")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 10
Effect of a combination of whole body vibration exercise and squat training on body balance, muscle power, and walking ability in the elderly
Authors Osugi T, Iwamoto J, Yamazaki M, Takakuwa M
Received 19 November 2013
Accepted for publication 31 December 2013
Published 20 February 2014 Volume 2014:10 Pages 131—138
DOI https://doi.org/10.2147/TCRM.S57806
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Tomohiro Osugi,1 Jun Iwamoto,2 Michio Yamazaki,1 Masayuki Takakuwa3
1Department of Rehabilitation, Takakuwa Orthopaedic Nagayama Clinic, Asahikawa, Hokkaido, 2Institute for Integrated Sports Medicine, Keio University School of Medicine, Shinjuku-ku, Tokyo, 3Department of Orthopaedic Surgery, Takakuwa Orthopaedic Nagayama Clinic, Asahikawa, Hokkaido, Japan
Abstract: A randomized controlled trial was conducted to clarify the beneficial effect of whole body vibration (WBV) exercise plus squat training on body balance, muscle power, and walking ability in the elderly with knee osteoarthritis and/or spondylosis. Of 35 ambulatory patients (14 men and 21 women) who were recruited at our outpatient clinic, 28 (80.0%, 12 men and 16 women) participated in the trial. The subjects (mean age 72.4 years) were randomly divided into two groups (n=14 in each group), ie, a WBV exercise alone group and a WBV exercise plus squat training group. A 4-minute WBV exercise (frequency 20 Hz) was performed 2 days per week in both groups; squat training (20 times per minute) was added during the 4-minute WBV training session in the WBV exercise plus squat training group. The duration of the trial was 6 months. The exercise and training program was safe and well tolerated. WBV exercise alone improved indices of body balance and walking velocity from baseline values. However, WBV exercise plus squat training was more effective for improving tandem gait step number and chair-rising time compared with WBV exercise alone. These results suggest the benefit and safety of WBV exercise plus squat training for improving physical function in terms of body balance and muscle power in the elderly.
Keywords: whole body vibration exercise, squat training, body balance, walking velocity, muscle power
Introduction
Fall-related injuries, including head injuries and fractures, are serious problems among the elderly as they often lead to prolonged or even permanent disability. Thus, prevention of falls and injuries associated with such falls can reduce disability, improve quality of life, and reduce the costs of health care. Thus, exercises aimed at improving physical function and preventing falls appear to be important for increasing the active life expectancy of elderly individuals.
Impairment of muscle strength and muscle power in the lower extremities, balance/postural control, and walking ability have been recognized as important risk factors for falls.1 However, muscle strength should be distinguished from muscle power: muscle strength is defined as the maximal force that a muscle can produce against a given resistance, while muscle power (force × velocity) is defined as the product of force and speed;1,2 the former is related to bone strength whereas the latter is related to falling.1–4 Thus, improvement of muscle power, rather than muscle strength, is likely to be important for preventing falls. Proximal leg muscle power can be evaluated by measuring the chair-rising time.
Whole-body vibration (WBV) exercise has been developed as a new modality in the field of physiotherapy and has been proposed as an exercise to improve physical function in the elderly. Previously, we conducted a randomized controlled trial to determine the effect of WBV exercise on physical function in postmenopausal osteoporotic women treated with alendronate5 and found that WBV exercise improved static body balance (one-leg standing time and tandem standing time) and walking velocity, but not dynamic body balance (Timed Up and Go [TUG]) and muscle power (chair-rising time) compared with nonexercising controls. We also conducted another randomized controlled trial to compare the effect of a one-leg standing exercise (static body balance training) and chair-rising exercise (muscle power training) on physical function in patients with locomotive disorders6 and found that the one-leg standing exercise improved static body balance while the chair-rising exercise was useful for improving walking velocity, dynamic body balance, and muscle power. Squat training, which mimics chair-rising training, may train the quadriceps and gluteus medius muscles and improve joint movement in the lower extremities. Based on the results of these two randomized controlled trials, we hypothesized that a combination of WBV exercise and squat training might be more effective than WBV exercise alone for improving physical function, especially in terms of dynamic body balance and muscle power, in the elderly. The objective of the present study was to clarify the beneficial effect of WBV exercise plus squat training on physical function, including body balance, muscle power, and walking ability in the elderly. The primary endpoint was physical function.
