")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Effect of Community-Based Health Insurance on Healthcare-Seeking Behavior for Childhood Illnesses Among Rural Mothers in Aneded District, East Gojjam Zone, Amhara Region, Northwest Ethiopia
Authors Simieneh MM , Yitayal M , Gelagay AA
Received 22 December 2020
Accepted for publication 29 March 2021
Published 21 April 2021 Volume 2021:14 Pages 1659—1668
DOI https://doi.org/10.2147/RMHP.S298658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Muluye Molla Simieneh,1 Mezgebu Yitayal,2 Abebaw Addis Gelagay3
1Department of Public Health, College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 2Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Reproductive Health, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Mezgebu Yitayal
Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, P. O. Box 196, Gondar, Ethiopia
Tel +251 947 057683
Email [email protected]
Background: Community-based health insurance (CBHI) schemes have been implemented in developing countries to facilitate modern medical care access. However, studies conducted on the effect of CBHI on healthcare-seeking behavior (HSB) have been limited and revealed inconsistent results. Therefore, this study aimed to assess the effect of CBHI on mothers’ HSB for common under-five childhood illnesses.
Methods: A community-based comparative cross-sectional study was conducted among 410 rural mothers (205 insured and 205 non-insured), and a multistage random sampling technique was used to select the study participants. Binary logistic regression and propensity score matching were used to identify factors associated with the mothers’ HSB, and estimate the effect of CBHI on mothers’ HSB, respectively.
Results: The overall mother’s HSB for childhood illnesses was 48.8% (200/410). From those mothers who visited healthcare, 92.0% were married, 86.0% were unable to read and write, 94.5% were farmers, and 54.5% were from low wealth status, 58.50% had a family size of ≤ 5, 54.0% had children less than 24 months of age. Besides, 63.0% were members of CBHI, 37.0% perceived their child’s illness as severe, 78.0% made a shared decision to visit a health facility, and 67.5% lived within less than five Kms from the nearby health facilities. Being a member of CBHI, the child’s age, decision to visit a health facility, and perceived disease severity were predictors of HSB. The CBHI had a significant effect on the HSB for childhood illnesses with ATT of 28.7% (t = 3.959).
Conclusion: The overall mothers’ HSB for common childhood illnesses was low though the CBHI has a significant effect. CBHI should be strengthened to improve the mothers’ HSB. It is also crucial to strengthen awareness creation regarding joint decision-making and educate mothers to visit the health facilities regardless of children’s age and disease severity.
Keywords: effect, community-based health insurance, mothers, health-seeking behavior, childhood illnesses
Background
Reducing child mortality is a worldwide priority and global sustainable development goals (SDGs). It has been planned to end preventable deaths of newborns and children under five years of age by 2030.1 Inappropriate medical care within the informal sector is a concern in sub-Saharan Africa, where malaria, diarrheal diseases, and lower-respiratory infections constitute the primary burden of illnesses.2 They are commonly treated through unsupervised self-medication, which may lead to delays in accessing the formal health sector.3
Ethiopia has invested substantially in the health sector in the last decades. Despite this, the utilization of maternal and child care remains among the lowest in Sub-Saharan Africa.4 The gap between availability and utilization is driven by the availability and quality of care and direct and indirect costs. Ethiopia introduced the Community-Based Health Insurance (CBHI), aiming to improve modern healthcare service utilization.5
Globally, more than half of under-five age children deaths are due to preventable conditions.6 Appropriate mothers’ healthcare-seeking behavior (HSB) could prevent many child deaths.7 The 2011 Ethiopian Demographic Health Survey (EDHS) showed that most mothers did not seek care for childhood illnesses,5 which leads to a large number of child mortality.8–10
The World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) developed the strategy, Integrated Management of Childhood and Neonatal Illness (IMCNI), to improve HSB.11,12 Prompt diagnosis and appropriate treatment can prevent death and long-term illnesses. The demographic health survey and local studies revealed that only a small number of children with common, potentially life-threatening conditions received appropriate care.13–16 Even after adopting ICCM within the Health Extension Program, HSB for childhood illnesses has not significantly improved.17–19
Evidence shows that the age of a child,20,21 the gender of the child,22–25 mothers’ age,19,26 educational status of mothers8,27 and husband,23,28 occupations,29 and decision-making power within the household27 are factors that influence mothers’ HSB. Awareness and perception about the disease status,10,18,22 the severity of the diseases,22 type of disease,8 and mothers’ media exposure,23,27 the household’s income,20,22,23 distance from health facilities,13,18,24 waiting time in health facilities,27 and health insurance30 also influence the mothers’ HSB.
However, studies on the effect of CBHI on HSB show inconsistent results. Some studies report that seeking formal medical treatment for childhood illnesses among insured members is better than non-insured members.31 On the contrary, some studies report no difference between the insured and non-insured populations.32 Besides, the effect of CBHI has not been studied in the study area. Therefore, this study aimed to assess the effect of CBHI on HSB for under-five childhood illnesses and other associated factors among rural mothers.
