")
Back to Journals » Clinical Optometry » Volume 9
Distance associated heterophoria measured with polarized Cross test of MKH method and its relationship to refractive error and age
Authors Kříž P , Skorkovská Š
Received 29 September 2016
Accepted for publication 29 November 2016
Published 31 March 2017 Volume 2017:9 Pages 55—65
DOI https://doi.org/10.2147/OPTO.S123436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Pavel Kříž,1 Šárka Skorkovská1,2
1Faculty of Medicine, Department of Ophthalmology and Optometry, Masaryk University, 2Eye Clinic NeoVize Brno, Brno, Czech Republic
Purpose: Due to the expansion of modern optotype liquid crystal display with the help of positive polarization, measurement of heterophorias (HTFs) by means of polarization, and thus partial dissociation of perceptions, has become more and more accessible. Our aims were to establish the prevalence of distance associated HTF by measuring with polarized Cross test of MKH [measuring and correcting methodology after H-J Haase] method and its association with age and refractive error in clinical population of wide age range.
Methods: A cross-sectional study was carried out with 170 clinical subjects aged 15–78 years with an average age of 40.7±16.62 years. All the participants had best-corrected visual acuity better than 20/25, stereopsis ≤60 second of arc, no heterotropia, not undergone vision therapy, and had no eye disease. The distance associated HTF was measured with the Cross test of the MKH methodology. The quantification of associated HTF was acquired by means of Risley rotary prism.
Results: The occurrence of distance associated HTF was found in 71.2% of participants. Of the total, 36.5% of the cases had esophoria (EP), 9.4% EP and hyperphoria, 10.6% exophoria (XP), 7.1% XP and hyperphoria, 7.6% hyperphoria, and 28.8% orthophoria. The mean distance horizontal associated HTF was +0.76±2.38 ∆. With EP, the mean value was +2.47±2.18 ∆, and with XP, −2.1±1.72 ∆. There was no correlation observed between the amount of distance associated HTF and age. There was no effect of the type and amount of a refractive error on the amount of distance associated HTF.
Conclusion: A high occurrence of distance associated HTF was revealed while performing the polarized Cross test of MKH method. The relationship between the degree of associated HTF and refractive error and age was not proved.
Keywords: associated heterophoria, Cross test, esophoria, exophoria, prisms, refractive error
Introduction
Heterophoria (HTF) is the tendency of the lines of sight (visual axes) to deviate from the relative positions necessary to maintain single binocular vision for a given distance of fixation.1 This tendency is identified by the occurrence of an actual deviation in the absence of an adequate stimulus to fusion, occurring in variously designated forms according to the relative direction or orientation of the deviation. HTF has been attributed to four main categories of etiologies namely anatomical, refractive, uniocular activity, and trauma.2
A small amount of HTF is present in 70%–80% of the population.3 This view differs from those of Schor and Ciuffreda4 and Dowley5 who reported that there is a high prevalence of distance orthophoria in the population despite a large number of mechanical, neural, and sensory variables. Several studies indicated that there is a relationship between HTF and age.6–11 While all of them support this relationship for near HTF,6–11 it is usually not proved with distance HTF.6,8,9 Several methods can be used to eliminate fusion so as to achieve dissociation of the eyes, allowing measurement of the phoria.12 Methods for measuring the degree of HTF require complete dissociation of the two eyes, for example the Maddox rod, the wing test,13 the cover test,12 and the von Graefe technique. Another approach is to dissociate only a part of the visual field.13 These methods leave the part of the visual field common to both eyes, providing a stimulus to fusion. The term used to describe this is fusion lock: it may be the central fixation area, or it can be a peripheral fusion lock. The dissociation is achieved by a septum (eg, Turville infinity balance test), by a method of cross-polarization, or by colored filters. The quantification of the phoria is achieved in different ways, usually by prism manipulation or by using various types of scales.12
HTF values may vary from one procedure to another.14–17 It has been found out that for the von Graefe technique, the average HTF was more exophoric than for the Maddox rod.15,16 Post hoc analysis using the Fisher protected least significant difference technique indicated significant differences between each of the mean findings obtained using the von Graefe, Maddox rod, and modified Thorington procedures.15 For instance, the mean value for von Graefe method, when measured with the phoropter, was −0.53±0.24 ∆ exophoria (XP), and for Maddox rod with the phoropter, the mean value was +1.81±0.26 ∆ esophoria (EP). The length of time that fusion is disrupted will also affect measurements in a way that a longer duration of dissociation will decrease vergence adaptation.18
Dissociated phoria follows when both retinal images differ so much (and so dissociate) that they represent no fusional stimuli.19 Probably, the most commonly used subjective dissociated phoria test is the von Graefe test.20 Another common test using a tangent scale and a Maddox rod over one eye is referred to as the modified Thorington test. Ogle et al21 already differentiated between dissociated and associated HTF, where “dissociated” referred to measurements under eliminated fusion and “associated” referred to measurements in the presence of fusion stimuli. The term associated phoria refers to the value of the prism that nulls a fixation disparity detected under conditions of partial dissociation.22 Fixation disparity and associated phoria have been thought to be an indicator of a decompensated phoria that gives rise to symptoms.23 It has been previously shown that there is little correlation between the degree of HTF and the compensation, but that fixation disparity and associated phoria are better indicators.24–26
HTF measured with the Cross test refers to the deviation under conditions of peripheral fusion, not total dissociation, for example, conditions similar to those of the traditional Turville infinity balance.22 The test is mainly used for the determination of what was described by Ogle et al21 as associated phoria. We can also find a description as follows: correction of motor-compensated associated HTF components and/or fixation disparity of the first type.27 Haase et al28 described a motor fully compensated HTF as a condition in which the vergence demand is matched by the fusional vergence. If stress is placed on the binocular visual system, either through an increased amount of near work (direct stress) or through stress on the patient’s well-being (indirect stress), small errors of the vergence system, fixation disparities, develop in the direction of the position of rest. This is designated disparate fusion by Haase, being the first stage of sensory adaptation to associated phoria. Both vertical and horizontal components can be examined with the Cross test.22 With the normal polaroid filter setting, the vertical broken line is seen with the right eye and the horizontal broken line with the left eye (Figure 1).
