")
Back to Journals » Cancer Management and Research » Volume 11
Dynamic impact of inflammation-based indices in colorectal cancer patients receiving FOLFOX-based chemotherapy
Authors Tao Y , Yuan D, Pang H, Wu H, Liu D, Jin N, Wu N, Qiu J, Cao Y
Received 24 October 2018
Accepted for publication 20 February 2019
Published 10 April 2019 Volume 2019:11 Pages 2817—2829
DOI https://doi.org/10.2147/CMAR.S191712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Yong Tao,1 Danping Yuan,1 Hongshuang Pang,1 Hongbiao Wu,1 Dongfang Liu,1 Ningning Jin,1 Ningning Wu,1 Jianming Qiu,2 Yuepeng Cao1
1Department of Colorectal Surgery, Ningbo City First Hospital, Ningbo, Zhejiang, 86-315000, People’s Republic of China; 2Department of Colorectal Surgery, Hangzhou Third People’s Hospital, Hangzhou, 86-310009, People’s Republic of China
Background: Inflammatory cellular response is implicated in the pathogenesis of colorectal cancer (CRC). Nevertheless, the dynamic effects of inflammatory index coNLR (neutrophil-to-lymphocyte ratio)-PLR (platelet-to-lymphocyte ratio) during chemotherapy remain elusive.
Methods: The baseline clinical data and laboratory parameters of 480 CRC patients who received palliative resection of primary tumors and FOLFOX-based chemotherapy from January 2007 to January 2013 were retrospectively analyzed. Receiver operating characteristic curves were plotted to obtain the predictive NLR and PLR values, and to calculate the coNLR-PLR score. The Kaplan–Meier method was used to estimate the rates of recurrence-free survival (RFS) and overall survival (OS), and the Cox proportional hazards model was employed for analysis.
Results: The dynamic cut-off values of NLR during four periods of chemotherapy were 3.029, 2.466, 2.102 and 1.795, respectively, and those of PLR were 216.438, 187.572, 169.027 and 174.368, respectively. A higher coNLR-PLR was significantly associated with lower rates of RFS and OS (P<0.05). Both univariate and multivariate analyses showed that coNLR-PLR was a significant independent prognostic factor for RFS and OS (P<0.05).
Conclusions: CoNLR-PLR was a significant prognostic predictor for CRC patients who received FOLFOX-based chemotherapy. Evaluating this index can accurately predict the clinical treatment outcomes after chemotherapy.
Keywords: colorectal cancer, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, FOLFOX-based chemotherapy, coNLR-PLR
Introduction
Recently, colorectal cancer (CRC) has become the third most frequent malignant tumor worldwide and the fourth deadliest cancer due to recurrence and metastasis.1 In China, patients diagnosed as advanced CRC account for approximately 6–8% of malignancies. Accumulating evidence has confirmed that the overall survival (OS) and recurrence-free survival (RFS) of patients with locally advanced CRC can be improved through perioperative chemotherapy besides surgical resection (R0).2–4 Regardless of improvements of surgical methods and combined chemotherapeutic regimens, the prognostic outcomes remain unsatisfactory.5 Conventionally, clinical and pathological characteristics, including high cancer stage, inadequate sampling from lymph nodes, poorly differentiated histology and lymph-vascular invasion, have been identified as significant risk factors for poor prognosis.6 The guidelines of the National Comprehensive Cancer Network (NCCN) recommend using adjuvant chemotherapy to prevent postoperative tumor recurrence. However, these traditional markers may sometimes be incapable of accurate prediction of the prognosis. Therefore, it is of great significance to find easily available and reliable prognostic factors for distinguishing high-risk cases and providing the optimum chemotherapeutic strategy, aiming to further enhance the therapeutic effects.
Several retrospective studies have revealed that adjuvant chemotherapy caused severer systemic inflammatory reaction and weaker adaptive immune response, bringing about an imbalance between inflammation and malignant tumor to stimulate cancer progression and recurrence.7,8 Predictive peripheral blood factors of inflammatory response include counts of neutrophils, white blood cells, monocytes, lymphocytes and platelets, together with expressions of acute-phase proteins. Moreover, platelet-to-lymphocyte ratio (PLR) and neutrophil-to-lymphocyte ratio (NLR) are well-known biomarkers closely associated with the survival of patients with biliary tract cancer, gastric cancer, ovarian cancer and CRC.9–12 Nevertheless, the roles of the two inflammatory indices remain controversial.13,14
To verify the predictive values of these biomarkers, we proposed a novel prognostic scoring system (coNLR-PLR) that combined NLR with PLR to evaluate the prognosis of CRC patients more accurately. We then employed this system to explore the potential role in augmenting the predictive capacity for the prognosis of chemotherapy.
Materials and methods
The study has been approved by the ethics committee of No. 3 Hangzhou People’s Hospital, and was performed in compliance with the standards of the Declaration of Helsinki. Before the study started, written informed consent has been obtained from all patients.
Selection of patients
A total of 480 patients with primary CRC, who received postoperative FOLFOX-based chemotherapy in Department of Colorectal Surgery, No. 3 Hangzhou People’s Hospital from January 2007 to January 2013, were enrolled and retrospectively analyzed. Inclusion criteria: (1) Patients who received surgical resection for CRC and were pathologically defined as TNM stage III/IV; (2) without hematological diseases, infections, renal dysfunction or hyperpyrexia; (3) without using drugs including NSAIDs; (4) without inflammation-related diseases or vascular disorders; (4) without receiving radiotherapy, chemotherapy or any other targeted therapies.
Protocol for adjuvant chemotherapy according to NCCN guidelines
All patients received adjuvant chemotherapy with the FOLFOX regimen according to the NCCN guidelines. FOLFOX regimen: 85 mg/m2 oxaliplatin, 200 mg/m2 calcium levofolinate and 400 mg/m2 bolus 5-fluorouracil (5-FU), all on day 1; infusion with 2,400 mg/m2 5-FU on days 1–3. The regimen was performed once every 2 weeks, 12 cycles in total.