Subjects and methods
Subjects
Thirty-five ambulatory patients (14 men and 21 women) with knee osteoarthritis of Kellgren-Lawrence grade7 1, 2, or 3 and/or spondylosis without spinal cord or nerve root compression symptoms who visited the Takakuwa Orthopaedic Nagayama Clinic (Hokkaido, Japan) between September 2012 and May 2013 were recruited. The inclusion criteria were age older than 60 years and the ability to measure the parameters described below. Exclusion criteria were use of vitamin D3 for osteoporosis,8 severe gait disturbance requiring an ambulatory aid, a severely rounded back because of osteoporotic vertebral fractures, an acute disease phase, and severe cardiovascular disease. Of 35 patients who were screened, 28 (80.0%, 12 men and 16 women, mean age 72.4 years) participated in the trial.
Each subject was assigned by means of table random numbering. The subjects were divided into two groups (n=14 in each group), ie, a WBV exercise alone group (control group) and a WBV exercise plus squat training group (squat training group). Squat training was performed on the rocking platform of a Galileo machine (G-900; Novotec, Pforzheim, Germany) during a 4-minute WBV exercise session. The study period was 6 months. Non-steroidal anti-inflammatory drugs were transiently prescribed for subjects who needed pain relief because of knee osteoarthritis and/or spondylosis. The WBV exercise and squat training were supervised and performed in the clinic on two days per week. Because the study was strictly conducted by physical therapists, adherence, ie, compliance and persistence with the exercises and training, was 100%. All participants completed the 6-month trial. The physical activity level at baseline was considered to be comparatively low in all participants because none had been laborers or engaged in any regular or leisure sporting activities. Further, no home exercise was prescribed for any of the participants. Informed consent was obtained from each of the subjects prior to participation in the study. The protocol was approved by the ethics committee of Takakuwa Orthopaedic Nagayama Clinic.
Assessment of physical function
After assessment of age, body weight, height, body mass index, history of falls in the previous year, and fall-related fractures after 50 years of age, physical function was evaluated by measuring tandem standing time, 10 m tandem gait time, tandem gait step number, 3 m TUG, 5-repetition chair-rising time, 10 m walking time, and 10 m walking step number. The tandem standing time is an index of static body balance. The tandem gait time, tandem gait step number, and TUG are indices of dynamic body balance. The chair-rising time is an index of muscle power.1 The 10 m walking time and walking step number are indices of walking ability.
The 5-repetition chair-rising time was measured with the subject’s arms crossed over the chest. The chair-rising time was the time required for a subject to stand up from a chair (45 cm in height) five times as quickly as possible without using their arms. The tandem standing time was determined by obtaining the mean value of two measurements, ie, one with the right foot forward and the other with the left foot forward. Physical performances including walking speed, chair-rising, tandem maneuver, and TUG are considered to be important determinants of musculoskeletal frailty and fall risk in older age.1,2,8,9
WBV exercise and squat training
WBV exercise was performed using a Galileo machine, a device that is used to apply WBV/oscillatory muscle stimulation. The subject stands with knees bent (by 45 degrees) and hips bent (by 45 degrees), with feet 20 cm apart on a rocking platform with a sagittal axle that alternately thrusts the right and left legs upwards and downwards, thereby activating the muscles of the lower extremities. The reaction of the neuromuscular system consists of a chain of rapid muscle contractions. This type of training provides reflex muscle stimulation with no serious adverse events. Each WBV exercise session was set at a frequency of 20 Hz and for a duration of 4 minutes. This frequency is thought to be comfortable and safe for elderly adults. In the control group, only WBV exercise was performed (Figure 1).
