")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Economic Evaluation of Umeclidinium/Vilanterol versus Umeclidinium or Salmeterol in Symptomatic Non-Exacerbating Patients with COPD from a UK Perspective Using the GALAXY Model
Authors Shukla S , Shah D, Martin A , Risebrough NA, Kendall R , Vogelmeier CF, Boucot I , Tombs L, Bjermer L , Jones PW , Kerwin E , Compton C, Maltais F , Lipson DA , Ismaila AS
Received 29 July 2021
Accepted for publication 25 October 2021
Published 13 November 2021 Volume 2021:16 Pages 3105—3118
DOI https://doi.org/10.2147/COPD.S331636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Soham Shukla,1 Dhvani Shah,2 Alan Martin,3 Nancy A Risebrough,4 Robyn Kendall,5 Claus F Vogelmeier,6 Isabelle Boucot,3 Lee Tombs,7 Leif Bjermer,8 Paul W Jones,3 Edward Kerwin,9 Chris Compton,3 François Maltais,10 David A Lipson,11,12 Afisi S Ismaila1,13
1Value Evidence and Outcomes, GSK, Collegeville, PA, USA; 2ICON, New York, NY, USA; 3Value Evidence and Outcomes, GSK, Brentford, Middlesex, UK; 4Global Health Economics, and Outcomes Research and Epidemiology, ICON, Toronto, ON, Canada; 5Global Health Economics, and Outcomes Research and Epidemiology, ICON, Vancouver, BC, Canada; 6Department of Medicine, Pulmonary and Critical Care Medicine, University Medical Center Giessen and Marburg, Philipps-Universität Marburg, Member of the German Center for Lung Research (DZL), Marburg, Germany; 7Precise Approach Ltd, Contingent Worker on Assignment at GSK, Brentford, Middlesex, UK; 8Respiratory Medicine and Allergology, Lund University, Lund, Sweden; 9Altitude Clinical Consulting and Clinical Research Institute of Southern Oregon, Medford, OR, USA; 10Centre de Pneumologie, Institut universitaire de cardiologie et de pneumologie de Québec, Université Laval, Québec, QC, Canada; 11Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 12Respiratory Clinical Sciences, GSK, Collegeville, PA, USA; 13Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada
Correspondence: Afisi S Ismaila
Value Evidence and Outcomes, GlaxoSmithKline
1250 South Collegeville Road, Collegeville, PA, 19426-0989, USA
Tel +1 919 315 8229
Email [email protected]
Introduction: Dual bronchodilators are recommended as maintenance treatment for patients with symptomatic COPD in the UK; further evidence is needed to evaluate cost-effectiveness versus monotherapy. Cost-effectiveness of umeclidinium/vilanterol versus umeclidinium and salmeterol from a UK healthcare perspective in patients without exacerbations in the previous year was assessed using post hoc EMAX trial data.
Methods: The validated GALAXY model was populated with baseline characteristics and treatment effects from the non-exacerbating subgroup of the symptomatic EMAX population (COPD assessment test score ≥ 10) and 2020 UK healthcare and drug costs. Outputs included estimated exacerbation rates, costs, life-years (LYs), and quality-adjusted LYs (QALYs); incremental cost-effectiveness ratio (ICER) was calculated as incremental cost/QALY gained. The base case (probabilistic model) used a 10-year time horizon, assumed no treatment discontinuation, and discounted future costs and QALYs by 3.5% annually. Sensitivity and scenario analyses assessed robustness of model results.
Results: Umeclidinium/vilanterol treatment was dominant versus umeclidinium and salmeterol, providing an additional 0.090 LYs (95% range: 0.035, 0.158) and 0.055 QALYs (− 0.059, 0.168) with total cost savings of £ 690 (£ 231, £ 1306) versus umeclidinium, and 0.174 LYs (0.076, 0.286) and 0.204 QALYs (0.079, 0.326) with savings of £ 1336 (£ 1006, £ 2032) versus salmeterol. In scenario and sensitivity analyses, umeclidinium/vilanterol was dominant versus umeclidinium except over a 5-year time horizon (more QALYs at higher total cost; ICER=£ 4/QALY gained) and at the lowest estimate of the St George’s Respiratory Questionnaire treatment effect (fewer QALYs at lower total cost; ICER=£ 12,284/QALY gained); umeclidinium/vilanterol was consistently dominant versus salmeterol. At willingness-to-pay threshold of £ 20,000/QALY, probability that umeclidinium/vilanterol was cost-effective in this non-exacerbating subgroup was 95% versus umeclidinium and 100% versus salmeterol.
Conclusion: Based on model predictions from a UK perspective, symptomatic patients with COPD and no exacerbations in the prior year receiving umeclidinium/vilanterol are expected to have better outcomes at lower costs versus umeclidinium and salmeterol.
Keywords: COPD treatment, cost-effectiveness, umeclidinium, salmeterol, umeclidinium/vilanterol
Plain Language Summary
Treatment of patients with chronic obstructive pulmonary disease (COPD) is expensive and uses extensive healthcare resources. UK clinical guidelines recommend a combination of two types of long-term bronchodilator medications for many patients with COPD. More evidence is needed to show that this is more cost-effective than treatment with one bronchodilator. We analyzed data from the 6-month EMAX clinical trial in patients who were not using a steroid inhaler. EMAX compared the benefits of two bronchodilators combined in a single inhaler, umeclidinium and vilanterol, with a single bronchodilator (either umeclidinium or salmeterol). We evaluated which treatment was likely to be more cost-effective over 10 years using a validated risk equation model, which predicts how patients with COPD respond to different treatments over time. We looked at patients who did not have any exacerbations in the year before the EMAX trial. Bronchodilator medications are recommended for these patients, who are at lower risk of future exacerbations than patients who have had recent exacerbations. Our analysis predicted that patients treated with umeclidinium/vilanterol were likely to live longer and have better quality of life compared with umeclidinium or salmeterol alone. Even though umeclidinium/vilanterol is more expensive, it was predicted to reduce overall costs compared with umeclidinium or salmeterol by lowering healthcare costs such as hospitalizations. This suggests that treatment with two bronchodilators might provide better outcomes for patients with no exacerbations in the prior year, and reduce the overall costs of treatment compared with one bronchodilator. An infographic summary is shown in Figure 1.
