")
Back to Journals » OncoTargets and Therapy » Volume 8
Early enteral and parenteral nutritional support after hepatectomy in patients with hepatic carcinoma: a systematic review and meta-analysis
Authors Gao L, Tian H, Wang X, Yu X, Guan Y, Chen M, Zhang J
Received 26 August 2014
Accepted for publication 31 October 2014
Published 10 March 2015 Volume 2015:8 Pages 623—631
DOI https://doi.org/10.2147/OTT.S73275
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Lin-Ben Gao,1* He Tian,2* Xing-Guang Wang,3 Xiao-Fei Yu,4 Yan Guan,2 Ming-Lu Chen,5 Jian Zhang6
1Department of Respiratory Medicine, Haiyang People’s Hospital, Haiyang, 2Department of Oncology, Shandong Province Tumor Hospital, Jinnan, 3Department of Respiratory Medicine, Provincial Hospital Affiliated to Shandong University, Jinnan, 4Department of Emergency, Haiyang People’s Hospital, Haiyang, 5Department of Nuclear Radiology, Shandong Province Tumor Hospital, Jinnan, 6Department of Gastroenterology, Haiyang People’s Hospital, Haiyang, People’s Republic of China
*These two authors contributed equally to this work
Background: This study sought to conduct a systematic review providing a comparative analysis of enteral nutrition (EN) and parenteral nutrition (PN) after hepatectomy.
Methods: PubMed, Embase, and the China National Knowledge Infrastructure databases were searched for publications describing randomized controlled trials that compared early EN and PN after hepatectomy. The time period for this search was from January 1990 to December 2013. In accordance with the inclusion criteria of this study, two researchers independently screened the retrieved literature, extracted data, and assessed methodological quality. A meta-analysis of the included publications was then performed using RevMan 5.2 software.
Results: The meta-analysis results indicated statistically significant differences between the group that received EN and the group that received PN during the early stages after hepatectomy with respect to average total bilirubin and alanine aminotransferase levels after nutrition, prealbumin levels, incidence of diarrhea and abdominal bloating, time to flatus, and average cost of nutrition. To varying degrees, better results were observed in the EN group than in the PN group for these metrics.
Conclusion: During the early stages after hepatectomy, EN has obvious advantages relative to PN; thus, EN merits more widespread promotion and application in this clinical context.
Keywords: hepatectomy, enteral nutrition, parenteral nutrition, systematic review, meta-analysis
Introduction
Hepatectomy is an important treatment method for benign and malignant liver disease.1 The pathophysiological changes that occur after hepatectomy are complex; in particular, one issue that patients face is that the residual liver must not only recover but also compensate for the functions of the removed portion of liver. Postoperative nutritional support helps to promote early recovery by patients who have undergone hepatectomy.2,3 Numerous studies have demonstrated that parenteral nutrition (PN) can easily deviate from physiological nutritional processes;4–6 these deviations may damage liver function, resulting in liver enzyme abnormalities, cholestasis, or even liver failure, among other complications.7 Relative to PN, enteral nutrition (EN) is considered to be more similar to physiological nutrition; thus, the use of EN instead of PN can avoid the disuse of intestinal function, prevent the translocation of intestinal flora, promote the recovery of intestinal barrier function, and promote the secretion of digestive and gastrointestinal hormones.8,9 However, some researchers still recommend conventional treatment typically consisting of PN therapy with a gradually supplemented diet after anal aerofluxus. Further, there is no evidence that PN or EN is better than no therapy. To address whether EN or PN is the preferred nutritional support approach during the early stages after hepatectomy, we performed a systematic review and meta-analysis of studies comparing early EN and PN after hepatectomy.
Materials and methods
Search strategy
We used the PubMed and Embase databases to search for relevant English language literature and the Wanfang and China National Knowledge Infrastructure databases to search for Chinese literature. The time period for the literature search was from January 1990 to December 2013. The literature search strategy utilized the following keywords: “enteral nutrition” or “parenteral nutrition” and “hepatectomy”.
Data selection
Inclusion criteria
All prospective randomized controlled trials (RCTs) that compared EN and PN during the early stages after hepatectomy and satisfied the following criteria were included: the study must have examined at least one of several defined outcome measures, ie, nutritional complications, time to flatus, liver function after the end of nutrition, serum albumin level, and cost of nutrition; publication in full text form; and a sample size of at least 30, because findings from studies with small samples have poor reliability.
Exclusion criteria
A study was excluded if it involved preoperative nutritional therapy, if it was an animal study, if it was not an RCT, if it was only published in abstract form, if it was a case report, if it did not provide recorded observations of any of the aforementioned outcome measures, if the patients had not had partial hepatectomy, or if random assignment was not strictly conducted.