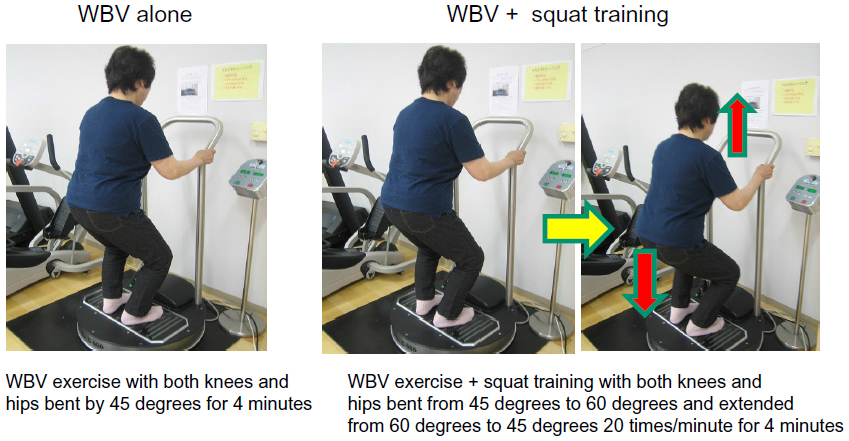 | Figure 1 WBV exercise and squat training. WBV exercise was performed using a Galileo machine (G-900; Novotec, Pforzheim, Germany). The subject stands with knees bent (by 45 degrees) and hips bent (by 45 degrees), with feet 20 cm apart on a rocking platform with a sagittal axle that alternately thrusts the right and left legs upwards and downwards, thereby activating the muscles of the lower extremities. Each WBV exercise session was set at a frequency of 20 Hz and for a duration of 4 minutes. In the control group, only WBV exercise was performed. In the squat training group, squat training was added on the rocking platform of the Galileo machine during the 4-minute WBV exercise session. |
In the squat training group, dynamic squat training was added on the rocking platform of the Galileo machine during the 4-minute WBV exercise session. Both knees and hips were bent from 45 degrees to 60 degrees and extended from 60 degrees to 45 degrees 20 times per minute for 4 minutes (Figure 1).
Statistical analysis
The data are expressed as the mean ± standard deviation in the tables and the mean ± standard error in the figures. An unpaired t-test was used to compare the anthropometric data and parameters of physical function at baseline. One-way analysis of variance with repeated measurements was used to analyze longitudinal changes in physical function parameters within a group. Two-way analysis of variance with repeated measurements was used to compare longitudinal changes in physical function parameters between the two groups. The Fisher’s exact test was used to compare the ratio of male to female patients, percentages of patients who had fallen in the past year, percentages of patients with prior clinical fractures, and the incidences of falls and fall-related fractures between the two groups. All statistical analyses were performed using the Stat View J 5.0 program (SAS Institute, Cary, NC, USA). The significance level was set at P<0.01 for all comparisons.
Results
Characteristics and physical function of study subjects at baseline
Table 1 shows the anthropometric characteristics of the study subjects. The mean age was 72.3 (range 65–80) years in the squat training group and 72.5 (range 63–83) years in the control group. No significant differences in the ratio of male to female subjects, age, height, body weight, or body mass index were observed between the two groups. In addition, no significant difference was seen in either the percentage of subjects who had experienced falls during the previous year (78.6% in the squat training group versus 71.4% in the control group) or the percentage of subjects who had a history of clinical fractures (14.3% in the squat training group versus 21.4% in the control group). A clinical fracture had occurred at the spine and proximal humerus (n=1) in the squat training group and at the spine (n=1) and distal radius (n=3) in the control group. The main locomotive disorders were knee osteoarthritis (n=11) and/or lumbar spondylosis (n=14) in the squat training group and knee osteoarthritis (n=12) and/or lumbar spondylosis (n=11) in the control group.