Methods
Study Design and Setting
A community-based cross-sectional study was conducted among 410 rural mothers (205 insured and 205 non-insured) in Aneded district, East Gojjam zone of Amhara region, from February to March 2016. Aneded district is located 283 km away from Addis Ababa, Ethiopia’s capital city, and 305 kms from Bahir Dar city, the capital city of Amhara region, and 40 Kms from Debre Markos, the capital city of East Gojjam zone. The district’s total population was estimated to be 104,053 (50,991 males and 53,062 females), and the total number of under-five children was 12,351. The district has 19 rural and one urban kebeles (the lowest administrative units in the country), five health centers, 20 health posts, three private clinics, and two drug stores. The CBHI was introduced in the district as a pilot scheme in 2011. At the time of this study, 8507 (41%) households were members of the CBHI scheme.
Study Population and Sampling Procedures
The source population was all rural mothers living in the Aneded district with at least one under-five child. The study population was all mothers who had children under-five years of age with a history of illness like diarrhea, fever, and/or acute respiratory infection (ARI) three months preceding the survey. Mothers working in the formal sectors and who were seriously sick were excluded from the study.
The sample size was determined by using the two-population proportion formula and calculated using Open Epi software. The assumptions taken to determine the sample size were the proportion of mothers’ HSB who had media exposure (69%) and those with no media exposure (47.7%),23 1:1 ratio, design effect of 2, and 10% non-response rate. The final sample size was 410 mothers, ie, 205 from households with CBHI coverage and 205 from households with no CBHI coverage.
A multistage sampling technique was used. Among the 19 rural Kebeles in the district, five Kebeles (25% of the study area), namely Gudalem, Amberzura, Daget, Yewobie, and Nefasam were selected first using a simple random sampling technique (lottery method). A minimum of 50% of “Ketenas” (a smaller division of kebele) from the selected Kebeles was selected using a simple random sampling method. The sample size was proportionally allocated to each kebele by considering the total population in each kebele. Households were visited to assess the presence of under-five children who were sick within the past three months. Each household was visited until the sample size was reached.
Study Variables
Outcome variable: The outcome variable of the study was HSB. We categorized the HSB into Yes or No response: Yes, if mothers undertook any response for signs and symptoms of illnesses to reduce severity and complication after recognizing the child’s disease, and visited health facilities, private and/or public health facilities; and No, if otherwise.
Independent variables: Socio-demographic factors or predisposing factors (maternal age, educational status, occupation, marital status, previous use of service, sex of the child, age of the child); enabling factors (distance from the health facility, cost to transportation, insurance status, income, waiting time at health facility); need factors (awareness about the disease, media exposure, perceptions on the use of timely health care seeking); and the CBHI membership status were the independent variables of the study.
The study participants’ wealth status was assessed based on housing conditions and durable assets and categorized into poor and rich. The term “rich” was used to describe those in the fourth or fifth quintile, whereas the term “poor” was used to explain those in the first three quintiles. Perceived illness severity was categorized into “mild,” “moderate,” and “severe” based on the perception of the mothers regarding the sickness of their child.
Data Collection Tools and Procedures
A structured questionnaire was prepared by adapting from the Anderson model and reviewing relevant literature.33 The questionnaire was designed in English and translated to the local language, Amharic, by a professional language expert for simplicity of understanding on the part of respondents and then translated it back to English. Five data collectors, who completed 12th grade to collect data, and two nurses, who have a diploma for the supervision of the data collection process were selected. The one-day training was given to the data collectors and supervisors about the research’s whole purposes and procedures to ensure the data quality.
A pre-test was conducted on 5% of the sample in one of the district’s kebeles, which we did not include in the actual data collection, and modification was made, based on the pre-test findings, before the beginning of the actual data collection. We conducted the data collection process at each household level. The investigator and supervisors checked the accuracy of the data collection process each day, and if problems were encountered, they communicated them to data collectors for immediate action. The principal investigator supervised the overall activity of the data collection.
Data Analysis
The data were entered into Epi-Info™ 3.5.1 (Centers for Disease Control and Prevention, Atlanta, GA, USA), and transferred to SPSS 20 (SPSS Inc., Chicago, IL, USA) for binary logistic regression analysis and STATA 12 (StataCorp LP, College Station, TX, USA) for propensity score analysis. Descriptive statistics such as mean and standard deviation were used to describe the study participants’ socio-demographic and economic characteristics.
A binary logistic regression was run to see the association of HSB of mothers or caregivers for childhood illnesses with predisposing, enabling, and needs factors. Multivariable logistic regression was also run to control the confounding factors and get less biased estimates of the association between explanatory and HSB. A level of significance of p-value ≤0.2 in the bivariable logistic regression was used as a cut-off point to select candidate variables for the final model, the multivariable logistic regression model.
