")
Back to Journals » Infection and Drug Resistance » Volume 15
Durability of Antibody Response Against Hepatitis B Virus for a Decreased Crowd: A Retrospective Polycentric Cohort Study from a 10-Year Follow-Up Clinical Study
Authors He P , Xia J, Zhang P, Yang W, Xia Z, Liu P, Zhu Y , Fang Y, Zhang Z , Shen J
Received 12 October 2022
Accepted for publication 2 December 2022
Published 14 December 2022 Volume 2022:15 Pages 7389—7399
DOI https://doi.org/10.2147/IDR.S392262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Pei He,1,2 Jie Xia,3 Peixin Zhang,3 Wensu Yang,1,2 Zhaoxin Xia,1,2 Ping Liu,4 Yi Zhu,1,2 Yaping Fang,5 Zhenhua Zhang,3 Jilu Shen1,2
1Department of Laboratory Medicine, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Department of Laboratory Medicine, Anhui Public Health Clinical Center, Hefei, People’s Republic of China; 3Department of Infectious Diseases, The Second Hospital of Anhui Medical University, Hefei, People’s Republic of China; 4Department of Infectious Diseases, People’s Hospital of Jieshou City, Fuyang, People’s Republic of China; 5Department of Clinical Laboratory, The Second Hospital of Anhui Medical University, Hefei, People’s Republic of China
Correspondence: Zhenhua Zhang; Jilu Shen, Email [email protected]; [email protected]
Aim: Hepatitis B surface antibody (HBsAb) plays an important role in the prevention of hepatitis B virus (HBV) infection, especially in immunocompromised individuals and in those infected with HBV.HBsAb levels often fluctuate and decrease.This study aimed to determine the regularity of HBsAb persistence among different populations. Moreover, the risk factors and the optimal cutoff value were determined to predict a decreasing population in HBsAb level.
Methods: The study involved 182 participants, including 76 patients with a 25% decrease in HBsAb levels and 106 patients with an HBsAb decrease rate of > 50%. Both hepatitis B core antibody negative and positive patients were included.These patients were followed up for 10 years. The follow-up demographic and laboratory data were recorded and compared among the groups. Fluctuations in HBsAb data and HBsAb persistent immunity were evaluated. The independent factors and the optimal cutoff value were recorded.
Results: The first HBsAb median of Group 4 was lower than that of the other groups, and its median was 50.8 mlU/mL. In addition, the persistent immunity of the case groups was shorter than that of the control groups (p < 0.05). Furthermore, previous HBV history, use of antiviral drugs, and low levels of first HBsAb were independent risk factors in people with obviously decreased antibody levels. Also, when the optimum cutoff value on the receiver operating characteristic curve of the HBsAb difference value was taken as 8.53 mIU/mL, its sensitivity and specificity were 94% and 70% between the control and case groups, respectively.
Conclusion: To maintain optimal immunity against HBV infection, patients with a previous HBV history, those taking antiviral drugs, and/or those with low levels of HBsAb should be reimmunized with the hepatitis B vaccine in a timely manner.
Keywords: a decreasing population, durability of HBsAb response, independent risk factors, optimal cutoff value
Introduction
Hepatitis B virus (HBV) infection is a global public health problem. The implementation of universal HBV vaccination programs has helped in reducing the incidence of acute and chronic HBV infections, liver cirrhosis and hepatocellular carcinoma.1 However, breakthrough HBV infections in vaccinated individuals are emerging and are caused by rheumatoid arthritis,2 autoimmune inflammatory rheumatic disease,3 hematological system diseases,4 organ transplantation,5,6 etc. Such breakthrough infections can even increase the occurrence of occult hepatitis B infection.7
In addition, HBV reactivation (HBVr) can occur owing to the presence of latent covalently closed circular DNA (cccDNA) in the liver if the individual has a weak immune system. The abovementioned diseases suppress immunity and cause HBVr. In a previous study, a child who had been vaccinated and had undergone liver transplantation was found to be positive for hepatitis B surface antigen (HBsAg) after 27 months.8 In patients with cancer, HBV reactivation can block chemotherapy and exert a negative impact on prognosis.9 The risk status of HBV reactivation is caused by the durability of host immunity, viral factors, treatment protocols, and doses.10 HBV reactivation can cause liver injury and low immunity because of viral replication.11 Briefly, HBV cccDNA may persist after HBsAg becomes negative, thus resulting in HBV reactivation. HBV reactivation can occur spontaneously or during follow-up of patients after HBV-related disease therapy, such as immunosuppressive therapy, solid organ transplantation, and/or autoimmune disease treatment.12
The durability of the hepatitis B surface antibody (HBsAb) response is influenced by several factors. First, the durability of the response is different in various age groups.13 Advanced age (>60 years) is a risk factor for seroconversion.14 Second, hematopoietic stem-cell transplantation patients and donors should be vaccinated against HBV before the surgery.15 Third, transplanted livers come from hepatitis B core antibody (anti-HBc)-positive donors at times, thus leading to de novo hepatitis B.16
Combined with clinical considerations, the presence of anti-HBc is considered a sensitive lifetime marker for HBV infection. Little is known about HBVr and fluctuations in the HBsAb levels in the immunosuppressive, solid organ transplantation, and/or autoimmune diseases. This study aimed to compare persistent HBsAb immunity and identify the risk factors for plummeting HBsAb levels. The study further intended to determine an optimal cutoff value to predict an obviously decreasing population.
Materials and Methods
Patients Selection and Study Design
This retrospective, polycentric, longitudinal study was conducted from September 2011 to July 2021 at two hospitals, namely, the People’s Hospital of Jieshou city and the Second Hospital of Anhui Medical University. This study was conducted in accordance with the ethical principles specified in the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of Anhui Medical University, and all patients provided written informed consent.
