")
Back to Journals » Patient Preference and Adherence » Volume 14
Does the Modality Used in Health Coaching Matter? A Systematic Review of Health Coaching Outcomes
Authors Singh H , Kennedy GA , Stupans I
Received 15 June 2020
Accepted for publication 4 August 2020
Published 24 August 2020 Volume 2020:14 Pages 1477—1492
DOI https://doi.org/10.2147/PPA.S265958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Harjit Singh,1 Gerard A Kennedy,1– 3 Ieva Stupans1
1The School of Health and Biomedical Sciences, RMIT University, Melbourne, VIC, Australia; 2School of Science, Psychology and Sport, Federation University, Melbourne, VIC, Australia; 3Institute for Breathing and Sleep, Austin Health, Melbourne, VIC, Australia
Correspondence: Harjit Singh
The School of Health and Biomedical Sciences, RMIT University, Bundoora, Melbourne, VIC 3083, Australia
Email [email protected]
Objective: The purpose of this review was to evaluate the modalities (e.g., face-to-face, telephone or electronic) of pharmacist health coaching providing the greatest improvement in patient outcomes, to enable a more comprehensive evaluation to be done and quality decision-making around health coaching modalities to be undertaken by pharmacists.
Methods: This systematic review followed the PRISMA guidelines. CINHAL, EMBASE, PubMed, PsychINFO and SCOPUS were searched (2000– 2019). Included articles were reviewed for the modality used to health coach, the training provided, and the outcomes.
Results: Twelve papers met the eligibility criteria. A majority of studies included involved a combination of modalities of pharmacist health coaching. Four papers referred to face-to-face sessions, and one study used telephone coaching. In each paper, coaching led to an improvement in clinical and non-clinical health outcomes.
Conclusion: The training provided to health coaches varied and in some cases was not reported. Inconsistencies in reports led to difficulties when comparing study outcomes. Therefore, conclusions about the modality providing the greatest improvement in patient outcomes and the most pragmatic health coaching modality are not possible. Studies that document the training, the modality, the outcomes and the cost benefits of coaching by pharmacists are warranted to enable a more comprehensive evaluation to be done and quality decision-making around health coaching modalities to be undertaken by pharmacists.
Keywords: health, coaching, pharmacy, modalities
Introduction
Unhealthy behaviors have been linked to the increasing prevalence of preventable chronic diseases worldwide, putting significant strain on healthcare infrastructures.1 The most common of these include; chronic respiratory disease, cardiovascular disease, diabetes and cancer.1 Chronic health conditions are those that are prolonged and complex in nature, and although treatable, are unable to be completely cured. Therefore, these conditions require ongoing monitoring and management.2
As comprehensively trained healthcare professionals at the front line of the health care system, pharmacists are ideally positioned to administer community programs and services that promote health.3 In spite of their extensive training and having the capability to provide a range of services, in Australia the skills of a pharmacist are often over-looked. Consequently, the main duties of a pharmacist continue to comprise of dispensing, despite the introduction of contemporary pharmacist services in the 1980s. These services included screening, medication reviews, medication education, and in-depth counseling sessions designed to promote patient-centered care.4–7
The introduction of pharmacy professional services has paved the way for pharmacists to utilize the knowledge and skills gained through education and training.7,8 A number of services have already been effectively implemented by pharmacists, but the incorporation of these services into routine pharmacy practice has been gradual.3,9,10 This has been attributed to the lack of time pharmacists have and the low rates of remuneration received for these services.10 However, services that have a beneficial effect on patient health outcomes are more likely to promote and expand the professional responsibilities of a pharmacist.11
Health coaching is a promising intervention, helping individuals change health behaviors positively.12,13 It is defined as a service that is provided to patients by health care professionals with the intent to promote health management/health risk prevention. The interaction between patient and health professional is collaborative and patient focused. It requires the healthcare professional to facilitate changes to the patients’ health behaviors through health education and motivation in order to achieve predetermined personal goals and targets. Patients have regular follow-up sessions with the health care professionals during which time both are held accountable for the patient’s outcomes.16 Health coaching has recently gained attention within the pharmacy profession, as a possible way to assist patients with health education, medication adherence, and prevention and management of chronic health conditions.17,18
Studies have shown that optimizing health and lifestyle behaviors can have a significant effect on the prevention and management of chronic health conditions.12,19 Health coaching is a professional service that is offered to patients by health care professionals with the intent to promote management of chronic health conditions and prevent complications. It involves a patient-focused interaction with the aim to improve health behaviors through goal setting and follow-up.16 Health coaching is distinct to other lifestyle and health improvement programs provided by health professionals, such as counselling. Counselling is characterized as having a rigid method to health education and management, as it involves the health care provider instructing the patient about changes to make, taking little acknowledgment of the patient’s own goals and desire for change.20–22 In contrast, health coaching can be individualized to a patient and can be adjusted to respect the needs and desires of the patient.22
Various health coaching modalities have been used by pharmacists. These include telephone, face-to-face, electronic including texts, online links, applications and videos, or a combination of these media.16,18,23-26
Globally, governments are acknowledging the need to improve patient access to quality pharmaceutical services and the need for choice across a range of services.27 The provision of new models of service delivery is dependent on the efficacy of various modalities and its economic viability from the perspective of the provider organizations and the patients.27
Pharmacist health coaching studies have not investigated the modalities of health coaching providing the greatest effect with respect to patient health outcomes. Studies have also not addressed the practicalities of coaching interventions or the specific training requirements for pharmacists engaged in health coaching. Limited studies have investigated the cost-effectiveness of health coaching interventions.
Telephone health coaching refers to patients being contacted by the pharmacist health coach over by telephone, usually at a mutually agreed time. The duration and number of, telephone health coaching sessions can vary.28 This mode of health coaching is considered convenient to patients, as there is no need to travel and thus is suitable for patients living in rural areas as well as those unable to travel.25 Furthermore, there are minimal costs associated with the delivery of a telephone health coaching service as the health coach directly contacts the patient.25
Face-to-face health coaching is undertaken in person. This may involve the health coach travelling to the patient’s home,29 alternatively the coaching may take place at the coach’s workplace18,23,24 or another mutually agreed location. Consequently, this mode of health coaching may be inconvenient for some patients. However, it promotes and helps maintains rapport and accountability between the patient and coach, without which the process of health coaching may not be successful.16,30
Electronic health coaching includes the use of text messaging, online links, applications and videos. This mode of health coaching is convenient and can be tailored to the individual. The time taken to implement some of these modes could be a drawback, but it is a modality that can be used to health coach multiple patients simultaneously.26
In an effort to reduce healthcare expenditure globally, public health care funders have shifted focus towards preventative health services, like health coaching.31 Studies have shown that investment in wellness programs prove cost-effective as they reduce financial pressures on health care systems, whilst promoting health and disease management. The programs also increase performance and productivity at work due to improved health and reduced sick days.32 This was demonstrated in a large-scale employer-sponsored Canadian study, whereby community pharmacist-led health coaching in patients with hypertension promoted employee productivity through improved medication adherence and patient health outcomes.33 Similarly, private health insurer and employer-sponsored health insurers in the United States have successfully funded the provision of pharmacist health coaching programs for patients with chronic issues such as; chronic artery disease, chronic obstructive pulmonary disease, diabetes, lower back pain and heart failure.31,34,35 Studies investigating the outcomes of such programs have reported positive health results, indicating that promoting collaborative decision-making and improving health literacy, self-management, and the health professional communication techniques to individuals at risk, can reduce health care expenditure and the utilization of resources.23,31,34,35 In Australia, as part of the healthcare system, medicare benefits are available for patients with established chronic health problems and monitored by their general practitioner (GP), but these benefits do not cover prevention or coaching programs.31,36,37 In response to the limited Australian research evaluating health coaching as well as the global debate about its cost-effectiveness,31 the private health insurer Bupa initiated the Costs to Australian Private Insurance – Coaching Health (CAPICHe) trial. The trial researched the effect of telephone health coaching in clients with chronic health problems: chronic obstructive pulmonary disease (COPD), diabetes, heart failure, low back pain or coronary artery disease (CAD), in comparison to usual care. These conditions are estimated to burden the provider most significantly with high-cost claims.37 The outcomes of CAPICHe showed that after 12 months of follow-up, although there were no significant differences in total costs between the health coaching and control groups, the hospital admission costs in the health coaching group were lower in comparison to the control group.37 The results of the trial provide an important step towards the promotion of health coaching in Australia; they also assess the generalisability of former health coaching trials from the United States to other nations. However, the ambiguity of the health coach and the rationale for the health coaching modality indicate the need for further health coaching research.