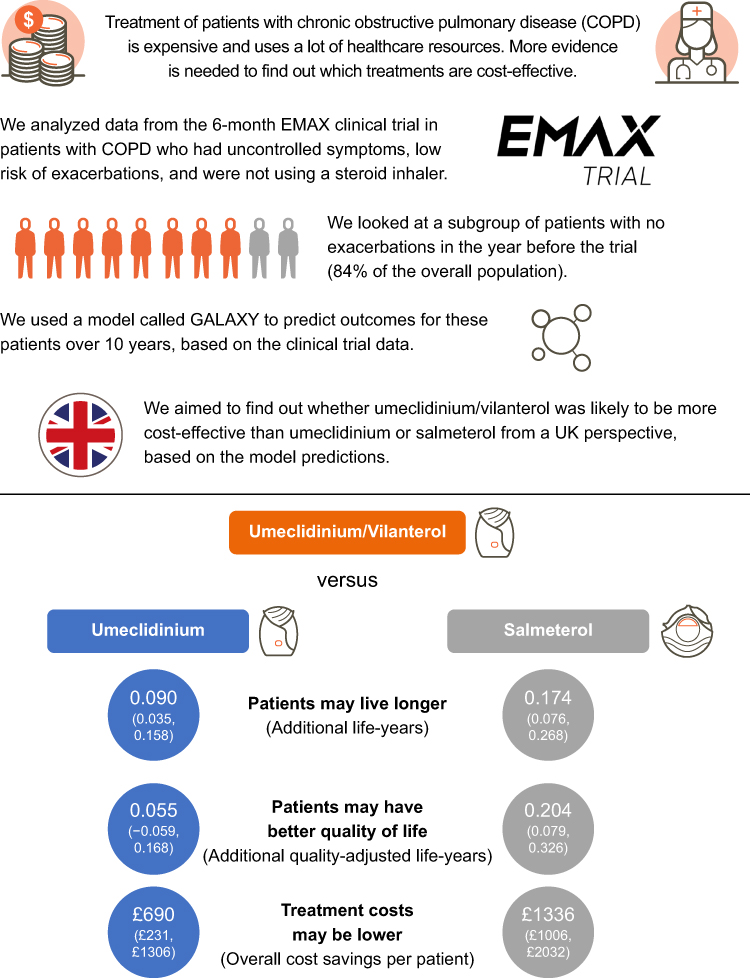 |
Figure 1 Infographic summary of the study background and base case results. |
Introduction
Patients with chronic obstructive pulmonary disease (COPD) experience significant morbidity and mortality, significant healthcare resource utilization (HRU), and high treatment costs.1–3 COPD is associated with a significant economic burden that persists despite the availability of effective maintenance treatment; in the UK, COPD was linked to total annual average societal costs exceeding $18,000 per patient in 2012–134 and total costs to the healthcare service of £1.9 billion in 2014.5
The American Thoracic Society recommends dual therapy with long-acting bronchodilators (long-acting muscarinic antagonist/long-acting β2-agonist [LAMA/LABA]) over LABA or LAMA monotherapy as initial maintenance therapy for all patients with COPD with dyspnea or exercise intolerance.6 Similarly, the UK National Institute of Health and Care Excellence (NICE) recommends LAMA/LABA as initial maintenance therapy for patients with COPD who have persistent symptoms or exacerbations despite short-acting bronchodilators and appropriate non-pharmacological management.7 Meta-analyses of clinical trial data have shown significantly better treatment outcomes for patients with COPD receiving dual long-acting bronchodilator therapy compared with monotherapy, with a similar safety profile.8,9 Consistent with this, the 24-week, multicenter, randomized, double-blind, double-dummy, parallel-group Early MAXimization of bronchodilation for improving COPD stability (EMAX) trial demonstrated improved lung function and symptoms in symptomatic patients with COPD at low risk of exacerbation not receiving inhaled corticosteroids (ICS) who received treatment with umeclidinium/vilanterol (UMEC/VI) compared with UMEC or salmeterol (SAL).10 These data suggest that dual bronchodilator therapy may be the optimal treatment for symptomatic patients with COPD who are at low risk for exacerbations. However, further evidence is needed to evaluate the cost-effectiveness of maintenance therapy with dual bronchodilators compared with monotherapy from a UK perspective.
This analysis used data from the EMAX trial10 and the existing validated GALAXY COPD model11–13 to assess the cost-effectiveness of UMEC/VI compared with UMEC and SAL from a UK healthcare perspective in patients without exacerbations in the previous 12 months. While patients with high baseline exacerbation risk may be expected to gain greater benefit from ICS-containing therapy,14 the subgroup with no exacerbations in the prior year was selected for this analysis because dual bronchodilator therapy is often recommended in symptomatic patients at low risk of future exacerbations,6,7,14 who represent almost one-third of patients with COPD who present for treatment.15 Furthermore, patients with no exacerbations in the prior year are at lower risk of future exacerbations than those with one exacerbation in the prior year,16 but many eventually experience moderate and severe exacerbations and mortality when long-term health outcomes are assessed up to 10 years.16,17 Therefore, it is of particular interest to demonstrate for payers the potential cost-effectiveness of dual bronchodilator treatment in patients who are not currently exacerbating.
Methods
Cost-Effectiveness Model
This analysis used the published and validated GALAXY COPD disease progression model.11–13 The GALAXY model was developed using data from a large patient cohort in the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study18,19 to quantify the relationships between disease parameters and clinical outcomes using linked risk equations.11,20 The model is populated with data on patient characteristics and treatment effects, and the risk equations predict changes in patients’ disease state over time, such as lung function decline, incidence of exacerbations, deterioration in symptoms, and exercise capacity. Based on these predicted disease states, treatment differences in health outcomes (survival and quality of life [QoL]) and costs can be predicted. A schematic of the GALAXY model has been published previously11,21 and is shown in Supplementary Figure S1.
In this analysis, the GALAXY model was populated with patient characteristics and treatment effects from the EMAX trial and UK healthcare cost data.
Model Inputs
The model inputs are shown in Table 1. The design and findings of the EMAX trial have been published previously.10 The EMAX trial was conducted in accordance with the principles of the 1964 Declaration of Helsinki and its later amendments, and received appropriate ethical approval (Supplementary Table S1). Patients provided written informed consent at the Pre-screening or Screening visit.
