")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Direct and Indirect Costs of Asthma Burden in Abu Dhabi: A Retrospective Analysis of Insurance Claims Data from 2015 to 2018
Authors Al Mazrouei K, Almannaei AI, Nur FM, Bachnak N, Alzaabi A
Received 20 September 2021
Accepted for publication 11 November 2021
Published 29 December 2021 Volume 2021:13 Pages 969—980
DOI https://doi.org/10.2147/CEOR.S331499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samer Hamidi
Khulood Al Mazrouei,1 Asma Ibrahim Almannaei,2 Faiza Medeni Nur,3 Nagham Bachnak,3 Ashraf Alzaabi4
1Pulmonology Department, Zayed Military Hospital, Abu Dhabi, United Arab Emirates; 2Department of Health, Healthcare Quality Division at the Abu Dhabi Health Authority, Abu Dhabi, United Arab Emirates; 3Healthcare Data and Analytics Division, Department of Health, Abu Dhabi Health Authority, Abu Dhabi, United Arab Emirates; 4Respiratory Medicine Division, Zayed Military Hospital, Abu Dhabi, United Arab Emirates
Correspondence: Ashraf Alzaabi
Respiratory Medicine Division, Zayed Military Hospital, Abu Dhabi, United Arab Emirates
Tel +971 506 474 488
Email [email protected]
Purpose: Asthma causes a high economic burden on the health-care system. Previous research on the cost of asthma in Abu Dhabi was in 2011 and revealed high medical costs. This work aimed to estimate both direct and indirect costs of asthma with trend analysis over a period of four years.
Patients and Methods: All data on medical costs, work absenteeism, and mortality were collected from the e-claims system of the national health insurance database. Medical costs included medication use, emergency room (ER) visits, non-ER visits, outpatient care, and hospitalization from 2015 to 2018. Indirect costs in terms of work absenteeism were calculated by multiplying the average daily income per employer by the number of workdays missed due to sick leaves documented in the database in 2019.
Results: Over the years, the total medical costs increased from AED 161,843,698 in 2015 to AED 206,548,620 in 2018. The largest contribution was attributed to outpatient care, while hospitalization accounted for the smallest proportion of the total costs in 2018. Likewise, the mean annual per-patient cost in 2015 was AED 1119 and increased to AED 1162 in 2018. Indirect costs were estimated to be AED 27,482,319 resulting from 30,948 sick leaves in the year 2019 only.
Conclusion: Asthma is a cause for huge expenditure from the health-care system perspective in Abu Dhabi. It also has a large impact on society through work absenteeism. Costs of asthma management are increasing every year, which suggests a call-to-action to improve the disease management status using cost-effective strategies.
Keywords: asthma, direct cost, indirect cost, economic burden, Abu Dhabi
Introduction
Asthma is a prevalent, chronic, inflammatory disorder that affects individuals of all age groups, with the highest incidence among children under five.1 Despite the rapid and massive developments in medical practice, asthma incidence has increased steadily over the past 25 years to reach 43.12 million new cases per year in 2017, while nearly 339 million people were estimated to suffer from asthma in the same year.2,3 Besides, asthma is a significant contributor to global mortality and accounted for almost 500,000 global deaths in 2017 alone.4 The incidence and burden of asthma show wide geographic and ethnic disparities, with higher asthma-related mortality rates in developing countries.5,6
The economic consequences of asthma are considerable, involving days lost from jobs and the inability to attend schools.6,7 Asthmatic patients usually present with recurrent, lifelong, attacks of breathlessness and wheezing of variable severity and frequency. The recurrent symptoms of asthma usually lead to insufficient night sleep and daytime fatigue. These symptoms contribute to reduced productivity for patients at school and work.8 According to the Global Burden of Disease (GBD) study in 2016, asthma was ranked 16th among the leading causes of years lived with disability (YLD).3,9
From the economic point of view, asthma continues to impose a large economic burden on the global level for both the associated direct and indirect costs. The economic burden of any disease depends on the disease prevalence, the costs of health-care services or products (direct costs), and societal costs resulting from productivity loss of patients or their caregivers (indirect costs).9 In the United States (US), the total asthma costs for the whole population per year increased from US$53 billion in 2002 to US$56 billion in 2011. Total costs of asthma for European people were €19.3 billion during 1999–2002.9 Besides, the high prevalence of poorly controlled asthma adds further economic burden; a meta-analysis from the US estimated that the excess direct costs associated with uncontrolled versus controlled asthma were $1349 per patient-year. On average, a person with uncontrolled asthma loses an extra 12.7% of their work time, compared to a person with controlled asthma.10
In the Gulf region, asthma prevalence among residents in the community was estimated to be 7.6%.11 In a recent cross-sectional study on five Middle Eastern countries in 2018, the estimated prevalence of asthma in the United Arab Emirates (UAE) was 4.9% [95% CI 4.2–6.6%]. Previous reports showed that the level of asthma control is still poor in the Middle East, with 44.2% of asthma patients reported uncontrolled asthma and these patients reported significantly lower utility values than controlled subjects.12,13 Another survey of 200 asthmatic patients in the UAE revealed that a considerable proportion of the patients had poorly controlled asthma in the form of sudden severe attacks, troublesome symptoms, school and work absenteeism, and emergency room visits.14 In the UAE, the economic burden of asthma was previously assessed in two studies, which demonstrated a high economic burden and lack of optimal disease management.15,16
This study aims to continue the work of the previous research performed in Abu Dhabi in 2011. The current study provides more in-depth insights and captures the bigger picture of the economic burden of asthma. On the one hand, the study captures asthma-related costs from the healthcare system perspective over an extended period of four years, which allows us to monitor the change of health expenditures over time. On the other hand, the study has secondary objectives including asthma’s indirect costs due to work absenteeism and mortality attributed to asthma.
