")
Back to Journals » Clinical Interventions in Aging » Volume 15
Driver Self-Regulation Practices in Older Drivers with and Without Mild Cognitive Impairment
Authors Feng YR, Meuleners L, Stevenson M, Heyworth J , Murray K, Maher S
Received 1 November 2019
Accepted for publication 13 December 2019
Published 14 February 2020 Volume 2020:15 Pages 217—224
DOI https://doi.org/10.2147/CIA.S236998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Ying Ru Feng,1 Lynn Meuleners,1 Mark Stevenson,2,3 Jane Heyworth,1 Kevin Murray,1 Sean Maher4
1School of Population and Global Health, The University of Western Australia, Perth, WA, Australia; 2Transport, Health and Urban Design, Melbourne School of Design, University of Melbourne, Melbourne, VIC, Australia; 3Melbourne School of Population and Global Health, University of Melbourne, Melbourne, VIC, Australia; 4Department of Rehabilitation and Aged Care, Sir Charles Gairdner Hospital, Perth, WA, Australia
Correspondence: Lynn Meuleners
School of Population and Global Health, The University of Western Australia (M431), 35 Stirling Hwy, Crawley, Perth, WA 6009, Australia
Tel +61 8 6488 7375
Email [email protected]
Objective: To assess the impact of cognitive, socio-demographic and driving-related characteristics on self-regulation practices in older drivers with mild cognitive impairment (MCI) (determined by the Telephone Cognitive Screen (T-CogS) score), compared with drivers with no cognitive impairment.
Design, Setting, Participants: A cross-sectional study collected information from 362 drivers with MCI and 611 drivers with no cognitive impairment, who were aged 65+ years, and were living in Western Australia between November 2018 and February 2019.
Measurements: Self-reported self-regulation driving practices.
Results: The majority of drivers with MCI (62.4%) and those with no cognitive impairment (57.1%) reported self-regulating their driving in at least one situation, in the past three months. The most common situations that both groups of drivers self-regulated in were “driving at night in the rain”, “parallel parking”, and “driving when raining”. Drivers with MCI were only significantly more likely to self-regulate when “making turns across oncoming traffic” and “driving at night”. They also had 39% greater odds of self-regulating in at least one driving situation, compared with drivers with no cognitive impairment (OR: 1.39, 95% CI=1.04– 1.85, p=0.02). Females also had 2.3 times greater odds of self-regulating (OR=2.34, 95% CI=1.76– 3.12, p< 0.001). Drivers aged 75+ years had 1.6 times greater odds of self-regulating, compared with drivers aged 65– 69 years (OR=1.58, 95% CI=1.12– 2.23, p=0.01).
Conclusion: Older drivers with MCI were more likely to self-regulate their driving, compared to drivers with no cognitive impairment, particularly in complex driving situations. This suggests that some drivers with MCI may be able to recognize their cognitive limitations and adjust their driving accordingly. However, several drivers with MCI, particularly males, did not self-regulate their driving. This highlights the importance of advising patients about the impact of MCI on driving ability, suitable self-regulation strategies, as well as monitoring their driving ability.
Keywords: driving, aging, self-regulation, older drivers, mild cognitive impairment
Introduction
An aging population and the need to drive in order to maintain independence and social inclusion1 has led to an increase in the number of older drivers on our roads.2 In Australia, the road crash fatality rate is higher for drivers aged 75+ years (over 10 per 100,000 population in 2013), compared to other age groups (approximately 6 per 100,000 population).2 As the proportion of Australian adults aged 65+ years is expected to reach 22% within the next forty years,3 the safety of older drivers is becoming increasingly important.
