")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Effect of Comprehensive Nursing Based on Cognitive Behavior on Psychological Function of Glioma Patients
Received 10 October 2020
Accepted for publication 5 January 2021
Published 10 March 2021 Volume 2021:17 Pages 777—785
DOI https://doi.org/10.2147/NDT.S286164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Yu-Hong Zhao, Yan Xu
Operating Room, Linyi Central Hospital, Linyi, Shangdong, 276400, People’s Republic of China
Correspondence: Yan Xu
Operating Room, Linyi Central Hospital, No. 17 Health Road, Yicheng Street, Yishui County, Linyi, Shangdong, 276400, People’s Republic of China
Tel +86-15964811679
Email [email protected]
Objective: The aim of our current study is to explore the effect of comprehensive nursing based on cognitive behavior on the psychological function of glioma patients.
Methods: A total of 108 patients with glioma were randomly divided into intervention group (n = 54) and control group (n = 54). Patients in the control group were given routine nursing for 3 months, while patients in the intervention group were given comprehensive nursing based on cognitive behavior for 3 months on the basis of control group. Parameters such as scores of simplified Fear of Progression Questionnaire-Short Form (FoP-Q-SF), Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS) as well as cancer-related fatigue and quality of life (QOL) were compared before and after the intervention.
Results: No significant difference was observed in the scores of FoP-Q-SF, SAS, SDS, cancer-related fatigue and quality of life between the two groups before intervention (P > 0.05). Conversely, after the intervention, the scores of FoP-Q-SF, SAS, SDS and cancer-related fatigue in the intervention group were significantly lower than those in the control group, and the scores of life quality in the intervention group were significantly higher than those in the control group (all P values < 0.05).
Conclusion: Our findings provide evidence that comprehensive nursing based on cognitive behavior can effectively improve the negative psychological state of patients such as anxiety and depression and cancer-related fatigue with improved life quality for patients harboring glioma.
Keywords: comprehensive nursing based on cognitive behavior, glioma, psychological function
Introduction
Glioma is common in clinical neurosurgery, accounting for about 60% of intracranial tumors with malignant feature.1 Its main characteristics include refractoriness, recurrence and local diffusion, with only 50% survival rate within 5 years and poor prognosis.2 Given the negative characteristics of the disease, the mental health and life quality of patients are seriously impaired. At present, surgery, radiotherapy and chemotherapy are widely used in the treatment of glioma, in which radiotherapy and chemotherapy can effectively prolong the survival time of patients and improve their quality of life. Nevertheless, patients have to suffer from great psychological pressure and physical discomfort in the process of radiotherapy and chemotherapy. Most of the patients will be influenced by varying degrees of pessimism, fear, anxiety and other negative emotions, which affects their adherence to the proposed treatments.3
Comprehensive nursing care based on cognitive behavior aims to correct patients' poor recognition of their disease, through cognitive evaluation, reconstruction and intervention measures, and encourages patients to improve their cognitive ability and behavior toward the disease through continuity, sustainability and comprehensive integrated nursing. Research results showed that cognitive behavior comprehensive nursing can effectively reduce the fear of disease progression in patients with glioma and relieve patients’ anxiety, depression and other negative psychology.4 Comprehensive nursing based on cognitive behavior seeks to provide help to patients for their negative cognition of the disease, which is corrected by cognitive evaluation, reconstruction and intervention. However, there are few comprehensive intervention measures in China about how to improve the mental state and cancer-related fatigue of glioma patients and improve their quality of life. Based on this, this study will explore the effects of cognitive behavior-guided comprehensive care on the psychological function of glioma patients. And our current study aims to help patients strengthen each process through continuous, comprehensive nursing, in an attempt to improve their cognitive ability and behavior toward the disease.
Methods
General Information
Following clinical examination, 108 patients with glioma were treated in the neurosurgery department of our hospital from February 2018 to February 2019. They were randomly divided into intervention group (n = 54) and control group (n = 54). The study was approved by the Ethics Committee of Linyi Central Hospital. The study was performed in accordance with the requirements of the Helsinki Declaration, and written informed consents were received from all patients. In order to prevent mutual contamination, the patients in the control group and the patients in the intervention group were separated. Patients with cognitive impairment were assessed and screened by mini-mental state examination (MMSE) and Montreal Cognitive Assessment Scale (MoCA): that is, the MMSE score ranges from 0 to 30, withscores less than 25 indicating cognitive impairment; and the MoCA score ranges from 0 to 30, with scores less than 26 indicating cognitive impairment.
Inclusion and Exclusion Criteria
Patients that met the inclusion criteria were included in our study: 1) patients who were admitted to hospital for the first time without earlier anti-tumor treatment before admission; 2) patients with pathologically diagnosed primary glioma; 3) patients and their families who agreed and signed informed consent; 4) patients with complete clinical data; 4) patients who were conscious; 5) patients with the ability to read and understand. Exclusion criteria were as follows: 1) patients participating in other researches; 2) patients with mental retardation or cognitive impairment; 3) patients without sufficient clinical data; 4) patients harboring serious diseases of other organs; 5) patients who had taken psychotropic drugs in the past 3 months; 6) patients with poor compliance or withdrawal.