Data extraction and quality assessment
In accordance with the inclusion and exclusion criteria for this systematic review, two literature assessors independently performed the literature screening, data extraction, and quality assessment. Disagreements regarding literature inclusion, data extraction, and quality assessment were resolved through discussion with the entire research group, which then made decisions regarding these differences of opinion. The extracted information included sample size, subject sex and age composition, manner and timing of providing EN, manner and timing of providing PN, occurrence of nutrition-related complications (such as diarrhea, bloating, and nutrition-related intravenous line infections), time to flatus, alanine aminotransferase and total bilirubin levels after the end of nutrition, serum albumin level, and the cost of nutrition.
Based on the quality assessment criteria for RCTs in version 5.2 of the Cochrane Handbook for Systematic Reviews of Interventions, the following aspects of the included studies were examined during the quality assessment process: use of an appropriate randomization method; use of a blinding method; use of a random allocation concealment method; and whether cases were lost to follow-up or dropped out of the study. For cases that were lost to follow-up or had dropped out of the study, the researchers examined whether intention-to-treat analysis was applied. Studies that satisfied all assessment criteria were categorized as class A studies, indicating that there was a minimal probability of biases relating to these criteria. Studies that satisfied at least one assessment criterion or partially satisfied multiple evaluation criteria (or if it was unclear how many assessment criteria were satisfied) were categorized as class B studies, indicating that there was a moderate probability of biases relating to these criteria. Studies that satisfied none of the assessment criteria were categorized as class C studies, indicating that there was a high probability of the presence of biases relating to these criteria.
Data consolidation and analysis
RevMan 5.2 software was utilized for the meta-analysis in this study. Depending on whether an examined variable was a categorical variable or a numerical variable, the value indicating the combined effect for the variable was presented as an odds ratio or a weighted mean difference (WMD) with a 95% confidence interval (CI). A P-value of 0.05 was used as the threshold for statistical significance. Statistical heterogeneity was evaluated using I2. When I2 was ≤50%, the heterogeneity among studies was regarded as insignificant, and a fixed-effects model was used to determine the combined outcome measures; when I2 was >50%, the heterogeneity among studies was regarded as significant, and a random-effects model was used to combine the outcome measures.
Results
Literature inclusion
Based on the search strategy described above, a total of 152 Chinese and English publications were retrieved; 97 of the retrieved publications were in English and 55 were in Chinese. Based on review of the titles of the retrieved publications, 118 were excluded; thus, 34 publications remained. A further 14 studies were excluded because they were published by the same institution as another retrieved study or utilized the same source data as another retrieved study; thus, 20 publications remained. After reading the abstract or the full text of the remaining publications, eleven further studies were excluded (for reasons including examination of fewer than 30 cases, a lack of the required outcome indicators, or administration of nutrition prior to hepatectomy). Finally, nine studies8–15 that examined a total of 677 cases were included in the current study. These nine studies included eight Chinese publications and one English publication (Figure 1).
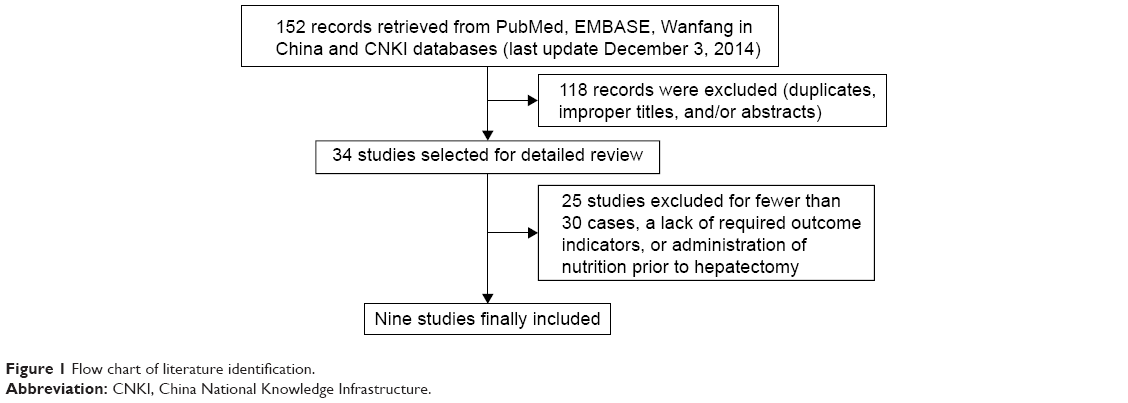 | Figure 1 Flow chart of literature identification. |
Basic quality assessments of the included trials
Table 1 lists the basic characteristics of each of the included RCTs; these characteristics include the sample grouping, the manner and timing of providing EN, the manner and timing of providing PN, and the main observed indicators for each trial. All studies were independently completed by an individual institution. Judgments about each risk of bias item for each included study are shown in Figures 2 and 3.
