")
Back to Journals » Patient Preference and Adherence » Volume 16
Do Patients Seek Women-Centered Cardiac Care? Patient Experience of an All-Female Multidisciplinary Heart Center for Women
Authors Finkelstein A, Leiter E , Reinfeld T, Levy O, Hoss S, Sloman L, Zwas DR
Received 22 February 2022
Accepted for publication 24 June 2022
Published 25 July 2022 Volume 2022:16 Pages 1749—1758
DOI https://doi.org/10.2147/PPA.S363325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Adi Finkelstein,1,* Elisheva Leiter,2,* Tanya Reinfeld,2 Ora Levy,2 Sara Hoss,2 Lori Sloman,2 Donna R Zwas2
1Department of Nursing, Faculty of Life and Health Sciences, Jerusalem College of Technology, Jerusalem, Israel; 2Linda Joy Pollin Cardiovascular Wellness Center for Women, Hadassah University Medical Center, Jerusalem, Israel
*These authors contributed equally to this work
Correspondence: Elisheva Leiter, Linda Joy Pollin Cardiovascular Wellness Center for Women, Cardiology Department, Hadassah University Medical Center Ein Karem, POB 12000, Jerusalem, 91120, Israel, Tel +1 972 54 332 9044, Email [email protected]
Purpose: Cardiovascular disease in women is frequently under-diagnosed and under-treated. Numerous heart centers for women have opened throughout the world to address these disparities; however, there is a paucity of data regarding participants’ perspectives. The current study assesses motivation to participate and perceived benefits in attending a heart center for women (HCW) in Jerusalem, Israel.
Methods: This study utilized qualitative methods to assess patients’ motivation and perceived benefits to attending a women’s heart center, particularly as they relate to gender medicine and single-sex staffing. A random sample of 42 clinic patients were asked to participate in interviews. Inclusionary criteria consisted of previous cardiovascular event, active cardiac symptom or three or more cardiovascular disease risk factors. Exclusionary criteria consisted of pregnancy, type 1 diabetes requiring insulin, psychiatric diagnosis that precluded participation, dementia, or other multidisciplinary clinic participation. Interviews were audio recorded and transcribed verbatim. Qualitative data analysis followed Braun and Clarke’s methodology of thematic analysis.
Results: The single-sex and gender medicine aspects did not motivate women to attend the HCW, although some participants perceived this as beneficial in retrospect. Women reported that the clinic visit enhanced their knowledge and awareness of issues related to heart disease in women as well as personal health benefits. They reported benefitting from the holistic approach, consideration of their lifestyle, the staff’s expression of concern, personalized attention, common language, and feeling understood.
Conclusion: This study describes the patient experience in an all-female HCW, highlighting their motivation for attendance and perceived benefits. While they did not actively seek women-centered care, women reported educational and care provision benefits to their attendance. The care attributes that women identified as beneficial typify the person-centered approach to care. These findings may inform both the design and evaluation of medical care facilities that aim to address the sex and gender disparities in cardiology as well as other medical specialties.
Keywords: gender medicine, patient experience, cardiovascular disease, person-centered care
Introduction
Cardiovascular disease is the leading cause of death in women throughout the world.1 Despite significant improvements over the past two decades, cardiovascular mortality is significantly higher in women than men after a heart attack and women are less likely to undergo cardiovascular screening tests, receive interventional treatment, or cardiac rehabilitation referrals.2–5 Risk factors specific to women have also been described, including gestational diabetes,6 polycystic ovary syndrome,7 and pre-eclampsia.8
In Israel, women have higher mortality rates than men from acute coronary syndrome (i.e heart attack and unstable angina), with 30-day mortality rates of 6.5% versus 3.6%.9
Critics of Israel’s medical system have indicated that it does not adequately address women’s gender-related health care needs, calling for national funding and policy changes that promote gender-sensitive medical care.10,11 Additionally, women in Israel are less likely to be counseled by their physician on issues such as nutrition, smoking, alcohol, or weight than women in the US, even when identified as high risk.12
Heart centers for women (HCW) were created to address these disparities, providing sex and gender-specific cardiovascular care.13,14 Despite the increasing prevalence of HCWs, there is little data assessing the patient’s perspective on this gender-specific method of health care delivery.15 Given that randomization is less feasible in health care delivery and complex clinical care settings, qualitative methods may provide the best approach to understanding and evaluating these questions. Investigating patients’ perspectives of a women-centered HCW can inform the design of other HCWs as well as medical centers targeting various women’s health issues. The current paper aims to identify patients’ preferences and perceived benefit to cardiovascular gender medicine and an all-female staff in a HCW through qualitative interviews.
