of food.
Objective: To determine the effect of microbial quality of washing water on the hand hygiene status of food handlers in Jimma town.
Methods: Laboratory-based cross-sectional study design was used. A total of 150 food handlers were selected randomly for hand hygiene examination, and 150 water samples were collected aseptically from water storage tanks, food handlers used to wash their hands. The samples were subjected for microbiological analysis using standardized protocol. Descriptive statistics and Pearson correlation coefficient were used to summarize the data and to determine the effect of microbial quality of water on hand hygiene of food handlers, respectively.
Results: Among 150 food handlers included in the study, 104 (69.0%) of them were males and 64 (43.0%) of them aged between 35 and 50 years. On the other hand, 64 (42.7%) of the study participants had not attended formal education. About three-fourth of them used stored water to wash their hands, and almost similar proportion of them were waiters. The mean coliform bacteria of water and hand rinsate samples were 4.2 ± 0.8 and 4.1 ± 0.8 log CFU/mL, respectively.
Conclusion: The study revealed that the microbial quality of water used to wash hands significantly affects the hand hygiene status of the food handlers. Hence, improving the microbial quality of washing water is important to improve the hand hygiene status of food handlers and consequently to prevent the occurrence of food-borne illness in the town.
Keywords: Jimma town, hand hygiene, stored water, food handler, hand rinsate
Introduction
A food handler is any person who prepares or serves food in food establishments. The hands of food handlers are a major vehicle of food contamination so that improved personal hygiene and handwashing would lead to the basic control of faeces to hand-to-mouth spread of potentially pathogenic microorganisms.1–3 Unwashed hands or hands washed with contaminated water pose a risk for higher levels of hand contamination.4 Escherichia coli measured on hands after hand washing has been found to have significant association with E. coli concentration in the hand washing water.5,6
Consumption of contaminated food may result in foodborne illness, which remains a major public health problem affecting about one-third of the population in developed countries. In the USA during 2017,841 foodborne outbreak was reported from 50 states, resulting in 14,481 illnesses, 827 hospitalization, and 20 deaths. A single etiologic agent was confirmed in 395 (47%) of the total outbreak, resulting in 8,954 (62%) illnesses. Bacterial was the leading etiologic agents. Consumption of contaminated mollusks, fish, chicken, and beef were the major causes of foodborne outbreaks. Scombroid, ciguatoxin, and salmonella in fish, and Clostridium botulinum in herbs were the most common confirmed etiologic agents where restaurants were found to be the sources for 44% of the illnesses.7
In developing countries, consumption of contaminated foods is also responsible for a wide range of diseases, including cholera, campylobacteriosis, E. coli gastroenteritis, salmonellosis, shigellosis, typhoid and paratyphoid fevers, brucellosis, amoebiasis and poliomyelitis, which accounted about 70% of diarrheal diseases.8
In Ethiopia, even though foodborne diseases are rarely investigated and under-reported, it is a major public health problem. Salmonella spp.,Shigella spp.,Staphylococcus aureus, E. coli O157:H7, Listeria spp., and Bacillus cereus were the major causes of foodborne outbreak identified from raw meat, dairy products, ice cream, chicken, and Pizza in many towns of the Ethiopia such as Modjo, Bishoftu, Jimma, Bahir Dar, Gondar, and Addis Ababa, the capital City of Ethiopia. Bacteria are responsible for more than 90% of the foodborne illnesses.4,9
A study conducted in Tigray Region, in Ethiopia, indicated that about 63% of the study participants harboured one or more of intestinal parasites, including; Entamoeba histolytica, Salmonella and Shigella species, which indicates poor food handling practices undertaken by the food handlers.10,11 Absence of food safety laws, poor handling and sanitation practice of the food, weak regulatory systems, poor personal hygiene of food handlers were the major causes of foodborne illness where contaminated hands contribute more in this regard.4,9
Hand washing is therefore a fundamental precautionary measure to reduce the transfer of bacteria, this transfer can occur from person to person or from bacterial counts of from water having increased bacterial counts used to process food in catering establishments to food contact surfaces.4 Water used to wash hands before or during food preparation, and serving should be of the same good quality as for human consumption; This water should be free from fecal coliforms and pathogenic microorganisms.12 In most cases, people worried about the quality of water used for drinking but give little attention to the quality of water they used to wash hands.
