")
Back to Journals » OncoTargets and Therapy » Volume 15
Ectopic Adrenocorticotropic Hormone-Secreting Pituitary Adenoma in the Clivus Region: A Case Report
Authors Zhang Y , Wu D, Wang R, Luo M, Wang D, Wang K , Ai Y, Zheng L, Zhang Q, Shi L
Received 13 June 2022
Accepted for publication 23 August 2022
Published 29 August 2022 Volume 2022:15 Pages 913—918
DOI https://doi.org/10.2147/OTT.S378353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Yan Zhang, Danrong Wu, Ruoqiu Wang, Min Luo, Dong Wang, Kaiyue Wang, Yi Ai, Li Zheng, Qiao Zhang, Lixin Shi
Department of Endocrinology and Metabolism, Guiqian International General Hospital, Guiyang, People’s Republic of China
Correspondence: Qiao Zhang; Lixin Shi, Department of Endocrinology and Metabolism, Guiqian International General Hospital, Guiyang, People’s Republic of China, Tel/Fax +86 851-86277666, Email [email protected]; [email protected]
Abstract: Ectopic pituitary adenoma (EPA) is a pituitary adenoma unrelated to the intrasellar component and is an extremely rare disease. EPA resembles typical pituitary adenomas in morphology, immunohistochemistry, and hormonal activity, and it may present with specific or non-specific endocrine manifestations. Here, we report a rare case of ectopic adrenocorticotropic hormone (ACTH)-secreting pituitary adenoma in the clival region. Only three patients with ACTH-secreting pituitary adenomas occurring in the clivus have been previously reported, and the present case was diagnosed as a clivus-ectopic ACTH-secreting pituitary macroadenoma. Thus, in addition to the more common organs, such as the lung, thymus, and pancreas, in the diagnosis of ectopic ACTH syndrome, special attention should be paid to the extremely rare ectopic ACTH-secreting pituitary adenoma of the clivus region.
Keywords: ectopic pituitary adenoma, Cushing’s syndrome, clivus, adrenocorticotropic hormone, endocrine
Introduction
The diagnosis of Cushing’s syndrome (CS), particularly its localization diagnosis, has always been a challenge in clinical practice.1,2 Endogenous CS can be divided into adrenocorticotropic hormone (ACTH)-dependent and non-ACTH dependent with the former accounting for 70% of CS cases. Ectopic ACTH syndrome accounts for 5–10% of CS cases, and its lesions are mainly located in the lungs, thymus, pancreas, and the thyroid gland.3 Finding such lesions in non-pituitary intracranial regions is extremely rare, and ectopic ACTH in the clivus region is even rarer. To date, less than 60 cases of ectopic ACTH-secreting pituitary adenomas have been reported,4 and determining their localization is a formidable challenge in CS diagnosis. It is difficult to make an accurate and prompt diagnosis of ectopic ACTH-secreting pituitary adenoma caused by hypercortisolism based on its clinical manifestation, routine laboratory tests, and radiologic examinations.1,4 Ectopic pituitary adenomas (EPAs) are mainly concentrated in the sphenoid sinus, suprasellar region, and cavernous sinus, and rare regions include the clivus, ethmoid sinus, and nasal cavity.5 A literature review showed that only three cases of primary EPA in the clivus region have been reported worldwide.6–8 Recently, we diagnosed a patient with ectopic ACTH-secreting pituitary macroadenoma in the clivus region that was confirmed by surgery and immunohistochemistry.
