")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Effect of COVID-19 Pandemic on Diagnosis and Treatment Delays in Urological Disease: Single-Institution Experience
Authors Li Z, Jiang Y, Yu Y, Kang Q
Received 8 January 2021
Accepted for publication 17 February 2021
Published 4 March 2021 Volume 2021:14 Pages 895—900
DOI https://doi.org/10.2147/RMHP.S299233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Zhen Li,1,* Yu Jiang,2,* Yang Yu,3,* Qianyu Kang3,*
1Department of Urology, The Fifth People’s Hospital of Dalian, Dalian, Liaoning, People’s Republic of China; 2Department of Pediatrics, Dalian Municipal Women and Children’s Medical Center, Dalian, Liaoning, People’s Republic of China; 3Department of Urology, The Second Hospital of Dalian Medical University, Dalian, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qianyu Kang; Yang Yu
Department of Urology, The Second Hospital of Dalian Medical University, 467 Zhongshan Road, Shahekou District, Dalian, Liaoning, 116023, People’s Republic of China
Tel +86-180-1895-0098
; +86-180-9887-7887
Email [email protected]; [email protected]
Purpose: In the background of the global pandemic, we aim to investigate the effect of COVID-19 on diagnosis and treatment delay in urology patients.
Patients and Methods: A total of 4919 inpatients were identified from the urological department in our institution, including 2947 and 1972 patients within 9 months before and after the outbreak (group A and group B). The baseline characteristics and residential population of different types of diseases were compared in the two groups. Patients who underwent delay of diagnosis or treatment with poor outcomes were described.
Results: Our result revealed a 33.1% decrease of total resident population as well as a 44.8% decline in bed utilization rate after the outbreak. Significant differences were found between group A and group B in gender (P=0.024) and patients living alone or not (P=0.026). The hospitalization rate of patients with malignancy increased significantly while that of benign patients decreased during the epidemic (P< 0.001). Besides, we identified 5 cases with bladder cancer and 3 cases with prostate cancer that underwent delay of diagnosis or treatment with unfavorable consequences.
Conclusion: With the impact of COVID-19, delay in diagnosis or treatment of non-COVID-19 diseases is inevitable whether the medical resources allocation is effective or not. Psychological status of patients might be the major cause of postponing diagnosis or treatment. For urological patients with locally advanced tumor or rapid progression, who need long-term postoperative intervention, the delay of regular treatment could lead to inevitable progression or recurrence.
Keywords: COVID-19, benign disease, prostate cancer, bladder cancer
Introduction
The pandemic disease that swept across the globe in 2020, which was named coronavirus disease 2019 (COVID-19), was initially identified in Wuhan City, China, in December 2019.1 Since the outbreak of the epidemic, the Chinese government has taken strict isolation measures to keep social distancing and prevent further spread of the disease, including the lockdown of areas with concentrated outbreaks, such as Wuhan City. Hospitals across the country strengthened the monitoring and screening of imported asymptomatic cases to avoid potential hospital outbreaks of COVID-19.2 For non-emergency patients who had visited the epidemic areas without fever or COVID-19-related respiratory symptoms, a minimum 14 days of medical observation was required before visiting the hospital.
Due to the strictness of hospital regulations for outpatient and inpatient visits and resource allocation, the outbreak of COVID-19 may have side effects on the diagnosis and treatment of normal patients, with a consequent major modification of the clinical practice of urological patients.3 This article attempts to compare the characteristics and population of urological inpatients in our institution within 9 months before and after January 31, 2020, when institutional anti-COVID-19 measures were activated, and discuss its effect on the treatment delays of benign and malignant urological diseases.