Interventions
Control Group
Patients in the control group were given routine nursing for 3 months. The primary nurse neurosurgical department helped glioma patients with health education, medication guidance, reasonable healthy diet, psychological guidance and so on.
Intervention Group
In addition to the nursing care given in the control group, patients in the intervention group were given comprehensive nursing based on cognitive behavior for 3 months. The details were as follows: (1) A comprehensive nursing team based on cognitive behavior was established, which was composed of one chief neurosurgeon, one clinical rehabilitation therapist, one psychologist and one head nurse, as well as two nurses with more than 5 years of work experience. And in order to ensure the scientificity and objectivity of the implementation of the program, it was supervised and guided by the chief neurosurgeon and the psychologist. (2) Preoperative nursing: 1) Cognition evaluation: after admission, members of the group communicated with the patients in detail to understand the patients’ cognition and psychological status of their disease, and any misunderstandings relating to the disease should be corrected in time. Patients should be correctly guided. We answered the questions raised by the patients in a timely manner, and told them to communicate honestly with their family members and friends when encountering problems, in order to settle problems with spiritual and material support. At the same time, the family members of the patients were told how to correctly cooperate with the clinical nursing team and the importance and role of clinical nursing. The patients were evaluated with the FoP-Q-SF scale for the fear of disease progression. The self-rating scale of cancer-related fatigue was used to evaluate the patients’ cancer-related fatigue. SAS and SDS scores were used to evaluate the psychological status of patients, and QLQ-C30 was used to evaluate the quality of life of patients. 2) Reconstruction of cognition: the primary nurses distributed the self-made health education manuals about gliomas to the patients and their families, and the nurses explained the physiological discomfort and bad emotion of patients to their families in detail, in order to make family members fully understand the psychology of patients and give them more emotional support and attentive care. Patients who chose radiotherapy and chemotherapy were informed of the relevant side effects, reasonable diet and appropriate exercise. Health knowledge lectures on glioma were given every Tuesday and Friday for more understanding of the disease. In the course of the lecture, patients with better glioma recovery were invited to share their anti-cancer experience, and 30 min were reserved to encourage patients to communicate with each other, so as to build confidence and determination of patients to fight the disease. Those patients who were discharged again were guided to accept themselves again, find what they are interested in, realize self-worth in the process of completion and make a reasonable plan for the future life and reintegrate into the society. 3) Cognitive behavior intervention: patients were treated with music relaxation therapy with light music and postoperative rehabilitation training during hospitalization. Before treatment, patients were encouraged to relax their muscles and visualize their favorite scenes for 25 minutes at a time once a day. (3) Intraoperative nursing: the perioperative patients were informed in detail of the matters needing attention in the perioperative period and the possible postoperative complications, such as proper vital capacity training before an operation, proper lower limb movement to prevent venous thrombosis, etc. Before the operation, the team members consulted the patient in detail about the music they like and what they are interested in. During the operation, they played the patient's chosen music or talked about what the patient is interested in so as to distract the patient’s attention and alleviate the fear of surgery. (4) Postoperative nursing: when the vital signs of the patient returned to normal, the members of the group communicated effectively with the patient, and created a targeted individualized rehabilitation program for the patient according to the specific situation of the patient. And patients exercised in the hospital, in order to exercise at home after discharge. In the process of exercise, it was necessary to detect the physiological indicators and physical status and observe the effect of exercise. At the same time, team members informed the family members of the importance of family care, and told them in detail about creating a good communication environment and place at home and provide emotional support for the patients. (5) Follow-up: the patients were followed up by telephone or WeChat twice a week to avoid the negative emotion of the patients in time; the team members would ask the patients about their rehabilitation program and would answer questions in detail. At the same time, patients were told to pay attention to a healthy diet and eat smaller but more frequent meals, with more fresh fruits and vegetables and other foods with high vitamin and protein content for 3 months. (6) Evaluation: three months later, the patients were evaluated by the comprehensive nursing team based on cognitive behavior, and the FoP-Q-SF scale was used to evaluate the fear of disease progression. The self-rating scale of cancer-related fatigue was used to evaluate the patients’ cancer-related fatigue. SAS and SDS scores were used to evaluate the psychological status of patients; QLQ-C30 was used to evaluate the life quality, and the progress of each part was analyzed. The motivation of patients should be improved. During the intervention period, three patients in the intervention group were removed from this study due to hospital transfer, financial issues and liver cirrhosis, respectively. Therefore, there were 52 cases in total in the intervention group.
Outcome Measurements
The psychological function mainly includes the fear of the disease progression and the change of the patient’s psychological state. Cancer-related fatigue includes four dimensions: cognition, emotion, perception and behavioral severity, which mainly reflects the fatigue symptoms of patients. Quality of life mainly includes the assessment of patients’ emotional function, role function, physical function, cognitive function, overall quality of life and social function in six areas.
The scores of the simplified Fear of Progression Questionnaire-Short Form (FoP-Q-SF), SAS, SDS, cancer-related fatigue and quality of life were compared between the two groups before and after intervention.