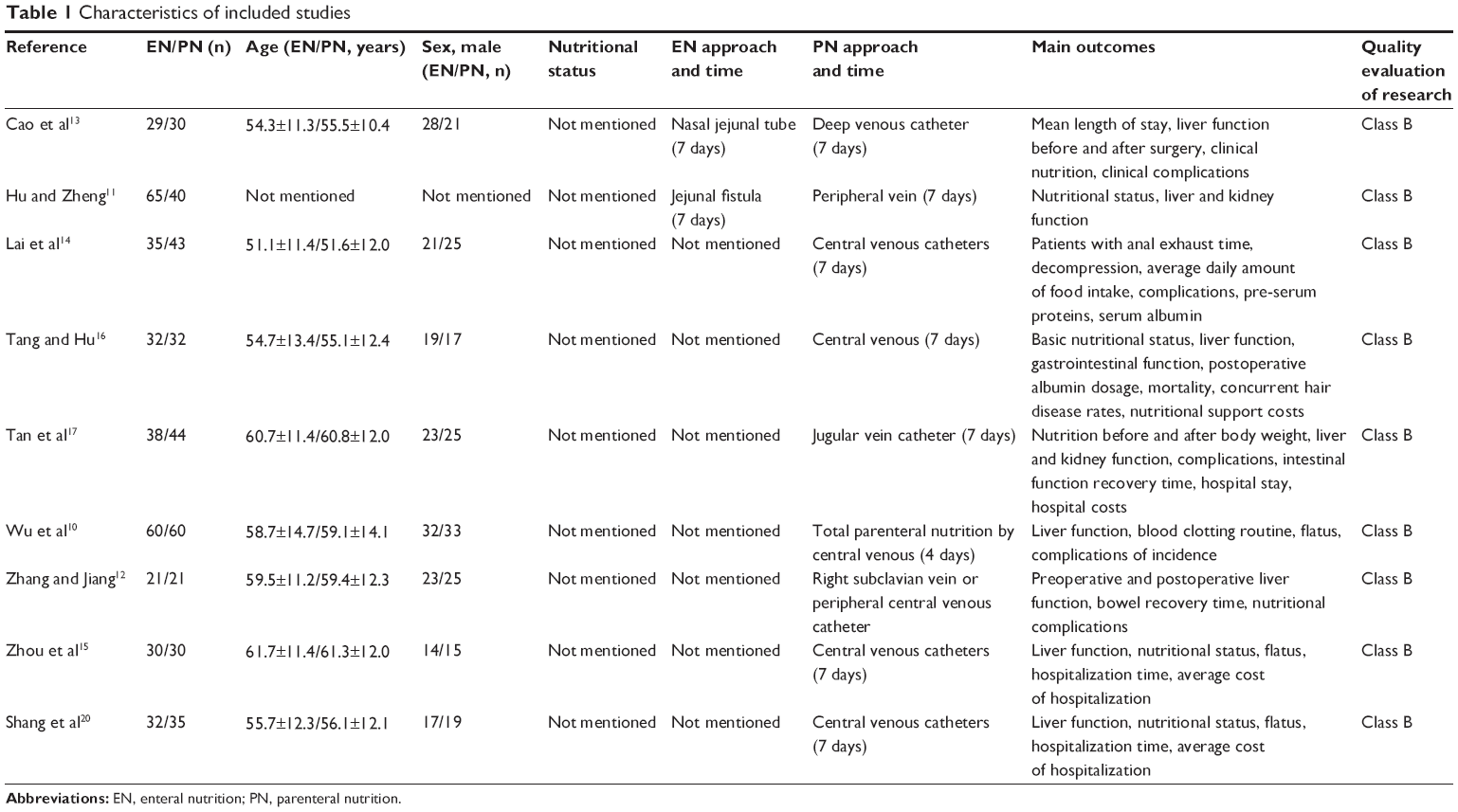 | Table 1 Characteristics of included studies |
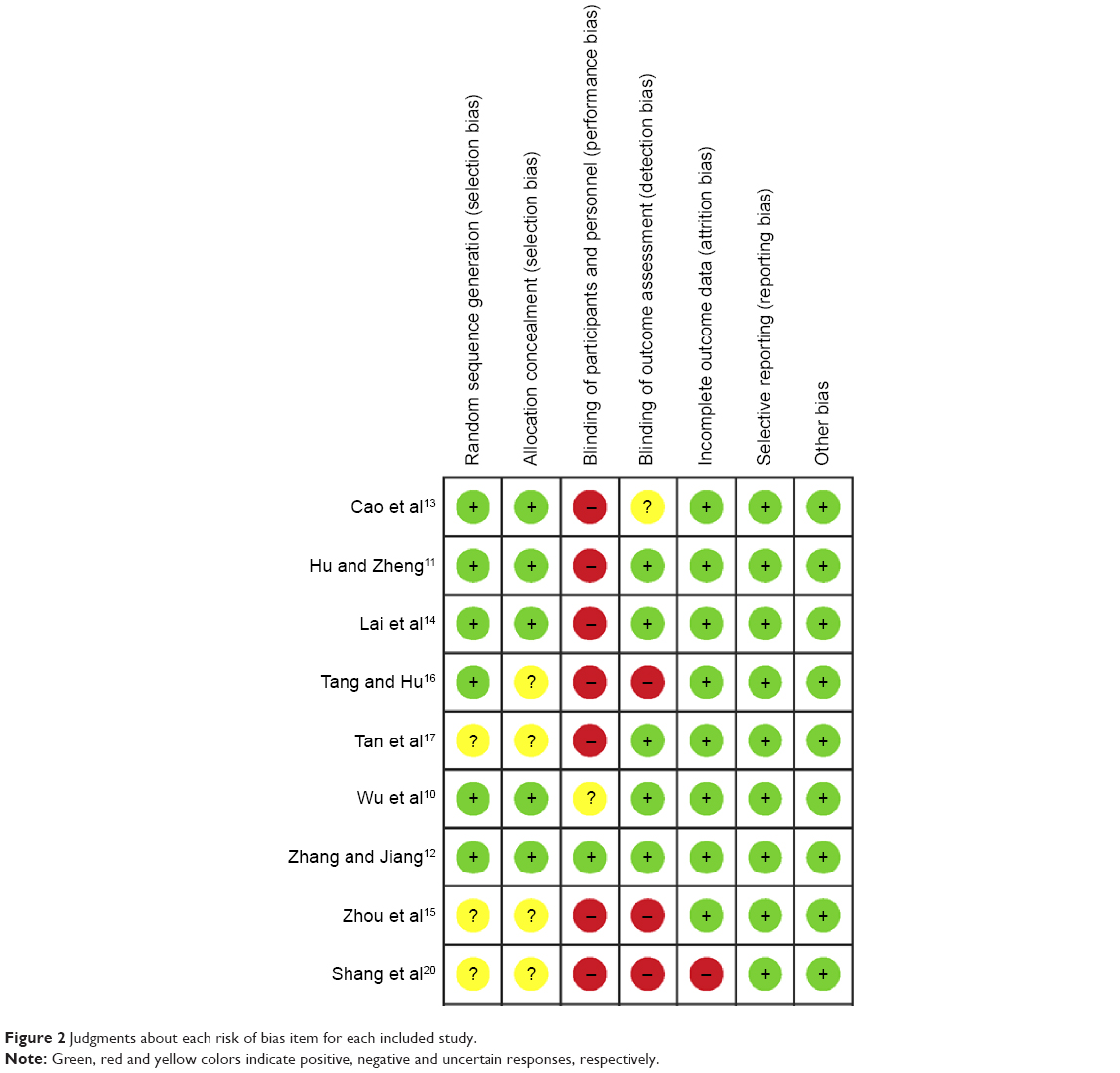 | Figure 2 Judgments about each risk of bias item for each included study. |
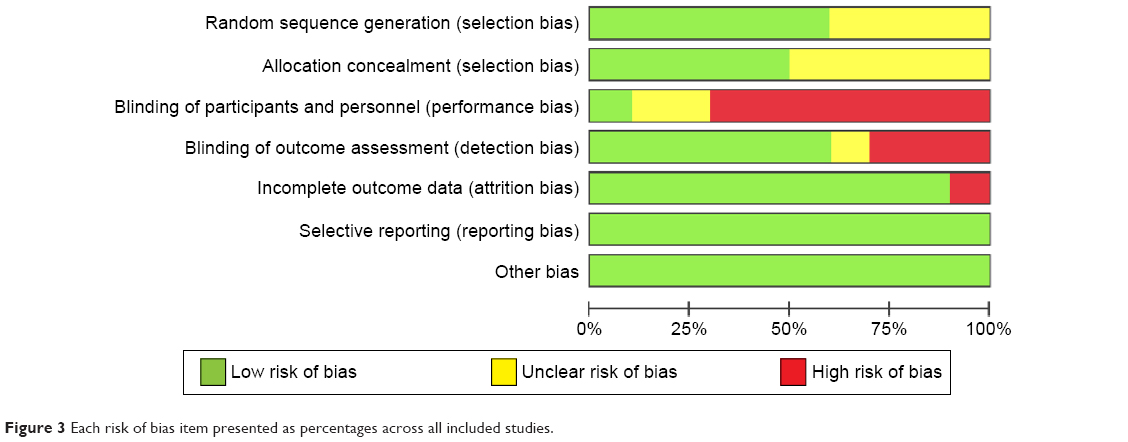 | Figure 3 Each risk of bias item presented as percentages across all included studies. |
Observed combined effects for main outcome measures
The combined effects for the main outcome measures were analyzed (Figures 4 and 5). These outcome measures for early EN and PN after hepatectomy included liver function, clinical nutrition indicators, nutritional complications, recovery of gastrointestinal motility, and the average cost of nutrition. Among these indicators, liver function after receiving nutrition, clinical nutrition indicators, and nutrition-related complications are the focus of this study. A forest plot revealed that early EN was superior to early PN with respect to maintenance of liver function. Combined effect analyses indicated that the mean serum total bilirubin level was lower after EN than after PN (WMD −4.29 μmol/L; 95% CI −5.55, −3.03; P<0.001) and that the mean serum alanine aminotransferase level was lower after EN than after PN (WMD −20.51 U/L; 95% CI −34.65, −6.37; P=0.004). There was no statistically significant difference in serum albumin levels between the two groups, with a combined effect across the included studies of 2.25 g/L (95% CI −0.24, 4.73; P=0.08). However, the mean plasma prealbumin level after nutrition was higher for the EN group than for the PN group (WMD 27.56 mg/L; 95% CI 9.02, 46.11; P=0.004), suggesting that EN is superior to PN in promoting liver protein synthesis and metabolism. With respect to major clinical complications of nutrition, there was no statistically significant difference between the two groups with respect to infections, which had an odds ratio of 0.63 (95% CI 0.32, 1.26; P=0.19). There was less abdominal diarrhea and bloating in the PN group than in the EN group, with an odds ratio of 1.95 (95% CI 1.33, 3.13; P=0.005) for the combined effects from the included studies. There was significantly better functional recovery of gastrointestinal motility in the EN group than in the PN group; in particular, examination of the combined effects from the included studies revealed that, on average, this recovery occurred 17.09 hours sooner in the EN group than in the PN group (95% CI −22.04, −12.13; P<0.001). Three studies compared the average cost of nutrition for EN and PN, and an examination of the combined effects from these three studies demonstrated that, on average, the cost of nutrition was 117.59 yuan (95% CI −133.52, −101.65; P<0.0001) cheaper per day for the EN group than for the PN group.
