")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Dysfunction of the thyroid gland during amiodarone therapy: a study of 297 cases
Authors Czarnywojtek A, Plazinska MT, Zgorzalewicz-Stachowiak M, Wolinski K, Stangierski A, Miechowicz I , Waligorska-Stachura J, Gut P, Krolicki L, Zioncheck M, Ruchala M
Received 18 September 2015
Accepted for publication 14 January 2016
Published 4 April 2016 Volume 2016:12 Pages 505—513
DOI https://doi.org/10.2147/TCRM.S96606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Agata Czarnywojtek,1,2,* Maria Teresa Płazińska,3,* Małgorzata Zgorzalewicz-Stachowiak,4 Kosma Woliński,1 Adam Stangierski,1 Izabela Miechowicz,5 Joanna Waligórska-Stachura,1 Paweł Gut,1 Leszek Królicki,3 Maja Zioncheck,6 Marek Ruchała1
1Department of Endocrinology, Metabolism and Internal Medicine, 2Department of Pharmacology, Poznan University of Medical Sciences, Poznan, 3Nuclear Medicine Department, Medical University of Warsaw, Warsaw, 4Department of Health Prophylaxis, Laboratory of Medical Electrodiagnostics, 5Department of Computer Science and Statistics, 6Poznan University of Medical Sciences, Poznan, Poland
*These authors contributed equally to this work
Aim: This study aims to explore and compare the efficacy of radioiodine treatment (RIT) in hyperthyroid and euthyroid patients who have been treated with amiodarone (AM) in the past or are currently undergoing AM treatment. Clinical observation of a group of patients with amiodarone-induced hypothyroidism during a 12-month follow-up period was used for comparison.
Design: This was a observational, two-centered study. Patients were assessed at baseline and at 2 months, 6 months, 8 months, and 12 months after RIT.
Patients: Group A: At baseline (61 males [M] and 17 females [F], mean age 50±19 years), there were 78 euthyroid patients with cardiac arrhythmias, who were treated with AM and developed amiodarone-induced thyrotoxicosis, and currently require retreatment with AM. Group B: Hyperthyroid patients (92 M and 26 F, mean age 72±11.8 years) after AM therapy in the past. Group C: Hyperthyroid patients (66 M and 13 F, mean age 63.9±13.2 years) currently treated by AM. Group D: Hypothyroid patients (6 M and 16 F, mean age 61.4±10.4 years) after AM therapy. The patients from Groups A, B, and C were retreated with AM after ~3–6 weeks of RIT.
Results: In Group A, after 12 months of RIT therapy, recurrent thyrotoxicosis was observed in six (7.7%) cases, and persistent hypothyroidism was diagnosed in 42 (53.8%) cases. In Group B, hyperthyroidism occurring during treatment with AM was found in 40 (33.9%) patients, and permanent hypothyroidism was observed in eleven (12.5%) cases. After annual follow-up in Group C, nine (11.4%) patients were diagnosed with hypothyroidism, while 27 (34.1%) patients were diagnosed with hyperthyroidism. In Group D, all patients had permanent hypothyroidism and when the concentration of serum thyroid-stimulating hormone was >10 µIU/mL, l-thyroxine was applied.
Conclusion: Our study showed that radioiodine administration is advisable in certain circumstances, even in euthyroid patients. It allows for continuation of further long-term AM treatment. Additionally, RIT allows for the reintroduction of AM therapy that was previously terminated. Hence, it can help control life-threatening tachyarrhythmias and decrease episodes of thyrotoxicosis.
Keywords: amiodarone, amiodarone-induced thyrotoxicosis, amiodarone-induced hypothyroidism, radioactive iodine, radioiodine treatment, paroxysmal atrial fibrillation, ventricular tachycardia
Introduction
Amiodarone (AM) is a popular and valued antiarrhythmic drug that has several electrophysiological activities.1–3 As a derivative of benzofuran, the structural formula of this drug resembles that of thyroxine. It contains two atoms of iodine, which constitute ~37.5% of its mass. Of this, 10%/d is deiodinated into free iodine,4,5 which means that with a daily dose of 200–400 mg AM, the human body receives 6–12 mg of iodine. Considering that a daily iodine requirement is only 150–200 μg, the need for this microelement is exceeded multiple times with AM therapy.5 The biological half-life of AM ranges from 2 weeks to 3 months. For this reason, after discontinuing the medication, its effect lingers for a considerable period of time.6
AM is used in the treatment of atrial fibrillation (AF) or atrial flutter, Wolff–Parkinson–White syndrome, and ventricular tachycardia. In the treatment of chronic cardiac arrhythmias, AM can be used in patients after myocardial infarction with left ventricular dysfunction or heart failure.3,7 AM rarely causes proarrhythmic effects in comparison to other antiarrhythmic drugs, but it may result in other side effects, such as thyroid dysfunction.8–10
While amiodarone-induced hypothyroidism (AIH) is not a significant clinical issue, amiodarone-induced thyrotoxicosis (AIT) is a grave problem even for an experienced endocrinologist.11–15 When other antiarrhythmic drugs and cardioversion turn out to be ineffective, AM may be the only life-saving drug left. Hence, a problem arises when these patients develop AIT. Our research shows that radioiodine (RAI) may be beneficial under these circumstances and may allow for continuation of AM therapy.
This study aims to explore and compare the efficacy of radioiodine treatment (RIT) in hyperthyroid and euthyroid patients who have been treated with AM in the past or who are currently undergoing AM treatment. Additionally, clinical observation of patients with AIH during 12 months of follow-up was used for comparison.
Material and methods
Patients
Medical records of patients who were treated in the Department of Endocrinology, Metabolism and Internal Medicine, Poznan, and in the Department of Nuclear Medicine, Warsaw, Poland, between 2002 and 2013 were included.