Methods
Setting
Heart Center for Women
The Linda Joy Pollin Cardiovascular Wellness Center for Women is a heart center for women in Jerusalem, Israel, primarily focused on disease prevention. On first visit, patients were evaluated by a female nurse, nutritionist, physiotherapist, psychologist and cardiologist. Patient cases were reviewed in a multidisciplinary meeting, providing patients with a summary and recommendations. Follow-up appointments were scheduled according to clinical indications. Inclusion criteria consisted of experiencing a cardiovascular event (eg, myocardial infarction, percutaneous coronary intervention, or stroke), having an active cardiac symptom (eg, chest pain or arrhythmia) or three or more risk factors (eg, diabetes, hypertension, hyperlipidemia, peripheral artery disease, smoking, family history of coronary disease, gestational diabetes, pregnancy-induced hypertension/pre-eclampsia, or obesity). Exclusion criteria consisted of pregnancy, having type 1 diabetes with insulin adjustment, a psychiatric diagnosis that precluded participation, dementia, or receiving care from another multidisciplinary clinic.
Sample
At the time of data collection, 363 patients were seen at the clinic, aged 21–91, 93.5% of whom were self-referred. Qualitative data were collected in two waves: (1) Patients who attended the clinic between January 2016-December 2017 were called in a random sequence to obtain consent until saturation was reached in the qualitative interviews. Thirty-one women consented and 25 ultimately were interviewed. (2) In order to deepen insights on the gender-focus of the clinic, additional interviews were conducted with a modified interview guide. Patients who attended the clinic between May 2019-January 2020 were called in a random sequence to obtain consent until saturation was reached. Of the 20 who consented, 17 ultimately were interviewed.
Data Collection
This data were collected as part of a larger clinic evaluation; the current analysis focused on motivation to participate and perceived benefits of attendance exclusively. Data were collected over two waves. The first wave included 25 semi-structured interviews conducted by phone using an interview guide. Questions were based on previous research,16 addressing patient experience rather than satisfaction, to avoid positive bias.17 Wave 1 interviews did not ask directly about gender in order to obtain unprompted perceptions regarding this aspect of care. Questions in wave 1 and wave 2 were identical except for 3 items, which were added following the initial analysis of wave 1 data. These items relate directly to motivation for attending this HCW as well as gener-related aspects of care. See Supplement 1 for the full interview questions. The second wave included 17 interviews, bringing the total number of interviews to 42. Interviews were audio recorded and transcribed verbatim.
Data Analysis
Qualitative data were analyzed manually using the six phases of Braun and Clarke’s thematic analysis18 and following Nowell et al’s criteria19 to achieve trustworthiness. Our full analysis included three stages (See Table 1). Phase implementation for each stage are detailed as follows:
