")
Back to Journals » OncoTargets and Therapy » Volume 14
Early Study of Tumor Abnormal Protein in Gastric Adenocarcinoma
Authors Zhang M, Wang X, Wang Z
Received 15 December 2020
Accepted for publication 13 February 2021
Published 5 March 2021 Volume 2021:14 Pages 1719—1726
DOI https://doi.org/10.2147/OTT.S297413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nicola Silvestris
Ming Zhang,* Xiaoyu Wang,* Zhenghua Wang
Department of Gastrointestinal Oncology (Ward I), The First Affiliated Hospital of Jinzhou Medical University, Jinzhou, Liaoning, 121000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhenghua Wang
Department of Gastrointestinal Oncology (Ward I), The First Affiliated Hospital of Jinzhou Medical University, No. 2, Section 5, Renmin Street, Jinzhou, Liaoning, 121000, People’s Republic of China
Email [email protected]
Objective: To study the correlation between tumor abnormal protein (TAP) and tumor markers, blood glucose, uric acid and coagulation function in gastric adenocarcinoma and to evaluate the clinical application of TAP in the diagnosis of gastric adenocarcinoma.
Methods: A total of 34 nontumor patients and 95 gastric adenocarcinoma patients admitted to the First Affiliated Hospital of Jinzhou Medical University were enrolled in this study. Fresh blood from patients’ fingertips was collected, all blood samples were examined with TAP testing kit, and then searched and measured the condensed particulate matter.
Results: The comparison of TAP between nontumor patients and gastric adenocarcinoma patients was statistically significant (P< 0.05). Bivariate correlation analysis was conducted between TAP and other related tumor markers (alpha-fetoprotein, carcinoembryonic antigen, carbohydrate antigen 19– 9 (CA199), carbohydrate antigen 72– 4 (CA72-4)), blood glucose, uric acid, and coagulation function-related indicators, and the results showed that the correlation between TAP and CA199, CA72-4, and activated partial prothrombin time was statistically significant. In addition, according to the analysis results, there was no significant difference among TAP and age, height and weight in the tumor population and the nontumor population.
Conclusion: TAP can be used for the screening and diagnosis of gastric adenocarcinoma, and the effect of TAP combined with other indicators is more significant than TAP alone.
Keywords: tumor abnormal protein, gastric adenocarcinoma, tumor markers, blood glucose, uric acid, coagulation function
Introduction
Followed by lung cancer and liver cancer in men and breast cancer and lung cancer in women, gastric cancer is still the third leading cause of cancer-related death.1 At present, the treatment of gastric cancer is mainly surgical operation supplemented by chemotherapy, radiotherapy, targeted therapy, immunotherapy and supportive treatment. Some early gastric cancer can be treated by endoscopic resection, and advanced gastric cancer can be treated by open or laparoscopic gastrectomy and lymph node dissection. Chemotherapy is suitable for neoadjuvant therapy before radical gastrectomy, for patients with unresectable lesions or postoperative recurrence, and for adjuvant treatment after radical gastrectomy. However, the mortality of gastric cancer remains high because of the stage and drug resistance of various chemotherapy drugs. Therefore, early screening of gastric cancer is particularly important.
Early screening of gastric cancer includes the determination of tumor markers, the detection of HP and other methods, but the specificity is not very high. Gastroscopy biopsy is the gold standard for the diagnosis of gastric cancer; because gastroscopy is an invasive examination method, it causes pain and discomfort to patients. Therefore, we need to find more accurate methods for the early screening and diagnosis of gastric cancer. Recently, it was found that the detection rate of tumor abnormal protein (TAP) is high in early gastric cancer. Tumor abnormal protein (TAP) is mainly caused by incomplete glycosylation or the activation of new glycosyltransferases to produce new glycosylation. Therefore, this study combined TAP with other tumor markers, blood glucose levels, uric acid levels and coagulation function-related indicators to explore the significance of screening, diagnosis and development of gastric cancer.
Methods
Study Population
We collected data from 95 patients with gastric cancer and 34 nontumor patients between July 2020 and January 2021. All patients with gastric cancer were required to be pathologically diagnosed with gastric adenocarcinoma. A total of 34 nontumor patients (21 males and 13 females; aged 27 to 85 years, with an average of 63.79±2.56 years) were included. A total of 95 gastric adenocarcinoma patients (65 males and 30 females; aged 37 to 87 years, with an average of 64.07±1.01 years) were included. Our study was conducted in accordance with the Declaration of Helsinki. All patients signed an informed consent form, and this study was approved by the Ethics Committee of The First Affiliated Hospital of Jinzhou Medical University.
