")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Effect of Flexible Half-Dose Gonadotropin-Releasing Hormone Antagonist Protocol on in vitro Fertilization Outcome in Predicted Normal Responder: A Study Protocol for a Multicentered, Randomized, Non-Inferiority, Parallel Controlled Trial
Authors Ma YJ, Li MY , Song JY , Sun ZG
Received 22 February 2023
Accepted for publication 11 May 2023
Published 24 May 2023 Volume 2023:17 Pages 1557—1566
DOI https://doi.org/10.2147/DDDT.S409557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Ying-Jie Ma,1,* Meng-Yao Li,1,* Jing-Yan Song,1,2 Zhen-Gao Sun1,2
1The First Clinical College, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, 250011, People’s Republic of China; 2Reproductive and Genetic Center of Integrative Medicine, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, 250014, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhen-Gao Sun; Jing-Yan Song, Reproductive and Genetic Center of Integrative Medicine, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, 42, Wenhua Road (W), Lixia District, Jinan, Shandong, 250014, People’s Republic of China, Email [email protected]; [email protected]
Background: Gonadotropin-releasing hormone antagonists (GnRH-ant) are widely used in current in vitro fertilization-embryo transfer (IVF-ET), however, whether the lowest daily dose of GnRH-ant is individualized remains unknown. Due to the negative effect of GnRH-ant on endometrial receptivity, lessening the amount of GnRH-antagonists used during controlled ovarian stimulation may be helpful for embryo implantation. As such, a randomized controlled study is essential to validate the feasibility and efficacy of daily GnRH-ant dose reduction to 0.125 mg geared towards providing scientific evidence for guidance in clinical practice.
Methods: In total, 620 infertile women undergoing in vitro fertilization will be enrolled in the multicentered, randomized, parallel controlled trial. Based on a computer-generated random list, they will be randomly and equally subdivided into half-dose GnRH-ant group or conventional-dose GnRH-ant group. The primary outcome is ongoing pregnancy ie, intrauterine pregnancy diagnosed by pelvic ultrasonography at more than 12 weeks of gestation accompanied by normal fetal heartbeats. Secondary outcomes include cycle cancellation, premature luteinizing hormone surge, positive pregnancy, embryo implantation rate, clinical pregnancy, early spontaneous abortion, and live birth. The intention-to-treat and per protocol analyses will be used to initially analyze the difference in ongoing pregnancy rate between the two groups, while the multiple imputation method was used to handle missing values in the data.
Discussion: At present, no randomized controlled trials (RCTs) have been performed on the use of the half-dose GnRH-ant protocol (0.125mg/d) to improve reproductive outcomes of IVF-ET in predicted normal responder, compared to conventional-dose GnRH-ant protocol (0.25mg/d). Half-dose GnRH-ant protocol might provide a suitable clinical solution for predicted normal responder undergoing IVF treatment. Thus, it is critical to conduct a well-designed RCT to evaluate the impact of a half-dose GnRH-ant protocol on the reproductive outcomes of IVF-ET in predicted normal responder.
Trial Registration: This study was registered in the Chinese Clinical Trials Registry Platform on August 29, 2020. (chictr.org.cn; identifier: ChiCTR2000037629). This trial is version 1.3.
Keywords: gonadotropin-releasing hormone antagonist, in vitro fertilization-embryo transfer, half-dose GnRH-ant protocol, predicted normal responder, randomized controlled trial
Introduction
Background
Gonadotropin-releasing hormone antagonists (GnRH-ant) protocols are widely used in present IVF-ET treatment. At the same time, the ESHRE guidelines strongly propose the use of GnRH-ant protocol during controlled ovarian hyperstimulation (COH) in predicted normal responders.1 Unlike gonadotropin-releasing hormone agonist (GnRH-A) protocol, GnRH-ant protocol has several advantages, including shortening the treatment time, reducing gonadotropin dosage, and the occurrence of severe ovarian hyperstimulation syndrome (OHSS), as well as preventing pituitary over-suppression and flare-up effects.2 Although the GnRH-ant protocol has been reported to be comparable to the GnRH-A protocol in terms of cumulative live birth rates,3,4 other studies have shown that the GnRH-ant protocol results in decreased clinical pregnancy rates.5,6 A recent systematic review revealed that frozen-thawed embryo transfer (FET) had no benefit on live birth rate compared to fresh embryo transfer, thus, the “freeze-all” strategy was not recommended for predicted normal responder due to the increased risk of preeclampsia.7 Additionally, a number of studies have shown that GnRH antagonists are associated with decreased frequencies of ongoing pregnancy in fresh embryo transfer cycles when compared to GnRH-A long protocol, whereas the detrimental effects of GnRH-ant on endometrial receptivity were the primary reasons for the poor pregnancy rate.5,8,9
To minimize the detrimental effect of GnRH-ant on endometrial receptivity, reproductive doctors have attempted to improve the GnRH-ant protocol by establishing a minimum dose of GnRH-ant. So far, starting on day 6 of ovarian stimulation (OS), 0.25 mg of cetrorelix per day is thought to maintain luteinizing hormone (LH) levels within a safe range, a dose frequently used in clinical practice.10–13 Nevertheless, a few studies have shown that limiting the daily dosage of GnRH-ant to 0.125–0.2 mg is similarly beneficial.14–16 Additionally, Wang and his colleges reported that routine GnRH-ant administration was not necessary during ovarian stimulation, since 87.2% of patients did not need any GnRH-ant mostly during COH cycle.17 As a result, the minimal effective dosage of GnRH-ant remains controversial.