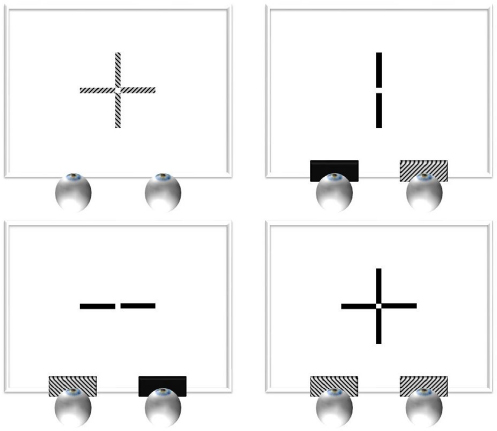 | Figure 1 Positively polarized Cross test. Notes: Left top: perception on the Cross test without polarization filters; right top: perception by the right eye with polarization filters; left bottom: perception by the left eye with polarization filters; right bottom: perception by both eyes with polarization filters. |
The studies that dealt with the relationship of the distance associated phorias measured with the Cross test and distance dissociated phorias measured with Maddox rod test have not found any statistically significant difference between the results.19,29,30 Therefore, the results of our study, which were obtained by the use of the Cross test, are also discussed with the methods that use complete dissociation.
Due to the expansion of modern optotype liquid crystal display (LCD) with the help of positive polarization, measurement of HTFs by means of polarization, and thus partial dissociation of perceptions, becomes more and more accessible. The overwhelming majority of the studies, which dealt with the HTFs occurrence, their amount, and relationship with other variables, use the tests with full dissociation of perceptions for measuring HTF. However, for the polarized Cross test of MKH [measuring and correcting methodology after H-J Haase] method, which offers partial dissociation of perceptions, there is a lack of scientific studies on HTFs occurrence, their amount, and relationship with other variables. The goal of this study is to determine the occurrence, amount, and relationship of HTF measured with the polarized Cross test of MKH method with relation to age and refractive error.
Methods
Participants
The participants were a clinical population of 170 patients of wide age range (15–78 years). The study design fulfilled the tenets of the Declaration of Helsinki. Written informed consent was obtained for this study from all of the study participants. Four of them were <16 years of age, and therefore, the written informed consent was obtained from their parents. Because of the requirement of normal binocularity, our classification criteria were as follows: best-corrected visual acuity ≥20/25, stereopsis ≤60 second of arc, no heterotropia, no history of vision therapy, and no eye disease.
Procedures
All the subjects were examined by the first author, with the same instruments under the same conditions. The tests and measurements were as follows: history and symptoms, visual acuity without correction, preliminary examination (gross fields, pupil reaction, motility), cover test, objective refraction, monocular subjective refraction, associated HTF measurements, visual acuity with correction, and binocular balancing. In order to exclude strabismus, the cover test was performed. The conditions of the optometrist’s office, devices used, measurement of refractive error, and associated phoria measured with the Cross test were in compliance with guidelines Richtlinien zur Anwendung der MKH available on www.ivbs.org. Associated HTF measurements were taken immediately after the completion of this routine and with correction of a refractive error. Stereopsis measurement and binocular balance were only performed after associated HTF measurement. Polarizing filters were used for measuring associated phoria in order to separate the visual objects for the right and left eyes. Targets were presented at a distance of 5.85 m on an LCD. Subjective correction and measurement of distance associated phorias were performed with the use of a manual phoropter. The quantification of distance associated phorias was achieved by means of Risley prisms. The values were detected to an accuracy of 0.25 ∆. The measurement of associated HTF is only sensible after the refractive correction has been carefully determined.27
The Cross test was presented monocularly without analyzers to the eye last refracted, that is, leaving the occluder in the trial frame.27 Prior to placing the polarization analyzers and removing the occlusion, the patient was given an explanation of the procedure that would follow. The goal of the Cross test is to achieve a steady zero test position (alignment) with the weakest possible prism in both types of presentation.27 If this goal cannot be achieved, the best possible symmetry must be strived for, that is, oscillation or jumping of the test detail seen unsteadily on both sides of alignment, equally far and equally often and long regarding position and time. As for the combination of horizontal and vertical deviation, the horizontal part was dealt with first, and after that, the vertical part was addressed.
The phoropter’s oculars were centered according to the individual monocular pupillary distances. In the course of measuring, the rule of the interpupillary distance change was used in relation to the amount of the applied prisms so that the sight axis always crossed optical centers of the correction spherical and cylindrical glasses.27 For the vertex distance of 12 mm, it is necessary, with 1 ∆ of an inserted wedge, to decenter the oculars of 0.25 mm against the direction of the base. When vertical prisms are applied, different heights of the oculars must be generated so that the sight axis still crosses optical centers of the correction spherical and cylindrical glasses. However, the majority of phoropters and trial frames do not allow for this function, and so was the case with the phoropter used in this study. Therefore, the result value of the vertical prism was added with a calculation with the use of Prentice’s equation (P = d∙S).27
Statistical analysis
The statistics were calculated using the software STATISTICA 12 (Statistica, Tulsa, OK, US). All quantitative data were expressed as mean ± standard deviation (SD). Box plots were used for visual comparison of the samples. Analysis of variance (ANOVA) test was used to distinguish between three groups of patients (emmetropia, myopia, and hyperopia). Relationships between two parameters or their changes were measured by coefficient of correlation (amount of horizontal associated HTF at distance and age, amount of vertical associated HTF at distance and age, amount of horizontal associated HTF at distance, and amount of spherical equivalent [SE] of refractive error). All tests were performed at the 5% level of significance.