TAP Detection
The first drop and the second drop of fresh whole blood from the fingertip of the tested person were taken and smeared on a slide for preparation. After natural air drying, TAP was detected using a TAP testing kit and examination system (Zhejiang Ruisheng Medical Technology, Ltd., Cixi, China). The condensed particles were observed under a microscope, and the particle area of the condensed particles was measured. In the blood, TAP reacted with the reagent and produced crystal-like condensation. When TAP was positive, the condensation area was greater than or equal to 225 µm2, and when TAP was weakly positive, the condensation area was 121–225 µm2.
Statistical Analysis
The results are shown as the mean ± standard error of the mean (SEM). SPSS 25.0 software was used for statistical analyses and variance tests. A P value less than 0.05 was set as a significant difference.
Results
Basic Characteristics of Gastric Adenocarcinoma Patients and Nontumor Patients
Ninety-five patients with gastric adenocarcinoma and thirty-four nontumor patients were enrolled in this study. The mean age of patients with gastric adenocarcinoma and nontumor patients was 64.07±1.01 years and 63.79±2.56 years, respectively. TAP was detected in patients with gastric adenocarcinoma and nontumor patients, and the previous difference between the two was statistically significant (Table 1). According to our analysis, TAP showed no statistically significant differences with age, sex, height, weight, tumor differentiation or tumor TNM stage (Table 2). The positive detection rate of TAP in gastric adenocarcinoma patients is significantly higher than that in nontumor patients, so TAP can be used to detect gastric adenocarcinoma.
 |
Table 1 Comparison of TAP Between Nontumor Patients and Gastric Adenocarcinoma Patients |
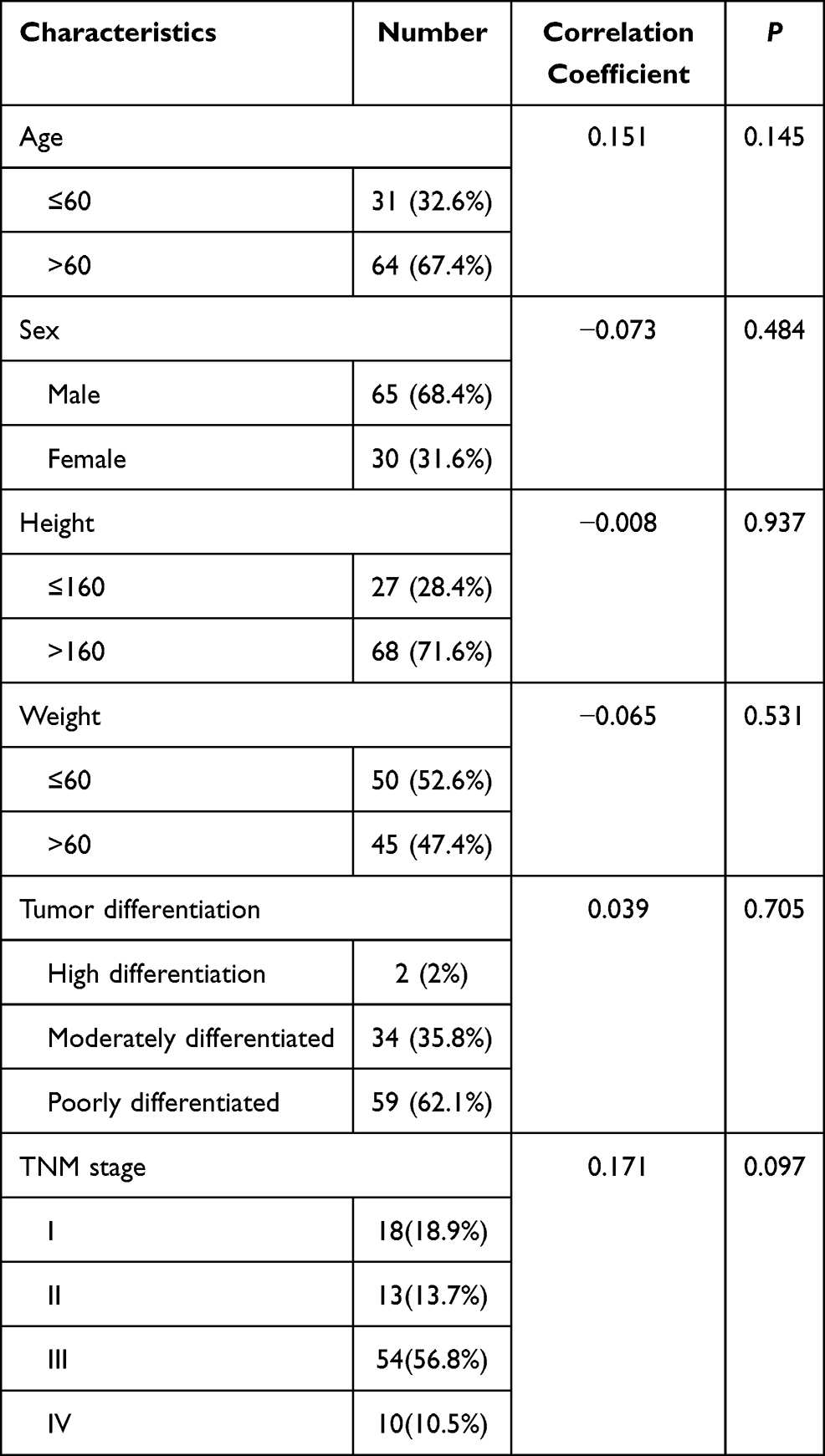 |
Table 2 Baseline Characteristics of Patients with Gastric Adenocarcinoma |
Correlation Between TAP and Tumor Markers
To evaluate the potential of the four tumor markers as predictive indicators for the diagnosis of gastric adenocarcinoma, bivariate correlation analysis was performed, and it was found that the correlation between TAP and alpha-fetoprotein (AFP) and CEA was not statistically significant, but the correlation between TAP and CA199 and CA72-4 was statistically significant, indicating that CA199 and CA72-4 can be used as independent predictive indicators (Table 3). We compared the specificity and sensitivity of TAP, CEA and CA199 and found that TAP has a high sensitivity and specificity in the diagnosis of gastric adenocarcinoma (Figure 1).