Patients were divided into the following four groups:
- A – euthyroid patients with AIT in anamnesis who required reintroduction of AM due to arrhythmia;
- B – patients with AIT, who discontinued therapy before RIT; AM was reintroduced in all patients 3 weeks or 6 weeks after RIT;
- C – patients with AIT continuing AM treatment, presenting very low radioiodine uptake (RAIU);
- D – hypothyroid patients treated with AM in the past.
The patients from Groups A, B, and C were retreated with AM after ~3–6 weeks of RIT.
Study design
This study was a analysis of available medical records with an observation period that spanned 1 year. Two hospitals in Poland – the Department of Endocrinology, Metabolism and Internal Medicine in Poznan and the Department of Nuclear Medicine in Warsaw – were involved in the study. Before being included in the study, all participating patients were educated on the methods and purpose of this study and gave their written informed consent. This study was approved by the Medical Ethics Committee at both the Department of Endocrinology, Metabolism and Internal Medicine in Poznan and the Department of Nuclear Medicine in Warsaw. Patients were scheduled to visit outpatient clinics at baseline (before RIT) and at 2-month, 6-month, 8-month, and 12-month intervals during 1 year of follow-up after the initiation of RIT. Thyroid-stimulating hormone (TSH), free triiodothyronine (fT3), free thyroxine (fT4), and thyroid autoantibodies were measured for evaluation at every visit to the outpatient clinics.
Diagnosis of AIT and AIH
The following diagnostic criteria for AIT were applied: 1) a history of AM treatment spanning at least 1 month and 2) signs and symptoms of hyperthyroidism further corroborated by increased TH and suppressed TSH levels that occurred during therapy or within 2 years after AM withdrawal. All eligible patients were not differentiated according to Types I and II AIT.16 The diagnosis of AIH was made using the following criteria: 1) signs and symptoms indicating hypothyroidism further corroborated by low serum levels of TH, 2) increased high serum levels of TSH, and 3) a history of the AM treatment in the period over 3 months.
Assays
Measurements of serum TSH levels (normal range: 0.27–4.2 μIU/mL) and hormonal assessment (fT4, normal range: 11.5–21.5 pmol/L and fT3, normal range: 3.9–6.8 pmol/L) were performed using a Hitachi Cobas e601 chemiluminescent analyzer (Hoffman-La Roche Ltd., Basel, Switzerland). The TSH concentrations were determined by third-generation assays (sensitivity: 0.005 μIU/mL). The concentrations of autoantibodies were determined by a radioimmunological method using second-generation antibodies (RIA-2 Dynotest TRAK human; BRAHMS Diagnostica GmbH, Berlin, Germany). The normal ranges of serum thyroid autoantibodies in our laboratory were as follows: thyroperoxidase antibody (TSHR-Ab) <2 IU/L, thyroid peroxidase antibody (TPO-Ab) <35 IU/mL, and thyroglobulin antibody (Tg-Ab) <115 IU/mL.
Sonography, RAIU, and scintigraphy
Ultrasonography of the thyroid was performed by using the Aloka SSD-500 (Aloka, Tokyo, Japan) with a 7.5 MHz linear transducer. Ultrasound was also used to measure thyroid volume with the ellipsoid model (width × length × thickness ×0.52 for each lobe) being used for calculation.17 Color-flow Doppler sonography was performed for the entire group. In the cases of patients with thyroid nodules, 150 MBq of 99mTc was administered intravenously, and after 30 minutes, a thyroid scintiscan was performed (Nucline gamma camera; Mediso Kft., Budapest, Hungary).
Treatment
Radioiodine
RAI was administered as a single, standard, oral dose of 740 MBq (20 mCi) in all patients in Groups: A, B, and C, regardless of thyroid size or the iodine uptake.
Amiodarone
Oral administration of AM was commenced in all patients around the same time – 3–6 weeks after RIT. An average dose of 200 mg was administered daily. After their hospital stay, the patients also received further treatment in an outpatient setting. In 18 cases (6.7%), patients relapsed and required immediate reinitiation of AM therapy to prevent the development of life-threatening tachyarrhythmias. In nine cases, AM was administered as a 150 mg bolus due to life-threatening tachyarrhythmias. Otherwise, in 250 (93.3%) patients, it was necessary to maintain chronic AM therapy as the antiarrhythmic agent of choice. This included patients who had survived sustained ventricular tachyarrhythmias with left ventricular dysfunction and patients with chronic arrhythmias after myocardial infarction who were unsuccessfully treated with β-blockers. Maintaining AM therapy also reduced the frequency of implantable cardioverter defibrillator shocks and controlled AF in selected highly symptomatic patients. AM was used as a second-line drug in the long-term treatment of AF in patients with structural heart disease, in highly symptomatic patients without heart disease, and in highly symptomatic patients without heart disease with atrial and atrioventricular tachycardia. Table 1 shows the exact indications for the acute and long-term treatment of AM.