Results
There were 170 probands included in this study, of which 65 were men and 105 women. The average age was 40.7±16.6 years. The most frequent representation was that of emmetropia (40%), and then myopia (28.2%), hypermetropia (22.9%), astigmatism (6.5%), and antimetropia (2.4%). A cover test was used in order to exclude heterotropia. All the participants in the study presented with stereopsis.
Due to the classification of distance associated HTF according to the direction of horizontal and vertical deviation, 36.5% of the cases had EP, 9.4% EP and hyperphoria, 28.8% orthophoria, 7.1% XP and hyperphoria, 7.6% hyperphoria, and 10.6% XP. When classifying associated HTF only according to the direction of horizontal deviation (ignoring vertical component), 45.9% of the cases had EP, 17.6% XP, and 36.5% orthophoria. The occurrence of distance associated HTFs within the examined group is illustrated in Table 1.
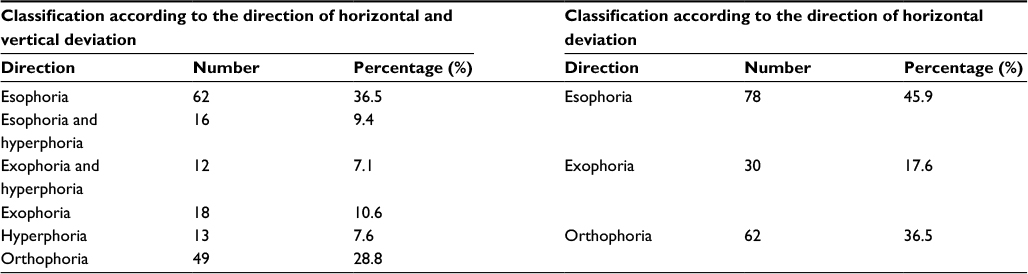 | Table 1 Occurrence of distance associated HTF Abbreviation: HTF, heterophoria. |
The distance horizontal associated HTF ranged from −8.75 ∆ to +14.5 ∆, with a mean of +0.76±2.38 ∆. EP ranged from +0.5 ∆ to +14.5 ∆ with a mean of +2.47±2.18 ∆. XP ranged from −8.75 ∆ to −0.25 ∆ with a mean of −2.1±1.72 ∆. The vertical associated phorias ranged from −5.5 ∆ left hyperphoria to +4.5 ∆ right hyperphoria with a mean of −0.06±0.69 ∆ left hyperphoria. For the purpose of this paper, EPs and right hyperphorias are marked by a plus sign, while XPs and right hypophorias are marked by a minus sign. The quoted values for the distance horizontal associated HTF, EP, and XP are shown in Table 2, and the distribution of the distance horizontal and vertical associated HTF for the group is illustrated in Figures 2 and 3. The mean values of SE of right and left eyes were −0.37±1.74 D. The distribution of SE is illustrated in Figure 4.
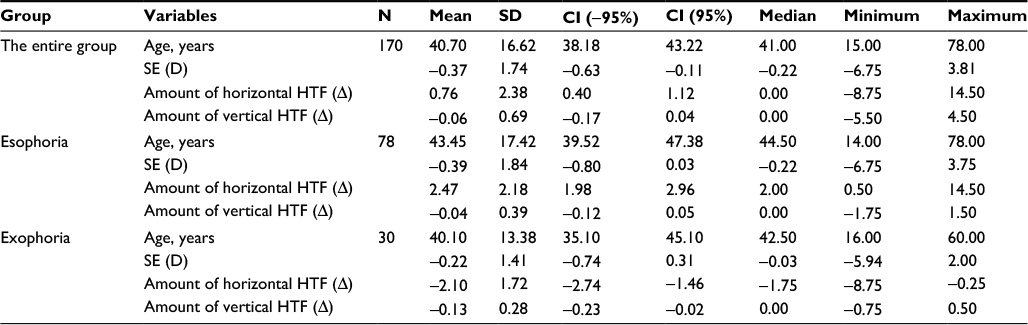 | Table 2 Descriptive statistics for the total group, esophorias, and exophorias Abbreviations: CI, confidence interval; D, diopter; HTF, heterophoria; SD, standard deviation; SE, spherical equivalent. |