The various health coaching modalities have successfully been used independently,23,25,34,35,38 and in combination18,24,29,39,40 to improve patient health outcomes. In order to promote the implementation and remuneration of health coaching services it is important to determine the most pragmatic modality; requiring minimal pharmacist training and time, but yet yielding the greatest improvement in the health outcomes for various patient groups.
Materials and Methods
Search Strategy
This systematic literature review followed the PRISMA guidelines.41 The databases CINHAL, EMBASE, PubMed, PsychINFO and SCOPUS were systematically explored to identify the literature, which related to the method of health coaching used by pharmacists. The search of the databases involved three stages (Table 1). The initial stage of the search focused on health coaching and pharmacy, while the second stage focused on the pharmacist and pharmacy health coaching. The third stage was directed towards the modalities of health coaching and included the search terms; telephone, text message, video, short message service (SMS), face-to-face. The outcomes of the search stages were collectively evaluated.
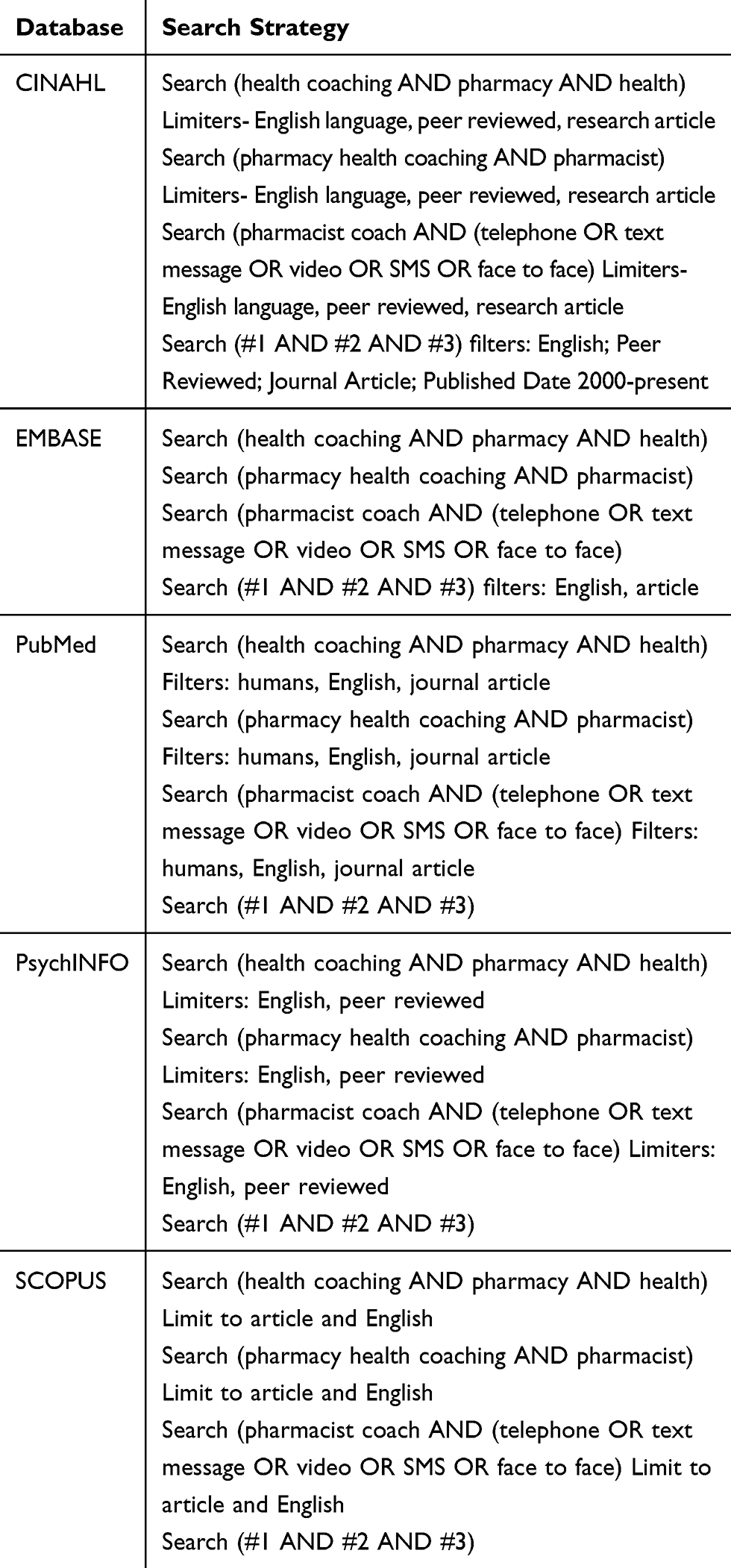 |
Table 1 Search Strings for Three Stage Search |
Searches were limited to the publication period 2000 to present; this decision was based on the finding that the concept of pharmacist health coaching was not reported prior to this.
Inclusion/Exclusion Criteria
Papers were initially included if they were peer-reviewed and were published between 2000 to the present, and contained the word “coaching” within the abstract, as this distinguished it as one of the main topics of the paper. The paper was also included if it referred to health coaching as per the concepts expressed in the grounded definition,16 such as patient-centered, facilitate, motivation, goal-setting and behavior change and, if they included text that referred to the modality of health coaching used by the pharmacist to coach patients. Papers were excluded if they: (1) were not published in the English language; (2) defined health coaching outside the context of pharmacy; (3) did not contain the term “coaching”; (4) were papers for which the full text could not be located; and (5) were grey literature. The inclusion and exclusion criteria used to identify abstracts and full papers is shown in Table 2.
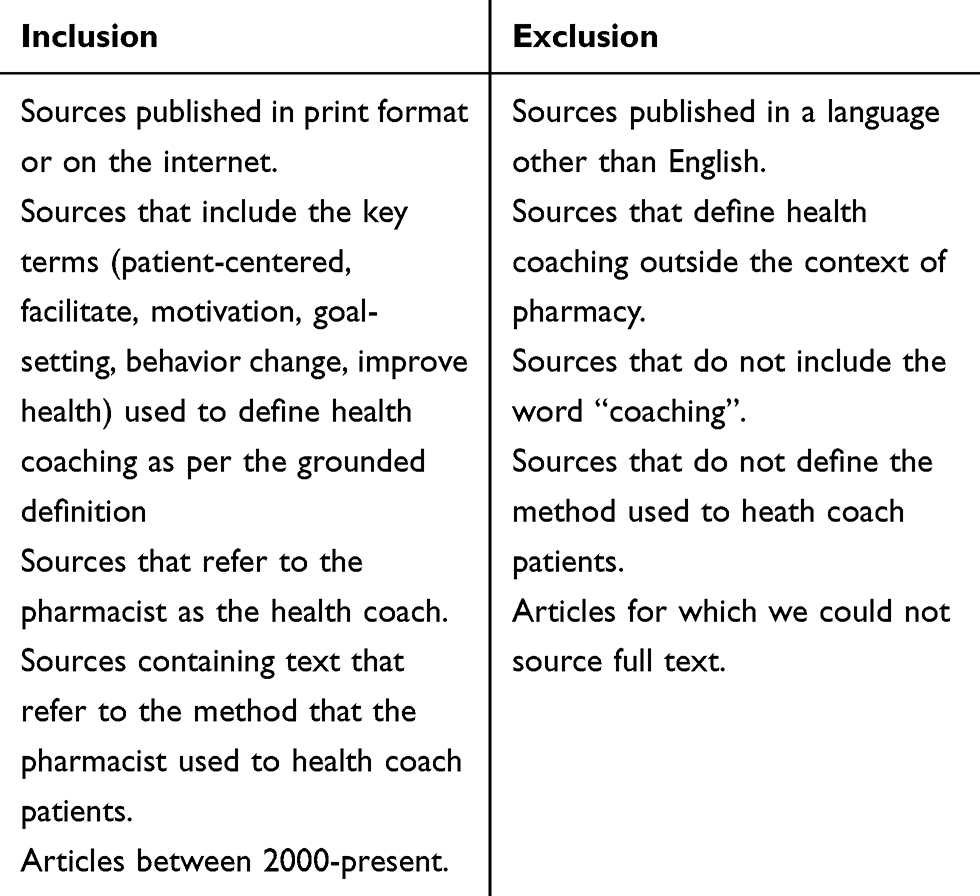 |
Table 2 Inclusion and Exclusion Criteria for Obtaining Sources for Abstract and Full Paper Review |
Quality of Studies
The Cochrane Handbook for Systematic Review of Interventions was considered when assessing the quality of the papers.42 Given the nature of the intervention being assessed, it was at times not feasible to blind participants and researchers, hence the reason for including non-randomized trials. The risk of bias of each paper included in this review was assessed as low. Furthermore, given the small number of studies in the field, the inclusion of all studies in our systematic review as valuable.