 |
Table 3 Correlation Between TAP and Tumor Markers in Patients with Gastric Adenocarcinoma |
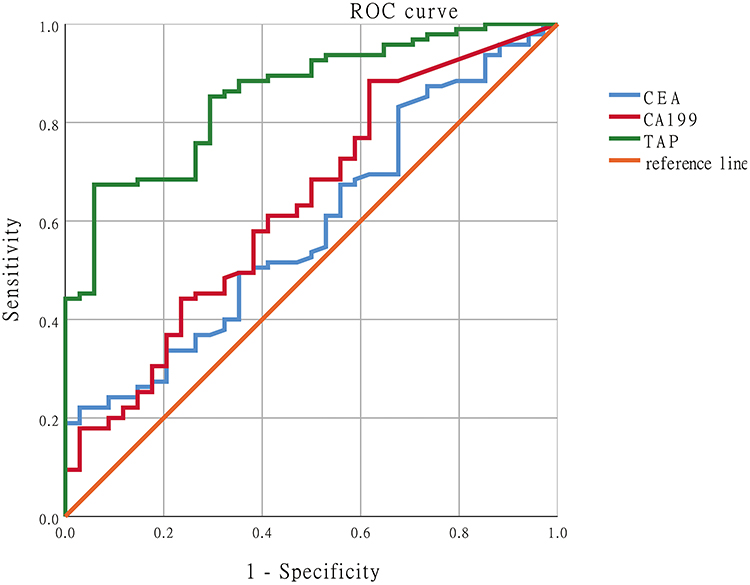 |
Figure 1 ROC curve of TAP, CEA and CA199 in the diagnosis of gastric adenocarcinoma. |
The Correlation of TAP with Blood Glucose, Uric Acid and Coagulation Function
The literature has shown that high glycemic load increases the risk of gastric cancer, especially in the Asian population.2 For this reason, the correlation between TAP and blood glucose was discussed, but the correlation between them was not statistically significant after analysis (Table 4). Excessive uric acid production in gastric cancer patients may be due to increased activity of xanthine dehydrogenase, which in turn may lead to proinflammatory activity leading to cell transformation.3 In Y V Dumanskiy et al’s article, purine metabolism disorder was observed in all gastric cancer patients in the experimental group, and the change in uric acid was more obvious in gastric cancer.4 Therefore, the correlation between TAP and uric acid was analyzed, but the correlation between them was not statistically significant (Table 5). The impaired balance between clotting and fibrinolysis leads to thrombus formation, and hypercoagulability is a risk factor for aggravating thrombus formation.5–7 Therefore, the correlation between coagulation function and TAP was analyzed and found to play a guiding role in the prognosis of gastric cancer patients (Table 6).