A propensity score analysis was run to determine the effect of the CBHI on the HSB of mothers or caregivers for childhood illnesses. A propensity score is a probability of being exposed to the intervention (in this case, being a member of CBHI) given a set of observed covariates, X. It was estimated using the logistic regression model. It constructs a statistical comparison group based on a model of the probability of participating in the treatment (CBHI), using observed characteristics. The nearest neighborhood matching was used in the analysis, which matches a given insured mother to non-insured members whose propensity score was closest to that of the treated subject or vice versa. The method could balance the insured and non-insured mothers so that a direct comparison would be possible for evaluating the effects of being the members of CBHI on the HSB. The insured mothers were matched based on this probability, or propensity score, to non-insured mothers. Then, the program’s average treatment effect (ATT) was calculated as the mean difference in outcomes across these two groups.
Results
Socio-Demographic and Economic Characteristics of the Study Participants
A total of 410 mothers or caregivers participated in this study. The study revealed that 57.8% of the respondents were in the age group of 25–34 years, with a mean age of 30.5 ± 6.3 years. Among study participants, 90% were married, 86.8% were illiterate, 96.1% of the mothers and 92.7% of their husbands were farmers, and 39.8% had a family size of ≥6 with the average number of family members 5.2. The study also revealed that 60% of the respondents were from low wealth status households, 84.4% had only one under-five child, and the mean age of children was 26.3 + 14.5 months (Table 1).
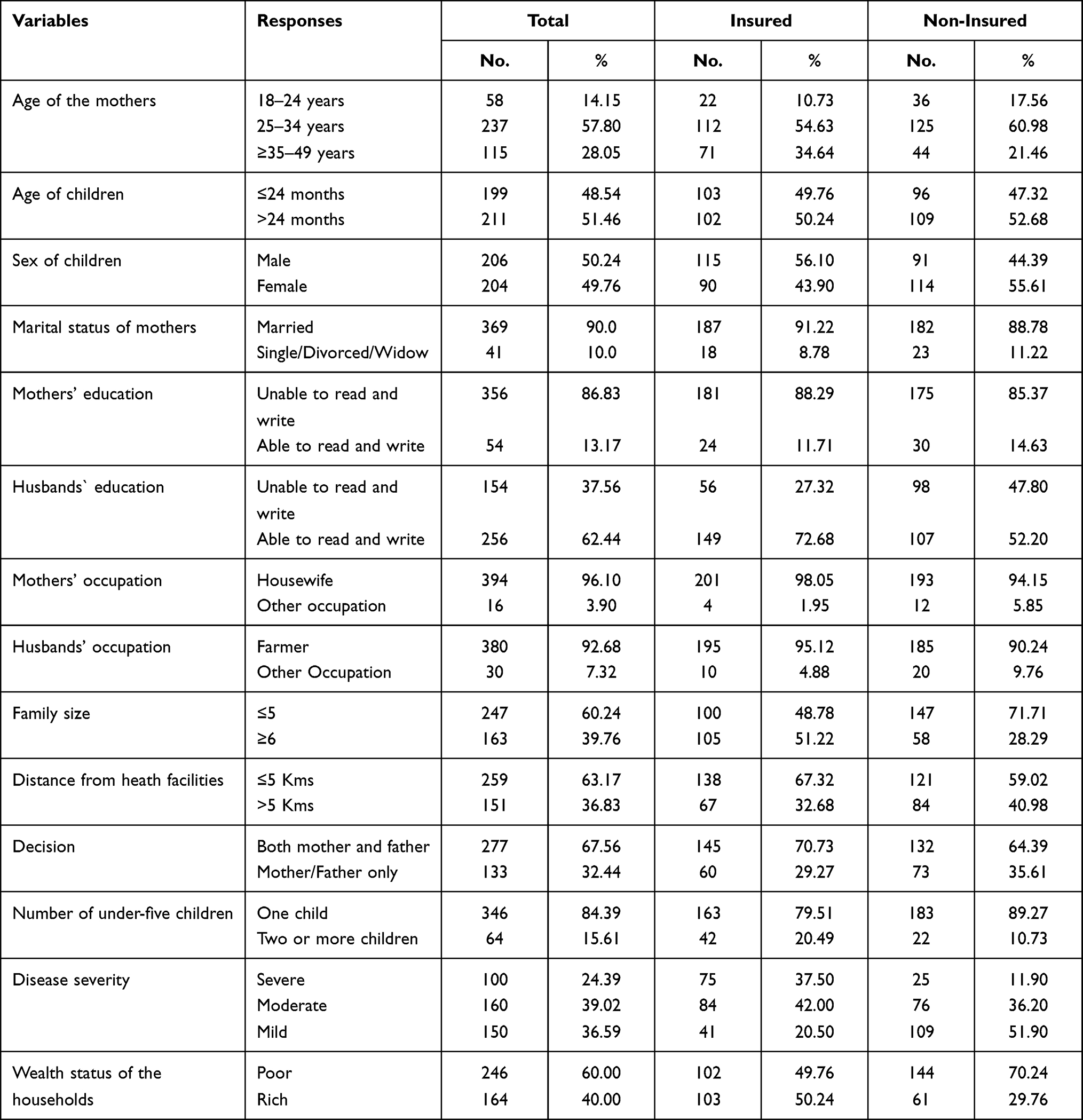 |
Table 1 Socio-Demographic and Economic Characteristics of Children and Mothers, and Health Facility-Related Factors in Aneded District, East Gojjam Zone, Amhara Region, Northwest Ethiopia, 2016 |
Healthcare-Seeking Behavior of the Study Participants
The study indicated that 200 (48.8%) of mothers visited health facilities during their child’s illness. From those mothers who visited health facilities, 184 (92.0%) were married, 172 (86.0%) were unable to read and write, 189 (94.5%) were farmers, and 109 (54.5%) were from low wealth status. Among those who sought healthcare, 117 (58.50) had a family size of ≤5, 171 (85.5%) had only one under-five child, and 108 (54.0%) had children less than 24 months of age. Besides, 135 (67.5%) lived within less than five Kms from the nearby health facilities, 74 (37.0%) perceived their child illness as severe, 156 (78.0%) made a shared decision, and 126 (63.00%) were members of CBHI (Table 2).
