")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Effect of Cardiac Rehabilitation on Hope Among Cardiac Patients After Coronary Artery Bypass Graft Surgery
Authors Rakhshan M , Toufigh A, Dehghani-firouzabadi A , Yektatalab S
Received 22 May 2020
Accepted for publication 5 August 2020
Published 25 August 2020 Volume 2020:13 Pages 1319—1326
DOI https://doi.org/10.2147/RMHP.S262656
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Mahnaz Rakhshan,1 Afsoon Toufigh,2 Azimeh Dehghani-firouzabadi,3 Shahrzad Yektatalab1
1Nursing Department, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran; 2Student Research Commitee, Shiraz University of Medical Sciences, Shiraz, Iran; 3Medical School, Shiraz University of Medical Sciences, Shiraz, Iran
Correspondence: Mahnaz Rakhshan
Nursing Department, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz 71936-13119, Iran
Tel +98 36474254
Email [email protected]
Purpose: Following coronary artery bypass graft (CABG) surgery, some patients experience psycho-mental problems such as hopelessness. The Phase 2 cardiac rehabilitation (CR) program is an important element of the secondary prevention program in treating patients with cardiovascular disease (CVD). The present study aimed to determine the effect of the Phase 2 CR program on the level of hope in cardiac patients after CABG surgery.
Patients and Methods: A clinical trial was conducted from July 2017 to late January 2018 at the Heart Surgery Centre, Al-Zahra Hospital, Shiraz, Iran. The target population was patients who sought CR therapy after CABG surgery. A total of 104 cardiac patients were recruited and equally divided into control and intervention groups. The intervention group received 20 sessions of Phase 2 CR program combined with education and counselling during 8 weeks. The control group only received routine observations and education. The data were collected pre- and post-intervention using a demographic form and the Miller Hope Scale (MHS). Descriptive statistics were expressed as percentages, frequency distribution, mean and standard deviation. Paired t-test and independent t-test were used for statistical inference. Data were analyzed using the SPSS statistical software (version 23.0) and P values < 0.05 were considered statistically significant.
Results: There was no significant difference in the mean score of hope between the control and intervention groups before the intervention. However, a significant difference between the groups was observed post-intervention (P< 0.001). The results showed a significant difference in the mean score of hope between pre-intervention (182.36± 23.07) and post-intervention (216.94± 23.05) in the intervention group (P< 0.001), whereas the difference in the control group was not significant (P=0.095). The measured post-intervention effect size was high (1.05).
Conclusion: The Phase 2 CR program combined with education and counseling increased hope in CVD patients after CABG surgery.
Keywords: cardiac rehabilitation, CABG surgery, hope, nursing intervention
Introduction
Cardiovascular diseases (CVDs) are recognized as a major health problem, highly prevalent, and the leading cause of death in the world.1 The disease may cause physical disability and put a huge financial burden on the affected patients and the national healthcare system.2 The statistics on ischemic heart disease are staggeringly high; mainly contributed to reduced mobility, low levels of physical activity, smoking, stress, and unsuitable diets.3 Currently, 6.4% of the total population in the United States are suffering from coronary artery disease (CAD) and it is projected to rise to 18% by 2030. The number of coronary artery bypass graft (CABG) surgeries in the United States is reported to be as high as 397,000 annually.4 In Iran, about 50,000 heart surgeries are performed every year, and CVDs account for 33–38% of mortalities and 23% of disabilities.5
Among the recommended treatments for patients with CAD, CABG surgery is the most invasive and expensive option, but it is the only treatment for cardiac patients. The main advantages of CABG surgery over other treatment modalities are enhanced abdominal efficiency, reduced pain and disability, and better quality of life (QoL) by alleviating angina symptoms and prolonging life.6 However, CABG surgery causes certain physical complications (issues related to the heart, lung, and neurology; inflammation and infection; kidney failure; bleeding) and psycho-mental problems (depression, anxiety, etc.).6,7 Hope can counter psycho-mental pressures in patients with open-heart surgery and plays an important role in the recovery of patients with CVDs. Researchers consider hope to be one of the most important contributing factors in enhancing the physical health of such patients.8 A previous study reported that hope could improve patients’ life satisfaction, personal growth, self-confidence, optimism, and resilience.9 To date, there are only a few studies that partially investigated the effect of hope in patients with CAD.10,11 Considering the high prevalence of the disease and the increasing number of CABG surgeries, there was a need to evaluate intervention methods that counter both the physical complications and psycho-mental side effects of the surgery. Research studies have shown that regular physical activity plays a significant role in the primary and secondary prevention of CVDs. Moreover, after myocardial infarction, people who changed their lifestyle in a radical way and exercised regularly had a better QoL and increased life expectancy.12,13
In CVD patients, Phase 2 CR is an important component of the secondary prevention program as it puts emphasis on physical activity and exercise.14 Based on the American Association of Cardiovascular and Pulmonary Rehabilitation and the American College of Sports Medicine guidelines, the Phase 2 CR program is mainly in the form of aerobics.15,16 It involves some standard curative exercises aiming at strengthening the muscles and improving the aerobic capacity of such patients.17 A previous study reported that the application of a CR program with a specific focus on phase 2 would improve patients’ exercise capacity and QoL, and significantly reduces mortality rate.14 The benefits of CR have been demonstrated in patients with various cardiac diseases such as post-myocardial infarction (MI), coronary artery bypass surgery, heart valve repair, percutaneous coronary interventions, stable angina, stable chronic heart failure, heart transplantation, cardiac arrhythmias, and severe arterial hypertension.18
Despite the importance of promoting hope in patients after open-heart surgery, only a few studies have investigated the effect of hope in patients with CAD. Hence, the aim of the present study to investigate the effect of the Phase 2 CR program on the level of hope in patients with CVD after CABG surgery. The outcome of our investigation would contribute to a better implementation of the Phase 2 CR program.