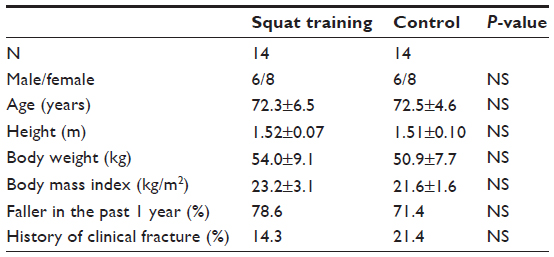 | Table 1 Baseline characteristics of study subjects |
Table 2 shows the baseline physical function of the study subjects. No significant differences in any of the baseline physical function parameters were observed between the two groups.
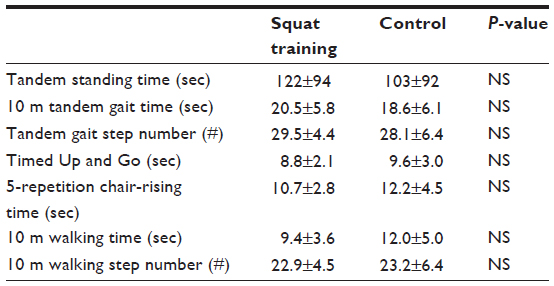 | Table 2 Baseline physical function–body balance, muscle power, and walking ability indices |
Changes in physical function
Figures 2 and 3 show the longitudinal changes in static body balance and walking ability parameters and in dynamic body balance and muscle power parameters, respectively. Table 3 shows the results of the one-way and two-way analyses of variance with repeated measurements. In the squat training group, all parameters improved significantly from baseline values, whereas in the control group, all parameters except for tandem gait step number and 5-repetition chair-rising time improved significantly from baseline values (one-way analysis of variance with repeated measurements). The tandem gait step number and 5-repetition chair-rising time improved significantly from baseline values in the squat training group compared with the control group (two-way analysis of variance with repeated measurements).
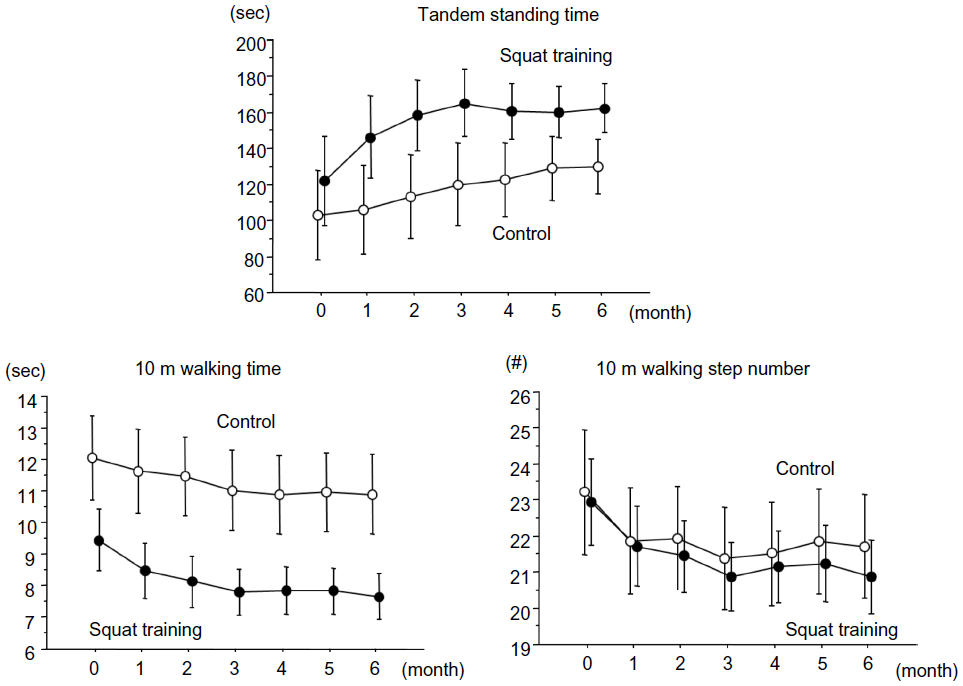 | Figure 2 Changes in static body balance and walking ability parameters. The data are expressed as the mean ± standard error. A one-way analysis of variance with repeated measurements showed that