FoP-Q-SF:5 the scale was analyzed by Chinese scholars Wu and Liu6 for the reliability and validity of FoP-Q (Germany, 2006) in Chinese in 2015. The Cronbach’s α coefficient was 0.883, with good reliability and validity. A total of 12 items were scored by Likert scale graded 1 to 5, all of which were reported by the patients themselves. “Always have” indicated 5 points, “no” indicated 1 point, and the maximum score was 60. In patients who were highly afraid of disease progression, 75% of the items would score more than 4 points. In patients with moderate fear of disease progression, 50% of the items would score more than 4 points. A higher score represented a higher degree of fear of disease progression.
SAS and SDS scores:7,8 they were developed by Chinese professor Zung; each scale is 20 items, with a score of 1 to 4 points, 4 points for most or all of the time, 3 points for most of the time, and 2 points for sometimes, and no or little time for 1 point. The scores of SAS and SDS were measured by the summed points of each item. The standard point was calculated through the sum of the points multiplied by 1.25, and the integer portion was retained. SAS and SDS scores have good effectiveness and objectivity for clinical research.
Cancer-related fatigue:9 the scale includes four dimensions: cognition, emotion, perception and behavioral severity, which can be divided into 27 items with a score of 0 to 10. According to the severity of symptoms, the score of severe fatigue is 10, and the score of no fatigue is 0. The more severe the fatigue symptoms, the higher the score.
Quality of life:10 the core questionnaire of quality of life (QLQ-C30) for cancer patients was used to evaluate the quality of life, with 100 points for each item. The lower the score, the lower the quality of life. It is divided into six functional areas: emotional function, role function, physical function, cognitive function, overall quality of life and social function. Some studies have confirmed that this questionnaire has been widely used in many countries with high reliability and validity.8
Statistical methods
SPSS 18.0 software was used for statistical analysis, and FoP-Q-SF, SAS, SDS scores and other measurement data were expressed as ( , score). T test was used for comparison, missing data were corrected by multiple imputation, and the evaluation results were analyzed by intentionality and sensitivity. Paired t-test was used for comparison between groups, and self-controlled t-test was used for comparison between groups before and after treatment. P < 0.05 indicated that there was statistical significance.
, score). T test was used for comparison, missing data were corrected by multiple imputation, and the evaluation results were analyzed by intentionality and sensitivity. Paired t-test was used for comparison between groups, and self-controlled t-test was used for comparison between groups before and after treatment. P < 0.05 indicated that there was statistical significance.
Results
Clinical Data of Patients
In the intervention group, there were 33 males and 21 females, ranging in age from 24 to 69 years old, with an average age of 49.05 ± 8.99 years. And the course of disease ranged from 2 to 6 months, with an average of 4.11 ± 0.34 months. The pathological grades were 20 cases of grade I–II and 34 cases of grade III–IV. The preoperative KPS (Karnofsky Performance Status) score was 75.26 ± 11.04. Three patients did not receive complete intervention treatment. The control group included 33 males and 21 females, ranging in age from 23 to 67 years old, aged 48.69 ± 8.92 years on average. The course of disease was 2 to 5 months, with an average of 4.09 ± 0.36 months; the pathological grades were 22 cases of grade I–II and 32 cases of grade III–IV. The preoperative KPS score was 76.11 ± 10.21. Four patients quit this study halfway, as shown in Figure 1. There was no significant difference in the general data between the two groups (P > 0.05), as shown in Table 1. During the treatment period, 1 patient in the control group was transferred to another hospital and 3 patients with personal financial problems were excluded from this study, hence there were a total of 51 patients in the control group. In addition, three patients in the intervention group were removed from this study due to hospital transfer, financial issues and liver cirrhosis, respectively. Therefore, there were 52 cases in total in the intervention group.