Clinical, pathological and laboratory data
To determine the predictive value, we collected the clinical, pathological and laboratory data of patients before receiving the 1st, 4th, 8th and 12th cycles of adjuvant chemotherapy. The clinical and pathological characteristics, such as gender, age, body mass index (BMI), as well as tumor site, differentiation, TNM stage and histological type, were collected from the medical records. Laboratory measurements were performed on the day before chemotherapy, which included counts of neutrophils, white blood cells, lymphocytes and platelets, as well as expressions of some biochemical factors such as serum carbohydrate antigen 199 (CA199), carcinoembryonic antigen (CEA) and C-reactive protein (CRP). Furthermore, the ratio of absolute count of neutrophils to that of lymphocytes was defined as NLR, and the ratio of absolute count of platelets to that of lymphocytes was defined as PLR.
NLR and PLR scoring method
Based on the optimum cut-off value obtained from the receiver operating characteristic (ROC) curve, the score of NLR was 1 or 0 when patient had a high or low NLR during each chemotherapy. Likewise, the score of PLR was 1 or 0 in the case of a high or low PLR. During the same period of chemotherapy, coNLR-PLR, ie, the combined score, was assigned a score of 1 when patient had a high NLR or PLR and a score of 0 when both values were low. Also, the score was 2 in the case of two high values. Therefore, the scores throughout the four periods of chemotherapy ranged from 0 to 8 scores. The coNLR-PLR scores during one period were defined as the sum of NLR and PLR scores.
Follow-up data of survival prognosis
Patients were regularly followed up through telephone calls and letters every 3–6 months until deadline or death. Colonoscopy and computed tomography were conducted at appointments during follow-up. Death was informed by outpatient medical records, social security death index of patient or notification from the family members. The time from the first day of palliative chemotherapy to recurrence or disease progression was defined as RFS, and the time from the first day of palliative chemotherapy to the last follow-up or death because of any reason was defined as OS. Follow-up was ended after January 1, 2018.
Statistical analysis
The best cut-off values for PLR and NLR as predictive markers for OS were determined by ROC analysis with the You-den Index. The association between PLR and NLR was analyzed by linear regression. The associations between coNLR-PLR score and pathological and clinical characteristics were assessed by the Fisher’s exact probability test or Chi-square test. To study prognosis, the Kaplan–Meier method was employed to calculate PFS and OS, with the differences compared by the log-rank test. Univariate and multivariate analyses were carried out by using the Cox proportional hazards model with 95% confidence interval to evaluate the effect of the above-mentioned characteristics and some significant prognostic factors (eg, PLR and NLR). P≤0.05 was considered statistically significant. All analyses were conducted using SPSS 11.5 for Windows.
Results
Patient characteristics and outcomes
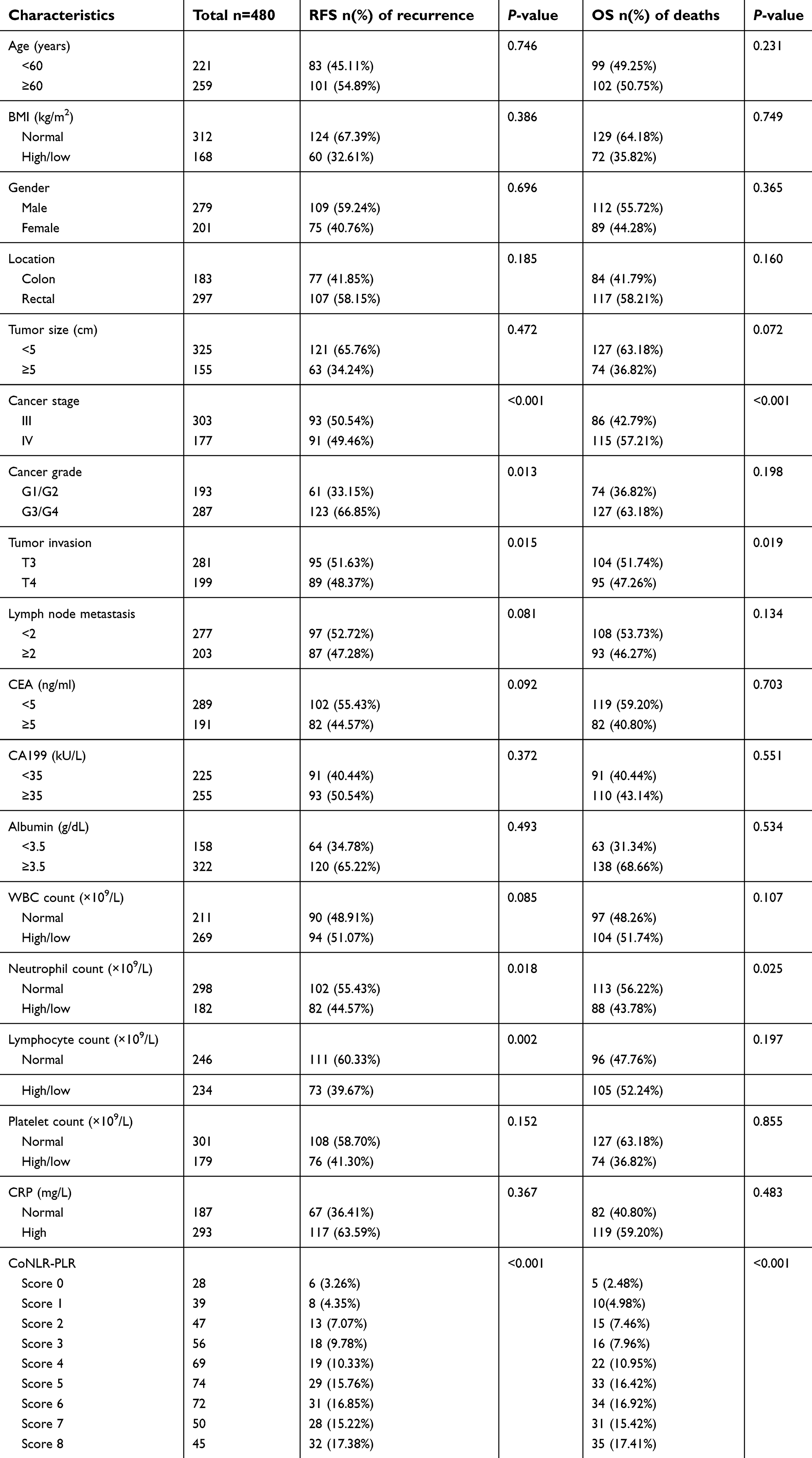
Table 1 summarizes the detailed clinical and pathological characteristics together with laboratory parameters of the 480 eligible patients. The average age was (62.7±18.19) years old, and the male/female ratio was 1.39. Of these patients, 297 and 183 were diagnosed as primary rectal cancer and colon cancer, respectively. Besides, 63.13% of the CRC patients were at stage III and 36.87% were at stage IV. The maximum size of primary lesion in 155 patients was 5 cm, and most tumors presented poorly differentiated histology (G3/G4) (59.79%). Most lesions of 281 patients (58.54%) reached an invasive depth of T3, and 203 patients (42.29%) were subjected to local nodal metastasis (≥2). The positive expression rates of serum CEA and CA199 were 60.21% and 53.13%, respectively. According to nutritional indices, a majority of the patients had normal BMI (65%) and high level of albumin (67.08%). With regard to laboratory parameters, the abnormal percentages of neutrophils, white blood cells, platelets, lymphocytes and CRP were 37.91%, 56.04%, 37.29%, 48.75% and 61.04%, respectively.