all parameters improved significantly from baseline values in both groups. However, a two-way analysis of variance with repeated measurements showed that improvement of one-leg standing time, but not tandem standing time, 10 m walking time, and 10 m walking step number, was significantly greater in the squat training group than in the control group. |
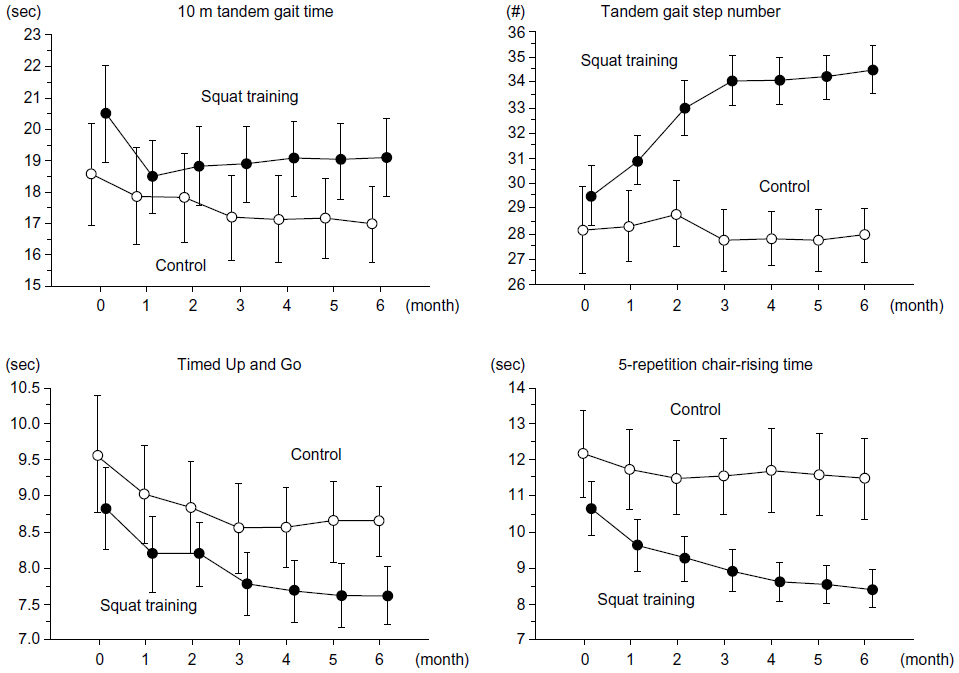 | Figure 3 Changes in dynamic body balance and muscle power parameters. The data are expressed as the mean ± standard error. A one-way analysis of variance with repeated measurements showed that all parameters improved significantly from baseline values in the squat training group, whereas 10 m tandem gait time and TUG improved significantly from baseline values in the control group. Tandem gait step number and 5-repetition chair-rising time improved significantly from baseline values in the squat training group compared with the control group. |
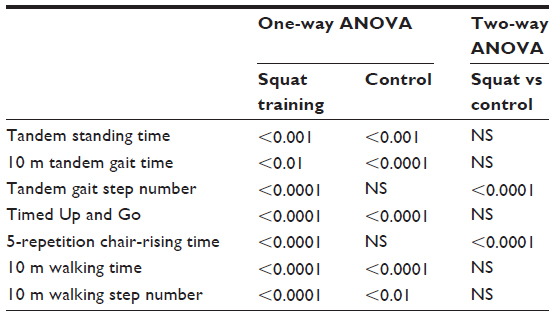 | Table 3 One- and two-way ANOVAs with repeated measurements (P-values) |
Incidence of falls and fall-related fractures
None of the participants in the squat training group fell, but two (14.3%) participants in the control group experienced two falls during the 6-month study period, with one participant suffering a mild contusion. No fall-related fractures were observed in any of the fallers. The incidence of falls and fall-related fractures did not differ significantly between the two groups.