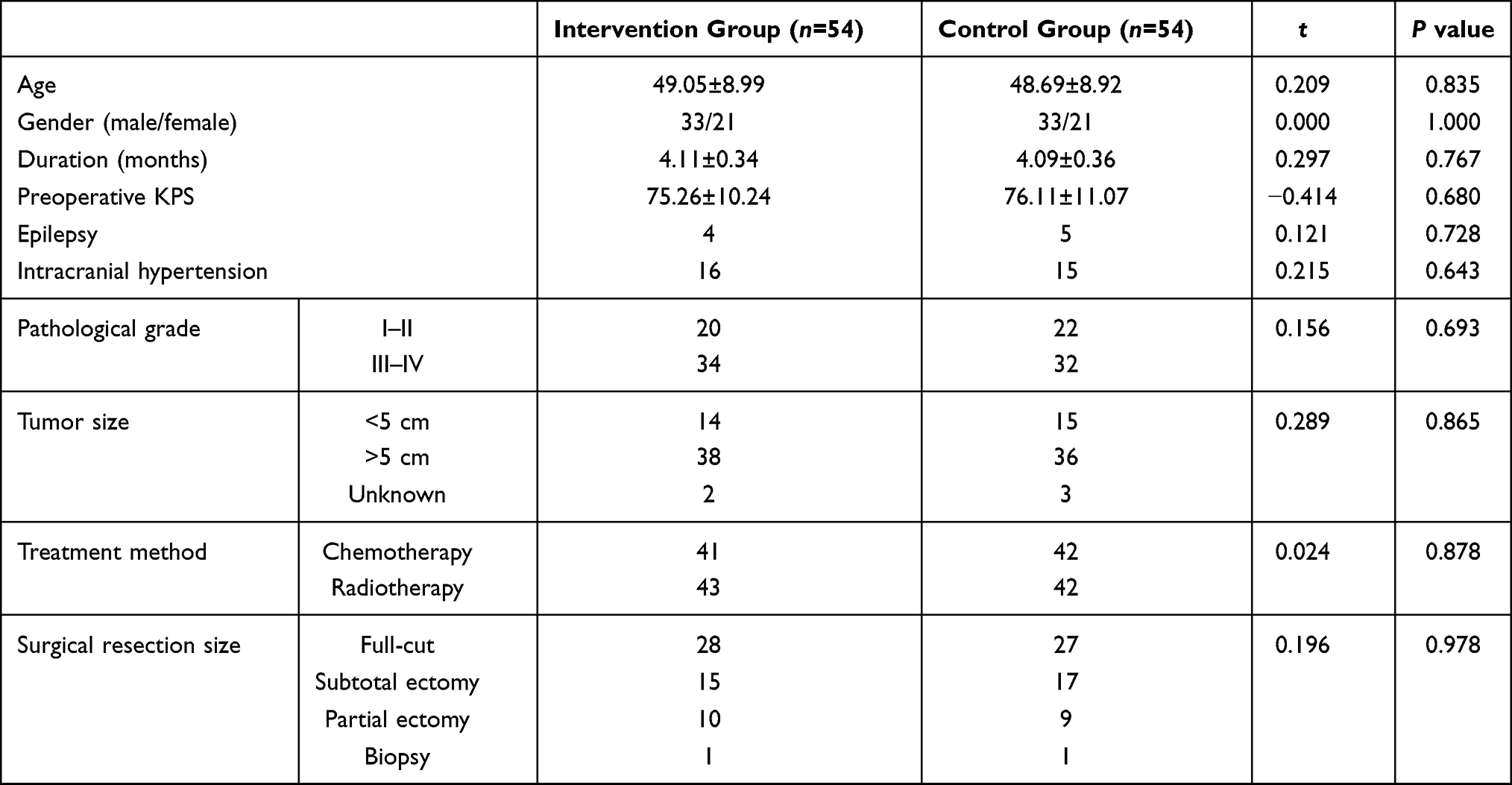 |
Table 1 The Comparison of General Information in Two Groups ( |

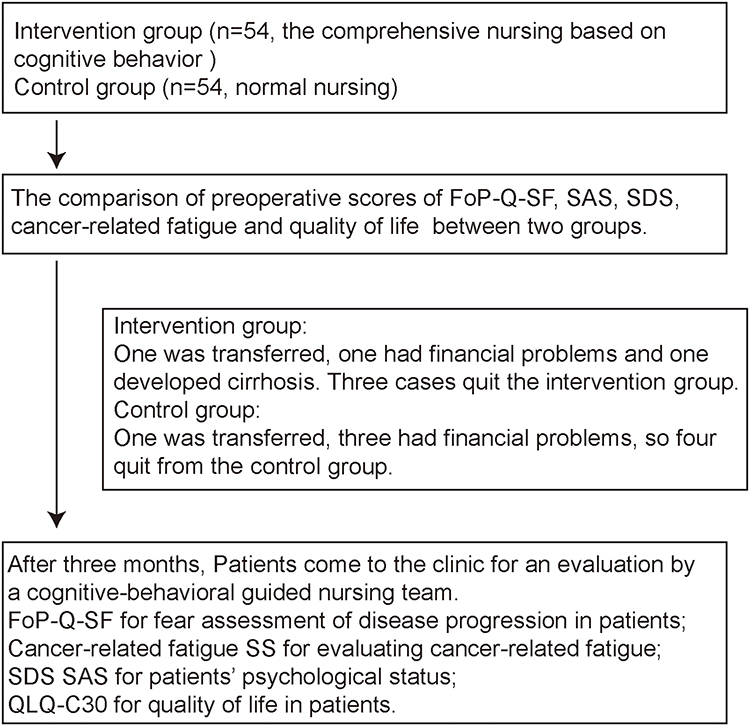 |
Figure 1 The flow chart of patient recruitment. Abbreviations: FoP-Q-SF, Fear of Progression Questionnaire-Short Form; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale; QLQ, questionnaire of quality of life. |
Comparison of FoP-Q-SF, SAS and SDS Scores Between the Two Groups Before and After Intervention
Before the intervention, there was no significant difference in FoP-Q-SF, SAS and SDS scores between the two groups. After the intervention, the scores of FoP-Q-SF, SAS and SDS in the intervention group were significantly lower than those in the control group (P < 0.05), as laid out in Table 2.