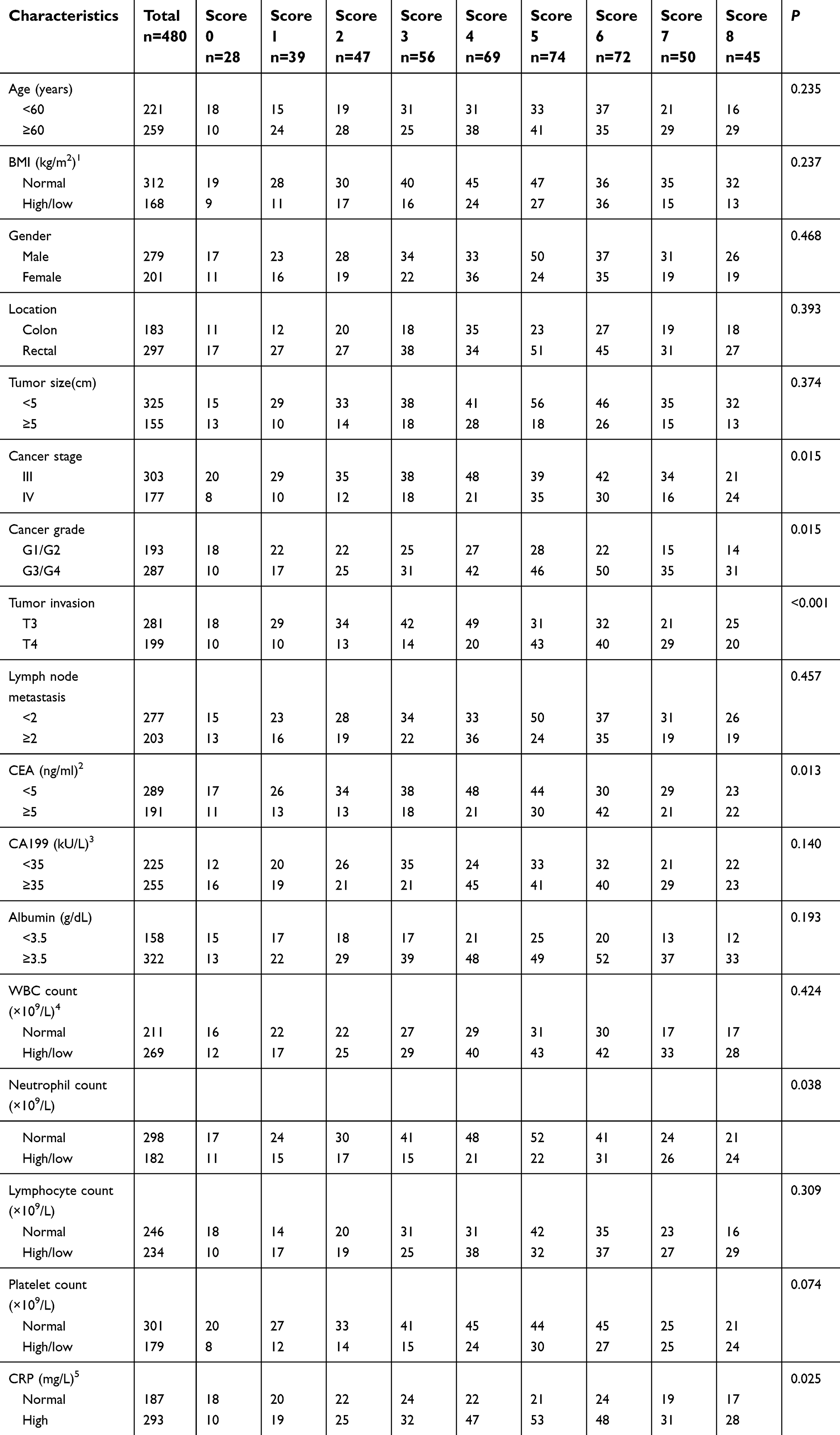 | Table 1 Relationships between clinical characteristics and coNLR-PLR |
Analysis of coNLR-PLR scoring system
Based on ROC curves, the optimum cut-off values of PLR and NLR for OS divided into four periods of chemotherapy were calculated (Figure 1). The optimum cut-off values of NLR were 3.029, 2.466, 2.102 and 1.795, respectively, and those of PLR were 216.438, 187.572, 169.027 and 174.368, respectively (Table 2). Clearly, these values gradually dropped, but the AUC values hardly changed. Then, linear regression analysis was performed to study whether there was significant correlation between NLR and PLR in each period (P<0.001) (Figure 2). Furthermore, NLR scores were more closely associated with coNLR-PLR scores during chemotherapy (Figure 3).