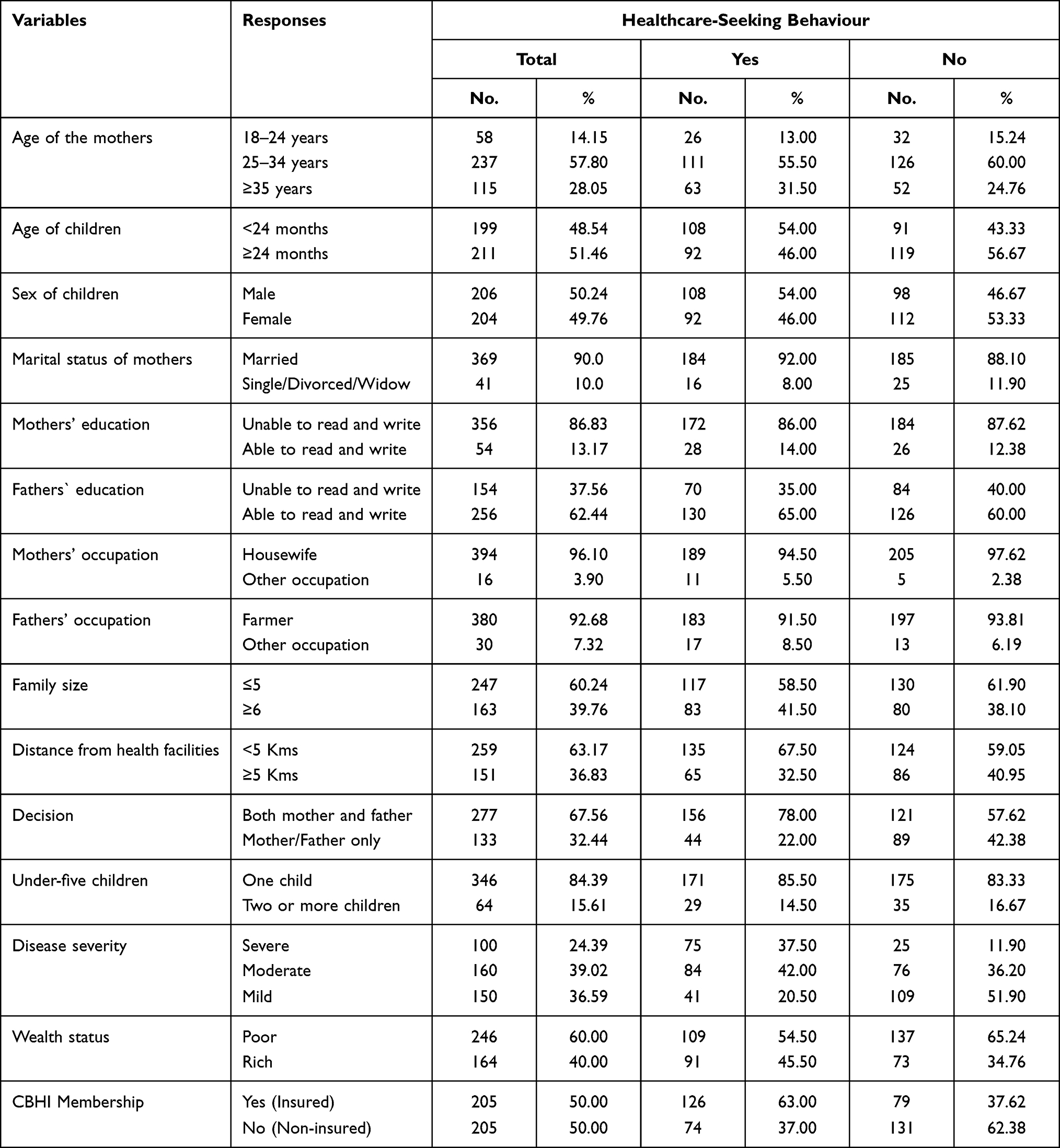 |
Table 2 Mothers’ Healthcare-Seeking Behavior for Childhood Illnesses in Aneded District, East Gojjam Zone, Amhara Region, Northwest Ethiopia, 2016 |
Factors Associated with Healthcare-Seeking Behavior of Mothers/Caregivers for Childhood Illnesses
The study indicated that the child’s age, decision-making to visit a health facility for childhood illnesses, disease severity, and CBHI membership had a statistically significant association with HSB.