Data Analysis
A single researcher initially screened the title and abstract of all papers. The full-text copies of papers that passed the initial screening process were subsequently reviewed by two researchers independently. When a decision about a paper could not be reached the third researcher was consulted, consensus was then reached with reference to the inclusion/exclusion criteria.
The data extracted from the studies included: (1) the country of the study; (2) participant population; (3) the modality of health coaching used by the pharmacist; (4) number of contacts between the participant and the pharmacist health coach; (5); the duration of the health coaching sessions; (6) the details about the training given to the pharmacist in order to health coach and (7) outcomes and impact of the study. Subsequently, the data were tabulated which allowed inferences to be made.
Results
Study Selection
Figure 1 shows the study selection process. There were 391 studies that were identified of which 234 were duplicates. After removal of duplicates, the titles and abstracts of 157 papers were reviewed. Sixty-one met the inclusion criteria; the full-text was retrieved and reviewed. Forty-eight papers were excluded, as they were not relevant, did not mention the modalities of health coaching used by the pharmacist. A total of 12 papers met the eligibility criteria, were included in the final review, and are summarized below in Table 3.
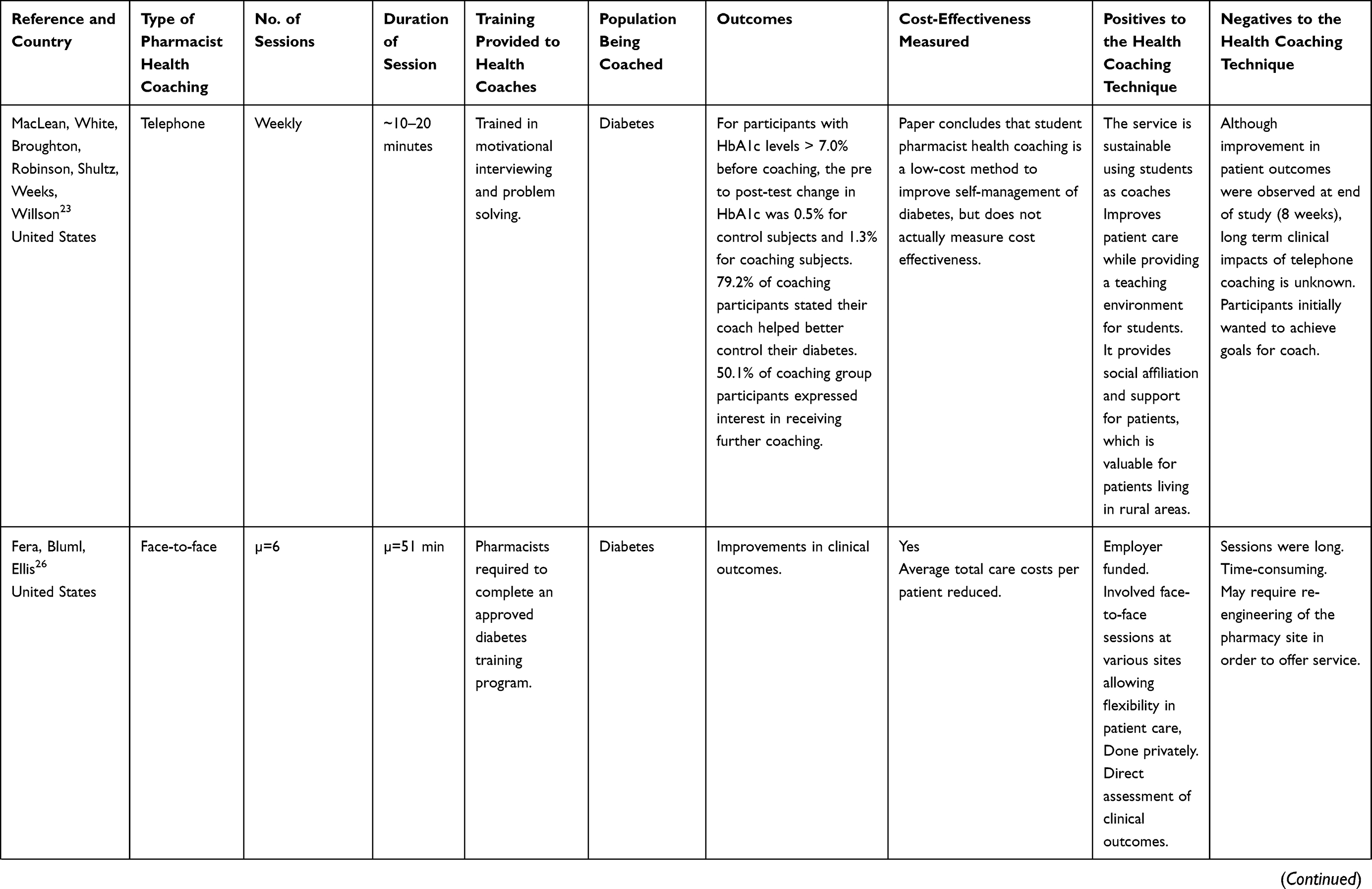 | 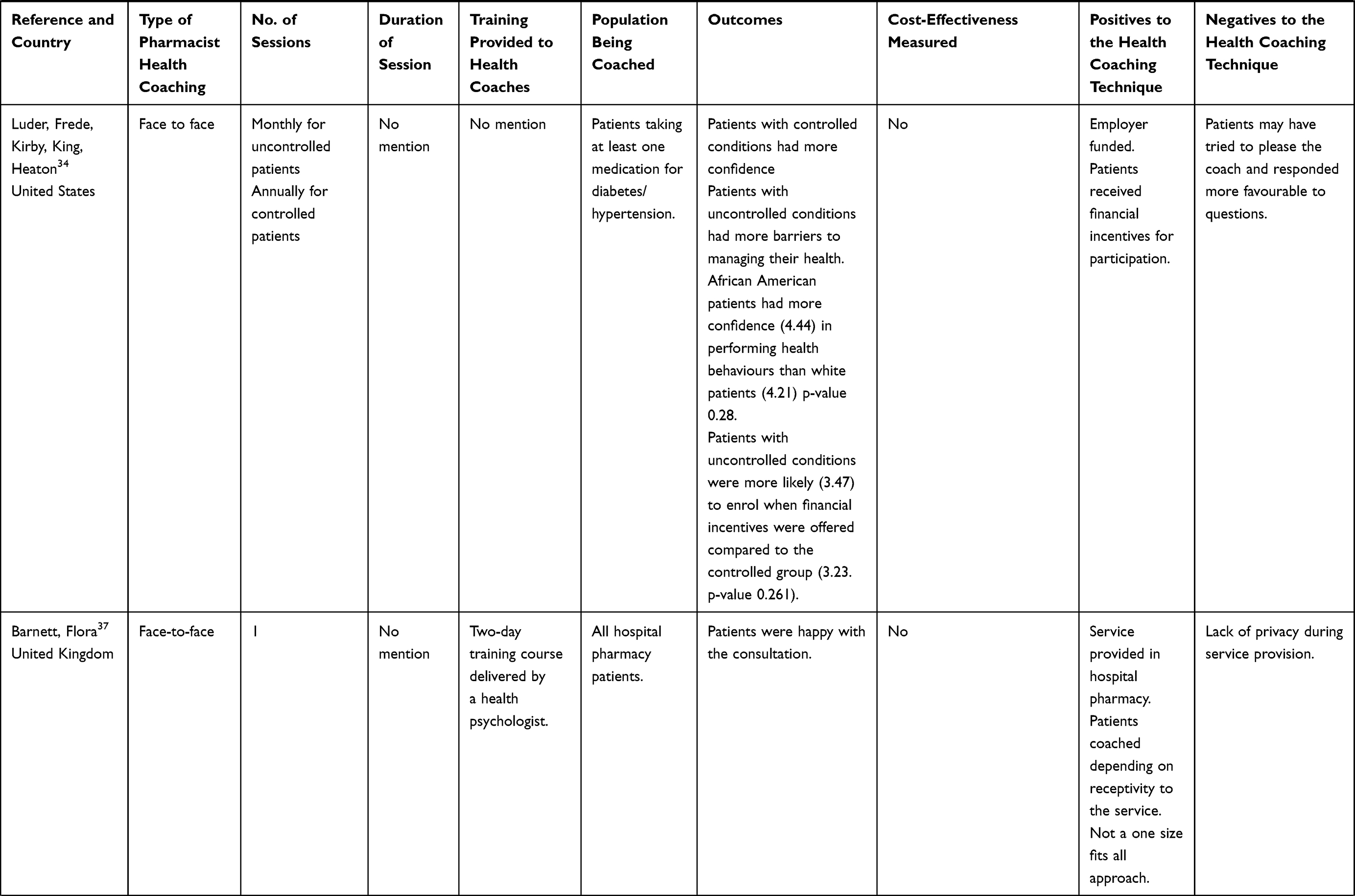 | 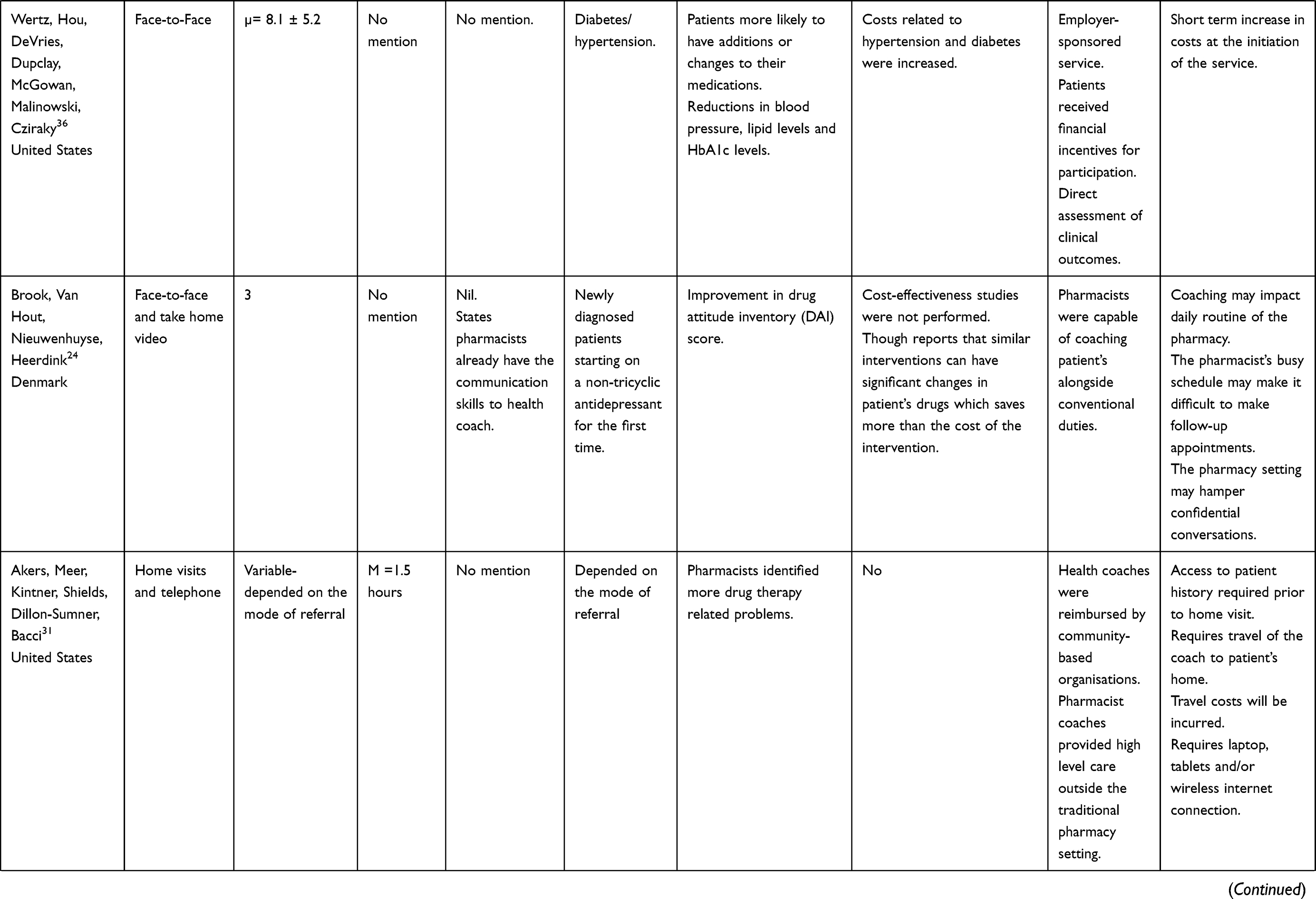 | 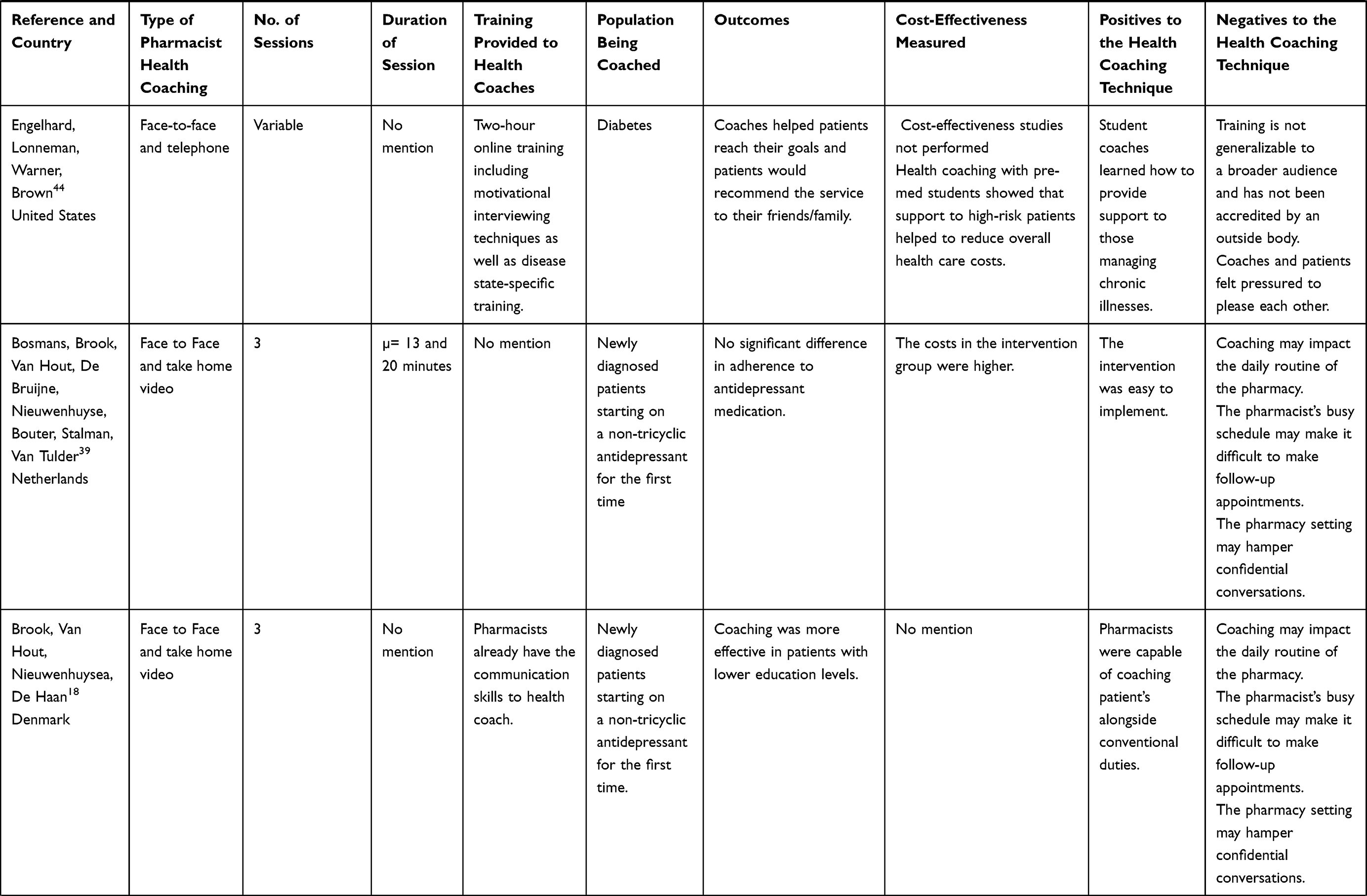 |
Table 3 Summary of Included Studies |
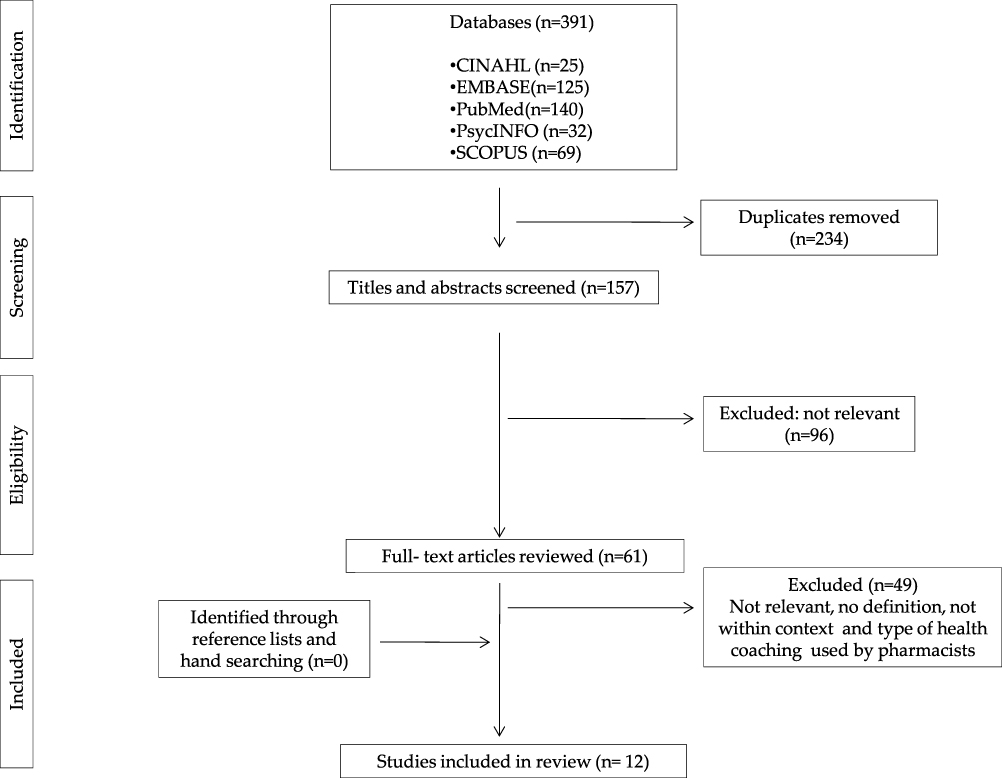 |
Figure 1 PRISMA flow chart of the literature search and study selection. |
Study Characteristics
Most of the studies included in this systematic review involved a combination of two or more health coaching modalities when health coaching patients.18,24,29,39,40 Four papers referred to face-to-face health coaching sessions with the pharmacist health coach23,34,35,38 and one study used only telephone coaching.25 Given the paucity of the included literature, synthesis between articles was not always possible; hence, the results are presented as a description of individual studies.
Telephone Health Coaching