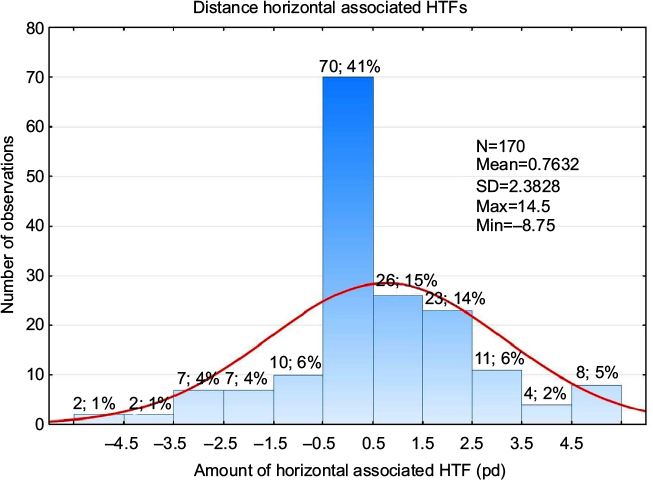 | Figure 2 Histogram of frequency representation of distance horizontal associated HTFs. Abbreviations: HTFs, heterophorias; pd, prism diopter (∆); SD, standard deviation. |
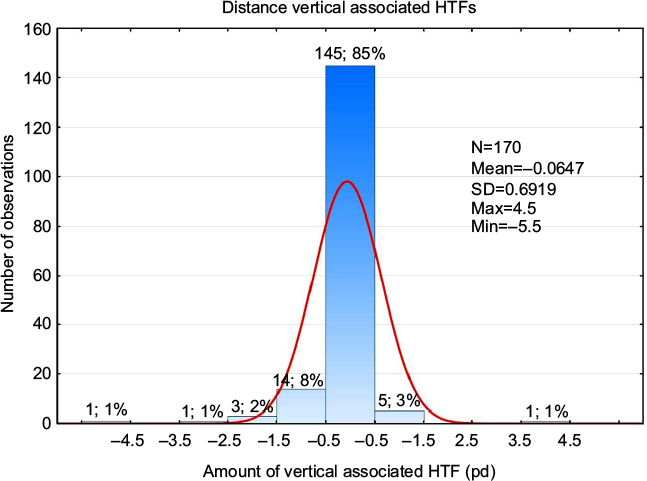 | Figure 3 Histogram of frequency representation of distance vertical associated HTFs. Abbreviations: HTFs, heterophorias; pd, prism diopter (∆); SD, standard deviation. |
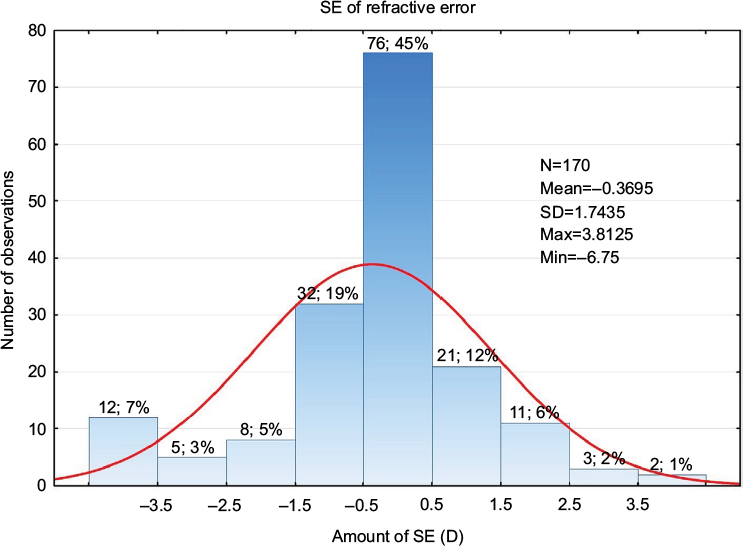 | Figure 4 Histogram of frequency representation of spherical equivalent of refractive error. Abbreviations: D, diopter; SD, standard deviation; SE, spherical equivalent. |
Dependence of associated HTF on age
The correlation between the amount of horizontal and vertical associated HTFs at distance and age was determined for the entire group and individually for EP and XP. The correlation did not appear with all the cases (horizontal associated HTF and age: r=0.0867, p=0.2611 [Figure 5]; EP and age: r=0.0193, p=0.867; XP and age: r=–0.0656, p=0.7305; vertical associated HTF and age: r=0.0625, p=0.4183 [Figure 6]).
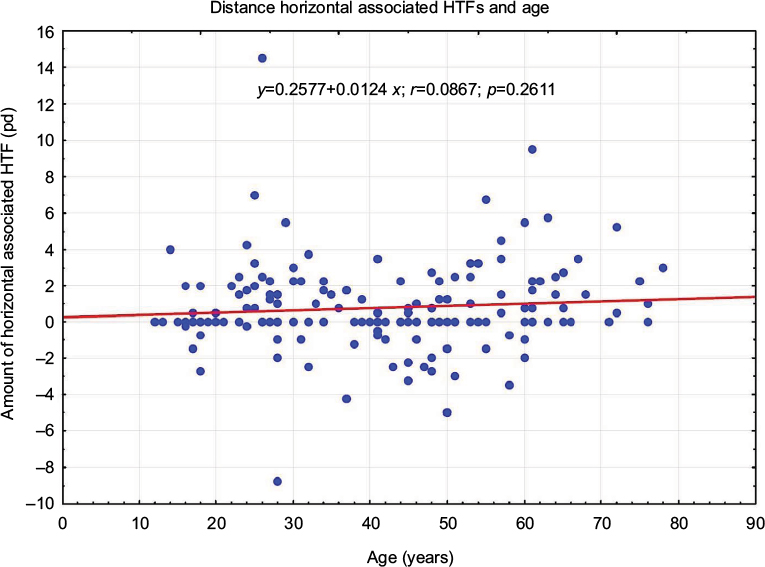 | Figure 5 Correlation between the amount of distance horizontal associated HTFs and age. Notes: Blue dots represent entities with varying amounts of horizontal associated HTFs and age. The red line represents the regression line. Abbreviations: HTFs, heterophorias; pd, prism diopter (∆). |
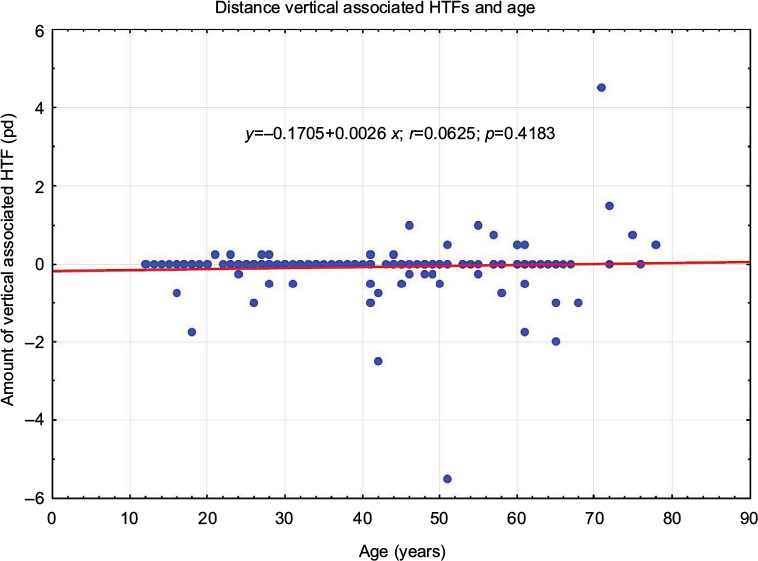 | Figure 6 Correlation between the amount of distance vertical associated HTFs and age. Notes: Blue dots represent entities with varying amounts of vertical associated HTFs and age. The red line represents the regression line. Abbreviations: HTFs, heterophorias; pd, prism diopter (∆). |
Associated HTF dependence on the refractive error type
While determining the relationship between distance associated HTF and refractive error, a statistically significant difference was verified by means of the ANOVA method within the mean values of associated horizontal HTF at distance for myopia, hyperopia, and emmetropia.