Mothers who had children aged ≥24 months were 37% (AOR = 0.63; 95% CI: 0.40, 0.99) less likely to seek healthcare than those aged <24 months. Mothers who jointly decided with their husbands to visit a healthcare facility for their childhood illnesses were 2.71 (AOR = 2.71; 95% CI: 1.63, 4.51) times more likely to seek healthcare facilities than a decision made by either the mother or the father. Mothers who perceived their child illnesses were severe and moderate were 9.29 (AOR = 9.29; 95% CI: 4.95, 17.43) and 3.20 (AOR = 3.20; 95% CI: 1.90, 5.37) times more likely to seek health care, respectively, compared with mothers who perceived their child illnesses were mild. Mothers/caregivers who were members of the CBHI scheme were 3.20 (AOR = 3.20; 95%: 1.90, 5.37) times more likely to seek healthcare than mothers/caregivers who were non-members CBHI (Table 3).
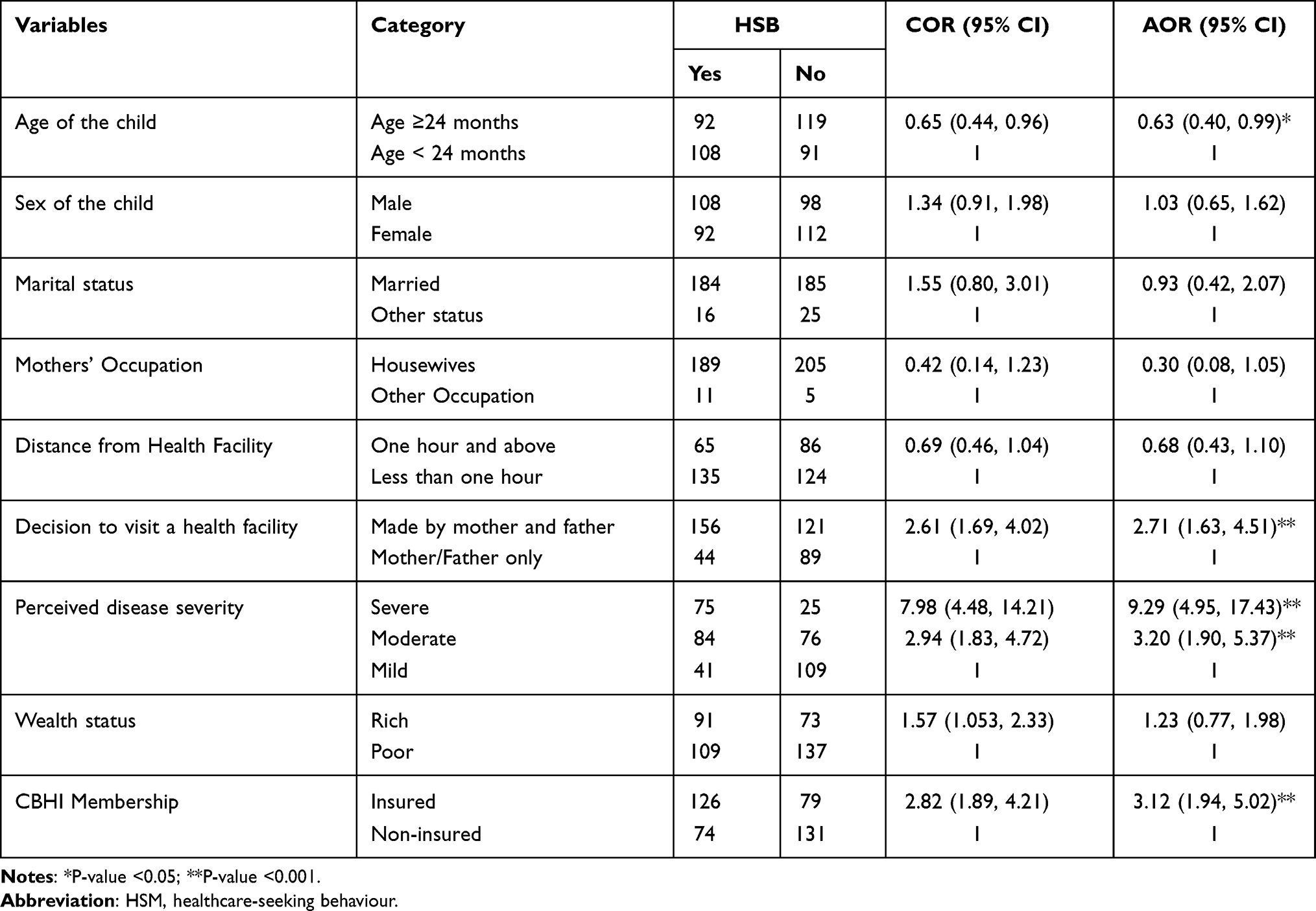 |
Table 3 Factors Associated with Mothers’ Healthcare-Seeking Behavior for Childhood Illnesses in Aneded District, East Gojjam Zone, Amhara Region, Northwest Ethiopia, 2016 |
Effect of CBHI on HSB of Mothers or Caregivers for Childhood Illnesses
Descriptive results of the study indicated that overall, 200 (48.78%) of mothers sought healthcare for their childhood illnesses, of which 126 (63.00%) were members of CBHI and 74 (37.00%) were non-members of CBHI. By statistically balancing 205 mothers from members of CBHI (insured group) and 203 mothers from non-members of CBHI (matched non-insured group) based on the propensity scores and all the variables used to construct it, the average treatment effect on treated (ATT) members of CBHI was found to be 0.287 points (t = 3.959) for appropriate HSB. This study indicated that being a member of the CBHI scheme contributed a 28.70% increase to HSB compared with non-members of the CBHI scheme using the Nearest Neighbor matching method at a 5% level of significance (Table 4).