Only one of the studies included in this review exclusively used weekly telephone coaching sessions as the modality of health coaching.25 The duration of this study was 8 weeks and coaches were in their second year of study for the doctor of pharmacy.25 Students received training in order to provide health coaching to participants who were previously part of an educational program for diabetes; on the road to living well with diabetes (OTR). Training also included specifics of diabetes self-management as well as a course about health communication, motivational interviewing and problem-solving.25 The student coaches followed a semi-structured guide, to coach participants, and the effectiveness of the telephone coaching was determined from an OTR questionnaire, the results of which were compared to a previous program, not supplemented with health coaching. The results showed that for participants with glycated hemoglobin (HbA1c) levels greater than 7.0% before coaching, the pre- to post change in HbA1c was 0.5% for subjects in the control group and 1.3% for participants who were coached. Approximately half (50.1%) of the participants who had been coached expressed interest in having additional health coaching to help manage their diabetes.25 The researchers reported that this modality to health coaching is a low-cost method, though did not specifically investigate the cost-effectiveness.
Face-to-Face Health Coaching
Four papers referred to the face-to-face health coaching sessions that occurred at a pharmacy.23,34,35,38 Only one paper included in this review referred to health coaching undertaken by hospital pharmacists.38 The hospital pharmacists received a two-day health coach training course, delivered by a health psychologist. Patients were allocated to groups; only patients receptive to information about the safe use of medicines, with immediate concerns and questions were provided with health coaching, supported by the 4Es model (explore, educate, empower enable). The outcomes of the study showed that patients reported being happy overall with the service. Pharmacists expressed greater satisfaction with their consultations as they were patient-centered and focused on patient needs. Pharmacists also felt well utilized, not wasting time with patients unlikely to be receptive.