Driving is a complex task and cognitive conditions such as mild cognitive impairment (MCI) may affect the ability to drive safely.4 MCI is the stage between normal cognitive aging and dementia where cognitive decline has not reached the threshold for a diagnosis of dementia.5 While many drivers with MCI may be able to safely operate a motor vehicle for an extended period, even small declines in cognition may impact on driving performance and crash risk.4,6 For example, drivers with MCI may exhibit poorer driving abilities in terms of lane control, speed management and gap judgment than drivers with no cognitive impairment.7,8
Driver self-regulation can be defined as situations when drivers modify their driving behavior to avoid challenging situations.9 Although self-regulation practices can be used by any driver, they are most commonly observed in older drivers, due to an increase in the number of age-related impairments.10 Driver self-regulation is an important road safety strategy for older drivers. When drivers can recognize their declining abilities and avoid driving situations they find difficult, it may allow them to keep driving safely for longer, as well as reduce crash involvement.11–13 Examples of situations where drivers may self-regulate include reducing the number of kilometers traveled, driving only in familiar areas, and eliminating driving in more difficult situations, such as at night.14 However, there is concern that a lack of insight associated with MCI may reduce a driver’s capacity to self-regulate their driving accordingly.15
A systematic review consisting of 12 studies found strong evidence that older drivers with cognitive impairment engage in self-regulation by either reducing their driving or avoiding certain situations.16 A number of studies, predominantly with small sample sizes, have specifically examined MCI and driving self-regulation. These studies consistently reported lower driving frequency or self-reported driving avoidance among those with cognitive impairment compared to normal controls.13,17–20
Less is known, however, about driver self-regulation practices in specific driving situations that a person with MCI may find difficult. A small study in the United States (US) on 40 older drivers with clinical MCI reported that they avoided driving in unfamiliar areas and on high traffic roads significantly more than drivers without any cognitive impairment.13 A large Danish study (n=840) also reported that lower functioning participants were significantly more likely to avoid certain driving situations.20 These included slippery conditions, driving in the dark, long trips, dense traffic, overtaking, unfamiliar areas, areas with cyclists, and intersections with no traffic lights.20 It should be noted however that this study differentiated participants’ cognitive status based on self-reported cognitive problems, rather than a cognitive assessment or screening.20 This early evidence suggests that older drivers with MCI may avoid more complex driving situations. A large study examining older drivers by their self-regulation status as well as the specific driving situations in which they self-regulate would add valuable information to the body of knowledge. Therefore, this study aimed to assess the impact of cognitive, socio-demographic and driving-related characteristics on self-regulation practices in older drivers with MCI (determined by the Telephone Cognitive Screen (T-CogS) score) compared with drivers with no cognitive impairment.
Methods
Study Design
A cross-sectional study was undertaken of current drivers with and without MCI who were aged 65+. This study is part of a larger prospective cohort study examining the association between cognitive ability and driving outcomes. Ethics Committee approval was obtained from The University of Western Australia Human Ethics Committee #RA/4/20/5126.
Sample
Potential participants were identified from a WA database of all older drivers and randomly selected to be contacted by one of fourteen trained interviewers from the Survey Research Centre, located at Edith Cowan University. They were contacted between 9AM and 9PM, Monday to Friday, from November 2018 to February 2019. As the study aimed to recruit both drivers with MCI and with no cognitive impairment, participants living in seven local government areas were targeted, as there is a higher prevalence of people with cognitive impairment and dementia living in these locations.21 Inclusion criteria stipulated that participants were aged 65+ years, had a current WA driver’s license, drove a minimum of twice a week, and lived in the Perth metropolitan area. Exclusion criteria were: a diagnosis of Parkinson’s disease, severe hearing loss, or did not speak English.
The Telephone Cognitive Screen (T-CogS) was used to determine the cognitive status of drivers, which was administered over the phone. The 26 item T-CogS was developed by Newkirk et al (2004) and is a telephone version of Folstein’s Mini-Mental State Examination (MMSE) which measures cognitive function.22,23 It includes tests of orientation, attention, memory and language. It has been validated against the MMSE in a group of patients with Alzheimer’s disease with a correlation of 0.88.22 MCI was defined as a score of 21 to 24 in the T-CogS, and normal cognition was a score of 25 or 26.22,24 Participants who scored ≤20 were excluded from the study. It is important to note that in this study the categorization of participants as having MCI was based on their score on the T-CogS. This categorization does not infer that participants have clinically defined MCI, which can be diagnosed using the Peterson/Mayo criteria.5
Sample Size Calculation
It was conservatively estimated that if 35% of drivers with MCI self-regulate their driving in at least one driving situation, then a sample of 365 drivers with MCI and 550 drivers with no cognitive impairment would have 90% power to detect a difference in the proportion of drivers who self-regulated in at least one situation at a significance level α=0.05.
Data Collection
Before any information was collected informed consent was obtained from each participant. Participation was voluntary and individuals were told that they could withdraw from the study at any time during the interview. A structured telephone questionnaire was administered which took approximately 25 minutes. Information on age, gender, marital status, highest education achieved, living arrangements, comorbidities, and prescription medication was obtained. Participants self-reported their diagnosed comorbidities and any prescription medications they were taking. Information related to driving license, car ownership, number of crashes and infringements they had received in the past year was also obtained.
