")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Effect of a Feedforward Control Model on Nursing Attitudes in the Operating Room
Received 6 June 2022
Accepted for publication 23 September 2022
Published 19 October 2022 Volume 2022:15 Pages 2399—2406
DOI https://doi.org/10.2147/JMDH.S377581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lifang Ma,1,* Youyuan Yuan,2,* Xiumei Wang3
1Department of Hospital Infection Management Office, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences,Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 2Department of Interventional Therapy for Tumor and Vascular Disease, Shanxi Bethune Hospital Shanxi Academy of Medical Sciences,Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 3Department of Central Operating Room, Shanxi Bethune Hospital Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, Shanxi, 030032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Youyuan Yuan, Department of Interventional Therapy for Tumor and Vascular Disease, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, No. 99, Longcheng Street, Taiyuan City, Shanxi, 030032, People’s Republic of China, Tel +86 13934554638, Fax +86 10 48993553, Email [email protected]
Objective: To evaluate the effect of a feedforward control model on nursing error behaviour and nursing attitudes in the operating room.
Methods: A total of 216 patients admitted to our hospital from January 2018 to December 2020 were randomly selected as the research subjects and divided into a control group and a research group, with 108 cases in each. The control group received routine surgical nursing management, while the research group received surgical nursing management with a feedforward control model. Nursing quality, error behaviour, and work attitude score, as well as the occurrence of safety hazards and patient satisfaction, were compared between the two groups of patients.
Results: Compared with the control group, the nursing quality score, including nursing document quality (72.0 ± 1.8 vs 97.2 ± 2.0), quality control inspection (75.4 ± 1.9 vs 95.5 ± 1.2), disinfection and isolation (73.4 ± 2.4 vs 96.6 ± 2.0) and nursing safety management (71.1 ± 2.2 vs 98.0 ± 1.8), were higher in the research group (P < 0.05); the scores for nursing error behaviour (13.2 ± 1.0 vs 19.4 ± 1.8) and work attitudes of the research group (14.0 ± 1.2 vs 19.0 ± 2.0) were higher (P < 0.05); and the research group had a lower incidence of safety hazards (11.1% vs 0.9%, P < 0.05); finally, the research group had higher patient satisfaction (71.3% vs 93.5%, P < 0.05).
Conclusion: The application of a feedforward control model for nursing management in the operating room can significantly reduce nurses’ errors and improve their attitudes, continuously reduce the incidence of safety incidents, improve the quality of operating room nursing and increase the satisfaction of patients and their families with the nursing care they received.
Keywords: operating room nursing management, feedforward control model, nurse nursing error behaviour, nursing attitude, impact
Introduction
Feedforward control, also known as pre-control, refers to the following implementation process: predict the consequences of possible influencing factors, and then take the corresponding measures needed to prevent them to the extent required to achieve the intended purpose.1 In recent years, the feedforward control system management model has been introduced from engineering projects into hospitals, especially in the field of operating room nursing. By their very nature, operating rooms are special. They are not only an important workplace for the hospital but also the core technical department of the hospital. Operating room nursing management is a nursing method that uses a variety of standard institutional procedures to improve the safety of surgical nursing. The feedforward control model can prevent possible nursing errors and improve nursing safety to a large extent2,3. It has been found that the application of feedforward control nursing models in surgical safety management shifts the focus of prevention and control forward and provides a means to analyse the hazards of the process, find out the control links, take effective preventive measures, emphasise the principle of systematic management and preventive control, and prevent problems before they occur. This can minimise the incidence of human error on the part of the nurses, thereby improving the quality of care and improving the effect of surgical treatment.4 To investigate the effectiveness of feedforward control, this comparative study examines how it affects error behaviour and nursing attitudes among operating room nurses, providing a basis for using a feedforward control model to formulate standardised operating procedures for surgical nursing safety management.
Materials and Methods
General Information
A total of 216 surgical patients admitted to The Shanxi Bethune Hospital from January 2018 to December 2020 were selected by simple random sampling to be study subjects. They were then divided into a control group (n = 108), which was treated with routine operating room nursing, and a research group (n = 108), which was treated with feedforward control nursing management, according to a random number table All patients were handled in the same department by 30 nurses who were randomly divided into a research group and a control group for nursing management. This study was conducted in accordance with the declaration of Helsinki and with approval from the Ethics Committee of Shanxi Bethune Hospital (NO. YXLL-2022-058). Written informed consent was obtained from all participants.