 |
Table 4 Impact of CBHI (ATT) on Mothers’ Healthcare-Seeking Behavior for Childhood Illnesses in Aneded District, East Gojjam Zone, Amhara Region, Northwest Ethiopia, 2016 |
Discussion
This study revealed that the mothers’ HSB during their common childhood illness was low. This finding is in line with a study conducted in Yemen.10 However, this finding is higher than a study conducted in Ethiopia,14 Osun State, southwestern Nigeria,7 Chitwan, and Nepal;34 and lower than a study conducted in Sierra Leone.2 This difference might be due to the study participants’ socio-economic characteristics and the design and sample size of the studies.
The study showed that mothers who had children aged ≥24 months were less likely to seek appropriate health care than those aged <24 months. This finding is consistent with studies conducted in southwestern Nigeria,7 developing countries,8 Sub-Saharan Africa,20 and Pakistan.21
Mothers who perceived their child illnesses were severe and moderate were more likely to seek health care than mothers who perceived their child illnesses were mild, respectively. This finding is consistent with studies conducted in rural communities of Osun State, southwestern Nigeria,7 Yemen,10 and Chitwan, Nepal.34
Mothers who jointly decided with their husbands to visit a healthcare facility for their childhood illnesses were more likely to seek a healthcare facility than a decision made by either the mother or the father. This study is consistent with a survey conducted in Chitwan, Nepal, which states that HSB was higher among mothers involved in the household decision-making process.34 This finding is also consistent with a study conducted in Bangladesh, which reported that husbands’ involvement is of paramount importance in HSB, especially for maternal health services.35
This study revealed that mothers` CBHI membership was significantly associated with the HSB for childhood illnesses and significantly affected HSB during childhood illness with mean HSB difference between the insured and non-insured mothers (ATT). This result is consistent with a study conducted in Tanzania30 and Ghana.31 It is also compatible with the survey conducted in Vietnam that indicates insured patients are more likely to seek healthcare services in terms of outpatient facilities.32
However, the study indicated that the sex of the child; age, educational status, and occupational status of the mothers; distance from health facilities; and wealth status of the households were not significantly associated with the HSB for childhood illness. However, a study conducted in rural communities of Osun State, southwestern Nigeria, indicates that mothers age <35 years; employment status has a significant association with the HSB.7 This difference might be due to age and occupational status distribution, ie, in this study, nearly 89% of the mothers aged >35 years and 32.0% were farmers, whereas, in our study, 28.05% of mothers aged ≥35 years and 96.10% were farmers. A study conducted in Yemen indicates that seeking medical care is significantly associated with a higher level of schooling.10 The caretakers sought medical care significantly more when they had a higher level of school education. This difference could be justified by the proportion of study participants’ educational status as this study reported 27.36% no schooling/illiterate, whereas our research reported 86.83%. A study conducted reported that in Chitwan who had enough household income and health facility within 30 minutes distance were more likely to seek healthcare services.34
Limitations and Strengths
Recall bias may be a potential limitation for this study. Moreover, the propensity score matching could not control unobservable differences. This study used two models to check the effect of the program on HSB. The PSM model is strong enough to control all observable confounders, which leads to unbiased estimation to evaluate the effect of CBHI on HSB.
Conclusion
The overall mothers’ HSB for common childhood illnesses was low though the CBHI has a significant positive effect. Being a member of CBHI, the child’s age, decision-making process to visit a health facility for childhood illnesses, disease severity was positively associated with mothers’ HSB for common childhood illnesses. Hence, CBHI should be strengthened and promoted to improve the mothers’ HSB. It is also crucial to strengthen awareness creation programs regarding joint decision-making to visit health facilities and educate mothers to visit the health facilities for childhood illnesses regardless of their age and disease severity.
