")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 12
Drug-Therapy Problems and Predictors among Hospitalized Heart-Failure Patients: A Prospective Observational Study
Authors Fentie Wendie T , Tarekegn Angamo M
Received 22 June 2020
Accepted for publication 14 November 2020
Published 22 December 2020 Volume 2020:12 Pages 281—291
DOI https://doi.org/10.2147/DHPS.S268923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajender R Aparasu
Teklehaimanot Fentie Wendie,1 Mulugeta Tarekegn Angamo2
1Department of Pharmacy, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Pharmacy, College of Public Health and Medical Sciences, Jimma University, Jimma, Ethiopia
Correspondence: Teklehaimanot Fentie Wendie Email [email protected]
Background: Heart-failure patients are at high risk of experiencing drug-therapy problems, owing to polypharmacy, comorbidities, and usually advanced age. Drug-therapy problems can lead to poor clinical outcomes, increased health-care costs and decreased quality of life, and thus strategies for identifying, resolving, and preventing them are urgently needed. Therefore, this study aimed at investigating the incidence and predictors of drug-therapy problems among hospitalized heart-failure patients.
Methods: This hospital-based prospective observational study was conducted from February 1 to May 31, 2014 at Jimma University Specialized Hospital. Patients of either sex aged 18 years and above with chronic heart failure and complete medical records were enrolled. Patients with high-output heart failure, < 1 day of hospital stay, unwilling to give written informed consent, and unconscious without caregivers were excluded. Data were collected from medication charts, laboratory reports, patients/caregivers, morning multidisciplinary meetings, and ward rounds. Multivariate binary logistic regression analysis was done to identify independent predictors of drug-therapy problems.
Results: A total of 104 heart-failure patients (mean age 51.20± 15.66 years, females 51.9%) were consecutively enrolled, and 95 (91.3%) had experienced at least one drug-therapy problem (total 268, mean 2.82± 1.39 encounters per patient). Of these problems, 45.5% were the need for additional drugs, followed by noncompliance (22.0%), inappropriate dosing (9.3%), unnecessary drugs (9.0%), ineffective drugs (8.2%), and adverse drug reactions (6.0%). None of the independent variables was found to be an independent predictor of having at least one drug-therapy problem. However, the number of clinical/pharmacological risk factors (AOR 7.93), female sex (AOR 3.24), and length of hospital stay (AOR 12.98) were predictors of noncompliance.
Conclusion: Patients suffered from a large number of drug-therapy problems. Drugs with survival benefit were underused. Noncompliance and the need for additional drug therapy were the most frequently identified drug-therapy problems. Numbers of clinical/pharmacological risk factors, length of hospital stay, and female sex were identified as predictors for noncompliance.
Keywords: heart failure, drug-therapy problems, predictors
Introduction
Despite improvements in the prevention and treatment of heart failure over the last 25 years,1–7 prognosis remains poor, with median survival of 2.3 and 1.8 years for men and women, respectively.8,9 This may be due to nonadherence of physicians to treatment guidelines,10–13 patients’ nonadherence to their medications,8,14,15 or the high prevalence of drug-therapy problems.16,17 The aim of heart-failure medical treatment is to optimize the mainline drug therapies, such as angiotensin-converting enzyme (ACE) inhibitors and β-blockers, anduse diuretics only intermittently for symptom relief.1,10,18
However, these classes of drugs are underutilized, influencing prognosis and health-care costs. Treatment dosages have been in general only 50% of targets and not optimized during long-term treatment.3,11–14,19–30 Barriers to utilization include misperceptions that various heart-failure subpopulations, such as the elderly and patients with renal insufficiency, do not need certain medical therapies, a fear of polypharmacy, inappropriate assumptions about adverse effects and contraindications, and cost. In fact, optimal prescribing of evidence-based therapy can actually reduce costs.31–36
Despite there being substantial room for improvement, drug-therapy problems are common among hospitalized heart-failure patients, in whom advanced age, comorbidities, polypharmacy, multiple changes in medication regimens, and lack of continuity of care are common.12,17,37–51 These are associated with negative effects on clinical outcomes and lead to substantial morbidity and mortality, reduced quality of life, prolonged hospital stays, and increased health-care expenditure, which in turn affects both patients and society.8,50,52–54 The economic burden of drug-therapy problems is also high.55–57
A vast amount of research has explored the fact that numerous factors related to the patient (eg, age and sex), disease, treatment (eg, complexity of a regimen, such as dosing frequency), and health-care system are known to be associated with drug-therapy problems.58–60 Studies have also shown that a majority of drug-therapy problems (50%–80%) are often preventable. Multidisciplinary management strategies involving clinical pharmacists reduce incidence of drug-therapy problems, hospitalization, mortality, length of hospital stay, adverse drug reactions, medication errors, and cost of care, and increase patients’ health-related quality of life. Despite this, there has been little improvement in the incidence of drug-therapy problems, and worldwide they are considered a critical barrier to treatment success.14,24,31,49,60–67
Studies on prevalence and close characterization of drug-therapy problems among heart-failure patients in hospitals are lacking in Ethiopia and at Jimma University Specialized Hospital in particular. Given the economic and medical burdens, strategies for identifying, resolving, and preventing drug-therapy problems are urgently needed. Moreover, a greater understanding of predictors and management systems is needed to institute clinical pharmacy services for rational use of drugs and efficient utilization of health-care resources. As such, the aims of this study were investigating the nature of drug-therapy problems, estimating their incidence, and identifying risk factors among hospitalized heart-failure patients so that pharmacists can play an important role in identifying, resolving, and preventing these problems.
Methods
Study Design, Population, and Period
This prospective observational study was conducted from February 1 to May 31, 2014 at Jimma University Specialized Hospital, the only teaching and referral hospital in southwestern Ethiopia. The study was conducted in accordance with the Declaration of Helsinki after approval by the institutional review board of Jimma University and subsequent permission from the hospital. Written informed consent was obtained from each patient, and none refused. Confidentiality of information obtained from each study participant was guaranteed by omitting names or any personal identifiers. Data were kept safe throughout the whole process of the research to limit accessibility to third parties. All heart-failure patients hospitalized during the study period who fulfilled the inclusion criteria were eligible. Patients of either sex of aged ≥18 years admitted with a diagnosis of heart failure and complete medical records were consecutively enrolled. Patients were excluded if they were had high-output heart failure, discharged before 24 hours with unknown status, unwilling to participate, unconscious, or had hearing problems (for the interview). Patients with high-output heart failure were excluded, as they would be not be eligible once the underlying cause, eg, thyrotoxicosis or anemia, had been treated.
Data-Collection Procedure
Data were collected by a clinical pharmacist using a structured and pretested questionnaire. Patient medical records (case notes, care plan, progress notes, medication charts and laboratory reports), patientcaregiver interviews, and morning multidisciplinary meetings and routine ward rounds where each patient is discussed with regard to diagnosis, therapy, and follow-up were used as sources of data. Patients/caregivers were interviewed for information on sociodemographics, social drug use, medication adherence prior to admission (using the four-item Morisky scale), medical history, history of allergies/adverse drug reactions, and home (herbal and over the counter) medications. Issues that were addressed by medication reviews included all drugs the patient received at and during admission, indications for drug use, dosage, frequency, duration of treatment, drug-safety profile, potential drug–drug/disease interactions, therapeutic or pharmacological duplication, and probability of undertreatment. Also, most commonly acknowledged clinical/pharmacological risk factors of drug-therapy problems were recorded. Data were critically evaluated by two clinical pharmacists and an internist to determine if all the patient’s medications had been appropriately indicated, the most effective available and safest possible agent used, and that the patient was able and willing to take the medication as intended. Each patient was followed from the day of admission until s/he was discharged home, transferred to a nonmedical ward within the same hospital, or transferred to another health-care facility (Figure 1).