Self-Reported Driver Self-Regulation
Questions on driver self-regulation behavior were collected from a driving questionnaire, which was validated on a Western Australian population.25 Self-regulation status was determined by whether a participant had or had not driven in at least one of the following driving situations in the past three months: “driving when it is raining”, “driving alone”, “parallel parking”, “making turns across oncoming traffic”, ''driving on highways or freeways'', “driving on heavy traffic roads”, “driving in peak hour traffic”, “driving at night” and “driving at night in the rain”. If a participant self-reported that they had not driven in at least one of the driving situations, they were considered to be a “self-regulator”. If a participant responded that they had driven in all the driving situations, they were considered a “non self-regulator”.15,26 The total number of driving situations that a participant reported self-regulating in was also determined.
Statistical Analysis
Descriptive statistics were used to summarize all variables of interest. Chi-square tests were used to test for differences in self-regulation practices between those with MCI and those with no cognitive impairment in the nine driving situations.
The outcome of interest was self-reported self-regulation in at least one driving situation (yes/no). A multivariate logistic regression model was undertaken to examine the association between cognitive status (MCI/no cognitive impairment), socio-demographic characteristics (age, gender, highest education achieved, living arrangement, comorbidities and prescription medications), driving characteristics and self-regulation status. Interactions between cognitive status/gender, and cognitive status/age group were tested, however, neither interaction was significant and they were not included in the final logistic regression model. All statistical analyses were undertaken using SAS 9.4.
Results
Socio-Demographic Characteristics
The interviewers contacted 2525 participants. Of these participants, 1175 were ineligible with 1077 (93.9%) under 65 years of age, 48 (4.2%) were too ill, 22 (1.9%) did not speak English, and 28 participants scored ≤20 on the T-CogS. Of the remaining 1350 participants, 377 refused to participate in the study with a final sample of 973 eligible participants. This represented a response rate of 72.1%.
Overall, 362 drivers with MCI and 611 drivers with no cognitive impairment were recruited for the study. For drivers with no cognitive impairment the mean T-CogS score was 25.5 (SD=0.50, range=25–26) and for drivers with MCI the mean T-CogS score was 23.3 (SD=0.90, range=21–24).