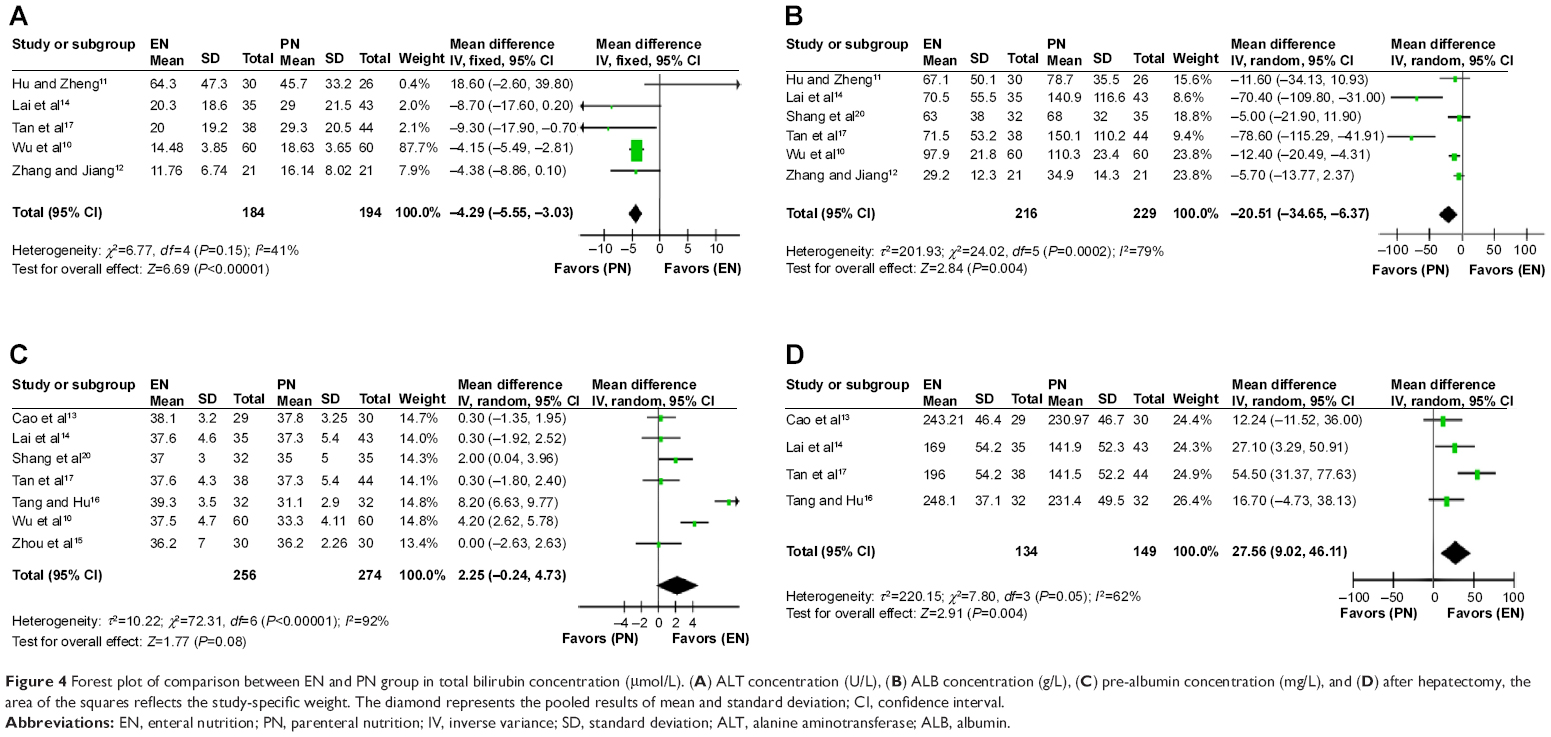 | Figure 4 Forest plot of comparison between EN and PN group in total bilirubin concentration (μmol/L). (A) ALT concentration (U/L), (B) ALB concentration (g/L), (C) pre-albumin concentration (mg/L), and (D) after hepatectomy, the area of the squares reflects the study-specific weight. The diamond represents the pooled results of mean and standard deviation; CI, confidence interval. |
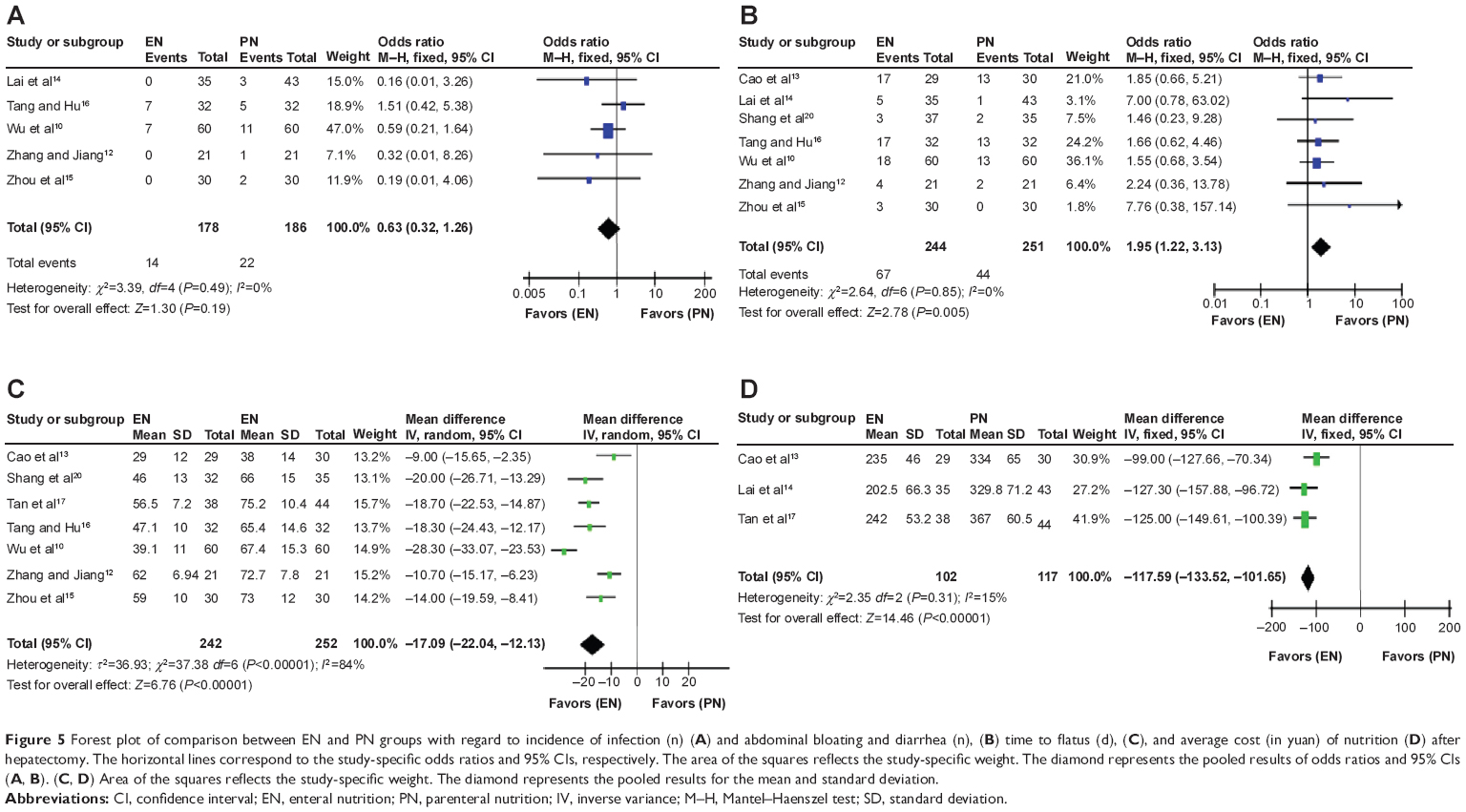 | Figure 5 Forest plot of comparison between EN and PN groups with regard to incidence of infection (n) (A) and abdominal bloating and diarrhea (n), (B) time to flatus (d), (C), and average cost (in yuan) of nutrition (D) after hepatectomy. The horizontal lines correspond to the study-specific odds ratios and 95% CIs, respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of odds ratios and 95% CIs (A, B). (C, D) Area of the squares reflects the study-specific weight. The diamond represents the pooled results for the mean and standard deviation. |
Sensitivity analysis
In this study, various outcome measures were further analyzed after excluding low-quality studies and recombining the results of the remaining studies. Comparisons of the meta-analysis results before and after this exclusion revealed no significant differences; the analysis exhibited relatively low sensitivity, so the analysis results were relatively robust and credible.