Patients and Methods
The present clinical trial study was conducted from July 2017 to late January 2018 at the Heart Surgery Centre, Al-Zahra Hospital, Shiraz, Iran. The target population was patients who underwent CABG surgery and were subsequently referred to Al-Zahra Heart Hospital (Shiraz, Iran) for a CR treatment program. The hospital is one of the main specialty heart clinics in the Southern Iran.
The patients were recruited in accordance with the inclusion criteria and randomly allocated to a control and an intervention group. The staff at the CR clinic (individuals other than those involved with the study) allocated patients into two groups with the same number of participants using the double-blind procedure. To ensure full participation of the patients, the education and counseling sessions were initially discussed with each of them and subsequently tailored according to their specific needs and conditions. In addition, the patients were assured full insight into their individual performances and the final study findings. Nonetheless, measures were taken to replace a patient in case of possible withdrawal.
The sample size was determined in accordance with a previous study using the G*Power software.19,20 Initially, a sample size of 48 patients per group was estimated (power>0.80, α=0.05). However, considering the probability of loss to follow-up, four additional patients per group were recruited. At the end of the selection process, 104 cardiac patients (n=52 per group) were recruited. The inclusion criteria were at least 4 weeks post-CABG surgery and willingness to participate. The exclusion criteria were cardiac complications, systemic diseases, and absent from more than two educational sessions. CONSORT flow diagram of the participants from enrollment to analysis is shown in Figure 1.
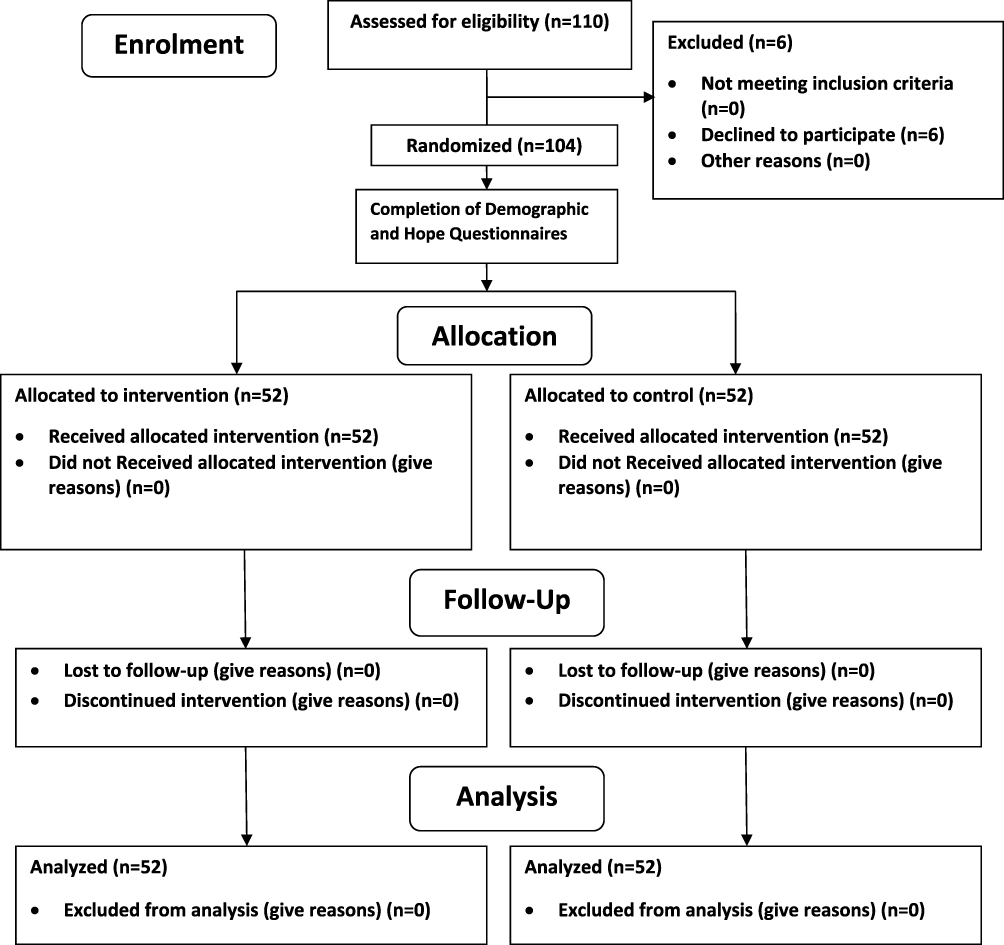 |
Figure 1 CONSORT Flow Diagram. |
Intervention
At the start, a member of the research team introduced herself to the patients and presented them with the study approval letter from the Ethics Committee of Shiraz University of Medical Sciences. The goals of the study and relevant information about the forms were described. Then, those willing to participate in the study were requested to sign an informed consent form and fill in the Miller Hope Scale (MHS) as well as a demographic information form. The participants were then equally divided into control and intervention groups. The participants in the intervention group followed 20 sessions of a CR program with specific focus on phase 2 combined with education and counseling. The latter included informative items on CAD, heart risk factors, CAD treatments, diet and weight control, relaxation techniques, self-motivation, skills involved in developing hope, and stress management techniques. The CR sessions were conducted over 8 weeks (2–3 sessions per week) and each session lasted about 60 minutes. Sessions 1–6 included education, counseling, and information related to Phase 2 CR exercises. The remaining sessions7–20 focused on the actual physical activities related to the Phase 2 CR exercises. Each exercise session consisted of three stages, namely warm-up (repeated controlled movements targeting the specific range of motion around the major joints), ergometric treadmill exercises (training the upper- and lower-limbs), and cool-down period (returning the heart and breathing rates back to normal). Depending on the tolerance of each participant, the total activity (duration, speed, and intensity) was increased by 5–7%.