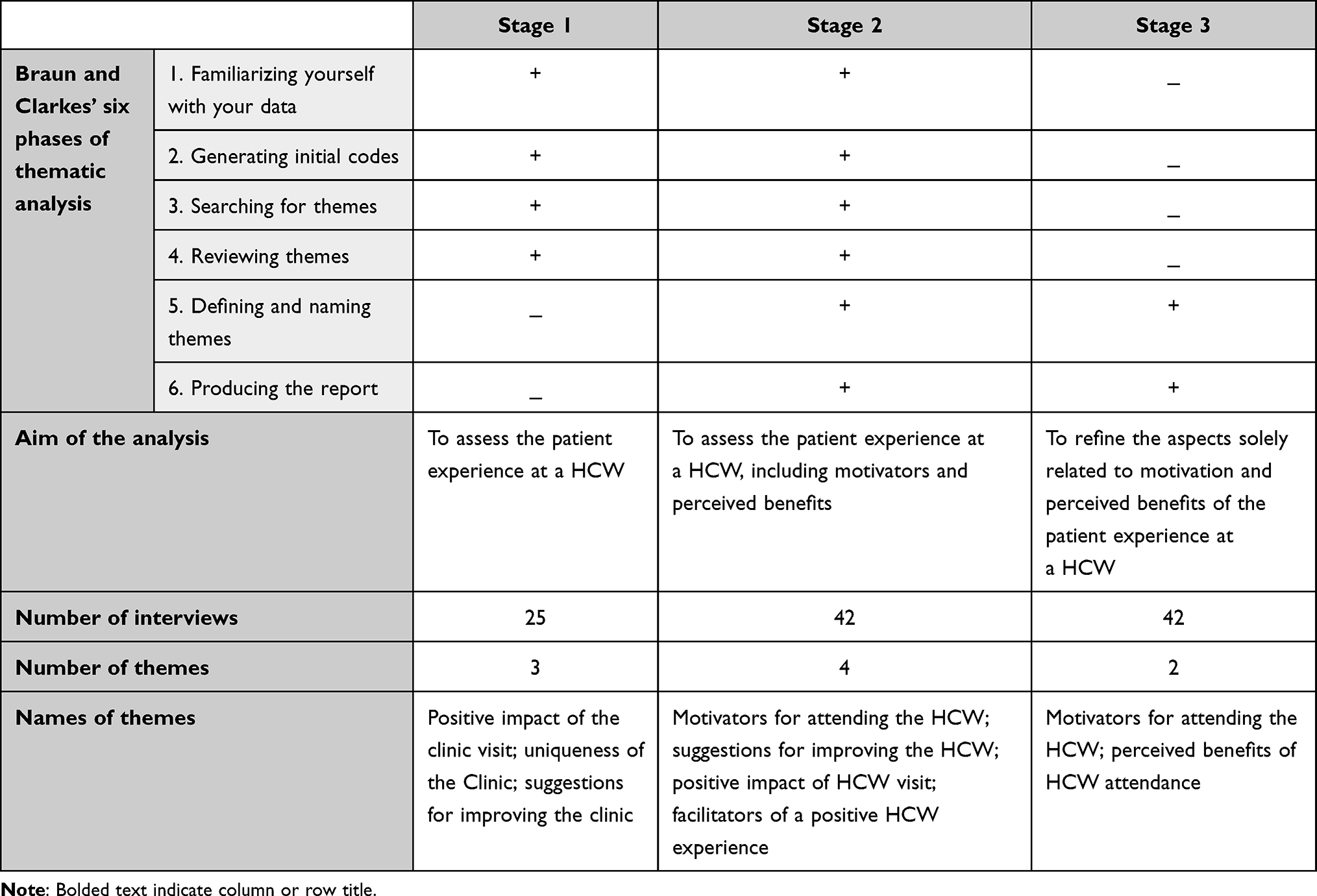 |
Table 1 Three Stages of the Full Analysis |
Stage 1
During the first stage, the initial 25 interviews (wave 1) were analyzed following the first 4 phases of Braun and Clarke. Phase 1 and 2 were done by AF and research assistants and was reviewed by TR, who worked separately, sharing insights until consensus of a code book was reached. First, transcribed interviews were read several times to get familiar with the data and to search for possible meanings and patterns. Ideas were marked for coding in subsequent phases. The second phase involved the production of initial codes from the data. Phase 3 was led by AF and completed with TR and EL. Different codes were sorted into potential patterns (themes) and all relevant coded data extracts were coded within the identified themes and sub-themes. Phase 4 was done by AF and reviewed by DZ.
Stage 2
The second stage included both the initial 25 interviews (wave 1) and the additional 17 interviews (wave 2). During this stage, all 42 interviews were analyzed as one data set following Braun and Clarkes’ phase 1–6. Phase 1 and 2 were done by AF and reviewed independently by EL, sharing insights until consensus of a code book was reached. Transcribed interviews were initially read several times to establish familiarity with the data and then to search for possible meanings and patterns. During the second phase, initial codes were produced. Phase 3 was completed by AF. Codes were sorted into potential patterns (themes) and all relevant coded data extracts were coded within the identified themes and sub-themes. Phase 4 was completed by AF and reviewed by DZ. Phases 5 and 6 were completed by AF and EL, with the final report reviewed by DZ.
Stage 3
During stage 3, we looked exclusively at the themes of motivation to participate and perceived benefits of attendance and detailed all of the relevant coding (phases 5–6). These phases were done by AF and EL. Phase 5 entailed defining themes and sub-themes by detecting the story that each theme tells and considering how it fits into the broader context of our data. In the final phase, examples that best captured the essence of each of the themes were chosen. The final report (phase 6) was reviewed by DZ.
Ethical Considerations
Human subject approval was obtained from the hospital IRB, the Helsinki Committee of Hadassah Medical Organization (Hadassah University Medical Center, Study # HMO- 0094-15). This study complies with the Declaration of Helsinki. All participants provided informed consent, which included publication of anonymized responses. For anonymity, patients were encoded A1-A25 (first phase) and B1–B17 (second phase). Given the sensitive nature of the data collected, requests to access the dataset from qualified researchers trained in human subject confidentiality protocols may be sent to DZ.
Results
Demographic descriptors of the participants are presented in Table 2. Final thematic map of the interviews and detailed map of the stage 3 analysis are presented in Figures 1 and 2, respectively. The themes identified in stage 3 included: (1) motivators for attending a heart center for women and (2) perceived benefit of a heart center for women.