Assessment of publication bias
Publication bias is an important factor that affects the authenticity of the results of meta-analyses. For various reasons, the literature published in journals may differ from unpublished studies. The existence of this type of bias cannot be completely resolved by a meta-analysis itself. In this investigation, a funnel plot was drawn using the Funnel plot command in the RevMan software (Figure 6), which indicated no publication bias in the studies included.
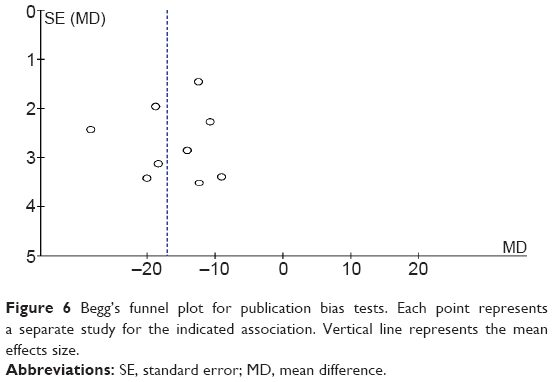 | Figure 6 Begg’s funnel plot for publication bias tests. Each point represents a separate study for the indicated association. Vertical line represents the mean effects size. |
Discussion
The results of this meta-analysis indicate that average total bilirubin and alanine aminotransferase levels were lower for patients who received early EN after hepatectomy than for those who received early PN after hepatectomy. These findings suggest that EN was more conducive to the recovery of liver function after hepatectomy than PN, and that the use of EN could avoid the complication of PN-related liver damage. A possible mechanism for this phenomenon is that the nutritional factors enter the liver during EN, accelerating blood circulation in the portal venous system and allowing the liver cells to receive more complete nutrient support.16
In addition, EN fully mimics in vivo nutrient metabolism processes and can therefore promote the recovery of physiological hormone secretion; thus, EN can affect how liver cell functions responding to hormones at the molecular level and can thereby contribute to liver cell metabolism.17 In contrast, during PN, nutrients in uniform configurations directly enter the body; the majority of these nutrients can be directly transported to the liver for metabolic processes without prior screening. This type of nutrition is therefore unable to consider individual differences and is likely to increase the burden on the liver. Animal experiments have demonstrated that even reasonable forms of PN (containing an energy supply of 105 kJ/mg and a nitrogen supply of 0.15 g/kg) can cause sclerotic damage to the liver and cannot increase serum albumin levels. Clinical studies have also found that PN can significantly increase the incidence of intrahepatic cholestasis.18
Mean plasma prealbumin levels after nutrition was higher in the EN group than in the PN group, and the time to flatus was significantly earlier in the EN group than in the PN group. These findings suggest that during the early stages after hepatectomy, liquid delivered by EN can be completely absorbed in the intestine and thereby provide a positive stimulus that may accelerate the recovery of gastrointestinal function and promote liver protein synthesis and metabolism. In contrast, a patient’s body is unable to mobilize various metabolism-related hormones, such as gastrointestinal hormones, if PN was performed. In addition, nutrients delivered by EN are selectively absorbed by the intestinal mucosa; thus, EN can fulfill individual treatment needs. In fact, the same EN preparation can even be administered to different patients and successfully meet the differing nutritional needs of these various individuals. However, PN enters the body directly without selective absorption; thus, it is difficult to tailor total PN to the needs of the individual patient.
With respect to nutritional complications, although the results of our analysis indicate that rates of infection did not differ significantly between the two groups, the incidence of infection was higher in the PN group than in the EN group. During PN, the gastrointestinal mucosa is unused and begins to atrophy, leading to damage at the intestinal mucosal barrier, translocation of intestinal bacteria, and an increased probability of intestinal infection. However, EN can maintain the integrity of the intestinal mucosa and reduce the permeability of the intestinal tract;19 concurrently, EN may increase intestinal blood flow, which in turn increases blood flow to the liver, thereby protecting the reticuloendothelial system of the liver and maintaining the ability of the liver to combat pathogens.19 With respect to diarrhea, the analysis again revealed no statistically significant difference between the two groups, although diarrhea was more likely to occur in the EN group than in the PN group. The incidence of abdominal bloating was significantly higher in the EN group than in the PN group. However, in the included studies, symptoms of diarrhea and abdominal bloating were generally relatively mild; various approaches, such as slowing the infusion rate of the nutrient solution and slowly increasing the quantity of nutrients administered, could be utilized to ensure that these symptoms were tolerable for most patients. In addition, the average daily cost of EN was significantly lower than the average daily cost of PN; thus, in accordance with economic principles, the use of EN could effectively reduce the patients’ medical expenses and the financial burden on patients.