The inclusion criteria were participants who were HBsAb(+) at the baseline and whose HBsAb levels were tested at least twice. The patients were screened within a 25% reduction of the HBsAb level and >50% decline. In the screening test, all study subjects were required to have undergone HBV serological tests for HBsAg, HBeAg, HBsAb, anti-HBe, and anti-HBc that were qualitatively analyzed. The exclusion criteria specified participants who were infected with HIV, HAV, HCV, HDV, or HEV viruses. In addition, the HBsAb level increased over time.
When combined with our research concept, these members were classified into 4 groups based on the status of anti-HBc and HBsAb: Group 1 comprised a decreasing HBsAb <25% of participants who had the status of anti-HBc(-)HBsAb(+). Group 2 comprised a decreasing HBsAb <25% of participants who had the status of anti-HBc(+)HBsAb(+). Group 3 comprised a decreasing HBsAb >50% of participants who had the status of anti-HBc(-)HBsAb(+). Finally, Group 4 comprised a decreasing HBsAb >50% of participants who had the status of anti-HBc(+)HBsAb(+). Finally, groups 1 and 2 served as the control groups. Groups 3 and 4 served as the case groups. Moreover, the endpoint was the loss of protective immunity, including the falling standards in the control and case groups (Figure 1).
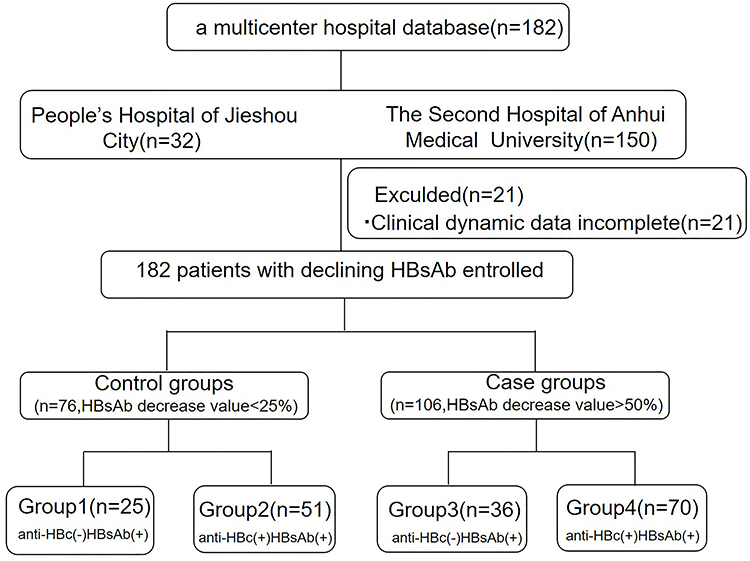 |
Figure 1 Flow chart depicting the numbers of decreasing crowd screened and enrolled in the study (at the time of enrollment). A declined response to HBsAb indicated that the anti-hepatitis B surface antibody (HBsAb) levels of the recipients were >50% of the baseline levels (first). |
Follow-Up Demographic and Laboratory Measurements
The follow-up information, consisting of family history of HBV B infection, HBV previous history, blood system diseases, the use of antiviral drugs, and immunosuppressors and organ transplantation, was obtained via telephonic interview and by using the doctor workstation system. In addition, all clinical indicators, such as HBsAg, HBeAg, HBsAb, anti-HBe, and anti-HBc, were quantified at the baseline (first) and then at the end (second) through chemiluminescence particle imaging (i2000SR, Sligo, Ireland).
Statistical Analysis
Data analysis was performed using SPSS version 27 software (SPSS, IBM, Chicago, USA). Univariate logistic regression analysis was adopted to verify the independent factors for case group diagnosis. The survival analysis between groups was assessed by using GraphPad Prism 8.0. Differences in all tests showing P < 0.05 were considered to indicate statistical significance.
Results
Clinical Characteristics of the Study Population
Table 1 shows the baseline demographics and clinical follow-up characteristics of the 182 patients. These patients were categorized into four groups. According to the follow-up results, the HBsAg interval between the descent and the use of antiviral drugs was significant (P < 0.05). Furthermore, family histories of HBV infection were considered significant (P < 0.01). In addition, age, previous HBV history, HBeAg, HBeAb, anti-HBc, first-HBsAb levels, and HBsAb difference values at two different times for a decreased population were evidently different (P < 0.001).