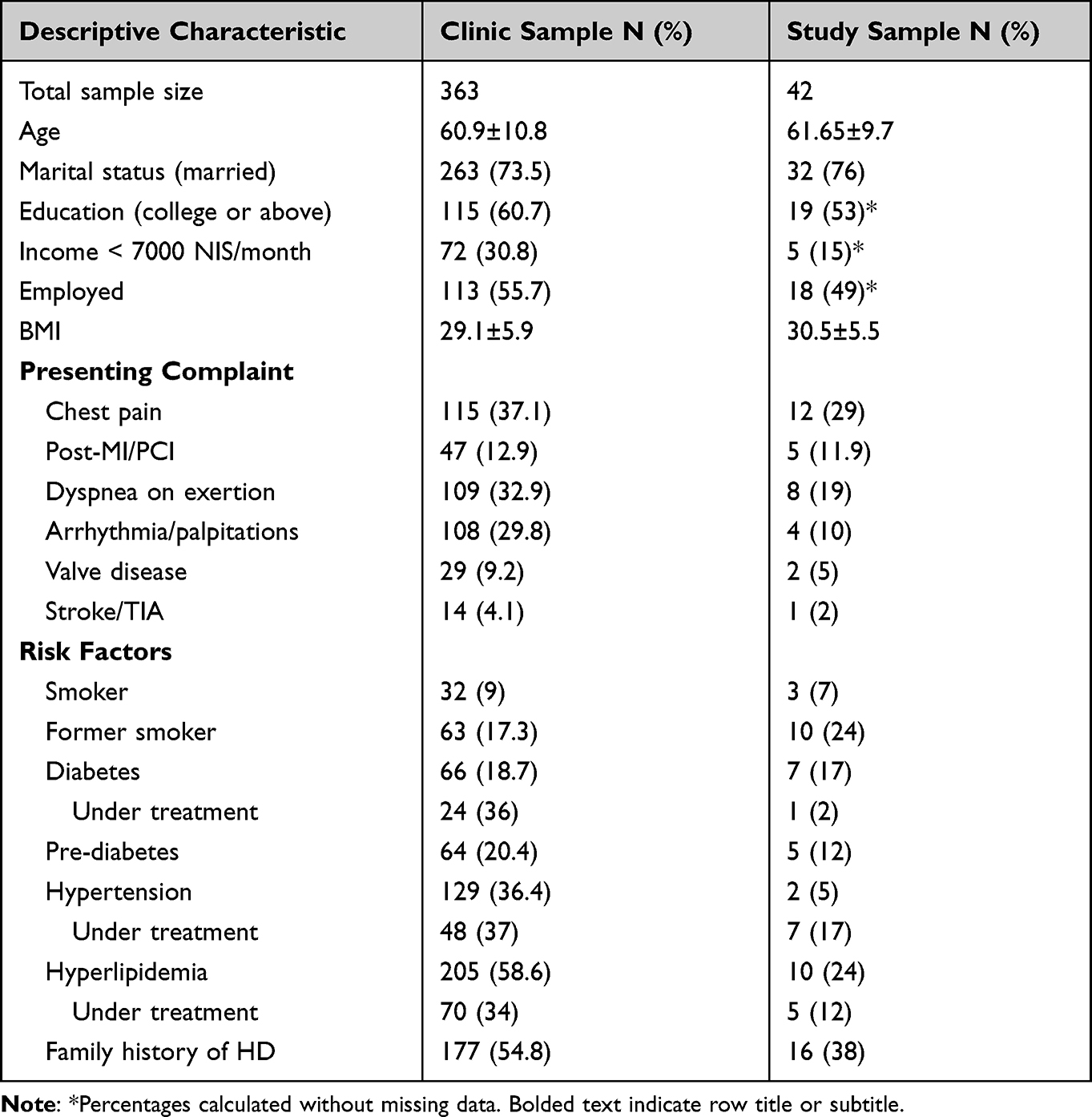 |
Table 2 Clinic and sample Demographics, Presenting Complaints, and Risk Factors |
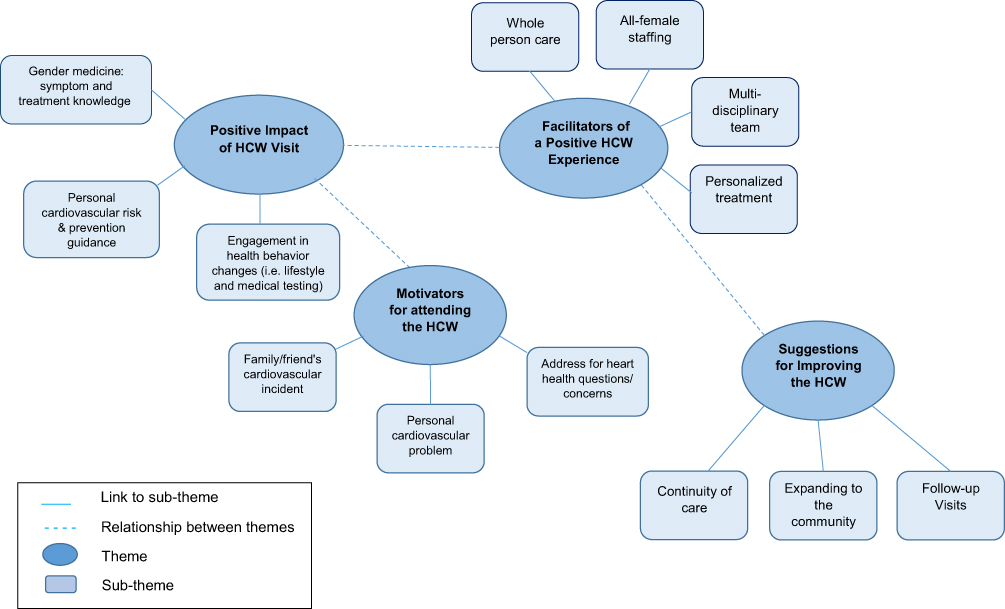 |
Figure 1 Final thematic map of interviews. |
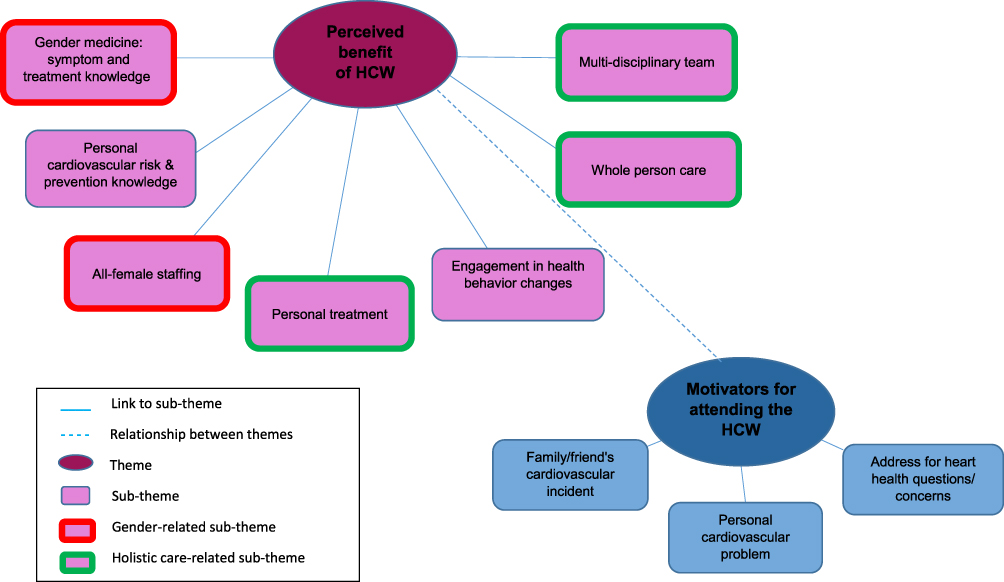 |
Figure 2 Visual representation of stage 3 analysis. |
Motivators for Attending a Heart Center for Women
Participants did not identify the women-centered aspects of the HCW as motivating factors for attending the clinic. This was consistent in wave 1 and even in wave 2, where participants were directly asked if the gender aspects influenced their decision to attend the clinic.
No, no I did not [come to the clinic because it is for women specifically]. Even though I think … you probably also need to check women … I don’t like the differentiation of men and women, gender … [B17]
I didn’t even think about it [the fact that it is a clinic specifically for women] at all. [B14]
It [The fact that the clinic is specifically for women] was completely not a factor [in my decision to come]. [B4]
A few participants stated that they did not even realize that it was a women’s heart clinic.
I did not notice if it was for men or women … [B1]
While the gender aspects of the HCW were not motivating factors to their attendance, participants did state that they came to the HCW out of fear for their own health or following a personal cardiovascular problem.
I got scared one night. I had very strong chest pains. I immediately thought of the heart, but the doctor told me it was reflux. I was not satisfied with that [answer]. I wanted to stop it right away. [B9]
I want to see if the risk of heart disease at the moment is really high for me. It’s very important to me. I need to see what else can help to prevent another attack. [A17]
Participants also reported making an appointment at the HCW after a family member or friend experienced a concerning cardiovascular event.
I have a good friend that had … a heart attack at a relatively young age. And she goes to this clinic. [B2]
Participants stated that they were looking for a place that would address their concerns related to heart health.
Really, I wanted to have an immediate address … here I found an address for the heart issues. [B4]
I came voluntarily … following a workshop that gave a lecture … it was important for me to check my heart. [A25]
Perceived Benefit of a Heart Center for Women
Participants stated that, as a gender medicine clinic, the HCW addressed the differences between men and women related to symptoms and treatment, which many first learned about during their visit.
