")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Effect of Lowering the Blood Alcohol Concentration Limit to 0.03 Among Hospitalized Trauma Patients in Southern Taiwan: A Cross-Sectional Analysis
Authors Huang CY, Chou SE, Su WT, Liu HT, Hsieh TM, Hsu SY, Hsieh HY, Hsieh CH
Received 21 February 2020
Accepted for publication 20 May 2020
Published 16 June 2020 Volume 2020:13 Pages 571—581
DOI https://doi.org/10.2147/RMHP.S250734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Chun-Ying Huang,1,* Sheng-En Chou,1,* Wei-Ti Su,1 Hang-Tsung Liu,1 Ting-Min Hsieh,1 Shiun-Yuan Hsu,1 Hsiao-Yun Hsieh,2 Ching-Hua Hsieh2
1Department of Trauma Surgery, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University and College of Medicine, Kaohsiung 83301, Taiwan; 2Department of Plastic Surgery, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University and College of Medicine, Kaohsiung 83301, Taiwan
*These authors contributed equally to this work
Correspondence: Ching-Hua Hsieh
Department of Plastic Surgery, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Taiwan
Tel +886-7-7327476
Email [email protected]
Background: In June 2013, the legal blood alcohol concentration (BAC) limit for driving was lowered from 0.05 to 0.03 mg/mL in Taiwan. Thus, this study aimed to assess the epidemiological changes in terms of drinking among drivers in southern Taiwan before and after the law was imposed.
Methods: Only patients who had undergone the BAC test at the emergency room were included in the study. The patients during the study period before (n = 2735) and after (n = 2413) the implementation of the law were selected for comparison. Drunk patients were defined as those who had a BAC ≥ 0.005 and were considered as driving under the influence (DUI) of alcohol. Meanwhile, driving while intoxicated (DWI) was defined as a BAC ≥ 0.05, which was the level adopted in the new law.
Results: Since the BAC limit lowered to 0.03, the number of DUI patients significantly decreased from 340 (12.4%) to 171 (7.1%), and that of DWI patients significantly reduced from 273 (10.0%) to 146 (6.1%) based on the alcohol test. In addition, after the implementation of the law, the number of associated injuries did not significantly decrease from that before the law was implemented in patients involved in alcohol-related crashes.
Conclusion: After lowering the legal BAC limit from 0.05 to 0.03, responsiveness to the change in law was observed among the studied population. However, such responsiveness may not be observed in some citizens who may need special interventions to help reduce their behavior of drinking and driving.
Keywords: alcohol, blood alcohol concentration, BAC, driving under the influence (DUI) of alcohol, driving while intoxicated, DWI, alcohol-related crashes, law sanction, mortality
Background
Drinking is one of the major risk factors of traffic crashes. Approximately one-third of individuals who died from traffic crashes are intoxicated.1 The association between blood alcohol concentration (BAC) and driving skill had been widely studied. A significant decrease in driving skills was noted in drivers with a BAC of 0.05 g/dL in a review of 112 studies.2 In single-vehicle crashes, the relative risk for fatality in drivers with BACs of 0.05–0.079 is 7–21 times higher than those with a BAC of 0.00.3 The risk of fatal traffic accidents among drivers with BAC between 0.021 and 0.05 was 3.8 times higher than that of drivers with a BAC of 0.00.4 Laboratory studies have also revealed that impaired driving increased with elevated alcohol level, beginning at a BAC of 0.01 up to a BAC of 0.24.5 In motor vehicle accidents, drivers with a BAC=0.01 are 46% more likely to be blamed for a crash than sober drivers.5 One large-scale study on traffic crashes in the United States has found that even minimally buzzed drivers (BAC=0.01) are significantly more dangerous than those who are sober.6
In the United States, the legal BAC limit is generally 0.08. However, the value varies per state and has changed over the years.7 In most countries worldwide, the legal limit of BAC is 0.05.8,9 While Japan and Poland have a legal BAC limit of 0.03,9,10 Norway, Sweden, and Russia have a legal BAC limit of 0.02,11,12 and Vietnam even has a zero tolerance for drivers of all motorized vehicle except motorcyclists.13 A number of studies had shown a reduction in the BAC level at which individuals can legally drive to effectively reduce alcohol-related traffic crashes.3,8,10,14-17 The lowering of the illegal level of BAC from 0.10 to 0.08 resulted in reductions in alcohol-related crashes and fatalities up to 5%–16%.3,8 After lowering the BAC legal limit from 0.08 to 0.05, the fatal crashes involving drunk drivers decreased to at least 5%–8% and up to 18% in other countries,17–20 and the number of fatalities reduced from approximately 100 to 64 after implementing the law in France,21 and an overall 9.4% decrease in alcohol-related crashes was observed in Austria.18 Furthermore, the lowering of the legal BAC limit from 0.05 to 0.03 in Japan led to a reduction in alcohol-related crashes by 50% and 52% in adult men and women, respectively, as well as by 64% in teenagers.10
In Taiwan, a series of amendments were made in relation to the Road Traffic Management and Penalty Act, Road Traffic Security Rules, and Article 185 of the Criminal Law22 in 2013 to lower the BAC legal limit from 0.05 to 0.03. Furthermore, the penalties were increased from New Taiwan Dollars (NTD) 15,000–60,000 (~$500–2000) to NTD 15,000–90,000 (~$500–3000) according to the BAC and the type of vehicle used (motorcycle, car, or bus). Driving with a BAC of 0.05 or higher is considered a criminal act, and some administrative penalties, such as license suspension or revocation, may be imposed. According to the national traffic statistics, the number of casualties from drunk driving reduced after implementing these sanctions.22 Moreover, after the BAC limit change, airbag use in car crashes (OR: 0.30, 95% CI 0.10 to 0.88, p=0.007) and helmet use in motorcycle crashes (OR: 0.20, 95% CI 0.15 to 0.26, p<0.001) was lower in DUI patients than non-DUI patients.23 However, data about the effectiveness of lowering the legal BAC limit on injuries and mortality among drunk drivers involved in alcohol-related crashes are not available. Using the registered trauma data from the hospital, this study aimed to assess the epidemiological change in the behavior of drunk drivers in southern Taiwan before (from July 2009 to December 2012) and after (from July 2013 to December 2016) the implementation of the law.