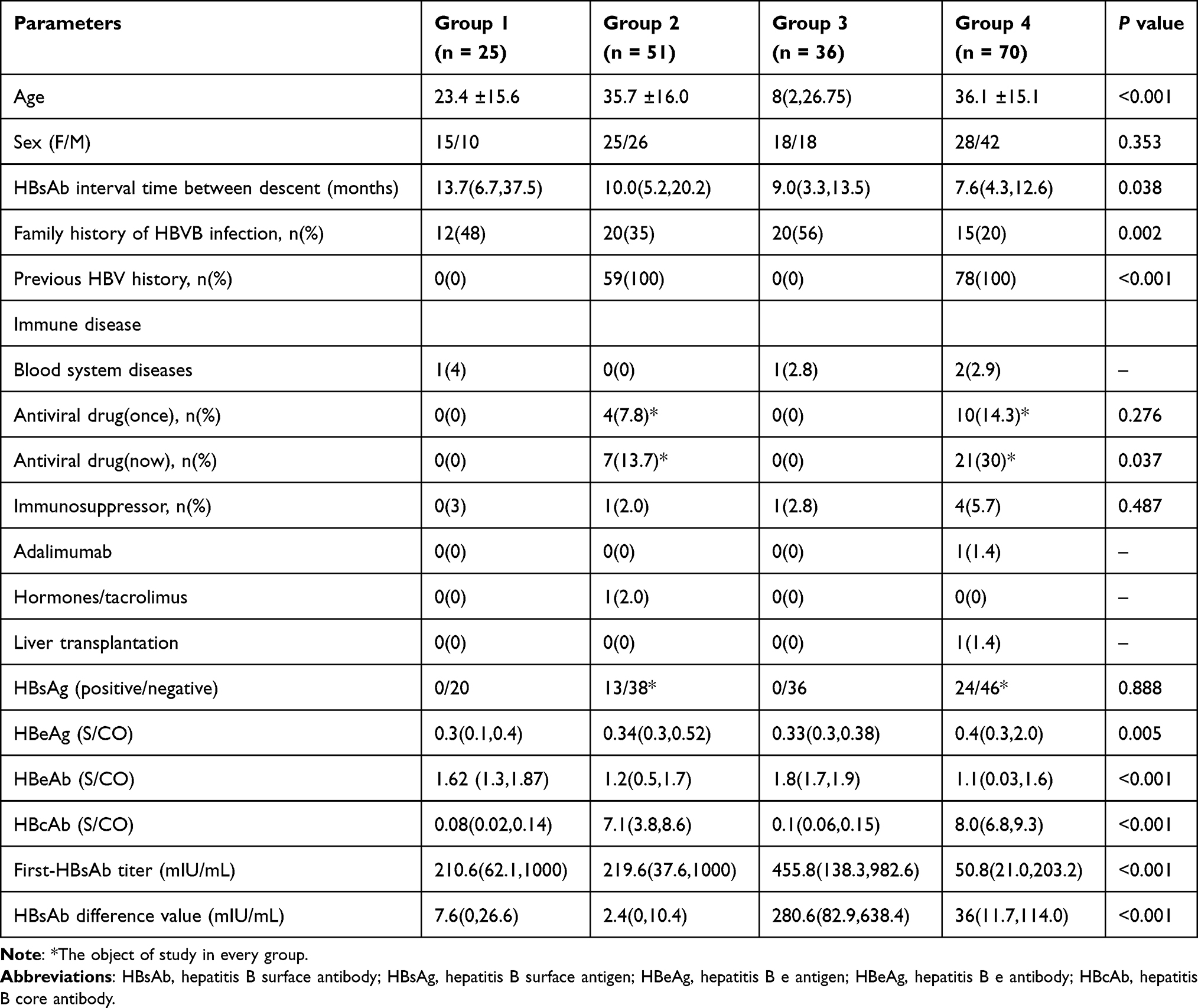 |
Table 1 Baseline Demographics and Clinical Characteristics of the Study Population |
Comparison and Distribution of Fluctuations in HBsAb Levels Among the Groups
To assess the fluctuations in HBsAb levels among the groups, independent-samples
t-test was used to compare the groups. Overall, the HBsAb median levels of Group 4 were lower than the first-HBsAb levels of the other groups, and the comparison was different at baseline than in the control groups (P < 0.01), with a median of 50.8 mlU/mL (Figure 2A). After the HBsAb level decreased (HBsAb-second), the data suggested that Group 4 was obviously significantly different (P < 0.0001) (Figure 2B). Moreover, the HBsAb fluctuation in Group 3 was the highest, but it was not significantly different from that of the control groups (P > 0.05) (Figure 2C–F).
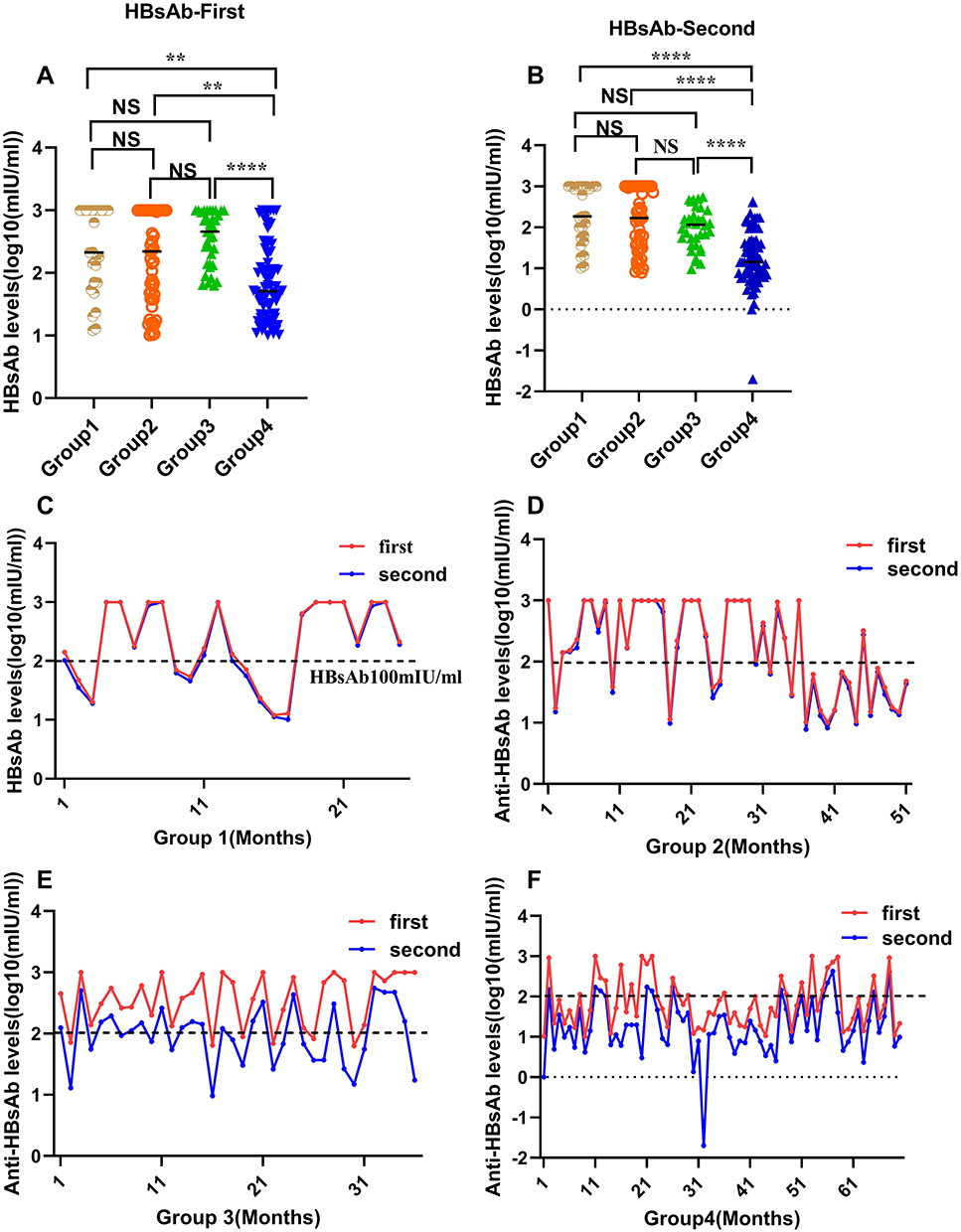 |
Figure 2 Comparison and distribution of fluctuations in the HBsAb levels between the groups. (A) The HBsAb-First levels among the four groups. (B) The HBsAb-Second levels among the four groups. (C–F) The first and second HBsAb levels fluctuations for the four groups. **P < 0.01, ****P < 0.0001. Abbreviation: NS, nonsignificant. |
Comparison of the Persistence of HBsAb Levels in Each Group
To further evaluate the persistence of HBsAb levels in each group and discern a trend of reduction in HBsAb titers, survival analysis was performed (Figure S3 First, the interval was found to be longer than that in the case groups (P < 0.05). Second, the interval from the first to the second HBsAb level in Group 4 was shorter than that in Group 1 (P < 0.05). The persistence of HBsAb levels was not different among the other groups. In addition, to comprehend the regularity of HBsAb persistence and aid in the clinical guidance of vaccination, patients with HBsAb levels >100 mIU/mL and 10–100 mIU/mL were selected for further follow-up, and downward trends were observed in the four