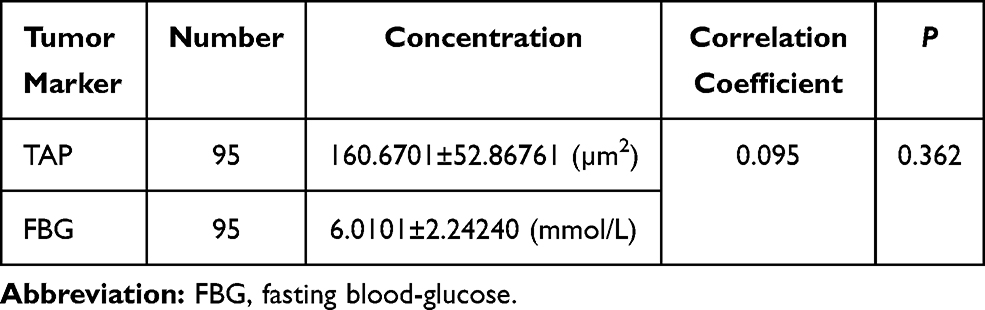 |
Table 4 Correlation Between TAP and Fasting Blood-Glucose |
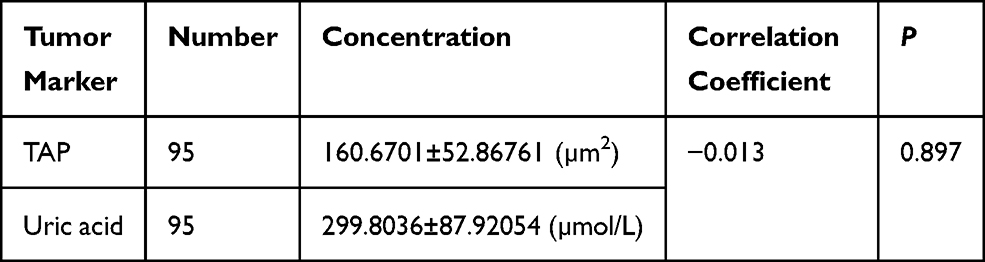 |
Table 5 Correlation Between TAP and Uric Acid |
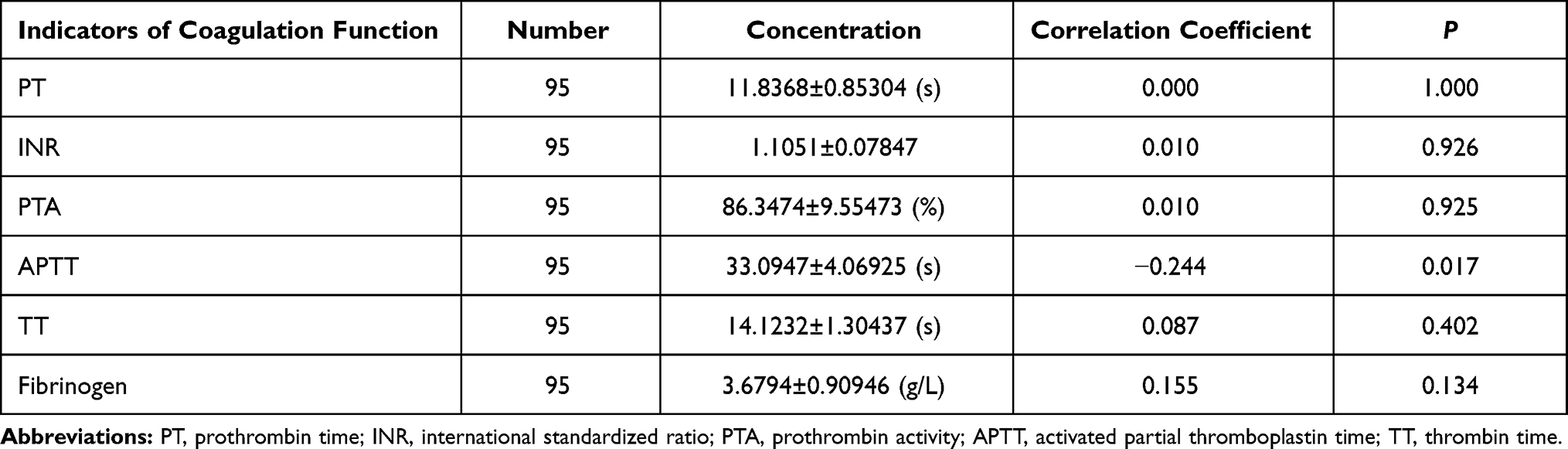 |
Table 6 Correlation Between TAP and Coagulation Function |
The Correlation Analysis of the Remaining Indexes
By analyzing the data of all patients, it was concluded that there was no correlation between disease status and age, sex, height, weight, stage or HER-2 (p>0.05). However, CA199 was significantly correlated with staging (Table 7). TAP expression levels were divided into a normal group, weakly positive group and positive group, and the relationship between CA199, CA72-4 and APTT and the three TAP expression groups was analyzed according to the groups. The analysis found that the difference in CA199 between the normal group and the positive group was statistically significant, the difference in CA199 between the weak positive group and the positive group was statistically significant, and the difference in CA199 between the positive group and the other two groups was statistically significant. The analysis found that the difference in CA72-4 between the normal group and the positive group was statistically significant, the difference in CA72-4 between the weak positive group and the positive group was statistically significant, and the difference in CA72-4 between the positive group and the other two groups was statistically significant. The analysis found that the difference in APTT between the normal group and the other two groups was statistically significant. (P <0.05) (Table 8).