Methods
The institutional review board (IRB) of the Kaohsiung Chang Gung Memorial Hospital, a level I regional trauma center in southern Taiwan,24–26 had approved this study (reference number: 201600001B0). Due to the retrospective nature of the study that used registered data from a trauma database, the need for informed consent waived off according to the regulation of the IRB. The study protocol conforms to the ethical guidelines of patient data confidentiality and compliance with 1975 Declaration of Helsinki. This study included all patients with trauma who had been suspected with drunk driving and admitted for treatment. Only the patients who had undergone the BAC test at the emergency room were included. Those with incomplete data were excluded. This study was designed to compare the occurrence of drunk driving during the 2-year study period before and after the law was imposed. Implementation of the revised part of the Road Traffic Act in Taiwan that lowered the legal limit for drivers from a BAC level of 0.05 to 0.03 with increased penalties was executed in June 13, 2013. In this study, due to some minor revisions during the propaganda that occurred approximately 6 months before the legislation, the patients were selected based on the two time periods for comparison: from January 1, 2011 to December 31, 2012 (a 2-year period before imposing the law) as well as from July 1, 2013 to June 30, 2015 (a 2-year period after imposing the law). Drunk patients were defined as those who had a BAC ≥ 0.005 and were considered as driving under the influence (DUI) of alcohol. Meanwhile, driving while intoxicated (DWI) was defined as a BAC ≥ 0.05, which was the level adopted in the new law. The term alcohol-related crashes indicated a traffic accident involving DUI or DWI patients. Those with a BAC < 0.005 were not considered drunk. The following data about the patients were obtained: age; sex; trauma mechanism (driver or passenger; motor vehicle or motorcycle); BAC at the emergency room; Glasgow Coma Scale (GCS) score; abbreviated injury scale (AIS) score and associated injuries in six body regions; injury severity score (ISS); length of stay (LOS) in the hospital; rates of admission in the intensive care unit (ICU); in-hospital mortality; and the expenditure in total and per patient, including cost of operation (operation and operation supplies), cost of examination (physical examination, hematology test, pathological examination, radiography, electrocardiography, echography, endoscopy, electromyography, cardiac catheterization, and electroencephalography), cost of medicines (medicine and medicine services), and cost of other fees (administrative fees).
We used the Statistical Package for the Social Sciences software version 22.0 (IBM Corp., Armonk, NY) for statistical analysis. In-hospital mortality was the primary outcome; LOS in the hospital and the rates of ICU admission were the secondary outcomes. The odds ratios (ORs) with 95% confidence intervals (CIs) of the associated conditions of the patients were presented. For continuous variables, the Levene’s test was used to estimate the homogeneity of variance, and the one-way analysis of variance with Games–Howell post hoc test was performed to assess the differences between the groups. Continuous data were expressed as mean ± standard deviation. The ISS was expressed as median and interquartile range (IQR: Q1–Q3). A p value < 0.05 was considered statistically significant.
Results
Characteristics of the Injury and Patients Who Underwent BAC Measurement