Patients and Methods
Data Collection and Analysis
The study protocol was approved by the ethics committee of the Second Hospital of Dalian Medical University. The data are anonymous, and the requirement for informed consent was therefore waived. The study was conducted in accordance with the principles of the Declaration of Helsinki. Patient data confidentiality and compliance were guaranteed. A total of 4919 inpatients recorded in the urological department were identified from our institution between May 1, 2019 and November 14, 2020, and the data of all patients were collected from their medical documents. Outbreak in this study is defined as the date when the government took isolation and restrictive measures, and the hospital took measures to prevent nosocomial infection of COVID-19, i.e., January 31, 2020. The cohort was divided into two groups according to the date. Group A included patients from May 1, 2019 to January 31, 2020, and group B included patients from February 1, 2020 to November 14, 2020. The baseline characteristics of the two groups were compared, including gender, age, residence location, living alone or not, average length of stay and bed utilization rate. The proportions of patients with different type of diseases were also compared in the two groups. Patients who underwent delay of diagnosis or treatment due to the influence of COVID-19 with adverse consequences were individually described.
Clinical Management Path
Except for a two-week closure in April 2020, all people could visit the clinic with a green tour code on their phone (which can prove that you did not visit an epidemic area within 14 days and is admitted on a nation-wide scale). For patients who needed residential treatment, routine blood test, a negative result of reverse transcriptase-polymerase chain reaction (RT-PCR) for coronavirus and chest computed tomography (CT) without suspicious signs of pneumonia were essentially required before hospitalization. The results of all the tests could be obtained