Table 1 presents the socio-demographic and driving characteristics of drivers by self-reported driver self-regulation and cognitive status. For drivers with MCI, who self-regulated their driving, the majority were female (53.5%), ≥75 years (47.8%), in a married/de facto relationship (76.1%), had achieved higher education (51.6%), did not live alone (80.5%), had 1–3 comorbidities (58.4%), and were on prescription medications (84.1%). Compared with drivers with MCI who did not self-regulate a similar pattern was evident, however the majority in this group were male (72.1%) and between 70–74 years (54.3%).
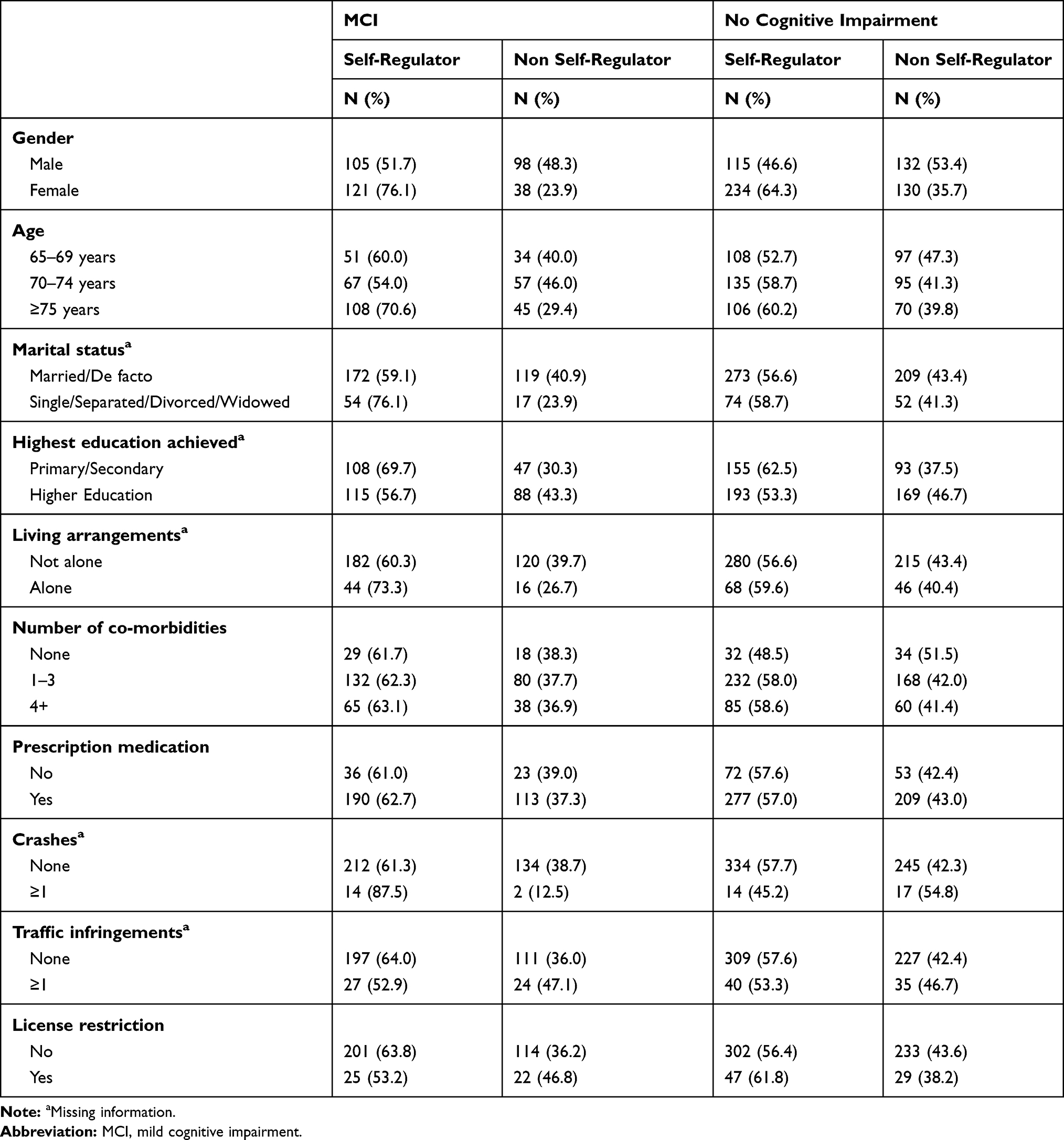 |
Table 1 Socio-Demographic and Driving Characteristics of Older Drivers with MCI and with No Cognitive Impairment by Self-Regulation Status |
The majority of drivers with no cognitive impairment who self-regulated their driving were female (67.0%), 70–74 years (38.7%), in a married/de facto relationship (78.2%), had achieved higher education (55.3%), did not live alone (80.2%), had 1–3 comorbidities (66.5%), and were on prescription medications (79.4%). These demographics were also similar for drivers with no cognitive impairment who did not self-regulate however, the majority were male (50.4%), and aged between 65–69 years (37.0%).
Driving Characteristics
Almost 88% (n=14) of drivers with MCI who were involved in at least one crash in the past year self-regulated their driving compared with only 45% (n=14) of drivers with no cognitive impairment who crashed and reported self-regulating their driving.
Of drivers with MCI who had received an infringement, the majority self-regulated their driving (52.9%, n=27). Similarly, for drivers with no cognitive impairment who had received an infringement, the majority also self-regulated their driving (53.3%, n=40).
Similar to traffic infringements, the majority of drivers with MCI (53.2%, n=25) and with no cognitive impairment (61.8%, n=47) who had license restrictions reported self-regulating their driving.
Driver Self-Regulation
Table 2 summarizes the driving situations in which drivers with MCI and no cognitive impairment self-regulated their driving. Overall, 62.4% (n=226) of drivers with MCI and 57.1% (n=349) of drivers with no cognitive impairment self-regulated their driving in at least one situation. The average number of situations in which older drivers self-regulated their driving was 1.34 (SD=1.50) for drivers with MCI and 1.17 (SD=1.39) for drivers with no cognitive impairment. “Driving at night in the rain” (p=0.203), “parallel parking” (p=0.747), and “driving when raining” (p=0.744) were the most frequently reported situations in which both drivers with MCI and with no cognitive impairment self-regulated their driving. The only significant differences reported between drivers with MCI and no cognitive impairment was when “driving at night” (p=0.021), and “making turns across oncoming traffic” (p=0.048).