Many towns in Ethiopia do not have continuous water supply of tap water. Due to this, stored water is commonly used to wash hands in food service establishments. Hence, investigation of hand contamination of food handlers could have of great importance to understand the hygienic practice of food handlers and consequently to reduce foodborne disease. In Jimma Town, the hand hygiene status of food handlers and its connection with the microbial quality of washing water is not studied. Therefore, this study aimed to determine the effect of microbial quality of washing water on the hand hygiene status of food handlers.
Methods
Study Area Description
The study was conducted in Jimma Town located 356 km to southwest of Addis Ababa at a latitude range from 7013ʹ to 8056 ‘N and longitude range 35052ʹ to 37037ʹ E at an elevation ranging from 880 meters to 3360 meters above sea level. The town receives a mean annual rainfall of about 1530 millimeters, which comes from the long and short rainy seasons.13 According to the population projection conducted by the central statistical agency of Ethiopia, there are 177,943 people of whom 89,233 are women.14 The town serves as a business center for the surrounding areas leading to the increment of food service centers. Lack of regular monitoring on the sanitary condition of these establishments is a great problem in foodservice investment.15
Sample Size and Sampling Technique
For this study, 150 food-service establishments were selected using simple random sampling techniques. The list of food service establishments was obtained from Jimma Town administration and used as a sampling frame. Then, simple random sampling technique was used to select food service establishment from the list. One-food handler from each establishment was selected randomly for hand hygiene examination, making the total hand rinsate sample to be 150. In addition, 150 water samples were collected for microbial investigation.
Sample Collection and Analysis
Before sample collection, verbal consent was obtained from food service establishment management and from each food handler. From each of the selected cafeterias, restaurants and hotels, 100 mL water samples were collected directly from tap water and water storage tanks from where the food handlers use to wash their hands. In addition, 150 hand rinsate samples were collected by swabbing using sterile cotton headed swabs from both hands of the food handlers working in the selected cafeterias, restaurants and hotels using a sterile template measuring 2.5×2.5 cm2. The sample was collected after the food handlers washed their hands and get dried. Hand rinsate sample was taken directly from both hands of food handlers. Thereafter, the swab stick was placed into the tubes containing 9 mL sterile peptone water. Finally, the tubes and water samples were labeled and put into cold box with an ice pack and transported to the Laboratory of Environmental Health Science and Technology Department in Jimma University for analysis within four hours of collection.16
In the laboratory, serial dilution was made by transferring one mL sample into the first test tube containing nine mL sterilized peptone water to make 10−1 dilution. Then, one mL from the first tube was transferred to a second test tube containing nine mL sterilized peptone water to give 10−2 dilution and the process is continued similarly until the desired dilution is obtained. One mL diluent from the appropriate dilution was taken and spread plated in triplicate onto a separate plate containing sterilized MacConkey agar (Oxoid, UK) and incubated at 37°C and 44°C for 24 hours. Colonies appearing pink to red were identified as coliform and E. coli bacteria, respectively.17–19
Data Quality Assurance
Close supervision was conducted during the actual sample collection. All sample analyses were carried out in triplicate with its control. All media and reagents used were up to date, and all microbiological analysis was carried out inside level II biosafety cabinet (BDK, Genkingen, Germany). All culture media and materials were sterilized using autoclave (Astell, England). The adequacy of sterilization was also assured using sterilization indicator.
Statistical Analysis
The laboratory results were recorded on each day of counting. Each bacterial count was transformed to log values. Descriptive measures including mean and standard deviation were used. To determine the relationship between water quality and the hand hygiene status of the food handlers, the Pearson correlation coefficient was calculated. P < 0.05 was considered statistically significant.