The inclusion criteria were as follows: ① aged over 18 years; ② complete clinical data; ③ high compliance; and ④ patients who were informed about and agreed to participate in the study. The exclusion criteria were: ① patients with heart, liver, kidney and other vital organ disorders; ② patients with a consciousness disorder and vague consciousness; ③ patients with coagulation or immune system dysfunction; and ④ patients who dropped out of the study. This study was approved by the Ethics Committee of our hospital, and all patients signed the informed consent form.
Methods
In the Control Group, the Patients Received Conventional Nursing Methods
The nursing protocol was as follows: the patient should make appropriate preoperative preparations, and their body temperature, blood pressure, heart rate and other vital signs should be closely observed during the operation. In case of any abnormality, the nurses should immediately inform the doctor and assist them in timely treatment of the patient.
In the Research Group, All Patients Received Surgical Nursing Management with a Feedforward Control Model
The research group performed the following nursing protocol: ① a feedforward control management responsibility group was established, which was led by the head nurse and composed of four nurses with rich experience in the undergraduate laboratory; ② the nurses were instructed on the concept of feedforward control management, and the head nurse organised all the team members to discuss and summarise previous operations, analyse the risk factors in the operating room, formulate the feedforward control management plan for the operating room and overall improve the working process; ③ safe nursing and operation technology training was conducted for operating room nursing staff, head nurses were provided with a system to perform regular assessments of team members, medical risk prevention techniques were emphasised to the operating room nursing staff and the nursing operations for operating rooms, including the use of both technologies and processes, were standardised; ④ the head nurse continuously improved the system in response to feedback from the operating rooms and department management and enforced strict compliance among the operating room nursing staff with the proper procedures; ⑤ communication between nurses and patients in the operating room was strengthened, allowing nurses to grow closer with their patients, identify problems in a timely manner and reduce the occurrence of disputes; and ⑥ to help avoid errors, continuity of nursing work in the operating room and related departments was strengthened.
Observation Indicators
Potential Safety Hazards
The occurrence of potential safety hazards was compared, including the unqualified quality of the operating room restricted area, incorrect operation sequences, incomplete surgical instruments and contamination of histopathological specimens, as shown in Supplementary Tables 1 and 2.
Nursing Quality Scores
An operating room nursing quality evaluation table was used to comprehensively evaluate the nursing quality of the nursing staff that worked on the upper level (the test–retest reliability correlation coefficient of the questionnaire data was r = 0.833, P < 0.05, suggesting that the questionnaire has good content reliability). The questionnaire was compiled by referencing the relevant literature.5 The Cronbach’s alpha of the questionnaire is 0.893. The scale includes 17 sub-items spread across four dimensions: environmental management, technical management, disinfection and infection management and humanistic care. Each item is scored on a scale from zero to 100; the higher the score, the higher the quality of care. The nursing error behaviour and nursing attitude scores were scored on a scale from zero to 20; higher scores denoted better nursing quality and nursing attitudes, as shown in Supplementary Table 3.
Nursing Satisfaction of Patients
Patient satisfaction is the degree to which the health services obtained met their needs and expectations, as judged subjectively by the patient. The day after the patient’s care and before leaving the hospital, a patient satisfaction questionnaire was used to investigate how satisfied patients were with the quality of the nursing they received, as well as the attitudes of the nursing staff. The questionnaire included basic information about patients, preoperative preparation and precautions. A total of 20 items were divided into three parts: patients’ satisfaction with nursing staff in the operating room, patients’ satisfaction with preoperative preparation and patients’ satisfaction with postoperative education. The test-retest reliability was r = 0.866, P < 0.05, indicating that the internal reliability of the scale was good. The questionnaire was compiled by referencing the relevant literature.6 The Cronbach’s alpha of the questionnaire is 0.912, with a total score of 100. Here, 90–100 points indicated that a patient was “very satisfied”, 70–89 points that they were “basically satisfied” and <70 points that their experience was “unsatisfactory”. Total satisfaction was calculated in the following way: Total Satisfaction = (very satisfied + basically satisfied) cases / total cases × 100%,7 as shown in Supplementary Tables 4 and 5.
Statistical Methods
In this study, SPSS 22.0 statistical software was used for data analysis and comparison. The measurement data were expressed by  and the comparison was made by means of a t-test; the counting data were expressed as rates (%), with comparisons made by means of the χ2 test. A value of P < 0.05 was considered to be statistically significant.
and the comparison was made by means of a t-test; the counting data were expressed as rates (%), with comparisons made by means of the χ2 test. A value of P < 0.05 was considered to be statistically significant.