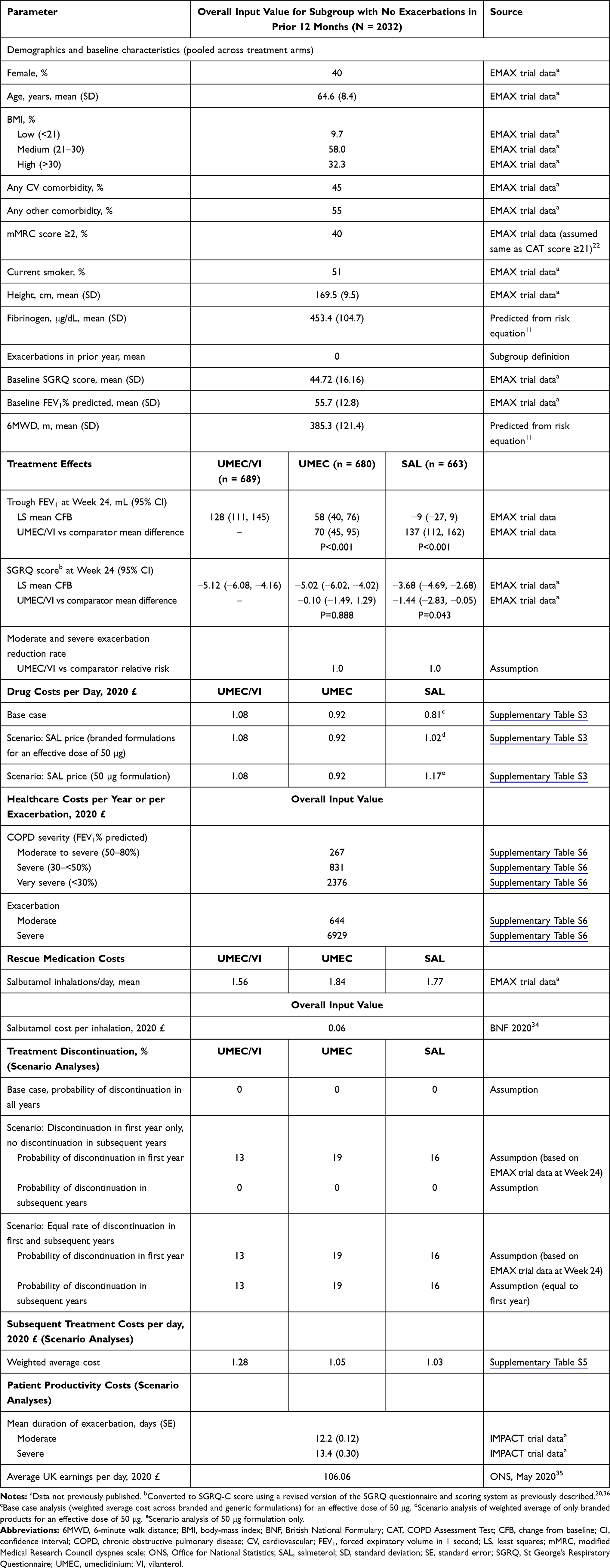 |
Table 1 Model Inputs |
Patient Population
Patients were eligible to participate in the EMAX trial if they had experienced ≤1 moderate and no severe COPD exacerbations in the year prior to the trial, had a pre- and post-salbutamol forced expiratory volume in 1 second (FEV1)/forced vital capacity ratio of <0.7, post-salbutamol FEV1 of ≥30 to ≤80% predicted, and had a COPD Assessment Test (CAT) score of ≥10; full eligibility criteria have been published previously.10 This analysis was performed using data from a post hoc analysis in the subgroup of patients without any exacerbations in the prior year, unless otherwise stated.
Baseline characteristics were similar across treatment arms (Supplementary Table S2), so pooled data across treatment arms was used to populate the model for each comparator. As such, all treatment groups had the same starting values for baseline characteristics.
The GALAXY model includes baseline values for some parameters that were not assessed in the EMAX trial, including modified Medical Research Council (mMRC) dyspnea scale, 6-minute walk distance (6MWD), and fibrinogen, so estimated values were used for these parameters. The proportion of patients with mMRC score ≥2 was assumed to be the same as the proportion of patients with CAT score ≥21, based on a previous evaluation of equivalence between these scales.22 Plasma fibrinogen and 6MWD values were predicted using a risk equation developed using data from ECLIPSE, as previously described.11,20,21
Treatment Effects
Treatment effects at 24 weeks for UMEC/VI versus each comparator (UMEC and SAL) in the subgroup of patients with no history of moderate exacerbations in the prior year were used in the model. Treatment effects beyond the end of the trial are unknown, so were assumed to continue until treatment discontinuation. Treatment effects are incorporated in the model as the incremental effect of UMEC/VI versus UMEC and SAL, as reference treatments, and so the predicted outcomes are the same for both UMEC and SAL. Because exacerbation rate was not an endpoint in the EMAX trial, relative rate reduction for exacerbations with UMEC/VI versus UMEC and SAL was set to 1 at the beginning of the modeling period (ie, it was assumed that there was no difference in the effect of treatment on exacerbation risk between treatment arms). This means that any reduction in exacerbations in later model cycles was due to the linked effects of improvements in lung function and reduced symptoms.
Since improvement in FEV1 is a predictor of other effects in the model, including St George’s Respiratory Questionnaire (SGRQ), the magnitude of these treatment effects was adjusted to avoid double-counting or under-prediction. The FEV1 treatment effect was entered into the model first, followed by SGRQ treatment effects.
Discontinuation was not included in the base case because the EMAX trial protocol required that treatment was discontinued in patients experiencing >1 moderate or ≥1 severe exacerbation, making discontinuation rates difficult to interpret for economic analysis. In scenario analyses, discontinuation rates at Week 24 of the EMAX trial were used for the first year (since 1-year data were not available), and for subsequent years discontinuation rates were assumed to be either 0% or equal to the first year (Table 1).
Utilities
In each model cycle, annual model-predicted SGRQ scores were translated to EuroQol-5 Dimensions 3 Level (EQ-5D-3L) index scores using a published, validated algorithm.23
Costs
Drug costs were calculated based on dose, pack size, and cost per pack (Supplementary Table S3). For SAL, the cost per day in the base case was the weighted average across branded and generic formulations, based on UK market share (Supplementary Table S4).
Subsequent treatment costs were estimated (as no data on subsequent treatment was available from EMAX) and included in scenario analyses only. All patients who discontinued treatment were assumed to receive subsequent treatment with a specified medication class contingent upon the reason for discontinuation and original treatment (Supplementary Table S5). Efficacy of the treatment received after discontinuation was assumed to be the same as that of the original treatment (UMEC/VI, UMEC, or SAL) for the remaining duration of the analysis. Subsequent treatment costs were calculated based on the assumed treatment and published drug costs, weighted by UK market share for each medication class.
Healthcare costs were applied to health states and events (Supplementary Table S6). Based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification of airflow limitation severity,14 three health states were defined for costing purposes based on percent predicted FEV1: moderate to severe (50–<80%), severe (30–<50%), and very severe (<30%). The appropriate annual costs were applied according to predicted health state occupancy for each model cycle. Events included moderate and severe exacerbations, and were costed individually. Additional drug treatments for moderate exacerbations outside of physician encounters were included (Supplementary Table S7); the net cost was £9.14 per moderate exacerbation. Treatment costs for use of salbutamol as rescue medication were also included in the analysis.
Productivity costs (for scenario analysis) were calculated based on the mean duration of moderate and severe exacerbations in the IMPACT trial (assumed to be equal to the number of days absent from usual activities; IMPACT trial data, not previously published) and average UK earnings per day (Table 1).
Base Case Settings and Assumptions
For the base case analysis, a 10-year time horizon was used, and a 3.5% annual discount rate was applied for costs and benefits beyond the first year, in accordance with NICE methodological guidelines.24 It was assumed that the EMAX trial population was representative of the UK population with COPD who are likely to receive UMEC/VI, UMEC, or SAL; that treatment effects were persistent at a constant rate for all patients receiving UMEC/VI; and that there was no treatment discontinuation. Patient productivity costs were excluded.