within one or two days. For emergency patients requiring admission, an isolation ward and private operation room were provided, and after achieving negative RT-PCR result and non-suspicious chest CT, isolation management was terminated. Only one accompanying person was allowed for each patient during the pandemic and a negative result of coronavirus was required.
Statistical Methods
We performed chi-square and t-test on the baseline clinical characteristics and type of diseases. A two-sided P-value was calculated and P<0.05 was considered significant. All the statistical analyses used SPSS 21.0.
Results
There were 2947 and 1972 patients in group A and group B, respectively. The baseline characteristics of the two groups are described and compared in Table 1. The result shows that the proportion of female patients increased (P=0.024) and the proportion of patients living alone decreased significantly after the outbreak (P=0.026). Besides, due to the reduction of the inpatient population, the utilization rate of beds declined by 44.8% after the outbreak. The proportion of different types of diseases was recorded and compared in Table 2. It demonstrated that despite an overall decline in the number of inpatients, the hospitalization rate of patients with malignant tumor significantly increased while that of patients with benign disease significantly decreased (P<0.001). In patients with malignancy, the proportion of ureteral and prostate cancer decreased by 3.6% and 4.1%, respectively, while the others increased. And in patients with benign diseases, the proportion of benign prostatic hyperplasia (BPH), cyst, endocrinotherapy, neurogenic bladder and overactive bladder (OAB) reduced by 0.6%, 1.5%, 2.2%, 0.5% and 0.3%, respectively, with endocrinotherapy the most.
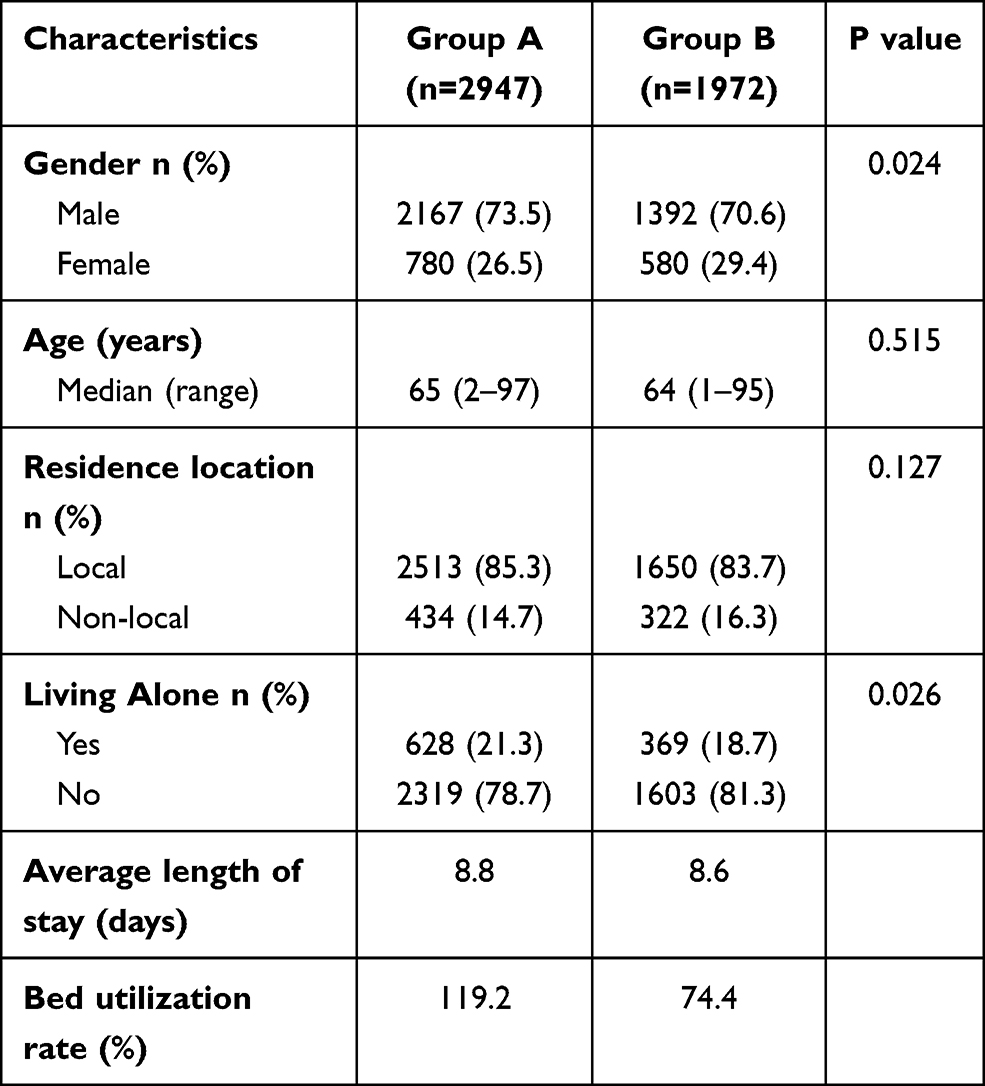 |
Table 1 Comparison of the Baseline Characteristics of Inpatients Before and After the Outbreak of COVID-19 |
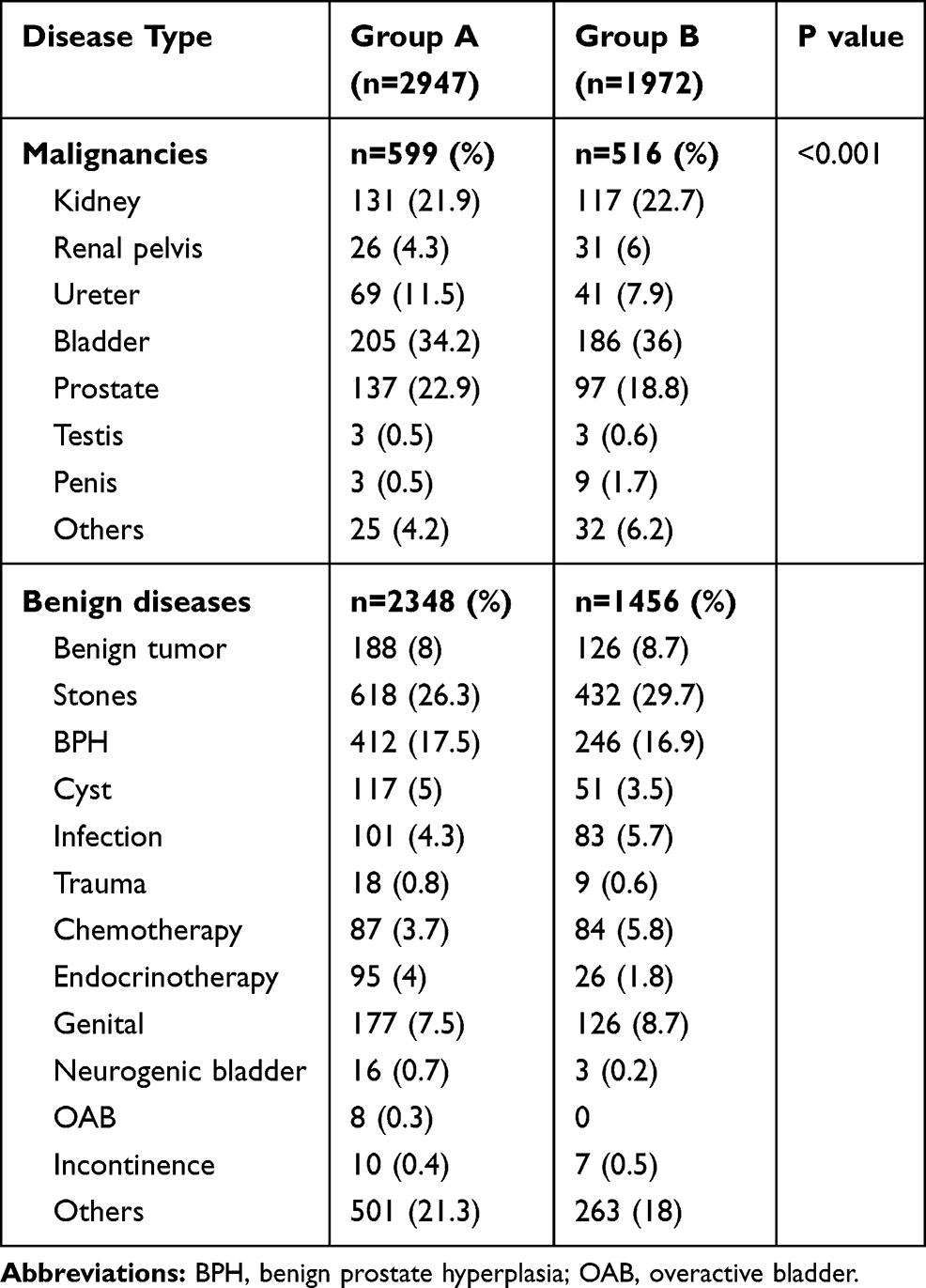 |