Adverse events of WBV exercise and squat training
No serious adverse events, such as severe injuries or adverse cardiovascular effects, were observed. The exercise and training programs were considered to be safe and were well tolerated.
Discussion
The present study confirmed that WBV exercise alone improves indices of body balance and walking velocity from baseline values in elderly adults. However, WBV exercise plus squat training was more effective for improving tandem gait step number and chair-rising time compared with WBV exercise alone. These results suggest a beneficial effect of WBV exercise plus squat training for improving physical function in terms of dynamic body balance and muscle power in elderly adults with locomotive disorders such as knee osteoarthritis and spondylosis.
We administered WBV exercise to the subjects on two days per week at a frequency of 20 Hz and for a duration of 4 minutes. The intensity and frequency of the exercise program were considered to be reasonable for elderly adults (mean age 72.4 years), enabling the exercise to be continued for 6 months without any fatigue or difficulty. Compliance with exercise is an important factor for preventing falls among the elderly, and was 100% in our study. WBV exercise not only improved the subjects’ physical functioning, ie, body balance (tandem standing time, tandem gait time, and TUG), and walking velocity from baseline values, but was also well tolerated. No serious adverse events, such as fall-related fractures or adverse cardiovascular effects, were observed in any of the subjects during the exercise program, suggesting the safety of WBV exercise.
One possible mechanism explaining the effect of WBV exercise on physical function may be that a chain of rapid muscle contractions during exercise might directly activate the neuromuscular system in the lower extremities. Another possibility may be the rapid stimulation of growth hormone secretion after WBV exercise, because WBV exercise has been shown to elicit an acute growth hormone profile and neuromuscular performance responses immediately after the exercise.10
However, because of the lack of a non-WBV exercise control group, whether these changes in physical function parameters were attributable to the WBV exercise itself remain uncertain. Our previous randomized controlled trial in postmenopausal osteoporotic women (mean age 74.2 years) treated with alendronate showed that WBV exercise improved tandem standing time and walking velocity, but not TUG and chair-rising time compared with nonexercising controls.5 The present study confirmed that WBV exercise plus squat training was more effective for improving tandem gait step number (dynamic body balance) and chair-rising time (muscle power) than WBV exercise alone and was also well tolerated. Squat training might have trained the quadriceps and gluteus medius muscles and improved joint movement in the lower extremities, resulting in improvements in body balance and muscle power.
Several studies have determined the benefit of a combination of WBV exercise and squat or resistance training on physical function and muscle activity compared with squat training alone in young adults. Lamont et al11–13 showed that a 6-week squat training program with WBV exercise was more effective for improving the 20 kg squat jump height, the peak power of a 20 kg squat jump and 30 cm depth jump, and the rate of force development to the initial peak in force as evaluated using an isometric squat test, compared with squat training alone. Hazell et al14 showed that addition of WBV exercise to dynamic squatting resulted in increased muscle activity in the lower limbs. Conversely, Kvorning et al15 reported that combined WBV and resistance training did not additionally increase the maximal isometric voluntary contraction during the leg press. Artero et al16 reported that addition of WBV exercise to resistance training during an 8-week study period did not result in greater improvement of muscular performance compared with an identical exercise program performed without vibration. Rønnestad17 showed that squatting on a vibration platform resulted in a similar improvement in maximal strength and explosive power compared with squatting without vibration. Based on these previous reports, whether combination of WBV exercise and squat training has a beneficial effect on physical function compared with squat training alone in young adults remains controversial.