Model Outputs
The model outputs were disaggregated direct costs (including COPD medications and non-drug costs), total direct costs, total moderate and severe exacerbations, the proportion of patients surviving, total life-years (LY) gained, and total quality-adjusted LYs (QALY) gained. Incremental cost-effectiveness ratios (ICER) were calculated as the ratio of incremental costs to incremental QALYs.
Scenario and Sensitivity Analyses
Scenario analyses were conducted to examine the impact of alternative model settings or assumptions. These included alternative time horizons (5 years and lifetime) and discount rates (0 and 5%), treatment discontinuation, alternative drug costs for SAL (weighted mean across branded products only, and costs for the 50 μg formulation only to align with the dose used in EMAX; Table 1), baseline characteristics and treatment effects from the EMAX intent-to-treat (ITT) population (Supplementary Table S8), and alternate health state and exacerbation event costs used in the economic evaluation of COPD maintenance treatments supporting the NICE guideline.25
One-way sensitivity analyses were conducted to test the robustness of the base case findings to alternate values for baseline covariate values that were not available in the EMAX data and for treatment effects. For the predicted fibrinogen and 6MWD values, corresponding data from ECLIPSE were used to approximate the 95% confidence interval (CI), and the upper and lower limits were used. For mMRC dyspnea score, it was not possible to approximate a 95% CI, so ±25% limits were used. Treatment effects were varied to the upper and lower limits of the 95% CI from the EMAX trial data.
Probabilistic analyses were conducted to address uncertainty in the input values, by assigning distributions to the input parameters and randomly sampling from these distributions over 5000 Monte Carlo simulations.
Results
Patient Population
Of the 2425 patients included in the EMAX ITT population,10 2032 (84%) had no exacerbations in the prior year. In the subgroup with no exacerbations in the prior year, the mean CAT score at screening was 19.3 and baseline patient characteristics were similar between treatment arms (Supplementary Table S2).
Base Case
Based on the model predictions over a 10-year time horizon, UMEC/VI was the dominant treatment versus UMEC, providing an additional 0.090 LYs (95% range: 0.035, 0.158) and 0.055 QALYs (95% range: −0.059, 0.168) (Table 2) in the subgroup of patients with no exacerbations in the prior year. Patients receiving UMEC/VI were predicted to have fewer total moderate and severe exacerbations (−0.023; 4% reduction) and severe exacerbations (−0.009; 8% reduction), and the proportion of patients surviving was 1.9% greater at the end of the time horizon, compared with those receiving UMEC. UMEC/VI provided overall cost savings of £690 (95% range: £231, £1306) per patient compared with UMEC; drug costs were higher for UMEC/VI (incremental difference: £416), but were offset by a larger reduction in non-drug costs, comprising exacerbation and maintenance costs (incremental difference: −£1106).
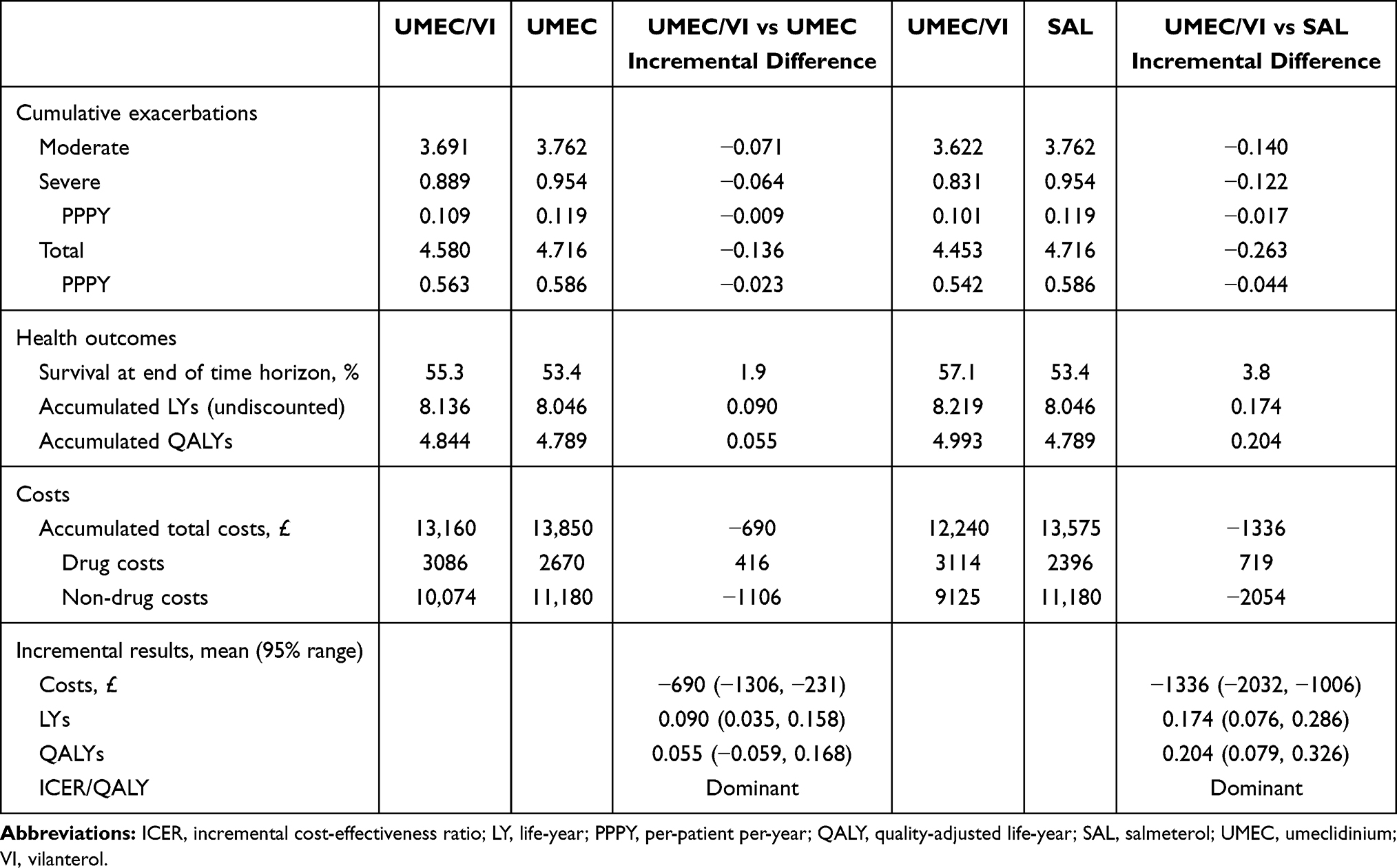 |
Table 2 Cumulative and Incremental Predicted Outcomes for UMEC/VI versus UMEC and SAL Over a 10-Year Horizon |
UMEC/VI was also the dominant treatment option versus SAL, with the model predicting an additional 0.174 LYs (95% range: 0.076, 0.286) and 0.204 QALYs (95% range: 0.079, 0.326) in the subgroup of patients with no exacerbations in the prior year (Table 2), fewer total moderate and severe exacerbations (−0.044; 8% reduction) and severe exacerbations (−0.017; 14% reduction), and a 3.8% increase in the proportion of patients surviving at the end of the time horizon. UMEC/VI provided overall cost savings of £1336 (95% range: £1006, £2032) per patient compared with SAL; drug costs were higher for UMEC/VI (incremental difference: £719), but were compensated by a larger reduction in exacerbation and maintenance costs (incremental difference: −£2054).