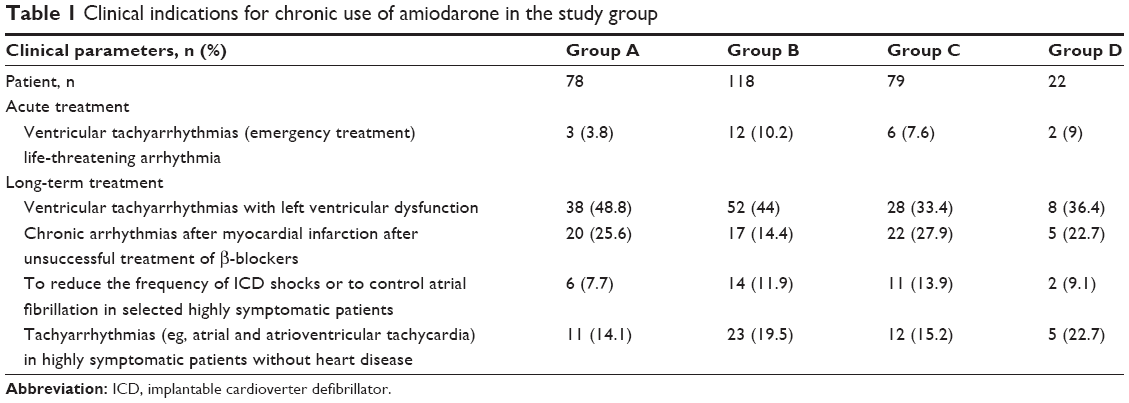 | Table 1 Clinical indications for chronic use of amiodarone in the study group |
L-thyroxine
In all patients with AIH, L-thyroxine was supplied. However, due to the risk of increasing the severity of tachyarrhythmias, the L-thyroxine treatment was applied only if the concentration of serum TSH was >10 μIU/mL.
Statistical analysis
All gathered information was computerized and analyzed. The data were processed by Statistica 10 software from StatSoft (Dell, Austin, TX, USA). The adopted statistical significance was α=0.05. The result was considered statistically significant when P<α. To describe the analyzed parameters, the average standard deviation was used. In order to establish the differences between individual groups (TSH, fT3, fT4, and thyroid autoantibodies), the Dunn’s multiple comparison test was performed. The Friedman test was performed to compare the variables measured on the interval scale (TSH, fT4, and fT3, on account of the lack of conformity with the normal distribution).
Results
The serum levels of TSH, thyroid hormones, and thyroid autoantibodies were examined at baseline and after 2 months, 6 months, 8 months, and 12 months of follow-up.
Of 391 elderly subjects who were assessed, 297 were eligible for this study. Reasons for ineligibility (n=94, 24%) were 1) patient death (n=24, 25.5%), 2) refusal to sign a consent form (n=3, 3.2%), 3) inadequate information (n=13, 13.8%), and 4) incomplete laboratory data (n=54, 57.5%).
The initial part of this investigation involved a retrospective analysis of the medical records of 297 patients who were treated in the Department of Endocrinology, Metabolism and Internal Medicine in Poznan (n=58 patients from Group A, n=61 from Group B, n=79 from Group C, and n=22 from Group D) and in the Department of Nuclear Medicine in Warsaw in Poland (n=20 patients from Group A and n=57 patients from Group B) between 2002 and 2013. There were 225 males and 72 females, with a male:female ratio of 3.1:1, with ages ranging from 37 years to 88 years (median age 65).
The patients were divided into the following four groups:
- Group A – 61 males (M) and 17 females (F), mean age 50±19 years. In this group, the median time of AM treatment prior to RIT was 2.4 years, ranging from 1.8 years to 3.4 years. The median time of antithyroid drug (ATD) usage was 3.9 years, ranging from 2.3 to 4.2. The RAIU was in the normal range, after 5 hours, it was 17.8%±3.4%, and after 24 hours, it was 31.7%±9.2%.
- Group B – 92 M and 26 F, mean age 72±11.8 years. The median time of AM therapy was 3.7 years, ranging from 3.3 years to 4.9 years, and the median time of ATD usage was 2.9 years, ranging from 3.3 years to 9.1 years, respectively. AM was reintroduced in 62 (52.5%) patients after 3 weeks and in 56 (47.5%) cases ~6 weeks after RIT. After 5 hours, the RAIU was 15.1%, and after 24 hours, it was 15.2%.
- Group C – 66 M and 13 F, mean age 63.9±13.2 years with very low RAIU (3.2%±1.8% after 5 hours and 2.9%±2.3% after 24 hours), currently on AM therapy. Median therapy of AM was 2.9 years, ranging from 3.1 years to 6.1 years, and the median time of ATD usage was 6.7 years, ranging from 3.8 years to 8.6 years.
- Group D – six M and 16 F, mean age 61.4±10.4 years. The median time of AM discontinuation was 12.5 months, ranging from 4 months to 37 months.
All of the patients were receiving ATDs and/or glucocorticosteroids (before RIT) within the time span preceding the study in the following proportions: 76 (97.4%) patients in Group A, 76 (64.4%) patients in Group B, and 52 (65.8%) patients in Group C. Additionally, iopanoic acid was used in four (5.4%) patients in Group C. Second RAI was used in seven (8.9%) patients in Group A, eleven (9.3%) patients in Group B, and 17 (21.5%) patients in Group C. Thyroidectomy was applied in two (2.6%) patients in Group A, two (1.7%) patients in Group B, and four (5%) patients from Group C.
In Group A (Figure 1) differences in the serum level of TSH were recorded between levels after 2 and 6 months and between 12 months and all other measurements. At the serum level of fT4, changes were significantly different after 2 and 12 months in comparison to the baseline (P<0.001). Additionally, significant changes were observed between the fT4 level after 2 and after 6, 8 and 12 months of follow-up (P<0.01) of follow-up. Statistically significant differences in fT3 serum levels were observed between baseline and levels after 2 and 12 months, as well as between the ft3 level after 2 months and after 8 and 12 months of follow-up.