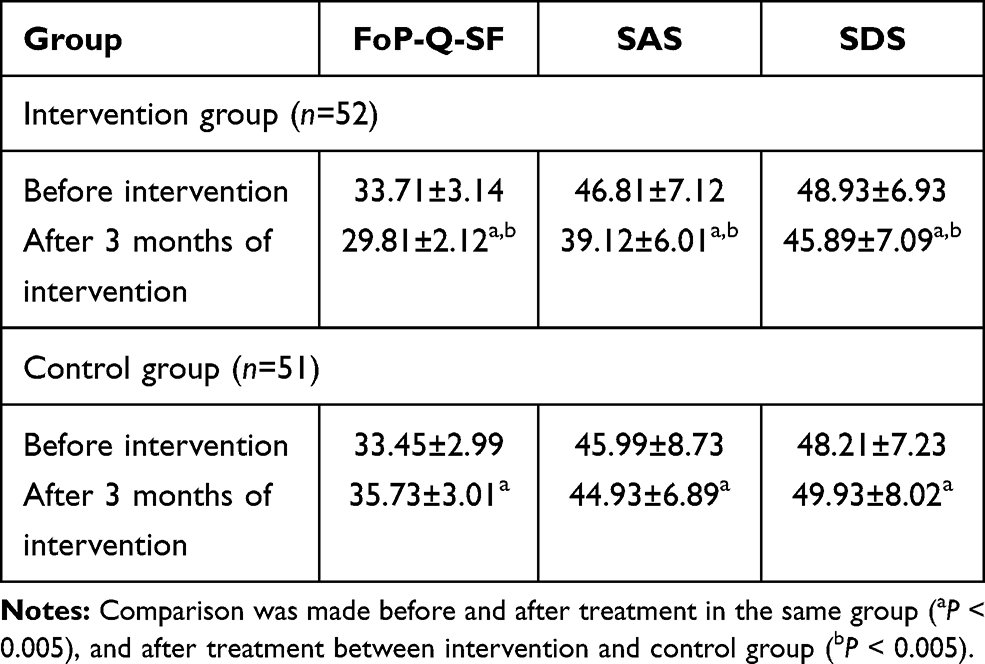 |
Table 2 Comparison of FoP-Q-SF, SAS and SDS Scores Between the Two Groups Before and After Treatment ( |

Comparison of Cancer-Related Fatigue Between the Two Groups Before and After Intervention
Before the intervention, there was no significant difference in the scores of cognition, emotion, perception and behavioral severity between the two groups (P > 0.05). After the intervention, the scores of cognition, emotion, perception and behavioral severity of cancer-related fatigue decreased in both groups, and the scores of the abovementioned five parameters in the intervention group were lower than those in the control group, with significant difference (P < 0.05). See Table 3.
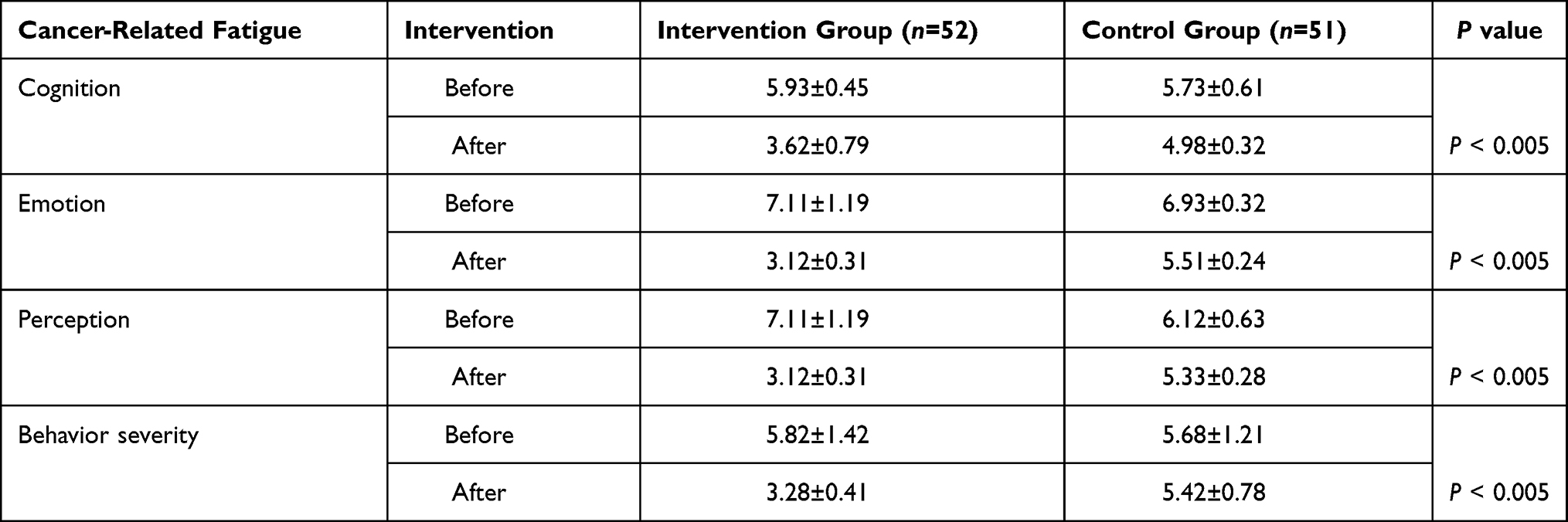 |
Table 3 Comparison of Cancer-Related Fatigue Between the Two Groups Before and After Treatment ( |

Comparison of Quality of Life Between the Two Groups Before and After Intervention
Before the intervention, there was no significant difference in the score of life quality between the two groups (P > 0.05). After the intervention, the scores of life quality in the intervention group were significantly higher than those in the control group (P < 0.05), as laid out in Table 4.