A total of 2735 and 2413 patients underwent the BAC test from January 1, 2011 to December 31, 2012 (a 2-year period before implementing the law) and from July 1, 2013 to June 30, 2015 (a 2-year period before implementing the law), respectively (Table 1). After implementing the law, in vehicle crashes, the number of male patients was significantly lower, and that of old patients was higher. No significant difference was observed in terms of trauma mechanism, with motorcycle drivers accounting for most of the patients in this trauma population. The number of DUI patients significantly decreased from 340 (12.4%) to 171 (7.1%), and that of DWI patients significantly reduced from 273 (10.0%) to 146 (6.1%) based on the alcohol test. However, in terms of BAC, no significant difference was observed before and after implementing the law among DUI patients (BAC ≥ 0.005) or DWI patients (BAC ≥ 0.05). After the law was imposed, the percentage of injuries to body regions, such as the head/neck and extremity, but not to the other body regions, significantly decreased. No significant change was observed in terms of the GCS score and ISS after implementing the law. After implementation, a significantly longer LOS in the hospital (10.7 days vs 9.4 days, respectively; p < 0.001) and a higher rate of admission in the ICU (24.0% vs 20.7%, respectively; p = 0.005) were observed in patients who underwent the alcohol test. However, no significant difference was observed in terms of mortality rate (1.7% vs 1.6%, respectively; p = 0.338) among patients who underwent the alcohol test.
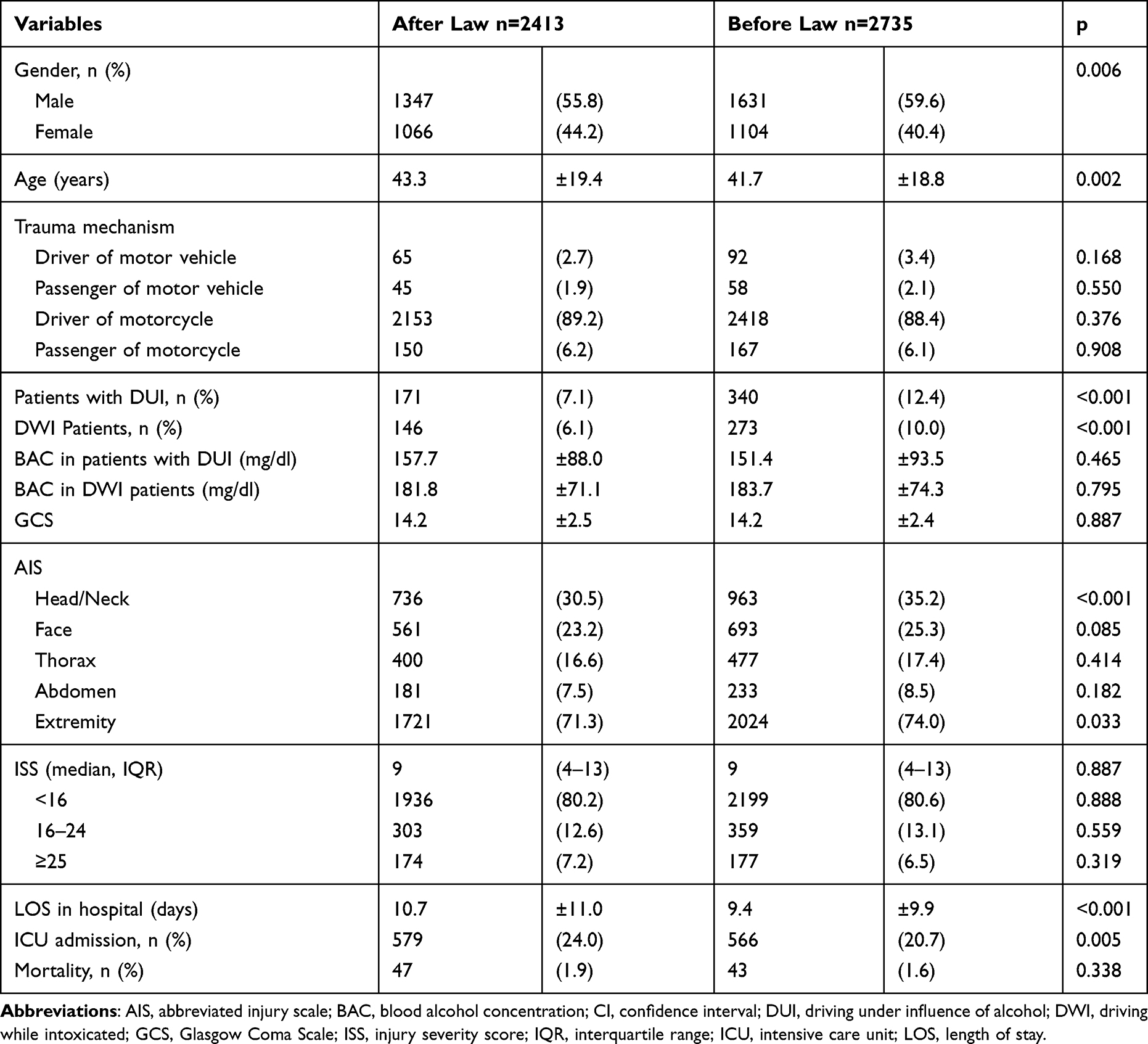 |
Table 1 Characteristics of Injury and Patients with Trauma Who Underwent Measurement of Blood Alcohol Concentration (BAC) at the Emergency Room During the 2-Year Study Period Before and After the Law Was Imposed |
Characteristics of the Injury and DUI Patients
A total of 340 and 171 patients were drunk and driving under the influence of alcohol (ie BAC ≥ 0.005) during the 2-year study period before and after implementing the law (Table 2). After the law was imposed, no significant changes were observed in terms of gender, age, GCS score, AIS score, and ISS. However, the percentage of injuries to the extremity significantly decreased. After implementing the law, no significant difference was observed in the LOS in the hospital (12.8 days vs 12.0 days, respectively; p = 0.464) and mortality rate (7.6% vs 4.7%, respectively; p = 0.224) of DUI patients. A higher rate of ICU admission (54.4% vs 40.0%, respectively; p = 0.003) was found after implementing the law.
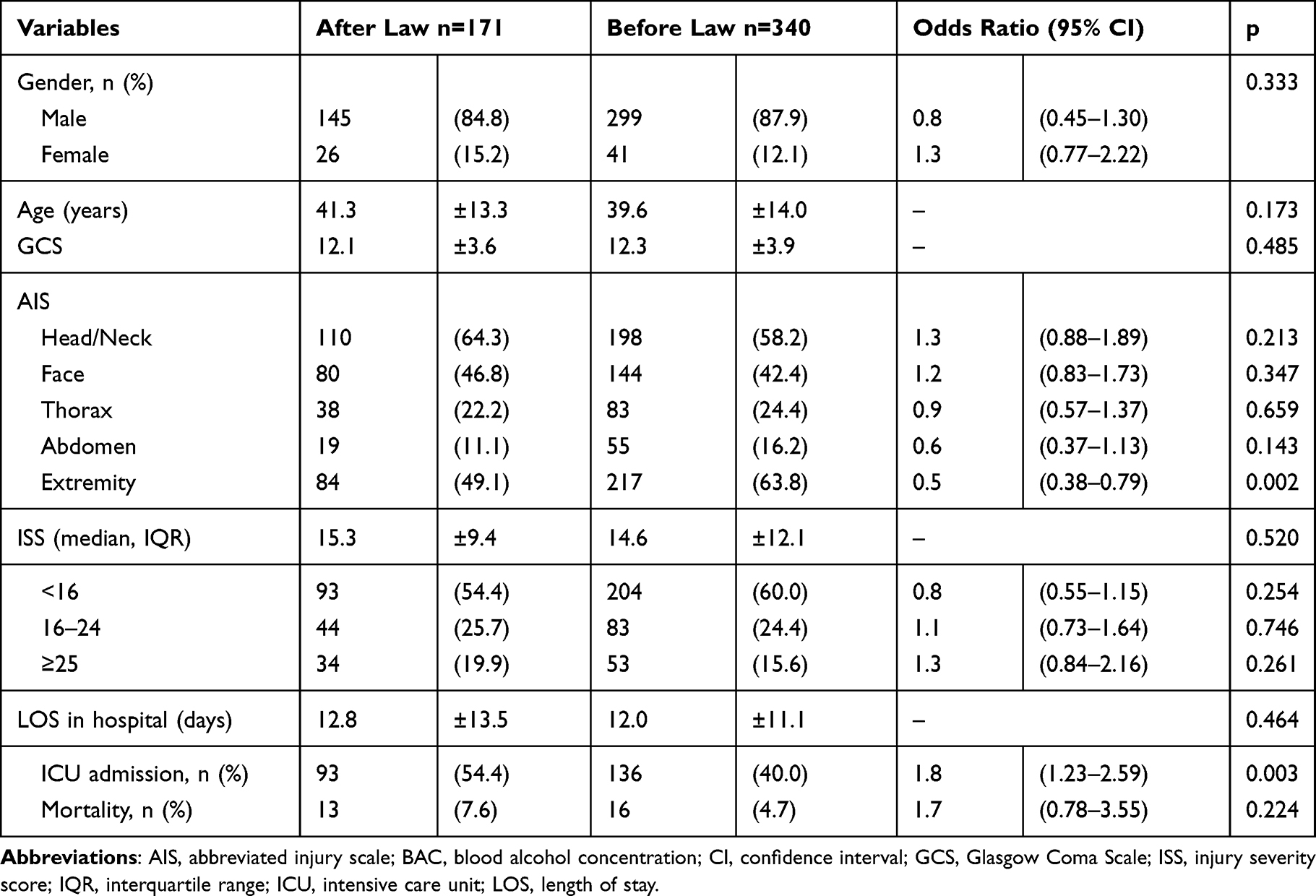 |
Table 2 Characteristics of Injury and Patients with Trauma Who Were Driving Under the Influence of Alcohol (BAC ≥ 0.005) at the Emergency Room Before and After the Law Was Imposed |
Characteristics of Injury and DWI Patients
A total of 273 and 146 DWI patients (ie BAC ≥ 0.05) were recorded during the 2-year study period before and after implementing the law (Table 3). After the law was imposed, no significant changes in terms of gender, age, GCS score, AIS score, and ISS were found. However, the percentage of injuries to the extremity significantly decreased. After implementing the law, no significant difference was observed in the LOS in the hospital (13.0 days vs 11.9 days, respectively; p = 0.385), the rate of admission in the ICU (51.4% vs 41.0%, respectively; p = 0.050), and mortality rate (4.8% vs 4.8%, respectively; p = 1.000) among DWI patients.