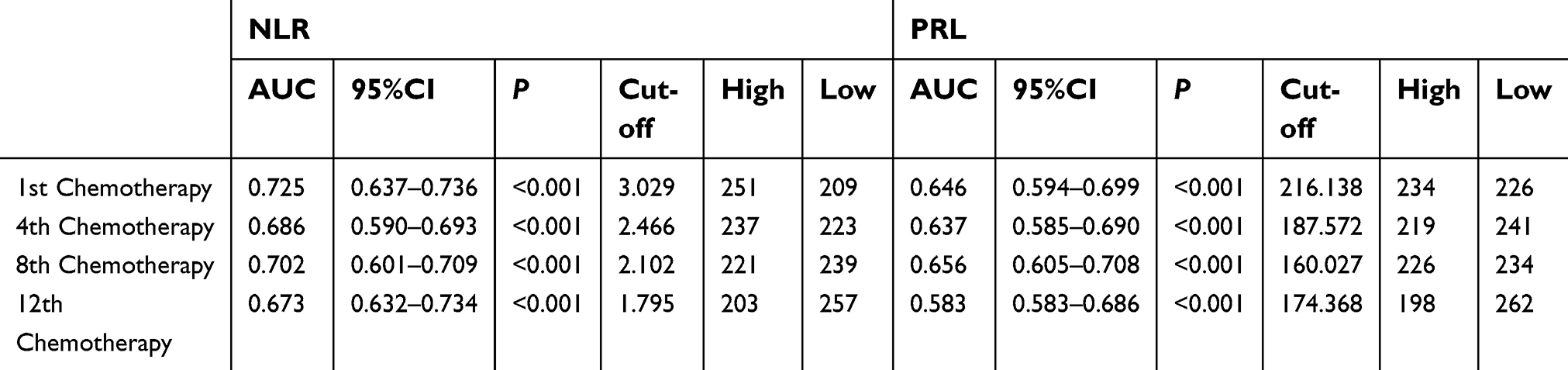 | Table 2 Combined score of NLR-PLR by ROC curve analysis |
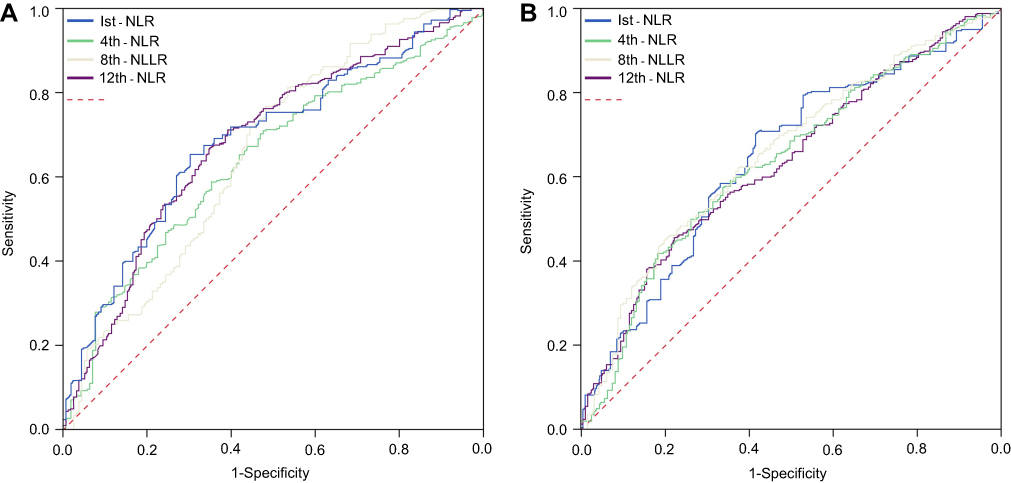 | Figure 1 Receiver operating characteristic curve analysis for OS and RFS between NLR and PLR in four periods of chemotherapy. (A) For NLR, the optimal cut-off values were 3.029, 2.466, 2.102 and 1.795 in periods of chemotherapy. (B) For PLR, the optimal cut-off values, respectively, were 216.138, 187.572, 160.027 and 171.368 in periods of chemotherapy. Abbreviations: NLR, neutrophil-to-lymphocyte; PLR, platelet-to-lymphocyte; ROC, receiver operating characteristic; AUC, area under the curve. |
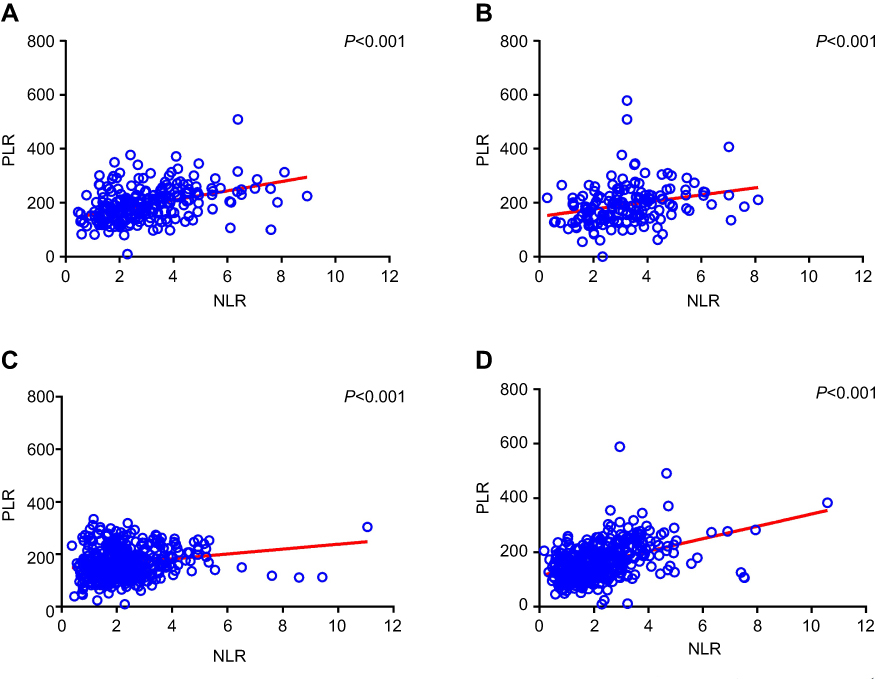 | Figure 2 Linear regression of NLR and PLR during the four periods of adjuvant chemotherapy. (A) During the 1st period, the linear correlation coefficient of NLR and PLR was 0.672 and P-value was less than 0.001. (B) During the 4th period, the linear correlation coefficient of NLR and PLR was 0.622 and P-value was less than 0.001. (C) During the 12th period, the linear correlation coefficient of NLR and PLR was 0.781 and P-value was less than 0.001. Abbreviations: RFS, recurrence-free survival; OS, overall survival; BMI, body mass index; CEA, carcinoembryonic antigen; CA199, carbohydrate antigen; WBC, white blood cells; CRP, C-reactive protein; coNLR-PLR, combined neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio. |
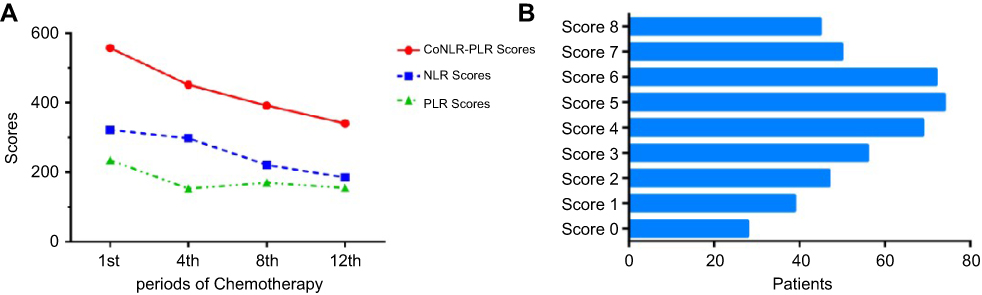 | Figure 3 Distribution between score and chemotherapy period. (A) According to the four periods, NLR score curve was closer to coNLR-PLR than PLR. (B) According to the coNLR-PLR score, distribution of the number of patients was in each score. Abbreviations: OS, overall survival; BMI, body mass index; CEA, carcinoembryonic antigen; CA199, carbohydrate antigen; WBC, white blood cells. |
Relationships of clinical characteristics with coNLR-PLR scores
Table 1 lists the baseline clinical characteristics according to coNLR-PLR scores. The age, BMI, gender, lymph node metastasis, tumor site and size, CA199 level, albumin level, white blood cell count, lymphocyte count and platelet count of all groups were similar (P>0.05). In contrast, cancer stage, grade, invasion, serum CEA level, neutrophil count and CRP level were significantly associated with coNLR-PLR scores (P<0.05). In detail, the patients with high scores had high cancer stage, grade, invasive capacity, serum CEA level, neutrophil count and CRP level. Collectively, high coNLR-PLR scores were closely related with poor prognosis.