With the myopia group, the mean of horizontal associated HTF at distance was identified as +1.1±2.32 ∆, for hyperopia group as +1.2±2.26 ∆, and for emmetropia group as 0.3±2.4 ∆. EP was predominant with all these groups, the most with myopia, then with hyperopia, and the least with emmetropia group. Nevertheless, no statistically significant difference has been proved for the groups of myopia, hyperopia, or emmetropia (F(2;152)=2.4048; p=0.0937) (Figure 7).
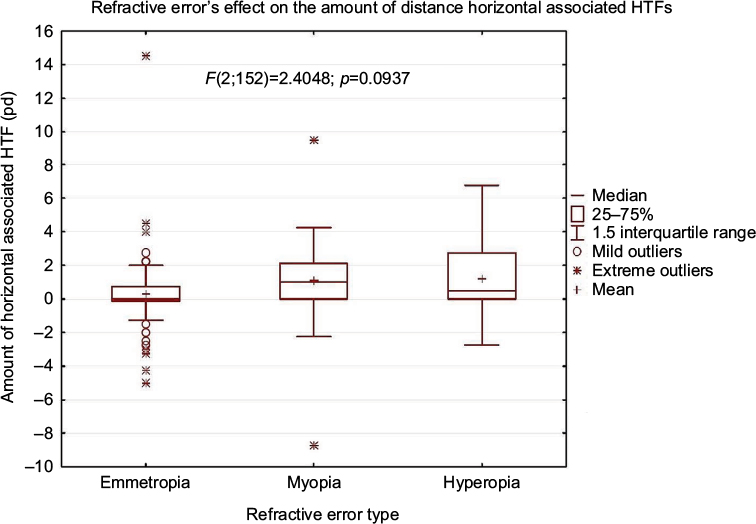 | Figure 7 Box plot illustrates values of distance horizontal associated HTF for refractive errors. Abbreviations: HTFs, heterophorias; pd, prism diopter (∆). |
Next, a correlation between the amount of EP and the amount of SE of refractive error was determined. The correlation was not proved (r=0.0072, p=0.9258) (Figure 8).
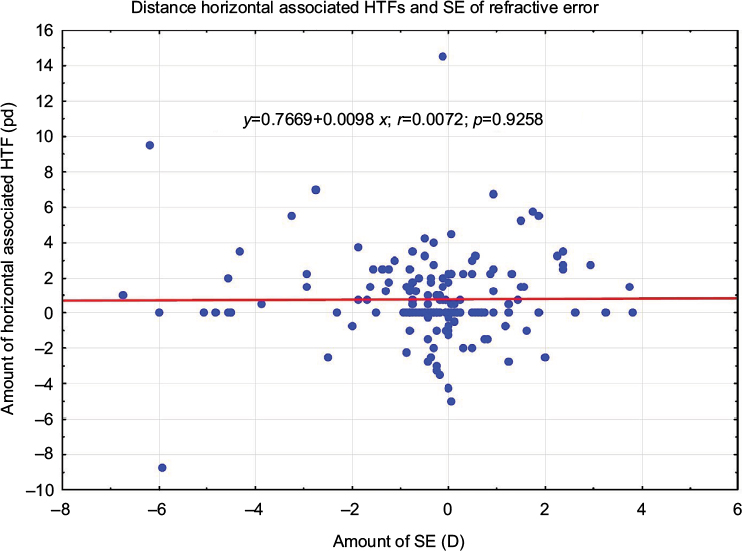 | Figure 8 Correlation between amount of distance horizontal HTF and amount of spherical equivalent. Notes: Blue dots represent entities with varying amounts of horizontal associated HTFs and SE of refractive error. The red line represents the regression line. Abbreviations: D, diopter; HTFs, heterophorias; pd, prism diopter (∆); SE, spherical equivalent. |
Discussion
With the reduced division of associated HTF only into horizontal and individual vertical deviations, the most frequent representation was with EP (45.9%), and then with orthophoria (28.8%), XP (17.6%), and vertical phoria (7.6%). Mean distance horizontal associated HTF values were +0.76±2.38 ∆ EP ranging from −8.75 ∆ XP to +14.5 ∆ EP. EP ranged from +0.5 ∆ to +14.5 ∆ with a mean of +2.47±2.18 ∆. As for XP, the range was from −8.75 ∆ to −0.25 ∆ with a mean of −2.1±1.72 ∆. The study has not proved any correlation between distance associated HTF and refractive error and age.
Occurrence of HTF
Makgaba31 researched a clinical population ranging from 18 to 30 years of age. The total number of the examined patients was 475, and they were black South Africans. HTF was measured for each patient using the von Graefe method. XP was the most common for distance vision (61%, N=287), followed by orthophoria (20%, N=95) and EP (19%, N=90). Horizontal HTF for distance vision, measured at 6 m, ranged from +16 ∆ EP to −12 ∆ XP with a mean of −0.74±2.84 ∆ XP. For distance vision, EP ranged from +0.5 ∆ to +16 ∆ with a mean of +3.08±3.09 ∆, while XP ranged from −0.5 ∆ to −12 ∆ with a mean of −2.21±1.82 ∆. The HTF occurrence and the mean values of EP and XP were very similar to those in our paper. However, the mean HTF for the entire group significantly differed. In the above-mentioned study, it appears to be XP, but in our study, it is EP. The reason for the dissimilar results can be the fact that entirely different dissociation techniques were used there. Another reason can be the fact that the values obtained in Makgaba’s study31 were obtained by several students and therefore there may be inter-examiner differences.