Case Presentation
A 53-year-old female patient sought medical attention at our hospital for hypertension, headache, and dizziness with a blood pressure as high as 180/100 mmHg. Her medical history showed that she had developed similar symptoms 2 years ago. At that time, she had hypertension (180/100 mmHg), headache, and dizziness, and she was treated with amlodipine (5 mg per day), benazepril hydrochloride (10 mg per day), and metoprolol tartrate (50 mg per day). The patient was not hospitalized for treatment and did not undergo systemic examination. Three months before admission, the patient had a thoracic vertebrae fracture caused by moving heavy objects. One month before admission, she had a bilateral rib fracture due to falling on flat ground. Her physical examination results were as follows: blood pressure, 160/85 mmHg; height, 147 cm; weight, 55.2 kg; and body mass index (BMI), 25.54 kg/m2. In the physical examination, moon facies, buffalo hump, concentric obesity, facial plethora, and large patches of ecchymosis at the blood sampling site were observed. Purple striae were absent below the axilla, abdomen, and limbs. Her hematological examination results were as follows: cortisol (COR) rhythm with 33.52 µg/dL (reference range: 4.26–24.85) at 8:00 AM, 34.3 µg/dL at 4:00 PM, and 33.14 µg/dL at 12:00 AM; 1 mg dexamethasone overnight suppression test indicated 22.21 µg/dL COR at 8:00 AM; 24 h urine COR was 962.16 µg/24 h (reference range: 50–437 µg/24 h); 8:00 AM ACTH at two different times was 74 pg/mL and 90.8 pg/mL (reference range: <46); high-dose dexamethasone suppression test (HDDST) was 21.44 µg/dL COR (serum COR level was not suppressed by more than 50%); serum potassium was 3.38 mmol/L (reference range: 3.5–5.5); insulin-like growth factor-1 (IGF-1) was 106.6 ng/mL (reference range: 84–236); serum luteinizing hormone (LH) was <0.07 IU/L (reference range: 1.9–12.5); serum follicle stimulating hormone (FSH) was 0.37 IU/L (reference range: 2.5–10.2); prolactin (PRL), testosterone, progesterone, and estradiol test results were normal; FT4 was 8.25 pmol/L (reference range: 10.44–24.38); TSH was 1.116 mIU/L (reference range: 0.55–4.78); oral glucose tolerance test (OGTT) indicated that fasting blood glucose was 6.3 mmol/L and 2-h blood glucose was 18.72 mmol/L; and glycated hemoglobin (HbA1c) was 7.1%. A bone mineral density test suggested osteoporosis (dual energy X-rays: L1-L4 T values were −3.4).
Magnetic resonance (MR) scans were performed using a SIGNA Pioneer 3.0T (GE Healthcare, Waukesha, WI, USA), and computed tomography (CT) scans were performed using a 256 slice CT scanner (Revolution CT; GE Healthcare, Waukesha, WI, USA). The enhanced MR scan of the sellar lesion showed a soft tissue mass with abnormal signals in the occipital bone clivus. T1WI showed an isointense signal, and T2WI showed an isointense/slightly hyperintense signal in a large area of approximately 30 mm × 46 mm. The lesion extended anteriorly to completely fill the entire sphenoidal sinus, and it was in a close proximity to the right internal carotid arteries. Significant invasion, liquefaction, and necrosis were not observed in the bilateral cavernous sinuses. Pituitary gland morphology was normal with a superoinferior diameter of 3.14 mm, and the pituitary gland was located in the center. An occipital bone clival space-occupying lesion was considered with a tendency of low malignancy and a possibility of chordoma (Figure 1A–C). Non-enhanced high-resolution CT scans of the nasal sinuses showed osteolytic destruction, and a soft tissue mass was observed in the occipital bone clivus. The mass had a large area of 20 mm × 30 mm × 46 mm (Figure 1D). Enhanced CT of the adrenals showed bilateral adrenal gland hyperplasia.
