")
Back to Journals » Vascular Health and Risk Management » Volume 18
Direct Oral Anticoagulants for the Prevention and Acute Treatment of Cancer-Associated Thrombosis
Authors Attard LM, Gatt A , Bertoletti L , Delluc A, Riva N
Received 16 August 2022
Accepted for publication 5 October 2022
Published 13 October 2022 Volume 2022:18 Pages 793—807
DOI https://doi.org/10.2147/VHRM.S271411
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Video abstract presented by Laura M Attard.
Views: 161
Laura M Attard,1 Alex Gatt,2 Laurent Bertoletti,3– 5 Aurelien Delluc,6 Nicoletta Riva2
1Medical School, University of Malta, Msida, Malta; 2Department of Pathology, Faculty of Medicine and Surgery, University of Malta, Msida, Malta; 3Service de Médecine Vasculaire et Thérapeutique, CHU de St-Etienne, Saint-Etienne, France; 4INSERM, UMR1059, Université Jean-Monnet, Saint-Etienne, France; 5INNOVTE, CHU de Saint-Etienne, Saint-Etienne, France; 6Ottawa Hospital Research Institute, Department of Medicine, University of Ottawa, Ottawa, ON, Canada
Correspondence: Nicoletta Riva, Department of Pathology, Faculty of Medicine and Surgery, University of Malta, Msida, MSD 2080, Malta, Email [email protected]
Abstract: Cancer is a major risk factor for venous thromboembolism (VTE), and cancer-associated thrombosis (CAT) constitutes approximately 15– 25% of all VTE cases. For decades, the standard treatment for CAT used to be daily subcutaneous low molecular weight heparin (LMWH). Data on the safety and efficacy of the direct oral anticoagulants (DOACs) in this population emerged only in recent years and specific DOACs were included into recent guidelines recommendations. In this narrative review of the literature, we reported the results of the phase III randomized controlled trials that evaluated the DOACs for the prevention and the acute treatment of CAT. For the acute phase treatment, the anti-Xa inhibitors (apixaban, edoxaban, rivaroxaban) showed better efficacy than LMWH in preventing VTE recurrence; however, rivaroxaban and edoxaban were also associated with an increased risk of bleeding events. For primary prevention of CAT in ambulatory cancer patients starting chemotherapy, apixaban and rivaroxaban showed better efficacy than placebo but a trend towards higher bleeding rates. Recent guidelines suggest the DOACs for the treatment of CAT in selected cancer patients (eg, low bleeding risk, no luminal gastrointestinal or genitourinary malignancies, no interfering medications). The DOACs are also suggested for primary thromboprophylaxis in selected ambulatory cancer patients at high risk of VTE (eg, Khorana score ≥ 2 prior to starting new chemotherapy, low bleeding risk, no interfering medications).
Keywords: cancer, venous thromboembolism, apixaban, edoxaban, rivaroxaban
Introduction
Cancer is a major risk factor for venous thromboembolism (VTE), and cancer-associated thrombosis (CAT) constitutes approximately 15–25% of all VTE cases.1 Active cancer has been recently defined as cancer with ongoing treatment, evidence of treatment failure, or not receiving potentially curative treatment.2 Patients with active cancer have been shown to carry a significantly higher risk burden of recurrent VTE and bleeding, compared to patients with a history of cancer.3
For decades, the standard treatment for CAT used to be daily subcutaneous low molecular weight heparin (LMWH) for at least 6 months. However, recent guidelines have also included specific direct oral anticoagulants (DOACs) for this indication.4,5
The DOACs for VTE treatment were approved around 10 years ago; however, patients with active cancer were excluded from the initial large phase III randomized controlled trials (RCTs) that led to the marketing authorization of the DOACs. Thus, data on the safety and efficacy of the DOACs in this population emerged only in recent years.
We aimed to review the current evidence on the use of the DOACs in the prevention and the acute treatment (first months) of CAT.
The Direct Oral Anticoagulants
Pharmacological Properties
The DOACs are a group of oral anticoagulants that target specific coagulation factors, namely factor Xa (ie apixaban, edoxaban, rivaroxaban) or thrombin (ie dabigatran).6 The DOACs have a rapid onset of action, with peak plasma concentration levels reached within 2 hours from administration. They have relatively short half-lives, with trough plasma concentrations generally reached within 12–24 hours from the last administration.7 Different DOACs have different degrees of renal versus non-renal clearance (Table 1). They are all substrates of the transporter P-glycoprotein (P-gp), while apixaban and rivaroxaban also have hepatic metabolism via the cytochrome P450 (particularly CYP3A4).8 Thus, the concomitant administration of P-gp or CYP3A4 inhibitors may result in increased DOAC plasma concentrations, while the concomitant administration of P-gp or CYP3A4 inducers may result in reduced plasma concentrations.9 Advantages and disadvantages of the DOACs compared to vitamin K antagonists (VKAs) and LWMH are summarised in Figure 1.
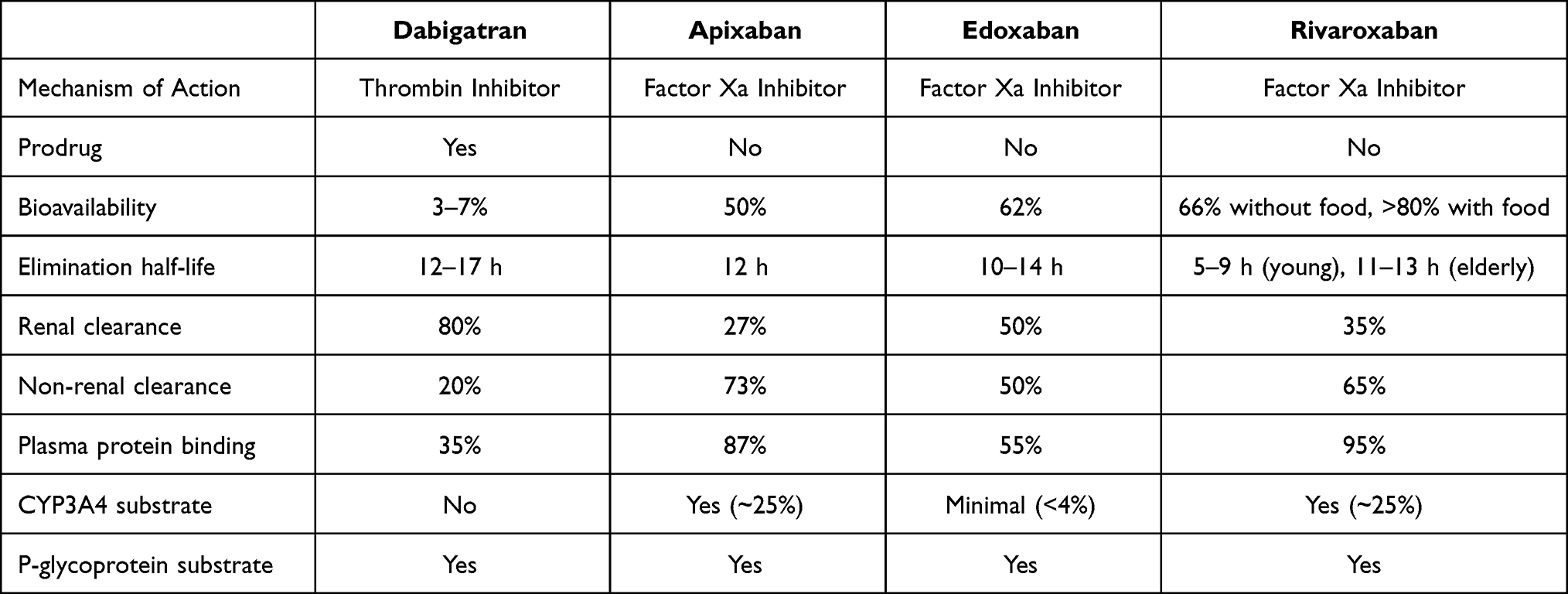 |
Table 1 Pharmacological Properties of the Direct Oral Anticoagulants |
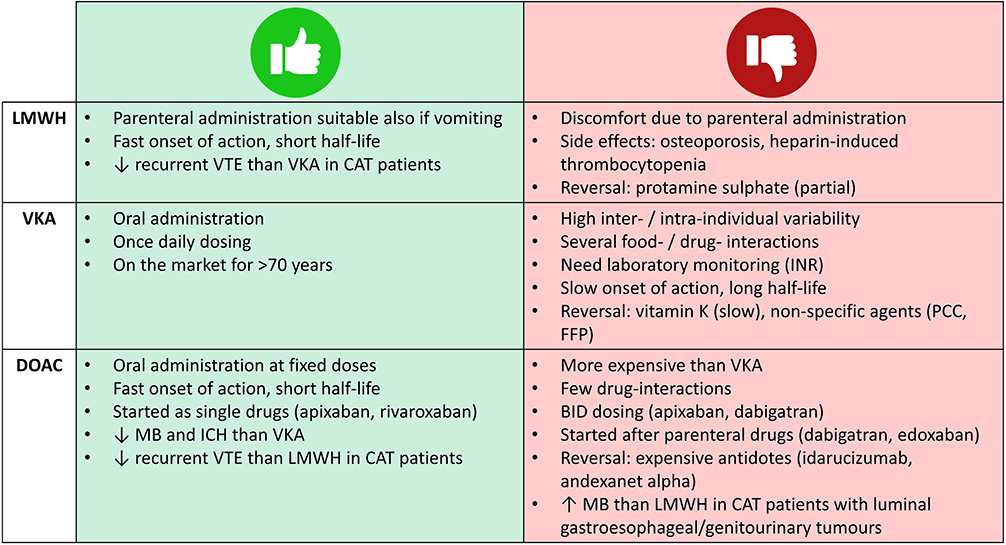 |
Figure 1 Pros and cons of different anticoagulant drugs in cancer patients. Abbreviations: BID, twice daily; CAT, cancer-associated thrombosis; DOAC, direct oral anticoagulant; FFP, fresh frozen plasma; ICH, intracranial haemorrhage; INR, international normalised ratio; LMWH, low molecular weight heparin; MB, major bleeding; PCC, prothrombin complex concentrates; VKA, vitamin K antagonist; VTE, venous thromboembolism. |
Of note, cancer patients might have comorbidities which contraindicates the use of the DOACs. Due to their high degree of renal clearance, the DOACs should not be used in patients with end-stage chronic kidney disease (creatinine clearance < 15 ml/min) or on dialysis; apixaban, edoxaban and rivaroxaban can be used with caution in patients with severe renal impairment (creatinine clearance 15–30 ml/min), while dabigatran is contraindicated also in this category.8 The DOACs should not be used in patients with severe hepatic impairment (Child-Pugh class C), and rivaroxaban also in moderate hepatic impairment (Child-Pugh class B), due to its higher hepatic clearance.8 Finally, since the DOACs can cross the placenta and are excreted into breastmilk, they are contraindicated in pregnant and lactating women.10
Efficacy and Safety Profile Outside Active Cancer
The DOACs have already been studied in several RCTs for the prevention and treatment of lower extremities deep vein thrombosis (DVT) and pulmonary embolism (PE), both in the acute phase and secondary prevention: AMPLIFY and AMPLIFY-EXT;11,12 Hokusai-VTE;13 EINSTEIN-DVT, EINSTEIN-PE, EINSTEIN-Extension and EINSTEIN-CHOICE;14–16 RE-COVER, RE-COVER II, RE-MEDY and RE-SONATE17–19 trials.