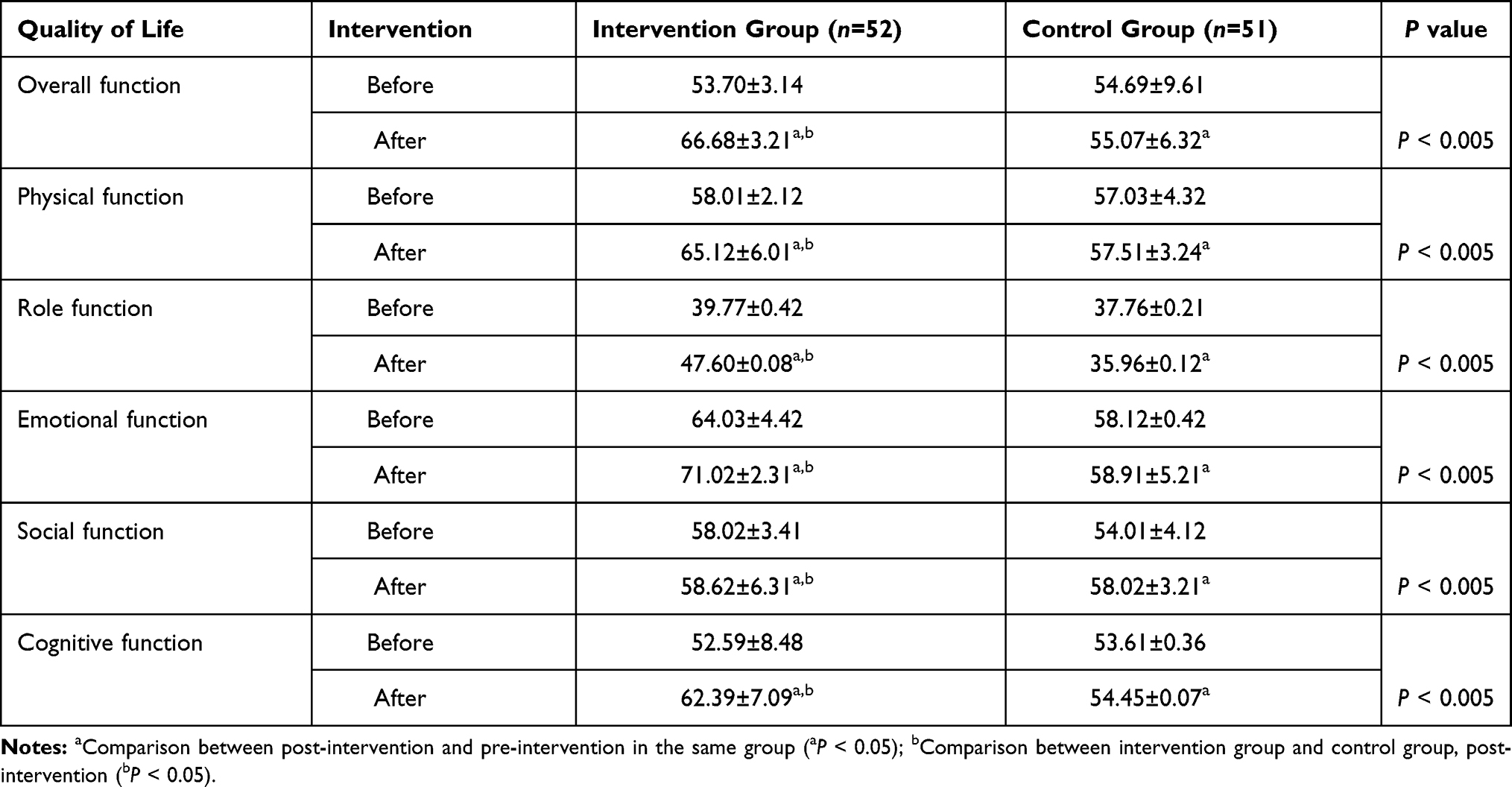 |
Table 4 Comparison of QLQ-C30 Scores Between the Two Groups Before and After Treatment ( |

Discussion
Our study confirmed that comprehensive nursing based on cognitive behavior can improve the psychological function of patients.11,12 Fear of disease progression is the patient’s fear of the progression of their disease. According to relevant research, more than 70% of patients with chronic diseases and cancer have moderate to high levels of fear of disease progression, accompanied by varying degrees of anxiety and depression. And the fear itself for disease progression is regarded as an important factor of stress affecting the physical and mental health of patients, especially for glioma patients who have been newly admitted to the hospital, unfamiliar with the new environment and uncertain of the effects of their disease. In addition to their physical pain, patients with advanced cancer also suffer from great psychological pain.13 The anxiety, depression, fear and other negative emotions tend to increase for patients. Furthermore, in the process of treatment, with little entertainment, the attention to their current disease and the attitude and emotions of family members also directly affect and lead to negative emotion of the patients, with increasing trend of progression of the disease. Through more than ten years of clinical experience, the author concludes that patients have different degrees of fear at different stages of the disease. Due to the limited time of doctors, patients are unable to consult their doctors each time they have questions about their condition. In addition, family members and nurses do not communicate negative information about the patient’s condition, indirectly leading to negative thoughts of patients for their disease progression, which is also bad for prognosis. In this study, the comprehensive nursing team based on cognitive behavior attended to the patients’ cognition of their disease by communicating with the patients in detail. The self-made health education manual and health knowledge lectures on gliomas were given to patients and their families to increase patients’ understanding of gliomas and their disease. Patients who recovered better were invited to talk to the other patients to alleviate other patients’ fear of disease. Moreover, patients were given correct guidance during follow-up to improve their understanding, build up their confidence to fight the disease and restore their self-confidence so that the patients can better integrate into the society. A Chinese study found that the satisfaction with supportive care for gastric cancer patients was not ideal, and personalized nursing plans should be developed to meet the needs of patients by evaluating their experience of symptoms and their fear of disease progression.14 A recent study15 confirmed that the outcome of treatment, communication between health care workers and patients, and supportive needs were proportional to the progress of fear diseases. According to the current study, the scores of FoP-Q-SF, SAS and SDS in the intervention group were lower than those in the control group, and the results were similar to those of Zhang et al,16 indicating that the application of cognitive behavior as the guide of comprehensive nursing in glioma patients could effectively reduce the fear of disease progression and alleviate the negative psychology such as anxiety and depression.
Comprehensive nursing based on cognitive behavior can alleviate cancer fatigue. Cancer-related fatigue is closely related to cancer or cancer treatment, resulting in a persistent feeling of tiredness for cancer patients which affects normal activity. Related clinical studies17 suggest that cancer-related fatigue can be associated with cancer patients for a long time, which has an impact on the normal life of patients on some level. The randomized controlled trial conducted by Han et al18 confirmed that effective nursing intervention could remarkably reduce cancer-related fatigue in patients with advanced cancer. The randomized controlled trial completed by Chen et al19 suggested that nursing intervention could effectively alleviate the fatigue degree of glioma patients. The