Survival prognosis for each coNLR-PLR score
According to the follow-up results, 184 (38.33%) patients underwent recurrence, of whom 54 and 130 were subjected to local recurrence and distant metastasis, respectively. Additionally, 201 (44.79%) patients were dead due to tumor recurrence (169 cases), chemotherapeutic toxicity (2 cases) and unknown reasons. Table 3 lists the relationships of clinical characteristics with prognosis of RFS and OS. High cancer stage (IV), severe invasion (T4), abnormal neutrophil count (high/low) and evaluated coNLR-PLR scores had significant associations with poor OS and RFS (P<0.05). As suggested by the log-rank test and Kaplan–Meier curve, the median OS was significantly shortened with increasing coNLR-PLR score (P<0.001) (Figure 4A). Similarly, the median RFS also decreased as the coNLR-PLR score increased (P<0.001) (Figure 4B). Thus, patients can be effectively differentiated using the coNLR-NLR scoring system.
 | Table 3 Association of clinical baseline characteristics with RFS and OS |
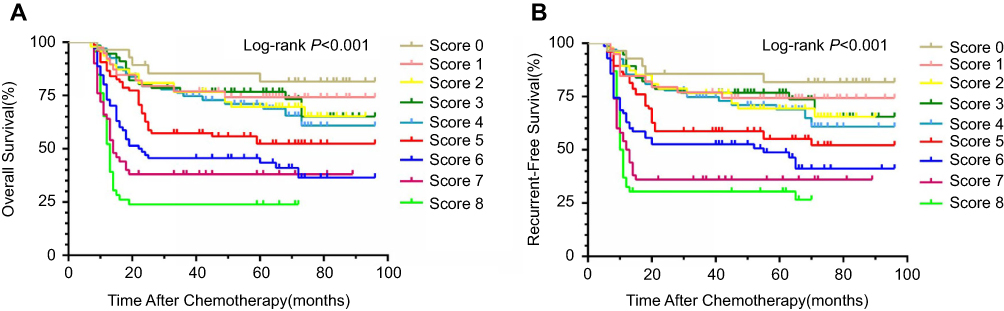 | Figure 4 Comparison of survival prognosis in each coNLR-PLR score. (A) For overall survival, patients with higher had poorer prognosis (log-rank p<0.001). (B) For recurrent-free survival, patients with higher had poorer prognosis (log-rank p<0.001). Abbreviations: RFS, recurrence-free survival; CEA, carcinoembryonic antigen; CA199, carbohydrate antigen; WBC, white blood cells; CRP, C-reactive protein. |
Independent prognostic value of elevated coNLR-PLR score for poor survival
Univariate and multivariate analyses were carried out for various parameters to identify independent factors for survival prognosis (Tables 4 and 5). Univariate analysis revealed that high cancer stage, low differentiation grade, severe invasion, lymph node metastasis, serum CEA level, neutrophil count and raised coNLR-PLR score were all significantly associated with both OS and RFS (P<0.05). Platelet count and serum CA199 were significantly associated with RFS (P<0.05) but not OS. Nevertheless, lymphocyte count was significantly associated with OS (P=0.037) instead of RFS. Subsequently, the significant factors (P<0.05) in univariate analysis were included in the Cox proportional hazards model for multivariate analysis. High cancer stage, severe invasion, lymph node metastasis and increased coNLR-PLR score had significant associations with poor prognosis of RFS and OS (P<0.05).