Upon completion of the 20 sessions, both the control and intervention groups completed the MHS form again. Note that the control group only received routine education and did not follow any CR sessions. However, at the end of the study, they were provided with an informative booklet on CR and phase 2exercises.
Data Collection Instruments
The data were collected using a demographic form and the MHS. The demographic information was defined in accordance with a previous study21 and based on the recommendation of CR specialists and two nurses familiar with CVDs and psycho-mental problems. The demographic characteristics included age, sex, education level, and occupation.
Miller Hope Scale (MHS)
The scale was developed by Miller and Powers in 1988 to measure hope in adults. The MHS has no subscales and thus the scores of all items are added to calculate the total score; ranging from 48 to 240. Higher scores indicate a higher level of hope.22 The validity and reliability of MHS have been confirmed by its developers and by various other studies.23–26 Miller and Powers confirmed the convergent validity of the MHS by calculating the correlation of each item with the Symptom Hope Scale in adults. The reported correlation between these two tools was 89%, indicating a high level of validity. The reliability was reported by a Cronbach’s alpha of 88%-89%.22 An Iranian study by Ahmarian et al, in 2015, also reported the validity and reliability of MHS as 0.93 and 0.71, respectively, and the Cronbach’s alpha coefficient was 0.9.27
Data Analysis
The data were analyzed using SPSS statistical software (version 23.0). Descriptive statistics were used to examine the characteristics of the patients. Qualitative and quantitative variables were analyzed using the Chi-square test and independent t-test, respectively. The independent t-test was used to compare the mean scores between the two groups and the paired t-test was used to compare the mean scores of pre- and post-interventions in each group. P values <0.05 were considered statistically significant.
Results
The participants in the present study (n=104) included 79 men and 25 women, with an average age of 58.18±8.71 years. Among the hazardous risk factors, high blood pressure was prominent in both the intervention (n=28, 53.8%) and the control group (n=31, 59.6%). In terms of cardiac risk factors, only diabetes showed a significant difference between groups (P=0.008) (Table 1). To investigate the effect of diabetes on the patients’ hope score, normal distribution of the scores was examined separately in each group. Since the data were not distributed normally, the Mann–Whitney test was used to compare the scores between the groups.