However, patients with active malignancy were excluded or poorly represented in these RCTs (for instance, in the EINSTEIN trials only approximately 5% of patients had active cancer at randomization).14,15 Taken together, these studies showed that the DOACs, outside active cancer, are as effective as VKAs, with a better safety profile. In fact, the DOACs were associated with a reduction in the risk of major bleeding (MB), intracranial bleeding and fatal bleeding.20
The DOACs were also evaluated in the paediatric population (EINSTEIN-Jr21 and DIVERSITY22 trials). Compared to the standard of care in paediatrics (mainly LMWH, eventually switched to VKAs in 34–54% of cases), the DOACs showed a similar safety and efficacy profile.23 However, only approximately 10% of the patients enrolled in these trials had active cancer or a history of cancer.
Cancer-Associated Thrombosis
Epidemiology of Cancer-Associated Thrombosis
Cancer is a strong risk factor for VTE. The risk of VTE in cancer patients is 4–7 times higher than that of non-cancer patients.24,25 VTE can also be the first clinical manifestation of occult malignancy; in fact, around 4% of patients have a malignancy discovered within 1 month after VTE diagnosis and around 6% within 1 year.26
The development of VTE in cancer patients is associated with a reduction in overall survival rate and is associated with a 2-time increased risk of death.27 The clinical course of VTE is more aggressive in cancer patients, with fatal PE being 3-times more common in cancer patients compared to non-cancer patients.28 Cancer patients have a 3.2-fold higher risk of recurrent VTE and a 2.2-fold higher risk of MB during anticoagulant treatment compared to patients without cancer.29 The risk of recurrent VTE is 2.8-fold higher in patients with locally advanced cancer and 3.3-fold higher in patients with metastatic cancer, compared to patients with localised cancer.30 The VTE risk is greater in non-ambulatory compared to ambulatory cancer patients.31 Certain types of cancer have a higher incidence of VTE (such as pancreatic, cerebral, gastric and ovarian cancers), while others have a relatively lower incidence (such as prostatic, breast cancer and melanoma).32 Differences have also been reported in the rates of VTE recurrence and MB during anticoagulant treatment. For instance, in patients with lung cancer, the rates of VTE recurrence are approximately 2 times higher than MB, while in patients with prostate cancer the rates of MB are approximately 2 times higher than VTE recurrence.33 Several bleeding risk scores have been applied to cancer patients, however their predictive performance was poor.34
In oncological patients, VTE is frequently incidentally detected. For instance, incidental PE is found in 3.36% of cancer patients undergoing computed tomography for tumour staging.35 A recent meta-analysis highlighted that incidental VTE in cancer patients is associated with lower rates of VTE recurrence and a trend towards higher rates of MB, compared to symptomatic VTE.36
Cancer is an independent predictor of non-leg DVT.37 Oncological patients have a 43-fold increased risk of upper extremity DVT compared to patients without malignancy.38 Upper extremity DVT is particularly common in the presence of indwelling central venous catheters, which are commonly used for intravenous chemotherapy, nutrition or antibiotics. However, cancer patients without central venous catheters still have an 18-fold increased risk of upper extremity DVT compared to patients without malignancy.38
Cancer is a frequent risk factor also for splanchnic vein thrombosis.39 In a large prospective cohort study of patients with splanchnic vein thrombosis, solid cancer was found in 22.7% and myeloproliferative neoplasms in 8.2% of patients.40 In addition, the prevalence of solid cancer was higher in patients with incidentally detected compared to symptomatic splanchnic vein thrombosis (35% vs 18%, p<0.0001).41 A study comparing cancer-associated splanchnic vein thrombosis versus usual site VTE noted that the most common locations of cancer were hepatobiliary and pancreatic in the former and gastrointestinal in the latter.42
Cerebral vein thrombosis can also be the first clinical manifestation of solid cancers, especially brain tumours,43 or myeloproliferative neoplasms. The presence of the Janus Kinase 2 (JAK2) V617F mutation, commonly found in myeloproliferative neoplasms, has been reported in 6.6% of patients with cerebral vein thrombosis.44
Biological Mechanisms and Cancer-Specific Risk Factors
From a pathophysiological point of view, CAT is a multifactorial disorder. Several procoagulant mechanisms have been described, such as direct activation of coagulation, inhibition of fibrinolysis, cancer-induced platelet aggregation and inflammatory response.45 Cancer can act on the three elements of the Virchow triad: blood stasis can be due to extrinsic compression by the tumoral mass on the blood vessels; hypercoagulability can be due to the production of inflammatory cytokines and procoagulant molecules; endothelial injury can be due to direct vessel invasion by the tumoral mass.46
In addition, cancer can coexist with other VTE risk factors (such as immobilization, indwelling central venous catheters, chemotherapy, radiotherapy, surgery). Chemotherapy with its different types (eg, adjuvant, antiangiogenic, immunomodulatory, hormonal, or erythropoiesis-stimulating drugs) is an independent risk factor for VTE.47 Cancer patients receiving chemotherapy have a 6.5-fold increased risk of VTE compared to the general population.24
Treatment of CAT: Acute Phase
The standard treatment for CAT was based on evidence from RCTs comparing LMWHs to VKAs. In the CANTHENOX trial, enoxaparin (1.5 mg/kg/daily) was associated with a non-significant reduction of MB events (7.0% vs 16.0%, p=0.09) and similar rates of recurrent VTE (2.8% vs 4.0%), compared to VKA during a 3-month follow-up.48 In the CLOT trial, dalteparin (200 IU/kg/daily for 1 month, then 150 IU/kg/daily) was associated with a 52% reduction of recurrent VTE (9% vs 17%; hazard ratio [HR] 0.48, 95% CI 0.30–0.77) and similar rates of MB (6% vs 4%, p=0.27), compared to VKA during a 6-month follow-up.49 In the ONCENOX trial, after an initial treatment with enoxaparin 1.0 mg/kg twice daily (BID), patients received either enoxaparin 1.0 mg/kg/daily or enoxaparin 1.5 mg/kg/daily or warfarin for 6 months.50 Numerically less patients in the enoxaparin groups experienced recurrent VTE during treatment compared to VKA (6.9% and 6.3% vs 10.0%, respectively). MB events occurred in 6.5% of patients in the enoxaparin 1.0 mg/kg/daily, 11.1% in the enoxaparin 1.5 mg/kg/daily and 2.9% in the VKA group.50 Finally, in the CATCH trial, tinzaparin 175 IU/kg/daily was associated with non-significantly lower 6-month incidence of VTE recurrence (7.2% vs 10.5%; HR 0.65, 95% CI 0.41–1.03), and similar rates of MB (2.7% vs 2.4%; HR 0.89, 95% CI 0.40–1.99) compared to VKA.51
Until recently, LMWH was the mainstay treatment for CAT, since it has been shown to be more effective than VKAs in preventing recurrent VTE, and as safe as VKA in terms of MB. In particular, the CLOT trial49 is considered a milestone for CAT treatment and most of the RCTs evaluating the DOACs used the same dalteparin regimen as comparison.
Treatment of CAT: Secondary Prevention
It is still debated what is the optimal anticoagulant treatment duration in cancer patients in order to prevent recurrent VTE, since there are no published RCTs after the initial acute phase. The highest incidence of recurrent VTE is reported in the first 6 months after the index event, thus the majority of cancer patients are treated for at least 6 months.52 However, cancer patients with certain risk factors (such as metastatic disease, pancreatic or lung cancer, residual vein occlusion) are at particularly high risk of recurrence if anticoagulation is stopped after 6 months.53 A recent systematic review highlighted that VTE recurrence remains high after 6 months (up to 12%), while major bleeding rates are relatively low (2–5%).54
Thus, guidelines suggest that patients with active cancer or high risk of recurrent VTE should receive extended treatment (beyond 6 months), if no major contraindications (eg, active bleeding, severe thrombocytopenia).4 Whether a reduced dose of anticoagulants for the extended treatment phase might be applied to cancer patient is still debated. The results of ongoing RCTs (API-CAT55 and EVE56) will help to elucidate this point.