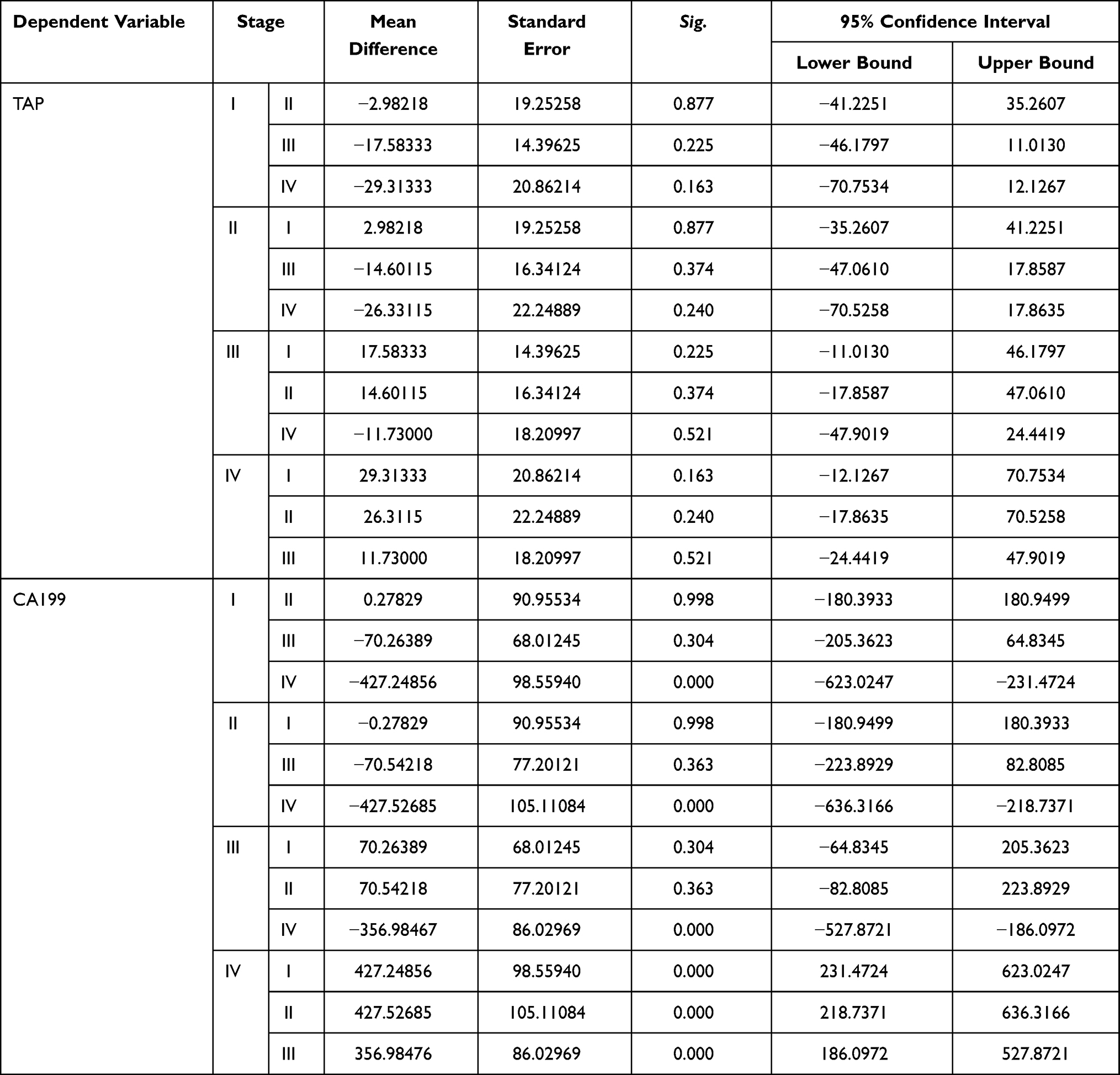 |
Table 7 Correlation Analysis of TAP and CA199 in the Patients with Their Tumor Stage |
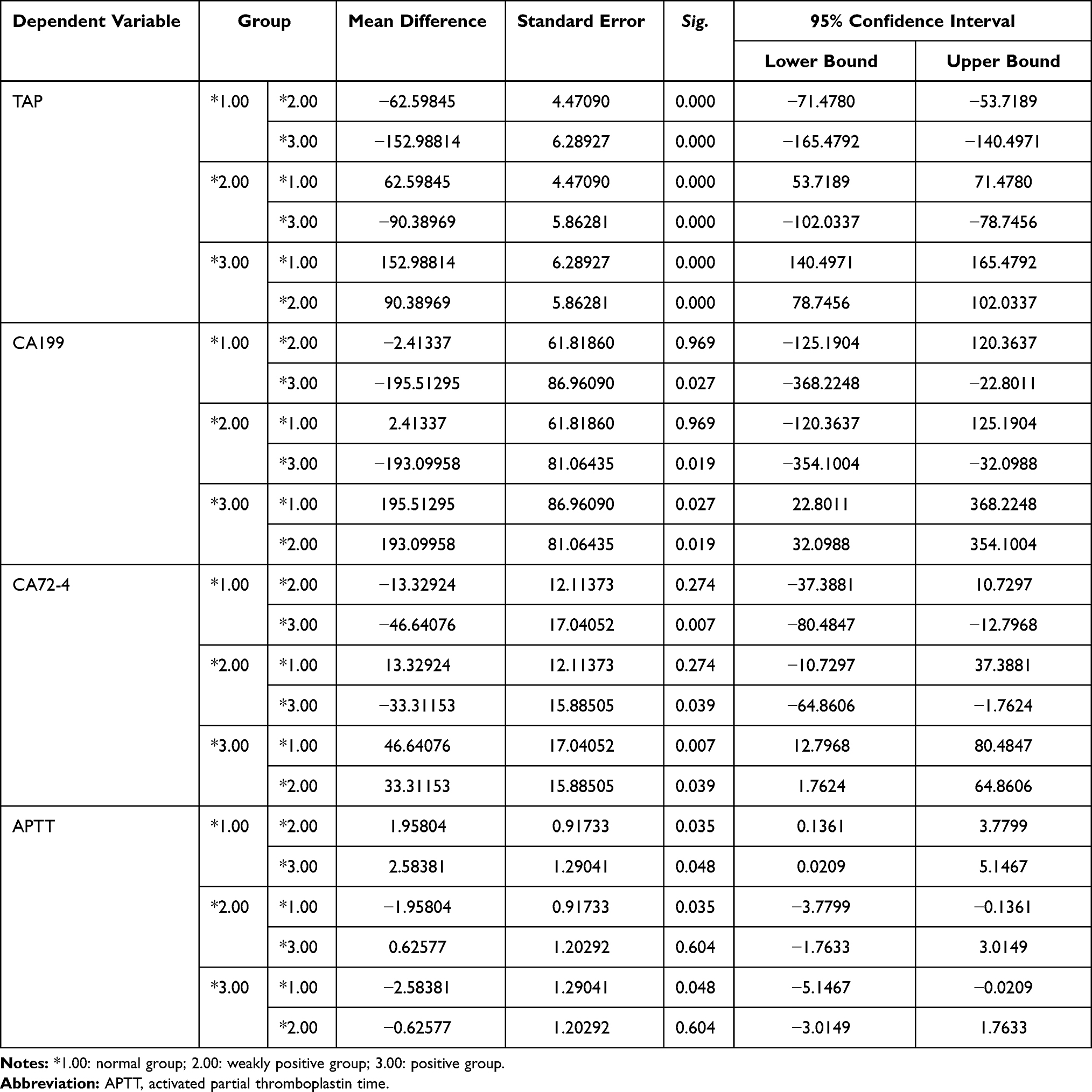 |
Table 8 Correlation Analysis of CA199, CA72-4, APTT in the Patients with TAP Grouping |
Discussion
Currently, the mortality rate of gastric cancer is high, and most deaths are due to recurrence and metastasis. Therefore, early screening diagnosis is particularly important for the prognosis of patients. In recent years, an increasing number of scholars have been devoted to studying the occurrence, development and prognosis of tumors to better improve the prognosis of patients and prolong their survival time. Many recent studies have demonstrated the sensitivity and specificity of TAP for the early screening, diagnosis, and prognosis of tumors.8–11 In this study, we collected peripheral blood samples from 95 patients with gastric adenocarcinoma and 34 nontumor patients and evaluated the influence of TAP expression on screening diagnosis based on these samples. The positive rate of TAP in patients with gastric adenocarcinoma (68.4%) was significantly higher than that in nontumor patients (23.5%), indicating that TAP is more sensitive to gastric cancer; in other words, TAP can be used to monitor gastric adenocarcinoma. In addition, TAP also plays a significant role in diagnosing lung cancer patients and monitoring disease progression.12