The von Graefe method was also used in the study by Letourneau and Giroux,32 which was carried out on a large group of children (N=2048) at the age of 6–13 years. HTF was measured at the distance of 3 m, and prism was applied with the use of the prism bars. The mean value of HTF for the entire group was +0.57±2.54 ∆, and the most frequent representation was with orthophoria, next with EP, and then XP. The mean value of HTF was similar to our study. The difference in the representation of the direction types of HTF between the study by Letourneau and Giroux32 and our study can be again partly ascribed to different dissociation technique and a different method of quantification of HTF with the use of prism bars, thus determining the values to be taken only in terms of rather large steps. Due to the fact that the prism bars for measuring a horizontal deviation usually provide the lowest value of 1 ∆, the lowest HTF values are considered to be a condition of orthophoria for this study. This might be one of the reasons for the fact that orthophoria has the highest representation within this study. The distance from which distance HTFs were measured also differed significantly.
The prevalence of orthophorias was also found out by the study “Heterophoria” by Dowley,5 where a large group of 925 probands were measured by means of a modified Maddox rod technique. EP was represented more than XP. In comparison to our study, there was a different method of dissociation as well as its length, which lasted 15 s in a totally darkened room. Also, the phoria was measured quickly (in <5 s to reduce adaptive effect) with a Risley prism.
EP also predominated over XP in the study by Scobee and Groen,17 which proved reliability of the Maddox rod phoria test by comparing phoria measurements taken by two examiners on different days. Examiner A found the mean of 1.1 ∆ EP, and examiner B found the mean of 1.3 ∆ EP.
When comparing two methods of measurement of dissociated phoria, it was proved that the values were significantly more exophoric when measured by means of the von Graefe method.15,16,33 Maples et al33 found the mean phoria at distance with the von Graefe method was −1.75 ∆ XP and with the Howell card was −0.11 ∆ XP. More exophoric values of dissociated phoria between the von Graefe method and Maddox rod method were found in the studies by Casillas Casillas and Rosenfield15 and Schroeder et al.16 Our results concerning the representation of the direction type of HTF and the mean values of HTF are more similar to the studies that use the Maddox rod method.
Kromeier et al19 examined the relationship between occurrences of dissociated phorias, measured by Maddox rod test and associated phorias measured by the Cross test at the distance of 5 m. The paper evaluated results of 43 participants who suffered from HTF >1 ∆. The amount of HTF was measured by means of a polarized Cross test, and Risley prism, as it was the case with our study. A 10-min break was taken between the measurements of dissociated phorias and associated phorias. Sixty-three percent of the participants had EP and 37% XP. The correlation between the results obtained with the white Maddox rod test and the Cross test was r=0.89 (p<0.0001). The methods used for measuring the associated HTF in Kromeier et al’s study19 are identical with our study, and higher EP occurrence than XP occurrence was proved, which corresponds with our results. No statistically significant difference between the values of HTF measured with the Maddox rod test and those measured with the Cross test was found by Hilz and Heinen29 and Wulff.30
Letourneau and Giroux32 found distance vertical HTF within the range from 2 prism diopter (pd) left hyperphoria to 2 pd right hyperphoria with a mean of 0.07 pd (SD=±0.69). Very similar results were also reported in the study by Mathebula et al34 in terms of the range of vertical HTF from 1.8 pd left hyperphoria to 2 pd right hyperphoria with a mean of 0.01 pd right hyperphoria (SD=±0.22). Makgaba31 measured a higher range of distance vertical HTF – from −5 ∆ left hyperphoria to +3 ∆ right hyperphoria with a mean of +0.05±0.76 ∆ right hyperphoria. These results are closest to our paper’s results, where the range of distance vertical HTF is from −5.5 ∆ left hyperphoria to +4.5 ∆ right hyperphoria with a mean of −0.06±0.69 ∆ left hyperphoria. The mean values of vertical HTF are very similar. The high range of vertical HTF, as it was discovered in our study, can be ascribed to the different method of dissociation as well as the way of quantification of HTF. Razavi et al35 found the representation of hyperphoria within the examined group to be lower than in our study, while Jackson and Bedell36 found it considerably higher. Vertical HTF in our study was measured with the same test as horizontal HTF, and only after, it had been corrected by means of the Risley prisms.
Distance HTF’s dependence on age
Our study has not supported correlation between the amount of distance associated HTF and patients’ age.
The same conclusion was made by Freier and Pickwell6 who examined the patients who underwent optometric examination. The sample comprised 663 patients. The degree of HTF for distance vision was measured by the Maddox groove method with the patient’s spectacle correction, if there was any. The division was into 15 age categories per 5 years, while the youngest age group included 5- to 9-year-old children. The oldest age group ranged from the age of 75–85 years. The mean distance HTF was +0.3±2.18 ∆ EP. The change of distance HTF with relation to age was not statistically significant. A comparison between males and females revealed no significant difference in HTF of any age to the distance.
The relationship between HTF and age was not supported by Palomo Alvarez et al’s37 study either, where the von Graefe technique was used for dissociation and the quantification of distance associated phorias was achieved by means of Risley prisms. The study population consisted of 271 subjects (104 women and 167 men) stratified into six age groups – from 20 to 80 years of age, each group per every 10 years. The study revealed no significant changes in mean distance phoria with the age groups. Both of the above-mentioned studies6,37 and Makgaba’s study31 correspond with the findings in our study where no relationship between HTF and age was identified. Similarly, the studies by Walline et al38 and Letourneau and Giroux32 did not find any significant changes of HTF with age of children.
Different results were obtained by Hirsch et al,10 using the von Graefe prism method through the subjective correction, which showed that average distance phoria became gradually more esophoric with age. Also in the study by Kephart and Oliver,7 the coefficients of correlation between age and phoria scores at the far distance indicated a slight tendency toward EP with increasing age for both males and females.