 | Table 4 Prognostic factors associated with OS in univariate and multivariate analysis |
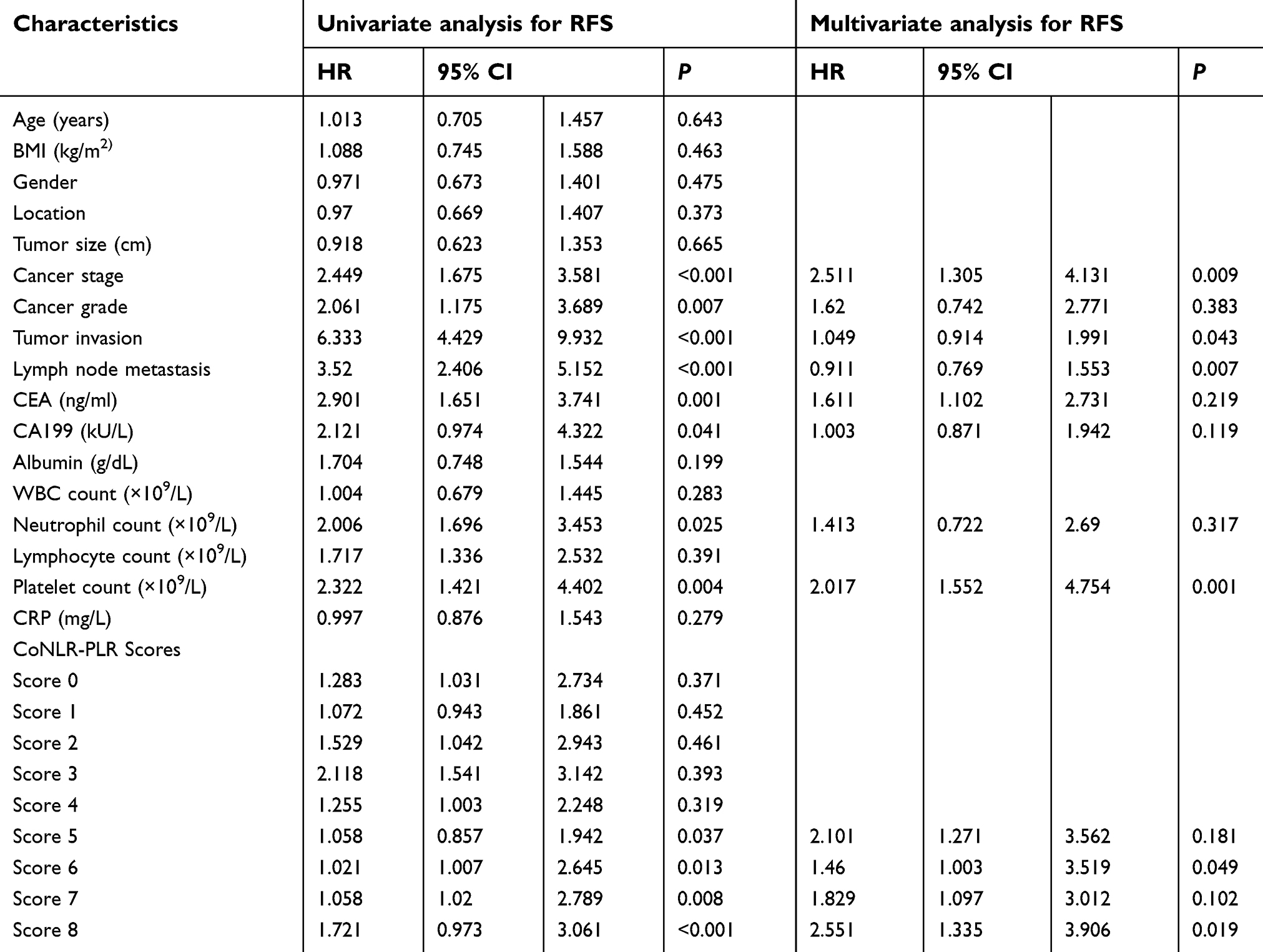 | Table 5 Prognostic factors associated with RFS in univariate and multivariate analysis |
Discussion
Because of persistent response to chronic inflammation, some predictive biomarkers can dynamically indicate the survival prognosis of patients receiving adjuvant chemotherapy.15 Cell factors in the peripheral blood, such as NLR and PLR, typically reflect the inflammatory status.16,17 In this study, we proposed a novel index combining NLR with PLR, which could accurately predict the survival prognosis of CRC patients receiving FOLFOX-based chemotherapy.
Researchers have endeavored to unravel the mechanisms for the inflammatory responses of malignant tumors for decades.18 The growth of tumor cells promotes the necrosis, hypoxia and injury of local tissues, thereby disturbing the homeostasis and activating immune responses. As a result, IL-1, IL-6, IL-8, vascular endothelial growth factor, tumor necrosis factor and some other pro-inflammatory cytokines are secreted by tumor cells and/or inflammatory cells related with tumors. These cytokines thereafter result in tumor growth, angiogenesis, metastasis and invasion, reverse adaptive immune responses, and boost the resistance to cytotoxic substances.19,20 Notably, elevated PLR and NLR were accompanied by increase of platelet and neutrophil counts but decrease of lymphocyte count, indicating that inflammatory responses associated with platelets and neutrophils were enhanced and the antitumor immune responses mediated by lymphocytes were attenuated.
In the presence of inflammatory signals, neutrophils are activated quickly and migrate to inflammatory sites.21 Because of chronic inflammation, the persistent stimulus to neutrophils aggravates oxidative stress that damages the epithelium and induces pro-mutagenic DNA lesions.22 Besides, neutrophils may suppress lymphocyte activity upon antitumor immune responses and promote remodeling of the extracellular matrix.23,24 Herein, neutrophil count was significantly associated with prognosis only in univariate analysis.
Baseline platelet count has been recognized as an index of chemotherapy prognosis for advanced CRC.25 Aggregation of platelets in the circulation is able to protect tumor cells from immune surveillance and shear stress by forming platelet cloaks.26 Moreover, chemoresistance can be triggered by platelets throughout epithelial–mesenchymal transition, direct protection, anti-apoptotic pathways mediated by PAI-1 or immunosuppression regulated by NKG2-D down-regulation.27 We herein assessed the predictive value of platelet count in CRC patients receiving chemotherapy, which was an independent factor for RFS only in univariate analysis.