Hence, we assume that there exists no specific GnRH-ant dose suitable for each participant, therefore, it is absolutely critical that the dosage of GnRH should be tailored to the needs of each patient. Based on the definition of premature LH surge, ie, serum LH level ≥ 10 IU/L and progesterone (P) level ≥ 1.0 ng/mL, and the less effective GnRH-ant dose described in previous studies,18–20 we tried a novel and flexible half-dose GnRH-ant protocol in a small number of patients and design this randomized controlled trial in which the daily GnRH-ant dose will be reduced to 0.125 mg. The daily GnRH-ant dose will be increased to 0.25 mg until the trigger day if the LH level rises above 10 IU/L.
Methods/Design
Study Design
A multicenter, prospective, randomized parallel controlled trial will be conducted in four reproductive centers in China Mainland. The study institutions were the First Affiliated Hospital of Shandong University of Traditional Chinese Medicine, the Second Affiliated Hospital of Shandong University of Traditional Chinese Medicine, the Second Affiliated Hospital of Tianjin University of Traditional Chinese Medicine and the Reproductive and Genetic Center of Shandong University. The flow chart for this study is shown in Figure 1, and the study process schedule is shown in Figure 2.
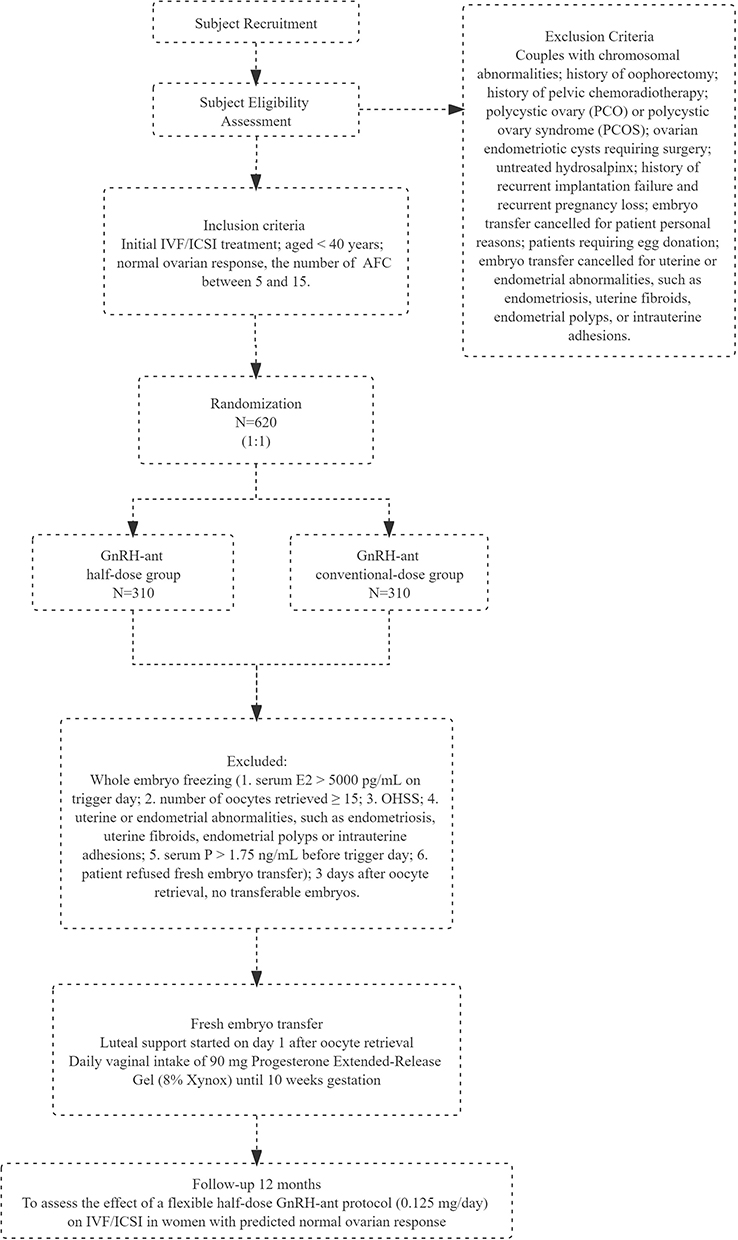 |
Figure 1 Flowchart showing the study process. |
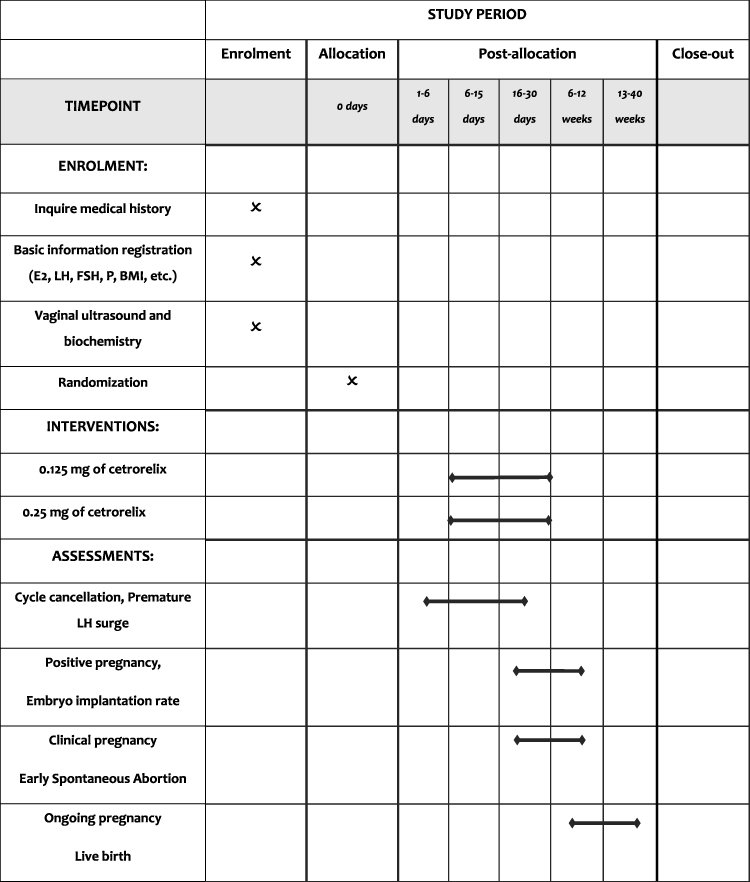 |
Figure 2 Schedule of the study process. |
Objectives
GnRH-ant is believed to be negatively correlated with the capacity for endometrium receptivity.21 When using the GnRH-ant protocol, lowering GnRH-ant doses during controlled OS can aid in embryo implantation. Nonetheless, whether the minimum daily dose of GnRH-ant should be individualized remains unknown. Thus, this study aims to resolve the concerns about the efficacy and safety of administering GnRH-ant a regular dose of 0.125mg.