Results and Discussion
Socio-Demographic Characteristics of the Study Subjects
Out of 150 respondents from establishments included in the study, 104 (69.0%) of them were males and 64 (43.0%) of them aged between 35 and 50 years. On the other hand, 64 (42.7%) of the study participants had not attended formal education, whereas similar proportion of the study participants, 61 (40.7%), reported to have attended elementary schools. In addition, 41.3% of them had food handling experience of 1 to 2 years while about a third of them had experience of 3 to 5 years. About three-fourth of them used stored water to wash their hands, and almost similar proportion of the study participants were waiters (Table 1).
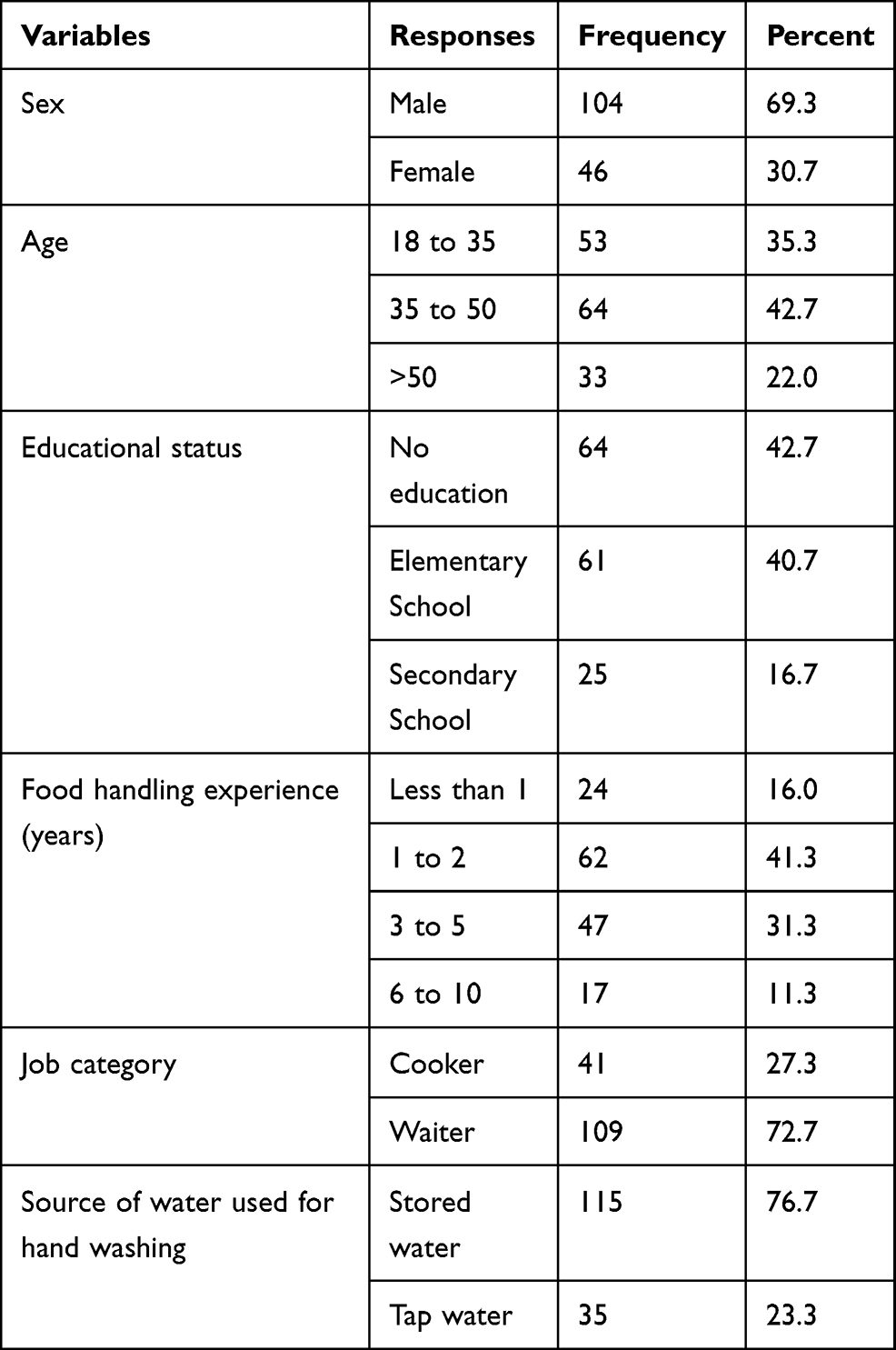 |
Table 1 Socio-Demographic Characteristics of the Food Handlers Working in Jimma Town Food Service Establishments |
Keeping good hand hygiene practice is an important means of preventing the occurrence of foodborne illness as contaminated hands serve as a vehicle for microorganisms causing a potential risk to public health.1 In this study, the mean coliform and E. coli count of water samples were 5.4 and 5.0 log CFU/mL, respectively, while the mean coliform and E. coli count of the hand rinsate samples were 4.9 and 4.2 log CFU/mL, respectively (Table 2). The high coliform bacteria in a washing water sample indicates that effective hygienic practices were not implemented during the storage, handling, and collecting of water at the point of processing.20 In this study about three-fourth of the food handlers used stored water to wash their hands. This implies that there is a possibility of transferring diseases causing agents from the hand washing water to the hands of food handlers and then to the food they handle. This may cause various foodborne diseases to the consumers.