Table 2 Comparison of Inpatients Number in Different Urological Diseases Before and After the Outbreak of COVID-19 |
We identified 5 cases with bladder cancer and 3 cases with prostate cancer who underwent delay of diagnosis or treatment due to the impact of COVID-19. The detailed information of these 8 cases is summarized in Table 3. The descriptions of 4 representative cases are as follows. Case 1 is an 81-year-old man who presented with intermittent painless gross hematuria since February 2020. However, out of concern about the epidemic situation, he chose to come to the hospital 10 months after the observation of symptoms. Cystoscopy showed a 3-cm sessile tumor on the right side of the bladder wall close to the ureteral orifice and a 1-cm pedicled tumor on the upper side of the bladder. Due to the size and shape of the tumor, this patient eventually underwent robot-assisted laparoscopic partial cystectomy. Case 2 is a 68-year-old man with bladder tumor (T1N0M0) who underwent trans urethral resection of bladder tumor (TURBT) twice in the last 4 years. The patient stopped regular intravesical instillation after the outbreak and cystoscopy in October 2020 revealed a 1-cm tumor on the upper side of the bladder. The patient had to undergo TURBT for a third time. Case 3 is a 58-year-old man diagnosed with prostate cancer (T4N2M1c). He had been receiving endocrine therapy (bicalutamide + goserelin) for 2 years. The prostate specific antigen (PSA) value in the last examination before the outbreak was 0.53 ng/mL, and after two-time suspension of endocrine therapy for 3 months from February to October, it increased to 1.42 and then 5.77 ng/mL, which is defined as biochemical progress with no positive sign of clinical progress. Case 4 is a 67-year-old man with prostate cancer (T3aN0M0), who had been receiving endocrine therapy (goserelin + flutamide) after radical prostatectomy. He suspended the endocrine therapy for 6 months during the epidemic and was eventually diagnosed with biochemical recurrence with an increase of PSA.