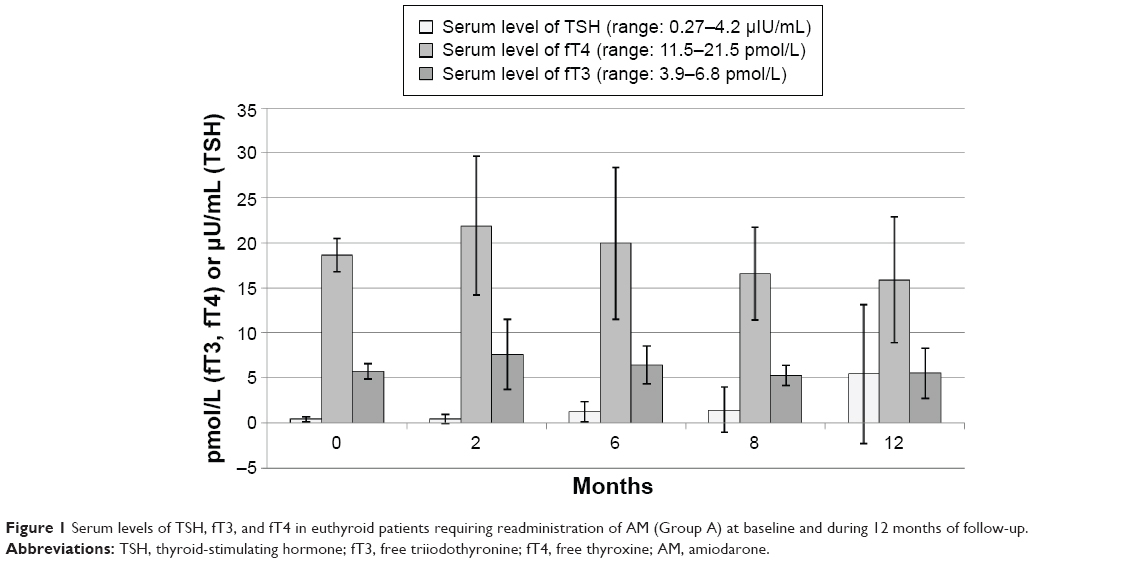 | Figure 1 Serum levels of TSH, fT3, and fT4 in euthyroid patients requiring readministration of AM (Group A) at baseline and during 12 months of follow-up. |
In Group B (Figure 2), significant differences in the serum level of TSH were recorded at 2 months and after 12 months, after 6 months and 12 months, and after 8 months and 12 months of follow-up (P<0.001) and between the baseline and all further measurements.
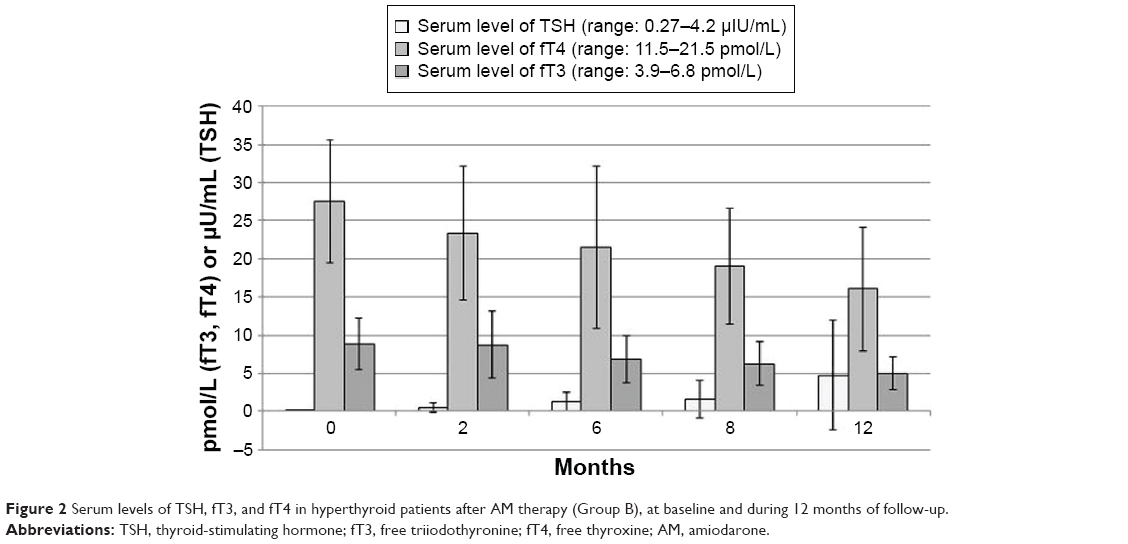 | Figure 2 Serum levels of TSH, fT3, and fT4 in hyperthyroid patients after AM therapy (Group B), at baseline and during 12 months of follow-up. |
Significant differences in the serum level of fT4 were recorded in most cases (P<0.001) except from fT4 at baseline from fT4 after 2 months and fT4 after 6 months to 8 months of follow-up. At serum level of fT3, changes were significantly different at baseline and 12 months (P<0.001) and after 2 months and 12 months (P<0.01) of observation.
In Group C (Figure 3), statistically significant differences in TSH serum levels were observed at baseline and after 6 months, 8 months, and 12 months of follow-up and between 2 months, 6 months, 8 months, and 12 months of follow-up. Similarly, as in Group B, statistically significant differences in fT4 serum levels were observed in most cases (P<0.001, Figure 3) -at baseline and after 2 months, 6 months, and 8 months of 12 months of follow-up. At the serum level of fT3, changes were significantly different between the level at the baseline and all further measurements.