Participants
Inclusion Criteria
Initial IVF/ICSI treatment; 18 years < Age < 35 years; predicted normal responder, ie, the number of basal antral follicles count (AFC) was between 5 and 15.22
Exclusion Criteria
Couples with chromosomal abnormalities; history of oophorectomy; history of pelvic chemoradiotherapy; polycystic ovary (PCO) or polycystic ovary syndrome (PCOS); ovarian endometriotic cysts requiring surgery; untreated hydrosalpinx; history of recurrent implantation failure (ie the failure to achieve a viable pregnancy, following a greater than 3 embryo transfers with high-quality embryos) and recurrent pregnancy loss (ie couples with two or more consecutive spontaneous miscarriages); embryo transfer cancelled for patient personal reasons; patients requiring egg donation; embryo transfer cancelled for uterine or endometrial abnormalities, such as endometriosis, uterine fibroids, endometrial polyps, or intrauterine adhesions; abnormal BMI, immunological infertility, congenital or acquired uterine malformations and other serious malformations of reproductive organs; presence of reproductive system tumors, thyroid dysfunction, hyperprolactinemia, and other endocrine dysfunction history; recent ovarian stimulation treatment or OCP within the last three months, and other contraindications for assisted reproductive technology.
Recruitment
Detailed history, transvaginal ultrasound, and biochemistry will be required before COH, and if inclusion and exclusion criteria are met, the patient will be contacted by a research assistant, where the study details will be explained to her, then invited to join the study. Each individual may willingly attend the study and will be provided a detailed explanation of the trial. At the same time, their permission will be sought before being recruited into the study. Patients must sign a written informed consent.