Additionally, lymphocytes play an important role in antitumor immune responses.28 By changing the tumor microenvironment, lympho-depletion probably contributes to the attenuation of intestinal tumorigenesis and anti-tumor immune responses.29,30 Furthermore, lymphopenia has also been linked to elevated circulating IL-7 level that facilitates lymphangiogenesis, tumor proliferation, and metastasis.31 Hence, the CRC chemotherapy-related lymphopenia in this study may be partly explained.
Given that these inflammatory indices are intrinsically correlated, NLR and PLR before treatment are significant factors for predicting the responses of a variety of cancers to chemotherapy.32 Nevertheless, using only one index may bring about bias and risk in detection. Therefore, we employed a coNLR-PLR scoring system to analyze RFS and OS more accurately during four periods of FOLFOX-based chemotherapy. The coNLR-PLR score was calculated by adding up continuous cycles of optimum cut-off values according to ROC curve analysis, unlike the Glasgow prognostic score with three stratifications (0, 1 and 2).33 To the best of our knowledge, this is a rare study regarding the association between coNLR-PLR score and the prognosis of CRC patients receiving chemotherapy. This index was a significant independent prognostic factor, and a higher one suggested poorer prognosis for RFS and OS. Also, the coNLR-PLR scoring system was superior to NLR or PLR alone.
Similar to the results of literature before, factors related with cancer stage and invasion besides coNLR-PLR were also identified by univariate and multivariate analyses as significant prognostic indices.34,35 However, only univariate analysis showed that serum CEA and CA199 levels had associations with poor prognosis, which was contrary to a previous study.36 This inflammatory biomarker, which is facilely detectable, simple, objective, economical and reproducible, can be tested at the beginning of chemotherapy and dynamically monitored throughout the treatment process.37 As a complicated model, coNLR-PLR may provide more reliable prognostic evidence for clinicians.
Regardless, this study still has limitations. First, it is a single-center retrospective study. In addition, prospective studies are in need to clarify whether the proposed index can be incorporated into the stratification systems for patients with cancers to individualize treatment regimens.
Conclusion
In summary, we proposed a coNLR-PLR scoring system, as a novel index correlated independently with survival prognosis, and verified that peripheral blood cells dominantly bridged the interaction between cancer and host during adjuvant chemotherapy. Nevertheless, these findings ought to be validated by in-depth prospective studies.
Abbreviation list
CRC, colorectal cancer; BMI, body mass index; CEA, carcinoembryonic antigen; CA199, carbohydrate antigen; CRP, C-reactive protein; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; coNLR-PLR, combined neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio; NCCN, National Comprehensive Cancer Network; RFS, recurrence-free survival; OS, overall survival.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
The authors thank the members of Hangzhou Third People’s Hospital for Follow-up of Colorectal Cancer with FOLFOX Chemotherapy for collecting the clinical data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
2. Sun Z, Gilmore B, Adam MA, et al. Adjuvant chemotherapy after preoperative chemoradiation improves survival in patients with locally advanced rectal cancer. Dis Colon Rectum. 2017;60(10):1050–1056. doi:10.1097/DCR.0000000000000907
3. Markovina S, Youssef F, Roy A, et al. Improved metastasis- and disease-free survival with preoperative sequential short-course radiation therapy and FOLFOX chemotherapy for rectal cancer compared with neoadjuvant long-course chemoradiotherapy: results of a matched pair analysis. Int J Radiat Oncol Biol Phys. 2017;99(2):417–426. doi:10.1016/j.ijrobp.2017.05.048
4. Chapman BC, Hosokawa P, Henderson W, et al. Impact of neoadjuvant chemoradiation on perioperative outcomes in patients with rectal cancer. J Surg Oncol. 2017;115(8):1033–1044. doi:10.1002/jso.24613
5. van Eden WJ, Kok NF, Jóźwiak K, et al. Timing of systemic chemotherapy in patients with colorectal peritoneal carcinomatosis treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Dis Colon Rectum. 2017;60(5):477–487. doi:10.1097/DCR.0000000000000774
6. Szkandera J, Pichler M, Absenger G, et al. The elevated preoperative platelet to lymphocyte ratio predicts decreased time to recurrence in colon cancer patients. Am J Surg. 2014;208(2):210–214. doi:10.1016/j.amjsurg.2013.10.030
7. Huang A, Cao S, Tang L. The tumor microenvironment and inflammatory breast cancer. J Cancer. 2017;8(10):1884–1891. doi:10.7150/jca.17595
8. Jakubowska K, Kisielewski W, Kańczuga-Koda L, Koda M, Famulski W. Diagnostic value of inflammatory cell infiltrates, tumor stroma percentage and disease-free survival in patients with colorectal cancer. Oncol Lett. 2017;14(3):3869–3877. doi:10.3892/ol.2017.6639
9. Cho KM, Park H, Oh DY, et al. Neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and their dynamic changes during chemotherapy is useful to predict a more accurate prognosis of advanced biliary tract cancer. Oncotarget. 2017;8(2):2329–2341. doi:10.18632/oncotarget.13731
10. Wang F, Liu ZY, Xia YY, et al. Changes in neutrophil/lymphocyte and platelet/lymphocyte ratios after chemotherapy correlate with chemotherapy response and prediction of prognosis in patients with unresectable gastric cancer. Oncol Lett. 2015;10(6):3411–3418. doi:10.3892/ol.2015.3783