In elderly adults, Avelar et al18 showed that addition of WBV exercise to squat training failed to result in significant improvements in functional performance or self-reported status of knee osteoarthritis compared with squat training alone. This result might be partly attributable to the relatively short duration of treatment (12 weeks). However, the benefit of squat training in addition to WBV exercise remains uncertain. Our positive outcome (WBV exercise plus squat training versus WBV exercise alone) might have been related to the longer period of treatment (6 months) and performance of adequate WBV exercise plus squat training as instructed by experts. Thus, it is recommended that physicians prescribe exercise therapy with WBV exercise plus squat training, rather than WBV exercise alone, in elderly adults.
Despite a favorable improvement in physical function, the incidence of falls was not significantly reduced by WBV exercise plus squat training compared with WBV exercise alone (0% in the squat training group versus 14.3% in the exercise group). Thus, the magnitude of the clinical effect of squat training in addition to WBV exercise remains uncertain. However, one possibility for the lack of a significant effect of WBV exercise plus squat training on the incidence of falls may be inadequate statistical power. The duration of the presently reported study was 6 months and the sample size was 28 (n=14 in each group). Further, the standard deviations of some physical function parameters were relatively high because the groups were heterogeneous (especially in terms of age, which certainly influences muscle mass). Long-term exercise is needed to reduce the lifetime risk of falls and fall-related fractures in elderly adults. However, because our exercise program was relatively easy for subjects (mean age 74.2 years) to continue, we believe that it could be continued without any difficulty.
TUG, which consists mainly of chair-rising, walking, turning, and sitting, is known to be a reliable and valid test for quantifying functional mobility.19 However, the results for TUG were not improved by WBV exercise plus squat training compared with WBV exercise alone, suggesting that our exercise program may not be useful for turning actions in patients with locomotive disorders such as knee osteoarthritis or spondylosis.
The limitations of the present study should be discussed. First, the study period was relatively short (6 months). Long-term exercise is needed to reduce the lifetime risk of falls and fall-related fractures. Second, the number of study subjects was too small to obtain significant results regarding the incidence of falls, even though statistically significant results regarding physical function were obtained. Third, we did not evaluate vitamin D insufficiency/deficiency by measuring serum 25(OH)D levels, and we did not provide calcium/vitamin D supplements to the subjects. In Japan, vitamin D supplementation is uncommon, and measurement of serum 25(OH)D levels is not covered by health insurance. Because low serum levels of 25(OH)D are correlated with an increased risk of falls and vitamin D supplementation reduces the incidence of falls in elderly adults,20–22 evaluating vitamin D status is important. Fourth, because there was no control group in which participants performed either WBV exercise or squat training, the effect of WBV exercise alone on physical function remains unclear. Fifth, because of the open-label nature of this study, physical function was not assessed in a blinded manner, so its outcome might have been biased. Further, the study was performed at a single center so there might have been a bias in selection of the study subjects. Thus, further studies are needed to overcome these study limitations.
In conclusion, we conducted the present study to confirm the beneficial effect of 6 months of WBV exercise plus squat training on physical function, including body balance, muscle power, and walking ability, in elderly adults with knee osteoarthritis and/or spondylosis. WBV exercise alone improved indices of body balance and walking velocity from baseline values. However, WBV exercise plus squat training was more effective for improving tandem gait step number and chair-rising time compared with WBV exercise alone. These results suggest the benefit and safety of WBV exercise plus squat training for improving physical function in terms of body balance and muscle power in elderly adults.
Disclosure
The authors report no conflicts of interest in this work.