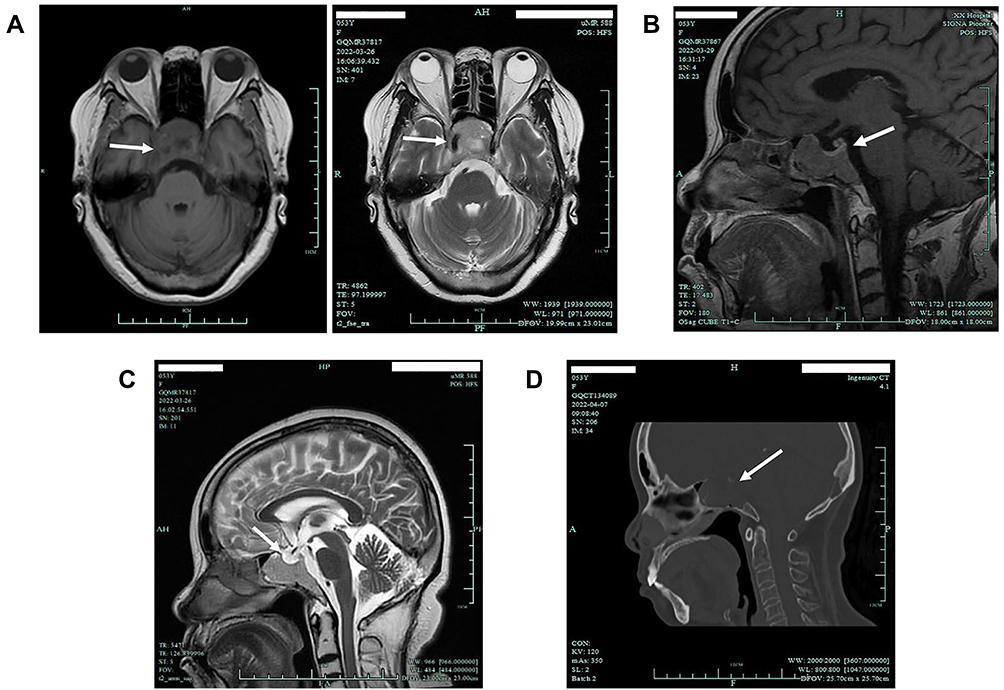 |
Figure 1 (A) MR T1+T2 scan (transverse view). MR T1 scan (left) shows the soft tissue mass of the occipital clivus (white arrow), and MR T2 scan (right) shows that the right internal carotid artery, cavernous sinus, and tumor are within close proximity to each other (white arrow). (B) MR T1 enhanced scan (sagittal view) shows clear demarcation between normal pituitary gland and mass (white arrow). (C) MR T2 scan (sagittal view) shows that the pituitary fossa is normally present (white arrow). (D) CT (sagittal view) shows bony destruction of dorsum sellae, clivus, and sphenoid sinus by mass (white arrow). |
Bilateral inferior petrosal sinus sampling (IPSS) combined with a desmopressin stimulation test had the following results: baseline ACTH at left inferior petrosal sinus/periphery (IPS/P), 5.4; post-stimulation IPS/P, 3.42; stimulation corrected (ACTHPRL) IPS/P, 2.8; right baseline IPS/P, 1.64; post-stimulation IPS/P, 9.34; and stimulation corrected IPS/P, 6.92. The left inferior petrosal sinus was the dominant side (Table 1).