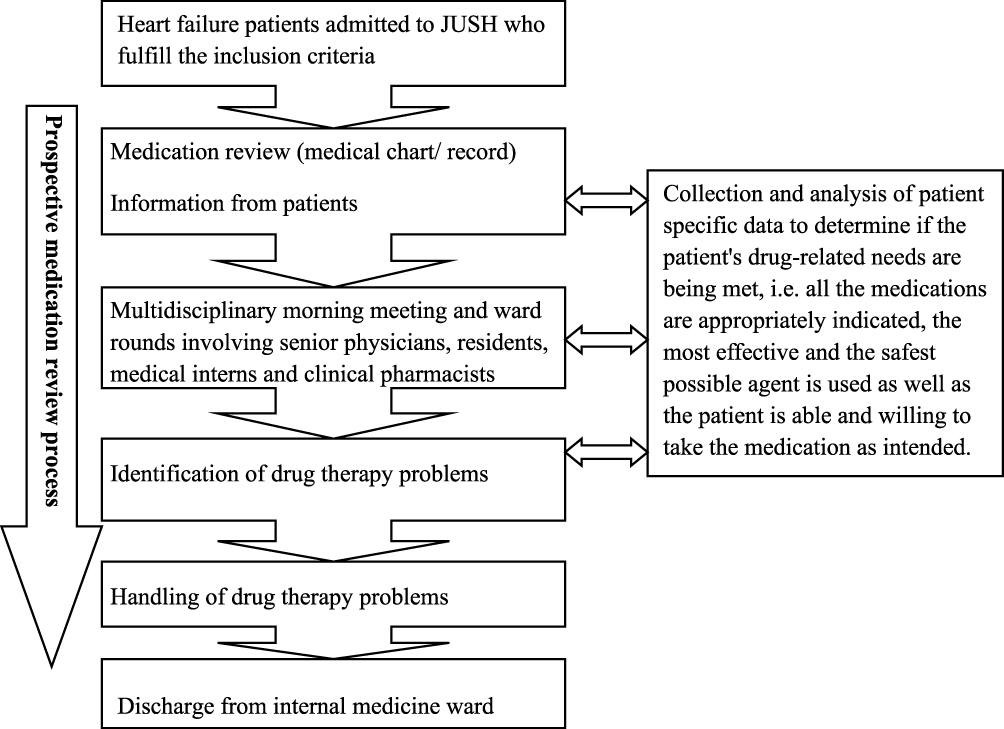 |
Figure 1 Flowchart of the study. |
Identification and Classification of Drug-Therapy Problems
Any undesirable event experienced by a patient that involves or is suspected to involve drug therapy and that actually or potentially interferes with achieving the desired goals of therapy was considered a drug-therapy problem and identified based on evidence-based guidelines1,3,5 and consensus of the multidisciplinary team of the hospital, which consists of a senior physician (internist), a clinical pharmacist, a cardiologist, residents, medical interns, and nurses.Problems identified were discussed at the multidisciplinary meeting and/or dealt with. Drug-therapy problems with drugs involved, potential issues, and pharmaceutical interventions, defined as any recommendation made with the intent of changing drug treatment, such as dose reduction and drug substitution, were noted and reported. All drug-therapy problems were categorized according to Cipolle’s classification.68
Definition of Terms and Explanations
Adverse Drug Reaction (ADR)
An ADR was defined as a noxious, unintended and undesired effect of a drug occurring at doses used in humans for prophylactics, diagnosis, or therapy.
Clinical/pharmacological risk factors were a composition of clinical, pharmacological, and patient-related factors assumed to increase the risk of drug-therapy problems, eg, polypharmacy, reduced renal and liver function, diabetes, heart failure, and history of ADRs.
Compliance referred to how well a patient followed instructions for a treatment regimen. Noncompliance is often defined as <80% of the medicines being taken as prescribed.
Dosage Too Low
dosage interval being too infrequent, drug interactions reducing the amount of active drug available, or duration of drug therapy being too short to produce the desired response.
Dosage Too High
This was defined as dosing frequency being too short, duration of drug therapy too long, drug interaction resulting in toxicity or a drug being administered too rapidly.
A drug-therapy problem is any undesirable event experienced by a patient that involves or is suspected to involve drug therapy, actually or potentially interferes with achieving the desired goals of therapy, and requires professional judgment to resolve.16
A drug therapy is considered “ineffective” if it is not able to produce the desired beneficial result in a specific patient.
Heart failure is a complex clinical syndrome that results from any structural or functional impairment of ventricular filling or ejection of blood.1
Indication is the reason for the use of drug therapy, ie, treatment, prevention, or diagnosis of a condition (illness, symptom) in a specific patient. Indication-related drug-therapy problems may be either “unnecessary drug therapy” or “need for additional drug therapy”.
Medication review is an evaluation of prescribed medicines with the aim of managing the risks and optimizing the outcomes of drug therapy by detecting, resolving, and preventing drug-therapy problems.
Polypharmacy is defined as the daily consumption of five or more medications, since this threshold has been consistently associated with important negative health outcomes.
Statistical Analysis
Data were entered into EpiData 3.1 and analyzed using SPSS 23.0 Inc. Descriptive statistics were applied for analysis of patient characteristics and categorical variables analyzed using Pearson’s χ2 test. Independent variables were assessed for multicolinearity and associations to rule out correlations between two or more independent variables using the variance-inflation factor. Independent variables with P<0.25 on univariate analysis were entered into a multivariate binary logistic regression model to determine independent predictors of drug-therapy problems. Multivariate binary logistic regression analysis was also performed to identify predictors of noncompliance. Pearson’s correlation coefficient was calculated to find associations between drug-therapy problems and various patient factors. Two-sided P<0.05 was considered statistically significant.
Results
Patient Characteristics and Drug-Therapy Problems
In sum, 104 heart-failure patients (54 female and 50 male) with a mean age of 51.20±15.66 years, were consecutively enrolled. The majority of patients were married (64.4%), illiterate (63.5%), free of any social drug use (57.7%), and New York Heart Association functional class IV at inclusion (Table 1). Patients were followed clinically for an average of 14 (2–42) days, and in-hospital mortality was 9.6% (ten patients).