Abbreviations
HSB, Health Care Seeking Behaviour; SDGs, Sustainable Development Goals; ATT, Average Treatment of Treated; COR, Crude Odds Ratio; AOR, Adjusted odds ratio.
Data Sharing Statement
The datasets supporting the conclusions of this article are available at reasonable request to the corresponding author.
Ethical Approval and Consent to Participants
The study was conducted following the Declaration of Helsinki. Ethical clearance was obtained from the Ethical Review Committee of the Institute of Public Health, University of Gondar. Before communicating with study participants, a support letter was received from the Amhara Regional State Health Bureau, East Gojjam Zonal Health Department, and Aneded District Health Office. All the study participants were informed about the study’s purpose by reading the information sheet and the consent form. They were requested for verbal consent only as the investigation had minimal risk to the study participants. The Institute of Public Health Ethical Review Board, University of Gondar, approved the study’s protocol, including verbal consent. The confidentiality of the information and participants’ right to withdraw was ensured at any time of the data collection process.
Acknowledgments
We would like to thank the Institute of Public Health, University of Gondar, for the proper review and approval of this research paper. Our deepest gratitude goes to Amhara Regional Health Bureau for their supportive letter to do this research project. We would like to thank the study participants and the data collectors, and supervisors for their valuable cooperation during the data collection period.
Author Contributions
All authors contributed to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, interpretation, or in all these areas. They took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the manuscript has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This manuscript is part of a master thesis funded by Amhara National Regional State Health Bureau, Ethiopia. We presented the preliminary findings of the study at the Institute of Public Health, University of Gondar. The funders had no role in the study design, data collection, analysis, decision to publish, or manuscript preparation.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. UNICEF. Committing to child survival: a promise renewed. eSocialSciences; 2015.
2. Diaz T, George AS, Rao SR, et al. Healthcare seeking for diarrhoea, malaria and pneumonia among children in four poor rural districts in Sierra Leone in the context of free health care: results of a cross-sectional survey. BMC Public Health. 2013;13(1):157. doi:10.1186/1471-2458-13-157
3. Schoeps A, Lietz H, Sie A, et al. Health insurance and child mortality in rural Burkina Faso. Glob Health Action. 2015;8(1):27327. doi:10.3402/gha.v8.27327
4. Mebratie A, Van de Poel E, Debebe ZY, Abebaw D, Alemu G, Bedi AS. Self-reported health care seeking behavior in rural Ethiopia: evidence from clinical vignettes. ISS Work Paper Series Gen Series. 2013;551(551):1–30.
5. Mebratie AD, Sparrow R, Yilma Z, Abebaw D, Alemu G, Bedi A. Impact of Ethiopian pilot community-based health insurance scheme on healthcare utilisation: a household panel data analysis. Lancet. 2013;381:S92. doi:10.1016/S0140-6736(13)61346-X
6. World Health Organization. Millennium Development Goals (MDGs). Millennium Development Goals (MDGs); 2015 [updated 2018; cited 2020 December 18, 2020].
7. Adedire Elizabeth B, Asekun-Olarinmoye Esther O, Fawole O. Maternal perception and care-seeking patterns for childhood febrile illnesses in rural communities of Osun State, South-Western Nigeria. Science. 2014;2(6):636–643.
8. Geldsetzer P, Williams TC, Kirolos A, et al. The recognition of and care seeking behaviour for childhood illness in developing countries: a systematic review. PLoS One. 2014;9(4):e93427. doi:10.1371/journal.pone.0093427
9. Källander K, Hildenwall H, Waiswa P, Galiwango E, Peterson S, Pariyo G. Delayed care seeking for fatal pneumonia in children aged under five years in Uganda: a case-series study. Bull World Health Organ. 2008;86:332–338. doi:10.2471/BLT.07.049353
10. Webair HH, Bin-Gouth AS. Factors affecting health seeking behavior for common childhood illnesses in Yemen. Patient Prefer Adherence. 2013;7:1129. doi:10.2147/PPA.S51124
11. World Health Organization. Ending preventable child deaths from pneumonia and diarrhoea by 2025: the integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD); 2013
12. Kalyango JN, Alfven T, Peterson S, Mugenyi K, Karamagi C, Rutebemberwa E. Integrated community case management of malaria and pneumonia increases prompt and appropriate treatment for pneumonia symptoms in children under five years in Eastern Uganda. Malar J. 2013;12(1):340. doi:10.1186/1475-2875-12-340
13. Deressa W, Ali A, Berhane Y. Maternal responses to childhood febrile illnesses in an area of seasonal malaria transmission in rural Ethiopia. Acta Trop. 2007;102(1):1–9. doi:10.1016/j.actatropica.2007.02.009
14. Assefa T, Belachew T, Tegegn A, Deribew A. Mothers’health care seeking behavior for childhood illnesses in Derra District, North Shoa Zone, Oromia Regional State, Ethiopia. Ethiop J Health Sci. 2008;18(3).