Scenario and Sensitivity Analyses
UMEC/VI was the dominant treatment option compared with UMEC and SAL across all scenario analyses (Table 3). The greatest cost savings with UMEC/VI were observed versus UMEC where patient productivity costs were included (−£853), and versus SAL where the cost of the 50 μg formulation was used (−£2252). A small incremental increase in costs was seen for UMEC/VI versus UMEC when the time horizon was reduced to 5 years resulting in an ICER of £4 per QALY. Results from scenarios where discontinuation was included were consistent with the base case versus both UMEC and SAL.
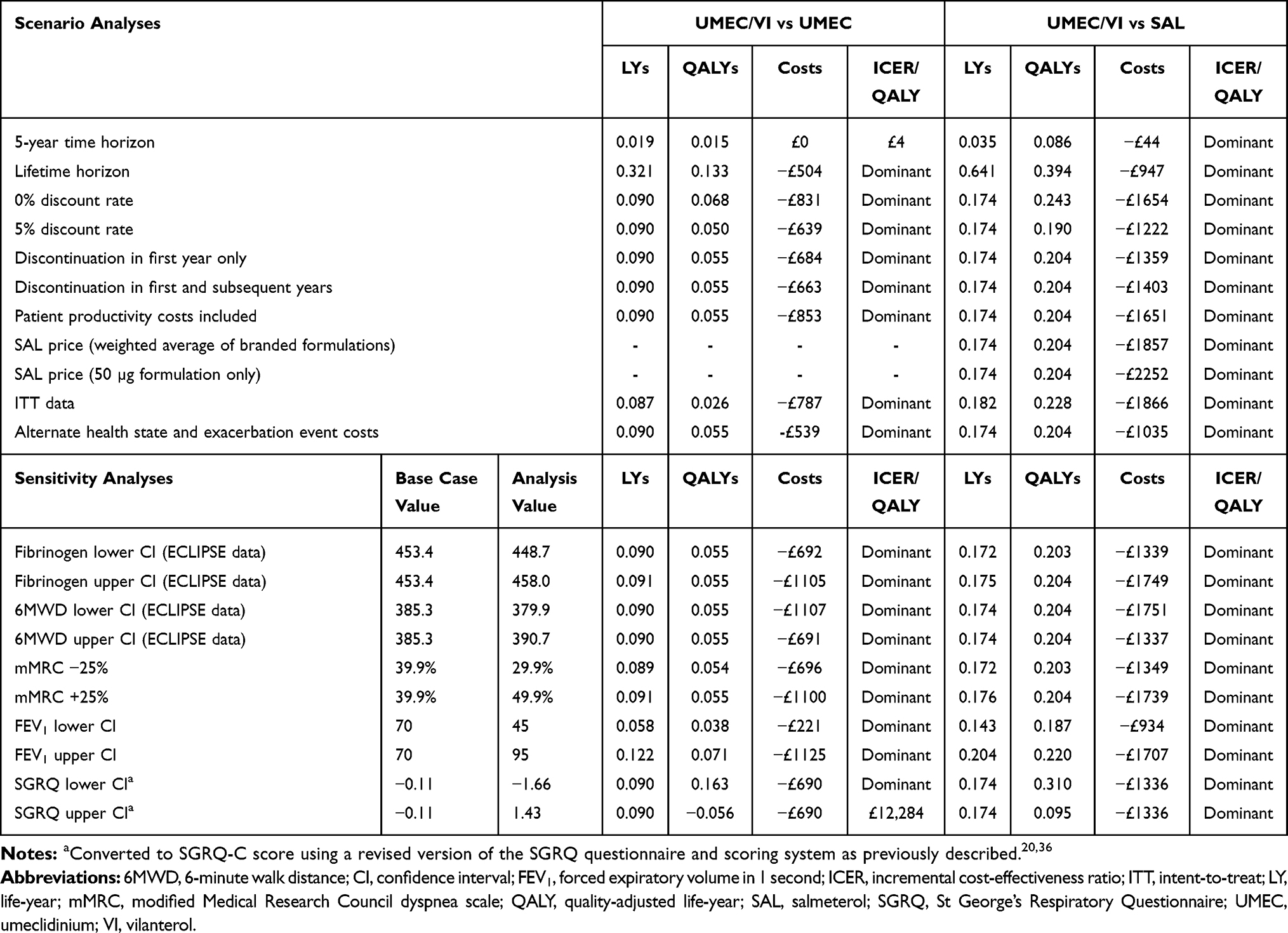 |
Table 3 Scenario and Sensitivity Analyses |
UMEC/VI was the dominant treatment option compared with SAL across all sensitivity analyses, and compared with UMEC for all but the sensitivity analysis using the upper CI of SGRQ treatment effect (ie, the lowest estimate of treatment effect on SGRQ with UMEC/VI vs UMEC) as the input value (Table 3). In that analysis, UMEC/VI showed fewer QALYs and lower costs versus UMEC, with an ICER of £12,284 per QALY.
In the probabilistic analyses, UMEC/VI was consistently less costly compared with UMEC across all iterations and showed higher QALYs in 82% of iterations (Figure 2A); compared with SAL, UMEC/VI was less costly and provided more QALYs in 99% of iterations (Figure 2B). At a willingness-to-pay threshold of £20,000 per QALY, the probability that UMEC/VI was cost-effective was 95% versus UMEC and 100% versus SAL (Figure 3A and B).