I was told that a woman’s symptoms are not the same as a man’s … They told me the risks that exist. [A25]
… when I heard about it [that the clinic focuses on a woman’s heart], then I said: ‘why a woman’s heart, and not a heart in general?’ So they [the staff] told me that many times the symptoms of heart disease for women are a little different from men, and a lot of doctors have a tendency to think that if you do not have these symptoms of men, then you probably have no heart problem. [B12]
Participants indicated that the all-female aspect of the HCW was a valuable part of their experience at the HCW.
But it was nice when I came … It was nicer for me that they were all women, yes. [B4]
Yes, I think it’s an advantage that everyone is a woman … [B9]
Participants said that the all-female staff made them feel more comfortable; it created a pleasant atmosphere, they had a common language with the staff, and they felt cared for and understood.
Women understand women better- not just the disease but the experience. Going through menopause, she understands what it means, what it does to the body, to mood - to the entire woman. [B9])
Women, their heads work differently, its more comfortable, more pleasant … It’s easier for them to understand, easier to understand lifestyle, there is much more shared … no matter the age, religious or not religious, these things are easier to bridge the moment that there is a shared foundation [of being a woman]. [B3]
It was more pleasant; the whole approach is different with men. It’s a different world … the fact that everyone is a woman and professional and kind and they all truly make you feel like they care about you, giving personal attention … very different. [B6]
Some participants reported benefits that were not directly related to attending a women-centered clinic specifically, but that may not be addressed in a standard clinic. This included personalized treatment, holistic care, and multi-disciplinary treatment all under one roof, in one day.
The treatment is personal, you get the full attention, which does not happen in other clinics that … you are one of many and here you feel really … like the only child. [B14]
I felt that someone was really looking at all the parameters, and all the things, to understand my condition … [B2]
The approach there is holistic. They don’t just look at the symptom … they look at the person as a whole and not as a specific point problem. [B8]
I met with a series of experts, a nurse, a doctor, a nutritionist, with a physical therapist. It was [a] long [day], but it was worth it. [A18]
And every field was … another area of the whole topic … nutrition … exercise … even psychological. And then the doctor who took all the data and analyzed it along with me. [A5]
A few participants mentioned that their visit at the HCW had a positive impact on their knowledge, health, and health behaviors.
I felt it contributed to my awareness of heart health … and to pay attention to the signs of … [when] something is wrong …. They gave [me] guidance. [B10]
As for the physical activity … I was given all sorts of tips … They told me the risks that exist … Fats or physical inactivity … that can cause all kinds of problems in the future. It was important to me. [A25]
I did change my lifestyle with a lower carbohydrate diet, I do more sports … Let’s say I’m a happier woman … I feel it both in body and mind. [B4]
I don’t think it’s an exaggeration to say that you really saved my life because until I visited the clinic, I didn’t know that I had any problem with high blood pressure. [A2]
Discussion
HCWs have been proposed as part of a comprehensive policy for addressing gender equity in women’s cardiovascular care.14,20 The current study used qualitative methods to explore the patient perspective at an all-female HCW in order to understand the perceived benefit of women-centered care, including cardiovascular gender medicine and a single-sex health care delivery setting. The women in our study did not seek care at this HCW in order to obtain women-centered care; they were motivated exclusively by fear and concern for their health. While these aspects of care did not motivate attendance, the women did report added benefits of increased awareness of heart disease in women, improved health, and behavior changes, as well as the positive interpersonal and emotional benefit of an all-female staff. Women did not spontaneously identify these benefits, however; they were only identified upon subsequent targeted inquiry, in retrospect. To our knowledge, this is the first report of a qualitative assessment of patients who seek care in a HCW setting.
Single-Sex Aspect
Our findings indicate that women did not specifically seek an all-female facility. This was apparent through both indirect and direct questioning about motivation for attending the clinic. It is possible that women prefer same-sex medical care for more intimate and uniquely female care, such as gynecology or breast health,21,22 rather than cardiology. While women in our study did not seek women-centered care, they did appreciate aspects of care that they attributed to the female-to-female interaction: feeling comfortable, being understood and cared for, personalized care, and consideration of their experience and lifestyle. Women also stated that they benefitted from the clinic’s whole-person treatment.