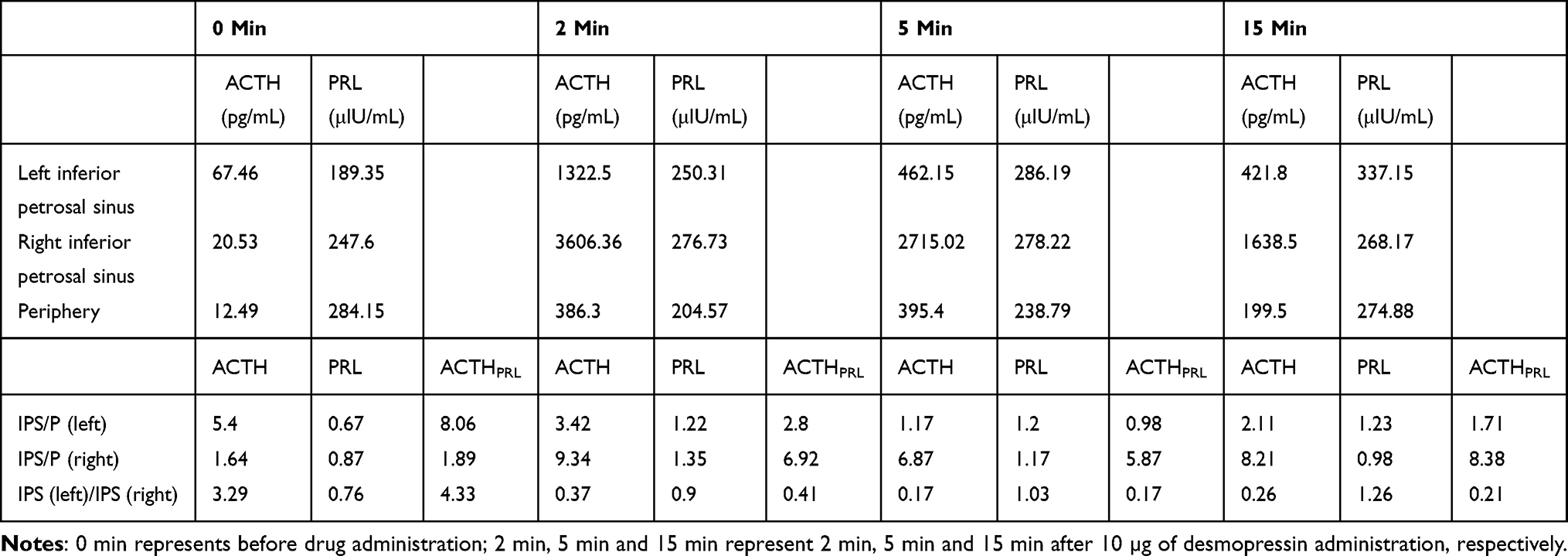 |
Table 1 Bilateral Inferior Petrosal Sinus Sampling Combined with Desmopressin Stimulation Test |
The patient underwent endoscopic transsphenoidal clival lesion resection surgery, and the postoperative pathology test results showed EPA (Figure 2). The immunohistochemistry staining results were as follows: CK (+), SYN (+), CgA (+), ACTH (+), growth hormone (GH) (−), LH (−), TSH (−), PRL (−), FSH (−), and Ki-67 (<1% +). The COR level at 10 days after surgery was 15.87 µg/dL, and the ACTH level was 31.37 pg/mL (Table 2).
 |
Table 2 Changes in COR and ACTH Levels During Course of Treatment |
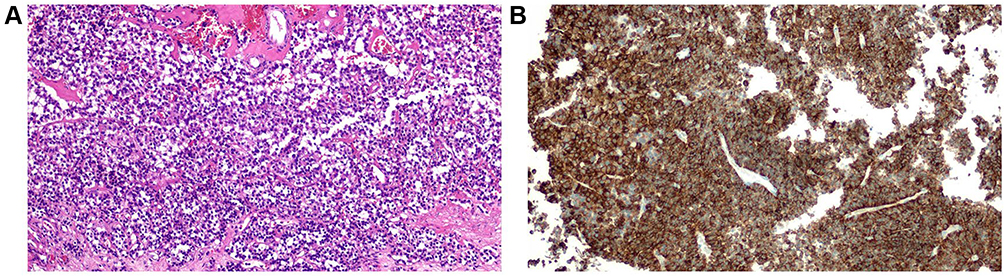 |
Figure 2 Pathological diagnosis of (clivus) ectopic pituitary adenoma. (A) Pituitary adenoma revealing a trabecular and nested structure revealing vascular invasion (hematoxylin and eosin (HE) stain, 200x) composed of two distinct types of cells. (B) ACTH expression in the EPA (200x, ACTH-antibody, Dako). |
After admission, her blood and urine COR levels were significantly elevated, and a qualitative diagnosis of CS was obtained. Etiological examination found that ACTH was also significantly elevated, suggesting that the CS was ACTH dependent. The HDDST results showed that the serum COR level was not suppressed by more than 50% and was accompanied by hypokalemia, suggesting that the ACTH-dependent CS may be ectopic ACTH syndrome. Ectopic ACTH syndrome is relatively rare, and the lesions are caused by non-pituitary tumors. No lesions were identified in the lung, thymus, pancreas, and thyroid of our patient. Regarding the IPSS examination, the IPS/P ratio was greater than 2, which suggested that the ectopic ACTH was located intracranially and not at the periphery. Radiologic testing suggested that the pituitary structure was normal and that a space-occupying lesion in the clivus region was present. Therefore, ectopic ACTH-secreting adenoma in the clivus region was considered, and postoperative pathological biopsy was used to confirm the diagnosis.