Primary Prevention in Ambulatory Patients
Given the strong association between cancer and VTE, it is discussed whether oncological patients should receive any type of thromboprophylaxis to prevent thrombosis from happening in the first place. For the majority of cancers, primary thromboprophylaxis is not routinely recommended by clinical practice guidelines4 because the absolute reduction of VTE risk is modest, it increases the bleeding risk, and is associated with higher costs and inconvenience. A recently updated Cochrane review reported that thromboprophylaxis with LMWH in ambulatory cancer patients receiving chemotherapy decreases the incidence of symptomatic VTE (RR 0.62, 95% CI 0.46–0.83; high-certainty evidence) but increases the risk of MB (RR 1.63, 95% CI 1.12–2.35; moderate-certainty evidence), compared to no thromboprophylaxis.57
Several predictive models for the risk of CAT in ambulatory cancer patients have been developed. The Khorana risk score58 includes the site of cancer (2 points for tumours at very high risk of VTE, such as stomach or pancreas; 1 point for tumours at high risk, such as lung, lymphoma, gynaecological, bladder or testicular); the pre-chemotherapy platelet count (1 point if ≥350 x 109/L); the haemoglobin level (1 point if < 100 g/L or use of red cell growth factors); the pre-chemotherapy leukocytes count (1 point if >11.0 × 109/L); the body mass index (1 point if ≥ 35kg/m2). The score was originally divided into three categories: low risk (0 points), intermediate risk (1–2 points), and high risk (3–6 points) of VTE.58
Two evolutions of the Khorana score have been proposed. Apart from the five predictive variables of the original Khorana score, the Vienna Cancer and Thrombosis Study (CATS) score included elevated levels of sP-selectin (1 point if ≥ 53.1 ng/mL) and elevated levels of D-dimer (1 point if ≥ 1.44 μg/mL) at baseline;59 while the Protecht score included details of the anticancer treatment (1 point if cisplatin/carboplatin-based chemotherapy or gemcitabine, 2 points if both).31 Another score has been proposed to predict VTE after the initiation of anticancer treatment: the COMPASS-CAT includes details of cancer-related risk factors (eg, specific anticancer treatment, time since cancer diagnosis, presence of central venous catheter, stage of cancer), predisposing risk factors (eg, cardiovascular risk factors, recent hospitalisation, personal history of VTE) and biomarkers (eg, platelet count).60
The performance of these prediction scores has been recently questioned.61 A systematic review and meta-analysis reported that the incidence of CAT, using the Khorana score, was 5.0% in the low-risk score, 6.6% in the intermediate-risk score and 11.0% in the high-risk score patients,62 suggesting that a relevant number of VTE events still occur in the low- and intermediate-risk groups. These findings contribute to the uncertainties regarding which ambulatory cancer patients should receive primary thromboprophylaxis.
Direct Oral Anticoagulants for the Acute Treatment of Cancer-Associated Thrombosis
Recent phase III RCTs specifically focused on VTE treatment in cancer patients by comparing the DOACs to the standard treatment with LMWH (Table 2). All these trials had an open-label design with blinded endpoint adjudication. Up to date, there are no RCTs evaluating dabigatran, specifically in patients with VTE and active cancer.
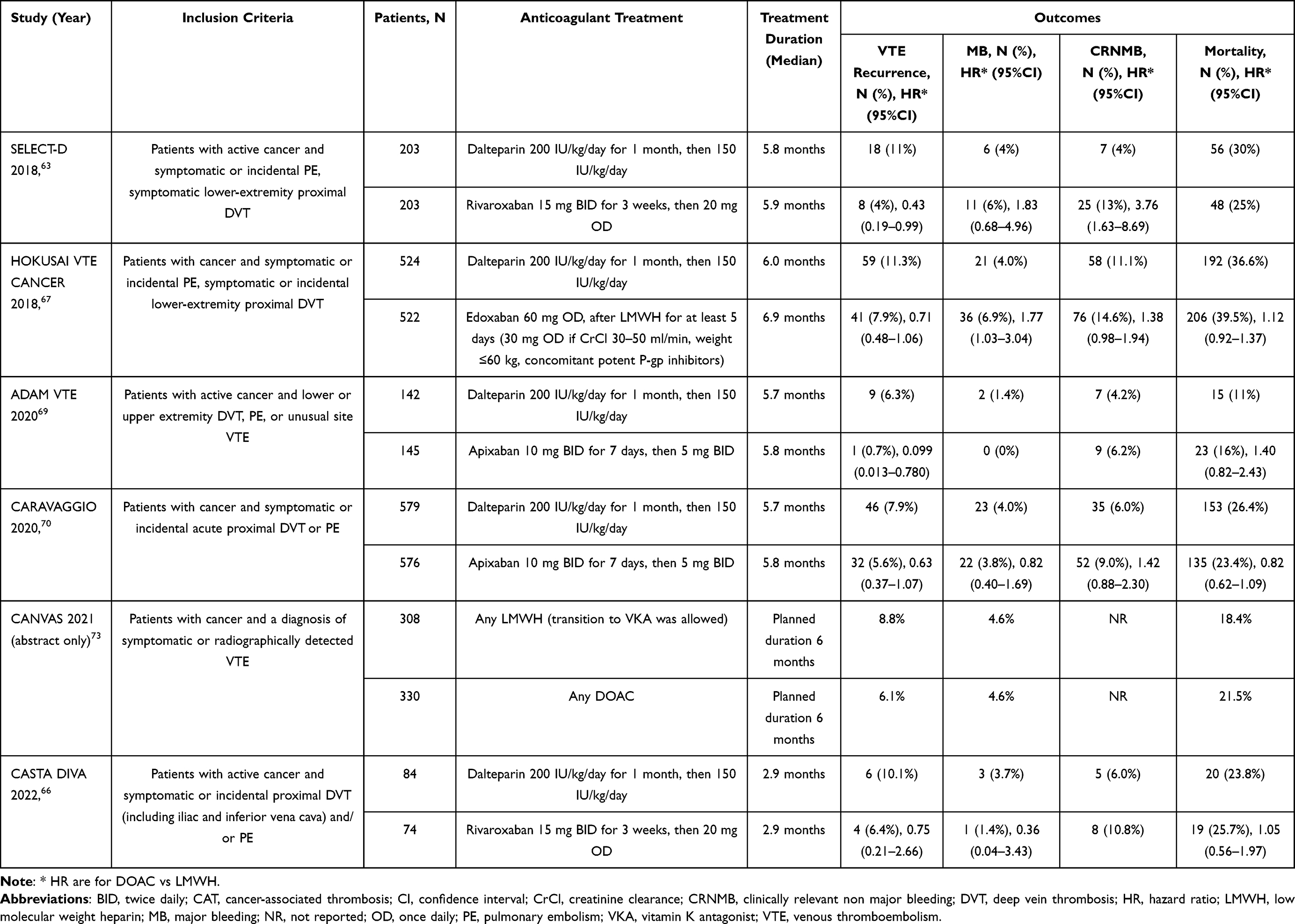 |
Table 2 Randomized Controlled Trials Evaluating the Use of the Direct Oral Anticoagulants for the Acute Treatment of Cancer-Associated Thrombosis |
Rivaroxaban
In the SELECT-D pilot trial,63 406 patients with active cancer and VTE were randomly assigned to rivaroxaban (15 mg BID for 3 weeks, then 20 mg once daily [OD]), or to dalteparin (200 IU/kg/day for the first month, then 150 IU/kg/day). This pilot trial was planned as a feasibility study, without a priori statistical calculation of the sample size. At 6 months follow-up, rivaroxaban showed a reduction in the primary outcome of recurrent VTE (4% vs 11%; HR 0.43, 95% CI 0.19–0.99). Regarding the safety outcomes, it was associated with non-significantly higher rates of MB (6% vs 4%; HR 1.83, 95% CI 0.68–4.96), but significantly higher rates of clinically relevant non-major bleeding (CRNMB) (13% vs 4%; HR 3.76, 95% CI 1.63–8.69) compared to dalteparin.
An interim safety analysis highlighted that the administration of rivaroxaban in patients with oesophageal or gastroesophageal cancers was associated with a trend towards higher rates of MB, thus these types of cancers were excluded from the remaining period of enrolment.63 Upper gastrointestinal bleeding events have been commonly reported in patients on rivaroxaban.64 Possible mechanisms include the high peak level obtained with the OD administration and the incomplete absorption of rivaroxaban, which is administered in its active form, leading to high local anticoagulant effect.65
In the CASTA DIVA pilot trial,66 158 patients with active cancer and a newly diagnosed symptomatic or incidental proximal DVT and/or PE were randomized to rivaroxaban or dalteparin (at the same dosages reported above) for 3 months. Rivaroxaban was associated with a non-significant 25% risk reduction of the primary outcome recurrent VTE, compared to dalteparin (6.4% vs 10.1%, respectively; subdistribution HR 0.75, 95% CI 0.21–2.66; p for non-inferiority = 0.13). MB or CRNMB occurred in 12.2% of patients in the rivaroxaban group vs 9.8% in the dalteparin group (subdistribution HR 1.27, 95% CI 0.49–3.26). This trial was interrupted prematurely due to slower than anticipated recruitment rates, thus the predefined non-inferiority criterion for the primary efficacy outcome was not reached. However, the safety and efficacy profile of rivaroxaban was consistent with previous data.