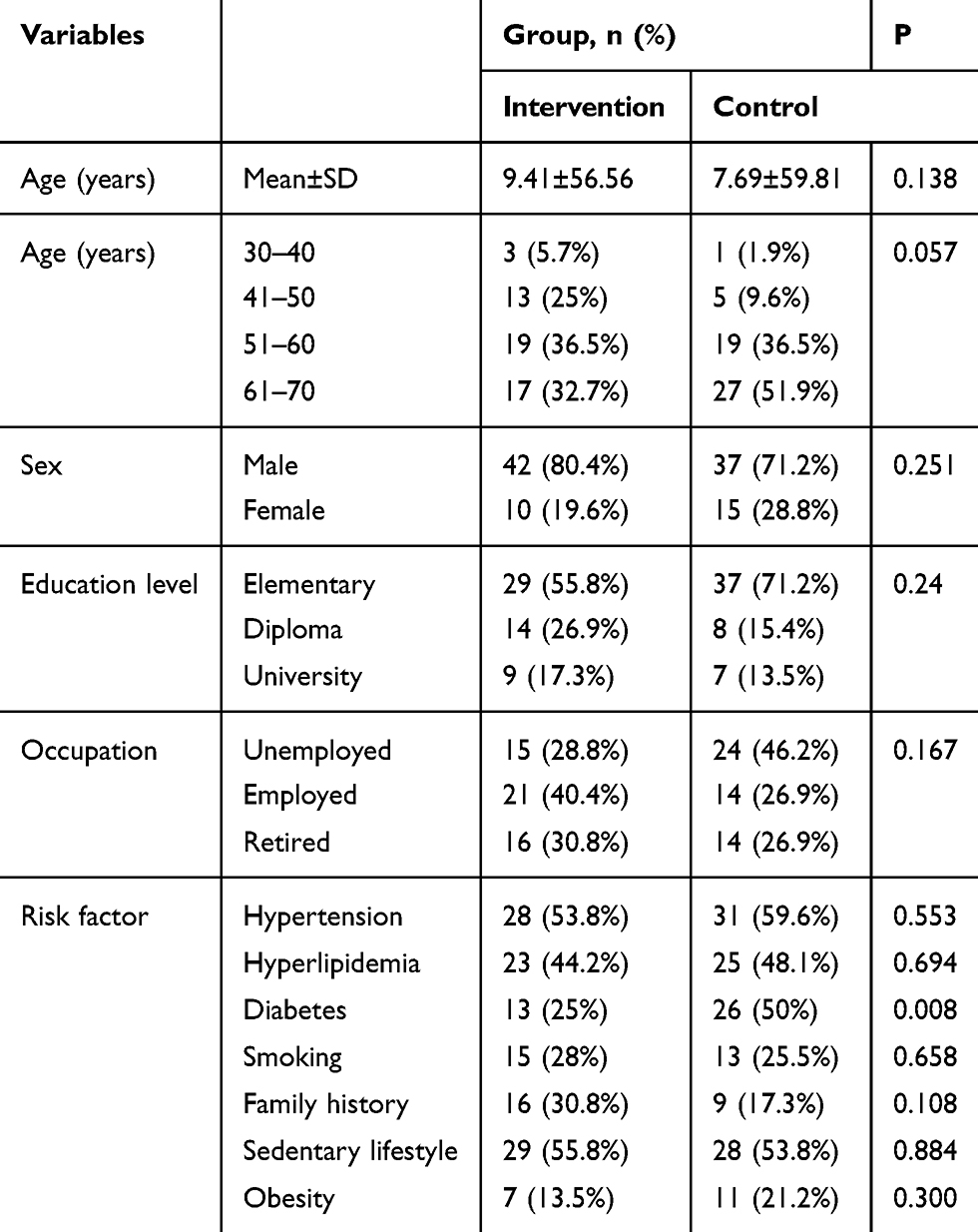 |
Table 1 Demographic Characteristics of the Patients in the Intervention and Control Groups |
As shown in Table 2, there was no significant difference in the mean score of hope in both groups before the intervention. However, the difference in the mean score of hope between pre-intervention (182.36±23.07) and post-intervention (216.94±23.05) was significant in the intervention group (P<0.001). In the control group, the difference between pre-intervention (187.03±21.26) and post-intervention (192.09±30.24) was not significant (P=0.095).