Discussion
EPA is an extremely rare disease that occurs outside of the sella turcica, and it is not linked to the intrasellar pituitary. The morphology, immunohistochemistry, and hormone activity of EPAs are similar to typical pituitary adenomas. EPAs can manifest as specific or non-specific endocrine disorders, and they account for 0.48% of all pituitary adenomas.9 The pathogenesis of EPA is still currently unknown. It is generally considered that during the development of the anterior pituitary lobe, the incompletely degraded Rathke cleft cyst remnants of the Rathke pouch lead to the formation of EPAs in the nasopharynx, sphenoid, and clivus.10,11 EPA is rare in China. Zhu et al5 recorded 14,357 pituitary gland patients in the last 20 years; of these patients, only 14 were diagnosed with EPA (0.098% of all cases), but none of the lesions originated from the clivus region. Previous literature reviews4,5 revealed that non-functioning EPAs in the clivus region are the most common (50%); the most common hormone-secreting functional adenomas are PRL adenomas and GH adenomas, which account for 25.0% and 21.4% of EPAs, respectively, whereas ACTH-secreting EPAs are extremely rare and only account for 3.6% of cases.
The postoperative pathological and immunohistochemical results of the tumor tissue in the patient demonstrated that it was an ectopic ACTH-secreting pituitary macroadenoma in the clivus region. Most EPAs are microadenomas (diameter <1 cm), except those in the clivus region, which are macroadenomas.5 Adenoma size generally does not affect the patient’s clinical and biochemical characteristics, and it may be related to tumor location or extension.12 Encasement of the internal carotid artery is a characteristic feature of EPA invasion into surrounding tissues.5 Encasement of the right internal carotid artery by the tumor was also observed in our patient. Therefore, surgery cannot completely remove the tumor and may ultimately affect surgical outcomes, and radiotherapy may even be required in the future. The serum COR and ACTH levels of our patient were evaluated 10 days after surgery. Although the levels were significantly lower than those before the surgery, the COR level was still significantly higher than the cutoff value of 1 µg/dL,13,14 suggesting that the patient may not have complete remission due to the incomplete tumor resection in the area adjacent to the carotid artery during surgery. Another feature that was observed in our patient was bone invasion. Because the clivus is composed of abundant cancellous bone that is connected to surrounding bone structures, EPAs or other tumors may cause bone destruction and affect the sphenoidal sinus and cavernous sinus, which is also consistent with literature reports.15,16
Due to the low incidence of EPAs, most EPA cases are reported as case reports in the literature. We performed an English literature search using the PubMed and Web of Science Core Collection databases with the following predetermined terms: “Cushing’s syndrome”, “pituitary adenomas”, “clivus”, “ectopic pituitary adenoma”, and “adrenocorticotropic”. The literature was included if it met the following criteria: (i) the confirmed diagnosis of CS or ectopic ACTH syndrome was described in the literature; (ii) the diagnosis of EPA was confirmed by postoperative inspection; and (iii) EPA occurred in the clivus. After excluding cases of clival invasion from other sites, we found only three reports of ectopic ACTH-secreting adenoma in the clivus region,6–8 and they were all female patients. Ortiz-Suarez and Erickson6 employed transfrontal craniotomy to demonstrate that the ectopic ACTH-secreting adenoma was an extension of extrasellar lesion to the clivus. In a case report by Pluta et al,7 the patient was found to have cavernous sinus and clival ACTH-positive tumors through transphenoidal surgery. In a case report by Aftab et al,8 the patient only presented a space-occupying lesion with unilateral vision loss; the patient was initially diagnosed with clival chordoma, but the postoperative results supported the diagnosis of EPA. Based on preoperative imaging, the possibility of chordoma was also considered to be high in our patient. We combined the clinical manifestation and laboratory test results of the patient and considered the etiology of CS to conclude that the patient had clival ectopic ACTH-secreting adenoma instead of chordoma.