Edoxaban
In the Hokusai VTE Cancer trial,67 1050 patients with active cancer and acute symptomatic or incidental VTE were randomly assigned to edoxaban (60 mg OD) after at least 5 days of LMWH or to dalteparin (200 IU/kg/day for the first month, then 150 IU/kg/day) for at least 6 months, and up to 12 months at the discretion of the treating physicians. A lower dose of edoxaban (30 mg OD) was used in patients with reduced creatinine clearance (30–50 ml/min), low body weight (≤60 kg), or receiving concomitant treatment with strong P-gp inhibitors. The primary outcome was a composite of recurrent VTE and MB, and occurred in 12.8% of patients in the edoxaban group vs 13.5% in the dalteparin group (HR 0.97, 95% CI 0.70–1.36; p=0.006 for non-inferiority; p=0.87 for superiority). When considering the efficacy and safety outcomes separately, edoxaban was associated with non-significantly lower rates of recurrent VTE (HR 0.71, 95% CI 0.48–1.06), but higher rates of MB (HR 1.77, 95% CI 1.03–3.04) compared to dalteparin. However, median treatment duration was 6.0 months in the dalteparin group vs 6.9 months in the edoxaban group (p=0.01). Subgroup analyses by types of cancer showed that only in patients with gastrointestinal cancer edoxaban was associated with a higher risk of MB than dalteparin (12.7% vs 3.6%; risk difference 9.2%, 95% CI 3.2–15.1),68 and that more than 90% of these events were gastrointestinal bleeding.
Apixaban
In the ADAM-VTE trial,69 300 patients with CAT were randomized to apixaban (10 mg BID for 7 days, then 5 mg BID) or to dalteparin (200 IU/kg/day for the first month, then 150 IU/kg/day) up to 6 months. The primary outcome MB occurred in 0% of patients assigned to apixaban vs 1.4% in patients assigned to dalteparin (the HR could not be calculated because of zero events in the apixaban group). Amongst the secondary outcomes, recurrent VTE occurred less frequently in apixaban compared to dalteparin patients (0.7% vs 6.3%; HR 0.099, 95% CI 0.013–0.780). However, MB rates were lower than expected in both treatment groups and this trial did not meet its predefined primary outcome. The low MB rates can be partly explained by the low proportion of patients with upper gastrointestinal malignancy enrolled in this trial (3.7%), and partly by the less severe population, since mortality rates were lower (11–16%) compared to the other CAT trials. The ADAM-VTE trial also evaluated the quality of life of anticoagulated patients and showed that patients on apixaban had lower overall burden and lower negative impact on their quality of life, and higher overall satisfaction with the anticoagulant treatment.
In the CARAVAGGIO trial,70 1170 patients with cancer and symptomatic or incidental acute proximal DVT or PE were randomized to apixaban or dalteparin (at the same dosages reported above) for 6 months. Apixaban was non-inferior to dalteparin in the primary outcome of recurrent VTE, which occurred in 5.6% vs 7.9% of patients, respectively (HR 0.63, 95% CI 0.37–1.07; p<0.001 for non-inferiority; p=0.09 for superiority). The rates of MB events were comparable in the two groups (HR 0.82, 95% CI 0.40–1.69).70 The rates of MB were also similar in the subgroup of patients with gastrointestinal cancer.71
A sub-analysis of the CARAVAGGIO trial evaluating the concomitant use of anticancer drugs showed that CYP3A4/P-gp inducers/inhibitors had no effect on the clinical outcomes, which occurred at similar rates in both the apixaban and dalteparin groups.9 Another sub-analysis evaluating the impact of renal function on clinical outcomes showed that the presence of renal impairment was associated with similar rates of MB in the two groups and that in patients with moderate renal impairment (defined as creatinine clearance 30–59 ml/min) apixaban was actually associated with lower rates of recurrent VTE than dalteparin (HR 0.27, 95% CI 0.08–0.96).72
Pooled Results
The CANVAS, currently published only in abstract form, was a pragmatic trial that enrolled cancer patients with a recent diagnosis of VTE treated with any DOAC or LMWH, and included a randomized and a preference cohort. In the randomized cohort, the DOACs showed similar risk of recurrent VTE (6.1% vs 8.8%; difference −2.7%, 90% CI −6.1 to 0.7%) and MB (4.6% vs 4.6%; difference 0%, 90% CI −2.7 to 2.7%) compared to LMWH at 6-month follow-up.73
Overall, these RCTs63,66,67,69,70,73 provided evidence on the safety and efficacy profile of the DOACs for the treatment of acute VTE in cancer patients. Their study design is comparable and most of them used dalteparin as comparison. Of note, the majority of these trials were pilot studies, while the Hokusai VTE cancer and CARAVAGGIO trials were dedicated phase III RCTs. In general, in all trials most patients had PE as the index event; the most common types of tumours were colorectal, lung and breast cancers, whilst metastatic disease was present in more than half of the recruited patients (53–76%). However, other populations were poorly represented, such as patients with brain tumours (<5% of all cancers). The rates of MB in the dalteparin group were similar in the SELECT-D, CASTA DIVA, Hokusai VTE cancer and CARAVAGGIO trials (~4%), while they were very low in the ADAM VTE trial (~1%), a finding that can be partly explained by differences in the enrolled population (eg, lower prevalence of patients with upper gastrointestinal malignancy). Whether the results of these RCTs can be generalised to the whole population of cancer patients is a matter of debate, since a recent study highlighted that >50% of patients evaluated in real-life clinical practice for acute CAT would have not been eligible for a RCT.74