The remainder of the face-to-face health coaching studies were employer-initiated programs.23,34,35 Two of these studies investigated the outcomes of participants with diabetes or hypertension.23,34 In both studies, the pharmacist was trained to provide health coaching, although the specifics of training were not discussed. During the health coaching sessions, the pharmacist promoted lifestyle modification, education, medication adherence, monitoring of clinical outcomes as well as goal setting in order to improve health outcomes. However, each study had different endpoints.23,34 One study evaluated patient health behaviors and beliefs that forecast interest in disease management services within pharmacy,34 while the two others explored the clinical and financial consequences of a pharmacist health coaching program.23
Depending on their current diabetes or hypertension status, participants in the health beliefs study were assigned to groups.34 Each group received health coaching by the pharmacist; monthly for patients regarded as having uncontrolled diabetes or hypertension and annually for patients regarded as having controlled diabetes or hypertension. The results showed that participants with controlled conditions had greater confidence in managing their health, while those with uncontrolled conditions experienced more barriers to managing their health. It was also reported that the mean expenditure per patient was reduced at the completion of the study.
In the study investigating the clinical and financial consequences of a pharmacist health coaching program, participants selected to receive coaching or the control condition.23 The control group participants did not receive coaching by the community pharmacist, while those within the intervention groups met with the pharmacist health coach regularly and had an average number of six visits with the pharmacist health coach. The results indicated that patients who were coached were more likely to have additions or changes made to their medications during the study period, indicating that they were more likely to be actively managed by their GPs. Participants with hypertension that received health coaching experienced a reduction in blood pressure from 136.1/83.5 mmHg at enrollment to 129.5/79.3 mmHg (p < 0.05) at end of study. Similarly, a reduction in low-density lipoprotein (LDL) was observed in enrolled patients with hypertension and diabetes; 104.1 to 97.2 mg/dL and 91.6 to 84.0 mg/DL, respectively. The HbA1c levels of participants with diabetes also improved from baseline (7.9%) to follow-up. (7.1%, p < 0.05).23 Despite the improvements to clinical parameters costs related to diabetes and hypertension increased during the study.