There are several limitations in the present study. On the one hand, the majority of the included studies come from the People’s Republic of China, so we did not perform subgroup analyses. On the other hand, we did not included literatures published in other languages (eg, German, French, Spanish), which may have resulted in a degree of selection bias. In addition, funnel plot analysis is only valid if there are more than ten trials, and only nine papers were included in our study, which is another limitation.
In conclusion, this study suggests that administration of EN during the early stages after hepatectomy has significant advantages when compared with administration of PN. Therefore, EN warrants more widespread promotion and application in this clinical context.
Disclosure
The authors report no conflicts of interest in this work.
References
Yang Y, Zhao LH, Fu SY, et al. Selective hepatic vascular exclusion versus Pringle maneuver in partial hepatectomy for liver hemangioma compressing or involving the major hepatic veins. Am Surg. 2014;80:236–240. | ||
Barlow R, Price P, Reid TD, et al. Prospective multicentre randomised controlled trial of early enteral nutrition for patients undergoing major upper gastrointestinal surgical resection. Clin Nutr. 2011;30(5):560–566. | ||
Ghafouri A, Salehi OA, Keshavarz SA, Hosseini S, Shojaifard A, Khorgami Z. Evaluation of supporting role of early enteral feeding via tube jejunostomy following resection of upper gastrointestinal tract. Med J Islam Repub Iran. 2012;26(1):7–11. | ||
Chiarla C, Giovannini I, Giuliante F, et al. Parenteral nutrition in liver resection. J Nutr Metab. 2012;2012:508103. | ||
Cao J, Luo SM, Liang L, Lai J. Effects of parenteral nutrition without and with growth hormone on growth hormone/insulin-like growth factor-1 axis after hepatectomy in hepatocellular carcinoma with liver cirrhosis. JPEN J Parenter Enteral Nutr. 2007;31:496–501. | ||
Richter B, Schmandra TC, Golling M, Bechstein WO. Nutritional support after open liver resection: a systematic review. Dig Surg. 2006;23:139–145. | ||
Wu XT. [Nutritional support in surgical patients with hepatic dysfunction]. Zhong Guo Shi Yong Wai Ke Za Zhi. 2005;25:715–717. Chinese. | ||
Patton KM, Aranda-Michel J. Nutritional aspects in liver disease and liver transplantation. Nutr Clin Pract. 2002;17:332–340. | ||
Javid PJ, Collier S, Richardson D, et al. The role of enteral nutrition in the reversal of parenteral nutrition-associated liver dysfunction in infants. J Pediatr Surg. 2005;40:1015–1018. | ||
Wu JX, Rong WQ, Wang LM. [Clinical study of parenteral combined enteral nutrition therapy after partial hepatectomy]. Chang Nei Yu Chang Wai Ying Yang. 2009;16:209–211. Chinese. | ||
Hu QG, Zheng QC. The influence of enteral nutrition in postoperative patients with poor liver function. World J Gastroenterol. 2003;9:843–846. | ||
Zhang WB, Jiang HP. [Impact of enteral nutrition on liver function after hepatectomy]. Guangdong Medicine. 2005;26:528–529. Chinese. | ||
Cao JY, Wu LQ, Lu HJ. [Comparative study of early enteral and parenteral nutrition support after hepatectomy]. Zhonghua Pu Tong Wai Ke Za Zhi. 2006;21:117–119. Chinese. | ||
Lai JM, Liang LJ, Hua YP. [A prospective randomized study of early enteral and parenteral nutrition support after hepatectomy]. Zhonghua Gan Dan Wai Ke Za Zhi. 2010;16:604–607. Chinese. | ||
Zhou D, Liu S, Ying MG. [Comparing between enteral and parenteral nutrition support therapy in patients with liver cancer]. Chang Nei Yu Chang Wai Ying Yang. 2012;19:50–51. Chinese. | ||
Tang SP, Hu ZM. [Early enteral nutrition in patients after partial hepatectomy]. Xian Dai Lin Chuang Hu Li Za Zhi. 2011;10:51–53. Chinese. | ||
Tan JY, Xiong Li, Li YQ. [Enteral nutrition therapy in patients with after partial hepatectomy]. Dang Dai Hu Shi. 2011;12:40–41. Chinese. | ||
Hotta T, Kobayashi Y, Taniguchi K, et al. Evaluation of postoperative nutritional state after hepatectomy for hepatocellular carcinoma. Hepatogastroenterology. 2003;50:1511–1516. | ||
Li JS. [Enteral nutrition-the preferred surgical clinical pathways]. Chang Nei Yu Chang Wai Ying Yang. 2003;10:129–130. Chinese. | ||
Shang CZ, Zhang L, Yu DC, Cao J, Chen YJ. The value of early postoperative enteral nutrition in half hepatectomy for hepatocellular carcinoma patients. Zhong Hua Gan Zang Wai Ke Shou Shu. 2013;2:(5): 298–301. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.