Tumor markers are produced by tumor cells and exist in cells, tissues or body fluids. They are chemical substances that can reflect the presence of tumors. Their presence or quantitative changes can indicate the nature of tumors to better understand histogenesis and cell differentiation to help tumor diagnosis, prognosis judgment and treatment selection. It is well known that the elevation of tumor markers (such as AFP, CEA, CA199, and CA72-4) in the serum of gastric cancer patients can contribute to the diagnosis, staging, prognosis and treatment of gastric cancer. In relevant reports, the most specific tumor marker for gastric cancer is CA72-4, and the elevation of CA72-4 is closely related to tumor stage and distant metastasis.13–19 The concentrations of serum CA72-4, CA199 and CA50 returned to normal with radical surgical resection of gastric cancer or decreased through palliative surgical resection. The change in serum CA199 levels before and after surgery has been confirmed to be an independent prognostic factor for gastric cancer patients.20 However, when we conducted data statistics, we found that most of the patients’ tumor markers were within the normal range and not higher than the normal value. The size of tumor tissue, blood supply, differentiation of tumor cells, and tumor stage all affect the concentration of tumor markers to varying degrees. Therefore, we believe that tumor markers (such as AFP, CEA, CA199, CA72-4) are not very specific for the diagnosis of gastric cancer, so we need some new indicators to help us discover and diagnose gastric cancer.