The fourth face-to-face study involved pharmacist health coaching in patients with diabetes.35 In this study, the pharmacist health coach received diabetes education training or was certified in diabetes care. The role of the pharmacist health coach focused on clinical assessment of the patient progress towards a clinical target and working with the patient to set personal health goals. The pharmacist health coaches met with their patients regularly; with an average of six patient-pharmacist visits over 14 months. The outcomes of the study showed statistically significant improvements for key clinical measures after a year; the mean glycosylated hemoglobin improved from 7.5% to 7.1% (p = 0.002). There was also an overall decrease in medical costs, which compensated for the new spending on professional pharmacist services.35
Combination of Health Coaching Modalities
Seven studies used a combination of health coaching modalities to coach patients.18,24,29,39-43 In four of the studies, newly diagnosed patients commenced on a non-tricyclic antidepressant for the first time and received a take-home video in addition to three face-to-face health coaching sessions with the pharmacist in the store.18,44 Reports on the training and education provided to the pharmacist health coach were different.39,43,45 Two studies did not mention the training provided.29,44 While another two mentioned that pharmacists had formerly acquired the communication skills needed to health coach18,24 Each study had a different endpoint in terms of; cost-effectiveness,44 psychological symptoms,18 drug attitude24 and adherence.40
The study that specifically examined cost-effectiveness reported that the costs incurred within the health coaching group of patients were higher in comparison to the control, though the difference was not statistically significant.44 In another study, medical costs were lower in the patients that received health coaching. This was attributed to fewer hospital admissions.39 Without having performed a cost analysis, one study reported that health coaching could reduce overall costs by supporting high-risk patients.45
For the study investigating drug attitude, improvements in drug attitude inventory scores (DAI-30) were apparent at 3 months,24 this correlated with an improvement in psychological symptoms. Two-thirds of patients were in remission at 6 months approximately, and were satisfied with the service; 86% of the health coaching patients reported they would recommend the service others.18 However, in the study investigating adherence to antidepressants the analysis showed that health coaching had no intervention effects on adherence.40
Of the seven studies that used a combination of modalities to health coach, two used pharmacy students as the health coach. Each of these studies investigated the outcomes of health coaching on different patient populations; diabetes45 and hypertension.43 Students in both studies received health coach training, which included techniques of motivational interviewing, though the degree of training varied from 2 hours of online training45 to 6 hours of face-to-face content.43
In the study investigating the outcomes of health coaching on patients with diabetes, the student health coaches initially met with the participants face-to-face and supplemented this with weekly phone calls, over a three-month period. During sessions, coaches helped patients set Specific, Measurable, Achievable, Realistic, and Timely (SMART) goals. At the completion of the study, nine out of the 12 participants reported that they successfully reached their personal goal. Participants also indicated that they would recommend the service to their friends/family.45
As part of the protocol for the second study engaging students as the health coaches, participants initially received weekly email, texts, and phone calls.43 However, due to significant participant drop out and lack of follow-up, the method of health coaching was modified to face-to-face contact. Coaches subsequently met with participants collectively during weekly face-to-face group sessions. During sessions, coaches encouraged participants to make healthier choices and made recommendations to support the achievement of their goals. The outcomes of the study showed that students were confident in their ability to perform coaching (85%), though did not feel comfortable about educating patients about hypertension (86%). The students in this study received health coach training which included the techniques of motivational interviewing as well as disease state-specific training.
In another study, face-to-face in-home health coaching by a community pharmacist was supported with telephone calls.29 No specific training was provided to the pharmacists in order to engage in health coaching. During sessions, pharmacist’s identified drug therapy-related problems and provided medication education. The pharmacists spent an average of 1.5 hours with the patients in their homes and had a 1-hour follow-up visit. Pharmacists discovered a mean of 11 drug therapy-related issues per patient.
Lastly, one study supplemented telephone coaching with web links, video and print materials, including DVDs on collaborative decision-making.39 The study did not allude to the training given to pharmacists to coach. During the study, pharmacist coaches instructed participants about shared decision-making and motivated them to make behavioral changes. Patients included in this study had varying health conditions and were referred through their insurer health support service. Participants with chronic health conditions and/or high-risk health conditions received the most health coaching sessions. The study showed that mean costs to medical and pharmacy per patient that received health coaching were 3.6% (p = 0.05) lower than those that did not receive health coaching. This was attributed to the reduction in annual hospital admissions.
Discussion
The relative paucity of the data on the process of health coaching by pharmacists should be noted. Indeed, there are studies that report health coaching interventions undertaken by pharmacists, though the specifics regarding training and facilitation of the service are often underreported, further, clinical outcomes were reported in only 8 of 12 studies.18,23-25,29,34,35,39 Without this, difficulties arise when comparing study outcomes as a result of the inconsistencies between them. Thus, the results of this review reveal that the conclusions about the most pragmatic modality of health coaching are not possible.
Variations were apparent in the number of health coaching sessions that pharmacists had with patients; ranging from 138 to 8.2 ± 5.2.23 However, regardless of the number of health coaching sessions patients had with the pharmacist coach, they experienced an overall improvement in health outcomes23,24,29,34,35 and, or experiences.34,38,45
Most pharmacist health coaching studies utilized a combination of modalities to coach patients,18,24,29,39-43 including face-to-face contact with the pharmacist,18,44 supplemented with telephone coaching,43,45 videos,18,24,44 email,43 print materials,39 texts43 web links,39 and DVDs.39 Similar, to the number of health coaching sessions, favorable outcomes were reported in each study regardless of the health coaching modality, or a combination thereof, used.
Consequently, there does not appear to be an ideal number of health coaching sessions, or a superior modality of pharmacist health coaching. In each instance, the pharmacist health coaching intervention provided patients with the support and guidance to achieve their health goals.18,23-25,29,34,35,38-43 This review did not explicitly focus on the cost-effectiveness of the pharmacist health coaching modalities. Considering limited studies reported on cost-effectiveness, it is not possible to draw any definitive conclusions. However, despite the variability in clinical outcomes, the economic value of professional pharmacy services is well established as they reduce resource utilization and costs.46 For this reason, it is reasonable to suggest that health coaching would perform similarly. Comparable to professional pharmacy services such as vaccination, costs will be incurred at initiation and delivery of pharmacist health coaching, which would be recuperated with prolonged service delivery, reducing costs to healthcare infrastructures.46 Additional research is needed to investigate the long-term benefits and financial implications of pharmacist health coaching modalities.47
Given the difficulty associated with following up patients, it would be more pragmatic and efficient to implement health coaching modalities not requiring face-to-face contact with the pharmacist.39,48
Moreover, electronic modalities of health coaching are more likely to ensure continuity as they are of greater convenience to patients. The health coaching modality, may, however, pose challenges in building rapport, between the patient and the pharmacist health coach, without which patient accountability and engagement in such services is otherwise poor.49 However, by identifying factors that affect patient health management, pharmacists can facilitate appropriate health care and education delivery.50 One study was confronted with a similar setback, whereby the health coaching modality within the study protocol was changed from telephone coaching to face-to-face meetings with the pharmacist health coach. This enhanced patient follow-up during the study as well as the engagement of the pharmacist health coach.43
Contrary to this, a study which exclusively utilized the modality of telephone health coaching showed that patients experienced improved health outcomes; a decrease in HbA1c levels.25 Further, there was no mention of patients being lost to follow-up or difficulties in doing so. This is a reasonable outcome, as telephone coaching has shown to be convenient for patients with the absence of travel and associated costs.51 Therefore, considering only one study reported on the challenges of electronic modalities of pharmacist health coaching further research in the area is warranted.