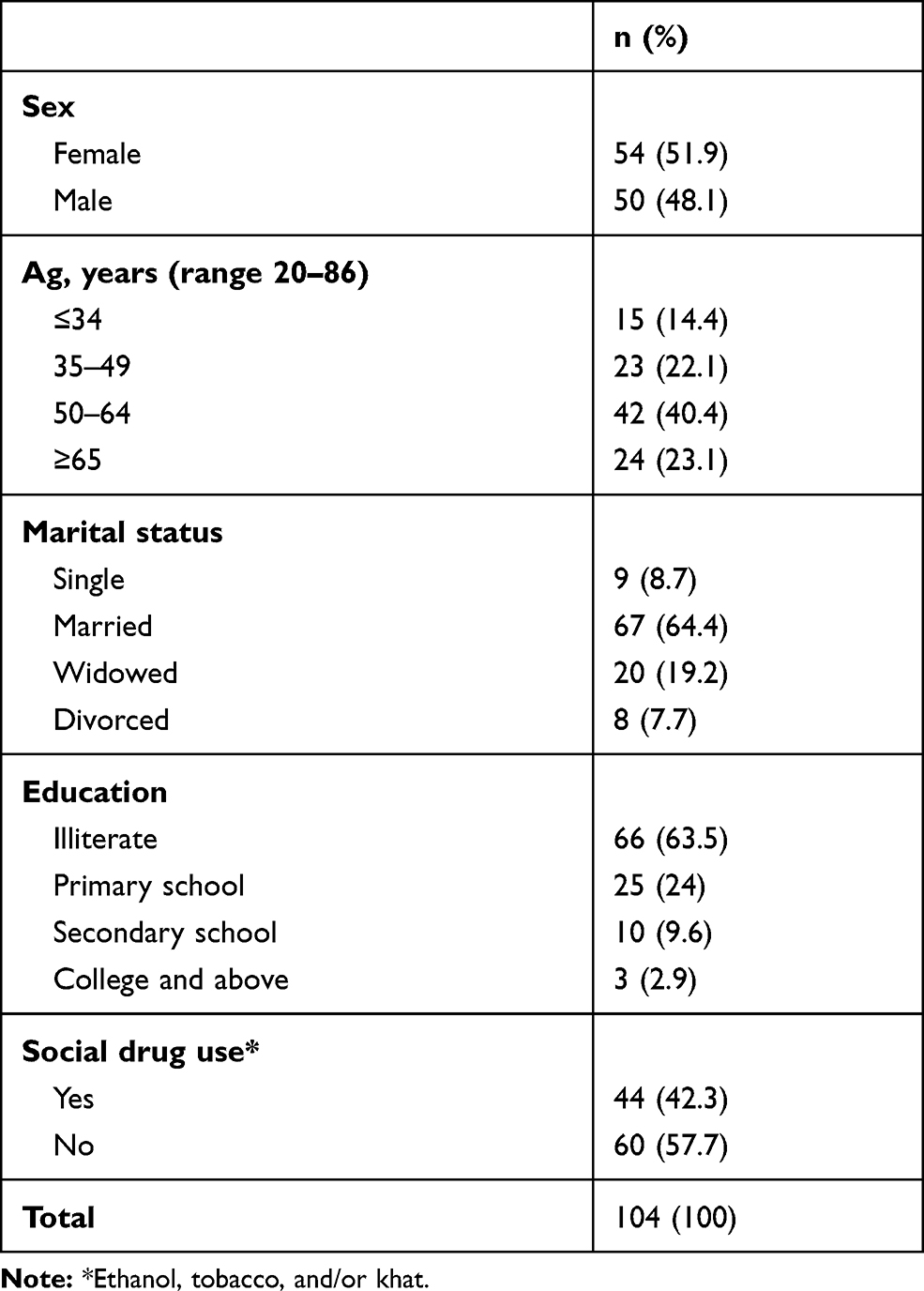 |
Table 1 Sociodemographic Characteristics of Heart-failure Patients, Jimma University Specialized Hospital, Ethiopia, 2014 |
Of the 104 patients, 91.3% experienced at least one drug-therapy problem, (total 268, mean 2.82±1.39 per patient, range one to eight). The most commonly encountered drug-therapy problem was “insufficiently treated health problem”, ie, the need for additional drug therapy, followed by noncompliance (22%, Figure 2).
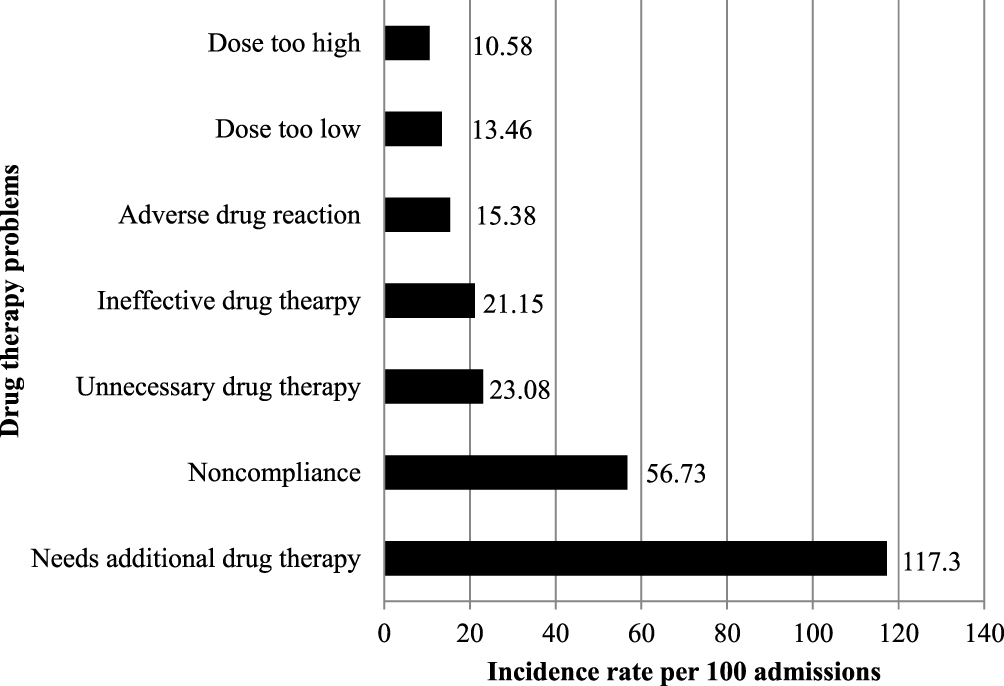 |
Figure 2 Incidence per 100 admissions of drug-therapy problems among heart-failure patients admitted to Jimma University Specialized Hospital, Ethiopia, 2014. |
Drug classes most implicated in drug-therapy problems were ACE inhibitors (50.5% of the 95 patients with drug therapy problems), β-blockers (50.5%), diuretics (40%), and antibiotics (33.7%; Table 2). Diuretics, ACE inhibitors, digoxin, β-blockers, spironolactone, and direct vasodilators were prescribed for 99%, 49%, 40.4%, 30.8%, 8.7%, and 2.9% of patients, respectively. Only 18.3% of patients received β-blockers licensed for heart failure. Daily dosage of ACE inhibitors and β-blockers was on average below the recommended target dose.