Methodology
Ethical Statement
The Ethical Committee of the Zayed Military Hospital approved the study’s protocol (No. 2019.1). Due to the retrospective nature of the present study, the need for informed consent was waived by the ethics committee. We confirm that all study’s procedures run in concordance with the principles of the Declaration of Helsinki and its latest version.
Study Design
This retrospective study assessed the economic burden from all direct medical costs of asthma in Abu Dhabi. The data were retrieved from the insurance claims electronic database of the Abu-Dhabi Health Insurance and covered the period from 2015 to 2018. As all medical expenses in Abu Dhabi are totally paid for through the health insurance system, the study outcomes represent the cost of the asthma from the healthcare system perspective. For the secondary objectives of the study, work absenteeism and mortality are also analyzed retrospectively from the same electronic database.
Study Population and Study Duration
The study targeted resources used by all asthma patients who are residents of Abu Dhabi (nationals and expatriates) and are covered under the umbrella of the National Health Insurance of Abu Dhabi. The national insurance covers 98% of the total population. Asthma patients were identified from the database of the Department of Health (DoH) based on WHO 10th International Classification of Disease (ICD-10).17 The ICD codes are used based on the physician’s reported diagnosis.
Consecutive patients of all ages who visited a public or private health-care provider because of asthma from 2015 to 2018 were included in the analysis without restrictions. Data on sick leaves attributed to asthma were available only for the years 2018 and 2019 and were used to estimate indirect costs in these two years.
Data Collection
We included all data related to direct medical and indirect costs of asthma. To identify patients, the patient should have at least one encounter/visit with a principal diagnosis of asthma. Unique count of patients was identified by the health insurance member ID. For direct cost estimation, we collected all data on physician consultations, hospital admissions, emergency room visits, and medications. All encounters and prescriptions had ICD-10 codes to identify only asthma-related activities with a high degree of accuracy. To estimate indirect costs, we collected data related to disease-related work absenteeism and mortality. As in medical costs, sick leaves and mortality are also coded with ICD system; therefore, only asthma-attributed events were identified. All data were collected by DoH staff, who are only authorized to access the database. No accessible data were available on patients’ demographics or clinical characteristics (such as medical history, disease severity, and comorbidities).
Health Insurance System in Abu Dhabi
The DoH determines the pricing of health services in Abu Dhabi for both public and private facilities. The real costs charged are then negotiated between the providers and insurers. Subsequently, claims are submitted for reimbursement. In the 2014 report, we described the organizational structure of different health insurance programs in Abu Dhabi.16
Estimating Direct Medical Costs
Costs were analyzed based on claims submitted to DoH from the insurance companies and costs from health-care providers. Both sources’ compilation gave us the best estimate of the real costs of asthma imposed on the health-care system. Costs are reported in Dirhams (AEDs) without discounting.
To analyze the change in the mean cost per patient per year, we had to eliminate the effect of change in unit prices over the years due to inflation. As there was no access to unit prices of each service but only the total costs, the consumer price index (CPI) was used to adjust prices. Costs in years 2016 till 2018 were adjusted to the costs of the year 2015 as a baseline using the following formula:
Adjusted Costs for any subsequent year = cost in this year X (CPI of 2015/CPI of this year)
CPI for medical care in the United Arab Emirates was obtained from the Statista website.18
For comparison purposes, all costs mentioned in the discussion section were converted to USD in year 2015 as all costs in the study are adjusted for this year. Historical exchange rates were retrieved using the PACIFIC Exchange Rate Service from the University of British Columbia (monthly averages, price notation)19 Prices were adjusted to 2015 levels before currency conversion using CPI indices of each country (monthly averages, all items) from the International Monetary Fund (IMF) website.20
Estimating Indirect Costs Due to Work Absenteeism
A literature review was performed to calculate the average cost per working day per person for Abu Dhabi. Using the percent increase in employees’ compensation from the Statistical Yearbook of Abu Dhabi, 2019, we estimated the compensation received by employees in 2019 to be AED 259,296 million.21 In 2019, there was a total of 261 working days. An average income per day of AED 993,471,264 was calculated accordingly.