results of this study suggest that, compared with the control group, glioma patients effectively reduced cancer-related fatigue after 3 months of comprehensive nursing based on cognitive behavior in the intervention group. The following reasons are associated with the results. On the one hand, comprehensive nursing based on cognitive behavior, carried out step by step from preoperative nursing to intraoperative nursing to postoperative nursing, and from the evaluation of cognition to cognitive reconstruction to cognitive behavior intervention in the process of patient nursing, improves the understanding of glioma for patients. Patients’ attention to the disease can be distracted because of the cultivation of interest. Light music also makes patients physically and mentally happy and comfortable, so as to alleviate the symptoms of fatigue. On the other hand, clinical studies20 have confirmed that aerobic exercise can effectively alleviate cancer-related fatigue in patients with significant effect. In this study, the comprehensive nursing group also established a specialized individual rehabilitation program for patients. On the basis of this program, patients can improve metabolism, increase the blood supply of important organs and improve the loss and functional status of the body, hence alleviate the cancer fatigue of patients.
Comprehensive nursing based on cognitive behavior can improve the life quality of patients. With the progress of modern medical technology, the concept of modern nursing has also changed, and the nursing level of nurses has been continuously improved. Comprehensive nursing with cognitive behavior is patient-centered, through cognitive and behavioral methods, to correct the patients’ bad cognition of the disease. A series of nursing measures, such as education, psychotherapy, intraoperative nursing, postoperative nursing, can be used in an attempt to provide comprehensive, systematic and scientific comprehensive nursing care for patients, so that patients can obtain high-quality and high-level diagnosis and treatment services. Tang found that positive psychological intervention could improve cancer patients’ mental health and quality of life.21 Moreover, Zhang’s study showed that effective nursing intervention could decrease the incidence of postoperative complications and improve the patients’ life activity ability and life quality.22 In this study, the intervention group mastered the knowledge related to glioma and changed the bad cognition of the disease from the comprehensive nursing based on cognitive behavior, as the team rebuilt the patients’ cognition of glioma and carried out targeted cognitive and behavioral intervention. In addition, the team increased the patients' glioma-related knowledge, so that patients could correctly understand and fight the disease. Professional psychological counseling and support from family members could be obtained for patients to deal with the bad emotion towards glioma and effectively improve the life quality. Moreover, the emotional support of family members and other patients enhanced the patients’ sense of social belonging and increased the patients’ self-confidence. The aggregated results showed that the scores of life quality in the intervention group were higher than those in the control group (P < 0.05), indicating that the comprehensive nursing based on cognitive behavior could effectively improve the life quality of the patients in the intervention group (P < 0.05). The present study also confirmed that cognitive behavior as the guide of comprehensive nursing can effectively alleviate negative emotions, improve cancer-related fatigue and improve the life quality of patients. However, there were still some limitations about this study: the sample size was not big enough; the comparison between grade I–II and III–IV tumors within each group to each other was not explored; other factors such as the tumor MRI, postoperative survival status of patients and degree of nerve injury should be considerations in future studies as to provide evidence for clinical practice.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of Linyi Central Hospital. Informed consent was obtained from all the study subjects before enrollment.