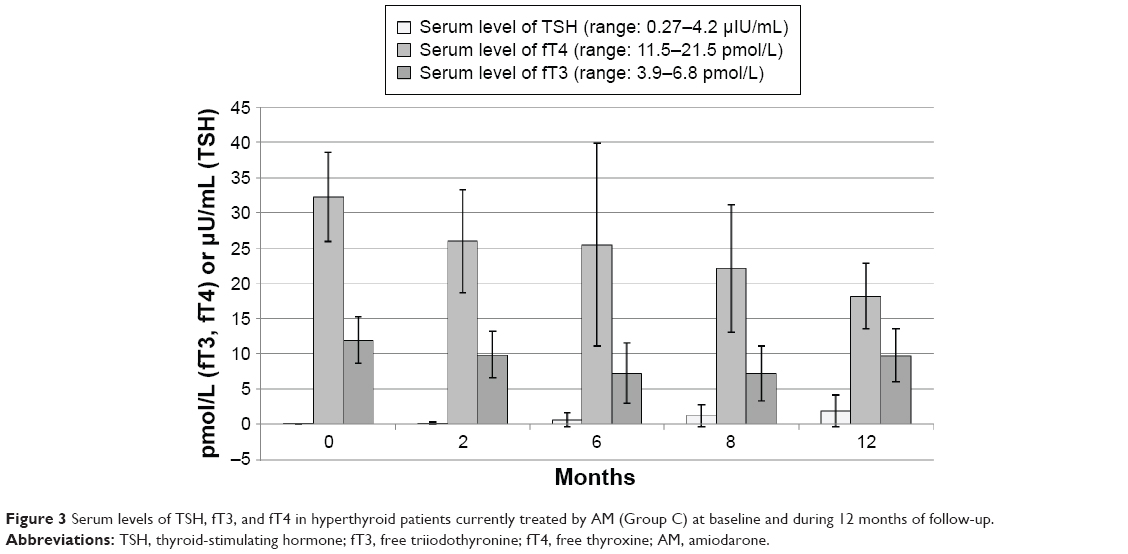 | Figure 3 Serum levels of TSH, fT3, and fT4 in hyperthyroid patients currently treated by AM (Group C) at baseline and during 12 months of follow-up. |
In Group D (Figure 4), no statistically significant differences in the serum levels of TSH, fT3, and fT4 were observed at baseline and during 12 months of follow-up.
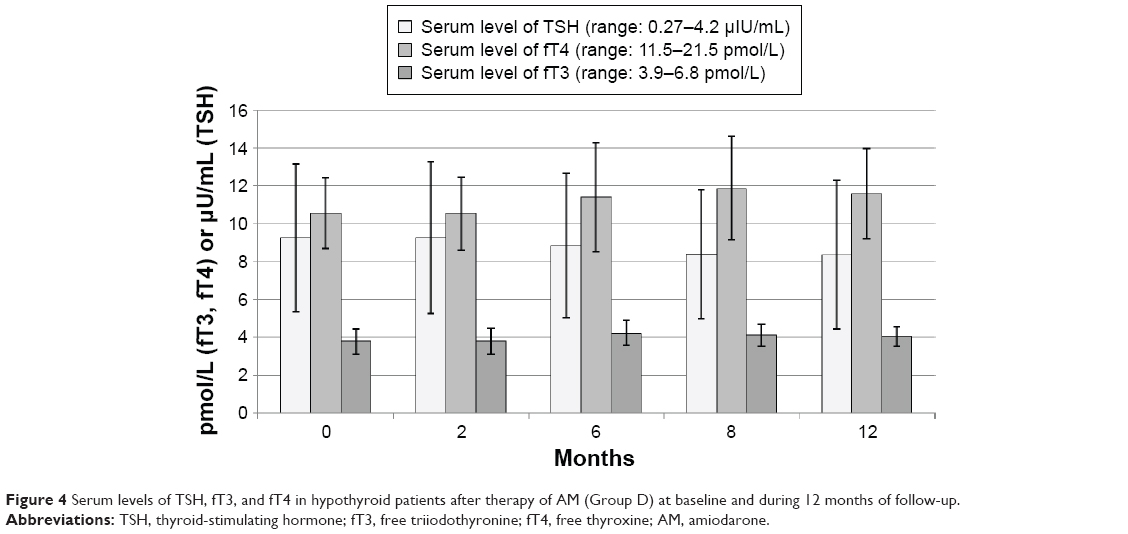 | Figure 4 Serum levels of TSH, fT3, and fT4 in hypothyroid patients after therapy of AM (Group D) at baseline and during 12 months of follow-up. |
No significant differences in the serum titers of Tg-Abs, TPO-Abs, or TSHR-Abs were observed. Serum TSHR-Abs titers were not elevated, and the mean values at baseline and after 2 months, 6 months, 8 months, and 12 months of follow-up were as follows: in Group A: 0.4±0.1 IU/L, 0.8±0.2 IU/L, 1.0±0.6 IU/L, 1.0±0.7 IU/L, and 0.4±0.3 IU/L; in Group B: 0.5±0.2 IU/L, 1.3±0.5 IU/L, 1.0±0.7 IU/L, 1.0±0.7 IU/L, and 0.4±0.3 IU/L; in Group C: 0.8±0.2 IU/L, 1.1±0.5 IU/L, 1.0±0.4 IU/L, 0.9±0.8 IU/L, and 0.7±0.5 IU/L; in Group D: 0.5±0.3 IU/L, 0.4±0.4 IU/L, 0.3±0.7 IU/L, 0.5±0.7 IU/L, and 0.3±0.3 IU/L, respectively.
Serum titers of Tg-Abs were in normal range for most cases in the studied groups (at baseline, after 2 months, 6 months, 8 months, and 12 months of follow-up): in Group A: 38.7±27.7 IU/mL, 65.7±36.9 IU/mL, 49.7±24.1 IU/mL, 38.7±27.7 IU/mL, and 32.2±22.4 IU/mL; in Group B: 48.7±34.7 IU/mL, 68.7±25.5 IU/mL, 43.7±26.9 IU/mL, 49.6±23.1 IU/mL, and 42.3±19.5 IU/mL; in Group C: 52.7±34.8 IU/mL, 67.4±26.9 IU/mL, 56.7±23.1 IU/mL, 43.2±16.3 IU/mL, and 47.9±16.2 IU/mL; in Group D: 58.7±36.8 IU/mL, 52.1±32.3 IU/mL, 67.1±27.8 IU/mL, 55.9±24.6 IU/mL, and 60.4±22.4 IU/mL, respectively.