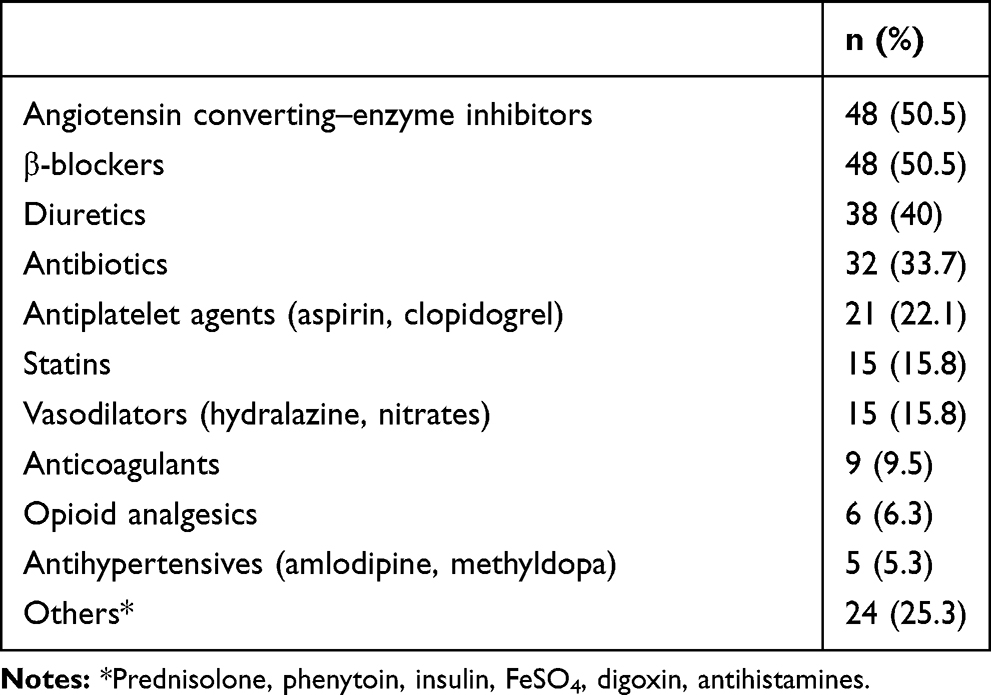 |
Table 2 Drug Classes Commonly Involved with Drug Therapy Problems Among Heart Failure Patients, Jimma University Specialized Hospital, Ethiopia, 2014 (n=95) |
Commonly identified causes of drug-therapy problems were untreated medical condition (35.8% of a total 268), drug product too expensive for the patient (12.3%), no medical indication, wrong dose (6.7% each), synergistic/potentiating agent required, more effective alternative available (6% each), preventive/prophylactic agent required, and drug product not available to the patient (3.7% each; Table 3).
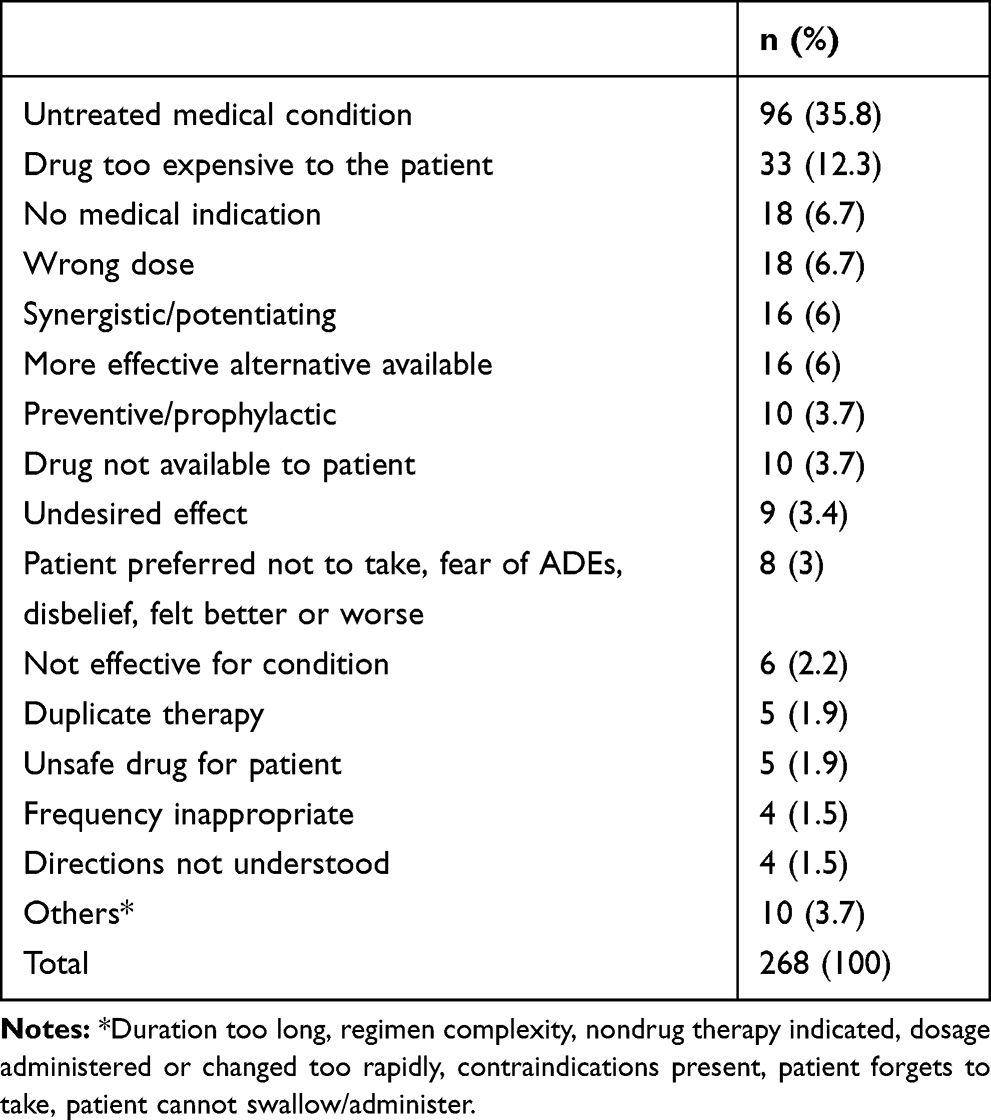 |
Table 3 Identified Causes of Drug-therapy Problems Among Heart-failure Patients Admitted to Jimma University Specialized Hospital, Ethiopia, 2014 (n=268) |
Predictors of Drug-Therapy Problems
Univariate logistic regression analysis showed that drug-therapy problems were significantly associated with length of hospital stay (COR 5.111, P=0.039). However, multivariate analysis showed that no independent variables to be to be independent risk factors (Table 4).