Similar to this review, other studies have investigated the various modalities to consultations. These studies have shown that the use of video techniques produces similar outcomes in terms of nature and composition of the sessions, though like telephone sessions would not be appropriate for health problems requiring physical consultations.52 The main issue that video techniques bear is the initial infrastructure costs and intermittent technical issues, which is not an issue for telephone consultations or health coaching sessions.53 However, video consultations are being increasingly adopted as they compensate for barriers pertaining to patient access to healthcare such as geography, environmental issues, and physical incapabilities.27,54 It also overcomes the barriers associated with professional isolation health practitioners in rural localities experience.27 Though, when given the option, telephone interventions were more popular in individuals over the age of 50.52 Given that chronic health conditions affect older populations, it is reasonable to suggest that telephone health coaching would be the most suitable modality in this group. Despite the benefits with telehealth care, some studies have shown poor43 or declined usage over time;55,56 for patients with comorbidities and complications, interpersonal contact may be more appropriate.57 Notably, a recent US-based health coaching study showed that face-to-face coaching was effective in improving health outcomes in patients complex health conditions.48
Despite the inability to draw conclusions about the most efficacious and economically valuable modality to health coaching, arguably it is most important to acknowledge the patient’s choice as health-coaching is a patient-centered service16 Furthermore, demand for additional choice broadens to health care delivery. Evidence shows that patients have varying needs and expectations of pharmaceutical services. Therefore, even while one health coaching modality could be better than another, the choice of delivery should be left to the patient.27 Hence, there is a need for patient satisfaction to be investigated more rigorously, along with other dimensions of patient experience.58 With regards to health coach training provided to the pharmacists, reports were inconsistent. Not all qualified pharmacists that took part in the health coaching studies received training.18,24,29,39,44 The specifics for those that did receive training were unclear.23,34,35,38 However, irrespective of the health coaching modality used by the student pharmacists to health coach, all received training. Training featured the concept and process of motivational interviewing.25,43,45 Including this as part of a health coach training program is valuable, considering it is a communication technique which can facilitate the behavior change process during health coaching.59
Therefore, from the data, it was not possible to determine the level of training required for each health coaching modality, as details were underreported.
The modalities of pharmacist health coaching included in this review varied as did the endpoints of the studies. In spite of this, each study reported an overall improvement in the clinical outcomes of patients with diabetes,23,35,45 hypertension,23 high cholesterol,23 and depression.18 Pharmacist health coaching also encouraged improvements in non-clinical outcomes including medication adherence,34 attitude towards drug therapy,24 medical costs35,39 and patient satisfaction towards the service.18,38,45 This proposes that pharmacists can successfully health coach patients with a range of health conditions and can facilitate an improvement in a number of clinical and non-clinical measures. However, considering the disparities amongst study protocols it was not possible to determine the most pragmatic modality of health coaching, suggesting that further research is warranted in this area.
Limitations
A systematic modality was used to conduct this literature review. A small range of search strings and terminology were agreed upon by the research team. This made identifying articles within the databases and specific to health coaching manageable. Since this may be considered a limitation, where important information may have been overlooked; the full search string has been included which allows for replication. The use of the key terms to guide the selection of papers for the review may be considered as a limitation to the selection of eligible articles. However, these key terms were used to define health coaching as per the grounded definition published within the literature. The search strategy for the review spanned a 20-year period, during this time considerable changes to health care systems of the countries included would have occurred which could have influenced the articles that were selected. In order to further minimize bias two independent reviewers carried out the final review and selection of papers. The small sample size used for this review may also be considered a limitation; however, in light of the predetermined, thorough and transparent search strategy used, the sample size is justified. Lastly, considering there is no standard process for the analysis and reporting qualitative data in a systematic review,60 the inclusion of a non-randomized study in this review is justified.23 Although participant self-selection biases could have influenced the outcomes of this study, it is important to acknowledge that as a professional pharmacy service, health coaching is to be provided to patients if they choose to receive it. For this reason, the outcomes of this type of study would be a realistic representation of pharmacist health coaching service delivery.
Conclusions
In this review, we take a pragmatic modality as to the modalities used for pharmacist health coaching interventions. We hope that in recognizing the variability in reporting amongst the included studies future pharmacist health coaching studies have more rigorous study designs. Studies, which document the training, the modality, the outcomes and the cost benefits of coaching by pharmacists, are warranted to enable a more comprehensive evaluation and quality decision-making around health coaching modalities undertaken by pharmacists. Fundamentally, pharmacists must recognize the patient’s preference in the modality used as health coaching is a patient-centered service. Since the details of the health coach training provided to pharmacists were not always clear, it was not feasible to determine the health coaching modality for which there were minimal training requirements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Wolever RQ, Simmons LA, Sforzo GA, et al. A systematic review of the literature on health and wellness coaching: defining a key behavioral intervention in healthcare. Glob Adv Health Med. 2013;2(4):38–57. doi:10.7453/gahmj.2013.042
2. Dowrick C, Dixon-Woods M, Holman H, Weinman J. What is Chronic Illness? Sage UK: London, England: Sage Publications; 2005.
3. Dalton K, Byrne S. Role of the pharmacist in reducing healthcare costs: current insights. Integr Pharm Res Pract. 2017;6:37. doi:10.2147/IPRP.S108047
4. Negaard BJ, Lyons KP, Nichol CL, Polgreen LA. What does a pharmacist do? A time and motion study. Res Social Adm Pharm. 2019. doi:10.1016/j.sapharm.2019.03.007
5. George P, Molina J, Cheah J, Chan S, Lim B. The evolving role of the community pharmacist in chronic disease management - A literature review. Ann Acad Med Singapore. 2010;39:861–867.
6. Gregório J, Cavaco AM, Lapão LV. How to best manage time interaction with patients? Community pharmacist workload and service provision analysis. Res Social Adm Pharm. 2017;13(1):133–147. doi:10.1016/j.sapharm.2016.02.008
7. Spencer JA, Edwards C. Pharmacy beyond the dispensary: general practitioners’ views. BMJ. 1992;304(6843):1670–1672. doi:10.1136/bmj.304.6843.1670
8. Roberts AS, Benrimoj SI, Chen TF, Williams KA, Hopp TR, Aslani P. Understanding practice change in community pharmacy: a qualitative study in Australia. Res Social Adm Pharm. 2005;1(4):546–564. doi:10.1016/j.sapharm.2005.09.003
9. Feletto E, Wilson LK, Roberts AS, Benrimoj SI. Flexibility in community pharmacy: a qualitative study of business models and cognitive services. Pharm World Sci. 2010;32(2):130–138. doi:10.1007/s11096-009-9355-3
10. Garcia-Cardenas V, Benrimoj SI, Ocampo CC, Goyenechea E, Martinez–Martinez F, Gastelurrutia MA. Evaluation of the implementation process and outcomes of a professional pharmacy service in a community pharmacy setting. A case report. Res Social Adm Pharm. 2017;13(3):614–627. doi:10.1016/j.sapharm.2016.05.048
11. Schumock GT, Butler MG, Meek PD, et al. Evidence of the economic benefit of clinical pharmacy services: 1996–2000. Pharmacotherapy. 2003;23(1):113–132. doi:10.1592/phco.23.1.113.31910
12. Palmer S, Tubbs I, Whybrow A. Health coaching to facilitate the promotion of healthy behaviour and achievement of health-related goals. Int J Health Promot Educ. 2003;41(3):91–93. doi:10.1080/14635240.2003.10806231
13. Olsen JM, Nesbitt BJ. Health coaching to improve healthy lifestyle behaviors: an integrative review. Am J Health Promot. 2010;25(1):e1–e12. doi:10.4278/ajhp.090313-LIT-101
14. Herborg H, Haugølle LS, Sørensen L, Rossing C, Dam P. Developing a generic, individualised adherence programme for chronic medication users. Pharm Pract (Granada). 2008;6(7):148–157. doi:10.4321/S1886-36552008000300006
15. DiDonato KL, May JR, Lindsey CC. Impact of wellness coaching and monitoring services provided in a community pharmacy. J Am Pharm Assoc. 2013;53(1):14–21. doi:10.1331/JAPhA.2013.11227
16. Singh HK, Kennedy GA, Stupans I. A systematic review of pharmacy health coaching and an evaluation of patient outcomes. Res Social Adm Pharm. 2019;15(3):244–251. doi:10.1016/j.sapharm.2018.04.012
17. Lonie JM, Austin Z, Nguyen R, Gill I, Tsingos-Lucas C. Pharmacist-based health coaching: a new model of pharmacist-patient care. Res Social Adm Pharm. 2017;13(3):644–652. doi:10.1016/j.sapharm.2016.06.015
18. Brook OH, Van Hout HPJ, Nieuwenhuysea H, De Haan M. Effects of coaching by community pharmacists on psychological symptoms of antidepressant users: A randomised controlled trial. Eur Neuropsychopharmacol. 2003;13(5):347–354. doi:10.1016/S0924-977X(03)00031-2
19. Bauer UE, Briss PA, Goodman RA, Bowman BA. Prevention of chronic disease in the 21st century: elimination of the leading preventable causes of premature death and disability in the USA. Lancet. 2014;384(9937):45–52. doi:10.1016/S0140-6736(14)60648-6
20. McNeilly RB. Coaching for solutions: a new world of opportunity. Psychotherapy Aust. 2003;9(4):70.
21. Griffiths K, Campbell MA. Semantics or substance? Preliminary evidence in the debate between life coaching and counselling. Coaching. 2008;1(2):164–175.