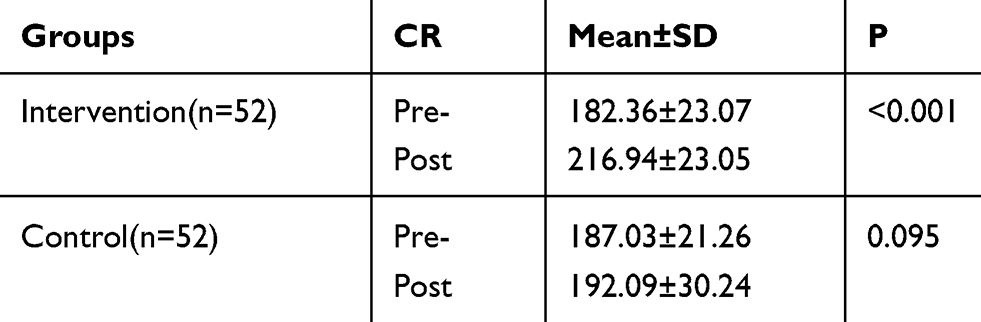 |
Table 2 The Difference in the Mean Pre- and Post-Intervention Scores for Hope in the Intervention and Control Groups |
The results showed that there was no significant difference between the mean total score of hope in pre- and post-intervention with respect to demographic variables such as age, sex, education level, and occupational status in the intervention group (P>0.05) (Table 3).
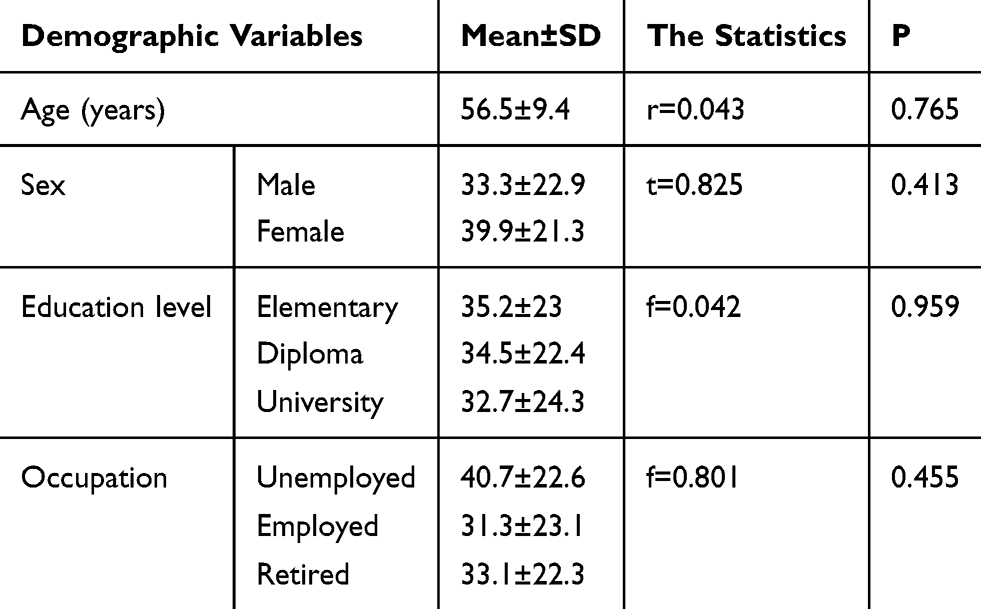 |
Table 3 Determination of the Difference Between the Mean Total Score for Hope Pre- and Post-Intervention in Terms of Demographic Variables (Age, Sex, Level of Education, and Occupational Status) in the Intervention Group |
In the pre-intervention stage, the measured effect size for hope in the intervention and control groups was 1.49 and 0.22, respectively. However, post-intervention, the effect size was high (1.05) in both groups (Table 4).
 |
Table 4 Effect Size for Hope Pre- and Post-Intervention in the Intervention and Control Groups |
The pre-intervention left ventricular ejection fraction (LVEF) level in the intervention and control groups was 50.19±5.50 and 51.53±6.06, respectively. However, 8 weeks post-CABG, a significant improvement in LVEF was observed in both the control (52.21±5.97) and intervention (51.25±4.63) groups (P<0.05) (Table 5).