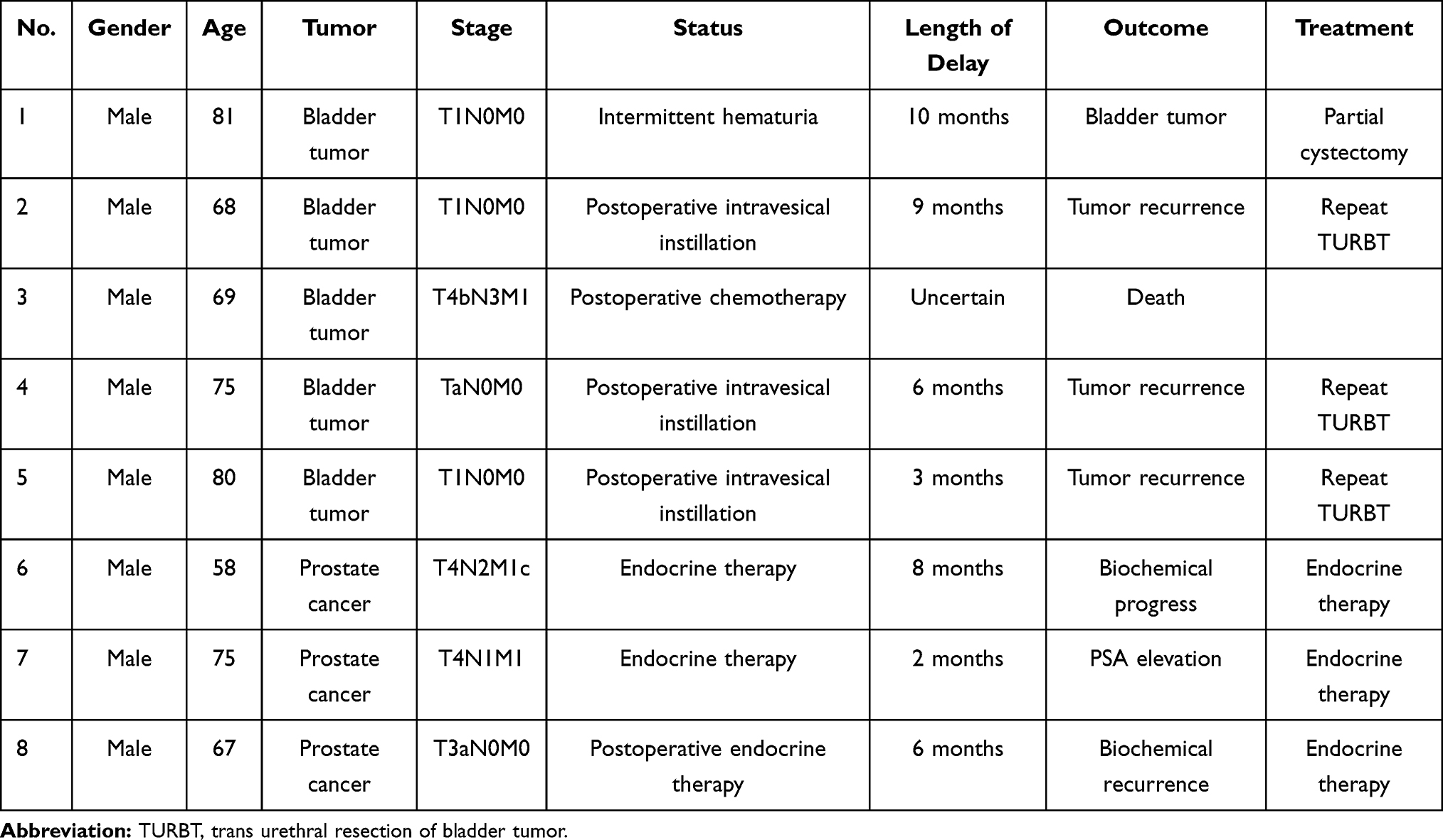 |
Table 3 Detailed Information of Patients Who Underwent Delay of Diagnosis or Treatment During COVID-19 |
Discussion
The outbreak of COVID-19 in 2020 profoundly affected medical care systems all over the world. As the detector of the pandemic, the Chinese government has attached great importance to the prevention and control of the situation from the very beginning. Local governments also responded very quickly to the strict isolation measures to prevent further spread of the disease after the lockdown of Wuhan City in late January 2020. Except for Hu Bei province, which was the epicenter of COVID-19, the epidemic situation in most regions of China was quickly under control by the end of February or March. People diagnosed with COVID-19 are transferred to the Infectious Disease Hospital for centralized treatment. Normal patients can still get outpatient consultations and necessary hospitalization in major hospitals during the epidemic period. The extra effort for COVID-19 screening with a standard workup only added 1–2 days to the waiting time of hospitalization.