Serum titers of TPO-Abs were also not elevated in most studied groups: in Group A: 26.9±10.3 IU/mL, 37.8±12.7 IU/mL, 34.8±14.7 IU/mL, 31.4±14.5 IU/mL, and 28.3±9.6 IU/mL; in Group B: 25.7±9.4 IU/mL, 41.1±14.3 IU/L, 35.6±23.8 IU/mL, 31.4±15.3 IU/mL, and 29.7±9.6 IU/mL; in Group C: 29.1±10.2 IU/mL, 32.9±11.3 IU/L, 35.8±21.9 IU/mL, 28.13±11.2 IU/mL, and 25.8±7.9 IU/mL; in Group D: 21.6±19.4 IU/mL, 23.1±12.3 IU/L, 18.9±10.2 IU/mL, 19.8±7.8 IU/mL, and 20.8±8.3 IU/mL, respectively. No statistically significant differences, which could have important clinical implications, were found between antibody titers and patients with AIT and AIH.
Clinical status
In Group A, where all the patients were euthyroid prior to RIT, recurrent thyrotoxicosis was observed after 6 months of follow-up in nine (11.5%) patients and after 12 months in six (7.7%) cases. In all these cases, retreatment with RIT was necessary. After 1 year of follow-up, persistent hypothyroidism was observed in 42 (53.8%) cases.
In Group B, normalization of the thyroid function was obtained in 37 (31.4%) cases after 2 months and in 49 (41.5%) patients after 6 months of follow-up. Permanent hypothyroidism was observed in eleven (9.3%) cases and control of arrhythmias was established in 67 (56.8%) cases. In all the remaining cases, recurrent thyrotoxicosis was still observable.
In Group C, where AM was administered on a daily basis, euthyroidism was found in only two (2.5%) patients, whereas hyperthyroidism was found in 54 (69.2%) patients after 2 months of follow-up. After a 6-month follow-up period, hyperthyroidism was present in 46 (58.2%) respondents, while permanent hypothyroidism was observed in six (7.7%) patients. After the annual follow-up, nine (11.4%) patients had hypothyroidism, while hyperthyroidism was observed in 27 (34.1%) patients. Therefore, once again radical treatment with RAI was performed.
In Group D, all patients had permanent hypothyroidism, and when the concentration of serum TSH was >10 μIU/mL, L-thyroxine was applied.
Discussion
Because AM chemically resembles fT4, it is able to block the thyroid hormone nuclear receptor. Blocking this receptor on the heart leads to a lower incidence of arrhythmias, reduces oxygen consumption, and prolongs the refractory period and the duration of action potentials.1,2,7 Unfortunately, AM and its metabolite also have direct cytotoxic effects on the thyroid, which lead to destruction of thyroid cells and the release of stored thyroid hormones.18 Exposure of thyroid cell cultures to AM and desethylAM leads to the release of cytochrome-c from the mitochondria and an increase in cell apoptosis.19
In patients treated with AM, a full-blown thyrotoxicosis may occur.10,20–22 Approximately 16%–20% of AM-treated patients suffer from thyroid-related disorders. Due to the accumulation of the drug and its metabolites in the body, AIT can develop during the administration of the drug or up to several months after the withdrawal of this medication.6 There are two mechanisms involved in AIT:
- Accumulation of a large amount of iodine in the gland of a patient with latent Graves’ disease, or even in a previously normal gland, can lead to the development of Type I AIT. This is called the Jod–Basedow effect. In Type I, AIT thyroid iodine uptake is usually normal or increased. This is particularly evident in patients with Graves’ disease, autonomous nodules, and a deficiency of iodine in the diet.
- The direct toxic effect of AM and its metabolite leads to destructive inflammation, subacute thyroiditis, and a release of T3 and T4, resulting in severe hyperthyroidism. This is Type II AIT and it often develops in people with a normal thyroid and in areas rich in iodine.10 Low thyroid iodine uptake (<2% in a 24-hour iodine uptake assay) is suggestive of Type II AIT.
Although AIT is sometimes divided into two types, in clinical practice these different categories are very difficult to distinguish, even by a skilled clinician. As in our previous publication, we do not recognize a distinction between Types I and II AIT. In the studied groups, there were no cases of patients who developed AIT secondarily to undiagnosed Graves’ disease or toxic nodular goiter, that would fulfill the definition of Type I AIT. The levels of autoantibodies (especially TSHR-Abs) were within the normal range in most patients. Moreover, it is difficult to introduce division for Types I and II AIT on the basis of C-reactive protein,23,24 interleukin 6,25 or thyroid ultrasonography.16 Indeed, AM causes thyrotoxicosis, but the underlying mechanism is still unclear.
It is also interesting that although in case of AIT it was not possible to distinguish between two types of AIT – “destructive” and resulting from underlying thyroid disease, our previous study with interferon-alpha-induced thyrotoxicosis (IIT) shows that in most cases it was quite easy to divide patients into two groups: IIT resembling Graves’ disease (Type I IIT conceptually similar to Type I AIT) and Hashitoxicosis (Type II IIT, similar to Type II AIT).26
In addition, treatment of AIT remains a controversial issue. Theoretically, treatment of Type I and Type II is different. However, in cases where it is not possible to determine the type of thyrotoxicosis and in patients with diagnosed mixed form of AIT, a combined treatment including ATDs,12,27–30 iopanoic acid,31,32 glucocorticosteroids,27,29,30 thyroidectomy,33,34 RIT,22,35,36 or a rarely recombinant human TSH as an adjuvant to RAI for Type II AIT37,38 is most commonly used.