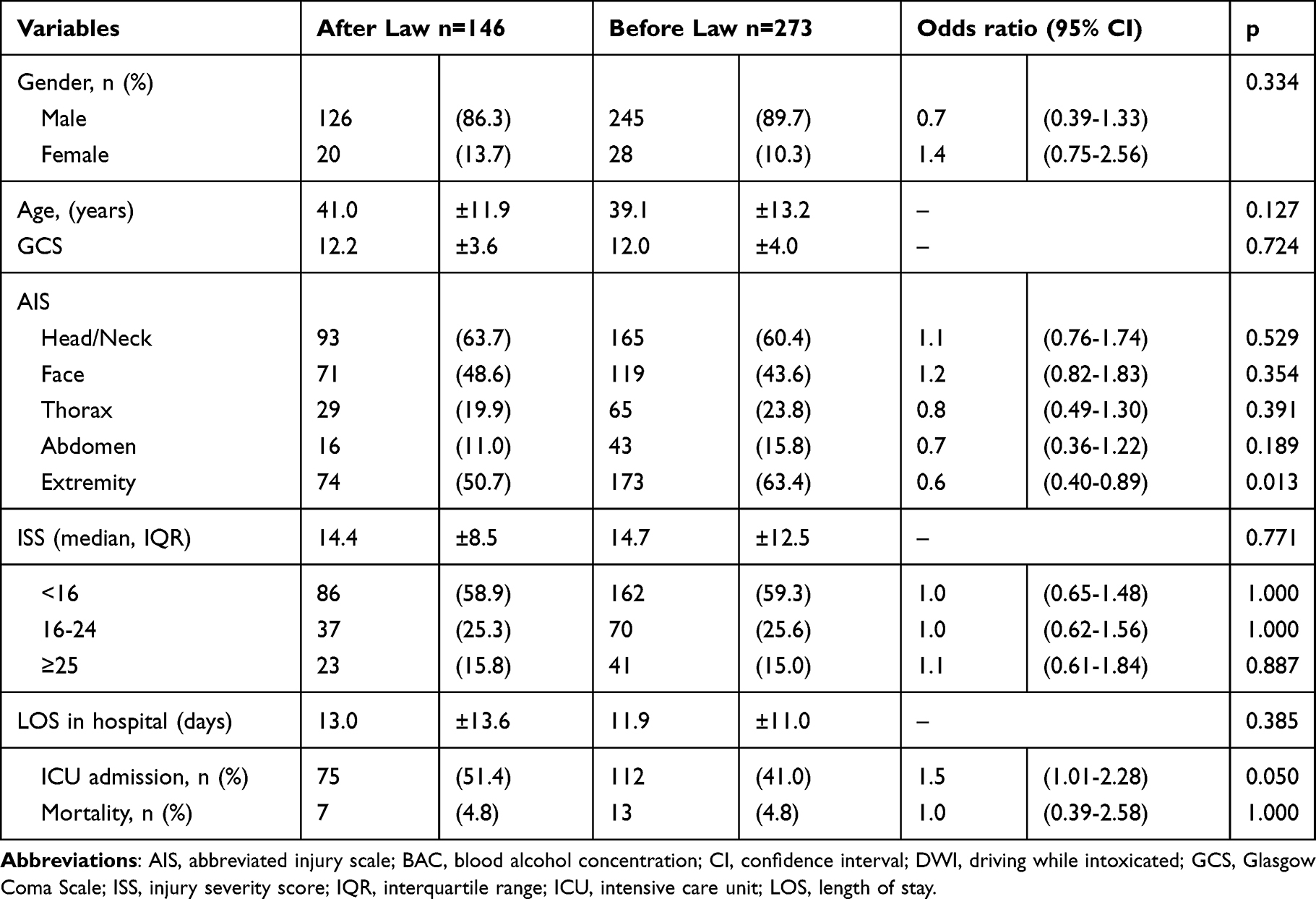 |
Table 3 Characteristics of Injury and DWI Patients with Trauma (BAC ≥ 0.05) at the Emergency Room Before and After the Law Was Imposed |
Associated Injuries in DUI and DWI Patients
The associated injuries in the body regions of DUI (Table 4) patients with trauma and DWI (Table 5) before and after implementing the law are listed. After the law was imposed, the odds for subdural hematoma (SDH), subarachnoid hemorrhage, and mandibular fracture were significantly higher. However, those for hemothorax in DUI patients were low (Table 6). In DWI patients, the odds for SDH, mandibular fracture, and femoral fracture were significantly higher after the law was imposed (Table 7).