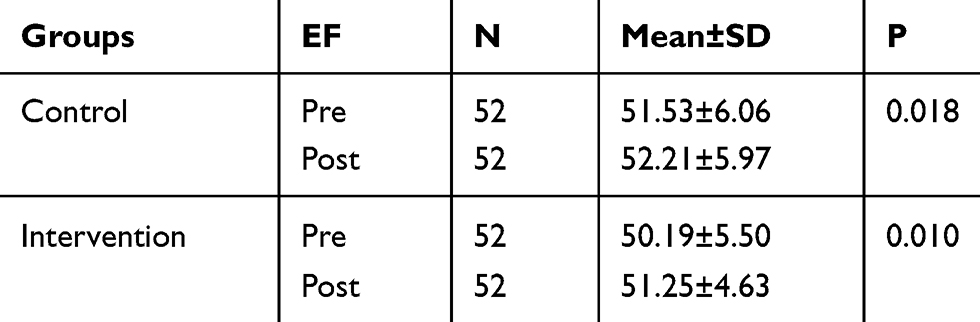 |
Table 5 Determination of the Difference Between the Mean Total EF Pre- and Post-Intervention in the Intervention and Control Groups |
Discussion
In a clinical trial study, we investigated the effect of the Phase 2 CR program in cardiac patients after CABG surgery using the MHS. Overall, the results showed that the hope score had significantly increased after 20 sessions of Phase 2 CR.
A previous study by Komlesh et al (2018) investigated the effect of a CR program on QoL and physiological parameters after CABG surgery.28 They reported that the QoL of their patients improved after the CR program. In relation to our study, one could consider hope and QoL to be interrelated variables. Participation of male patients (66%) and the average age of the patients (60±8.3 years) in their study were similar to ours. However, they conducted 8 sessions of CR program combined with education, whereas we performed 20 sessions of CR program combined with education and counseling. Another study by Dallier et al (2013) investigated the effect of a short duration CR program on depression and anxiety in cardiac patients after CABG surgery.29 They reported that depression and anxiety decreased after the CR program. Again, we consider depression and anxiety to have a direct inverse relationship with hope. In line with our study, their participants were mainly men (70%), the average age was 58.8±9.07 years, and they mostly had an elementary education (29%). The main difference between the studies was the number of sessions; 8 sessions of CR program and education versus our 20 sessions of CR program combined with education and counseling.
A previous study conducted in Iran by Sharif et al (2012) investigated the effect of a CR program on depression in cardiac patients after CABG surgery.30 Although they did not specifically address hope in their study, they stated that a decrease in depression after the CR program was associated with the level of hope in their patients. Note that Sharif et al conducted 8 sessions of CR program combined with education, which was less than ours and without counseling sessions. Kalka et al (2007) also investigated the effect of a CR program on QoL, depression, and anxiety in patients with heart failure.31 Similar to our study, they conducted 20 sessions of CR program with education (without counseling) in which the majority of the participants were men (72%), had an elementary education (44%), and the average age was 59±10.7 years. They showed a reduction in depression and anxiety and improvement in QoL of their patients after the CR program. Note that they did not specifically address the effect of the program on the level of hope in their patients. A previous study conducted in the United States by Beckie et al (2015) investigated biopsychosocial health disparities among young women enrolled in a CR program.32 They reported that variables such as health perception, QoL, optimism, hope, social support, and stress were significantly worse in young women compared to older women. Also, the symptoms of depression and anxiety were significantly greater in young women. Furthermore, in comparison with those who completed the CR program, the participants who withdrew prematurely tended to be younger women, more obese, worse QoL, and greater symptoms of depression and anxiety. In a randomized clinical trial, Beckie et al (2010) also investigated the effects of a dedicated CR program on the global QoL.33 They reported that the CR program, which was specifically tailored for women, significantly improved the global QOL compared to traditional CR. It is recommended to conduct further studies to explore the mechanisms by which such programs affect QoL.
A previous study conducted by Salami et al (2017) investigated the effect of spiritual self-care group therapy on life expectancy in Iranian patients with CAD.34 In line with our study, they showed that a CR program increased the level of life expectancy. The reported mean life expectancy a week after the intervention was significantly higher in the intervention group (176.76±43.38) compared to the control group (159.50±41.87) (P=0.035). They also reported the mean score of life expectancy (post-intervention) had significantly increased in the intervention group compared to pre-intervention (mean difference of 13.35±14.07, P<0.001). Similar to our study, their participants were mainly male patients (63%) and had an undergraduate degree (67%). However, they only conducted three sessions of intervention with training compared to our 20 sessions.
Among the few studies that have investigated the effect of hope, Don et al (2011) studied the effect of a Phase 2 CR program on reducing hopelessness in CAD patients at home and in hospitals.35 In line with our findings, they reported a significant hopelessness reduction in their patients. Similar to our study, most of their participants were men (67%) and unemployed (67.3%). However, their intervention period was almost 12 weeks compared to our 20 sessions in 8 weeks.