Clinical symptoms of AIT are usually poorly expressed, even though the concentrations of thyroid hormone in the serum may be high. This can be due to the influence of AM on β-adrenergic receptors, (resulting in a reduction of clinical symptoms from sympathetic stimulation), AM inhibition of the conversion of T4 to T3, and the blockage of AM and its metabolites from binding to T3 nuclear receptors in the heart.14 Even though clinical symptoms may not always be evident, it should not be forgotten that AIT is associated with an increased mortality, especially in patients with impaired left ventricular function.39
It still remains controversial if or when AM therapy should be discontinued. On the one hand, AIT in patients with arrhythmias constitutes very severe complication. On the other hand, unique properties of AM make the decision about discontinuation of the therapy very difficult. Other antiarrhythmic drugs (ATDs) are often less effective and can worsen chronic heart failure due to negative inotropic effect.10 Moreover, as AM accumulates in tissues, thyrotoxicosis does not retreat immediately. During the course of our study, we found no extrathyroidal side effects being indications to withdrawal of AM. However, in some patients with AIT and lack of efficacy of RIT therapy, replacement of AM with other ATDs was necessary.
In our study, high RAIU was present only in patients from Group A, scarcely observable in Group B, and extremely decreased in Group C. However, as in our previous study, RIT was applied even at extremely reduced RAIU.22 As indicated by our observations, RIT can be used repeatedly, preferably in intervals of at least 3 months. It is worth to remember that RAI administration is not associated with serious side effects other than potential hypothyroidism. However, as Hermida et al35 state, “hypothyroidism should be viewed as a goal rather than a complication” as it can easily be treated with thyroid hormone replacement. Advantages of AIT seem to exceed such adverse effects. In Group A – euthyroid patients with thyrotoxicosis in anamnesis – only ~11% developed hyperthyroidism in 6 months. In Group B including patients with AIT who discontinued therapy before RIT and reintroduced AM after 3–6 weeks, over a half of subjects were eu- or hypothyroid after 6 months, after a year mean TSH in the group was 4.7, median 2.5. In Group C, consisting of patients with AIT, who received RIT without discontinuation of AM therapy, euthyroidism was very difficult to obtain, and thus these patients required frequent clinical examination. However, even in this group with extremely decreased RAIU, RIT brought noticable effects – only ~35% of patients were hyperthyroid after a year; even after as short period as 2 months ~30% of patients became eu- or hypothyroid. In the case of AIH (Group D), there was no particular danger, and hypothyroidism required only the L-thyroxin therapy.
RIT is sometimes viewed as a questionable method of therapy and its use can be considered controversial, especially in patients with low RAIU. According to our results, RIT is justifiable when it allows for the extension or reintroduction of AM therapy.22 The prevention or treatment of AIT by RIT, despite low RAIU, appears to be safe and effective, especially in patients who require a steady administration of AM.40 Hence, we have undertaken to apply a preventive dose of RIT as the treatment of choice for AIT. In the future, it would be interesting to evaluate the quality of life in this very small focus group of patients.
Conclusion
In conclusion, AIT is complicated and requires strict cooperation between cardiologists and endocrinologists. Our research has shown that RIT can be a safe and effective modality for the treatment of AIT. RAI administration is recommended in particular circumstances, even in euthyroid patients, because it opens up the possibility of continuing, reintroducing, and/or adhering to long-term AM treatment. Therefore, RIT helps control life-threatening tachyarrhythmias and decreases the possibility of thyrotoxicosis that can occur in association with AM.
Disclosure
The authors report no conflicts of interest in this work.
References
Roy D, Talajic M, Dorian P, et al. Amiodarone to prevent recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators. N Engl J Med. 2000;342:913–920. | ||
Siddoway LA. Amiodarone: guidelines for use and monitoring. Am Fam Physician. 2003;68:2189–2196. | ||
McEvoy GK. AHFS Drug Information 2000. Bethesda, MD: American Society of Health-System Pharmacist; 2000. | ||
Basaria S, Cooper DS. Amiodarone and the thyroid. Am J Med. 2005;118:706–714. | ||
Bogazzi F, Bartalena L, Gasperi M, Braverman LE, Martino E. The various effects of amiodarone on thyroid function. Thyroid. 2001;11:511–519. | ||
Hosaka F, Shiga T, Sakomura Y, Wakaumi M, Matsuda N, Kasanuki H. Amiodarone distribution in human tissues after long-term therapy: a case of arrhythmogenic right ventricular cardiomyopathy. Heart Vessels. 2002;16:154–156. | ||
Reiffel JA, Estes NA 3rd, Waldo AL, Prystowsky EN, DiBianco R. A consensus report on antiarrhythmic drug use. Clin Cardiol. 1994;17:103–116. | ||
Harjai KJ, Licata AA. Effects of amiodarone on thyroid function. Ann Intern Med. 1997;126:63–73. | ||
Iudica-Souza C, Burch HB. Amiodarone-induced thyroid dysfunction. Endocrinologist. 1999;9:216–227. | ||
Martino E, Bartalena L, Bogazzi F, Braverman LE. The effects of amiodarone on the thyroid. Endocr Rev. 2001;22:240–254. | ||