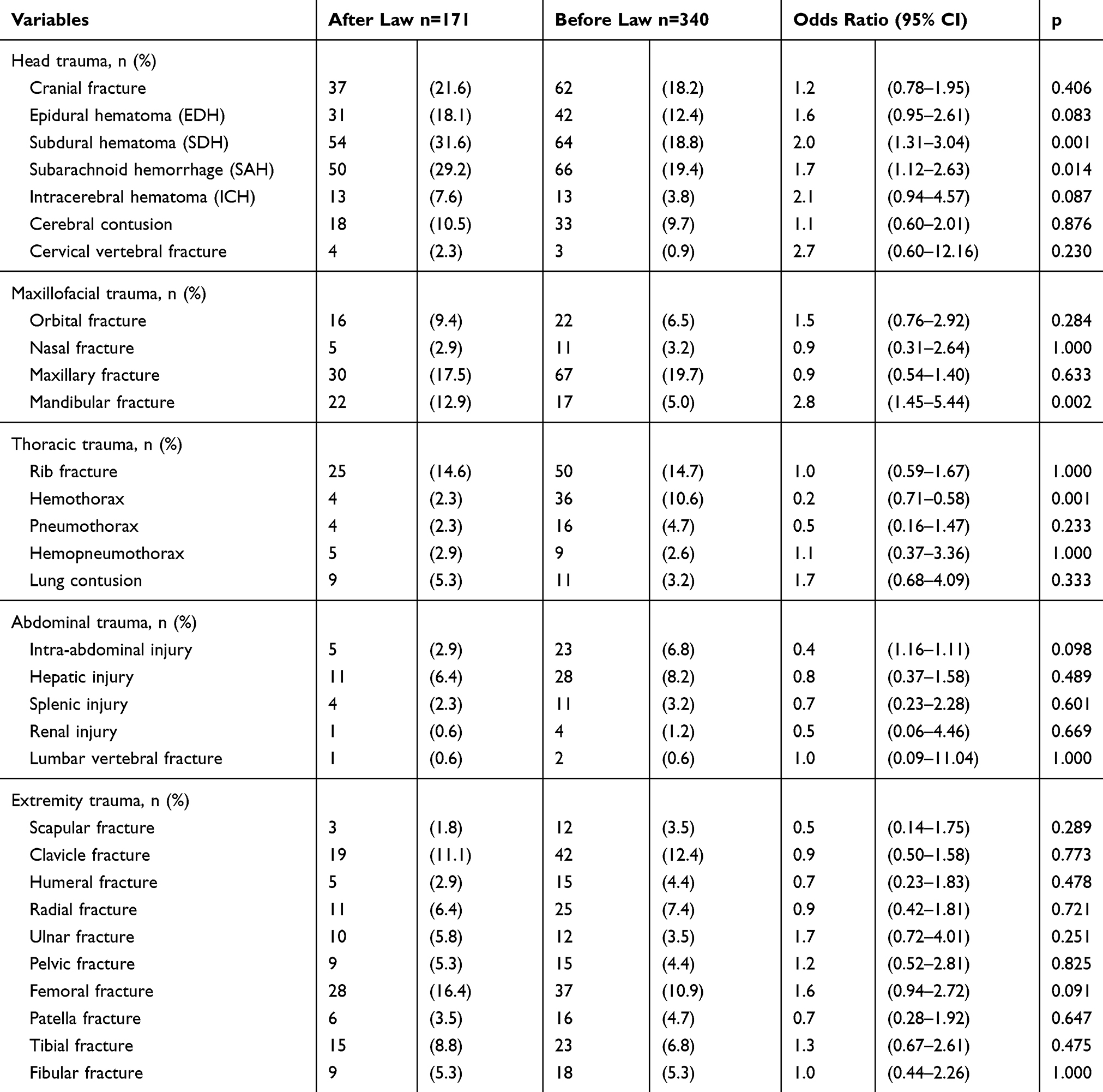 |
Table 4 Associated Injuries in the Body Regions of Patients with Trauma Who Had a Blood Alcohol Concentration ≥ 0.005 mg/mL at the Emergency Room During the 2-Year Study Period Before and After the Law Was Imposed |
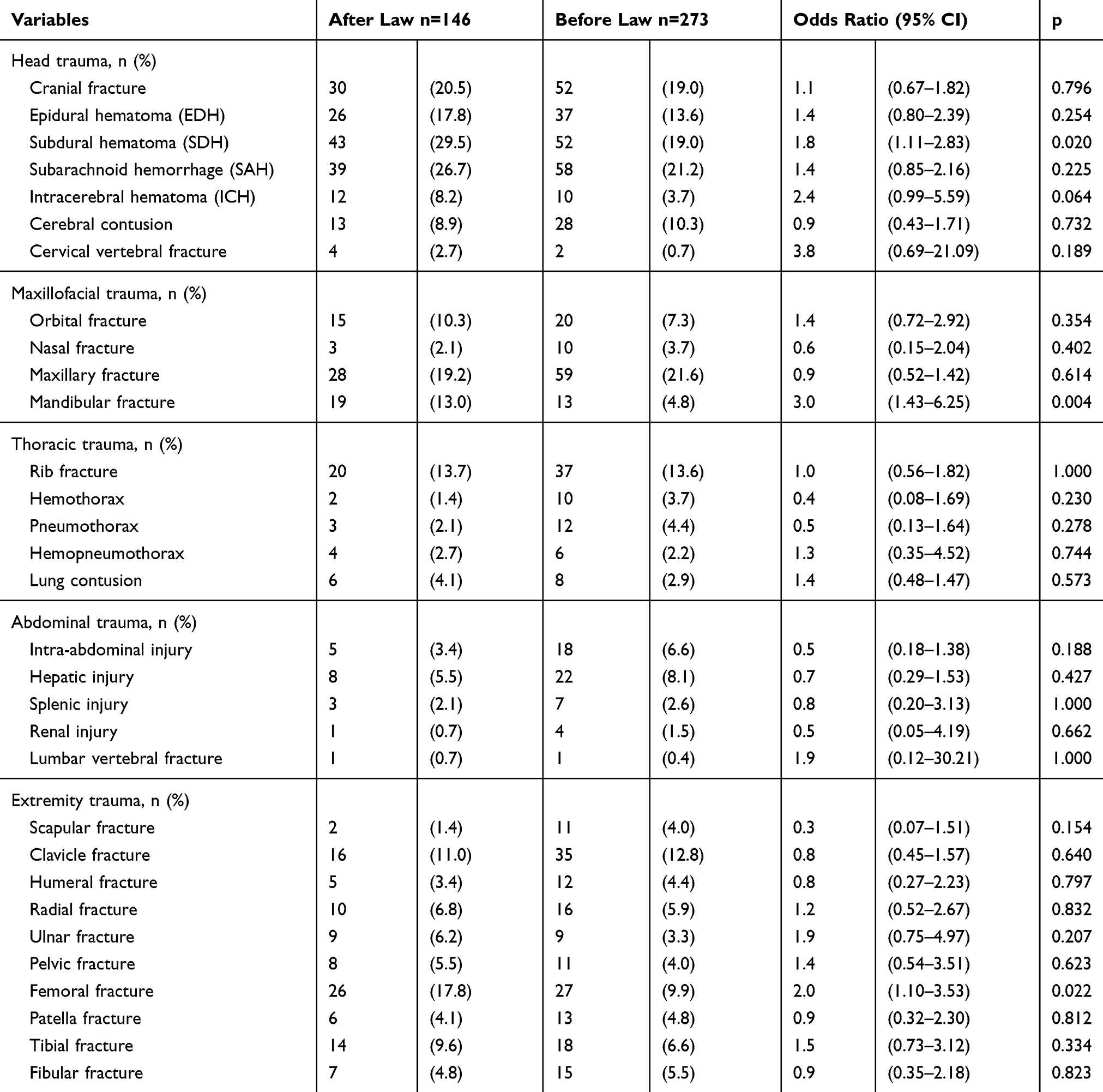 |
Table 5 Associated Injuries in the Body Regions of Patients with Trauma Who Had a Blood Alcohol Concentration ≥ 0.05 mg/mL at the Emergency Room During the 2-Year Study Period Before and After the Law Was Imposed |
 |
Table 6 Associated Injuries in the Body Regions of Patients with Trauma Who Were Driving Under the Influence of Alcohol (BAC ≥ 0.005) at the Emergency Room During the 2-Year Study Period Before and After the Law Was Imposed |
 |
Table 7 Associated Injuries in the Body Regions of DWI Patients with Trauma (BAC ≥ 0.05) at the Emergency Room During the 2-Year Study Period Before and After the Law Was Imposed |
Expenditure for DUI and DWI Patients
After the law was imposed, as the number of DUI (Table 8) and DWI (Table 9) patients was lower, the total expenditure had decreased to 41.6% and 38.1%, respectively, compared to that before the law was imposed. In addition, the cost for operation, examination, and medicines decreased by approximately 30%–50%. However, no difference was observed in terms of expenditure, including the cost of operation, examination, and medicines per person before or after the law was imposed in DUI or DWI patients.