In these circumstances, we compared the number of urological inpatients in our institution within 9 months before and after the launch of the epidemic control policies. Despite the viable access to medical treatment, the results of our study revealed a 33.1% decrease of the total resident population in the urological department as well as a 44.8% decline of the bed utilization rate, which probably represented a diagnosis or treatment delay of urological diseases under the context of the emerging infectious disease. In a recent study, Ferrara et al. reported a 44.9% drop of cancer diagnoses in 2020 compared with 2018 and 2019 in Northern and Central Italy, including a 45% and 43.6% diagnostic decrease in prostate and bladder cancer, respectively.4 Our study revealed a 10.7%, 40.6%, 9.3% and 29.2% decrease in the number of hospitalizations in renal, ureteral, bladder and prostate cancer, respectively.
Our result also showed that there is a significant difference in hospitalization decrease between malignant and benign urological diseases (P<0.001), which might indicate that patients with benign diseases were more likely to postpone their resident treatment in the impact of an epidemic. The outbreak response plan mainly focuses on the medical needs of those with immediate necessity and urgency, with limited attention to the delay of benign disease management.5,6 It is noteworthy that these patients could also experience extra anxiety and poor quality of life due to the incomplete treatment in this situation. Further investigation of the influence of COVID-19 on patients with benign conditions is still needed.
Significant disparities are also found in gender (P=0.024) and if the patient is living alone (P=0.026), which might be considered that patients without companions are less likely to go to the hospital during the epidemic situation. It is noteworthy that many patients would go to big cities seeking diagnosis and treatment, and multiple round-trips between cities might be a disadvantage to timely treatment under the restrictive policies of the hospital. However, there was no significant reduction of non-local patients after the outbreak in our study.
Besides the consequences of the epidemic itself, the delay of diagnosis or treatment for non-COVID-19 diseases, especially cancers, are the most common negative effects. Studies from China have demonstrated that patients with cancer were exposed to a higher risk of infection with COVID-19, and experienced worse outcomes after infection during the COVID-19 epidemic.7,8 However, in the case of cancer treatment, the postponement of a necessary scheduled treatment may represent a therapeutic disadvantage and have a significant impact on the prognosis of disease.
In the urological field, this consideration is of utmost relevance for patients with high-risk non-muscle-invasive bladder cancer (NMIBC) who require repeat visits to hospital for intravesical instillations of chemotherapeutic agents or Bacillus Calmette-Guérin (BCG) to decrease the risk of recurrence and progression after transurethral resection of the bladder (TURB).9,10 The median age of initial diagnosis of bladder cancer is over 70 years old and it has been reported that almost 30% of patients older than 65 years old may develop acute respiratory distress syndrome (ARDS) after contracting COVID-19.2,11 Therefore, the likelihood of being infected may hinder the patient’s initiative to visit hospital. In our study, 5 cases with bladder cancer were identified with delayed diagnosis or treatment associated with COVID-19. One case experienced diagnosis delay and one case is metastatic bladder cancer without regular chemotherapy. The other 3 cases are all postponement of regular intravesical instillation without permission during the epidemic. As a result, 4 of the patients experienced development or recurrence of bladder tumor in varying stages and required additional operations. Telephone contact revealed that the reasons for postponing chemotherapy included the anxiety of COVID-19 infection and intolerance of the side effects of chemotherapy, such as cystitis and hematuria. For diagnosing bladder cancer, Wallace et al. found that the delay from onset of symptoms to going to a doctor greater than 14 days had a consequent higher tumor stage and worse survival outcomes of 5% at 5 years compared with no delay.12 During the epidemic, patients tended to postpone their plan for visiting the hospital unless the symptoms were intolerable. One patient in our study did not come to the hospital until 10 months after the initial symptoms, which ultimately caused tumor progression and inevitable partial cystectomy. This stresses the importance of continuing to seek medical advice and performing screening cystoscopies during the epidemic for patients suspected to have bladder cancer in order to accurately identify the aggressiveness of the disease.