Results
Basic Characteristics of Research Objects
In the control group, there were 68 males and 40 females aged 19–76 years, with an average of 47.0 ± 1.5 years. The length of their hospital stay ranged from 10–28 days, with an average of 19.0 ± 1.9 days. In the research group, there were 69 males and 39 females aged 20–76 years, with an average age of 47.5 ± 1.6 years. The general demographic data of the patients in the two groups were comparable (P > 0.05) (Table 1).
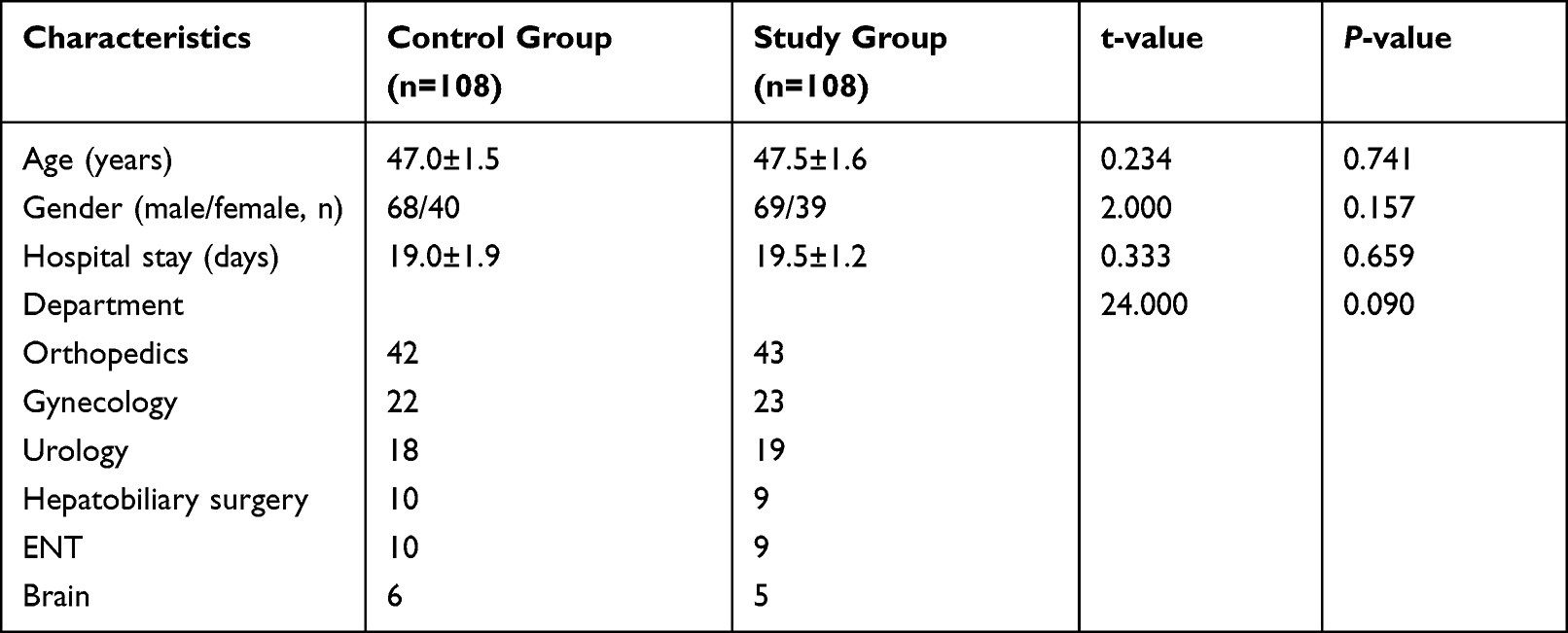 |
Table 1 Baseline Characteristics Description and Comparison Between the Control Group and the Study Group |
Nursing Quality
Compared with the control group, the nursing quality score, including the nursing document quality (72.0 ± 1.8 vs 97.2 ± 2.0), quality control inspection (75.4 ± 1.9 vs 95.5 ± 1.2), disinfection and isolation (73.4 ± 2.4 vs 96.6 ± 2.0) and nursing safety management (71.1 ± 2.2 vs 98.0 ± 1.8) scores, were higher in the research group, and the differences had statistical significance (P < 0.05), as shown in Table 2.
 |

Nursing Error Behaviour and Nursing Work Attitude Scores
Compared with the control group, the scores for nursing error behaviour (13.2 ± 1.0 vs 19.4 ± 1.8) and nursing attitudes in the research group (14.0 ± 1.2 vs 19.0 ± 2.0) were higher, and the differences had statistical significance (P < 0.05), as shown in Table 3.