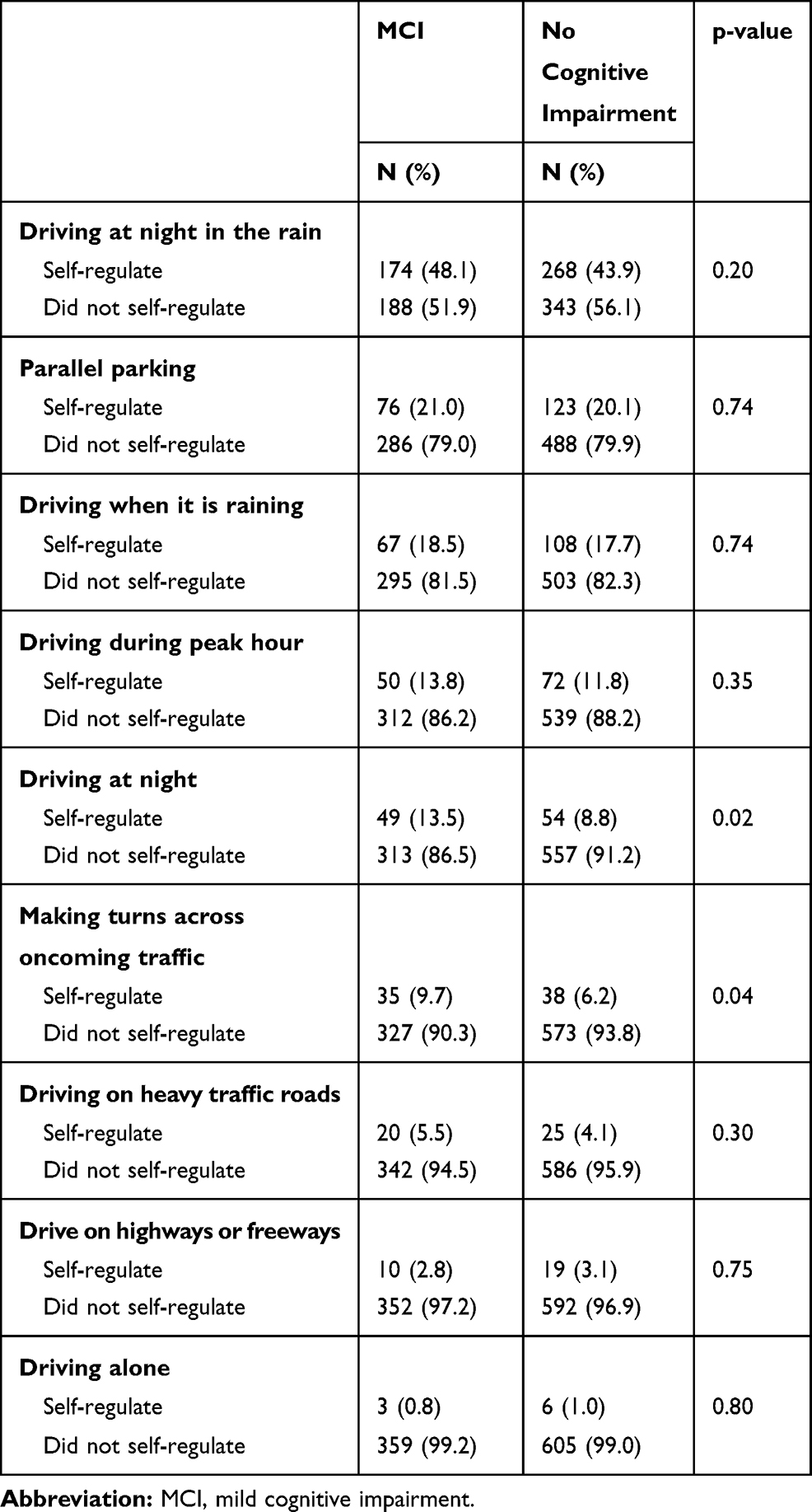 |
Table 2 Self-Regulation of Driving Situations for Drivers with MCI and with No Cognitive Impairment |
Table 3 presents the results from the multivariate logistic regression. The odds of self-regulating in at least one driving situation significantly increased by 39% for drivers with MCI, compared with drivers with no cognitive impairment (adjusted OR: 1.39, 95% CI=1.04–1.85, p=0.024). The odds were significantly more than double for self-regulation practices for female drivers compared with male drivers (adjusted OR=2.34, 95% CI=1.76–3.12, p=<0.001). The odds of self-regulating in at least one situation was 58% higher for drivers aged over 75 years, compared with drivers aged between 65 and 69 years (adjusted OR=1.58, 95% CI=1.12–2.23, p=0.010). There were no driving characteristics significantly associated with driver self-regulation practices.