 |
Table 8 Expenditure in US Dollars During Hospitalization in Patients with Trauma Who Were Driving Under the Influence of Alcohol (BAC ≥ 0.005) at the Emergency Room Before and After the Law Was Imposed |
 |
Table 9 Expenditure in US Dollars During Hospitalization in DWI Patients with Trauma (BAC ≥ 0.05) at the Emergency Room Before and After the Law Was Imposed |
Discussion
This study was conducted for a period of 2 years before and after the implementation of the 0.03 BAC legislation in 2013 in Taiwan to determine the effect of the law on the rates and outcomes of hospitalized patients with trauma due to alcohol-related crashes. Since the introduction of the 0.03 BAC law, the number of DUI and DWI patients who underwent the alcohol test significantly decreased, and as a result, the total expenditure for DUI and DWI patients decreased by 41.6% and 38.1%, respectively. However, for DUI and DWI patients, no significant difference was observed in their BAC level before and after the law was imposed. The mortality rate did not differ in individuals who underwent BAC measurement, DUI patients, and DWI patients before and after the law was imposed. After the introduction of the law, a significantly longer LOS in the hospital was noted in patients who underwent BAC measurement, and a higher rate of ICU admission was observed in those who underwent BAC measurement and DUI patients. Furthermore, after the law was imposed, the associated injuries were not significantly reduced but the odds for subdural hematoma and mandibular fracture were significantly higher in those patients with DUI and DWI after the implementation of the law, and the average expenditure per person was not significantly different from that before the law was implemented in patients involved in alcohol-related crashes.
Laws that consider driving with a high BAC as illegal is the most successful intervention among all efforts in reducing alcohol-related driving, and it decreases the associated injuries in individuals in developed countries.27 A study in Turkey has revealed that the mean BAC for private vehicle drivers is 0.05, which was significantly higher than that of drivers of public transport, commercial, and official vehicles as well as taxis who are subjected to a zero alcohol level (52.60 mg/dL vs 10.76 mg/dL, respectively, p < 0.001).28 However, a significant effort in reducing alcohol-related crashes and fatalities cannot be achieved all the time with just lowering the BAC legal limit. In Japan, the enactment of a 0.03 legal BAC legal limit law in 2002 resulted in significant decreases in the rate of alcohol-related crashes.10 In Chile, lowering the BAC legal limit for drivers from 0.05 to 0.03 and increasing license suspension periods for offenders lead to a significant decrease in alcohol-related crashes by 32% after the law was implemented and by 15% after 3 years. However, the reduction in alcohol-related crashes had no significant effects on mortalities.14 In Sweden, after the introduction of lowering the BAC legal limit from 0.05 to 0.02 in 1990, a reduction in fatal crashes, single-vehicle crashes, and all crashes by 9.7%, 11%, and 7.5% were observed, respectively,29 and the interrupted time series analysis has revealed a 15% reduction in overall traffic fatalities.30 In Norway, the enactment of the BAC legal limit from 0.05 to 0.02 in 2001 did not lead to any reduction in single-vehicle nighttime accidents, weekend personal injury, and fatal crashes compared with the situation 6 years before and after the decrease in the legal limit.12 The zero tolerance law was implemented to reduce the odds of an alcohol-impaired fatal crash by over 24% in a review covering 16 years of statistics in the United States.31 However, a study on zero tolerance laws did not result in a reduction of nighttime single-vehicle crashes in Texas compared to a decrease as much as 36% in Maine, 40% in Oregon, or as low as 5% in Florida.32
In this study, the legislation of lowering the legal BAC limit to 0.03 resulted in a statistically significant decrease in the number of hospitalized patients with trauma due to alcohol-related crashes on the road in Southern Taiwan. However, although the lowering in the legal BAC limit affects drivers at all levels of drinking, from the lighter to the heaviest drinkers, the reduced risk was not accompanied by a significant reduction in the mortality rates nor the BAC level in DUI and DWI patients, and this result indicates a responsiveness to the change in BAC limit among the studied population. However, such responsiveness may not be observed in some citizens. In 1011 nationally representative sample of licensed drivers in the United States, 63.9% of the respondents to a questionnaire survey indicated that the lowering of BAC limit to 0.05 would not have any effect on their decisions to drink and drive.33 Nearly 60% of the respondents did not know the accurate limit for BAC in their state, of which 14% reported a higher value and 7% reported a value lower than 0.08, and the rest did not know the limit.33 In general, the respondents also underestimated the number of drinks (approximately three drinks for a woman and four for a man) it would take to reach a BAC level of 0.08.33 Despite the laws and penalties for drunk driving, the drivers have a low perception regarding the chances of being caught and penalized by the police.13 In this study, the percentage of injuries to the head/neck of the patients underwent measurement of BAC was significantly decreased after the law was imposed. However, the odds of associated injuries as subdural hematoma, subarachnoid hemorrhage, and mandibular fracture were significantly higher in those patients with DUI (Table 6) and the odds of subdural hematoma, mandibular fracture, and femoral fracture were significantly higher in those patients with DWI (Table 7) after the implementation of the law. The results imply that, after lowering the legal BAC limit from 0.05 to 0.03, responsiveness to the change in law was observed among the studied population but not in all citizens. Those patients who were accustomed to alcohol drinking may still not obey to the new law. Therefore, the assumption that drunk drivers will comply with the lower limit by reducing the amount of alcohol consumed prior to driving may not be fit for all drivers. In this study,