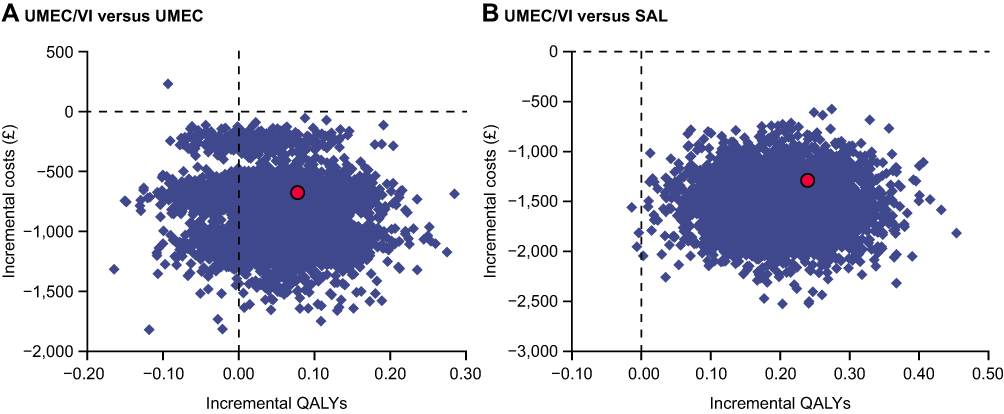 |
Figure 2 Probabilistic sensitivity analysis of incremental cost-effectiveness with (A) UMEC/VI versus UMEC and (B) UMEC/VI versus SAL, showing incremental differences between costs and QALYs between treatments over 5000 Monte Carlo simulations where distributions of input parameters were assigned and sampled randomly. Red circles indicate the base case results. Abbreviations: QALY, quality-adjusted life-year; SAL, salmeterol; UMEC, umeclidinium; VI, vilanterol. |
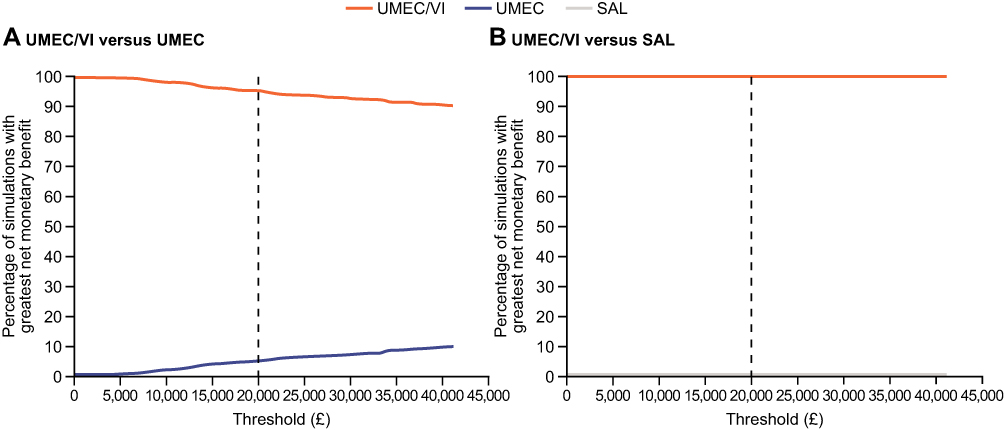 |
Figure 3 Net benefit acceptability curves for with (A) UMEC/VI versus UMEC and (B) UMEC/VI versus SAL, showing the relative probability of cost-effectiveness across the range of £0–45,000 per QALY for competing treatments included in the model. The dashed vertical line indicates the willingness-to-pay threshold at £20,000. Abbreviations: SAL, salmeterol; UMEC, umeclidinium; VI, vilanterol. |
Discussion
In this cost-effectiveness analysis from a UK perspective using the GALAXY model, UMEC/VI was the dominant treatment option (ie, provided more QALYs at a lower cost) compared with UMEC and SAL based on baseline characteristics and treatment effects from a subgroup of patients with no exacerbations in the prior year in the EMAX trial. Over a 10-year horizon, UMEC/VI was 95–100% more likely to be cost-effective versus UMEC or SAL at the accepted willingness-to-pay threshold of £20,000 per QALY. According to the model predictions, UMEC/VI improved survival and QoL for patients compared with monotherapy, as demonstrated by increases in LYs and QALYs. Although UMEC/VI was associated with higher drug costs than UMEC or SAL, these were offset by the larger reduction in non-drug exacerbation and maintenance costs, resulting in overall cost savings. A major contributor to these cost savings was the lower number of severe COPD exacerbations with UMEC/VI (predicted 8 and 14% reductions vs UMEC and SAL), as severe exacerbations are a high-cost event. Smaller proportions of patients in the severe and very severe COPD health states also substantially contributed to the cost savings with UMEC/VI.
The results of scenario and sensitivity analyses were consistent with the base case, indicating that the findings are robust despite uncertainties around the input values. For the base case, a 10-year time horizon was selected to represent a realistic estimate of the time frame over which this patient population would be expected to receive dual bronchodilator therapy prior to disease progression necessitating additional therapy. A lifetime horizon was not used because it was anticipated that patients will typically escalate to triple therapy in response to disease progression over the course of their lifetime. However, UMEC/VI was the dominant treatment option compared with both monotherapies in the scenario analysis over a lifetime horizon, suggesting that the predicted incremental benefits of UMEC/VI could be maintained beyond the 10-year horizon used for the base case. The ICER for UMEC/VI versus UMEC was sensitive to a shorter time horizon, although UMEC/VI remained cost-effective with a very small ICER of £4 per QALY. Scenario analyses including treatment discontinuation were also consistent with the base case, suggesting that discontinuation rates did not affect the cost-effectiveness of UMEC/VI. In the sensitivity analyses, changes in baseline values that were unavailable from the EMAX trial (fibrinogen, 6MWD, and mMRC score) had minimal effects on the results, suggesting that the use of predicted or analogous values did not introduce bias. In particular, variation in the mMRC dyspnea score, which was estimated based on equivalence with CAT scores, did not alter the outcome of the analysis, in line with a previous implementation of the GALAXY model that used the same approach.21 Most sensitivity analyses using alternative input values for treatment effects were in line with the base case findings, although UMEC/VI was less costly and less effective versus UMEC in the analysis using the upper CI bound of the SGRQ treatment effect (ie, the lowest estimate of treatment effect on SGRQ).