A systematic review and meta-analysis based on the results of these six RCTs (for a total of 3690 CAT patients) was recently published.75 Compared to LMWH, the DOACs were associated with a 33% lower risk of recurrent VTE (RR 0.67, 95% CI 0.52–0.85), and a 66% higher risk of CRNMB (RR 1.66, 95% CI 1.31–2.09). There was also a non-significant 17% higher risk of MB (RR 1.17, 95% CI 0.82–1.67). Thus, the DOACs emerged as promising alternative to LMWH for the treatment of CAT, but caution should be exerted for patients at higher risk of bleeding, such as those with gastrointestinal or urothelial malignancies. Possible hypotheses have been raised to explain the higher bleeding tendency with the DOACs compared to LMWH, such as the local anticoagulant effect of the DOACs at the gastrointestinal absorption site, the lack of antithrombin which is necessary for LMWH activity in the gastrointestinal and genitourinary mucosae, or a possible greater anticoagulant potency of the DOACs.52 Despite the unavailability of head-to-head comparisons, apixaban seemed to be the DOAC associated with the lowest bleeding risk.76
Direct Oral Anticoagulants for the Prevention of Cancer-Associated Thrombosis
Two recent phase III double-blind RCTs evaluated the anti-Xa inhibitors for CAT prevention in ambulatory cancer patients (Table 3). These RCTs were placebo-controlled because current guidelines do not recommend routine thromboprophylaxis for cancer patients.4
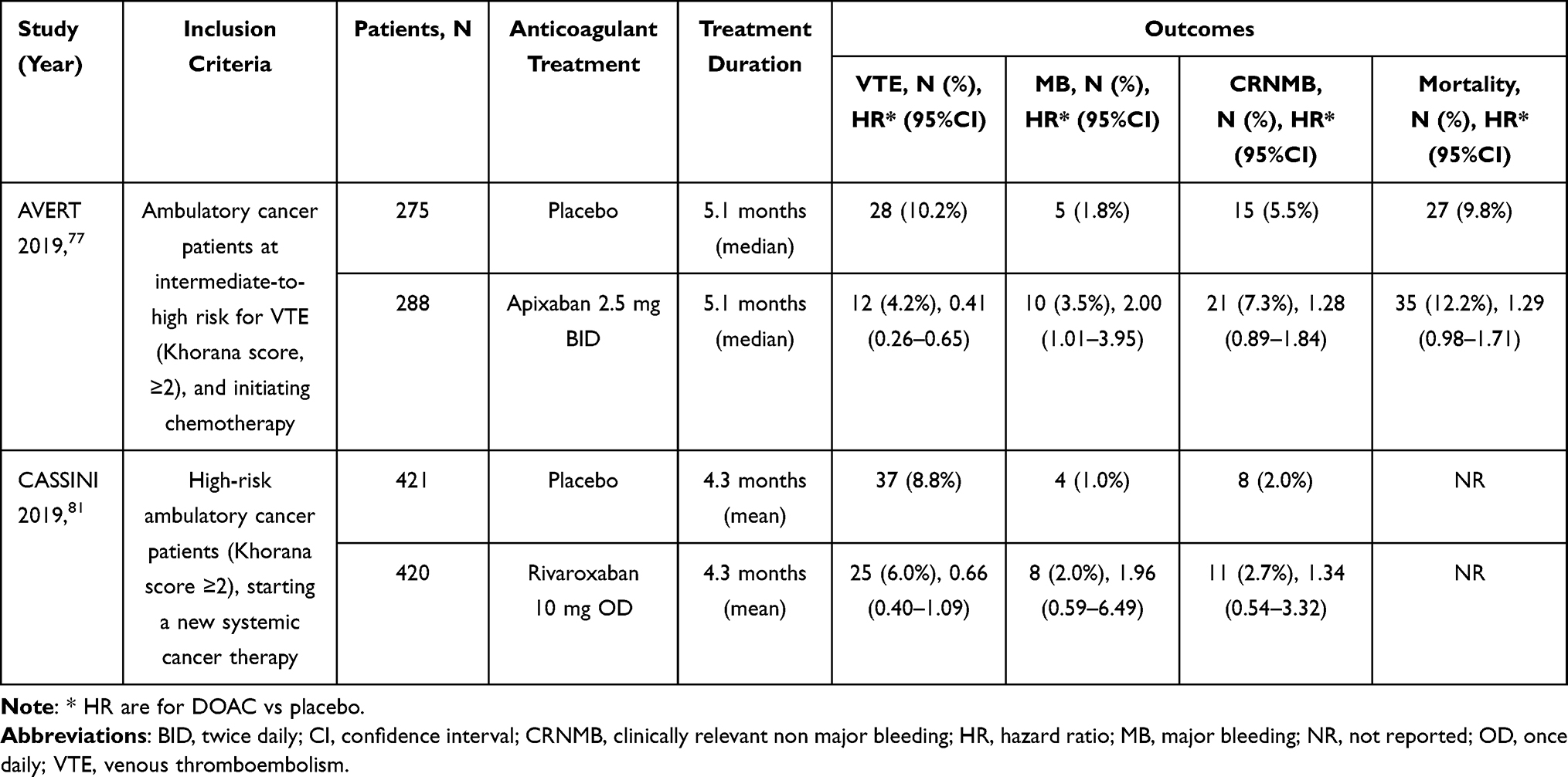 |
Table 3 Randomized Controlled Trials Evaluating the Use of the Direct Oral Anticoagulants for the Prevention of Cancer-Associated Thrombosis in Ambulatory Patients |
Apixaban
In the AVERT trial,77 574 ambulatory cancer patients at intermediate-high risk of VTE (defined as Khorana score ≥ 2) starting chemotherapy, were randomized to apixaban (2.5 mg BID) or placebo for 6 months. Apixaban was associated with a 59% reduction of the primary outcome of objectively diagnosed VTE compared to placebo (4.2% vs 10.2%; HR 0.41, 95% CI 0.26–0.65, p<0.001). However, it was also associated with a significant increase in MB rates (3.5% vs 1.8%; HR 2.00, 95% CI 1.01–3.95; p=0.046).77 None of the MB happened in patients with upper gastrointestinal or colorectal tumours.78 Sub-analyses of the AVERT trial confirmed the superior efficacy of apixaban also in cancer patients with a central venous catheter79 and in those with metastatic disease.80
Rivaroxaban
In the CASSINI trial81 841 high-risk ambulatory cancer patients (defined as Khorana score ≥ 2), without DVT on ultrasound at screening and starting on a new cancer therapy, were randomized to rivaroxaban (10 mg OD) or placebo for 6 months. Rivaroxaban was associated with a non-significant reduction in the risk of the primary efficacy endpoint (a composite of proximal lower extremity DVT, PE, symptomatic upper extremity DVT or distal lower extremity DVT, VTE-related death), which occurred in 6.0% of patients in the rivaroxaban group and 8.8% in the placebo group (HR 0.66, 95% CI 0.40–1.09, p=0.10). There was also a non-significant increase in the risk of the primary safety endpoint of MB, which occurred in 2.0% vs 1.0%, respectively (HR 1.96, 95% CI 0.59–6.49, p=0.26). Sub-analyses of the CASSINI trial reported similar results in patients with pancreatic cancer82 and with gastric/gastroesophageal junction cancer.83
Pooled Results
A systematic review and meta-analysis based on the results of these two RCTs (for a total of 1415 ambulatory cancer patients)84 reported that the DOACs were associated with a 44% lower risk of VTE (RR 0.56, 95% CI 0.35–0.89) compared to placebo. However, there was a non-significant 96% higher risk of MB events on treatment (RR 1.96, 95% CI 0.80–4.82) and 28% higher risk of CRNMB (RR 1.28, 95% CI 0.74–2.20). A subgroup analysis showed that patients with the highest risk of VTE showed a greater absolute VTE risk reduction (−6.08% if Khorana score ≥ 3) compared to those at intermediate risk (−3.31% if Khorana score = 2).
Current Guidelines on the Prevention and Treatment of Cancer-Associated Thrombosis
Guidelines addressing the role of the DOACs for CAT prevention and treatment are summarised in Tables 4–5.
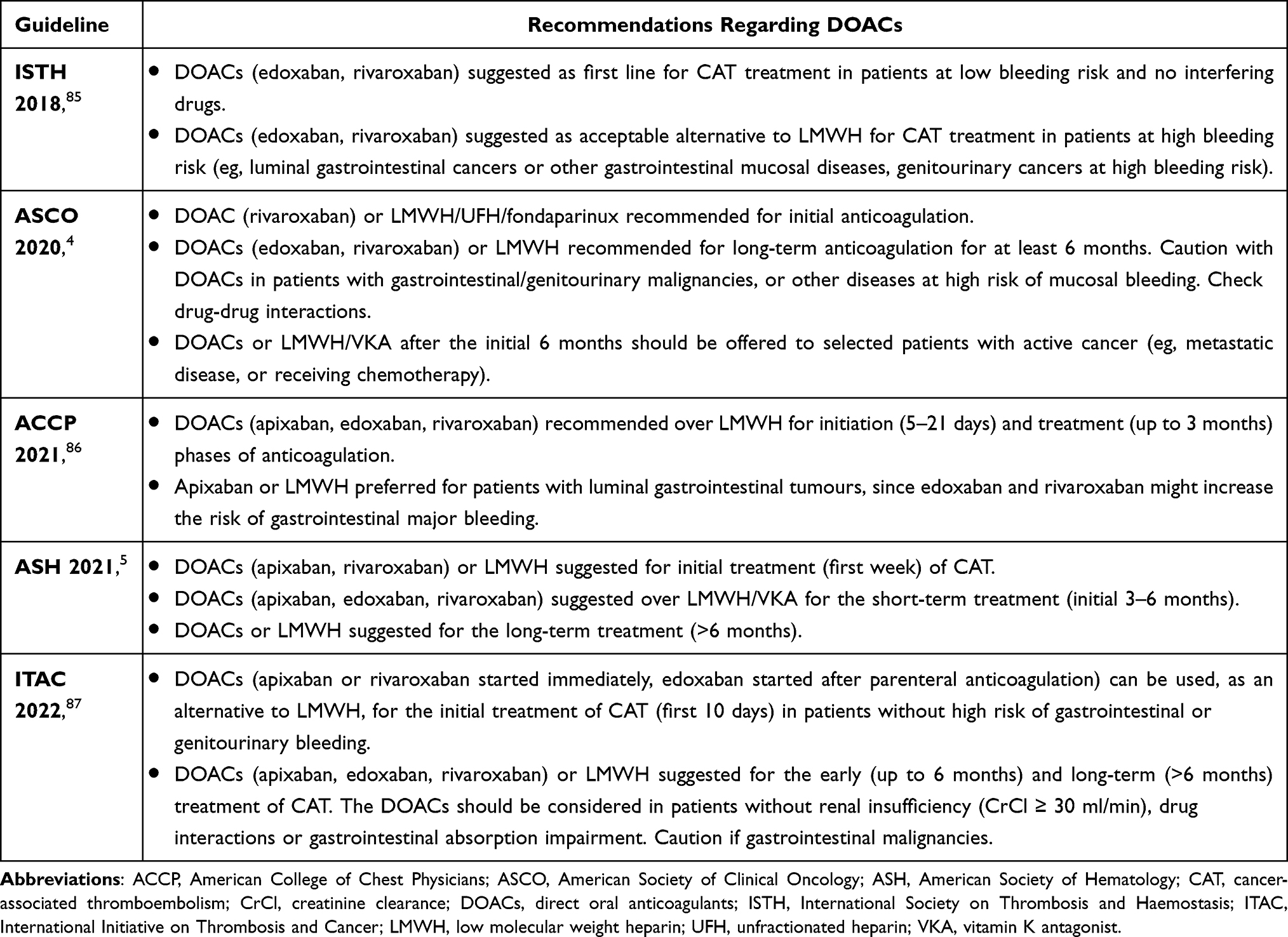 |
Table 4 Role of the Direct Oral Anticoagulants in the Acute Treatment of Cancer-Associated Thrombosis in Recent Guidelines |
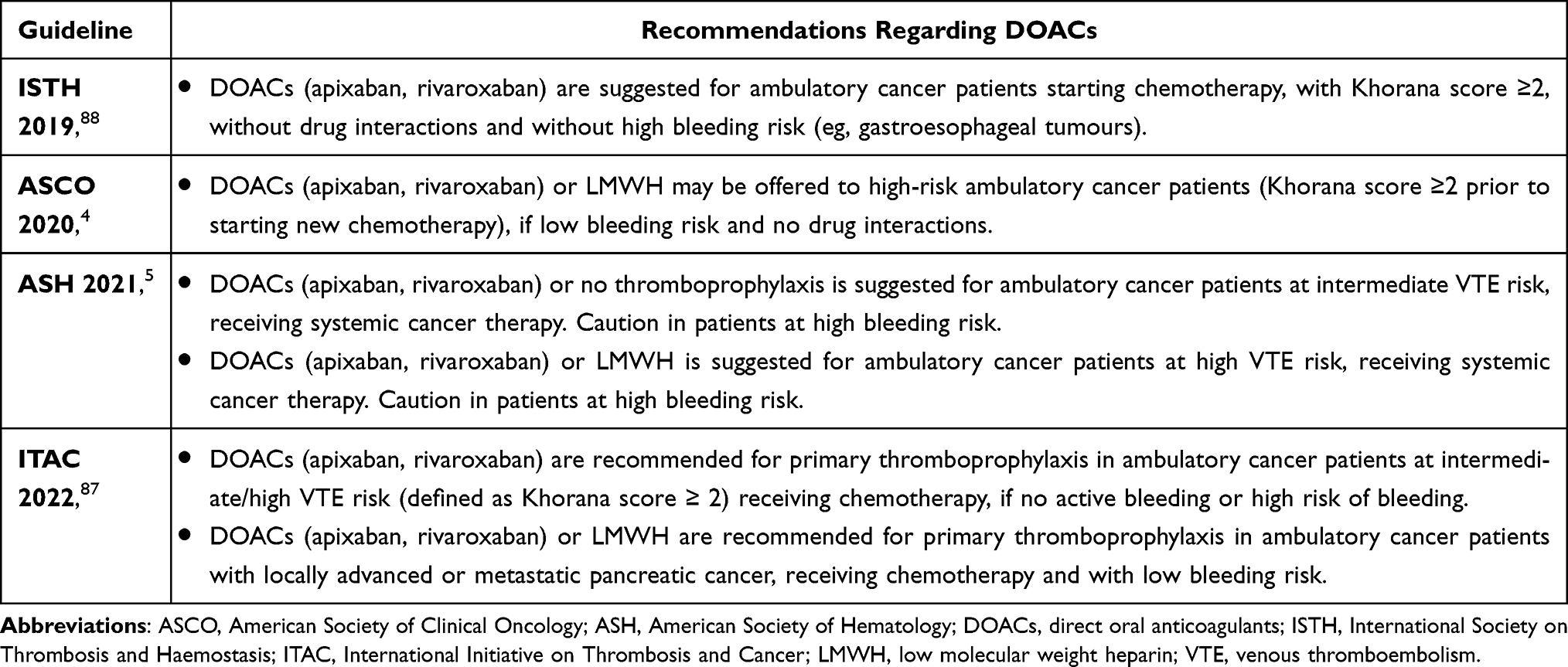 |
Table 5 Role of the Direct Oral Anticoagulants in the Prevention of Cancer-Associated Thrombosis in Ambulatory Patients in Recent Guidelines |
CAT Treatment
A 2018 guidance from the International Society on Thrombosis and Haemostasis (ISTH)85 recommended individualised treatment for cancer patients with VTE, using a shared decision-making approach and considering also patient preferences and values. Specific DOACs (namely edoxaban and rivaroxaban which were the only ones with available evidence at that time) were suggested as first line for CAT treatment in patients at low bleeding risk and no interfering drugs, while LMWH was considered as an acceptable alternative. LMWH was suggested as first line for CAT treatment in patients at high bleeding risk (eg, luminal gastrointestinal cancers or other gastrointestinal mucosal diseases, genitourinary cancers at high bleeding risk), and DOACs were considered as an acceptable alternative.