groups. Moreover, a statistical method was used to evaluate the descent trend. On the one hand, the probability of persistent immunity was not different at the 10–100 mIU/mL level (P > 0.05) (Figure 3A). On the other hand, at the HBsAb level of >100 mIU/mL, the decent times of the case groups were shorter than those of the control groups (P < 0.05) (Figure 3B). Finally, the decline time was not significant between the groups because of the limited number of samples (P > 0.05) (Figure 3C–F).
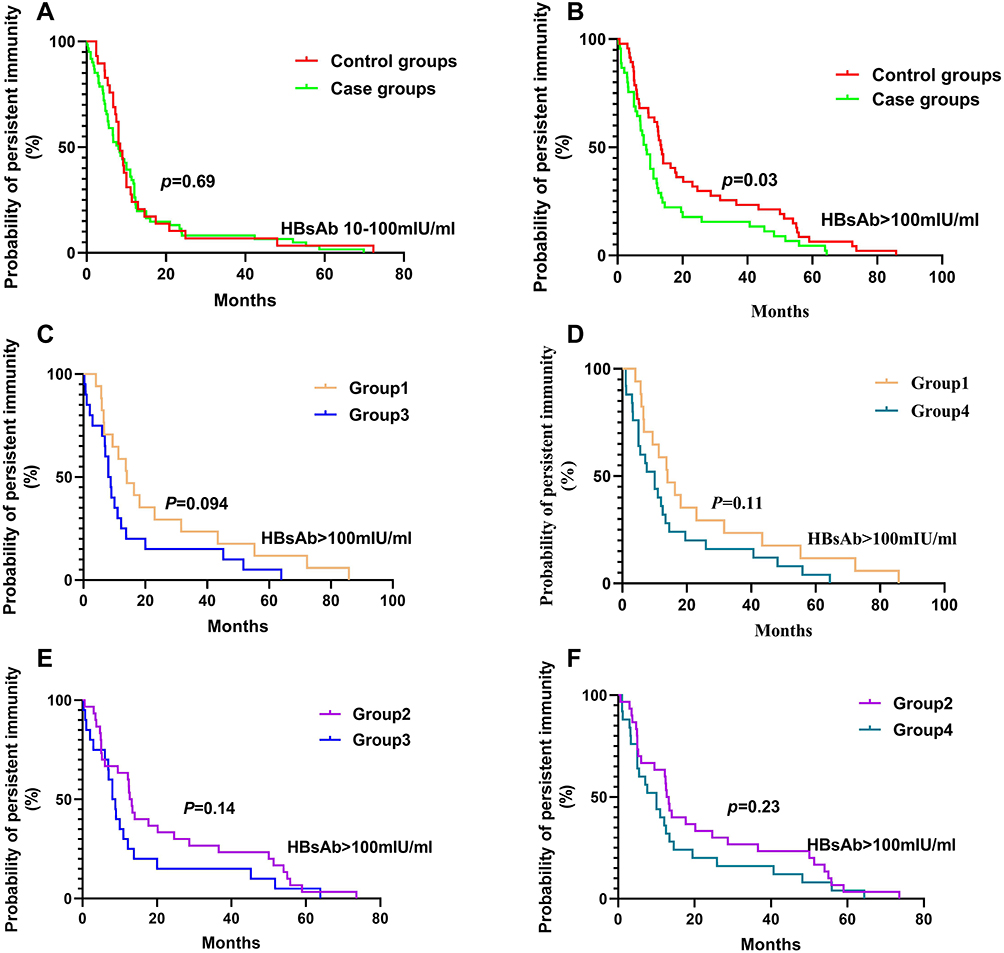 |
Figure 3 Comparison of the persistence of HBsAb at different levels in each group. (A) The persistence of HBsAb levels (10–100 mIU/mL) between the case and control groups. (B) The persistence of HBsAb levels (>100 mIU/mL) between the control and case groups. (C–F) The persistence of HBsAb levels (>100 mIU/mL) between different groups. |
Risk Factors and a Good Threshold for Fluctuating HBsAb Levels
To investigate whether the case groups were related to some clinical factors (Table 2), a univariate analysis was performed to identify the independent risk factors. As shown in Table 2, sex, age, family history of HBV infection, antiviral drug (once), immunosuppressor, anti-HBc, HBsAb, HBeAg, and HBeAb were not significantly different between the control and case groups (P > 0.05). Some parameters, such as the HBsAb interval time between descent, antiviral drugs, and first-HBsAb levels, were different (P < 0.05), and previous HBV history was distinctly significant (P < 0.001)(Figure 4A–C). In addition, the HBsAb difference value was obviously different (P < 0.001) (Figure 4D). In view of the data analysis and the clinical significance, previous HBV history, antiviral drug use, and/or low levels of first-HBsAb were considered to be independent risk factors for the case groups. In other words, when a participant is infected with HBV, is taking antiviral drugs, and has low levels of first-HBsAb, their HBsAb level is likely to decline.