Adherence
In order to improve patient compliance, we will provide patients with basic examinations, back and forth transportation costs and meal subsidies free of charge, and so on. And ensure the effectiveness of data, a variety of methods will be used to track records, including uploading data at each visit, weekly telephone follow-up, asking about the visit time in advance, etc. The investigator will track and record the patient and record whether there are adverse reactions.
Interventions
Cetrorelix acetate can be provided in two groups: some patients will be treated with a regular dose, whereas others will get a low dosage. In the GnRH-ant half-dose group, on day five or six of COH, 0.125mg of GnRH-ant (Cetrorelix acetate, Merck Serono, Switzerland) will be subcutaneously injected daily. Patients will be subjected to serological testing at 1- or 2-days interval, and once LH levels exceed 10 mIU/mL, the daily cetrorelix dose will be adjusted to 0.25mg until the trigger day. In the GnRH-ant conventional-dose group, on day five or six of COH, 0.25mg of GnRH-ant will be subcutaneously injected daily until the trigger day.
In vitro Fertilization Procedure
OS begins on the second day of menstruation, and all patients will be provided recombinant follicle-stimulating hormone (r-FSH) (75U, Gonal-F, Merck Serono, Switzerland). The initial FSH dose was established by the physician based on age, AFC, basal FSH, and body mass index (BMI), usually ranging from 150–225 IU/day. This dose is adjusted every 2–3 days, depending on ovarian response, ie, serum estradiol levels and follicular growth under ultrasound monitoring. Then, all patients will be treated with GnRH-ant (0.25mg, Cetrorelix acetate, Merck Serono, Switzerland) from day 5 or 6 of COH until the day before the trigger. Finally, 250μg of recombinant human chorionic gonadotropin (250μg, r-hCG, Merck Serono, Switzerland) will be injected when the mean diameter of ≥ 3 follicles reach 17 mm. After 35 to 37 hours of r-hCG injection, oocyte retrieval will be guided by transvaginal ultrasound. Notably, intracytoplasmic sperm injection (ICSI) will be performed only in cases of severe oligozoospermia and asthenozoospermia (ie, those with sperm density < 5x106/mL, < 30% viable sperm, sperm motility Grade I, or even sperm immotile but confirmed with viable sperm by eosin staining).
In our present study, only fresh embryo(s) will be transferred. On day three after oocyte recovery, embryo transfer will commence. All patients should undergo embryo transfer on the third day after oocyte retrieval, except for the following conditions: (1) serum E2 > 5000 pg/mL on the trigger day; (2) number of oocytes retrieved ≥ 15; (3) OHSS; (4) serum P > 1.75 ng/mL before the trigger day;23 or (5) patients who violate informed consents and waived fresh embryo transfer. The number of embryos transferred will be determined based on the individual patient’s condition and the doctor’s professional judgment, with no more than 2 embryos transferred at a time. This approach aims to increase the chances of pregnancy while reducing the risk of multiple pregnancies.
Luteal support will start on the first day after oocyte retrieval with 8% micronized vaginal progesterone gel 90 mg (Crinone®; Central Pharma Ltd, UK) once daily and dydrogesterone (Duphaston®; Abbott Biologicals, Netherlands) 20 mg orally daily until 10 weeks of gestation.
Concomitant Care
Except for the relevant administration in the test, similar drugs shall not be taken or injected during the treatment, so as not to affect the accuracy of the test results.
Primary Outcome
Ongoing pregnancy: intrauterine pregnancy confirmed by pelvic ultrasonography at more than 12 weeks of gestation accompanied by normal fetal heartbeats.
Secondary Outcomes
(1) Cycle cancellation: premature ovulation, absence of follicular development, failure to pick up eggs, and personal reasons;
(2) Premature LH surge: serum LH level ≥ 10 IU/L or P level ≥ 1.0 ng/mL;
(3) Positive pregnancy or chemical pregnancy: 14 days after embryo transfer, serum β-hCG ≥ 10 mIU/mL;
(4) Embryo implantation: the number of gestational sacs identified via pelvic ultrasonography divided by the total number of embryos transferred;
(5) Clinical pregnancy: intrauterine gestational sac with fetal heartbeat was identified by B-mode ultrasound at 6 gestational weeks;
(6) Early spontaneous abortion: spontaneous termination of pregnancy occurring in less than 12 weeks of gestation;
(7) Live birth: delivery of a neonate with a gestational age ≥ 20 weeks and heartbeat and respiration.
(8)Pregnancy related complications: gestational diabetes, gestational hypertension, preeclampsia, and preterm delivery.
Randomization
When patients volunteering to participate in the study will be joined, stratified block randomization will be used, ie, stratified by study site. The block length will be set to four. The random number will be generated then block randomization will be performed based on R language version 3.5.1. The researchers will register the participants.