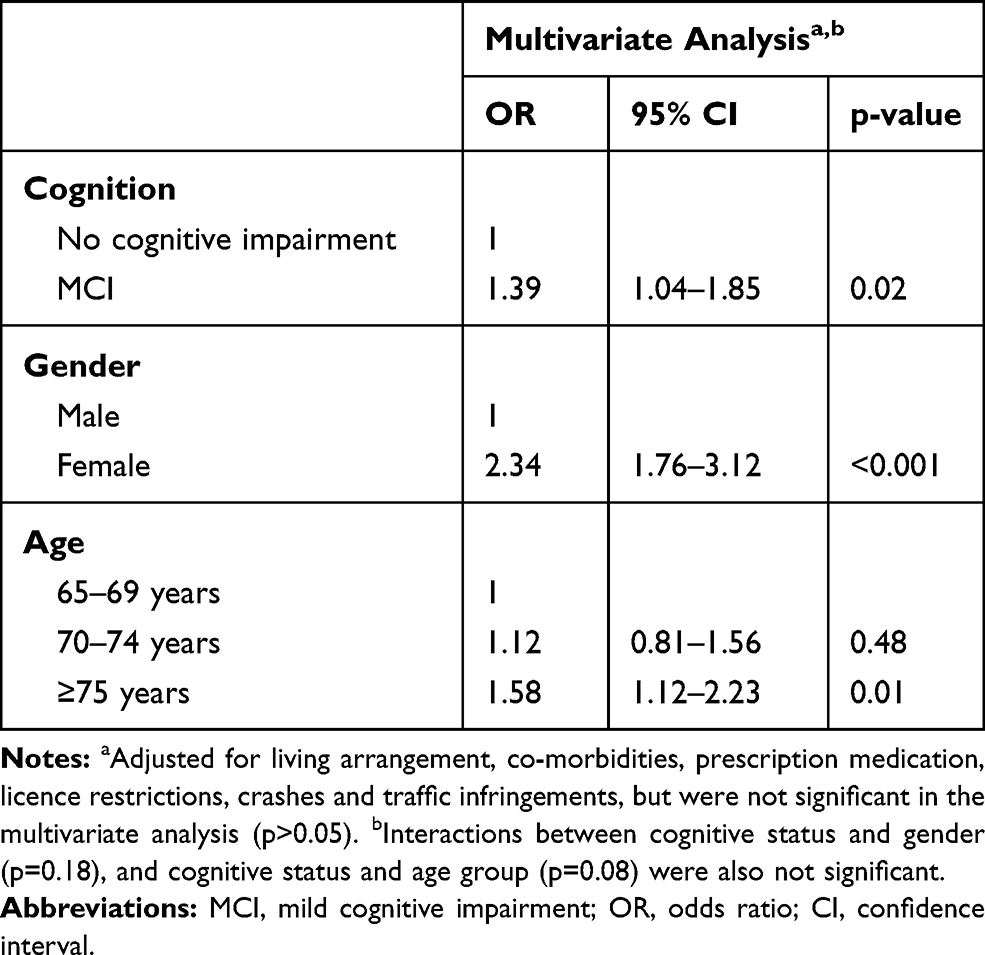 |
Table 3 Multivariate Logistic Regression Analysis of Driver Self-Regulation in at Least One Driving Situation for Drivers with MCI and with No Cognitive Impairment |
Discussion
This study found that drivers with MCI were significantly more likely to adopt driver self-regulation practices compared with drivers with no cognitive impairment and is consistent with previous research.13,16,18,20 It also suggests that drivers with MCI may have recognized their cognitive limitations and adjusted their driving accordingly. Female drivers and drivers who were aged 75+ years were also more likely to self-regulate their driving, which is consistent with previous research.9,10,27 Earlier studies have presented several reasons for these findings including that males are more often the main driver,28 females enjoy driving less,29 and that females recognize and acknowledge a decline in their driving performance more easily than males leading to a change in driving habits.29 It is also possible that due to driving less when younger, females are more familiar with other modes of transport facilitating driver self-regulation.30
There were similarities in the driving situations in which both drivers with MCI and no cognitive impairment reported self-regulation practices however, drivers with MCI were more likely to avoid “making turns across oncoming traffic” and “driving at night”, compared with drivers with no cognitive impairment. These represent more complex driving situations. Turning across oncoming traffic involves processing information quickly and MCI may affect this ability.31 This was evident in a simulator study which found that the MMSE score negatively correlated with the number of collisions involving turns across oncoming traffic.32 Impairments in visual processing ability may also explain why drivers with MCI restrict their driving at night.33 Previous studies from the US and Denmark have reported that drivers with MCI avoided complex situations, including driving at night,20 unfamiliar areas and high density traffic.13,20 This is the first study to report self-regulation when making turns across traffic with MCI and may reflect different traffic environments and infrastructure between countries.
Although a large majority of drivers with MCI reported self-regulating their driving 36% of drivers with MCI did not self-regulate in any of the nine driving situations. For many older adults driving cessation can contribute to poorer quality of life and a lack of independence.34 It is possible that some drivers in our study with MCI may have been reluctant to make changes to their usual driving patterns or were not aware of their cognitive impairment and felt it was unnecessary to self-regulate. As our study only examined whether drivers had driven in certain driving situations, future research should examine the motives behind self-regulation practices.