Hormone tests in our patient suggested secondary pituitary-gonadal axis and decreased pituitary-thyroid axis function. These changes in endocrine function may be due to pituitary suppression by hypercortisolism. After surgery, the corresponding markers recovered, indicating that the suppression was transient. The patient has a history of fracture and a bone mineral density suggestive of osteoporosis, which may also be associated with CS hypercortisolemia.
Treatment modalities for EPA include adenoma resection surgery, radiotherapy, and drugs. The first-line recommended treatment is surgical resection. Craniotomy is considered the surgical procedure of choice for EPA, and endoscopic transsphenoidal surgery (TSS) is considered a feasible method for preserving pituitary function while simultaneously treating EPA. However, due to limitations with the surgical operation space, there are still concerns whether sufficient exploration and effective tumor resection can be achieved.17 Because there are few case reports of such patients, the long-term outcomes of these two surgical procedures require further validation. Due to differences in EPA sites and functions, the efficacy of surgery also differs. Zhu et al5 reported that compared to the radical resection rate of sphenoidal sinus and cavernous sinus EPA (72.3% and 73.3%, respectively), the radical resection rate of clival EPA is only 45.0%, and this difference is statistically significant.
The three clival EPA patients described in the three relevant publications6–8 all showed significant improvements in postoperative signs, symptoms, and hormone levels after complete surgical removal of the lesions or combined with radiation therapy. In our patient, however, radical resection of the tumor could not be achieved due to the close proximity of the tumor mass to the right internal carotid artery, and surgery could not be used to achieve complete remission, which is similar to the case reported by Zhu et al.5 For such patients, radiotherapy can be considered as a second-line treatment for EPA. To control hormone levels, drugs and bilateral adrenalectomy are also treatment options.5,18,19
Conclusion
EPA is a rare disease, and clival EPA is even rarer. From the entire diagnosis and treatment course, this unique and rare EPA case was preliminarily diagnosed through a comprehensive hormone panel and IPSS, and it was confirmed by pathology and immunohistochemistry after surgery. In the diagnosis of ectopic ACTH syndrome, attention should also be paid to extremely rare pituitary ectopic sites, such as the sphenoid sinuses, parasellar region, and the clivus, in addition to common sites, such as the lungs, thymus, pancreas, and thyroid.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Informed Consent Statement
Prior written permission was obtained from the patient for treatment as well as for the preparation of this manuscript and for publication. Our institution approved the publication of the case details.