The proportion of subjects in the two groups is 1:1. The specific grouping details are mastered by the drug management center and the statisticians, and the subjects will be randomly assigned to one of the following two groups: (1) GnRH-ant half-dose group: On the 6th day of COH, 0.125 mg cetrorelix was subcutaneously injected daily. Patients underwent serological testing at 1- or 2-days interval, and once LH levels exceed 10 mIU/mL, the daily cetrorelix dose will be adjusted to 0.25 mg until the trigger day; (2) GnRH-ant conventional-dose group: On the 6th day of COH, 0.25 mg cetrorelix is injected subcutaneously daily until the trigger day.
Blinding
Because of the nature of the trial, neither the researchers nor the patients will be blinded. Nevertheless, the embryologists performing the quality assessment must be blinded to the grouped interventions.
Estimation of Sample Size
Pass software version 11.0 (NCSs, Inc., kesville, Utah, USA) will be used to calculate the sample size of the two groups. It is worth noting that according to the data of our reproductive center at the time of trial design, the continuous pregnancy rate of each fresh embryo transfer is about 30%. In addition, it is calculated that the GnRH ant low dose group (intervention group) and GnRH ant conventional dose group The sample size of (control group) was 279 cases, and the total sample 45t size was 558 cases. On both sides α= 0.05, the total sample size of the two groups is 620 and 310 in each group, which is enough to establish equivalence (bilateral 95% CI and 80% efficacy) and prove non inferiority. The margin is based on clinically and statistically important differences, ethical standards, cost and feasibility, and the margin of the main pregnancy outcome is 10%. The calculation assumption is bilateral Z-test. The sample size calculation allows 10% loss of follow-up.
Interim Analyses and Stopping Guidelines
In our non-inferiority test, a mid-term analysis is planned at the halfway point of the trial, that is, after half of the participants have completed their treatments and follow-ups. This mid-term analysis is primarily aimed at comparing the clinical pregnancy rates between the two groups. If this analysis shows a significant improvement in clinical pregnancy rates in the group receiving the half-dose GnRH antagonist regimen compared to the group receiving the full-dose regimen, the trial will continue. This decision is based on the indication that the half-dose regimen is potentially more beneficial and not inferior to the full-dose regimen.
On the other hand, if the mid-term analysis does not show a clear benefit of the half-dose regimen, or if it reveals superior results with the full-dose regimen, the trial will be terminated. In such a case, the control group will continue with the original full-dose treatment regimen. This strategic planning ensures the safety and benefit of the patients involved in the trial.
Data Monitoring and Adverse Event Assessment
The research employs an autonomous Data Monitoring Committee (DMC), composed of professionals who are independent of the investigative team. The primary responsibility of the DMC is to monitor and evaluate data integrity and safety throughout the trial. It regularly assesses trial data, which encompasses aspects such as study quality, participant safeguarding, data completeness, accuracy, and the occurrence of adverse events. Additionally, the DMC has the discretion to decide on the necessity for interim analysis and can consider the early termination of the trial in cases of significant safety issues or apparent efficacy disparity.
Adverse events that could potentially be associated with the trial treatment will be assessed. These include, but are not limited to, adverse reactions to medications, complications during treatment, and any incidents that might jeopardize the safety and welfare of participants.
Regarding the termination of the trial in relation to the incidence of adverse events, our approach is to adhere to the DMC’s guidance and recommendations. The DMC makes decisions on trial termination based on real-time data on the incidence of adverse events, clinical pregnancy rates, and other factors, taking into account the overall welfare of participants and the risk/benefit ratio of the trial.
Statistical Analysis
Intention-to-treat and per protocol analyses will be used to analyze the difference of persistent pregnancy rate between the two groups in the main analysis. The multiple interpolation method will be used to deal with the missing values in the data of this study. We calculated as 10% missing values.
Demographic characteristics and baseline data are compared between the two groups.
Primary outcome be aggregated as mean or median.
Students’ t-test is used to compare continuous variables, while the χ2 test is used to compare classified variables. Additionally, a subgroup analysis-age ≤ 35 years old vs > 35 years old will be conducted to further explore the effect of flexible half-dose GnRH-ant regimen on in vitro fertilization outcomes in predicted normal responders. All the data will be statistically analyzed using SPSS version 26.0, P < 0.05 is considered as statistically significant.
Feasibility Analysis
Regarding the feasibility of research ideas, this trial considers the population with predicted normal response and a wide range of beneficiary populations. Moreover, a recent meta-analysis including eleven high-quality randomized controlled trials (RCTs) suggested that the whole embryo freezing strategy is not recommended for predicted normal responder due to the increased risk of preeclampsia compared to fresh embryo transfer.24 The adverse effect of traditional GnRH-ant protocol on the clinical pregnancy rate of fresh embryo transfer is the original intention of this trial. This trial sights to improve the clinical pregnancy rate in this population by reducing the dosage of GnRH-ant to alleviate its adverse effect on the endometrium.