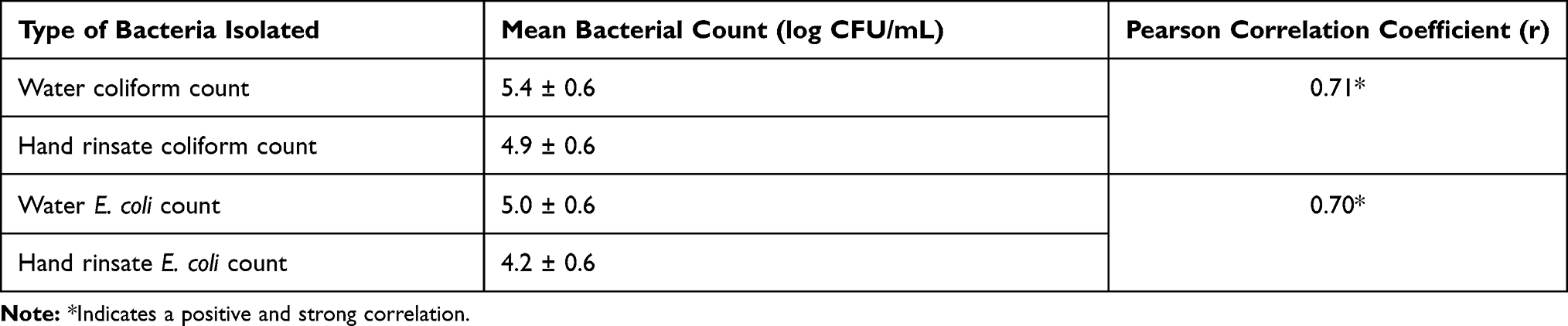 |
Table 2 Correlation Between Mean Bacterial Counts of Water and Hand Rinsate Samples in Food and Drinking Establishments of Jimma Town |
The presence of E. coli in hands of food handlers indicates inadequate washing or washing hands using contaminated water.1 All of the analyzed hand rinsate and washing water samples had been contaminated with one or more coliform and E. coli bacteria. This value is much higher than the finding of the study done by Allam et al1 and Banik et al,21 where the prevalence of E. coli bacteria was found to be 41.7% and 20.7%, respectively. This level of E. coli in the hands of food handlers in the present study may indicate inadequate hand washing practices or using microbiologically poor water quality for hand wash. Since E. coli is found in the intestinal tract of human beings and other warm-blooded animals, the presence of this organism in the hands of food handlers is an indication of fecal contamination. Fecal contamination in turn indicates the presence of other harmful organisms.4 This situation leads to the transfer of microorganisms to the hands in the process of washing and then to the food they prepared.22 It is known that E. coli has frequently been implicated as the causative agent of diarrhea, urinary tract infection, hemorrhagic colitis, and hemorrhagic uremic syndrome.20 Hence, improving the microbial quality of washing water and following appropriate hand hygiene practices are of paramount importance in preventing the occurrence of foodborne infection and intoxication among the consumers.