Overall, the intervention period in the present study was longer compared to the above-mentioned studies. In addition, we specifically focused on the Phase 2 CR program combined with education and counseling. As a direct result, our CR program significantly improved the level of hope in cardiac patients after CABG surgery.
Research Limitations
The main limitations of the present study were the selection of patients from a single center and the limited time to perform the intervention. It is recommended that future studies include the participation of a wide range of health centers across different cities and extend the duration of the CR program beyond 8 weeks. Some variables such as blood pressure, blood lipids, and diabetes were measured only before the intervention. It is recommended to further enrich the data by measuring and comparing these variables in both pre- and post-intervention stages.
Conclusion
The Phase 2 CR program increased the level of hope in cardiac patients after CABG surgery. Considering the high prevalence of CVD in Iran and the key role nurses play in health promotion, more emphasis should be put on performing the Phase 2 CR program. The findings of the present study can be used to better design CR programs and improve health care for open-heart surgery patients.
Data Sharing Statement
The data that support the findings of this study are available on reasonable request from the corresponding author, [Mahnaz Rakhshan]. The data are not publicly available due to the privacy of research participants.
Ethical Considerations
The study was approved by the Ethics Committee of Shiraz University of Medical Sciences, Shiraz, Iran (number: IR.SUMS.REC.1395.204), and registered at the Iranian Registry of Clinical Trials (code: IRCT 2017041633344N2). This trial was conducted in accordance with the Declaration of Helsinki.
The participants of the present study were personally informed about the goals of the research, methodology, and confidentiality of any disclosed information. In addition, sharing of deidentified individual participant data was guaranteed and voluntary participation was assured. Written informed consent was obtained from all participants.
Acknowledgment
The present manuscript was part of the Master’s degree thesis of the second author. The study was financially supported by the Research Vice-Chancellor of Shiraz University of Medical Sciences. The authors would like to thank the patients and all those who collaborated in the study for their time and effort.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Correa-Rodríguez M, Abu Ejheisheh M, Suleiman-Martos N, et al. Prevalence of Depression in Coronary Artery Bypass Surgery: A Systematic Review and Meta-Analysis. jcm. 2020;1–25.
2. Schwartz J, Zipes D. Cardiovascular Disease in the Elderly. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine.
3. Gamissi J, Masoumi M, Hossinian A. Spatio-temporal distribution of coronary heart disease by geographic information system arc gis in ardabil province. J Ardabil Univ Med Sci. 2017;17(2):174–188.
4. Efird J, O’Neal W, Griffin W, et al. Increased coronary artery disease severity in black women undergoing coronary bypass surgery. Medicine. 2015;94(7):1–7. doi:10.1097/MD.0000000000000552
5. Darvish N, Ostovan M, Askarian M. Adherence to practice guidelines for coronary artery bypass graft surgery in Shiraz, Iran. ARYA Atheroscler. 2015;6(11):370–373.
6. Aranki SM, Aroesty J. Coronary artery bypass graft surgery: long-term clinical outcomes; 2016. Available from: https://www.uptodate.com/contents/coronary-artery-bypass-graft-surgery-causes-and-rates-of-graft-failure.
7. Woods S, Sivarajan E, Adams S, Bridges E. Cardiac Nursing. Cardiac Rehabilitation.
8. Hope theory: Rainbows in the mind. Psychological Inquiry Development and Validation of an Individual-Differences Measure of Hope; 2002.
9. Demirli A, Türkmen M, Arık R. Investigation of Dispositional and State Hope Levels’ Relations with Student Subjective Well-being. Soc Indic Res. 2015;120(2):601–613. doi:10.1007/s11205-014-0607-9
10. Tutton E, Seers K, Langstaff D. An exploration of hope as a concept for nursing. J Orthopaedic Nurs. 2009;13(3):119–127. doi:10.1016/j.joon.2009.07.006
11. Bjørnnes A, Parry M, Lie I, Falk R, Leegaard M, Rustøen T. The association between hope, marital status, depression and persistent pain in men and women following cardiac surgery. BMC Women’s Health. 2018;18(2):1–10. doi:10.1186/s12905-017-0501-0
12. Gerald F, Steven N, Blumenthal J, Caspersen C, Chaitman B, Epstein S. Benefits and recommendations for physical activity programs for all americans – a statement for health professionals by the committee on exercise and cardiac rehabilitation of the council on clinical. Cardiology. Am Heart Assoc. 1992;86(1):340–344.
13. Leon S, Franklin B, Costa F, et al. Cardiac rehabilitation and secondary prevention of coronary heart disease. Am Heart Assoc. 2005;111:369–376.