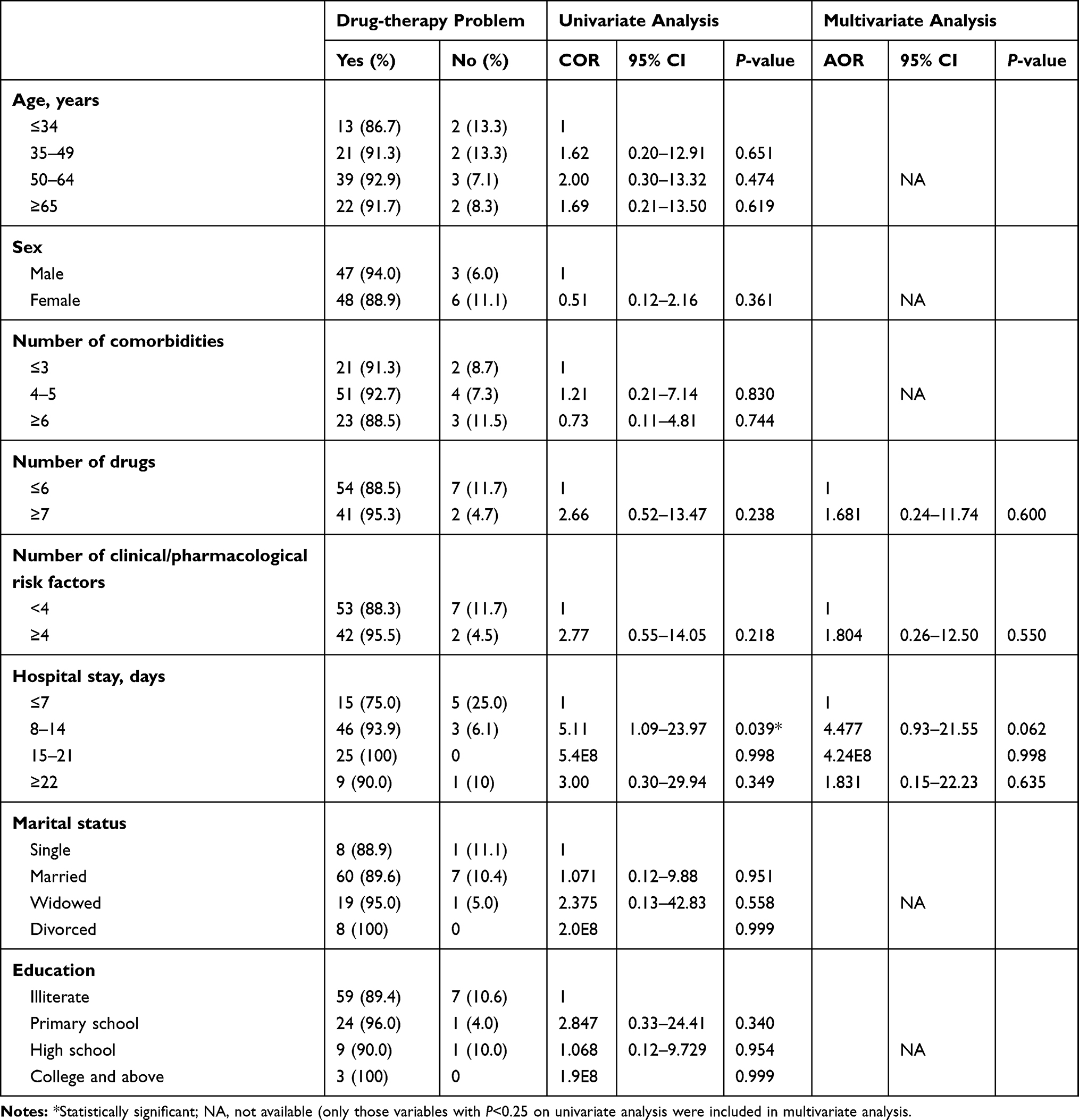 |
Table 4 Logistic Regression Results of Predictors of Drug-therapy Problems Among Heart-failure Patients, Jimma University Specialized Hospital, Ethiopia, 2014 |
Multivariate logistic regression analysis showed that females, those with four or more clinical/pharmacological risk factors, and patients who stayed >3 weeks in hospital were 3.24, 7.93, and 12.98 times as likely to be noncompliant asmales, patients with fewer than four clinical/pharmacological risk factors, and those staying ≤7 days in hospital, respectively, provided that other risk factors remained constant (Table 5).
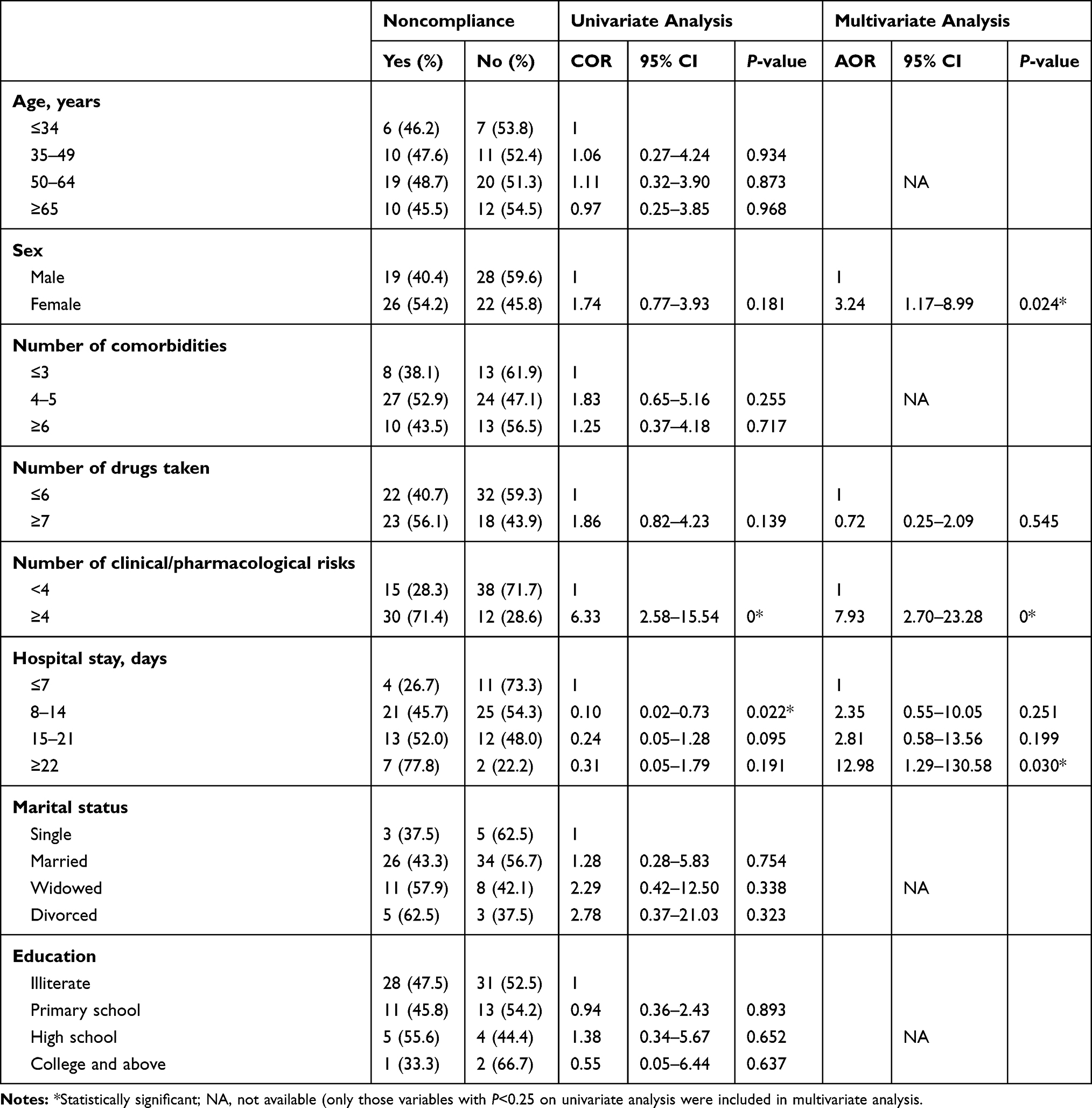 |
Table 5 Logistic Regression Results for Predictors of Noncompliance Among Heart-failure Patients, Jimma University Specialized Hospital, Ethiopia, 2014 |
In the present study, positive correlations was observed between number of drug-therapy problems and number of drugs taken (r=0.336, P=0.001) and number of clinical/pharmacological risk factors (r=0.235, P=0.022) and length of hospital stay (r=0.261, P=0.011), but not between age and number of comorbidities. This was also statistically significant on univariate linear regression analysis. However, multivariate analysis showed that only the number of drugs was an independent predictor of the total number of drug-therapy problems experienced (β=0.233, P=0.045), ie, each additional drug increased the risk of a drug-therapy problem by 0.233.