According to Codex Alimentarius Commission, improper food handling is one of the main causes of food contamination with poor hand hygiene representing a major risk factor. In the present study, a positive and strong correlation (r = 0.71; P ≤ 0.001) was observed between the microbial quality of washing water and the hands of food handlers. Similarly, E. coli count from water and hand rinsate had a positive and strong relationship (r = 0.70; p ≤ 0.001) (Table 2). This finding is supported by Daneshmand et al6 that showed E. coli counts of washing water had a significant association with the E. coli counts of hands after washing.
Conclusions
This study revealed that both the microbial quality of hand washing water and the hands of food handlers were poor. The quality of water used by the food handlers to wash their hands had a great effect on the hand hygiene status of food handlers. Hence, Jimma town water and sewerage authority in collaboration with café and restaurant owners should regularly check the water pipeline and train food handlers about the importance of using quality water to improve hand hygiene. Food handlers should avoid using stored water if possible. Food service establishment owners in collaboration with the town health department should regularly monitor the hand hygiene status of food handlers in Jimma food establishment. Further study should be performed to quantify the level of pathogenic microorganisms in washing water and hands of food handlers.
Data Sharing Statement
All the data of the manuscript can be obtained from the corresponding author upon request.
Ethical Consideration
The study was conducted following a set of ethical principles for medical principles involving human research that was initially adopted by the 18th Assembly of the World Medical Association in Helsinki. Ethical clearance was obtained from the ethical review board of Jimma University Institute of Health. Verbal permission was also obtained from the establishments’ management before collecting hand rinsate. It was difficult to obtain written consent from study participants since not all of the respondents were not educated. Consequently, verbal consent was obtained from study participants before the hand rinsate samples were taken after obtaining approval from the ethical review board. All the information obtained from each study participant was kept confidential.
Acknowledgments
Firstly, the authors would like to thank Jimma University for covering the cost of the study. The authors would also like to acknowledge the research assistant for collecting and analyzing samples. Environmental Health Science and Technology Laboratory is also acknowledged for allowing the laboratory facility. The authors are grateful to the owners of food service establishments and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allam HK, Al-Batanony MA, Seif AS, Awad ET. Hand contamination among food handlers. Br J Biomed Sci. 2016;13(5):1–8.
2. Baluka SA, Miller R, Kaneene JB. Hygiene practices and food contamination in managed foodservice facilities in Uganda. J Food Sci. 2015;9(1):31–42.
3. Lani MN, Mohdazmi MF, Ibrahim R, Alias R, Hassan Z. Microbiological quality of food contact surfaces at selected food premises of Malaysian heritage food (“Satar”) in Terengganu, Malaysia. Int J Eng Sci. 2014;3(9):66–70.
4. Lambrechts AA, Human IS, Doughari JH, Lues JFR. Bacterial contamination of the hands of food handlers as an indicator of hand washing efficacy in some convenient food industries. Pak J Med Sci. 2014;30(4):755–758.