11. Miao Y, Yan Q, Li S, Li B, Feng Y. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are predictive of chemotherapeutic response and prognosis in epithelial ovarian cancer patients treated with platinum-based chemotherapy. Cancer Biomark. 2016;17(1):33–40. doi:10.3233/CBM-160614
12. Wu Y, Li C, Zhao J, et al. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios predict chemotherapy outcomes and prognosis in patients with colorectal cancer and synchronous liver metastasis. World J Surg Oncol. 2016;14(1):289–295. doi:10.1186/s12957-016-1044-9
13. Li H, Song J, Cao M, et al. Preoperative neutrophil-to-lymphocyte ratio is a more valuable prognostic factor than platelet-to-lymphocyte ratio for nonmetastatic rectal cancer. Int Immunopharmacol. 2016;40:327–331. doi:10.1016/j.intimp.2016.09.014
14. Kim EY, Lee JW, Yoo HM, Park CH, Song KY. The platelet-to-lymphocyte ratio versus neutrophil-to-lymphocyte ratio: which is better as a prognostic factor in gastric cancer? Ann Surg Oncol. 2015;22(13):4363–4370. doi:10.1245/s10434-015-4518-z
15. De Weerdt A, Dendooven A, Snoeckx A, Pen J, Lammens M, Jorens PG. Prognosis and treatment of FOLFOX therapy related interstitial pneumonia: a plea for multimodal immune modulating therapy in the respiratory insufficient patient. BMC Cancer. 2017;17(1):586. doi:10.1186/s12885-017-3576-y
16. Song X, Zhu H, Pei Q, et al. Significance of inflammation-based indices in the prognosis of patients with non-metastatic colorectal cancer. Oncotarget. 2017;8(28):45178–45189. doi:10.18632/oncotarget.16774
17. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):493–503. doi:10.1016/S1470-2045(14)70263-3
18. Luo C, Zhang H. The role of proinflammatory pathways in the pathogenesis of colitis-associated colorectal cancer. Mediators Inflamm. 2017;2017:5126048. doi:10.1155/2017/5126048
19. Samples J, Willis M, Klauber-Demore N. Targeting angiogenesis and the tumor microenvironment. Surg Oncol Clin N Am. 2013;22(4):629–639. doi:10.1016/j.soc.2013.06.002
20. Chen ZY, Raghav K, Lieu CH, et al. Cytokine profile and prognostic significance of high neutrophil-lymphocyte ratio in colorectal cancer. Br J Cancer. 2015;112(6):1088–1097. doi:10.1038/bjc.2015.61
21. Uyanik B, Grigorash BB, Goloudina AR, Demidov ON. DNA damage-induced phosphatase Wip1 in regulation of hematopoiesis, immune system and inflammation. Cell Death Discov. 2017;3:17018. doi:10.1038/cddiscovery.2017.18
22. Ocana A, Nieto-Jiménez C, Pandiella A, Templeton AJ. Neutrophils in cancer: prognostic role and therapeutic strategies. Mol Cancer. 2017;16(1):137. doi:10.1186/s12943-017-0707-7
23. Galdiero MR, Bianchi P, Grizzi F, et al. Occurrence and significance of tumor-associated neutrophils in patients with colorectal cancer. Int J Cancer. 2016;139(2):446–456. doi:10.1002/ijc.30076
24. Han S, Liu Y, Li Q, Li Z, Hou H, Wu A. Pre-treatment neutrophil-to-lymphocyte ratio is associated with neutrophil and T-cell infltration and predicts clinical outcome in patients with glioblastoma. BMC Cancer. 2015;15:617. doi:10.1186/s12885-015-1584-3
25. Passardi A, Scarpi E, Cavanna L, et al. Inflammatory indexes as predictors of prognosis and bevacizumab efficacy in patients with metastaticcolorectal cancer. Oncotarget. 2016;7(22):33210–33219. doi:10.18632/oncotarget.8901
26. Radziwon-Balicka A, Medina C, O’Driscoll L, et al. Platelets increase survival of adenocarcinoma cells challenged with anticancer drugs: mechanisms and implications for chemoresistance. Br J Pharmacol. 2012;167(4):787–804. doi:10.1111/j.1476-5381.2012.01991.x
27. Lopez-Soto A, Huergo-Zapico L, Acebes-Huerta A, Villa-Alvarez M, Gonzalez S. NKG2D signaling in cancer immunosurveillance. Int J Cancer. 2015;136(8):1741–1750. doi:10.1002/ijc.28775
28. Lucas C, Barnich N, Nguyen HTT. Microbiota, inflammation and colorectal cancer. Int J Mol Sci. 2017;18(6):45–55.
29. Berntsson J, Svensson MC, Leandersson K, et al. The clinical impact of tumour- infiltrating lymphocytes in colorectal cancer differs by anatomical subsite: a cohort study. Int J Cancer. 2017;141(8):1654–1666. doi:10.1002/ijc.30869
30. Mei Z, Liu Y, Liu C, et al. Tumour-infiltrating inflammation and prognosis in colorectal cancer: systematic review and meta-analysis. Br J Cancer. 2014;110(6):1595–1605. doi:10.1038/bjc.2014.46
31. Lin J, Zhu Z, Xiao H, et al. The role of IL-7 in immunity and cancer. Anticancer Res. 2017;37(3):963–967. doi:10.21873/anticanres.11405
32. Dolan RD, McSorley ST, Horgan PG, Laird B, McMillan DC. The role of the systemic inflammatory response in predicting outcomes in patients with advanced inoperable cancer: systematic review and meta-analysis. Crit Rev Oncol Hematol. 2017;116:134–146. doi:10.1016/j.critrevonc.2017.06.002
33. Eren T, Burcu B, Tombalak E, et al. Clinical significance of the glasgow prognostic score for survival after colorectal cancer surgery. J Gastrointest Surg. 2016;20(6):1231–1238. doi:10.1007/s11605-016-3114-2
34. Kim JH, Lee JY, Kim HK, et al. Prognostic significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in patients with stage III and IV colorectal cancer. World J Gastroenterol. 2017;23(3):505–515. doi:10.3748/wjg.v23.i3.505
35. Jia J, Zheng X, Chen Y, et al. Stage-dependent changes of preoperative neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in colorectal cancer. Tumour Biol. 2015;36(12):9319–9325. doi:10.1007/s13277-015-3667-9
36. Chu-Yuan H, Jing P, Yi-Sheng W, et al. The impact of chemotherapy- associated neutrophil/lymphocyte counts on prognosis of adjuvant chemotherapy in colorectal cancer. BMC Cancer. 2013;3(13):177. doi:10.1186/1471-2407-13-177
37. Tohme S, Sukato D, Chalhoub D, McDonald KACA, Zajko A, Amesur N. Neutrophillymphocyte ratio is a simple and novel biomarker for prediction of survival after radioembolization for metastatic colorectal cancer. Ann Surg Oncol. 2015;22:1701–1707. doi:10.1245/s10434-014-4050-6
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.