The effects of lowering the legal BAC limit depend on the public’s compliance with the law. Several factors can influence compliance, which include the level of enforcement, fines, adjudication, public acceptance, and willingness to comply.34 The compliance behavior of drivers was found to be sensitive to the benefits of the policy of lowering BAC in different kinds of scenarios.34 The extent and limits of the benefits achieved by lowering the legal BAC limits may vary in terms of strategies in the reduction of alcohol-impaired driving.34 Thus, to effectively reduce the fatal outcomes from alcohol-related crashes, attention along with special actions may be applied to drivers who are less complaint to the prohibition of drinking prior to driving. However, the strategies should not only rely on lowering the BAC legal limit. For example, the frequency of sobriety checkpoints must be increased, and alcohol ignition interlocks should be required for all alcohol-impaired driving offenders, which is one of the most supported strategies for reducing alcohol-impaired driving.35 The enforcement with random breath testing is associated with a significant reduction in the rate of alcohol-related crashes.36 Immediate roadside prohibitions, which aimed to increase the efficiency of police and courts for processing drinking drivers, significantly reduced fatal and injury crashes than non-alcohol-related crashes.37 Furthermore, mass media are effective in the reduction of alcohol-related crashes.38 The reduction of the risk of traffic crashes by changing the behaviors of drinking and driving would lead to people’s support for the new law.39–41
The present study had some limitations that should be acknowledged. First, we only included hospitalized patients. Some drivers involved in alcohol-related crash may not require admission in the hospital. Since the legal BAC limit did not significantly affect the number of drivers with fatal injuries who were legally hit,42 therefore, some selection bias may exist, and the effect of lowering BAC cannot be estimated in those who drank and drive but were not hurt. Motorcycle accidents accounted for almost 95% of the accidents, and the rate was obviously higher than that in our previous reports, and this bias could also be found in this study.24,25,43 In addition, the fatality rate from car or motorcycle accidents differed. For motorcycle riders, an exponential increase was noted in the associated risk for crash even from a relatively low BAC.44 Second, the retrospective study design may cause a bias for outcome measurement. Third, the patients declared dead at the scene of the accident or upon arrival to the hospital were not included in the Trauma registry database, and selection bias on mortality assessment may exist. Fourth, the traffic accident recording system is not capable of showing detailed causative factors, such as driving skills, features of the road and vehicles, and the used protection apparatus. Finally, this study was limited to a regional level I trauma center, and the observation or conclusion may not be generalized to other areas, considering that there is a wide geographic variation in terms of alcohol drinking.
Conclusion
After lowering the legal BAC limit from 0.05 to 0.03, responsiveness to the change in law was observed among the studied population. However, such responsiveness may not be observed in some citizens who may require special intervention to reduce their behavior of drinking and driving.
Acknowledgments
We would like to thank the statistical analyst from Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital.
Disclosure
The authors declare that they have no competing interests associated with this article.
References
1. Analysis, N. C. f. S. a. State Alcohol-Impaired Driving Estimates: 2013 Data (Traffic Safety Facts. Report No. DOT HS 812 188). Washington, DC: National Highway Traffic Safety Administration; 2015.
2. Moskowitz H, Florentino D. A Review of the Literature on the Effects of Low Doses of Alcohol on Driving-Related Skills. Washington, DC: Department of Transportation, NHTSA; 2000. DOT HS 809 028; 2000.
3. Fell JC, Voas RB. The effectiveness of a 0.05 blood alcohol concentration (BAC) limit for driving in the United States. Addiction. 2014;109(6):869–874. doi:10.1111/add.12365
4. Idiz N, Karakuş A, Dalgıc M, Meseri M, Akg¨ur SA. The alcohol levels in fatal & nonfatal traffic accidents in Izmir. Turkiye Klinikleri J Forensic Med. 2011;8:6–11.
5. Phillips DP, Sousa AL, Moshfegh RT. Official blame for drivers with very low blood alcohol content: there is no safe combination of drinking and driving. Inj Prev. 2015;21:e28–e35. doi:10.1136/injuryprev-2013-040925
6. Phillips DP, Brewer KM. The relationship between serious injury and blood alcohol concentration (BAC) in fatal motor vehicle accidents: BAC = 0.01% is associated with significantly more dangerous accidents than BAC = 0.00%. Addiction. 2011;106:1614–1622. doi:10.1111/j.1360-0443.2011.03472.x
7. Administration., N. H. T. S. Setting Limit, Saving Lives: The Case for 0.08% BAC Laws (Publication No. DOT HS 808 524). Washington, DC: National Highway Traffic Safety Administration; 1997.
8. Fell JC, Voas RB. The effectiveness of reducing illegal blood alcohol concentration (BAC) limits for driving: evidence for lowering the limit to.05 BAC. J Safety Res. 2006;37:233–243. doi:10.1016/j.jsr.2005.07.006
9. Green RS, Kureshi N, Erdogan M. Legal consequences for alcohol-impaired drivers injured in motor vehicle collisions: a systematic review. Accid Anal Prev. 2015;80:106–116. doi:10.1016/j.aap.2015.04.005
10. Desapriya E, Pike I, Subzwari S, Scime G, Shimizu S. Impact of lowering the legal blood alcohol concentration limit to 0.03 on male, female and teenage drivers involved alcohol-related crashes in Japan. Int J Inj Contr Saf Promot. 2007;14(3):181–187. doi:10.1080/17457300701440634
11. Ahlner J, Holmgren A, Jones AW. Prevalence of alcohol and other drugs and the concentrations in blood of drivers killed in road traffic crashes in Sweden. Scand J Public Health. 2014;42(2):177–183. doi:10.1177/1403494813510792
12. Assum T. Reduction of the blood alcohol concentration limit in Norway–effects on knowledge, behavior and accidents. Accid Anal Prev. 2010;42:1523–1530. doi:10.1016/j.aap.2010.03.002
13. Nguyen NP, Passmore J, Tran LT, Luong AM. Role of alcohol in hospitalized road trauma in Viet nam. Traffic Inj Prev. 2013;14:329–334. doi:10.1080/15389588.2012.715253
14. Otero S, Rau T. The effects of drinking and driving laws on car crashes, injuries, and deaths: evidence from Chile. Accid Anal Prev. 2017;106:262–274. doi:10.1016/j.aap.2017.05.031
15. Mercer SL, Sleet DA, Elder RW, Cole KH, Shults RA, Nichols JL. Translating evidence into policy: lessons learned from the case of lowering the legal blood alcohol limit for drivers. Ann Epidemiol. 2010;20:412–420. doi:10.1016/j.annepidem.2010.03.005
16. Sleet DA, Mercer SL, Cole KH, Shults RA, Elder RW, Nichols JL. Scientific evidence and policy change: lowering the legal blood alcohol limit for drivers to 0.08% in the USA. Glob Health Promot. 2011;18(1):23–26. doi:10.1177/1757975910393707
17. Deshapriya EB, Iwase N. Impact of the 1970 legal BAC 0.05 mg% limit legislation on drunk-driver-involved traffic fatalities, accidents, and DWI in Japan. Subst Use Misuse. 1998;33(14):2757–2788. doi:10.3109/10826089809059349