Spierer and Hefetz11 studied changes of HTFs over 20 years with a single group of subjects. The testing conditions remained constant during the 20 years of the study. Binocular function tests for phorias at distance and near were performed by the Maddox rod (with prism bar) and Maddox wing, respectively. The mean distance HTF at the age of 18–22 years was compared with the mean distance HTF at the age of 34–38 years. The mean HTF for distance fixation for individuals aged 18–22 years was EP of +0.9±1.9 ∆, and for those aged 34–48 years, +1.80±2.6 ∆. A mean change of 0.9±1.7 ∆ increase in EP was found, and this was statistically significant (p < 0.001). It can be explained by a mild weakening of extraocular muscle function. In case of distance fixation, when the lateral rectus muscles play the major role, this weakening will result in more pronounced EP.11 The main advantage of the study presented here, compared with the previous reports, is the comparison of the variables of the same group of subjects at different ages.
The relationship between associated HTF and age is addressed in the clinical study of 201 asymptomatic patients by Godio and Rutstein.39 The associated HTF was recorded (with the refractive correction in the refractor) at a viewing distance of 6 m, and the quantification of associated phorias was achieved by means of Risley prisms. At distance, the associated phoria was determined while a patient was binocularly viewing the foveal lock, fixation disparity target of American Optical Vectograph slide through polaroid analyzers in the refractor. The amount of distance associated phoria was not statistically related to patient age or sex. Neither Pickwell et al40 supported the relationship between associated HTF and age.
Distance HTF’s dependence on refractive errors
In our study, no statistically significant difference has been proved for the groups of myopia, hyperopia, or emmetropia.
Risovic et al41 explored refractive errors and binocular dysfunctions in a population of 230 university students and 234 nonstudent subjects aged 18–27 years. Horizontal phoria was measured by Maddox wing method with correction of refractive error. XP was significantly more frequent in myopic subjects. EP was significantly more frequent in hypermetropic subjects.
The relationship between HTF and refractive error was also proved in the study by Leone et al.42 With children aged 6–12 years, HTF was measured by means of the alternating cover test with the use of Luneau prism bars. The children with hyperopia were significantly more likely to have EP at near and distance than those without refractive error. In the case of the older children, those with myopia were significantly more likely to be exophoric at near and distance than those without refractive error. In comparison with our study, where the relationship between HTF and age was not proved, both of the studies used entirely different dissociated methods. In addition, the study by Leone et al42 proved the relationship between HTF and refractive error when measured without glasses. For instance, with the association between EP and hyperopia, this may lead to the need for greater accommodative efforts to overcome hyperopia. Acting in concord with convergence, this tendency impacts ocular alignment, causing an esodeviation.43 The quantification of HTF and classification criteria also differed. Due to the use of prism bars in 2 ∆ steps, HTF was classified as far as the value >2 ∆.
The correlation between HTF and refractive error was, as it was the same case in our study, neither proved in the study by Gupta et al44 and Junghans et al.45
Conclusion
High distance associated HTF occurrence, measured with polarized Cross test of MKH method, which has been proved by this study, highlights the appropriateness of them being established as a regular part of the eye function measurement. In addition, the study has not proved any dependence of the distance associated HTF amount on refractive error or age. According to these findings, associated HTF does not occur only with high refractive errors and in elderly patients. This supports the appropriateness of performing screening with every client, primarily in case of typical symptoms of binocular function disorders.
Acknowledgments
The authors express their sincere gratitude to MD. Andrea Gaherova for her valuable guidance and constructive criticism, and also to all those who participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Hofstetter HW, Griffin JR, Berman MS, Everson RW. Dictionary of Visual Science and Related Clinical Terms. 5th ed. Boston: Butterworth-Heinemann Ltd; 2000. | ||
Lyle TK, Bridgeman GJO. The binocular reflexes and the treatment of strabismus. In: Worth CA, Bridgeman GJO, Chavasse FB, Lyle TK, editors. Worth and Chavasse’s Squint. Ballière: Tindall & Cox; 1959:345–355. | ||
Kommerell G, Kromeier M. [Prism correction in heterophoria]. Prismenkorrektion bei heterophorie. Ophthalmologe. 2002;99(1):3–9. German [with English abstract]. | ||
Schor CM, Ciuffreda KJ. Vergence Eye Movements: Basic and Clinical Aspects. Boston: Butterworth-Heinemann Ltd; 1983. | ||
Dowley D. Heterophoria. Optom Vis Sci. 1990;67(6):456–460. | ||
Freier BE, Pickwell LD. Physiological exophoria. Ophthalmic Physiol Opt. 1983;3(3):267–272. | ||
Kephart NC, Oliver JE. A study of the relationship between lateral phoria and age. Am J Optom Arch Am Acad Optom. 1952;29(8):423–429. | ||
Sheedy JE, Saladin JJ. Exophoria at near in presbyopia. Am J Optom Physiol Opt. 1975;52(7):474–481. | ||
Yekta AA, Pickwell LD, Jenkins TC. Binocular vision, age and symptoms. Ophthalmic Physiol Opt. 1989;9(2):115–120. | ||
Hirsch MJ, Alpern M, Schultz HL. The variation of phoria with age. Am J Optom Arch Am Acad Optom. 1948;25(11):535–541. | ||