22. Vale MJ, Jelinek MV, Best JD. Impact of coaching patients on coronary risk factors: lessons from The COACH Program. Dis Manage Health Out. 2005;13(4):225–244. doi:10.2165/00115677-200513040-00002
23. Wertz D, Hou L, DeVries A, et al. Clinical and economic outcomes of the cincinnati pharmacy coaching program for diabetes and hypertension. Manag Care. 2012;21(3):44–54.
24. Brook O, Van Hout H, Nieuwenhuyse H, Heerdink E. Impact of coaching by community pharmacists on drug attitude of depressive primary care patients and acceptability to patients; a randomized controlled trial. Eur Neuropsychopharmacol. 2003;13(1):1–9. doi:10.1016/S0924-977X(02)00074-3
25. MacLean LG, White JJR, Broughton S, et al. Telephone coaching to improve diabetes self-management for rural residents. Clin Diabetes. 2012;30(1):13–16. doi:10.2337/diaclin.30.1.13
26. Morgan M. Empowering diabetes patients with virtual self-help health coaching and apps. JMCN. 2014;12.
27. Phul S, Bessell T, Cantrill JA. Alternative delivery methods for pharmacy services. Int J Pharm Prac. 2004;12(2):53–63. doi:10.1211/0022357023709
28. !!! INVALID CITATION !!! 34.
29. Akers JL, Meer G, Kintner J, Shields A, Dillon-Sumner L, Bacci JL. Implementing a pharmacist-led in-home medication coaching service via community-based partnerships. J Am Pharm Assoc. 2019;59(2):243–251. doi:10.1016/j.japh.2018.11.008
30. Wolever RQ, Dreusicke MH. Integrative health coaching: a behavior skills approach that improves HbA1c and pharmacy claims-derived medication adherence. BMJ Open Diabetes Res Care. 2016;4(1):e000201. doi:10.1136/bmjdrc-2016-000201
31. Byrnes JM, Goldstein S, Venator B, et al. The impact of population-based disease management services for selected chronic conditions: the Costs to Australian Private Insurance-Coaching Health (CAPICHe) study protocol. BMC Public Health. 2012;12(1):114. doi:10.1186/1471-2458-12-114
32. Clarke JL. Preventive medicine: a ready solution for a health care system in crisis. Popul Health Manag. 2010;13(S2):
33. Ontario Pharmacists Association and Green Shield Canada. Impact of Community Pharmacist Interventions in Hypertension Management on Patient Outcomes: A Randomized Controlled Trial. Canada; 2014.
34. Luder H, Frede S, Kirby J, King K, Heaton P. Health beliefs describing patients enrolling in community pharmacy disease management programs. J Pharm Pract. 2016;29(4):374–381. doi:10.1177/0897190014566311
35. Fera T, Bluml BM, Ellis WM. Diabetes ten City challenge: final economic and clinical results. J Am Pharm Assoc. 2009;49(3):383–391. doi:10.1331/JAPhA.2009.09015
36. Biggs A. Chronic disease management: the role of private health insurance. Res Paper. 2013.
37. Scuffham PA, Byrnes JM, Pollicino C, Cross D, Goldstein S, Ng S-K. The impact of population-based disease management services on health care utilisation and costs: results of the CAPICHe trial. J Gen Intern Med. 2019;34(1):41–48. doi:10.1007/s11606-018-4682-5
38. Barnett NL, Flora K. Patient-centred consultations in a dispensary setting: a learning journey. Eur J Hosp Pharm. 2017;24(2):107–109. doi:10.1136/ejhpharm-2016-000929
39. Wennberg DE, Marr A, Lang L, O’Malley S, Bennett G. A randomized trial of a telephone care-management strategy. N Engl J Med. 2010;363(13):1245–1255. doi:10.1056/NEJMsa0902321
40. Brook OH, Van Hout H, Stalman W, et al. A pharmacy-based coaching program to improve adherence to antidepressant treatment among primary care patients. Psychiatr Serv. 2005;56(4):487–489. doi:10.1176/appi.ps.56.4.487
41. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
42. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Vol. 4. John Wiley & Sons; 2011.
43. Pounds K, Offurum A, Moultry AM. First year pharmacy students as health coach in the management of hypertension. Pharm Educ. 2015;15(1):111–115.
44. Bosmans JE, Brook OH, van Hout HP, et al. Cost effectiveness of a pharmacy-based coaching programme to improve adherence to antidepressants. Pharmacoeconomics. 2007;25(1):25–37. doi:10.2165/00019053-200725010-00004
45. Engelhard C, Lonneman W, Warner D, Brown B. The implementation and evaluation of health professions students as health coaches within a diabetes self-management education program. Curr Pharm Teach Learn. 2018;10(12):1600–1608. doi:10.1016/j.cptl.2018.08.018
46. Touchette DR, Doloresco F, Suda KJ, et al. Economic evaluations of clinical pharmacy services: 2006–2010. Pharmacotherapy. 2014;34(8):771–793. doi:10.1002/phar.1414
47. Wagner TH, Willard-Grace R, Chen E, Bodenheimer T, Thom DH. Currently reading costs for a health coaching intervention for chronic care management. Am J Manag Care. 2016;22(4):e141–6.
48. Watkins VA, Michaels NM, Jackson DL, Rhodes LA, Marciniak MW. The effect of community pharmacist–led health coaching on clinical outcomes. J Am Pharm Assoc. 2020;60(3):S65–S69. doi:10.1016/j.japh.2020.03.021
49. Bajorek BV, LeMay KS, Magin PJ, Roberts C, Krass I, Armour CL. Management of hypertension in an Australian community pharmacy setting–patients’ beliefs and perspectives. Int J Pharm Prac. 2017;25(4):263–273. doi:10.1111/ijpp.12301
50. Penn C, Watermeyer J, Evans M. Why don’t patients take their drugs? The role of communication, context and culture in patient adherence and the work of the pharmacist in HIV/AIDS. Patient Educ Couns. 2011;83(3):310–318. doi:10.1016/j.pec.2011.02.018
51. Collett K. A Case Study on the Effectiveness of Telephone Coaching. I-Coach Academy and Middlesex University Post Graduate Certificate in Coaching Practice; 2008.
52. Hammersley V, Donaghy E, Parker R, et al. Comparing the content and quality of video, telephone, and face-to-face consultations: a non-randomised, quasi-experimental, exploratory study in UK primary care. Br J Gen Pract. 2019;69(686):e595–e604. doi:10.3399/bjgp19X704573
53. Andersen KN, Medaglia R. Online health consultations: demand and channel management.
54. Calton B, Abedini N, Fratkin M. Telemedicine in the time of coronavirus. J Pain Symptom Manage. 2020;60(1):e12–e14. doi:10.1016/j.jpainsymman.2020.03.019
55. Friedman RH, Kazis LE, Jette A, et al. A telecommunications system for monitoring and counseling patients with hypertension: impact on medication adherence and blood pressure control. Am J Hypertens. 1996;9(4):285–292. doi:10.1016/0895-7061(95)00353-3
56. Canzanello VJ, Jensen PL, Schwartz LL, Worra JB, Klein LK Improved blood pressure control with a physician-nurse team and home blood pressure measurement.
57. Lu JF, Chi MJ, Chen CM. Advocacy of home telehealth care among consumers with chronic conditions. J Clin Nurs. 2014;23(5–6):811–819. doi:10.1111/jocn.12156
58. Raven M, Butler C, Bywood P. Video-based telehealth in Australian primary health care: current use and future potential. Aust J Prim Health. 2013;19(4):283–286. doi:10.1071/PY13032
59. Neuner-Jehle S, Schmid M, Grüninger U. The “Health Coaching” programme: a new patient-centred and visually supported approach for health behaviour change in primary care. BMC Fam Pract. 2013;14(1):100. doi:10.1186/1471-2296-14-100
60. Garside R. Should we appraise the quality of qualitative research reports for systematic reviews, and if so, how? Innovation. 2014;27(1):67–79.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.