Venous thromboembolism (VTE) is an important complication in patients with malignant tumors and one of the main causes of death.21,22 Venous thromboembolism includes deep venous thrombosis (DVT) and pulmonary embolism (PE).23,24 One large report of a large-scale epidemiological study showed that approximately 20% of new cases of VTE were related to potential tumors.25 Compared with patients without cancer, cancer patients have an increased risk of VTE,26,27 and those with metastases have a 4–13 times higher risk.28,29 The formation of VTE seriously affects the survival and mortality of cancer patients.30 The thrombotic process is a multifactorial continuous complication associated with the clotting, fibrinolysis, and endothelial systems.31,32 Coagulation function and pathological stage are closely related to the prognosis of tumors. Hypercoagulability may lead to thrombosis, and once thrombosis occurs, the prognosis of patients will be very poor. If the tumor stage is stage IV, which means distant metastasis, then the survival time of patients will be greatly affected. In this study, we can see that TAP does not show an obvious correlation with tumor stage; however, in terms of blood coagulation function, we can see that TAP is negatively correlated with APTT, indicating that when TAP is increased, the body’s blood coagulation function will also be hyperactive. The results of this study indicated that TAP, CA199 and CA72-4 could be independent influencing factors for the early screening and diagnosis of gastric adenocarcinoma and that CA199 and APTT could be independent influencing factors for the prognosis of gastric adenocarcinoma. TAP is significantly correlated with APTT, and TAP may be a good indicator for monitoring prognosis, which remains to be further explored.
Conclusion
TAP detection represents a promising diagnostic and prognostic tool for gastric cancer.
Acknowledgments
This paper was supported by grants from the Natural Science Foundation of Liaoning Province, China (20180550753).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Niccolai E, Taddei A, Prisco D, Amedei A. Gastric cancer and the epoch of immunotherapy approaches. World J Gastroenterol. 2015;21(19):5778–5793. doi:10.3748/wjg.v21.i19.5778
2. Bangalore S, Fayyad R, Messerli FH, et al. Relation of variability of low-density lipoprotein cholesterol and blood pressure to events in patients with previous myocardial infarction from the IDEAL trial. Am J Cardiol. 2017;119(3):379–387. doi:10.1016/j.amjcard.2016.10.037
3. Battelli MG, Bortolotti M, Polito L, Bolognesi A. Metabolic syndrome and cancer risk: the role of xanthine oxidoreductase. Redox Biol. 2019;21:101070. doi:10.1016/j.redox.2018.101070
4. Dumanskiy YV, Stoliarova OY, Syniachenko OV, Aliev RF, Iermolaeva МV, Sokrut ОP. Comparative evaluation of purine dysmetabolism in gastric and pulmonary adenocarcinomas. Exp Oncol. 2020;42(3):220–223. doi:10.32471/exp-oncology.2312-8852.vol-42-no-3.15068
5. Nierodzik ML, Karpatkin S. Thrombin induces tumor growth, metastasis, and angiogenesis: evidence for a thrombin-regulated dormant tumor phenotype. Cancer Cell. 2006;10:355–362. doi:10.1016/j.ccr.2006.10.002
6. Lip GY, Chin BS, Blann AD. Cancer and the prothrombotic state. Lancet Oncol. 2002;3(1):27–34. doi:10.1016/S1470-2045(01)00619-2
7. Prandoni P, Falanga A, Piccioli A. Cancer and venous thromboembolism. Lancet Oncol. 2005;6:401–410.
8. Chen R, Jiang C, Zhu Q, et al. Combining the tumor abnormal protein test with tests for carcinoembryonic antigens, cancer antigen 15-3, and/or cancer antigen 125 significantly increased their diagnostic sensitivity for breast cancer. Medicine. 2020;99(29):e21231. doi:10.1097/MD.0000000000021231
9. Cheng Y, Chen Y, Zang G, et al. Increased expression of TAP is predictive of poor prognosis in patients with non-small cell lung cancer. Cancer Manag Res. 2020;13(12):1941–1946. doi:10.2147/CMAR.S239593
10. Li LX, Zhang B, Gong RZ. Insights into the role of tumor abnormal protein in early diagnosis of cancer: a prospective cohort study. Medicine. 2020;99(11):e19382. doi:10.1097/MD.0000000000019382
11. Lan F, Zhu M, Qi Q, Zhang Y, Liu Y. Prognostic value of serum tumor abnormal protein in gastric cancer patients. Mol Clin Oncol. 2016;5(1):216–220. doi:10.3892/mco.2016.877
12. He P, Zhang M, Yuan F. The significance of detecting tumor abnormal protein in patients with lung cancer. J Hebei Med Univ. 2012;10:1225–1226.