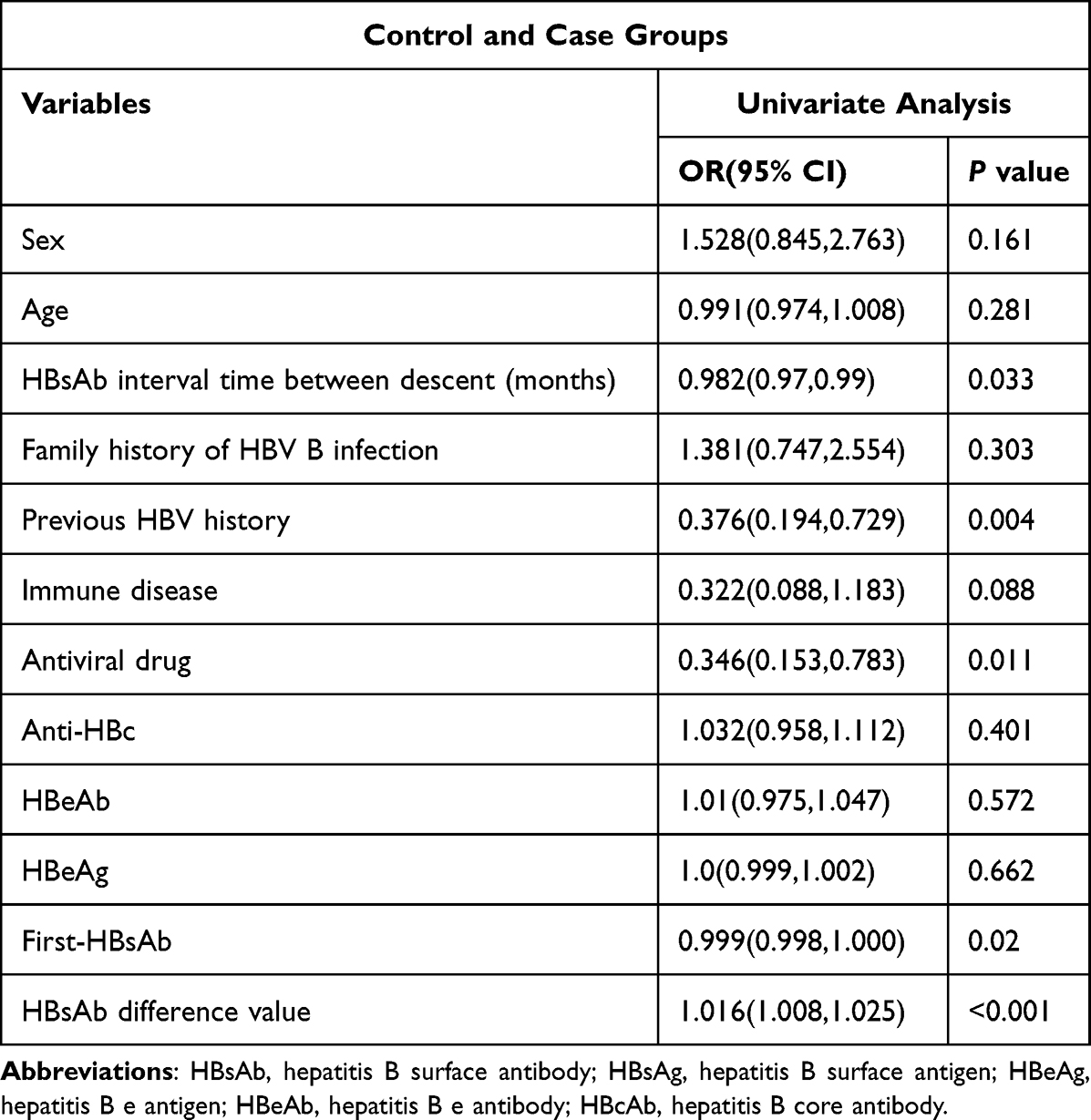 |
Table 2 Logistic Regression Analysis to Identify the Independent Influencing Factors for HBsAb Reduction in the Population |
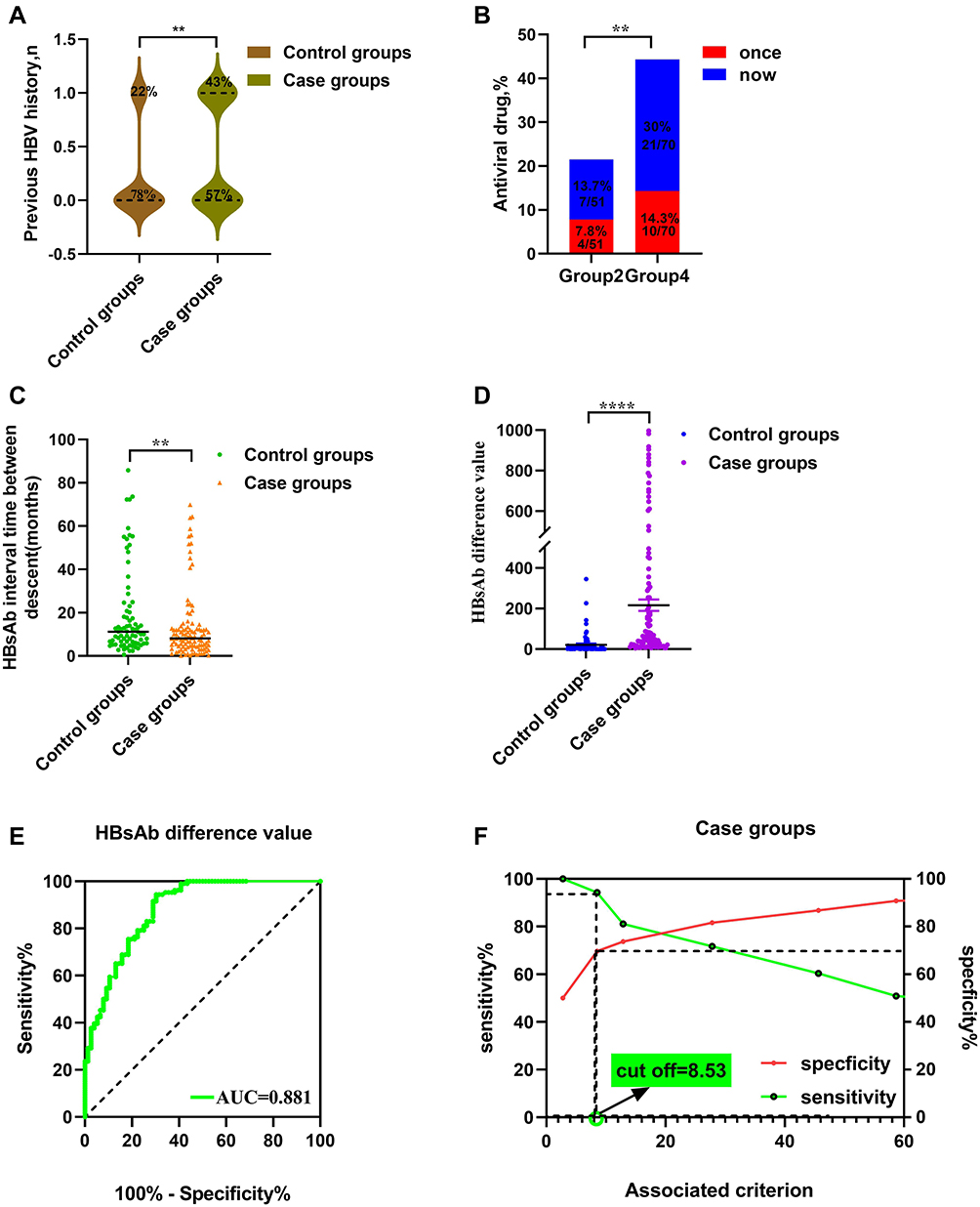 |
Figure 4 Risk factors and a good threshold for fluctuating hepatitis B surface antibodies. (A) previous HBV history; (B) antiviral drugs; (C) HBsAb interval time; (D) HBsAb difference value between the control and case groups; (E) The ROC area of HBsAb difference value in predicting the diagnosability between the control and case groups. (F) The sensitivity and specificity of the ROC curve of the HBsAb difference value in predicting the diagnosability between the control and case groups. **P < 0.01, ****P < 0.0001. |
To distinguish between the case and control groups, ROC curve analysis was used to assess the HBsAb difference values. Interestingly, the curve had a high AUC (0.881, 95% CI: 0.83–0.931) (Figure 4E). The optimum cutoff value was calculated using the Youden index. The value was found to be 8.53 mIU/mL. Furthermore, its sensitivity, specificity, positive and negative likelihood ratios (PLR and NLR), and positive and negative predictive values (PPV and NPV) were 94%, 70%, 3.12, 0.08, 0.81, and 0.9 between the control and case groups, respectively (Figure 4F, Table S1).
It was concluded that the median first–second HBsAb levels in the anti-HBc(+) group with a 50% decline were the lowest. Moreover, the HBsAb fluctuation in Group 3 was the highest. In addition, the persistence of HBsAb levels was shorter in the case groups, and the interval from the first to the second HBsAb levels was obviously shorter in