5. Verbyla ME, Pitol AK, Navab-Daneshmand T, Marks SJ, Julian TR. Safely managed hygiene: a risk-based assessment of handwashing water quality. Environ Sci Technol. 2019;53:2852–2861. doi:10.1021/acs.est.8b06156
6. Navab-daneshmand T, Friedrich ND, G¨achter M, et al. Escherichia coli contamination across multiple environmental compartments (soil, hands, drinking water, and handwashing water) in urban Harare: correlations and risk factors. Am J Trop Med Hyg. 2018;98(3):803–813. doi:10.4269/ajtmh.17-0521
7. Center for Diseases Control and Prevention. Surveillance for foodborne disease outbreaks United States, 2017: annual report. 2017. Available from: www.cdc.gov/mmwr/volumes.
8. Ifeadike CO, Ironkwe OC, Adogu OU, Nnebue CC. Assessment of the food hygiene practices of food handlers in the Federal Capital Territory of Nigeria. Tro J Med Res. 2014;17(1):10–15. doi:10.4103/1119-0388.130175
9. Ayana Z, Yohannis M, Abera Z. Foodborne bacterial diseases in Ethiopia. Acad J Nutr. 2015;4(1):62–76.
10. Chekol FA, Melak MF, Belew AK, Zeleke EG. Food handling practice and associated factors among food handlers in public food establishments, Northwest Ethiopia. BMC Res Notes. 2019;12(1):1–7. doi:10.1186/s13104-019-4047-0
11. Mardu F, Negash H, Legese H, et al. Assessment of knowledge, practice, and status of food handlers toward Salmonella, Shigella, and intestinal parasites: a cross-sectional study in Tigrai Prison Centers, Ethiopia. PLoS One. 2020;15(11November):1–13. doi:10.1371/journal.pone.0241145
12. Esterhuizen L. Drinking water quality and farming practices on dairy farms in the greater Mangaung Metro, South Africa. 2014.
13. Gashaw A, Gebrehiwot E. Study on milk hygiene, quality control in the market chain in Jimma. Adv Dairy Res. 2018;6(3):1–8.
14. Central Statistical Agency. Federal democratic Republic of Ethiopia. Population projection of Ethiopia for all regions at district level from 2014–2017. 2013.
15. Neme K, Hailu B, Belachew T. Assess sanitary condition and food handling practices of restaurants in Jimma Town, Ethiopia: implication for foodborne infection and food intoxication. Food Sci Qual Manag. 2017;60:1–9.
16. Hannan A, Shan S, Arshad M. Bacteriological analysis of drinking water from 100 families of Lahore by membrane filtration technique and chromagar. Biomedica. 2010;26:152–156.
17. Birgen BJ, Njue LG, Kaindi DM, Ogutu FO, Owade JO. Determinants of microbial contamination of street-vended chicken products sold in Nairobi Country. Int J Food Sci. 2020;2020:1–8. doi:10.1155/2020/2746492
18. Kaddumukasa PP, Imathiu SM, Mathara JM, Nakavuma JL. Bacterial contamination of selected fruits, fresh juice contact surfaces and processor’s hands: potential risk for consumers’ health in Uganda. J Food Sci Nutr Res. 2019;2(3):199–213. doi:10.26502/jfsnr.2642-11000020
19. Homaida MA, Goja AM. Microbiological quality assessment of drinking water at Ed-Dueim Town. New York Sci J. 2013;6(5):1–8.
20. Tadesse T, Atnafu T, Kejela T. Bacteriological quality of hand washing water in hotels and restaurants of Ilu Aba Bora Zone, Oromia Region, Southwestern Ethiopia. Life Sci. 2017;2:255–269.
21. Banik S, Chakrabarty S, Das N. Hand hygiene in food handlers working in canteens of an educational institution in Eastern India. Int J Community Med Public Health. 2020;7(7):2602–2606. doi:10.18203/2394-6040.ijcmph20202983
22. Lues JFR, Van Tonder I. The occurrence of indicator bacteria on hands and aprons of food handlers in the delicatessen sections of a retail group. Food Control. 2007;18(4):326–332. doi:10.1016/j.foodcont.2005.10.010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.