A subgroup of the EMAX trial population with no exacerbations in the year before the trial was chosen for the base case analysis. Baseline characteristics were similar in the ITT population and this non-exacerbating subgroup, which included the majority of the patients in the ITT population (84%). This subgroup was selected because bronchodilator therapy (LAMA, LABA, or LAMA/LABA) is typically recommended for patients currently at low risk of exacerbations. These patients are at lower risk of than patients who have had an exacerbation in the prior year but may nonetheless experience future exacerbations16,26,27 with a corresponding deterioration in lung function, health status, and the severity of symptoms.16,28 Patients who are not currently exacerbating therefore require effective treatment.7 The improvements in QoL and survival predicted for UMEC/VI versus UMEC and SAL in this study therefore provide further evidence to support the recommendation of dual bronchodilators as maintenance therapy for symptomatic patients with COPD at low risk of exacerbations.7 Furthermore, the model predictions indicate that there are likely to be overall cost savings for healthcare payers associated with early intensification of bronchodilator therapy prior to the onset of exacerbations, since the greater drug costs incurred by UMEC/VI were more than compensated by the overall reductions in non-drug costs compared with UMEC and SAL. An inherent prediction of this analysis is that a subset of the patient subgroup without exacerbations in the 12 months prior to the study will subsequently experience exacerbations within the time horizon of the cost-effectiveness analysis, since exacerbations are a disease status marker incorporated into the linked risk equations to predict outcomes. However, previously published findings suggest that this is likely to be the case; in an analysis of ECLIPSE data over 60% of patients in GOLD groups A and B, who had 0 or 1 exacerbation per year, experienced an exacerbation within the 3-year follow-up period.27
COPD is increasingly recognized as a heterogeneous and multifaceted disease, in which deteriorations in symptoms and QoL can occur in relation to a range of factors in addition to lung function decline.29–31 In contrast with other models of COPD disease progression, the GALAXY model incorporates relationships between a range of baseline characteristics, treatment effects, and outcomes, reflecting the multidimensional nature of COPD.12 This includes the impact of patient comorbidities, including both cardiovascular and other (non-cardiovascular) comorbidities, on outcomes.20 This relationship is important in cost-effectiveness analyses because comorbidities contribute to morbidity and mortality and are associated with increased healthcare costs for patients with COPD.32,33
The strengths of this study include a well-characterized patient population and the broad range of patient characteristics and treatment effects incorporated into the GALAXY model, maximizing the information based on which long-term disease progression was predicted. As is typical in this type of analysis, baseline characteristics were pooled across treatment arms to generate the input values for each treatment arm, such that all treatment arms had the same starting values; this approach prevents confounding due to baseline differences between treatment cohorts. A limitation of the EMAX trial design for this analysis was that patients were withdrawn from the trial if they experienced a severe exacerbation or >1 moderate exacerbation, which may reduce the applicability of the trial results to real-world clinical practice. In addition, 1-year discontinuation data were not available from EMAX, and so discontinuation was excluded from the base case; however, UMEC/VI remained dominant in scenario analyses that included discontinuation for the first year and/or subsequent years. Finally, it should be noted that the GALAXY model has been developed and validated in patients from the ECLIPSE study, who had an average of 0.9 exacerbations per patient in the prior year.19 This may limit its generalizability to the non-exacerbating subgroup included in this analysis, although similar findings were seen in a scenario analysis using data from the EMAX ITT population.
Conclusion
Based on the GALAXY model predictions from a UK National Health Service perspective, symptomatic patients with COPD and no exacerbations in the prior year who receive treatment with UMEC/VI are expected to have better outcomes (QALYs and survival) and lower overall healthcare costs compared with those receiving UMEC and SAL. These findings suggest that early intensification of bronchodilator therapy with UMEC/VI may reduce the economic burden of COPD compared with UMEC or SAL, providing overall cost savings for payers, and support the NICE recommendation for dual bronchodilators as initial maintenance therapy in symptomatic patients with COPD.
Abbreviations
6MWD, 6-minute walk distance; BMI, body mass index; BNF, British National Formulary; CAT, COPD assessment test; CFB, change from baseline; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; EQ-5D-3L, EuroQol-5 Dimensions-3 Level; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GP, general practitioner; HCP, healthcare provider; HRU, healthcare resource utilization; ICER, incremental cost-effectiveness ratio; ICS, inhaled corticosteroid; ICU, intensive care unit; ITT, intent-to-treat; LABA, long-acting ͎β2-agonist; LAMA, long-acting muscarinic antagonist; LS, least squares; LY, life-year; MDI, metered dose inhaler; MITT, multiple-inhaler triple therapy; MIMS, Monthly Index of Medical Specialities; mMRC, modified Medical Research Council; NA, not applicable; NICE, National Institute of Health and Care Excellence; ONS, Office for National Statistics; PPPY, per-patient per-year; QALY, quality-adjusted life-year; PSSRU, Personal Social Service Research Unit; QoL, quality of life; RP, respiratory practitioner; SAL, salmeterol; SD, standard deviation; SE, standard error; SGRQ, St George’s Respiratory Questionnaire; SITT, single-inhaler triple therapy; UMEC, umeclidinium; VIL, vilanterol.
Data Sharing Statement
Anonymized individual participant data and study documents can be requested for further research from www.clinicalstudydatarequest.com.
Ethics Approval and Informed Consent
The EMAX trial was performed according to the Declaration of Helsinki and received appropriate ethical approval (Supplementary Table S1). All patients provided written informed consent via a form signed at either the Pre-screening or Screening visit.
Acknowledgments
Editorial support (in the form of writing assistance including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing and referencing) was provided by Mark Condon, DPhil, and Maria Guillermina Casabona, PhD, of Fishawack Indicia Ltd, UK, part of Fishawack Health, and was funded by GSK. ELLIPTA and DISKUS are owned by/licensed to the GSK group of companies. An abstract based on this study was presented at the Virtual ISPOR 2021 congress as a poster presentation. The poster’s abstract was published in Value in Health 2021; 24:S214: https://doi.org/10.1016/j.jval.2021.04.1074.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The EMAX trial (GSK study number: 201749 [NCT03034915]) and this analysis (GSK study number 209845) were funded by GSK. GSK-affiliated authors had a role in study design, data analysis, data interpretation, and writing of the report and GSK funded the article processing charges and open access fee.
Disclosure
SS, AM, IB, CC, DAL, and ASI are GSK employees and hold shares and stocks in GSK. PWJ was a GSK employee at the time of the study and he is now a contingent worker on assignment at GSK, and holds shares and stocks in GSK. DS, NAR, and RK are ICON employees and hold shares and stocks in ICON. CFV has received grants from AstraZeneca, Boehringer Ingelheim, GSK, Grifols, and Novartis, and has received lecturing and personal fees from AstraZeneca, Boehringer Ingelheim, Berlin Chemie/Menarini, Chiesi, CSL Behring, GSK, Grifols, MedUpdate, Novartis, Aerogen and Nuvaira. LT is a contingent worker on assignment at GSK. LB has received honoraria for giving a lecture or attending an advisory board for Airsonett, ALK-Abelló, AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Meda, Novartis, and Teva. EK has served on advisory boards, speaker panels or received travel reimbursement for Amphastar, AstraZeneca, Boehringer Ingelheim, Chiesi, Connect Biopharma, GSK, Mylan, Novartis, Pearl, Sunovion, Teva, and Theravance, and has received consulting fees from Cipla and GSK. FM has received research grants for participating in multicenter trials for AstraZeneca, Boehringer Ingelheim, GSK, Sanofi, and Novartis, and has received unrestricted research grants and personal fees from Boehringer Ingelheim, Grifols, and Novartis. FM also reports financial participation in Oxynov, a company which is developing an oxygen delivery system. The authors report no other conflicts of interest in this work.
References
1. Ehteshami-Afshar S, FitzGerald JM, Doyle-Waters MM, Sadatsafavi M. The global economic burden of asthma and chronic obstructive pulmonary disease. Int J Tuberc Lung Dis. 2016;20(1):11–23. doi:10.5588/ijtld.15.0472
2. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of Chronic Obstructive Pulmonary Disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
3. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1204–1222.