18. Bartl G, Esberger R. Effects of lowering the legal BAC limit in Austria. In: Laurell H, Schlyter F, editors.
19. Smith DI. Effect on traffic safety of introducing a 0.05% blood alcohol level in Queensland, Australia. Med Sci Law. 1988;28:165–170. doi:10.1177/002580248802800217
20. Noordzij PC, Meester AC, Verschuur WL. Night-time driving: the use of seat-belts and alcohol. Ergonomics. 1988;31(4):663–668. doi:10.1080/00140138808966708
21. Mercier-Guyon C Lowering the BAC limit to 0.05: results of the French experience.
22. Chan YS, Chen CS, Huang L, Peng YI. Sanction changes and drunk-driving injuries/deaths in Taiwan. Accid Anal Prev. 2017;107:102–109. doi:10.1016/j.aap.2017.07.025
23. Tsai YC, Wu SC, Huang JF, et al. The effect of lowering the legal blood alcohol concentration limit on driving under the influence (DUI) in southern Taiwan: a cross-sectional retrospective analysis. BMJ Open. 2019;9:e026481. doi:10.1136/bmjopen-2018-026481
24. Hsieh CH, Hsu SY, Hsieh HY, Chen YC. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed J. 2017;40:113–120. doi:10.1016/j.bj.2016.10.005
25. Hsieh CH, Liu HT, Hsu SY, Hsieh HY, Chen YC. Motorcycle-related hospitalizations of the elderly. Biomed J. 2017;40:121–128. doi:10.1016/j.bj.2016.10.006
26. Hsieh CH, Chen YC, Hsu SY, Hsieh HY, Chien PC. Defining polytrauma by abbreviated injury scale >/= 3 for a least two body regions is insufficient in terms of short-term outcome: a cross-sectional study at a level I trauma center. Biomed J. 2018;41:321–327. doi:10.1016/j.bj.2018.08.007
27. Mohan D. Road safety in less-motorized environments: future concerns. Int J Epidemiol. 2002;31:527–532. doi:10.1093/ije/31.3.527
28. Karakus A, Idiz N, Dalgic M, Ulucay T, Sincar Y. Comparison of the effects of two legal blood alcohol limits: the presence of alcohol in traffic accidents according to category of driver in Izmir, Turkey. Traffic Inj Prev. 2015;16:440–442. doi:10.1080/15389588.2014.968777
29. Norström T, Laurell H Effects of lowering the legal BAC-limit in Sweden.
30. Ross HL, Klette H. Abandonment of mandatory jail for impaired drivers in Norway and Sweden. Accid Anal Prev. 1995;27:151–157. doi:10.1016/0001-4575(94)00047-P
31. Voas RB, Tippetts AS, Fell JC. Assessing the effectiveness of minimum legal drinking age and zero tolerance laws in the United States. Accid Anal Prev. 2003;35:579–587. doi:10.1016/S0001-4575(02)00038-6
32. Lacey JH, Jones RK, Wiliszowski CH. Zero Tolerance Laws for Youth: Four States’ Experience (DOT HS 809 053). Washington, DC: U.S. Department of Transportation, National Highway Traffic Safety Administration; 2000.
33. Eby DW, Molnar LJ, Kostyniuk LP, et al. Perceptions of alcohol-impaired driving and the blood alcohol concentration standard in the United States. J Safety Res. 2017;63:73–81. doi:10.1016/j.jsr.2017.08.013
34. Kostyniuk LP, Eby DW, Molnar LJ, St Louis RM, Zanier N, Miller TR. Potential effects of lowering the BAC limit on injuries, fatalities, and costs. J Safety Res. 2018;64:49–54. doi:10.1016/j.jsr.2017.12.005
35. Fell JC, Beirness DJ, Voas RB, et al. Can progress in reducing alcohol-impaired driving fatalities be resumed? Results of a workshop sponsored by the Transportation Research Board, Alcohol, Other Drugs, and Transportation Committee (ANB50). Traffic Inj Prev. 2016;17:771–781. doi:10.1080/15389588.2016.1157592
36. Homel R. Random breath testing in Australia: getting it to work according to specifications. Addiction. 1993;88 Suppl:27s–33s. doi:10.1111/j.1360-0443.1993.tb02159.x
37. Macdonald S, Zhao J, Martin G, et al. The impact on alcohol-related collisions of the partial decriminalization of impaired driving in British Columbia, Canada. Accid Anal Prev. 2013;59:200–205. doi:10.1016/j.aap.2013.05.012
38. Sedjo RL, Byers T, Barrera E
39. Carpenter C. How do zero tolerance drunk driving laws work? J Health Econ. 2004;23:61–83. doi:10.1016/j.jhealeco.2003.08.005
40. Karasov AO, Ostacher MJ. Alcohol and the law. Handb Clin Neurol. 2014;125:649–657.
41. Shults RA, Elder RW, Sleet DA, et al. Reviews of evidence regarding interventions to reduce alcohol-impaired driving. Am J Prev Med. 2001;21:66–88. doi:10.1016/S0749-3797(01)00381-6
42. McLean AJ, Kloeden CN, McColl RA, Laslett R Reduction in the legal blood alcohol limit from 0.08 to 0 05: effects on drink driving and alcohol-related crashes in Adelaide.
43. Hsieh TM, Tsai TC, Liu YW, Hsieh CH. How does the severity of injury vary between motorcycle and automobile accident victims who sustain high-grade blunt hepatic and/or splenic injuries? Results of a retrospective analysis. Int J Environ Res Public Health. 2016;13(7):739. doi:10.3390/ijerph13070739
44. Haworth N, Smith R, Brumen I. Case-Control Study of Motorcycle Crashes. Canberra, Australian Capital Territory. Australian Trans- port Safety Bureau; Report CR174; 2002.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.