 |
Table 3 Nursing Error Behavior, Nursing Work Attitude Score (Points, |

The Occurrence of Potential Safety Hazards
Compared with the control group, the research group had a lower incidence of safety hazards (11.1% vs 0.9%), such as the unqualified quality of the operating room restricted area, incorrect surgical sequences, incomplete surgical instruments and contamination of histopathological specimens. The differences had statistical significance (P < 0.05), as shown in Table 4.
 |
Table 4 Occurrence of Potential Safety Hazards (Cases, %) |
Nursing Satisfaction
Compared with the control group, the research group’s patients were more likely to claim that they were satisfied with the nursing they had received (71.3% vs 93.5%), and the differences had statistical significance (P < 0.05); see Table 5.
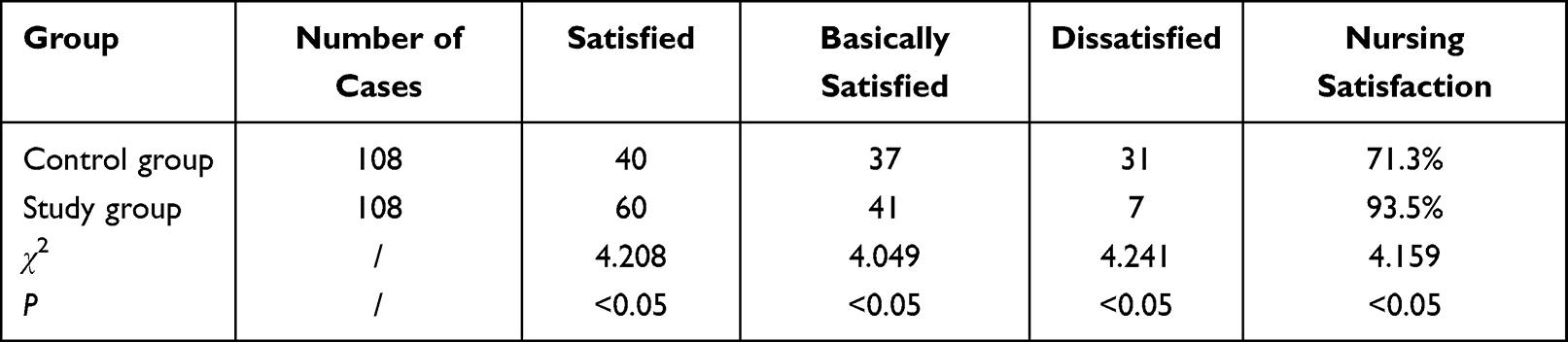 |
Table 5 Nursing Satisfaction (Cases, %) |
Discussion
Feedforward control, also known as advance control or preventive control, refers to a quality control method that predicts the consequences of management activities and takes preventive measures before management so that possible deviations can be avoided in advance.8,9 Feedforward control is characterised by an attitude of “prevention first”, and its application in fields of medicine can minimise risk to patients and ensure that the care they receive is in their best interest.10 In recent years, this method has been applied in clinical nursing work and has been shown to have certain unique advantages. Feedforward control is most useful for preventing “deviations” from the safest and most efficient procedures. Carrying out feedforward control of nursing safety quality overcomes the shortcomings of only paying attention to “treatment” (that is, correcting quality control problems after they have already occurred), which characterises legacy management systems, and establishes a system that can both “treat” and “prevent” by reducing the occurrence of mistakes by nurses and promoting the continuous improvement of nursing quality. Feedforward control of the quality of paediatric nursing services can improve the care that patients and their families receive to such an extent that some may consider it transformative. One study demonstrated that after the implementation of a feedforward control system, adverse events involving ICU catheters decreased from 55 to 23, suggesting that feedforward control management can also be used as an effective means of managing nurses who handle ICU catheters.11 The application of feedforward control models in surgical safety management shifts the focus of prevention and control forward, analyses the hazards inherent to the process, uncovers the relevant control links and takes action to prevent them, emphasises systematic management and preventive control principles and plays a role in preventing problems before they occur.12 Feedforward control models can effectively stimulate enthusiasm among nursing staff and help them take responsibility for the care they administer, cultivate foresight and adaptability, and improve the safety of surgical treatment.