13. Gaspar MJ, Arribas I, Coca MC, Diez-Alonso M. Prognostic value of carcinoembryonic antigen, CA19–9 and CA 72–4 in gastric carcinoma. Tumour Biol. 2001;22:318–322. doi:10.1159/000050633
14. Tocchi A, Costa G, Lepre L. The role of serum and gastric juice levels of carcinoembryonic antigen, CA19.9 and CA72.4 in patients with gastric cancer. J Cancer Res Clin Oncol. 1998;124(8):450–455. doi:10.1007/s004320050198
15. Ucar E, Semerci E, Ustun H, Yetim T, Huzmeli C, Gullu M. Prognostic value of preoperative CEA, CA 19–9, CA 72–4, and AFP levels in gastric cancer. Adv Ther. 2008;25(10):1075–1084. doi:10.1007/s12325-008-0100-4
16. Byrne DJ, Browning MC, Cuschieri A. CA72-4: a new tumour marker for gastric cancer. Br J Surg. 1990;77:1010–1013. doi:10.1002/bjs.1800770918
17. Spila A, Roselli M, Cosimelli M. Clinical utility of CA 72–4 serum marker in the staging and immediate post-surgical management of gastric cancer patients. Anticancer Res. 1996;16:2241–2247.
18. Carpelan-Holmstrom M, Louhimo J, Stenman UH. CEA, CA 19–9 and CA 72–4 improve the diagnostic accuracy in gastrointestinal cancers. Anticancer Res. 2002;22:2311–2316.
19. Hamazoe R, Maeta M, Matsui T, Shibata S, Shiota S, Kaibara N. Ca72-4 compared with carcinoembryonic antigen as a tumor-marker for gastric-cancer. Eur J Cancer. 1992;28A(8–9):1351–1354. doi:10.1016/0959-8049(92)90517-6
20. Song XH, Liu K, Yang SJ, et al. Prognostic value of changes in preoperative and postoperative serum CA19-9 Levels in Gastric Cancer. Front Oncol. 2020;10:1432. doi:10.3389/fonc.2020.01432
21. Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):
22. Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100(10):3484–3488. doi:10.1182/blood-2002-01-0108
23. Boonyawat K, Crowther MA. Venous thromboembolism prophylaxis in critically ill patients. Semin Thromb Hemost. 2015;41(1):68–74. doi:10.1055/s-0034-1398386
24. Khorana AA, Carrier M, Garcia DA, Lee AY. Guidance for the prevention and treatment of cancer-associated venous thromboembolism. J Thromb Thrombolysis. 2016;41(1):81–91. doi:10.1007/s11239-015-1313-4
25. White RH, Zhou H, Murin S, Harvey D. Effect of ethnicity and gender on the incidence of venous thromboembolism in a diverse population in California in 1996. Thromb Haemost. 2005;93(2):298–305. doi:10.1160/TH04-08-0506
26. Blom JW, Vanderschoot JPM, Oostindiër MJ, et al. Incidence of venous thrombosis in a large cohort of 66, 329 cancer patients: results of a record linkage study. J Thromb Haemost. 2006;4(3):529–535. doi:10.1111/j.1538-7836.2006.01804.x
27. Hans-Martin MBO, Mathijssen J, Ten Cate H, et al. Symptomatic venous thromboembolism in cancer patients treated with chemotherapy: an underestimated phenomenon. Arch Intern Med. 2004;164(2):190–194. doi:10.1001/archinte.164.2.190
28. Chew HK, Davies AM, Wun T, Harvey D, Zhou H, White RH. The incidence of venous thromboembolism among patients with primary lung cancer. J Thromb Haemost. 2008;6(4):601608. doi:10.1111/j.1538-7836.2008.02908.x
29. Pelzer U, Opitz B, Deutschinoff G, et al. Efficacy of prophylactic low-molecular weight heparin for ambulatory patients with advanced pancreatic cancer: outcomes from the CONKO-004 trial. J Clin Oncol. 2015;33(18):2028–2034. doi:10.1200/JCO.2014.55.1481
30. Khorana AA. Venous thromboembolism and prognosis in cancer. Thromb Res. 2010;125(6):490–493. doi:10.1016/j.thromres.2009.12.023
31. Levi M, Meijers JC. DIC:which laboratory tests are most useful. Blood Rev. 2011;25(1):33–37. doi:10.1016/j.blre.2010.09.002
32. Mei H, Jiang Y, Luo L, et al. Evaluation the combined diagnostic value of TAT, PIC, tPAIC, and sTM in disseminated intravascular coagulation: a multi-center prospective observational study. Thromb Res. 2019;173:20–26. doi:10.1016/j.thromres.2018.11.010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.