The 2020 clinical practice guidelines of the American Society of Clinical Oncology (ASCO)4 recommended LMWH, UFH, fondaparinux or rivaroxaban for initial anticoagulation of CAT. For long-term anticoagulation, the recommended options included LMWH, edoxaban or rivaroxaban for at least 6 months. Due to the lower efficacy, VKA can be used as alternative when LMWH or DOACs are not available. The DOACs should be used with caution in patients with gastrointestinal/genitourinary malignancies or other diseases at high risk of mucosal bleeding, and potential drug–drug interactions should be considered before starting a DOAC. After the initial 6 months, LMWH, DOACs or VKAs should be offered to selected patients with active cancer (eg, metastatic disease or receiving chemotherapy) and reassessed periodically.
The 2021 update of the American College of Chest Physicians guidelines86 recommended to treat CAT with an oral factor Xa inhibitors (apixaban, edoxaban, rivaroxaban) over LMWH for the initiation phase of anticoagulation (initial 5–21 days of treatment) and the treatment phase (up to 3 months). A particular situation is represented by patients with luminal gastrointestinal cancer, for whom apixaban or LMWH may be preferred, since edoxaban and rivaroxaban might increase the risk of gastrointestinal MB.
The 2021 guidelines of the American Society of Hematology (ASH)5 suggested DOACs (apixaban or rivaroxaban, since they are the only DOACs which can be started directly as a single-drug approach) or LMWH for the initial treatment (first week) of CAT. For the short-term treatment (initial 3–6 months), they suggested DOACs (apixaban, edoxaban, or rivaroxaban) over LMWH or VKA. If a DOAC cannot be used, they suggested LMWH over VKA. For the long-term treatment (>6 months), they suggested DOACs or LMWH.
The 2022 clinical practice guidelines from the International Initiative on Thrombosis and Cancer (ITAC)87 recommended LMWH for the initial treatment of CAT (first 10 days). The DOACs (apixaban or rivaroxaban started immediately, edoxaban started after parenteral anticoagulation with LMWH) were proposed as alternatives for patients without high risk of gastrointestinal or genitourinary bleeding. Other alternatives included UFH or fondaparinux. For the early (up to 6 months) and long-term (>6 months) treatment of CAT, they suggested LMWH or DOACs (apixaban, edoxaban, rivaroxaban) for a minimum of 6 months. The DOACs should be considered in cancer patients without renal insufficiency (CrCl ≥ 30 ml/min), drug interactions or gastrointestinal absorption impairment; furthermore, caution should be exerted in patients with gastrointestinal malignancies.
CAT Prevention in Ambulatory Patients
A 2019 ISTH guidance88 suggested DOACs (apixaban or rivaroxaban) for primary thromboprophylaxis for a specific category of ambulatory cancer patients (ie those with Khorana score ≥ 2, starting chemotherapy, without interfering medications and without high risk of bleeding), while LMWH was suggested for patients with drug interactions or high risk of gastrointestinal bleeding.
The 2020 ASCO clinical practice guidelines4 discouraged routine pharmacological thromboprophylaxis in ambulatory cancer patients undergoing chemotherapy. They stated that thromboprophylaxis with DOACs (apixaban or rivaroxaban) or LMWH may be considered in patients at high risk of VTE (defined as Khorana score ≥2 prior to starting new chemotherapy), if low bleeding risk and no interfering drugs.
The 2021 ASH guidelines5 suggested a different approach to ambulatory cancer patients receiving systemic cancer therapy according to their risk of VTE (based on validated assessment tools, such as the Khorana score). For patients at low VTE risk, no primary thromboprophylaxis is suggested. For patients at intermediate VTE risk, they suggest either no thromboprophylaxis or thromboprophylaxis with a DOAC (apixaban or rivaroxaban, since only apixaban and rivaroxaban were evaluated in RCTs of primary thromboprophylaxis in cancer patients). For patients at high VTE risk, they suggest either LMWH or a DOAC (apixaban or rivaroxaban). Caution should be exerted in patients at high bleeding risk. For patients with central venous catheter no primary thromboprophylaxis is suggested, since the risk of central venous catheter causing thrombosis is minimal, unless there are other concomitant risk factors.
The 2022 ITAC clinical practice guidelines87 recommended primary thromboprophylaxis with DOACs (apixaban or rivaroxaban) in ambulatory cancer patients at intermediate/high VTE risk (defined as Khorana score ≥ 2) receiving chemotherapy, if no active bleeding or high risk of bleeding. With regard to particular types of tumours, primary prophylaxis with LMWH or DOACs (apixaban, rivaroxaban) was recommended for ambulatory cancer patients with locally advanced or metastatic pancreatic cancer, receiving chemotherapy and with low bleeding risk, while it was not recommended for patients with locally advanced or metastatic lung cancer.
Conclusions
Three DOACs (apixaban, edoxaban, rivaroxaban) were assessed in RCTs for the acute treatment of CAT. They showed better efficacy than LMWH in preventing VTE recurrence. However, rivaroxaban and edoxaban were also associated with an increased risk of bleeding complications, especially in patients with gastrointestinal cancers, while apixaban did not seem to significantly increase the bleeding risk.
Two DOACs (apixaban, rivaroxaban) were assessed in RCTs for the prevention of CAT in ambulatory cancer patients starting chemotherapy. They showed better efficacy than placebo in preventing VTE occurrence. However, there was a trend towards higher rates of MB and CRNMB.
The DOACs were included in recent guidelines for the treatment of CAT in selected cancer patients (eg, low bleeding risk, no luminal gastrointestinal or genitourinary malignancies, no interfering drugs). The DOACs were also suggested for primary thromboprophylaxis in selected ambulatory cancer patients at high risk of VTE (eg, Khorana score ≥ 2 prior to starting new chemotherapy, low bleeding risk, no interfering drugs). Newer anticoagulant drugs under investigation (such as those targeting coagulation factor XI),89 have the potential to overcome some of limitations of the DOACs in CAT, in particular due to their lower bleeding risk.
Funding
No funding was provided for this manuscript.
Disclosure
The authors have no relevant conflicts to declare in relation to this paper.
References
1. Eichinger S. Cancer associated thrombosis: risk factors and outcomes. Thromb Res. 2016;140:S12–7. doi:10.1016/S0049-3848(16)30092-5
2. Kearon C, Ageno W, Cannegieter SC, Cosmi B, Geersing GJ, Kyrle PA. Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH. J Thromb Haemost. 2016;14(7):1480–1483. doi:10.1111/jth.13336
3. Frere C, Crichi B, Lejeune M, Spano JP, Janus N. Are patients with active cancer and those with history of cancer carrying the same risks of recurrent VTE and bleeding while on anticoagulants?. Cancers. 2020;12(4). doi:10.3390/cancers12040917
4. Key NS, Khorana AA, Kuderer NM, et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol. 2020;38(5):496–520. doi:10.1200/JCO.19.01461
5. Lyman GH, Carrier M, Ay C, et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. Blood Adv. 2021;5(4):927–974. doi:10.1182/bloodadvances.2020003442
6. Barnes GD, Ageno W, Ansell J, Kaatz S. Recommendation on the nomenclature for oral anticoagulants: communication from the SSC of the ISTH. J Thromb Haemost. 2015;13(6):1154–1156. doi:10.1111/jth.12969
7. Riva N, Ageno W. Pros and Cons of Vitamin K Antagonists and Non–Vitamin K Antagonist Oral Anticoagulants. Semin Thromb Hemost. 2015;41(2):178–187. doi:10.1055/s-0035-1544231
8. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa612
9. Verso M, Munoz A, Bauersachs R, et al. Effects of concomitant administration of anticancer agents and apixaban or dalteparin on recurrence and bleeding in patients with cancer-associated venous thromboembolism. Eur J Cancer. 2021;148:371–381. doi:10.1016/j.ejca.2021.02.026
10. Cohen H, Arachchillage DR, Middeldorp S, Beyer-Westendorf J, Abdul-Kadir R. Management of direct oral anticoagulants in women of childbearing potential: guidance from the SSC of the ISTH. J Thromb Haemost. 2016;14(8):1673–1676. doi:10.1111/jth.13366
11. Agnelli G, Buller HR, Cohen A, et al. Oral Apixaban for the Treatment of Acute Venous Thromboembolism. N Engl J Med. 2013;369(9):799–808. doi:10.1056/NEJMoa1302507
12. Agnelli G, Buller HR, Cohen A, et al. Apixaban for Extended Treatment of Venous Thromboembolism. N Engl J Med. 2013;368(8):699–708. doi:10.1056/NEJMoa1207541
13. Buller HR, Décousus H, Grosso MA, et al. Edoxaban versus Warfarin for the Treatment of Symptomatic Venous Thromboembolism. N Engl J Med. 2013;369(15):1406–1415.