The results of this study showed that the quality scores of nursing work and patient satisfaction in the research group were significantly higher than that in the control group, while the incidence rate of adverse events was lower, suggesting that the adoption of feedforward control management can significantly improve the quality of nursing care and reduce the incidence rate of adverse events if adopted in other contexts. The results also indicate that the application of operating room nursing management with a feedforward control model can effectively reduce the incidence of nursing error behaviour and improve nursing work attitudes, thereby improving the quality of nursing. This is mainly because the feedforward control model uses previous case data and experience to formulate an appropriate prevention and control scheme that analyses risk factors in order to reduce the incidence of nursing service deviations, improve the safety of nursing management in the operating room and improve the overall quality and efficiency of nursing work.13 Additionally, the feedforward control method can implement dynamic and rational management of the operating room and improve the safety of operating room nursing management through the effective management of personnel, items and the environment.14 Adding feedforward control to operating room nursing management can standardise operating room procedures, rules and regulations that strictly follow the nursing service principle of “people-oriented, life first”.15 At the same time, it can improve nurses’ safety awareness, cultivate their professional ethics and improve their sense of responsibility to achieve an end goal of reducing nursing error behaviour and improving their nursing work attitudes.16
The research results show that, compared with the control group, the research group had a lower incidence of safety hazards, such as unqualified quality of the operating room restricted area, incorrect surgical sequences, incomplete surgical instruments and contamination of histopathological specimens. Additionally, compared with the control group, the nursing satisfaction of the research group was higher, indicating that the application of operating room nursing management with a feedforward control model can effectively reduce the incidence of potential safety hazards, ensure the safety of patients and improve the nursing satisfaction of patients and their families. This is mainly because the application of the feedforward control model in operating room nursing safety management can fully stimulate the enthusiasm of nurses and enhance their sense of responsibility and ability to predict and adapt.17 The application of feedforward control management can also deepen nurses’ understanding of the theory of operating room nursing management, safety risk awareness and other professional knowledge, greatly improving the service quality of operating room nursing.18 At the same time, by cultivating the predictive thinking of nurses, the incidence of potential safety hazards in the nursing process of the operating room is reduced, and safety is improved.19 By doing all these things and by addressing both the practical and psychological aspects of nursing, feedforward control methods foster a harmonious relationship between nurses and patients and enhance patients’ overall satisfaction with their nurses’ service.20
Limitations of this study: The survey scope and number of respondents in this study were relatively small and confined to just one region, and the implementation of surgical safety management and nursing in different levels of hospitals was not included. In the future, the scope of investigation could be expanded to encompass multiple regions and levels of hospitals as well as nursing staff from different kinds of departments. A study with this broader scope would be better able to examine the factors that lead to nursing error behaviour and poor nursing quality in operating rooms.
Limitation
Due to the existence of individual differences in this study, the selection results may be biased. Additionally, this study may have been biased by the fact that it only included the respondents’ own situation and characteristics without considering the influence of the external environment. It is expected that in the future, a larger randomised study will be done to confirm the results of this study and determine whether there are additional factors that influence nursing quality; only then will we be able to draw firmer conclusions.
Conclusion
In summary, the advantage of feedforward control lies in “prevention before it occurs”, and the highly respected forward-looking technology in the field of risk management. The application of feedforward control can pre-empt the adverse factors that affect safety, minimise risk to patients and maximise the probability of good outcomes for patients. This study evaluated the application of feedforward control in operating room safety management nursing work from multiple perspectives, including potential safety hazards, nursing quality score, nursing error behaviour score, nursing attitude score and patient nursing satisfaction, while comprehensively analysing the effectiveness of a feedforward control model on patient safety in the operating room. Risk management based on feedforward control theory is a means to effectively control the occurrence of risks, and its application in operating room nursing management can effectively reduce the error behaviour of nurses, improve their nursing attitudes, continuously reduce the incidence of potential safety hazards and increase the satisfaction of patients and their families. By emphasising the refinement of each process through the feedforward control model, the work enthusiasm and professional awareness of nursing staff can be improved, their sense of responsibility can be enhanced and then economic and social benefits can be brought to hospitals to promote their healthy and sustainable development.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Shanxi Bethune Hospital. Written informed consent was obtained from all participants.
Consent for Publication
The manuscript is not submitted for publication or consideration elsewhere.