Adjuvant hormone therapy (AHT) after radical prostatectomy (RP) is one of the most common approaches for high-risk localized and locally advanced prostate cancer treatment.13 For metastatic prostate cancer, hormone therapy alone is also an acceptable method for treatment. Studies show patients who received AHT had a significant improvement in survival, recurrence and mortality outcomes.14 In our study, 3 patients postponed their hormone therapy during the outbreak, ranging from 2 to 8 months, and all of them were detected with elevation of prostate specific antigen (PSA) value. However, patients may have slow progression despite increasing PSA following RP and adjuvant hormonal therapy.15 In our study, no local progression or metastasis of tumor was observed despite biochemical progression or recurrence. Telephone contact revealed that the postponement of endocrine therapy is specifically associated with the worry about COVID-19 infection. In a previous study, van Tol-Geerdink et al. investigated 288 patients with prostate cancer and found a mild increase in depression in patients receiving hormonal therapy, which appeared to be related to both the hormone therapy and the high-risk status of diseases.16 Recent studies also demonstrated that patients with oncology presented an additional increase of mental stress during the COVID-19 crisis, leading to lower quality of life.17,18
Patients are shielding by minimizing the frequency of visiting hospital and staying home as much as possible, especially older patients, who are encouraged to do so. However, for urological patients with locally advanced tumor and rapid progression, we suggested that the patients should be treated in time, in case the optimal time frame of treatment is missing. For malignancies need long-term postoperative intervention, such as bladder and prostate cancer, postponing regular treatment without permission may increase the risk of recurrence. Healthcare systems should attempt to find a balance between minimizing the treatment process and protecting the safety of staff and patients during the pandemic.19 The crisis also strengthens the importance of improving internet medical care, so that patients with mild symptoms can have convenient consultations without approaching hospitals. A recent study of 399 urology patients showed that 63.2% were eligible for telemedicine and 84.7% preferred a telemedical consultation during the COVID-19 period.20
There were several limitations of this study. First, there is a selection bias for its retrospective nature, with small samples in a single center. Second, there are no long-term survival follow-up data for the patients with PSA elevation to fully evaluate the impact of delay on the prognosis of patients.
Conclusion
In the context of the global pandemic, delay in diagnosis or treatment of non-COVID-19 diseases is inevitable whether the medical resources allocation is effective or not. Psychological status of patients should be the major factor for postponing diagnosis or treatment. We suggest strengthening the psychological guidance of patients in the pandemic period, since for urological patients with locally advanced tumor or rapid progression, who need long-term postoperative intervention, such as prostate and bladder tumor, the delay of regular treatment could increase the risk of progression or recurrence.
Acknowledgments
Author Qianyu Kang expresses the deepest gratitude to her mentor, Prof Bo Yang, for his frequent encouraging and positive guidance in the past three years. Zhen Li and Yu Jiang contributed to the work equally and should be regarded as co-first authors. Yang Yu and Qianyu Kang contributed to the work equally and should be regarded as co-corresponding authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–733. doi:10.1056/NEJMoa2001017
2. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708–1720. doi:10.1056/NEJMoa2002032
3. Puliatti S, Eissa A, Eissa R, et al. COVID-19 and urology: a comprehensive review of the literature. BJU Int. 2020;125:E7–E14. doi:10.1111/bju.15071
4. Ferrara G, De Vincentiis L, Ambrosini-Spaltro A, et al. Cancer diagnostic delay in Northern and Central Italy during the 2020 lockdown due to the Coronavirus Disease 2019 pandemic. Am J Clin Pathol. 2020. doi:10.1093/ajcp/aqaa243
5. Ford ES, Mokdad AH, Link MW, et al. Chronic disease in health emergencies: in the eye of the hurricane. Prev Chronic Dis. 2006;3:A46.