Acknowledgments
We would like to thank the patient and her family.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Senanayake R, Gillett D, MacFarlane J, et al. New types of localization methods for adrenocorticotropic hormone-dependent Cushing’s syndrome. Best Pract Res Clin Endocrinol Metab. 2021;35:101513. doi:10.1016/j.beem.2021.101513
2. Young J, Haissaguerre M, Viera-Pinto O, et al. Management of Endocrine Disease: cushing’s syndrome due to ectopic ACTH secretion: an expert operational opinion. Eur J Endocrinol. 2020;182:R29–r58. doi:10.1530/EJE-19-0877
3. Hayes AR, Grossman AB. The ectopic adrenocorticotropic hormone syndrome: rarely easy, always challenging. Endocrinol Metab Clin North Am. 2018;47:409–425. doi:10.1016/j.ecl.2018.01.005
4. Zhu J, Lu L, Yao Y, et al. Long-term follow-up for ectopic ACTH-secreting pituitary adenoma in a single tertiary medical center and a literature review. Pituitary. 2020;23:149–159. doi:10.1007/s11102-019-01017-y
5. Zhu J, Wang Z, Zhang Y, et al. Ectopic pituitary adenomas: clinical features, diagnostic challenges and management. Pituitary. 2020;23:648–664. doi:10.1007/s11102-020-01071-x
6. Ortiz-Suarez H, Erickson DL. Pituitary adenomas of adolescents. J Neurosurg. 1975;43:437–439. doi:10.3171/jns.1975.43.4.0437
7. Pluta RM, Nieman L, Doppman JL, et al. Extrapituitary parasellar microadenoma in Cushing’s disease. J Clin Endocrinol Metab. 1999;84:2912–2923. doi:10.1210/jcem.84.8.5890
8. Aftab HB, Gunay C, Dermesropian R, et al. “An Unexpected Pit” - ectopic pituitary adenoma. J Endocr Soc. 2021;5:A557–A558. doi:10.1210/jendso/bvab048.1137
9. Li X, Zhao B, Hou B, et al. Case report and literature review: ectopic thyrotropin-secreting pituitary adenoma in the suprasellar region. Front Endocrinol. 2021;12:619161. doi:10.3389/fendo.2021.619161
10. Agely A, Okromelidze L, Vilanilam GK, et al. Ectopic pituitary adenomas: common presentations of a rare entity. Pituitary. 2019;22:339–343. doi:10.1007/s11102-019-00954-y
11. Tajudeen BA, Kuan EC, Adappa ND, et al. Ectopic pituitary adenomas presenting as sphenoid or clival lesions: case series and management recommendations. J Neurol Surg B Skull Base. 2017;78:120–124. doi:10.1055/s-0036-1592081
12. Akirov A, Shimon I, Fleseriu M, et al. Clinical study and systematic review of pituitary microadenomas vs. macroadenomas in cushing’s disease: does size matter? J Clin Med. 2022;11:1558. doi:10.3390/jcm11061558
13. Badiu C. Williams textbook of endocrinology. Acta Endocrinologica. 2019;15:416. doi:10.4183/aeb.2019.416
14. Rollin GA, Ferreira NP, Junges M, et al. Dynamics of serum cortisol levels after transsphenoidal surgery in a cohort of patients with Cushing’s disease. J Clin Endocrinol Metab. 2004;89:1131–1139. doi:10.1210/jc.2003-031170
15. Hu S, Cheng S, Wu Y, et al. A large cavernous sinus giant cell tumor invading clivus and sphenoid sinus masquerading as meningioma: a case report and literature review. Front Surg. 2022;9:861739. doi:10.3389/fsurg.2022.861739
16. Wu X, Ding H, Yang L, et al. Invasive corridor of clivus extension in pituitary adenoma: bony anatomic consideration, surgical outcome and technical nuances. Front Oncol. 2021;11:689943. doi:10.3389/fonc.2021.689943
17. Sun X, Lu L, Feng M, et al. Cushing syndrome caused by ectopic adrenocorticotropic hormone-secreting pituitary adenomas: case report and literature review. World Neurosurg. 2020;142:75–86. doi:10.1016/j.wneu.2020.06.138
18. Szabo Yamashita T, Sada A, Bancos I, et al. Differences in outcomes of bilateral adrenalectomy in patients with ectopic ACTH producing tumor of known and unknown origin. Am J Surg. 2021;221:460–464. doi:10.1016/j.amjsurg.2020.08.047
19. Szabo Yamashita T, Sada A, Bancos I, et al. Bilateral adrenalectomy: differences between cushing disease and Ectopic ACTH-producing tumors. Ann Surg Oncol. 2020;27:3851–3857. doi:10.1245/s10434-020-08451-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.