The strength of the study include the large sample size and the use of a comparison group of older drivers with no cognitive impairment. Furthermore, potential confounders, including driving related characteristics, were controlled for in the analyses. However, drivers’ cognitive status was classified using the T-CogS and is a limitation of this study. Although the T-CogS has been validated,22 it is not a diagnostic tool and does not test executive function.35 It was also not known whether participants who were classified as having MCI were aware of their impairment. The sample was a convenience sample and volunteer bias may be present as drivers more confident in their driving abilities would be more inclined to participate in the study. Information regarding self-regulation status was self-reported, which may lead to a social desirability bias. Furthermore, recall bias may be present, as participants were asked about driving situations in the past three months. Lastly, the study did not ask if the driver restricted their driving due to reasons related to loss of confidence or need and future research should examine the reasons for their driving restriction.
Conclusion
Older drivers with MCI were more likely to self-regulate their driving, compared to drivers with no cognitive impairment, particularly in complex driving situations like driving at night and making turns across oncoming traffic. This suggests that some drivers with MCI may be able to recognize their cognitive limitations and adjust their driving accordingly. However, over one-third of drivers with MCI did not self-regulate their driving and this was more common among males. It is therefore important for health professionals to advise patients, particularly males, of the impact of mild cognitive impairment on driving ability, suitable self-regulation strategies, alternative transport options, and how to monitor their driving ability.
Further longitudinal research is needed to examine changes in self-regulation practices in drivers with MCI and whether these practices are adequate to compensate for their declining cognitive impairment. Future research should also collect objective information on self-regulation practices using in-vehicle monitoring devices.
Acknowledgments
The authors would like to acknowledge the staff at the Survey Research Centre, Edith Cowan University for their assistance in the recruitment of study participants. They would also like to thank the study participants for their time and involvement in the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Australian Research Council Linkage Grant #LP160101446. The funding source had no role in the design of the study, methodology of the study, recruitment of study participants, collection of data, analysis of data, or preparation of manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mezuk B, Rebok GW. Social integration and social support among older adults following driving cessation. J Gerontol B Psychol Sci Soc Sci. 2008;63(5):S298–S303. doi:10.1093/geronb/63.5.S298
2. Bureau of Infrastructure Transport and Regional Economics. Road Safety of Older Australians: Recent Statistics. Canberra: BITRE, Australian Government; 2014.
3. Australian Institute of Health and Welfare. Older Australia at a Glance. Canberra: AIHW2018. Australian Government; 2018.
4. Fraade-Blanar Laura A, Ebel Beth E, Larson Eric B, et al. Cognitive decline and older driver crash risk. J Am Geriatr Soc. 2018;66(6):1075–1081.
5. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256(3):183–194. doi:10.1111/j.1365-2796.2004.01388.x
6. Anderson S, Rizzo M, Shi Q, Dawson J. Cognitive abilities related to driving performance in a simulator and crashing on the road.
7. Wadley VG, Okonkwo O, Crowe M, et al. Mild cognitive impairment and everyday function: an investigation of driving performance. J Geriatr Psychiatry Neurol. 2009;22(2):87–94. doi:10.1177/0891988708328215
8. Anstey KJ, Eramudugolla R, Chopra S, Price J, Wood JM. Assessment of driving safety in older adults with mild cognitive impairment. J Alzheimers Dis. 2017;57(4):1197–1205. doi:10.3233/JAD-161209
9. Charlton JL, Oxley J, Fildes B, Oxley P, Newstead S. Self-regulatory behaviours of older drivers. Annu Proc Assoc Adv Automot Med. 2003;47:181–194.