The project applicant, Zhen-Gao Sun, MD, presided over several National Natural Science Foundation of China. Also, the applicant presided over and participated in the implementation of several multicenter RCTs nationwide, with good scientific research literacy; the applicants and researchers had graduate degree or above and a good cooperation relationship. Besides, the members of the research group received systematic training through the National Natural Science Foundation of China and provincial projects, mastered the knowledge of protocol design, reproductive medicine, medical statistics, and other aspects of the study of this project, they also had strong technical strength.
Data Entry and Quality Control
Embryo lab data will be collected on day 3 or 5 post oocyte retrieval. A As per the study design, participants’ follow-up data will comprise information from the time they enrolled in the study and for the next year. Furthermore, case report forms from patients will be obtained for data input. Investigators will also be needed to determine the data accuracy levels (first and second levels), since both levels will involve data validation and monitoring, which will be performed on a regular basis by the Data Monitoring Committee (DMC) during the study. On a daily basis, data will be backed up to another computer in the same physical area as the server. Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in the current trial and for future use in ancillary studies, if applicable.
Patient and Public Involvement
Patients and the public are not involved in developing the research questions nor the study design. Moreover, they do not participate in the recruitment exercise of the study. Our results will be disseminated to participants and their families via telephone and patient organization platforms.
Existing Conditions and Work Basis
Based on the IVF-ET technology platform of the Reproductive Center, Affiliated Hospital of Shandong University of Traditional Chinese Medicine (TCM), the project research team performed IVF-ET for more than 10 years for the earliest TCM unit to start IVF technology. This was approved by the Ministry of Health in China, and implemented IVF/ICSI about 2000 cycles per year.
The members of the research group had a reasonable echelon, high quality, and a good relationship with many years of cooperation, in completion of many RCTs, and well completed the research work of this topic.
During the experiment, if the protocol is modified, we will quickly convey the plan of important protocol modification (such as changes in qualification criteria, results and analysis) to relevant parties (such as researchers, REC / IRB, test participants, test registry, journals and regulatory agencies) to ensure the accuracy of the experiment.
Ethics and Dissemination
Clinicians received written informed consent from each patient participating in the study before the study commences. Any adverse reactions and adverse factors caused by the test will be terminated. In case of injury caused by participating in the trial, special care will be given and compensation will be made according to relevant regulations. This study was approved by the Ethics Committee of Reproductive Medicine Ethics Committees of the Affiliated Hospital of Shandong University of TCM (SDTCM-RM-2022.611) in Jinan City, Shandong Province, China. The findings of this study were widely disseminated via conference papers, research reports, and academic publications.
Likewise, data will be electronically inputted, saved, and encrypted in secure computer files available only to the study’s research team and investigators. Additionally, the original study forms will be kept and maintained at the study location for three years after the end of the study. Also, the investigators will permit Institutional Review Board/Independent Ethics Committee (IRB/IEC) evaluations, audits, and monitoring of the trial’s data sources and required documents. Subsequently, participants will be asked to contact their physician with any study-related concerns.
Trial Status
This trial is at version 1.7, 29 August 2020 (ChiTR). The actual study start date was 5 January 2023 and the anticipated study end date is 31 December 2025. The recruitment start date was 15 January 2023; The anticipated recruitment end date is 31 October 2025.
Discussion
Premature LH surge is characterized as an LH level of 10 IU/L and a P level of 1.0ng/mL, and is produced by numerous follicle recruitment and fast estrogen rise.25,26 Premature LH surge during ovarian stimulation in IVF is detrimental to egg development, resulting in luteinization and premature ovulation, leading to poor reproductive results and even cycle cancellation.4 Although this is still disputed, pregnancy rates with the GnRH-ant protocol have been reported to be lower than those with the GnRH-agonist protocol, with reduced endometrial receptivity being the primary reason for this discrepancy. Reduced GnRH-ant dosages have been used by physicians in reproductive clinics to try to obtain acceptable pregnancy chances. However, the optimal daily dosage of GnRH-ant continues to be hotly debated. At the moment, 0.25 mg of Cetrorelix per day starting on day 5 or 6 of ovarian stimulation is considered the standard GnRH-ant protocol, and the LH level may be controlled within a safe range with this procedure. According to some other studies, limiting the GnRH-ant dosage to 0.125–0.2 mg per day is also beneficial. Daily GnRH-ant dosage requirements for the GnRH-ant regimen, we believe, should be determined on an individualized level. Based on previous studies,15,27 we tried to reduce the initial daily dose of cetrorelix to 0.125 mg, which was then individually adjusted to 0.25 mg based on LH levels during controlled ovarian stimulation and as a GnRH-ant half-dose group, furthermore individuals assigned to the GnRH-ant conventional-dose group will receive 0.25 mg cetrorelix daily for the duration of the controlled ovarian stimulation.