It has been argued that women-specific services necessitate going beyond the all-female environment, providing care that is substantially different than traditional care.23,24 The care attributes mentioned by the women in this study fall under “person-centered care”, an approach to medicine that incorporates five dimensions, specifically: holistic care, attendance to patients’ beliefs and values, authentic engagement, shared decision making, and sympathetic presence.25 Providing person-directed care, however, is not limited to female providers. As reflected in our study, women report that professional and personal factors are more important than gender in their medical provider selection.22,26 Similarly, a study of an all-female cardiac rehabilitation program found that staff members’ attention to patients’ personal health concerns (and peer support) facilitated participation.27 Research finds that patient-centered communication skills rather than physician’s gender influences patient satisfaction and compliance.28 While not exclusively female-provided, research suggests that female physicians are more likely to engage in this patient-oriented style of communication, particularly with female patients.29–31
Gender Medicine Aspects
Participants reported receiving sex-specific cardiovascular information, which they may not have received in a standard multidisciplinary clinic. Women, in particular young women, cite the lack of perceived personal risk as a barrier to performing cardiovascular health-promoting behaviors.32,33 Education and increased awareness of both the medical and non-medical sex and gender-based cardiovascular risk factors, such as socioeconomic and caregiver status, the long-term impact of abuse as well as polycystic ovary syndrome, gestational diabetes, etc., may facilitate more accurate assessment of personal risk and subsequent health behaviors.34
Limitations of this study include its use of a single HCW; however, saturation was reached in the interviews. Additionally, given that study participants continue to receive clinic service, this may reduce their likelihood to provide critical responses. Similarly, those with negative opinions may be more likely to refuse participation. The majority of participants were self-referred; findings may not generalize to patients who are referred to a HCW by a medical professional. This, however, increases the likelihood of determining patient motivators.
Conclusion
While they did not actively seek women-centered care, the women in this study subsequently reported educational, health, and care provision benefits to their HCW attendance. They particularly appreciated aspects of person-centered care, specifically holistic treatment, feeling understood, consideration of their experience and lifestyle, as well as receiving personal attention and concern. These findings may inform both the design and evaluation of medical care facilities that aim to address the gender disparities in cardiovascular health and other medical specialties.
Acknowledgments
We would like to thank the research assistants who were nursing students at the Jerusalem College of Technology for their significant help. We also wish to thank the women participants for their time and insights. The study was funded by a private grant from the Pollin Family Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Abate D, Hassen Abate K, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017 GBD 2017 causes of death collaborators*. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
2. Sabbag A, Matetzky S, Porter A, et al. Sex differences in the management and 5-year outcome of young patients (<55 years) with acute coronary syndromes.. Am J Med. 2017;130(11):
3. Manteuffel M, Williams S, Chen W, Verbrugge RR, Pittman DG, Steinkellner A. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J Women’s Heal. 2014;23(2):112–119. doi:10.1089/jwh.2012.3972
4. Weisz D, Gusmano MK, Rodwin VG. Gender and the treatment of heart disease in older persons in the United States, France, and England: a comparative, population-based view of a clinical phenomenon. Gend Med. 2004;1(1):29–40. doi:10.1016/s1550-8579(04)80008-80011
5. Colella TJF, Gravely S, Marzolini S, et al. Sex bias in referral of women to outpatient cardiac rehabilitation? A meta-analysis. Eur J Prev Cardiol. 2015;22(4):423–441. doi:10.1177/2047487314520783
6. Tobias DK, Stuart JJ, Li S, et al. Association of history of gestational diabetes with long-term cardiovascular disease risk in a large prospective cohort of US women. JAMA Intern Med. 2017;177(12):1735–1742. doi:10.1001/jamainternmed.2017.2790
7. Glintborg D, Rubin KH, Nybo M, Abrahamsen B, Andersen M. Cardiovascular disease in a nationwide population of Danish women with polycystic ovary syndrome. Cardiovasc Diabetol. 2018;17:37. doi:10.1186/s12933-018-0680-5
8. McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardiovascular sequelae of preeclampsia/eclampsia: a systematic review and meta-analyses. Am Heart J. 2008;156(5):918–930. doi:10.1016/j.ahj.2008.06.042
9. Kornowski R, Orvin K. Current status of cardiovascular medicine in Israel. Circulation. 2020;142(1):17–19. doi:10.1161/CIRCULATIONAHA.119.042516