10. Gwyther H, Holland C. The effect of age, gender and attitudes on self-regulation in driving. Accid Anal Prev. 2012;45:19–28. doi:10.1016/j.aap.2011.11.022
11. Baldock MR, Mathias JL, McLean AJ, Berndt A. Self-regulation of driving and its relationship to driving ability among older adults. Accid Anal Prev. 2006;38(5):1038–1045. doi:10.1016/j.aap.2006.04.016
12. Molnar LJ, Eby DW, Charlton JL, et al. Driving avoidance by older adults: is it always self-regulation? Accid Anal Prev. 2013;57:96–104. doi:10.1016/j.aap.2013.04.010
13. O’Connor ML, Edwards JD, Bannon Y. Self-rated driving habits among older adults with clinically-defined mild cognitive impairment, clinically-defined dementia, and normal cognition. Accid Anal Prev. 2013;61:197–202. doi:10.1016/j.aap.2013.05.010
14. Braitman KA, Williams AF. Changes in self-regulatory driving among older drivers over time. Traffic Inj Prev. 2011;12(6):568–575. doi:10.1080/15389588.2011.616249
15. Molnar LJ, Eby DW. The relationship between self-regulation and driving-related abilities in older drivers: an exploratory study. Traffic Inj Prev. 2008;9(4):314–319. doi:10.1080/15389580801895319
16. Devlin A, McGillivray JA. Self-regulation of older drivers with cognitive impairment: a systematic review. Australas J Ageing. 2014;33(2):74–80. doi:10.1111/ajag.2014.33.issue-2
17. O’Connor ML, Edwards JD, Wadley VG, Crowe M. Changes in mobility among older adults with psychometrically defined mild cognitive impairment. J Gerontol B Psychol Sci Soc Sci. 2010;65B(3):306–316. doi:10.1093/geronb/gbq003
18. Pavlou D, Papantoniou P, Papadimitriou E, et al. Self-assessment of older drivers with brain pathologies: reported habits and self-regulation of driving. J Transp Health. 2017;4:90–98. doi:10.1016/j.jth.2016.08.008
19. Vance DE, Roenker DL, Cissell GM, Edwards JD, Wadley VG, Ball KK. Predictors of driving exposure and avoidance in a field study of older drivers from the state of Maryland. Accid Anal Prev. 2006;38(4):823–831. doi:10.1016/j.aap.2006.02.008
20. Meng A, Siren A. Cognitive problems, self-rated changes in driving skills, driving-related discomfort and self-regulation of driving in old drivers. Accid Anal Prev. 2012;49:322–329. doi:10.1016/j.aap.2012.01.023
21. Access Economics Pty Limited for Alzheimer’s Australia WA. Projections of dementia prevalence and incidence in WA: 2010–2050. 2010.
22. Newkirk LA, Kim JM, Thompson JM, Tinklenberg JR, Yesavage JA, Taylor JL. Validation of a 26-point telephone version of the mini-mental state examination. J Geriatr Psychiatry Neurol. 2004;17(2):81–87. doi:10.1177/0891988704264534
23. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
24. Trzepacz PT, Hochstetler H, Wang S, Walker B, Saykin AJ. Relationship between the Montreal cognitive assessment and mini-mental state examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 2015;15:107. doi:10.1186/s12877-015-0103-3
25. Fraser ML, Meuleners LB, Lee AH, Ng JQ, Morlet N. Which visual measures affect change in driving difficulty after first eye cataract surgery? Accid Anal Prev. 2013;58:10–14. doi:10.1016/j.aap.2013.04.015
26. Devlin A, McGillivray J. Self-regulatory driving behaviours amongst older drivers according to cognitive status. Transp Res Part F Traffic Psychol Behav. 2016;39:1–9. doi:10.1016/j.trf.2016.02.001
27. Marie Dit Asse L, Fabrigoule C, Helmer C, Laumon B, Lafont S. Automobile driving in older adults: factors affecting driving restriction in men and women. J Am Geriatr Soc. 2014;62(11):2071–2078. doi:10.1111/jgs.13077
28. Brabyn JA, Schneck ME, Lott LA, Haegerstrom-Portnoy G. Night driving self-restriction: vision function and gender differences. Optom Vis Sci. 2005;82(8):755–764. doi:10.1097/01.opx.0000174723.64798.2b
29. D’Ambrosio LA, Donorfio LKM, Coughlin JF, Mohyde M, Meyer J. Gender differences in self-regulation patterns and attitudes toward driving among older adults. J Women Aging. 2008;20(3–4):265–282. doi:10.1080/08952840801984758
30. Hakamies-Blomqvist L, Siren A. Deconstructing a gender difference: driving cessation and personal driving history of older women. J Safety Res. 2003;34(4):383–388. doi:10.1016/j.jsr.2003.09.008
31. Cassavaugh ND, Domeyer JE, Backs RW. The effect of age on decision making during unprotected turns across oncoming traffic.
32. Dawson JD, Yu L, Chen K-H, et al. Neuropsychological predictors of safety in urban left-turn scenarios. Proc Int Driv Symp Hum Factors Driv Assess Train Veh Des. 2013;2013:226–232.
33. Owsley C, Ball K, McGwin G
34. Chihuri S, Mielenz TJ, DiMaggio CJ, et al. Driving cessation and health outcomes in older adults. J Am Geriatr Soc. 2016;64(2):332–341. doi:10.1111/jgs.13931
35. McDowell I. Measuring Health: A Guide to Rating Scales and Questionnaires. USA: Oxford University Press; 2006.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.