Wiersinga WM. Amiodarone and the thyroid. In: Weetman AP, Grossman A, editors. Pharmacotherapeutics of the Thyroid Gland. Berlin: Springer Verlag; 1997:225–287. | ||
Bartalena L, Bogazzi F, Martino E. Amiodarone-induced thyrotoxicosis: a difficult diagnostic and therapeutic challenge. Clin Endocrinol (Oxf). 2002;56:23–24. | ||
Jabrocka-Hybel A, Bednarczuk T, Bartalena L, et al. Amiodarone and the thyroid. Endokrynol Pol. 2015;66:176–186. | ||
Bogazzi F, Tomisti L, Bartalena L, Aghini-Lombardi F, Martino E. Amiodarone and the thyroid: a 2012 update. J Endocrinol Invest. 2012;35:340–348. | ||
Connolly SJ, Camm AJ, Halperin JL, et al. Dronedaron in high-risk permanent atrial fibrillation. N Engl J Med. 2011;365:2268–2276. | ||
Bogazzi F, Bartalena L, Brogioni S, et al. Color flow Doppler sonography rapidly differentiates type I and type II amiodarone-induced thyrotoxicosis. Thyroid. 1997;7:541–545. | ||
Ruchała M, Szczepanek E. Thyroid ultrasound – a piece of cake? Endokrynol Pol. 2011;61:330–344. | ||
Chiovato L, Martino E, Tonacchera M, et al. Studies on the in vitro cytotoxic effect of amiodarone. Endocrinology. 1994;134:2277–2282. | ||
Di Matola T, D’Ascoli F, Fenzi G, et al. Amidarone induces cytochrome c release and apoptosis through an iodine-independent mechanism. J Clin Endocrinol Metab. 2000;85:4323–4330. | ||
Eskes SA, Wiersinga WM. Amiodarone and thyroid. Best Pract Res Clin Endocrinol Metab. 2009;23:735–751. | ||
Eskes SA, Endert E, Fliers E, et al. Treatment of amiodarone-induced thyrotoxicosis type 2: a randomized clinical trial. J Clin Endocrinol Metab. 2012;97:499–506. | ||
Czarnywojtek A, Warmuz-Stangierska I, Woliński K, et al. Radioiodine therapy in patients with type II amiodarone-induced thyrotoxicosis. Pol Arch Med Wewn. 2014;23:695–703. | ||
Pearce EN, Bogazzi F, Martino E, et al. The prevalence of elevated serum C-reactive protein levels in inflammatory and noninflammatory thyroid disease. Thyroid. 2003;13:643–648. | ||
Czarnywojtek A, Owecki M, Zgorzalewicz-Stachowiak M, et al. The role of serum C-reactive protein measured by high-sensitive method in thyroid disease. Arch Immunol Ther Exp (Warsz). 2014;6:501–509. | ||
Bartalena L, Brogioni S, Grasso L, et al. Interleukin-6: a marker of thyroid-destructive processes? J Clin Endocrinol Metab. 1994;79:1424–1427. | ||
Czarnywojtek A, Zgorzalewicz-Stachowiak M, Wasko R, et al. Patients with chronic hepatitis type C and interferon-alpha-induced hyperthyroidism in two-years clinical follow-up. Neuro Endocrinol Lett. 2013;34:154–161. | ||
Roti E, Minelli R, Gardini E, Bianconi L, Braverman LE. Thyrotoxicosis followed by hypothyroidism in patients treated with amiodarone. A possible consequence of a destructive process in the thyroid. Arch Intern Med. 1993;153:886–892. | ||
Bartalena L, Wiersinga WM, Tanda ML, et al. Diagnosis and management of amiodarone-induced thyrotoxicosis in Europe: results of an international survey among members of the European Thyroid Association. Clin Endocrinol (Oxf). 2004;61:494–502. | ||
Tanda ML, Piantanida E, Lai A, et al. Diagnosis and management of Amiodarone-induced thyrotoxicosis: similarities and differences between North American and European thyroidologists. Clin Endocrinol. 2008;69:812–818. | ||
Bogazzi F, Tomisti L, Rossi G, et al. Glucocorticoids are preferable to thionamides as first-line treatment for amiodarone-induced thyrotoxicosis due to destructive thyroiditis: a matched retrospective cohort study. J Clin Endocrinol Metab. 2009;94:3757–3762. | ||
Reichert LJ, de Rooy HA. Treatment of amiodarone induced hyperthyroidism with potassium perchlorate and methimazole during amiodarone treatment. Br Med J. 1989;298:1547–1548. | ||
Bogazzi F, Miccoli P, Berti P, et al. Preparation with iopanoic acid rapidly controls thyrotoxicosis in patients with amiodarone-induced thyrotoxicosis before thyroidectomy. Surgery. 2002;132:1114–1147. | ||
Farwell AP, Abend SL, Huang SK, Patwardhan NA, Braverman LE. Thyroidectomy for amiodarone-induced thyrotoxicosis. JAMA. 1990;263:1526–1528. | ||
Meurisse M, Hamoir E, D’Silva M, Joris J, Hennen G. Amiodarone-induced thyrotoxicosis: is there a place for surgery? World J Surg. 1993;17:622–626. | ||
Hermida JS, Tcheng E, Jarry G, et al. Radioiodine ablation of the thyroid to prevent recurrence of amiodarone-induced thyrotoxicosis in patients with resistant tachyarrhythmias. Europace. 2004;6:169–174. | ||
Iskandar SB, Jordan RM, Peiris AN. Treating amiodarone-induced thyrotoxicosis with radioactive iodine. Tenn Med. 2004;97:408–410. | ||
Albino CC, Paz-Filho G, Graf H. Recombinant human TSH as an adjuvant to radioiodine for the treatment of type 1 amiodarone-induced thyrotoxicosis (AIT). Clin Endocrinol (Oxf). 2009;70:810–811. | ||
Bogazzi F, Tomisti L, Ceccarelli C, Martino E. Recombinant human TSH as an adjuvant to radioiodine for the treatment of type 1 amiodarone-induced thyrotoxicosis: a cautionary note. Clin Endocrinol (Oxf). 2010;72:133–134. | ||
O’Sullivan AJ, Lewis M, Diamond T. Amiodarone-induced thyrotoxicosis: left ventricular dysfunction is associated with increased mortality. Eur J Endocrinol. 2006;154:533–536. | ||
Czarnywojtek A, Zgorzalewicz-Stachowiak M, Woliński K, et al. Results of preventive radioiodine therapy in euthyroid patients with history of hyperthyroidism prior to administration of amiodarone with permanent atrial fibrillation-a preliminary study. Endokrynol Pol. 2014;65:269–274. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.