14. Schumann J, Zellweger MJ, Di Valentino M, Piazzalonga S, Hoffmann A. Sexual Dysfunction before and after Cardiac Rehabilitation. Rehabil Res Pract. 2010;2010:823060.
15. Linda S. ACSM Guideline. Vol. 9. 2013.
16. Loam D AACVPR2006. 53–74.
17. Han S, Hsiao M, Guey Wang T, Chen S, Yang W. Relation between serum myokines and Phase II cardiac rehabilitation. Medicine. 2017;96(16):1–6.
18. Bellmann B, Tina Lin T, Greissinger K, Rottner L, Rillig A, Zimmerling S. The Beneficial Effects of Cardiac Rehabilitation. Cardiol Ther. 2020;9(1):35–44. doi:10.1007/s40119-020-00164-9
19. Rakhshan M, Ansari L, Molazem Z, Zare N. Complications of heart rhythm management devices after cardiac rehabilitation program. Clin Nurse Spec. 2017;31(3):E1–E6. doi:10.1097/NUR.0000000000000293
20. G*power 2017; 2017. Available from: .
21. Demographics survey questions 2016; 2017 Available from: www.research organizing.org/uploads/pdfs/T-3-19_FINAL.pdf.
22. Miller J. Development of an Instrument to Measure Hope. Nurs Res. 1988;37(1):6–10.
23. Abdi N, Asadi Lari M. Standardization of three hope scales, as possible measures at the end of life, in Iranian population. Original Article. 2011;4(2):71–77.
24. Bahmani B, Motamed Najjar M, Sayyah M, Shafi-Abadi A, Haddad Kashani H. The effectiveness of cognitive-existential group therapy on increasing hope and decreasing depression in women-treated with haemodialysis. Glob J Health Sci. 2016;8(6):219–225. doi:10.5539/gjhs.v8n6p219
25. Mohammadpour S, Pouyanfar A, Najar Z, Jafari H, Rahmani S. The effectiveness of mindfulness-based cognitive group therapy on the quality of life and hope in the patients with coronary heart disease. Int j Indian Psychol. 2016;3(3):1–13.
26. Poorgholami F, Abdollahifard S, Zamani M, Kargar Jahromi M, Badiyepeyma Jahromi Z. The effect of stress management training on hope in hemodialysis patients. Glob J Health Sci. 2016;8(7):165–171. doi:10.5539/gjhs.v8n7p165
27. Ahmarian F, Khodabakhshi Koolaee A, Falsafinejad M. The effects of group logo-therapy on life expectancy and sleep quality in elderlies of boarding center of Tehran city. J Res Religion Health. 2015;1(3):11–18.
28. KamleshKumari S, Millind PHM, Kp J. A pilot study to assess the effectiveness of cardiac rehabilitative teaching program on quality of life and physiological parameters among patients undergoing coronary artery bypass grafting in tertiary care hospital. ORIGINAL ARTICLE. 2018;7(4):137–143.
29. Dalir Z, VahdatFeizabadi E, Mazlom R, Khorasani A. The Effect of short-term cardiac rehabilitation program on anxiety and depression in patients after coronary artery bypass surgery. Original Quantitative Qualitative Res Paper. 2013;3(3):33–42.
30. Sharif F, Shoul A, Jannati M, Koluri J, Zare N. The effect of cardiac rehabilitation on anxiety and depression in patients undergoing cardiac bypass graft surgery in Iran. BMC Cardiovasc Disord. 2012;1–7.
31. Kulcu D, Kurtais Y, Tur B, Gülec S, Seckin B. The effect of cardiac rehabilitation on quality of life, anxiety and depression in patients with congestive heart failure. A randomized controlled trial, short-term results. J Adv Nurs. 2007;43(4):489–497.
32. Theresa M, Fletcher G, Maureen W, et al. Biopsychosocial health disparities among young women enrolled in cardiac rehabilitation. NIH Public Access. 2015;35(2):103–113.
33. Beckie M, Beckstead JW. The effects of a cardiac rehabilitation program tailored for women on global quality of life: a randomized clinical trial. Journal of Women’s Health. 2010;19(11):1977–1985. doi:10.1089/jwh.2010.1937
34. Salimi T, Tavangar H, Shokripour S, Ashrafi H. The effect of spiritual self-care group therapy on life expectancy in patients with coronary artery disease: an educational trial. J Rafsanjan Univ Med Sci. 2017;15(10):917–928.
35. Dunn S, Dunn L, Rieth N, Olamijulo G. Impact of home- and hospital-based exercise in cardiac rehabilitation on hopelessness in patients with coronary heart disease. J Cardiopulm Rehabil Prev. 2016;37(1):1–10.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.