10. Swirski B, Knaaneh H, Avgar A. Health care in Israel. Isr Equal Monit. 1998;4(9):1–32.
11. Granek L, Nakash O, Carmi R. Women and health in Israel. Lancet. 2017;389(10088):2575–2578. doi:10.1016/S0140-6736(17)30563-9
12. Gross R, Tabenkin H, Schoen C, Brammli-Greenberg S, Simantov E. Health counseling for women in the absence of financial barriers: comparing reported counseling rates of women in the United States and Israel. Women Health. 2006;43(1):1–18. doi:10.1300/J013v43n01_01
13. Lundberg GP, Mehta LS, Volgman AS. Specialized care for women: the impact of women’s heart centers. Curr Treat Options Cardiovasc Med. 2018;20:9. doi:10.1007/s11936-018-0656-5
14. Aggarwal NR, Patel HN, Mehta LS, et al. Sex differences in ischemic heart disease: advances, obstacles, and next Steps. Circ Cardiovasc Qual Outcomes. 2018;11(2). doi:10.1161/CIRCOUTCOMES.117.004437
15. Low TT, Chan SP, Wai SH, et al. The women’s heart health programme: a pilot trial of sex-specific cardiovascular management. BMC Womens Health. 2018;18(1):56. doi:10.1186/s12905-018-0548-6
16. Jenkinson C. Patients’ experiences and satisfaction with health care: results of a questionnaire study of specific aspects of care. Qual Saf Heal Care. 2002;11(4):335–339. doi:10.1136/qhc.11.4.335
17. Di Palo MT. Rating satisfaction research: is it poor, fair, good, very good, or excellent? Arthritis Care Res. 1997;10(6):422–430. doi:10.1002/art.1790100610
18. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
19. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):160940691773384. doi:10.1177/1609406917733847
20. Lundberg GP, Mehta LS, Sanghani RM, et al. Heart centers for women: historical perspective on formation and future strategies to reduce cardiovascular disease. Circulation. 2018;138(11):1155–1165. doi:10.1161/CIRCULATIONAHA.118.035351
21. Kerssens JJ, Bensing JM, Andela MG. Patient preference for genders of health professionals. Soc Sci Med. 1997;44(10):1531–1540. doi:10.1016/S0277-9536(96)00272-9
22. Tam TY, Hill AM, Shatkin-Margolis A, Pauls RN. Female patient preferences regarding physician gender: a national survey. Minerva Ginecol. 2020;72(1). doi:10.23736/S0026-4784.20.04502-5
23. Carter AJ, Bourgeois S, O’Brien N, et al. Women-specific HIV/AIDS services: identifying and defining the components of holistic service delivery for women living with HIV/AIDS. J Int AIDS Soc. 2013;16(1):17433. doi:10.7448/IAS.16.1.17433
24. Shaw LJ, Pepine CJ, Xie J, et al. Quality and equitable health care gaps for women. J Am Coll Cardiol. 2017;70(3):373–388. doi:10.1016/j.jacc.2017.05.051
25. McCormack B, McCance TV. Person-Centred Practice in Nursing and Healthcare: Theory and Practice. London: Wiley-Blackwell; 2017.
26. Amir H, Tibi Y, Groutz A, Amit A, Azem F. Unpredicted gender preference of obstetricians and gynecologists by Muslim Israeli-Arab women. Patient Educ Couns. 2012;86(2):259–263. doi:10.1016/j.pec.2011.05.016
27. Rolfe DE, Sutton EJ, Landry M, Sternberg L, Price JAD. Women’s experiences accessing a women-centered cardiac rehabilitation program. J Cardiovasc Nurs. 2010;25(4):332–341. doi:10.1097/JCN.0b013e3181c83f6b
28. Christen RN, Alder J, Bitzer J. Gender differences in physicians’ communicative skills and their influence on patient satisfaction in gynaecological outpatient consultations. Soc Sci Med. 2008;66(7):1474–1483. doi:10.1016/j.socscimed.2007.12.011
29. Roter DL, Hall JA, Aoki Y. Physician gender effects in medical communication: a meta-analytic review. JAMA. 2002;288(6):756–764. doi:10.1001/jama.288.6.756
30. Sandhu H, Adams A, Singleton L, Clark-Carter D, Kidd J. The impact of gender dyads on doctor–patient communication: a systematic review. Patient Educ Couns. 2009;76(3):348–355. doi:10.1016/j.pec.2009.07.010
31. Roter DL, Hall JA. Physician gender and patient-centered communication: a critical review of empirical research. Annu Rev Public Health. 2004;25:497–519. doi:10.1146/annurev.publhealth.25.101802.123134
32. Gooding HC, Brown CA, Liu J, Revette AC, Stamoulis C, de Ferranti SD. Will teens go red? Low cardiovascular disease awareness among young women. J Am Heart Assoc. 2019;8(6). doi:10.1161/JAHA.118.011195
33. Mosca L, Hammond G, Mochari-Greenberger H, Towfighi A, Albert MA. Fifteen-year trends in awareness of heart disease in women: results of a 2012 American Heart Association national survey. Circulation. 2013;127(11):1254–1263. doi:10.1161/CIR.0b013e318287cf2f
34. O’Neil A, Scovelle AJ, Milner AJ, Kavanagh A. Gender/sex as a social determinant of cardiovascular risk. Circulation. 2018;137(8):854–864. doi:10.1161/CIRCULATIONAHA.117.028595
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.