Discussion
Of the total 104 patients, 91.3% experienced at least one drug-therapy problem, similar to a study done in Switzerland, in which 91% of patients had at least one drug-therapy problem.52 However, our study showed much greater incidence of drug-therapy problems than other studies conducted in Barcelona, Spain, in which 147 drug-therapy problems were detected among 97 heart-failure patients over 6 months (mean 1.5±1.4 per patient),49 and India, where only 20.42%66 and 11.93%48 of patients received intervention for having one or more drug-therapy problems. This discrepancy with other studies may be attributed to differences in study methods and settings, different study populations, different classification systems for drug-therapy problems, and different methods for assessing drug-therapy problems.
Regarding the distribution of drug-therapy problems, we identified the leading oneto be “insufficiently treated health problem”, ie, the need for additional drug therapy. A similar trend was found in earlier studies, although the magnitude of our finding is quite significant: 45.5% versus 31%49 and 28.1%.38 This may be due to fear of adverse effects and unavailability of certain evidence-based medicines, such as β-blockers licensed for heart failure, angiotensin-receptor blockers, and vasodilator combinations, in our setting. Frequently in routine clinical practice, there are fewer heart-failure drug prescriptions for patients meeting current clinical practice guidelines than recommended by large randomized clinical trials.31–36 The second–most frequently encountered drug-therapy problem was noncompliance (22.0%); which was much lower than findings of other studies (40%–72.7%),50,51,59 but higher than the Barcelona study (14%).49
ACE inhibitors, β-blockers, aldosterone-receptor antagonists, and direct vasodilator combinations were not appropriately prescribed.These have various benefits in the treatment of heart failure, but were underused: even prescribed patients got subtherapeutic doses of these life-saving agents. A similar problem has been revealed by numerous studies across the world.10–13,20,22,23,25,26,28,31 However, what makes our case worse is that most of the patients were on drugs recommended for symptomatic relief, such as diuretics (99% vs 82%–86.9% in the aforementioned studies) and digoxin (40.4%), rather than drugs of survival benefit, such as ACE inhibitors, β-blockers, aldosterone-receptor antagonists, and vasodilator combinations, for appropriate patients. This may be ascribed to the unavailability of certain drugs, such as angiotensin-receptor blockers, for ACE inhibitor–intolerant patients, β-blockers licensed for heart failure, and vasodilator combinations. It may also be due to inappropriate assumptions about adverse effects, contraindications, and cost.
The identification of risk factors for drug-therapy problems may be helpful in finding patients at risk. These patients can then be singled out for special attention with the hope of avoiding overt drug-therapy problems. Age, sex, marital status, education, number of comorbidities, number of drugs used, length of hospital stay, and numbers of clinical/pharmacological risk factors were analyzed to determine whether they could predict the possibility of having at least one drug-therapy problem. However, none was found to be an independent risk factor, though a vast amount of research has explored numerous factors related to the patient, disease, treatment, and health-care provider or system that are known to be associated with drug-therapy problems.58–60 This might be due to differences in analysis methods, different classification systems of drug-therapy problems, and different methods of assessing drug-therapy problems.
When examining each of the problem domains, statistically significant associations were observed between noncompliance and sex and number of clinical/pharmacological risk factors and length of hospital stay. This was in agreement with a study done in Norway.39
In the present study, positive correlations were observed between number of drug-therapy problems and number of drugs taken and number of clinical/pharmacological risk factors and length of hospital stay, but not between age and number of comorbidities, although this has been reported by other studies.12,17,66 However, only the number of drugs was found to be an independent predictor of the total number of drug-therapy problems experienced. Similar results have been reported by other studies.39,43,48,49
Although this study is the first to describe all facets of drug-therapy problems among heart-failure patients in hospitals in this country and had the advantage of being prospective, which enabled us to detect many drug-therapy problems that could otherwise have been overlooked if a retrospective approach had been applied, it had notable limitations. Firstly, there was no control group, as we thought this was not ethical, making it prone to bias from other health-care providers. Secondly, it remains unknown whether changes in medication lead to improvement in the health and well-being of patients, because such outcome data were methodologically difficult to obtain, especially after discharge. Lastly, a relatively large number of drug-therapy problems remain unresolved, because of unavailability of some recommended drugs and inability of patients to afford investigation and drug costs. In addition, the study was conducted only during daytime, so drug-therapy problems that occurred during the night might have been missed, sod causality was not proven.
Conclusion
This study demonstrated that patients with heart failure suffer from a large number of drug-therapy problems. Drugs with survival benefit were underused. The most frequently identified drug-therapy problems were noncompliance and the need for additional drug therapy. Numbers of clinical/pharmacological risk factors, length of hospital stay, and female sex were identified as important risk factors for noncompliance, a component of drug-therapy problems.
Data-Sharing Statement
The data sets are available from the corresponding author upon reasonable request.
Acknowledgment
Thanks to our dear family, colleagues, relatives, and friends, and especially Mr Mesenbet Terefe for his valuable contribution. FWT would like to express his sincere gratitude to his cousin Dessie Adugna for always helping and encouraging him.
Author Contributions
Both authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no financial or nonfinancial conflicts of interest.
References
1. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary. J Am Coll Cardiol. 2013;62(16):1495–1539. doi:10.1016/j.jacc.2013.05.020
2. Chatterjee K. Congestive heart failure: what should be the initial therapy and why? Am J Cardiovasc Drugs. 2002;2(1):1–6. doi:10.2165/00129784-200202010-00001
3. Gauci M. Evidence-based drug therapy in the management of heart failure. J Malta College Pharm Pract. 2011;17:5–10.
4. Failure Society of America H. Executive summary: HFSA 2010 comprehensive heart failure practice guideline. J Card Fail. 2010;16(6):475–539. doi:10.1016/j.cardfail.2010.04.005
5. McMurray JJV, Adamopoulos S, Anker SD, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2012;33:1787–1847.
6. Hanks SD. Overview of beta blockers for systolic heart failure. Continuing Educ Credit. 2006;31(2):112–119.
7. Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348(20):2007–2018. doi:10.1056/NEJMra021498
8. Molloy GJ, O’Carroll RE, Witham MD, McMurdo MET. Interventions to enhance adherence to medications in patients with heart failure: a systematic review. J Am Heart Assoc Circ Heart Fail. 2012;5:126–133. doi:10.1161/CIRCHEARTFAILURE.111.964569
9. MacIntyre K, Capewell S, Stewart S, et al. Evidence of improving prognosis in heart failure: trends in case fatality in 66,547 patients hospitalized between 1986 and 1995. Circulation. 2000;102(10):1126–1131. doi:10.1161/01.CIR.102.10.1126
10. Komajda M, Lapuerta P, Hermans N, et al. Adherence to guidelines is a predictor of outcome in chronic heart failure: the MAHLER survey. Eur Heart J. 2005;26(16):1653–1659. doi:10.1093/eurheartj/ehi251
11. Ekman I, Swedberg K. Patients’ persistence of evidence-based treatment of chronic heart failure: a treatment paradox. J Am Heart Assoc Circulation. 2007;116:693–695.