Group 4 than in Group 1. Furthermore, the decent times of the case groups were shorter than those of the control groups for HbsAb levels >100 mIU/mL. Finally, it is worth mentioning that HBV history, antiviral drug usage, and low levels of HBsAb were risk factors. Also, an optimum cutoff value was present to differentiate between the case and control groups.
Discussion
A decline in HBsAb levels is a common phenomenon in organ transplantation17,18 and immunosuppressive diseases.19,20 Nonetheless, it has not been reported systematically. This study attempted to obtain results and some regularities from a 10-year longitudinal analysis of a decline population in the HBsAb levels. A decrease in HBsAb levels from <25% and >50% was observed in the anti-HBc(-) and anti-HBc(+) populations. In the follow-up, anti-HBe titers showed a little predictive value for people with reduced antibody titers (Figure S2).
The anti-Hbc(+) groups, including a control group and a case group with inclusion criteria, were used to distinguish between previous and current infections. Anti-Hbc(+) patients were rather common in the census.21–24 However, the anti-Hbc(+) groups in the control groups and case groups have rarely been reported. Presently, the retrospective polycentric cohort study suggested that the median HBsAb level of Group 4 was lower than that of the other groups and that its median was 50.8 mlU/mL. Clinical data analysis revealed that the ratio of HBsAg+/HBsAb+ patients in Group 4 was the highest. Hence, the serum condition of Group 4 must have caused the formation of immune complexes,25 which may be a reason for the lower HBsAb levels.