14. Büller HR, Prins MH, Lensing AWA, et al. Oral Rivaroxaban for the Treatment of Symptomatic Pulmonary Embolism. N Engl J Med. 2012;366(14):1287–1297.
15. Bauersachs R, Berkowitz SD, Brenner B, Buller HR. Oral Rivaroxaban for Symptomatic Venous Thromboembolism. N Engl J Med. 2010;363(26):2499–2510.
16. Weitz JI, Lensing AWA, Prins MH, et al. Rivaroxaban or Aspirin for Extended Treatment of Venous Thromboembolism. N Engl J Med. 2017;376(13):1211–1222. doi:10.1056/NEJMoa1700518
17. Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus Warfarin in the Treatment of Acute Venous Thromboembolism. N Engl J Med. 2009;361(24):2342–2352. doi:10.1056/NEJMoa0906598
18. Schulman S, Kakkar AK, Goldhaber SZ, et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation. 2014;129(7):764–772. doi:10.1161/CIRCULATIONAHA.113.004450
19. Schulman S, Kearon C, Kakkar AK, et al. Extended Use of Dabigatran, Warfarin, or Placebo in Venous Thromboembolism. N Engl J Med. 2013;368(8):709–718. doi:10.1056/NEJMoa1113697
20. Van Es N, Coppens M, Schulman S, Middeldorp S, Büller HR. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: evidence from phase 3 trials. Blood. 2014;124(12):1968–1975. doi:10.1182/blood-2014-04-571232
21. Male C, Lensing AWA, Palumbo JS, et al. Rivaroxaban compared with standard anticoagulants for the treatment of acute venous thromboembolism in children: a randomised, controlled, phase 3 trial. Lancet Haematol. 2020;7(1):e18–27. doi:10.1016/S2352-3026(19)30219-4
22. Halton J, Brandão LR, Luciani M, et al. Dabigatran etexilate for the treatment of acute venous thromboembolism in children (DIVERSITY): a randomised, controlled, open-label, phase 2b/3, non-inferiority trial. Lancet Haematol. 2021;8(1):e22–33. doi:10.1016/S2352-3026(20)30368-9
23. Samji N, Bhatt MD, Kulkarni K. Challenges in Management of VTE in Children With Cancer: risk Factors and Treatment Options. Front Pediatr. 2022;10:(April):1–8. doi:10.3389/fped.2022.855162
24. Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med. 2000;160(6):809–815. doi:10.1001/archinte.160.6.809
25. Blom JW, Doggen CJM, Osanto S, Rosendaal FR. Malignancies, Prothrombotic Mutations and the Risk of Venous Thrombosis. Jama. 2005;293(6):715–722. doi:10.1001/jama.293.6.715
26. Carrier M, Le Gal G, Wells PS, Fergusson D, Ramsay T, Rodger MA. Systematic review: the Trousseau syndrome revisited: should we screen extensively for cancer in patients with venous thromboembolism?. Ann Intern Med. 2008;149(5):323–333. doi:10.7326/0003-4819-149-5-200809020-00007
27. Sorensen H, Mellemkjaer L, Olsen J, Baron J. Prognosis of cancer associated with venous thromboembolism. N Engl J Med. 2000;343:1846–1850. doi:10.1056/NEJM200012213432504
28. Gussoni G, Frasson S, La Regina M, Di Micco P, Monreal M. Three-month mortality rate and clinical predictors in patients with venous thromboembolism and cancer. Findings from the RIETE registry. Thromb Res. 2013;131(1):24–30. doi:10.1016/j.thromres.2012.10.007
29. Prandoni P, Lensing AWA, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100(10):3484–3488. doi:10.1182/blood-2002-01-0108
30. Verso M, Agnelli G, Munoz A, et al. Recurrent venous thromboembolism and major bleeding in patients with localised, locally advanced or metastatic cancer: an analysis of the Caravaggio study. Eur J Cancer. 2022;165:136–145. doi:10.1016/j.ejca.2022.01.023
31. Verso M, Agnelli G, Barni S, Gasparini G, LaBianca R. A modified Khorana risk assessment score for venous thromboembolism in cancer patients receiving chemotherapy: the Protecht score. Intern Emerg Med. 2012;7(3):291–292. doi:10.1007/s11739-012-0784-y
32. Wun T, White RH. Epidemiology of cancer-related venous thromboembolism. Best Pract Res Clin Haematol. 2009;22(1):9–23. doi:10.1016/j.beha.2008.12.001
33. Mahé I, Chidiac J, Bertoletti L, et al. The Clinical Course of Venous Thromboembolism May Differ According to Cancer Site. Am J Med. 2017;130(3):337–347. doi:10.1016/j.amjmed.2016.10.017
34. De Winter MA, Dorresteijn JAN, Ageno W, et al. Estimating Bleeding Risk in Patients with Cancer-Associated Thrombosis: evaluation of Existing Risk Scores and Development of a New Risk Score. Thromb Haemost. 2022;122(5):818–829. doi:10.1055/s-0041-1735251
35. Meyer HJ, Wienke A, Surov A. Incidental pulmonary embolism in oncologic patients—a systematic review and meta-analysis. Support Care Cancer. 2021;29(3):1293–1302. doi:10.1007/s00520-020-05601-y
36. Caiano L, Carrier M, Marshall A, et al. Outcomes among patients with cancer and incidental or symptomatic venous thromboembolism: a systematic review and meta-analysis. J Thromb Haemost. 2021;19(10):2468–2479. doi:10.1111/jth.15435
37. Lamontagne F, McIntyre L, Dodek P, et al. Nonleg venous thrombosis in critically Ill adults a nested prospective cohort study. JAMA Intern Med. 2014;174(5):689–696. doi:10.1001/jamainternmed.2014.169
38. Blom J, Doggen C, Osanto S, Rosendaal F. Old and new risk factors for upper extremity deep venous thrombosis. J Thromb Haemost. 2005;3:2471–2478. doi:10.1111/j.1538-7836.2005.01625.x
39. Cohen O, Caiano LM, Tufano A, Ageno W. Cancer-Associated Splanchnic Vein Thrombosis. Semin Thromb Hemost. 2021;47(8):931–941. doi:10.1055/s-0040-1722607
40. Ageno W, Riva N, Schulman S, et al. Long-term clinical outcomes of splanchnic vein thrombosis results of an international registry. JAMA Intern Med. 2015;175(9):1474–1480. doi:10.1001/jamainternmed.2015.3184
41. Riva N, Ageno W, Schulman S, et al. Clinical history and antithrombotic treatment of incidentally detected splanchnic vein thrombosis: a multicentre, international prospective registry. Lancet Haematol. 2016;3(6):e267–75. doi:10.1016/S2352-3026(16)30020-5
42. Valeriani E, Di Nisio M, Riva N, et al. Clinical history of cancer-associated splanchnic vein thrombosis. J Thromb Haemost. 2021;19(4):983–991. doi:10.1111/jth.15214
43. Martinelli I, De Stefano V. Rare thromboses of cerebral, splanchnic and upper-extremity veins: a narrative review. Thromb Haemost. 2010;103(6):1136–1144. doi:10.1160/TH09-12-0873
44. Passamonti SM, Biguzzi E, Cazzola M, et al. The JAK2 V617F mutation in patients with cerebral venous thrombosis. J Thromb Haemost. 2012;10(6):998–1003. doi:10.1111/j.1538-7836.2012.04719.x
45. Canonico ME, Santoro C, Avvedimento M, et al. Venous Thromboembolism and Cancer: a Comprehensive Review from Pathophysiology to Novel Treatment. Biomolecules. 2022;12(2):1–14. doi:10.3390/biom12020259
46. Lyman GH, Khorana AA. Cancer, clots and consensus: new understanding of an old problem. J Clin Oncol. 2009;27(29):4821–4826. doi:10.1200/JCO.2009.22.3032
47. Streiff MB. Association between cancer types, cancer treatments, and venous thromboembolism in medical oncology patients. Clin Adv Hematol Oncol. 2013;11(6):349–357.
48. Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular-weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med. 2002;162(15):1729–1735. doi:10.1001/archinte.162.15.1729
49. Lee A, Levine MN, Baker RI, et al. Low-Molecular-Weight-Heparin versus a Coumarin for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer. N Engl J Med. 2003;349:146–153. doi:10.1056/NEJMoa025313
50. Deitcher SR, Kessler CM, Merli G, Rigas JR, Lyons RM, Fareed J. Secondary prevention of venous thromboembolic events in patients with active cancer: enoxaparin alone versus initial enoxaparin followed by warfarin for a 180-day period. Clin Appl Thromb. 2006;12(4):389–396. doi:10.1177/1076029606293692
51. Lee AYY, Kamphuisen PW, Meyer G, et al. Tinzaparin vs warfarin for treatment of acute venous thromboembolism in patients with active cancer: a randomized clinical trial. JAMA. 2015;314(7):677–686. doi:10.1001/jama.2015.9243
52. Sanfilippo KM, Moik F, Candeloro M, Ay C, Di Nisio M, Lee AYY. Bri J Haematol 198 5 812–825; 2022 Unanswered Questions in Cancer-Associated Thrombosis.