A panel of seasoned professionals will perform this randomized controlled study. Based on our experience in conducting RCTs, this study will demonstrate that GnRH-ant half-dose group has a convincing effect on improving reproductive outcomes in patients with predicted normal response, compared to GnRH-ant conventional-dose group.
Abbreviations
GnRH-ant, gonadotropin-releasing hormone antagonists; IVF-ET, in vitro fertilization-embryo transfer; FET, frozen-thawed embryo transfer; RCT, randomized controlled trial; COH, controlled ovarian hyperstimulation; OHSS, ovarian hyperstimulation syndrome; OS, ovarian stimulation; LH, luteinizing hormone; AFC, antral follicle count; PCOS, polycystic ovary syndrome; FSH, follicle-stimulating hormone; BMI, body mass index; r-hCG, recombinant human chorionic gonadotropin; ICSI, intracytoplasmic sperm injection; CRF, case report form; TCM, traditional Chinese medicine.
Ethics Approval and Consent to Participate
We confirm that this trial will be conducted in accordance with the principles of the Declaration of Helsinki. This study was approved by the Reproductive Medicine Ethics Committee of the Affiliated Hospital of Shandong University of TCM (SDTCM-RM-2022.611) in Jinan, Shandong, China. All participate will be required to sign written informed consent.
Acknowledgments
We appreciate Jing-Yan Song and Zhen-Gao Sun for their valuable support in designing this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 81874484). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bosch E, Broer S, Griesinger G. ESHRE Guideline: ovarian stimulation for IVF/ICSI (dagger). Hum Reprod Open. 2020;2020(2):hoaa009. doi:10.1093/hropen/hoaa009
2. Copperman AB, Benadiva C. Optimal usage of the GnRH antagonists: a review of the literature. Reprod Biol Endocrinol. 2013;11:20. doi:10.1186/1477-7827-11-20
3. Xiao JS, Su CM, Zeng XT. Comparisons of GnRH antagonist versus GnRH agonist protocol in supposed normal ovarian responders undergoing IVF: a systematic review and meta-analysis. PLoS One. 2014;9(9):e106854. doi:10.1371/journal.pone.0106854
4. Al-Inany HG, Youssef MA, Ayeleke RO, Brown J, Lam WS, Broekmans FJ. Gonadotrophin-releasing hormone antagonists for assisted reproductive technology. Cochrane Database Syst Rev. 2016;4:CD001750. doi:10.1002/14651858.CD001750.pub4
5. Lambalk CB, Banga FR, Huirne JA, et al. GnRH accounting versus long agonist protocols in IVF: a systematic review and meta-analysis for patient antagonist type. Hum Reprod Update. 2017;23(5):560–579. doi:10.1093/humupd/dmx017
6. Al-Inany H, Aboulghar M. GnRH antagonist in assisted reproduction: a Cochrane review. Hum Reprod. 2002;17(4):874–885. doi:10.1093/humrep/17.4.874
7. Roque M, Haahr T, Geber S, Esteves SC, Humaidan P. Fresh versus elective frozen embryo transfer in IVF/ICSI cycles: a systematic review and meta-analysis of reproductive outcomes. Hum Reprod Update. 2019;25(1):2–14. doi:10.1093/humupd/dmy033
8. Xu B, Zhou M, Wang J, et al. Increased AIF-1-mediated TNF-alpha expression during implantation phase in IVF cycles with GnRH antagonist protocol. Hum Reprod. 2018;33(7):1270–1280. doi:10.1093/humrep/dey119
9. Xu B, Wang J, Xia L, Zhang D, Wu X, Zhang A. Increased uterine NK cell numbers and numbers in expression during the implantation phase in IVF cycles with GnRH antagonist protocol. Sci Rep. 2017;7:39912. doi:10.1038/srep39912
10. Marci R, Graziano A, Lo Monte G, et al. GnRH antagonists in assisted reproductive techniques: a review on the Italian experience. Eur Rev Med Pharmacol Sci. 2013;17(7):853–873.
11. Mokhtar S, Sadeghi MR, Akhondi MM, et al. ART outcomes in GnRH antagonist protocol (flexible) and long GnRH agonist protocol in randomized patients with polycystic ovary syndrome: a early clinical trial. J Reprod Infertil. 2015;16(3):148–154.