In addition, the data showed that the percentage of decline differed significantly between the case and control groups (Figure S1A). The decline was also obviously different in Group 3 (Figure S1B). This information revealed that anti-Hbc(+) patients should be monitored for HBsAb levels at regular intervals. First, surface antibody detection should be increased when the HBsAb level is low. Second, when the HBsAb titer is <10 mIU/mL, the patients should be revaccinated because of their low immune capacity.17,26–28
The durability of the antibody response varied among the participants.29–31 In the polycentric retrospective cohort study, the participants were categorized into four groups. The durability of the antibody response was not exactly the same (Figure 3C and E) and depended on the immune status of each group. Overall, the durability time of persistent immunity in the case groups was shorter than that in the control groups. Viewed separately, the durability of the antibody response in Group 4 was shorter than that in Group 1. Combined with the first and second HBsAg levels, the levels decreased faster in the anti-HBc(+) group of the case groups. In general, the durability of the antibody response is a concern when trying to prevent HBV infection; in particular, more attention should be given to anti-HBc(+) to obtain a functional cure.31
The 10-year follow-up study demonstrates risk factors and a good threshold for fluctuating HbsAb levels. Not surprisingly, previous HBV history was an independent risk factor for the case group because of lower immunity. Interestingly, antiviral drug use and low levels of first-HBsAb were also independent risk factors between the case and control groups. When the HBsAb titer of a participant was low at baseline, their HBsAb level fell more easily. Similarly, when patients with HBV infection were taking antiviral drugs, they were more likely to have damaged liver function, thereby leading to a decline in immunity.32
The optimum cutoff value was found to be 8.53 mIU/mL, which was determined from the clinical findings to predict the case groups. The cutoff value helped to preliminarily identify a decline in HBsAb levels. Thus, the results helped to avoid HBV reactivation and occult hepatitis B infection.
Conclusion
Our study has established that the first and second HBsAb levels of the anti-HBc(+) group were lower and more variable in the case groups than in the control groups. Moreover, the durability of HBsAb was lower in the case groups than in the control groups. These findings of risk factors and a good threshold suggest a supplementary clinical factor for the early prediction of a decline in HBsAb levels. This result further clarifies why patients with HBV infection should take antiviral therapy as early as possible.
Abbreviations
HBsAb, hepatitis B surface antibody; HBsAg, hepatitis B surface antigen; HBeAg, hepatitis B e antigen;HBeAb, hepatitis B e antibody;HBcAb, hepatitis B core antibody.
Data Sharing Statement
The datasets used and analyzed during the current study are available from Zhenhua Zhang on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the institutional Medical Ethics Review Board of Anhui Medical University (no. 2021005).
Funding
This work was supported by the Funds of the Second Hospital of Anhui Medical University [grant number 2019GMFY02], the Anhui Provincial Department of Education’s 2020 Anhui Provincial University Cooperation Research and Public Health Collaborative Innovation Project [grant number GXXT-2020-016] and the 2021 Anhui University Postgraduate Scientific Research Project [grant number YJS20210277].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qin Y, Liao P. Hepatitis B virus vaccine breakthrough infection: surveillance of S gene mutants of HBV. Acta Virol. 2018;62(2):115–121. doi:10.4149/av_2018_210
2. Intongkam S, Samakarnthai P, Pakchotanon R, Narongroeknawin P, Assavatanabodee P, Chaiamnuay S. Efficacy and safety of hepatitis B vaccination in rheumatoid arthritis patients receiving disease-modifying antirheumatic drugs and/or biologics therapy. J Clin Rheumatol. 2019;25(8):329–334. doi:10.1097/RHU.0000000000000877
3. Seo YB, Moon SJ, Jeon CH, et al. The practice guideline for vaccinating Korean patients with autoimmune inflammatory rheumatic disease. Infect Chemother. 2020;52(2):252–280. doi:10.3947/ic.2020.52.2.252
4. Yuan Q, Zhou F, Zhang H, et al. Efficacy and safety of hepatitis B re-vaccination in children after completion of chemotherapy and(or) hematopoietic stem cell transplantation. Zhonghua Er Ke Za Zhi. 2020;58(10):802–806. doi:10.3760/cma.j.cn112140-20200307-00195
5. Chang SH. Prevention of HBV Recurrence After Liver Transplant: long-Term Results. Transplant Proc. 2021;53(5):1707–1710. doi:10.1016/j.transproceed.2021.04.006
6. Urabe A, Imamura M, Tsuge M, et al. The relationship between HBcrAg and HBV reinfection in HBV related post-liver transplantation patients. J Gastroenterol. 2017;52(3):366–375. doi:10.1007/s00535-016-1240-y
7. Li AY, Liu Z, Song Y, et al. Reduction of the occurrence of occult HBV infection in infants by increasing the dose of hepatitis B vaccine: a large prospective cohort study. Emerg Microbes Infect. 2020;9(1):1881–1891. doi:10.1080/22221751.2020.1808533