53. Lapébie FX, Bura-Rivière A, Merah A, Bertoletti L, Monreal M. OC-15 Risk factors of recurrence in cancer-associated venous thromboembolism after discontinuation of anticoagulant therapy: a RIETE-based prospective study. Thromb Res. 2021;200:S15. doi:10.1016/S0049-3848(21)00157-2
54. Moik F, Colling M, Mahé I, Jara-Palomares L, Pabinger I, Ay C. Extended anticoagulation treatment for cancer-associated thrombosis—Rates of recurrence and bleeding beyond 6 months: a systematic review. J Thromb Haemost. 2022;20(3):619–634. doi:10.1111/jth.15599
55. Mahé I, Agnelli G, Ay C, et al. Extended Anticoagulant Treatment with Full- or Reduced-Dose Apixaban in Patients with Cancer-Associated Venous Thromboembolism: rationale and Design of the API-CAT Study. Thromb Haemost. 2022;122(4):646–656. doi:10.1055/a-1647-9896
56. McBane RD, Loprinzi CL, Ashrani A, et al. Extending venous thromboembolism secondary prevention with apixaban in cancer patients: the EVE trial. Eur J Haematol. 2020;104(2):88–96. doi:10.1111/ejh.13338
57. Rutjes AW, Porreca E, Candeloro M, Valeriani E, Di Nisio M. Primary prophylaxis for venous thromboembolism in ambulatory cancer patients receiving chemotherapy. Cochrane Database Syst Rev. 2020;2020(12). doi:10.1002/14651858.cd013521
58. Khorana A, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy- associated thrombosis. Blood. 2008;111(10):4902–4907. doi:10.1182/blood-2007-10-116327
59. Ay C, Dunkler D, Marosi C, et al. Prediction of venous thromboembolism in cancer patients. Blood. 2010;116(24):5377–5382. doi:10.1182/blood-2010-02-270116
60. Gerotziafas GT, Taher A, Abdel-Razeq H, et al. A Predictive Score for Thrombosis Associated with Breast, Colorectal, Lung, or Ovarian Cancer: the Prospective COMPASS–Cancer-Associated Thrombosis Study. Oncologist. 2017;22(10):1222–1231. doi:10.1634/theoncologist.2016-0414
61. van Es N, Di Nisio M, Cesarman G, et al. Comparison of risk prediction scores for venous thromboembolism in cancer patients: a prospective cohort study. Haematologica. 2017;102(9):1494–1501. doi:10.3324/haematol.2017.169060
62. Mulder FI, Candeloro M, Kamphuisen PW, et al. The khorana score for prediction of venous thromboembolism in cancer patients: a systematic review and meta-analysis. Haematologica. 2019;104(6):1277–1287. doi:10.3324/haematol.2018.209114
63. Young AM, Marshall A, Thirlwall J, et al. Comparison of an oral factor xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). J Clin Oncol. 2018;36(20):2017–2023. doi:10.1200/JCO.2018.78.8034
64. Piccini JP, Garg J, Patel MR, et al. Management of major bleeding events in patients treated with rivaroxaban vs. warfarin: results from the ROCKET AF trial. Eur Heart J. 2014;35(28):1873–1880. doi:10.1093/eurheartj/ehu083
65. Cheung KS, Leung WK. Gastrointestinal bleeding in patients on novel oral anticoagulants: risk, prevention and management. World J Gastroenterol. 2017;23(11):1954–1963. doi:10.3748/wjg.v23.i11.1954
66. Planquette B, Bertoletti L, Charles-Nelson A, et al. Rivaroxaban vs Dalteparin in Cancer-Associated Thromboembolism: a Randomized Trial. Chest. 2022;161(3):781–790. doi:10.1016/j.chest.2021.09.037
67. Raskob GE, van Es N, Verhamme P, et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N Engl J Med. 2018;378(7):615–624. doi:10.1056/NEJMoa1711948
68. Mulder FI, van Es N, Kraaijpoel N, et al. Edoxaban for treatment of venous thromboembolism in patient groups with different types of cancer: results from the Hokusai VTE Cancer study. Thromb Res. 2020;185:13–19. doi:10.1016/j.thromres.2019.11.007
69. McBane RD, Wysokinski WE, Le-Rademacher JG, et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: the ADAM VTE trial. J Thromb Haemost. 2020;18(2):411–421. doi:10.1111/jth.14662
70. Agnelli G, Becattini C, Meyer G, et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N Engl J Med. 2020;382(17):1599–1607. doi:10.1056/NEJMoa1915103
71. Ageno W, Vedovati MC, Cohen A, et al. Bleeding with Apixaban and Dalteparin in Patients with Cancer-Associated Venous Thromboembolism: results from the Caravaggio Study. Thromb Haemost. 2021;121(5):616–624. doi:10.1055/s-0040-1720975
72. Becattini C, Bauersachs R, Maraziti G, et al. Renal function and clinical outcome of patients with cancer-associated venous thromboembolism randomized to receive apixaban or dalteparin. Results from the Caravaggio trial. Haematologica. 2022;107(7):1567–1576.
73. Schrag D, Uno H, Rosovsky RPG, et al. The comparative effectiveness of direct oral anti-coagulants and low molecular weight heparins for prevention of recurrent venous thromboembolism in cancer: the CANVAS pragmatic randomized trial. J Clin Oncol. 2021;39(15_suppl):12020. doi:10.1200/JCO.2021.39.15_suppl.12020
74. Petit B, Soudet S, Poenou G, et al. PO-41: cancer-associated thrombosis: how many patients seen in clinical practice would be eligible to a randomized controlled trial?. Thromb Res. 2022;213(Suppl 2):S30. doi:10.1016/S0049-3848(22)00231-6
75. Frere C, Farge D, Schrag D, Prata PH, Connors JM. Direct oral anticoagulant versus low molecular weight heparin for the treatment of cancer-associated venous thromboembolism: 2022 updated systematic review and meta-analysis of randomized controlled trials. J Hematol Oncol. 2022;15(1):69. doi:10.1186/s13045-022-01289-1
76. Brea EJ, Tiu BC, Connors JM. A comprehensive review of DOACs for cancer associated VTE prophylaxis or treatment. Postgrad Med. 2021;133:71–79. doi:10.1080/00325481.2021.1955542
77. Carrier M, Abou-Nassar K, Mallick R, et al. Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. N Engl J Med. 2019;380(8):711–719. doi:10.1056/NEJMoa1814468
78. Ladha D, Mallick R, Wang T-F, Caiano L, Wells PS, Carrier M. Efficacy and safety of apixaban for primary prevention in gastrointestinal cancers: a post-hoc analysis of the AVERT trial. Thromb Res. 2021;1(202):151–154. doi:10.1016/j.thromres.2021.03.013
79. Brandt W, Brown C, Wang T-F, et al. Efficacy and safety of apixaban for primary prevention of thromboembolism in patients with cancer and a central venous catheter: a subgroup analysis of the AVERT Trial. Thromb Res. 2022;1(216):8–10. doi:10.1016/j.thromres.2022.05.014
80. Knoll W, Mallick R, Wells PS, Carrier M. Safety and efficacy of apixaban thromboprophylaxis in cancer patients with metastatic disease: a post-hoc analysis of the AVERT trial. Thromb Res. 2021;197:13–15. doi:10.1016/j.thromres.2020.10.026
81. Khorana AA, Soff GA, Kakkar AK, et al. Rivaroxaban for Thromboprophylaxis in High-Risk Ambulatory Patients with Cancer. N Engl J Med. 2019;380(8):720–728. doi:10.1056/NEJMoa1814630
82. Vadhan-Raj S, McNamara MG, Venerito M, et al. Rivaroxaban thromboprophylaxis in ambulatory patients with pancreatic cancer: results from a pre-specified subgroup analysis of the randomized CASSINI study. Cancer Med. 2020;9(17):6196–6204. doi:10.1002/cam4.3269
83. Mones JV, Streiff MB, Khorana AA, et al. Rivaroxaban thromboprophylaxis for gastric/gastroesophageal junction tumors versus other tumors: a post hoc analysis of the randomized CASSINI trial. Res Pract Thromb Haemost. 2021;5(5):1–8. doi:10.1002/rth2.12549
84. Li A, Kuderer NM, Garcia DA, et al. Direct oral anticoagulant for the prevention of thrombosis in ambulatory patients with cancer: a systematic review and meta-analysis. J Thromb Haemost. 2019;17(12):2141–2151. doi:10.1111/jth.14613
85. Khorana AA, Noble S, Lee AYY, et al. Role of direct oral anticoagulants in the treatment of cancer-associated venous thromboembolism: guidance from the SSC of the ISTH. J Thromb Haemost. 2018;16(9):1891–1894. doi:10.1111/jth.14219
86. Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic Therapy for VTE Disease: second Update of the CHEST Guideline and Expert Panel Report. Chest. 2021;160(6):e545–608. doi:10.1016/j.chest.2021.07.055
87. Farge D, Frere C, Connors JM, et al. Policy Review 2022 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer, including patients with COVID-19. Lancet Oncol. 2022;6:3–5.
88. Wang TF, Zwicker JI, Ay C, et al. The use of direct oral anticoagulants for primary thromboprophylaxis in ambulatory cancer patients: guidance from the SSC of the ISTH. J Thromb Haemost. 2019;17(10):1772–1778. doi:10.1111/jth.14564
89. Poenou G, Dimitru Dimitru T, Lafaie L, Mismetti V, Heestermans M, Bertoletti L. Factor XI Inhibition for the Prevention of Venous Thromboembolism: an Update on Current Evidence and Future perspectives. Vasc Health Risk Manag. 2022;18:359–373.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.