12. Rushton CA, Strömberg A, Jaarsma T, Kadam UT. Multidrug and optimal heart failure therapy prescribing in older general practice populations: a clinical data linkage study. BMJ Open. 2014;4(1):e003698. doi:10.1136/bmjopen-2013-003698
13. Cleland JG, Cohen-Solal A, Aguilar JC, et al. Management of heart failure in primary care (the IMPROVEMENT of heart failure programme): an international survey. Lancet. 2002;360(9346):1631–1639. doi:10.1016/S0140-6736(02)11601-1
14. Milfred-LaForest SK, Chow SL, DiDomenico RJ, et al. Clinical pharmacy services in heart failure: an opinion paper from the heart failure society of America and American College of clinical pharmacy cardiology practice and research network. Pharmacotherapy. 2013;33(5):529–548. doi:10.1002/phar.1295
15. Granger BB, Swedberg K, Ekman I, et al. Adherence to candesartan and placebo and outcomes in chronic heart failure in the CHARM programme: double-blind, randomised, controlled clinical trial. Lancet. 2005;366(9502):2005–2011. doi:10.1016/S0140-6736(05)67760-4
16. Bemt VD, Tcg E, Berg DJ, Brouwers VD. Drug-related problems in hospitalised patients. Drug Saf. 2000;22(4):321–333. doi:10.2165/00002018-200022040-00005
17. Sztramko R, Chau V, Wong R. Adverse drug events and Associated factors in heart failure therapy among the very elderly; systematic reviews/meta-analysis. Canadian Geriatrics J. 2011;14(4):79–92. doi:10.5770/cgj.v14i4.19
18. Gattis WA, O’Connor CM, Hasselblad V, Gheorghiade M. Predischarge initiation of carvedilol in patients hospitalized for decompensated heart failure results of the Initiation Management Predischarge: process for Assessment of Carvedilol Therapy in Heart Failure (IMPACT-HF) Trial. J Am Coll Cardiol. 2004;43:1534–1541. doi:10.1016/j.jacc.2003.12.040
19. Ong HT, Kow FP. Beta-blockers for heart failure: why you should use them more? Many physicians are afraid to prescribe beta-blockers for patients with heart failure. Yet in most cases, not prescribing them is a mistake. J Fam Pract. 2011;60(8):472–477.
20. Luzier AB, Forrest A, Adelman M, Hawari FI, Schentag JJ, Izzo JL. Impact of angiotensin-converting enzyme inhibitor underdosing on rehospitalization rates in congestive heart failure. Am J Cardiol. 1998;82(4):465–469. doi:10.1016/S0002-9149(98)00361-0
21. Majumdar SR, McAlister FA, Cree M, Chang WC, Packer M, Armstrong PW. Do evidence-based treatments provide incremental benefits to patients with congestive heart failure already receiving angiotensin-converting enzyme inhibitors? A secondary analysis of one-year outcomes from the Assessment of Treatment with Lisinopril and Survival (ATLAS) study. Clin Ther. 2004;26(5):694–703.
22. Gislason GH, Rasmussen JN, Abildstrom SZ, et al. Persistent use of evidence-based pharmacotherapy in heart failure is associated with improved outcomes. J Am Heart Assoc Circulation. 2007;116:737–744.
23. Fonarow GC, Yancy CW, Heywood JT. Adherence to heart failure quality-of-care indicators in US hospitals analysis of the ADHERE registry. Arch Intern Med. 2005;165:1469–1477. doi:10.1001/archinte.165.13.1469
24. Cheng JWM, Cooke-Ariel H. Pharmacists’ role in the care of patients with heart failure: review and future evolution. J Manag Care Pharm. 2014;20(2):206–213. doi:10.18553/jmcp.2014.20.2.206
25. Komajda M, Follath F, Swedberg K, et al. The EuroHeart failure survey program a survey on the quality of care among patients with heart failure in Europe part 2: treatment. Eur Heart J. 2003;24:464–474. doi:10.1016/S0195-668X(02)00700-5
26. Lenzen MJ, Boersma E, Reimer W, et al. Under-utilization of evidence-based drug treatment in patients with heart failure is only partially explained by dissimilarity to patients enrolled in landmark trials: a report from the Euro Heart Survey on Heart Failure. Eur Heart J. 2005;26:2706–2713. doi:10.1093/eurheartj/ehi499
27. Luzier AB, DiTusa L. Underutilization of ACE inhibitors in heart failure. Pharmacotherapy. 1999;19(11):1296–1307. doi:10.1592/phco.19.16.1296.30880
28. Kengne AP, Dzudie A, Sobngwi E. Heart failure in sub-Saharan Africa: a literature review with emphasis on individuals with diabetes. Vasc Health Risk Manag. 2008;4(1):123–130. doi:10.2147/VHRM.S2321
29. Bloomfield GS, Barasa FA, Doll JA, Velazquez EJ. Heart failure in Sub-Saharan Africa. Curr Cardiol Rev. 2013;9:157–173.
30. Damasceno A, Mayosi BM, Sani M, et al. The causes, treatment, and outcome of Acute Heart Failure in 1006 Africans from 9 countries: results of the Sub-Saharan Africa Survey of Heart Failure (THESUS-HF) study. Arch Intern Med. 2012;1–9.
31. Rodgers JE, Stough WG. Underutilization of evidence-based therapies in heart failure: the pharmacist’s role. Pharmacotherapy. 2007;27(4 Pt 2):18S–28S. doi:10.1592/phco.27.4part2.18S
32. Chin MH, Wang JC, Zhang JX, Lang RM. Utilization and dosing of angiotensin-converting enzyme inhibitors for heart failure; effect of physician specialty and patient characteristics. J Gen Intern Med. 1997;12:563–566. doi:10.1046/j.1525-1497.1997.07110.x
33. Baskota M, Rao BS, Shakya R. Study on the prescribing patterns of drugs used in heart failure Kathmandu University. J Sci Eng Technol. 2006;2(1):1–10.
34. Remme WJ, Riegger G, Hildebrandt P, et al. The Benefits of early combination treatment of carvedilol and an ACE-inhibitor in mild heart failure and left ventricular systolic dysfunction; The Carvedilol and ACE-Inhibitor Remodelling Mild Heart Failure Evaluation Trial (CARMEN). Cardiovascular Drugs Ther. 2004;1857–1866.
35. Brophy JM, Joseph L, Rouleau JL. Beta-blockers in congestive heart failure a bayesian meta-analysis. Ann Intern Med. 2001;134(7):550–560. doi:10.7326/0003-4819-134-7-200104030-00008
36. Gupta R, Tang WH, Young JB. Patterns of beta-blocker utilization in patients with chronic heart failure: experience from a specialized outpatient heart failure clinic. Am Heart J. 2004;147(1):79–83. doi:10.1016/j.ahj.2003.07.022
37. Haugbølle LS, Sørensen EW. Drug-related problems in patients with angina pectoris, type 2 diabetes and asthma – interviewing patients at home. Pharm World Sci. 2006;28:239–247. doi:10.1007/s11096-006-9023-9
38. Oliveira D, Brummel AR, Miller DB. Medication therapy management: 10 years of experience in a large integrated health care system. J Manag Care Pharm. 2010;16(3):185–195.