6. Slama S, Kim HJ, Roglic G, et al. Care of non-communicable diseases in emergencies. Lancet. 2017;389:326–330. doi:10.1016/S0140-6736(16)31404-0
7. Liang W, Guan W, Chen R, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21:335–337. doi:10.1016/S1470-2045(20)30096-6
8. Yu J, Ouyang W, Chua MLK, Xie C. SARS-CoV-2 transmission in patients with cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol. 2020;6:1108–1110. doi:10.1001/jamaoncol.2020.0980
9. Pawinski A, Sylvester R, Kurth KH, et al. A combined analysis of European Organization for Research and Treatment of Cancer, and Medical Research Council randomized clinical trials for the prophylactic treatment of stage TaT1 bladder cancer. European Organization for Research and Treatment of Cancer Genitourinary Tract Cancer Cooperative Group and the Medical Research Council Working Party on Superficial Bladder Cancer. J Urol. 1996;156:
10. Sylvester RJ, Oosterlinck W, Witjes JA. The schedule and duration of intravesical chemotherapy in patients with non-muscle-invasive bladder cancer: a systematic review of the published results of randomized clinical trials. Eur Urol. 2008;53:709–719. doi:10.1016/j.eururo.2008.01.015
11. Lenfant L, Seisen T, Loriot Y, Rouprêt M. Adjustments in the use of intravesical instillations of bacillus calmette-guérin for high-risk non-muscle-invasive bladder cancer during the COVID-19 pandemic. Eur Urol. 2020;78:1–3. doi:10.1016/j.eururo.2020.04.039
12. Wallace DM, Bryan RT, Dunn JA, Begum G, Bathers S. Delay and survival in bladder cancer. BJU Int. 2002;89:868–878. doi:10.1046/j.1464-410X.2002.02776.x
13. Das M. Androgen deprivation therapy for prostate cancer. Lancet Oncol. 2017;18:e567. doi:10.1016/S1470-2045(17)30670-8
14. Liu F, Sun D, Zhou X, et al. Effect of adjuvant hormone therapy in patients with prostate cancer: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2018;97:e13145. doi:10.1097/MD.0000000000013145
15. Sengupta S, Blute ML, Bagniewski SM, et al. Increasing prostate specific antigen following radical prostatectomy and adjuvant hormonal therapy: doubling time predicts survival. J Urol. 2006;175:
16. van Tol-geerdink JJ, Leer JW, van Lin EN, Schimmel EC, Stalmeier PF. Depression related to (neo)adjuvant hormonal therapy for prostate cancer. Radiother Oncol. 2011;98:203–206. doi:10.1016/j.radonc.2010.12.006
17. Juanjuan L, Santa-Maria CA, Hongfang F, et al. Patient-reported outcomes of patients with breast cancer during the COVID-19 outbreak in the epicenter of China: a cross-sectional survey study. Clin Breast Cancer. 2020;20:e651–e662. doi:10.1016/j.clbc.2020.06.003
18. Frey MK, Ellis AE, Zeligs K, et al. Impact of the coronavirus disease 2019 pandemic on the quality of life for women with ovarian cancer. Am J Obstet Gynecol. 2020;223:
19. Fauci AS, Lane HC, Redfield RR. Covid-19 - navigating the uncharted. N Engl J Med. 2020;382:1268–1269. doi:10.1056/NEJMe2002387
20. Boehm K, Ziewers S, Brandt MP, et al. Telemedicine online visits in urology during the COVID-19 pandemic-potential, risk factors, and patients’ perspective. Eur Urol. 2020;78:16–20. doi:10.1016/j.eururo.2020.04.055
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.