4. Foo J, Landis SH, Maskell J, et al. Continuing to confront COPD international patient survey: economic impact of COPD in 12 countries. PLoS One. 2016;11(4):e0152618. doi:10.1371/journal.pone.0152618
5. British Lung Foundation. Estimating the economic burden of respiratory illness in the UK; 2017. Available from: https://cdn.shopify.com/s/files/1/0221/4446/files/PC-1601_-_Economic_burden_report_FINAL_8cdaba2a-589a-4a49-bd14-f45d66167795.pdf?1309501094450848169.
6. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
7. National Institute for Health and Care Excellence (NICE). Chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2018. Available from: https://www.nice.org.uk/guidance/ng115/resources/chronic-obstructive-pulmonary-disease-in-over-16s-diagnosis-and-management-pdf-66141600098245.
8. Oba Y, Sarva ST, Dias S. Efficacy and safety of long-acting beta-agonist/long-acting muscarinic antagonist combinations in COPD: a network meta-analysis. Thorax. 2016;71(1):15–25. doi:10.1136/thoraxjnl-2014-206732
9. Rodrigo GJ, Price D, Anzueto A, et al. LABA/LAMA combinations versus LAMA monotherapy or LABA/ICS in COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:907–922. doi:10.2147/COPD.S130482
10. Maltais F, Bjermer L, Kerwin EM, et al. Efficacy of umeclidinium/vilanterol versus umeclidinium and salmeterol monotherapies in symptomatic patients with COPD not receiving inhaled corticosteroids: the EMAX randomised trial. Respir Res. 2019;20(1):238. doi:10.1186/s12931-019-1193-9
11. Briggs AH, Baker T, Risebrough NA, et al. Development of the galaxy Chronic Obstructive Pulmonary Disease (COPD) model using data from ECLIPSE: internal validation of a linked-equations cohort model. Med Decis Making. 2017;37(4):469–480. doi:10.1177/0272989X16653118
12. Hoogendoorn M, Feenstra TL, Asukai Y, et al. External validation of health economic decision models for Chronic Obstructive Pulmonary Disease (COPD): report of the third COPD modeling meeting. Value Health. 2017;20(3):397–403. doi:10.1016/j.jval.2016.10.016
13. Risebrough NA, Briggs A, Baker TM, et al. Validating a model to predict disease progression outcomes in patients with COPD. Value Health. 2014;17(7):A560–561. doi:10.1016/j.jval.2014.08.1852
14. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Report; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
15. Gedebjerg A, Szépligeti SK, Wackerhausen L-MH, et al. Prediction of mortality in patients with chronic obstructive pulmonary disease with the new Global Initiative for Chronic Obstructive Lung Disease 2017 classification: a cohort study. Lancet Respir Med. 2018;6(3):204–212. doi:10.1016/S2213-2600(18)30002-X
16. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in Chronic Obstructive Pulmonary Disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
17. Rothnie KJ, Mullerova H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
18. Vestbo J, Anderson W, Coxson HO, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points (ECLIPSE). Eur Respir J. 2008;31(4):869–873. doi:10.1183/09031936.00111707
19. Agusti A, Calverley PM, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11(1):122. doi:10.1186/1465-9921-11-122
20. Exuzides A, Colby C, Briggs AH, et al. Statistical modeling of disease progression for chronic obstructive pulmonary disease using data from the ECLIPSE study. Med Decis Making. 2017;37(4):453–468. doi:10.1177/0272989X15610781
21. Ismaila AS, Risebrough N, Schroeder M, et al. Cost-effectiveness of once-daily single-inhaler triple therapy in COPD: the IMPACT trial. Int J Chron Obstruct Pulmon Dis. 2019;14:2681–2695. doi:10.2147/COPD.S216072
22. Jones PW, Adamek L, Nadeau G, Banik N. Comparisons of health status scores with MRC grades in COPD: implications for the GOLD 2011 classification. Eur Respir J. 2013;42(3):647–654. doi:10.1183/09031936.00125612
23. Starkie HJ, Briggs AH, Chambers MG, Jones P. Predicting EQ-5D values using the SGRQ. Value Health. 2011;14(2):354–360. doi:10.1016/j.jval.2010.09.011
24. National Institute for Health and Care Excellence (NICE). Guide to the methods of technology appraisal; 2013. Available from: https://www.nice.org.uk/process/pmg9/chapter/foreword.
25. National Institute for Health and Care Excellence (NICE). Chronic obstructive disease in over 16s: diagnosis and management [H] Economic model report; 2018. Available from: https://www.nice.org.uk/guidance/ng115/evidence/h-economic-model-report-pdf-6602768757.
26. Han MK, Quibrera PM, Carretta EE, et al. Frequency of exacerbations in patients with chronic obstructive pulmonary disease: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(8):619–626. doi:10.1016/S2213-2600(17)30207-2
27. Agusti A, Edwards LD, Celli B, et al. Characteristics, stability and outcomes of the 2011 GOLD COPD groups in the ECLIPSE cohort. Eur Respir J. 2013;42(3):636–646. doi:10.1183/09031936.00195212
28. Mackay AJ, Kostikas K, Roche N, et al. Impact of baseline symptoms and health status on COPD exacerbations in the FLAME study. Respir Res. 2020;21(1):93. doi:10.1186/s12931-020-01354-8
29. Kostikas K, Greulich T, Mackay AJ, et al. Treatment response in COPD: does FEV1 say it all? A post hoc analysis of the CRYSTAL study. ERJ Open Res. 2019;5(1):00243–02018. doi:10.1183/23120541.00243-2018
30. Casanova C, de Torres JP, Aguirre-Jaíme A, et al. The progression of chronic obstructive pulmonary disease is heterogeneous: the experience of the BODE cohort. Am J Respir Crit Care Med. 2011;184:1015–1021. doi:10.1164/rccm.201105-0831OC
31. Oga T, Nishimura K, Tsukino M, Sato S, Hajiro T, Mishima M. Longitudinal deteriorations in patient reported outcomes in patients with COPD. Respir Med. 2007;101(1):146–153. doi:10.1016/j.rmed.2006.04.001
32. Chatila WM, Thomashow BM, Minai OA, Criner GJ, Make BJ. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):549–555. doi:10.1513/pats.200709-148ET
33. Chen W, FitzGerald JM, Sin DD, Sadatsafavi M; Canadian Respiratory Research Network. Excess economic burden of comorbidities in COPD: a 15-year population-based study. Eur Respir J. 2017;50(1):1700393. doi:10.1183/13993003.00393-2017
34. National Institute for Health and Care Excellence (NICE). British National Formulary; 2020. Available from: https://bnf.nice.org.uk/.
35. Office for National Statistics (ONS). EARN01: average weekly earnings; 2020. Available from: https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/earningsandworkinghours/datasets/averageweeklyearningsearn01/current.
36. Meguro M, Barley EA, Spencer S, Jones PW. Development and validation of an improved, COPD-specific version of the St. George respiratory questionnaire. Chest. 2007;132(2):456–463. doi:10.1378/chest.06-0702
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.