15. Breiman RF, Olack B, Shultz A, et al. Healthcare-use for major infectious disease syndromes in an informal settlement in Nairobi, Kenya. J Health Popul Nutr. 2011;29(2):123. doi:10.3329/jhpn.v29i2.7854
16. Agency CS. Ethiopia demographic and health survey 2011. Addis Ababa, Ethiopia; 2012:452
17. The Last Ten Kilometers Project. Integrated Community Case Management (iCCM) Survey in Amhara, SNNP, and Tigray regions. Addis Ababa, Ethiopia: JSI Research & Training Institute, Inc.; 2013.
18. Sisay S, Endalew G, Hadgu G. Assessment of mothers/care givers health care seeking behavior for childhood illness in Rural Ensaro District, North Shoa Zone, Amhara Region, Ethiopia 2014. Glob J Life Sci Biol Res. 2015;1(1):15.
19. Awoke W. Prevalence of childhood illness and mothers‘/caregivers’ care seeking behavior in Bahir Dar, Ethiopia: a descriptive community based cross sectional study. Open J Prev Med. 2013;3(2):155–159. doi:10.4236/ojpm.2013.32020
20. Noordam AC, Carvajal-Velez L, Sharkey AB, Young M, Cals JW. Care seeking behaviour for children with suspected pneumonia in countries in sub-Saharan Africa with high pneumonia mortality. PLoS One. 2015;10(2):e0117919. doi:10.1371/journal.pone.0117919
21. Anwar-ul-Haq HMD, Kumar R, Durrani SM. Recognizing the danger signs and health seeking behaviour of mothers in childhood illness in Karachi, Pakistan. Univ J Public Health. 2015;3:49–54. doi:10.13189/ujph.2015.030201
22. Burton DC, Flannery B, Onyango B, et al. Healthcare-seeking behaviour for common infectious disease-related illnesses in rural Kenya: a community-based house-to-house survey. J Health Popul Nutr. 2011;29(1):61. doi:10.3329/jhpn.v29i1.7567
23. Chandwani H, Pandor J. Healthcare-Seeking behaviors of mothers regarding their children in a tribal community of Gujarat, India. Electron Physician. 2015;7(1):990. doi:10.14661/2015.990-997
24. Kassile T, Lokina R, Mujinja P, Mmbando BP. Determinants of delay in care seeking among children under five with fever in Dodoma region, central Tanzania: a cross-sectional study. Malar J. 2014;13(1):348. doi:10.1186/1475-2875-13-348
25. Nasrin D, Wu Y, Blackwelder WC, et al. Health care seeking for childhood diarrhea in developing countries: evidence from seven sites in Africa and Asia. Am J Trop Med Hyg. 2013;89(1_Suppl):3–12. doi:10.4269/ajtmh.12-0749
26. Ajibade B, Amoo P, Adeleke M, Oyadiran G, Kolade O, Olagunju R. Determinants of mothers health seeking behaviour for their children in a Nigerian teaching hospital. IOSR J Nurs Health Sci. 2013;1(6):09–16.
27. Amin R, Shah NM, Becker S. Socio-economic factors differentiating maternal and child health-seeking behavior in rural Bangladesh: a cross-sectional analysis. Int J Equity Health. 2010;9(1):9. doi:10.1186/1475-9276-9-9
28. Gelaw YA, Biks GA, Alene KA. Effect of residence on mothers’ health care seeking behavior for common childhood illness in Northwest Ethiopia: a community based comparative cross–sectional study. BMC Res Notes. 2014;7(1):705. doi:10.1186/1756-0500-7-705
29. World Health Organization. Children: reducing mortality; 2012 [updated September 8, 2020; cited 2020 December 18, 2020]. Available from: http://www.who.int/mediacentre/factsheets/fs178/en/index.html.
30. Chomi EN, Mujinja PG, Enemark U, Hansen K, Kiwara AD. Health care seeking behaviour and utilisation in a multiple health insurance system: does insurance affiliation matter? Int J Equity Health. 2014;13(1):25. doi:10.1186/1475-9276-13-25
31. Gajate-Garrido G, Ahiadeke C. The Effect of Insurance Enrollment on Maternal and Child Health Care Utilization: The Case of Ghana. Intl Food Policy Res Inst; 2015.
32. Robyn PJ, Hill A, Liu Y, et al. Econometric analysis to evaluate the effect of community-based health insurance on reducing informal self-care in Burkina Faso. Health Policy Plan. 2012;27(2):156–165. doi:10.1093/heapol/czr019
33. Andersen RM, Davidson PL, Ganz PA. Symbiotic relationships of quality of life, health services research and other health research. Qual Life Res. 1994;3(5):365–371. doi:10.1007/bf00451728
34. Sigdel D, Onta M, Bista AP. Factors affecting health seeking behaviors for common childhood illnesses among rural mothers in Chitwan. Int J Health Sci Res. 2018;8(11):177–184.
35. Storya WT, Burgard SA. Couples' reports of household decision-making and the utilization of maternal health services in Bangladesh. Soc Sci Med. 2012;75(12):2403–2411. doi:10.1016/j.socscimed.2012.09.017
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.