Acknowledgments
No funding or sponsorship was received for this study or publication of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Man APN, Lam CKM, Cheng BCP, Tang KS, Tang PF. Impact of locally adopted simulation-based crew resource management training on patient safety culture: comparison between operating room personnel and general health care populations pre and post course. Am J Med Qual. 2020;35(1):79–88. doi:10.1177/1062860618824863
2. Ma DF, Wu JY, Wang YT, Yi WY. Application of detail management in nursing safety management in operating room. Minerva Med. 2020. doi:10.23736/S0026-4806.20.07107-4
3. Labrague LJ. Influence of nurse managers’ toxic leadership behaviours on nurse‐reported adverse events and quality of care. J Nur Manag. 2020;29(4):855–863. doi:10.23736/S0026-4806.20.07107-4
4. Liu GP. The value evaluation of PDCA cycle method in nursing quality management of gynecological tumor endoscopic surgery. Chinese J Cancer Prev Treat. 2019;26(S1):
5. Li JB, Zhang YJ. Influence of PDCA cycle method combined with humanized concept on safety management and nursing quality in operating room. Medl Forum. 2022;26(12):125–128. doi:10.19435/j.1672-1721.2022.12.040
6. Liu NJ, Yang H. Effects of psychological nursing combined with dietary nursing on emotion and nursing satisfaction of patients with thyroid surgery. Clin Med Res Pract. 2022;7(15):180–182. doi:10.19347/j.cnki.2096-1413.20221505
7. Chen JS, Su QX, Zhong CH, Gu QQ. Application effect of feedforward control theory in nursing management of opeSrating room. Chin Contemp Med. 2021;28(20):215–218. doi:10.3969/j.issn.1674-4721.2021.20.062
8. Du J. Application effect of feedforward control in the nursing safety management of operating room. Clin Res Pract. 2017;2(05):158–159. doi:10.19347/j.cnki.2096-1413.201705084
9. Song LF, Xu RX. Intervention strategies for the management of nosocomial infection among cleaning staff in the operating room. Chin J Nosocomiol. 2013;23(12):2963–2964.
10. Allen RW, Taaffe KM, Neilley V, Busby E. First case on-time starts measured by incision on-time and no grace period: a case study of operating room management. J Healthc Manag. 2019;64(2):111–121. doi:10.1097/JHM-D-17-00203
11. Yang F. Influence of feedforward control model on nursing error behavior and nursing attitude of nurses in operating room nursing management. Contemp Med. 2020;26(01):75–77.
12. Bai J. Perioperative nursing intervention based on feedforward control for patients with general surgery. J Clin Med Pract. 2020;24(16):106–108. doi:10.7619/jcmp.202016030
13. Ye YQ, Shi RL, Wang L. Influence of three-dimensional quality control management mode on nursing quality assessment and risk in operating room. Chin Remedies Clin. 2019;19(13):2294–2296. doi:10.11655/zgywylc2019.13.075
14. Gao RW, Plummer RV, Mckenna RL. International operating room nurses’ challenges in providing person-centered care during organ procurement surgery. J Perianesth Nurs. 2020;35(4):417–422. doi:10.1016/j.jopan.2019.12.005
15. Bao YX, Sun LJ, Yuan M, Yang XQ. Application effect evaluation of failure mode and effect analysis in nursing quality and safety management in operating room. Chin Remedies Clin. 2019;19(12):2110–2112. doi:10.11655/zgywylc2019.12.078
16. Wu HY, Wang ML, Yang B. Application of case-based learning teaching mode based on WeChat public platform in nursing teaching practice in operation room. Chin J Pract Nurs. 2019;35(4):303–305. doi:10.3760/cma.j.issn.1672-7088.2019.04.015
17. Escorcia-Hernández JM, Aguilar-Sierra H, Aguilar-Mejia O, Chemori A, Arroyo-Núñez JH. A new adaptive RISE feedforward approach based on associative memory neural networks for the control of PKMs. J Intell Robot Syst. 2020;100:827–847. doi:10.1007/s10846-020-01242-9
18. Yang DY, Wu YM. Analysis of the application effect of hierarchical group management mode in operating room nurses. Chin Remedies Clin. 2020;25(7):1197–1198. doi:10.11655/zgywylc2020.07.071
19. Lin P, Jiang H, Zheng ZD. Effects of plan-do-check-action cycle management model combined with detail nursing on improving safety management and nursing quality in operating room. Chin JMod Nurs. 2019;25(11):1429–1431. doi:10.3760/cma.j.issn.1674-2907.2019.11.026
20. Warth G, Frey M, Gauterin F. Usage of the cornering stiffness for an adaptive rear wheel steering feedforward control. IEEE Trans Veh Technol. 2019;68(1):264–275. doi:10.1109/TVT.2018.2883809
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.