References
Runge M, Rehfeld G, Resnicek E. Balance training and exercise in geriatric patients. J Musculoskel Neuronal Interact. 2001;1:61–65. | |
Runge M, Hunter G. Determinants of musculoskeletal frailty and the risk of falls in old age. J Musculoskel Neuronal Interact. 2006;6:167–173. | |
Frost HM. Defining osteopenias and osteoporosis: another view (with insights from a new paradigm). Bone. 1997;20:385–391. | |
Schiessl H, Frost HM, Jee WSS. Estrogen and bone-muscle strength and mass relationship. Bone. 1998;22:1–6. | |
Iwamoto J, Sato Y, Takeda T, Matsumoto H. Whole body vibration exercise improves body balance and walking velocity in postmenopausal osteoporotic women treated with alendronate: Galileo and Alendronate Intervention Trial (GAIT). J Musculoskelet Neuronal Interact. 2012;12:136–143. | |
Yamashita F, Iwamoto J, Osugi T, Yamazaki M, Takakuwa M. Chair rising exercise is more effective than one-leg standing exercise in improving dynamic body balance: a randomized controlled trial. J Musculoskelet Neuronal Interact. 2012;12:74–79. | |
Dukas L, Schacht E, Runge M, Ringe JD. Effect of a six-month therapy with alfacalcidol on muscle power and balance and the number of fallers and falls. Arzneimittelforschung. 2010;60:519–525. | |
Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502. | |
Lagari V, Gómez-Marín O, Levis S. The role of vitamin D in improving physical performance in the elderly. J Bone Miner Res. 2013;28:2194–2201. | |
Bosco C, Iacovelli M, Tsarpela O, et al. Hormonal responses to whole-body vibration in men. Eur J Appl Physiol. 2000;81:449–454. | |
Lamont HS, Cramer JT, Bemben DA, Shehab RL, Anderson MA, Bemben MG. Effects of a 6-week periodized squat training program with or without whole-body vibration on jump height and power output following acute vibration exposure. J Strength Cond Res. 2009;23:2317–2325. | |
Lamont HS, Cramer JT, Bemben DA, Shehab RL, Anderson MA, Bemben MG. Effects of 6 weeks of periodized squat training with or without whole-body vibration on short-term adaptations in jump performance within recreationally resistance trained men. J Strength Cond Res. 2008;22:1882–1893. | |
Lamont HS, Cramer JT, Bemben DA, Shehab RL, Anderson MA, Bemben MG. Effects of adding whole body vibration to squat training on isometric force/time characteristics. J Strength Cond Res. 2010;24:171–183. | |
Hazell TJ, Kenno KA, Jakobi JM. Evaluation of muscle activity for loaded and unloaded dynamic squats during vertical whole-body vibration. J Strength Cond Res. 2010;24:1860–1865. | |
Kvorning T, Bagger M, Caserotti P, Madsen K. Effects of vibration and resistance training on neuromuscular and hormonal measures. Eur J Appl Physiol. 2006;96:615–625. | |
Artero EG, Espada-Fuentes JC, Argüelles-Cienfuegos J, Román A, Gómez-López PJ, Gutiérrez A. Effects of whole-body vibration and resistance training on knee extensors muscular performance. Eur J Appl Physiol. 2012;112:1371–1378. | |
Rønnestad BR. Comparing the performance-enhancing effects of squats on a vibration platform with conventional squats in recreationally resistance-trained men. J Strength Cond Res. 2004;18:839–845. | |
Avelar NC, Simão AP, Tossige-Gomes R, et al. The effect of adding whole-body vibration to squat training on the functional performance and self-report of disease status in elderly patients with knee osteoarthritis: a randomized, controlled clinical study. J Altern Complement Med. 2011;17:1149–1155. | |
Podsiadlo D, Richardson S. The timed “Up and Go:” a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39:142–148. | |
Suzuki T, Kwon J, Kim H, et al. Low serum 25-hydroxyvitamin D levels associated with falls among Japanese community-dwelling elderly. J Bone Miner Res. 2008;23:1309–1317. | |
Sato Y, Iwamoto J, Kanoko T, Satoh K. Low-dose vitamin D prevents muscular atrophy and reduces falls and hip fractures in women after stroke: a randomized controlled trial. Cerebrovasc Dis. 2005;20:187–192. | |
Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et al. Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ. 2009;339:b3692. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.