Spierer A, Hefetz L. Normal heterophoric changes: 20 years’ follow-up. Graefes Arch Clin Exp Ophthalmol. 1997;235(6):345–348. | ||
Goss DA. Ocular Accommodation, Convergence, and Fixation Disparity: A Manual of Clinical Analysis. 2nd ed. Boston: Elsevier Health Sciences; 1995. | ||
Evans BJW. Pickwell’s Binocular Vision Anomalies. 5th ed. Edinburgh: Butterworth-Heinemann; 2007. | ||
Rainey BB, Schroeder TL, Goss DA, Grosvenor TP. Inter-examiner repeatability of heterophoria tests. Optom Vis Sci. 1998;75(10):719–726. | ||
Casillas Casillas E, Rosenfield M. Comparison of subjective heterophoria testing with a phoropter and trial frame. Optom Vis Sci. 2006;83(4):237–241. | ||
Schroeder TL, Rainey BB, Goss DA, Grosvenor TP. Reliability of and comparisons among methods of measuring dissociated phoria. Optom Vis Sci. 1996;73(6):389–397. | ||
Scobee RC, Groen EL. Tests for heterophoria; reliability of tests, comparisons between tests, and effect of changing testing conditions. Trans Am Acad Ophthalmol Otolaryngol. 1947;51:179–197. | ||
Griffin JR. Binocular Anomalies: Procedures for Vision Therapy: Diagnosis and Vision Therapy. 2nd ed. Chicago: Professional Press; 1982. | ||
Kromeier M, Schmitt C, Bach M, Kommerell G. Vergleich zwischen dissoziierter und assoziierter Heterophorie [Comparison between dissociated and associated heterophoria]. Ophthalmologe. 2002;99(7):549–554. German [with English abstract]. | ||
Goss DA, Reynolds JL, Todd RE. Comparison of four dissociated phoria tests: reliability and correlation with symptom survey scores. J Behav Optom. 2010;21:99–104. | ||
Ogle KN, Martens TG, Dyer JA. Oculomotor Imbalance in Binocular Vision and Fixation Disparity. Philadelphia: Lea & Febiger; 1967. | ||
Brautaset RL, Jennings JA. Associated phoria and the measuring and correcting methodology after H.-J. Haase (MKH). Strabismus. 2001;9(3):165–176. | ||
Mallett RF. Fixation disparity—its genesis and relation to asthenopia. Ophthalmic Opt. 1974;14:1159–1168. | ||
Pickwell D, Jenkins T, Yekta AA. The effect on fixation disparity and associated heterophoria of reading at an abnormally close distance. Ophthalmic Physiol Opt. 1987;7(4):345–347. | ||
Pickwell LD, Jenkins TC, Yetka AA. Fixation disparity in binocular stress. Ophthalmic Physiol Opt. 1987;7(1):37–41. | ||
Yekta AA, Jenkins T, Pickwell D. The clinical assessment of binocular vision before and after a working day. Ophthalmic Physiol Opt. 1987;7(4):349–352. | ||
Haase HJ. Winkelfehlsichtigkeiten mit Fixationsdisparation [Angular deviation fixation with fixation disparity]. Pforzheim: Verlag Bode; 1999. German. | ||
Haase HJ, Goersch H, Baust D, Tries R. Zur Fixationsdisparation: Eine erweiterte Theorie und praktische Folgerungen [To Fixation Disparation: An Advanced Theory and Practical Follow-up]. 2nd ed. Heidelberg: Verlag Optische Fachveröffentlichung; 2000. German. | ||
Hilz R, Heinen R. Untersuchungen zur Vergenzruhelage bei Kurz-und Langzeitdarbietung [Studies on the vergence resting position in short- and long-term performance]. Dtsch Opt Ztg. 1988;11:6–9. German [with English abstract]. | ||
Wulff U. Zusammenhang von Vergenzruhelage und Leuchtdichte zentral dargebotener Testzeichen [Context of vergence resting position and luminance of centrally presented test marks] [dissertation]. Berlin: Freie Universität; 1980. German. | ||
Makgaba NT. A retrospective analysis of heterophoria values in a clinical population aged 18 to 30 years. Afr Vis Eye Health. 2006;65(4):150–156. | ||
Letourneau JE, Giroux R. Nongaussian distribution curve of heterophorias among children. Optom Vis Sci. 1991;68(2):132–137. | ||
Maples WC, Savoy RS, Harville BJ, Golden LR, Hoenes R. Comparison of distance and near heterophoria by two clinical methods. Optom Vis Dev. 2009;40(2):100–106. | ||
Mathebula SD, Sheni DDD, Oduntan AO. Distribution of heterophoria among primary school children of South Africa. S Afr Optom. 2002;61:48–54. | ||
Razavi ME, Poor SSH, Daneshyar A. Normative values for the fusional amplitudes and the prevalence of heterophoria in adults. Iran J Ophthalmol. 2010;22(3):41–46. | ||
Jackson DN, Bedell HE. Vertical heterophoria and susceptibility to visually induced motion sickness. Strabismus. 2012;20(1):17–23. | ||
Palomo Alvarez C, Puell MC, Sánchez-Ramos C, Villena C. Normal values of distance heterophoria and fusional vergence ranges and effects of age. Graefes Arch Clin Exp Ophthalmol. 2006;244(7):821–824. | ||
Walline JJ, Mutti DO, Zadnik K, Jones LA. Development of phoria in children. Optom Vis Sci. 1998;75(8):605–610. | ||
Godio LB, Rutstein RP. The range of zero-associated phoria in an asymptomatic clinical population. Am J Optom Physiol Opt. 1981;58(6):445–450. | ||
Pickwell LD, Kaye NA, Jenkins TC. Distance and near readings of associated heterophoria taken on 500 patients. Ophthalmic Physiol Opt. 1991;11(4):291–296. | ||
Risovic DJ, Misailovic KR, Eric-Marinkovic JM, Kosanovic-Jakovic NG, Milenkovic SM, Petrovic LZ. Refractive errors and binocular dysfunctions in a population of university students. Eur J Ophthalmol. 2008;18(1):1–6. | ||
Leone JF, Cornell E, Morgan IG, et al. Prevalence of heterophoria and associations with refractive error, heterotropia and ethnicity in Australian school children. Br J Ophthalmol. 2010;94(5):542–546. | ||
Lyle TK, Jackson S, Wybar KC. Lyle and Jackson’s Practical Orthoptic in the Treatment of Squint and Other Anomalies of Binocular Vision. 5th ed. London: Lewis; 1967. | ||
Gupta NC, Narang RK, Khurana AK, Parmar IP, Ahluwalia BK. Exophoria and refractive errors-evaluation of 250 cases. Indian J Ophthalmol. 1987;35(4):204–206. | ||
Junghans B, Kiely PM, Crewther DP, Crewther SG. Referral rates for a functional vision screening among a large cosmopolitan sample of Australian children. Ophthalmic Physiol Opt. 2002;22(1):10–25. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.