12. Kolibianakis EM, Venetis CA, Kalogeropoulou L, Papanikolaou E, Tarlatzis BC. Fixed versus flexible gonadotropin-releasing hormone antagonist administration in vitro fertilization: a randomized controlled trial. Fertil Steril. 2011;95(2):558–562. doi:10.1016/j.fertnstert.2010.05.052
13. Hsieh YY, Chang CC, Tsai HD. Comparisons of different dosages of gonadotropin-releasing hormone (GnRH) antagonist, short-acting form and single, half-dose, long-acting form of GnRH agonist during controlled ovarian hyperstimulation and in vitro fertilization. Taiwan J Obstet Gynecol. 2008;47(1):66–74. doi:10.1016/S1028-4559(08)60057-1
14. Chang YL, Hsieh YY, Tsai HD. Preliminary report on the effect of a lower dose of gonadotropin-releasing hormone antagonist (cetrorelix) on ovarian hyperstimulation in lower-weight Asian women. Taiwan J Obstet Gynecol. 2006;45(4):317–320. doi:10.1016/S1028-4559(09)60250-3
15. Kerimoglu OS, Ercan CM, Keskin U, Korkmaz C, Duru NK, Ergun A. Effect of a low dose of gonadotropin-releasing hormone antagonist on in vitro fertilization outcomes. Arch Gynecol Obstet. 2013;288(3):691–695. doi:10.1007/s00404-013-2806-z
16. Chen HJ, Lin YH, Hsieh BC, Seow KM, Hwang JL, Tzeng CR. Is a lower dose of cetrorelix acetate effective for prevention of LH surge during controlled ovarian hyperstimulation? J Assist Reprod Genet. 2006;23(6):289–292. doi:10.1007/s10815-006-9054-0
17. Wang HL, Lai HH, Chuang TH, et al. A patient friendly corifollitropin alfa protocol without routine pituitary suppression in normal responders. PLoS One. 2016;11(4):e0154123. doi:10.1371/journal.pone.0154123
18. Albano C, Smitz J, Camus M, Riethmuller-Winzen H, Van Steirteghem A, Devroey P. Comparison of different doses of gonadotropin-releasing hormone Cetrorelix during controlled ovarian hyperstimulation. Fertil Steril. 1997;67(5):917–922. doi:10.1016/S0015-0282(97)81407-0
19. Albano C, Felberbaum RE, Smitz J, et al. Ovarian stimulation with HMG: results of a prospective Phase III European study comparing the einizing hormone-releasing hormone (LHRH) -cetrorelix and the LHRH-agonist antagonist buserelin. Eur Cetrorelix Study Group Hum Reprod. 2000;15(3):526–531. doi:10.1093/humrep/15.3.526
20. Engel JB, Ludwig M, Felberbaum R, Albano C, Devroey P, Diedrich K. Use of cetrorelix in combination with clomiphene citrate and gonadotrophins: a friendly approach to ‘IVF’? Hum Reprod. 2002;17(8):2022–2026. doi:10.1093/humrep/17.8.2022
21. Xu DF, Liu PP, Fan L, et al. GnRH antagonist weakens endometrial stromal cells growth ability by decreasing c-kit receptor expression. Reprod Biol Endocrinol. 2022;20(1):29. doi:10.1186/s12958-021-00886-y
22. Yeung T, Chai J, Li R, Lee V, Ho PC, Ng E. A double-blind randomized controlled trial on the effect of dehydroepiandrosterone on ovarian reserve markers, ovarian response, and number of responders in normal ovarian oocytes. BJOG. 2016;123(7):1097–1105. doi:10.1111/1471-0528.13808
23. Xu B, Li Z, Zhang H, et al. Serum progesterone level effects on the outcome of in vitro fertilization in patients with different ovarian response: an analysis of more than 10,000 cycles. Fertil Steril. 2012;97(6):1321–1327. doi:10.1016/j.fertnstert.2012.03.014
24. Zaat T, Zagers M, Mol F, Goddijn M, van Wely M, Mastenbroek S. Fresh versus frozen embryo transfers in assisted reproduction. Cochrane Database Syst Rev. 2021;2(2):CD011184. doi:10.1002/14651858.CD011184.pub3
25. Olivennes F, Belaisch-Allart J, Emperaire JC, et al. Prospective, randomized, controlled study of in vitro fertilization-embryo transfer with a single dose of a luteinizing hormone-releasing hormone (LH-RH) antagonist (cetrorelix) or a depot formula of an LH-RH agonist (triptorelin). Fertil Steril. 2000;73(2):314–320. doi:10.1016/S0015-0282(99)00524-5
26. Engel JB, Felberbaum RE, Eilers W, Polack S, Ortmann O, Diedrich K. Clomiphene-induced LH surges and cetrorelix. Reprod Biomed Online. 2002;5(2):109–111. doi:10.1016/S1472-6483(10)61611-2
27. Zhang D, Xia L, Xu H, et al. Flexible low-dose GnRH antagonist protocol is effective in patients with sufficient ovarian reserve in IVF. Front Endocrinol. 2018;9:767. doi:10.3389/fendo.2018.00767
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.