8. Xinias I, Vasilaki K, Argiropoulou E, Mavroudi A, Tsiatsiou O, Roilides E. De novo HBV Hepatitis in a Child with Liver Transplantation. Maedica. 2021;16(2):293–296. doi:10.26574/maedica.2020.16.2.293
9. Shouval D, Shibolet O. Immunosuppression and HBV reactivation. Semin Liver Dis. 2013;33(2):167–177. doi:10.1055/s-0033-1345722
10. Huang SC, Yang HC, Kao JH. Hepatitis B reactivation: diagnosis and management. Expert Rev Gastroenterol Hepatol. 2020;14(7):565–578. doi:10.1080/17474124.2020.1774364
11. Hoofnagle JH. Reactivation of hepatitis B. Hepatology. 2009;49(Suppl):S156–S165. doi:10.1002/hep.22945
12. Shi Y, Zheng M. Hepatitis B virus persistence and reactivation. BMJ. 2020;1(370):m2200. doi:10.1136/bmj.m2200
13. Lai MW, Lin TY, Liang KH, Lin WR, Yeh CT. Hepatitis B viremia in completely immunized individuals negative for anti-hepatitis B core antibody. Medicine. 2016;95(49):e5625. doi:10.1097/MD.0000000000005625
14. Hashemi B, Mahdavi-Mazdeh M, Abbasi M, Hosseini-Moghaddam SM, Zinat NH, Ahmadi F. Efficacy of HBV vaccination in various stages of chronic kidney disease: is earlier better? Hepat Mon. 2011;11(10):816–820. doi:10.5812/kowsar.1735143X.1771
15. Gentile G, Antonelli G. HBV reactivation in patients undergoing hematopoietic stem cell transplantation: a narrative review. Viruses. 2019;11(11):1049. doi:10.3390/v11111049
16. Horlander JC, Boyle N, Manam R, et al. Vaccination against hepatitis B in patients with chronic liver disease awaiting liver transplantation. Am J Med Sci. 1999;318(5):304–307. doi:10.1016/S0002-9629(15)40643-3
17. Chancharoenthana W, Leelahavanichkul A, Udomkarnjananun S, et al. Durability of antibody response against the hepatitis B virus in kidney transplant recipients: a proposed immunization guideline from a 3-year follow-up clinical study. Open Forum Infect Dis. 2018;6(1):ofy342. doi:10.1093/ofid/ofy342
18. Rosenau J, Hooman N, Hadem J, et al. Failure of hepatitis B vaccination with conventional HBsAg vaccine in patients with continuous HBIG prophylaxis after liver transplantation. Liver Transpl. 2007;13(3):367–373. doi:10.1002/lt.21003
19. Avakolpour S, Alavian SM, Sali S. Hepatitis B reactivation during immunosuppressive therapy or cancer chemotherapy, management, and prevention: a comprehensive review-screened. Hepat Mon. 2016;16(4):e35810. doi:10.5812/hepatmon.35810
20. Wang L, Hu H, Zhang R, et al. Changes in the hepatitis B surface antibody in childhood acute lymphocytic leukemia leukemia survivors after treatment with the CCLG-ALL 2008 protocol. Clin Exp Immunol. 2021;203(1):80–86. doi:10.1111/cei.13513
21. Hang ZQ, Shi BS, Lu W, Liu DP, Huang D, Feng YL. Quantitative Anti-HBc in liver pathological states in patients with chronic hepatitis B virus infection. Can J Infect Dis Med Microbiol. 2019;2019:6545642. doi:10.1155/2019/6545642
22. Moretto F, Catherine FX, Esteve C, Blot M, Piroth L. Isolated Anti-HBc: significance and management. J Clin Med. 2020;9(1):202. doi:10.3390/jcm9010202
23. Drößler L, Lehmann C, Töpelt K, et al. HBsAg-negative/anti-HBc-positive patients treated with rituximab: prophylaxis or monitoring to prevent hepatitis B reactivation? Infection. 2019;47(2):293–300. doi:10.1007/s15010-019-01271-z
24. Yenilmez E, Cetinkaya RA. Overuse of prophylaxis in HBsAg and/or anti-HBc positive patients after increasing awareness to prevent reactivation in patients receiving immunosuppressive therapies: how rational are our prophylaxis decisions according to the literature? Infez Med. 2019;27(3):299–307.
25. Bazinet M, Anderson M, Pântea V, et al. Analysis of HBsAg immunocomplexes and cccDNA activity during and persisting after nap-based therapy. Hepatol Commun. 2021;5(11):1873–1887. doi:10.1002/hep4.1767
26. Kovacic V, Sain M, Vukman V. Efficient hemodialysis hemodialysis improves the response to hepatitis B virus vaccination. Intervirology. 2002;45(3):172–176. doi:10.1159/000065873
27. Saberifiroozi M, Gholamzadeh S, Serati AR. The long-term immunity among health care workers vaccinated against hepatitis B virus in a large referral hospital in southern Iran. Arch Iran Med. 2006;9(3):204–207.
28. Lô G, Sow-Sall A, Diop-Ndiaye H, et al. Hepatitis B virus (HBV) infection amongst children in Senegal: current prevalence and seroprotection level. Pan Afr Med J. 2019;25(32):140.
29. O’Bryan TA, Rini EA, Okulicz J, et al. HIV viraemia during hepatitis B vaccination shortens the duration of protective antibody levels. HIV Med. 2015;16(3):161–167. doi:10.1111/hiv.12189
30. Kalchiem-Dekel O, Grupel D, Bouchnik L, Sikuler E, Ben-Yakov G. Efficacy and long-term durability of intradermal recombinant hepatitis B virus vaccine among intramuscular vaccine nonresponders: a prospective study in healthcare personnel. J Gastroenterol Hepatol. 2015;30(12):1782–1787. doi:10.1111/jgh.13022
31. Huang D, Wu D, Wang P, et al. End-of-treatment HBcrAg and HBsAb levels identify durable functional cure after Peg-IFN-based therapy in patients with CHB. J Hepatol. 2022;77(1):42–54. doi:10.1016/j.jhep.2022.01.021
32. Xiang D, Ren X, Chen Q, Yu H, Li X, Liu D. Association of ACEI/ARB, inflammatory cytokines, and antiviral drugs with liver dysfunction in patients with hypertension and COVID-19. Clin Exp Hypertens. 2021;43(4):305–310. doi:10.1080/10641963.2020.1867160
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.