Consent for Publication
All authors are in agreement with the content of the manuscript.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Zhang X, Yang B, Shao D, et al. Longitudinal association of subjective prospective and retrospective memory and depression among patients with glioma. Eur J Oncol Nurs. 2019;42:1–6. doi:10.1016/j.ejon.2019.07.003
2. Yi S, Yang F, Jie C, Zhang G. A novel strategy to the formulation of carmustine and bioactive nanoparticles co-loaded PLGA biocomposite spheres for targeting drug delivery to glioma treatment and nursing care. Artif Cells Nanomed Biotechnol. 2019;47(1):3438–3447. doi:10.1080/21691401.2019.1652628
3. Philip J, Collins A, Staker J, Murphy M. I-CoPE: a pilot study of structured supportive care delivery to people with newly diagnosed high-grade glioma and their carers. Neurooncol Pract. 2019;6(1):61–70. doi:10.1093/nop/npy010
4. Miao N. The effect of cognitive behavioral intervention on the fear of disease progression and negative emotion in patients with glioma. Attend Pract Res. 2019;16(6):140–141.
5. Mehnert A, Herschbach P, Berg P, Henrich G, Koch U. [Fear of progression in breast cancer patients–validation of the short form of the Fear of Progression Questionnaire (FoP-Q-SF)]. Z Psychosom Med Psychother. 2006;52(3):274–288. doi:10.13109/zptm.2006.52.3.274.German.
6. Wu Q, Liu P. Reliability and validity of Chinese version of fear of progression questionnaire-short form for cancer patients. Chin J Nurs. 2015;50(12):1515–1519.
7. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
8. Wang X, Wang X, Ma H. Mental Health Rating Scale Manual. Vol. 12. Beijing: Chinese Mental Health Magazine; 1999.
9. Ji X, Liu Y. Effect of family nursing intervention on cancer-related fatigue and quality of life in postoperative chemotherapy patients with glioma. Chin J Clin Oncol Rehabil. 2018;25(5):589–591.
10. Feng N. Application effect of seamless seamless care mode in patients with glioma. Shanxi Med J. 2016;45(123–124).
11. Niu L, Liang Y, Niu M. Factors influencing fear of cancer recurrence in patients with breast cancer: evidence from a survey in Yancheng, China. J Obstet Gynaecol Res. 2019;45(7):1319–1327. doi:10.1111/jog.13978
12. Krebs J, Wasner S, Egloffstein S, et al. [Resilience, fear of progression and psychosocial distress in patients with breast cancer and gynecological tumors seeking a second opinion]. Psychother Psychosom Med Psychol. 2019;69(7):293–300. doi:10.1055/a-0668-1206.German.
13. Shim EJ, Shin YW, Oh DY, Hahm BJ. Increased fear of progression in cancer patients with recurrence. Gen Hosp Psychiatry. 2010;32(2):169–175. doi:10.1016/j.genhosppsych.2009.11.017
14. Chen Y, Yuan X, Peng J. Current situation and influencing factors of supportive care for gastric cancer patients. PLA Nurs J. 2020;404(2):54–57.
15. Huang X, Xia L, Lan F, Shao YW, Li W, Xia Y. Treatment of nivolumab results in hyperprogressive disease in a patient harboring EGFR Exon 20 insertion and MYC amplification. J Thorac Oncol. 2019;14(9):e189–e191. doi:10.1016/j.jtho.2019.04.009
16. Zhang Y, Wang Y, Zhao J, Meng Y, Han L, Yan D. Effects of cognitive behavioral intervention on fear of disease progression and negative emotion in patients with glioma. Chin J Mod Nurs. 2018;24(1):39–44.
17. Yan M. Investigation and analysis of cancer-related fatigue during chemotherapy in patients with malignant tumor. J Chin Practi Diagn Ther. 2018;32(6):123–125.
18. Han L, Li L, Si Z. Effect of palliative care on cancer-related weakness in patients with advanced cancer. Guangdong Med J. 2018;39(13):170–172.
19. Chen J, Xu G, Guo H, Zhang X. Effect of nursing intervention on life quality, anxiety, depression and fatigue in postoperative radiotherapy patients with glioma. J China Med Univ. 2016;45(12):1139–1142.
20. Wang X, Duan P, Mei S, Yang L. Critical appraisal of domestic intervention studies of aerobic exercise in cancer-related fatigue patients. J Nurs Adm. 2016;16(1):10–12.
21. Tang H, Xu H. Influence of positive psychological intervention based on Internet technology on mood state and life quality of breast cancer patients undergoing chemotherapy after surgery. China Med Herald. 2020;28.
22. Zhang Q, Wu L. Influence of 5A nursing intervention on postoperative complication rate, life activity ability and life quality score of lung cancer patients. Guizhou Med. 2020;44(2):325–327.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.