39. Blix HS, Viktil KK, Reikvam A, et al. The majority of hospitalized patients have drug-related problems: results from a prospective study in general hospitals. Eur J Clin Pharmacol. 2004;60:651–658. doi:10.1007/s00228-004-0830-4
40. Hohmann C, Neumann-Haefelin T, Klotz JM, Freidank A, Radziwill R. Drug-related problems in patients with ischemic stroke in hospital. Int J Clin Pharm. 2012;34(6):828–831. doi:10.1007/s11096-012-9690-7
41. Ruths SVK, Blix HS. Classification of drug-related problems. Tidsskr nor Laegeforen. 2007;127:3073–3076.
42. Mysore CT, Nagar SJ, Adepu R. Assessment of drug related problems in stroke patients admitted to a south Indian tertiary care teaching hospital. Indian J Pharm Pract. 2012;5(4):28–33.
43. Lien CTC, Gillespie ND, McMurdo MET, Struthers AD. Heart failure in frail elderly patients: diagnostic difficulties, co-morbidities, polypharmacy and treatment dilemmas. Eur J Heart Fail. 2002;4:91–98. doi:10.1016/S1388-9842(01)00200-8
44. Rama M, Viswanathan G, Acharya LD, Attur RP, Reddy PN, Raghavan SV. Assessment of drug-drug interactions among renal failure patients of nephrology ward in a South Indian Tertiary Care Hospital. Indian J Pharm Sci. 2012;74(1):63–68. doi:10.4103/0250-474X.102545
45. Sato I, Akazawa M. Polypharmacy and adverse drug reactions in Japanese elderly taking antihypertensives: a retrospective database study. Drug Healthc Patient Saf. 2013;5:143–150.
46. Viktil KK, Blix HS, Moger TA, Reikvam A. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol. 2006;63(2):187–195. doi:10.1111/j.1365-2125.2006.02744.x
47. Koh Y, Kutty FBM, Li SC. Drug-related problems in hospitalized patients on polypharmacy: the influence of age and gender. Ther Clin Risk Manag. 2005;1(1):39–48. doi:10.2147/tcrm.1.1.39.53597
48. Abraham RR. Drug related problems and reactive pharmacist interventions for inpatients receiving cardiovascular drugs. Int J Basic Med Sci Pharm. 2013;3(2):42–48.
49. Gastelurrutia P, Tuneu L, Benrimoj SI, Mangues MA, Espejo J, Bayes-Genis A. Negative clinical outcomes associated with drug-related problems in Heart Failure (HF) Outpatients: impact of a pharmacist in a multidisciplinary HF clinic. J Card Fail. 2011;17(3):217–223. doi:10.1016/j.cardfail.2010.10.009
50. Riegel B, Lee CS, Ratcliffe SJ, et al. Predictors of objectively measured medication nonadherence in adults with heart failure. Circ Heart Fail. 2012;5(4):430–436. doi:10.1161/CIRCHEARTFAILURE.111.965152
51. Stromberg A. Patient-related factors of compliance in heart failure: some new insights into an old problem. Eur Heart J. 2006;27:379–381. doi:10.1093/eurheartj/ehi664
52. Niquille A, Bugnon O. Relationship between drug-related problems and health outcomes: a cross-sectional study among cardiovascular patients. Pharm World Sci. 2010;32:512–519. doi:10.1007/s11096-010-9401-1
53. Currie CJ, Peyrot M, Morgan C, et al. The impact of treatment noncompliance on mortality in people with type 2 diabetes. carediabetesjournalsorg. 2012;35:1279–1284.
54. Dilla T, Ciudad A, Álvarez M. Systematic review of the economic aspects of nonadherence to antipsychotic medication in patients with schizophrenia. Patient Prefer Adherence. 2013;7:275–284. doi:10.2147/PPA.S41609
55. Gyllensten H, Rehnberg C, Jönsson AK, Petzold M, Carlsten A, Sundell KA. Cost of illness of patient-reported adverse drug events: a population-based cross-sectional survey. BMJ Open. 2013;3(e002574). doi:10.1136/bmjopen-2013-002574
56. Rahmawati F, Pramantara IDP, Rohmah W, Sulaiman SAS. Polypharmacy and unnecessary drug therapy on geriatric hospitalized patients in Yogyakarta hospitals, Indonesia. Int J Pharm Pharm Sci. 2009;1(Suppl 1):6–11.
57. Ernst FR, Grizzle AJ. Drug-related morbidity and mortality: updating the cost-of-illness model. J Am Pharm Assoc. 2001;41:192–199.
58. Wal M, Jaarsma T, Veldhuisen D. Non-compliance in patients with heart failure; how can we manage it? Eur J Heart Fail. 2005;7(1):5–17. doi:10.1016/j.ejheart.2004.04.007
59. Mujtaba SF, Masood T, Khalid D. Personal and social factors regarding medical non-compliance in cardiac failure patients. J Coll Physicians Surg Pak. 2011;21(11):659–661.
60. Toh CT, Jackson B, Gascard DJ, Manning AR, Tuck EJ. Barriers to medication adherence in chronic heart failure patients during home visits. J Pharm Pract Res. 2010;40:27–30. doi:10.1002/j.2055-2335.2010.tb00721.x
61. Viktil KK, Blix HS. The impact of clinical pharmacists on drug-related problems and clinical outcomes. Basic Clin Pharmacol Toxicol. 2008;102(MiniReview):275–280. doi:10.1111/j.1742-7843.2007.00206.x
62. Gattis WA, Hasselblad V, Whellan DJ, O’Connor CM, Pharmacist in Heart Failure Assessment Recommendation and Monitoring (PHARM) Study Investigators. Reduction in heart failure events by the addition of a clinical pharmacist to the heart failure management team: results of the pharmacist in heart failure assessment recommendation and monitoring (PHARM) study. Arch Intern Med. 1999;159(16):1939–1945. doi:10.1001/archinte.159.16.1939
63. Koshman SL, Charrois TL, Simpson SH, McAlister FA, Tsuyuki RT. Pharmacist care of patients with heart failure: a systematic review of randomized trials. Arch Intern Med. 2008;168(7):687–694. doi:10.1001/archinte.168.7.687
64. McAlister FA, Stewart S, Ferrua S, McMurray JJJV. Multidisciplinary strategies for the management of heart failure patients at high risk for admission a systematic review of randomized trials. J Am Coll Cardiol. 2004;44(4):810–819.
65. Wijeysundera HC, Trubiani G, Wang X, et al. A population-based study to evaluate the effectiveness of multidisciplinary heart failure clinics and identify important service components. Circ Heart Fail. 2013;6:68–75. doi:10.1161/CIRCHEARTFAILURE.112.971051
66. Kumar SB, Dahal P, Ventakaraman R, Fuloria PC. Assessment of clinical pharmacist intervention in tertiary care teaching hospital of southern India. Asian J Pharm Clin Res. 2013;6(Suppl 2):258–261.
67. Cipolle RJ, Strand LM, Morley PC. Pharmaceutical Care Practice. New York, NY: McGraw Hill; 1998.
68. Strand LM, Morley PC, Cipolle RJ, Ramsey R, Lamsam GD. Drug-related problems: their structure and function. DICP. 1990;24(11):1093–1097. doi:10.1177/106002809002401114
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.