In 2019, the population of Abu Dhabi was 1.81 million. The labor force accounted for 65.2% of the total population, and the percentage of employed to the labor force was 94.8%. Thus, a population of 1,118,753.76 were employed.21 The average income per day for the whole population was divided by the employed population to estimate the average income per employee per day. This number was multiplied by the number of days off work due to asthma for patients 18 years and older to calculate the total indirect cost for 2019 due to asthma-related work absenteeism. The same method was applied to estimate indirect cost attributed to sick leaves for the year 2018 using the value of total compensation for all employees in this year which was AED 250,013 million.21
Statistical Analysis
For descriptive statistics, results were expressed as a mean for continuous variables and as a percentage for categorical variables. Trends in the mean costs per patient over the study period were evaluated using a one-part model with a linear equation predicting the log(cost+1) with a random effect for each patient and a fixed effect for the cost year. In this way, a patient-specific mean log(cost) was estimated and captured the between-patient variability in costs while enabling an estimation of the mean log(cost) per patient for each year.
Results
A total of 144,597 asthma patients were identified on the DoH database who visited a health-care facility because of asthma in 2015. The number increased to 177,693 patients in 2018. Those patients represent the whole population of the study.
Direct Medical Costs
Breakdown of Costs Among Resource Items
The medical cost utilized by the study population was AED 206,548,620 during the year 2018. Figure 1A illustrates the distribution of these costs between ER visits, non-ER visits, and medications. The item responsible for the highest cost was non-ER visits, which accounted for 49.63% of the total costs (AED 102,502,721), followed by medications representing 39.84% (AED 82,295,679); the majority of the medication costs were attributable to controller medications that alone represented 37.83% of the total costs. The ER-visits were the last item, which accounted for 10.53% of the total medical costs (AED 21,750,220).
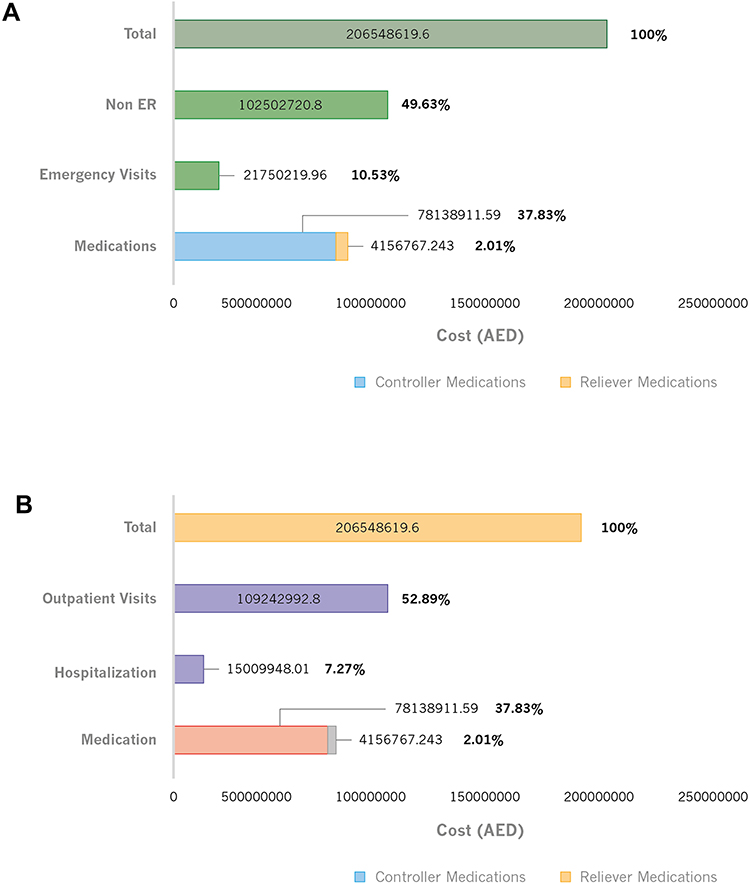 |
Figure 1 Distribution of medical costs according to categories of resources use. (A) Breakdown of medical costs between emergency visits, non-emergency visits and medications. (B) Breakdown of medical costs between outpatient visits, hospitalizations and medications. Abbreviation: ER, emergency. |
After the initial ER or non-ER visits, patients may be either hospitalized or managed in the outpatient setting. The outpatient and hospitalization care costs are overlapping with the initial visits’ costs in the dataset. It is not possible from the available data to extract these items separately. Therefore, the total medical costs were also analyzed according to the management pathway as outpatient vs hospitalized (Figure 1B). Outpatient care accounted for the largest part of the cost representing 52.89% of the total costs (AED 109,242,993), followed by medication costs representing 39.84% (AED 82,295,679). Finally, hospitalization costs were 7.27% of the total medical costs (AED 15,009,948).
Trend Analysis of Costs and Resources Used Over Years
Annual Total Costs
By comparing the total medical costs for all patients between different years from 2015 till 2018, it was found that total medical costs are increasing every year, starting from AED 161,843,698 in 2015 to AED 206,548,620 in 2018. In contrast, the contribution of medications relative to the total costs was decreasing every year (Figure 2A). However, when analyzing medications costs only, it was found that medication costs increased every year until 2017 but dropped in 2018, as illustrated in Figure 2B. These figures indicate that although the absolute expenditure on medications increased, this increase was less than the increase in other medical activities. Accordingly, the contribution of medications to total costs decreased over time.
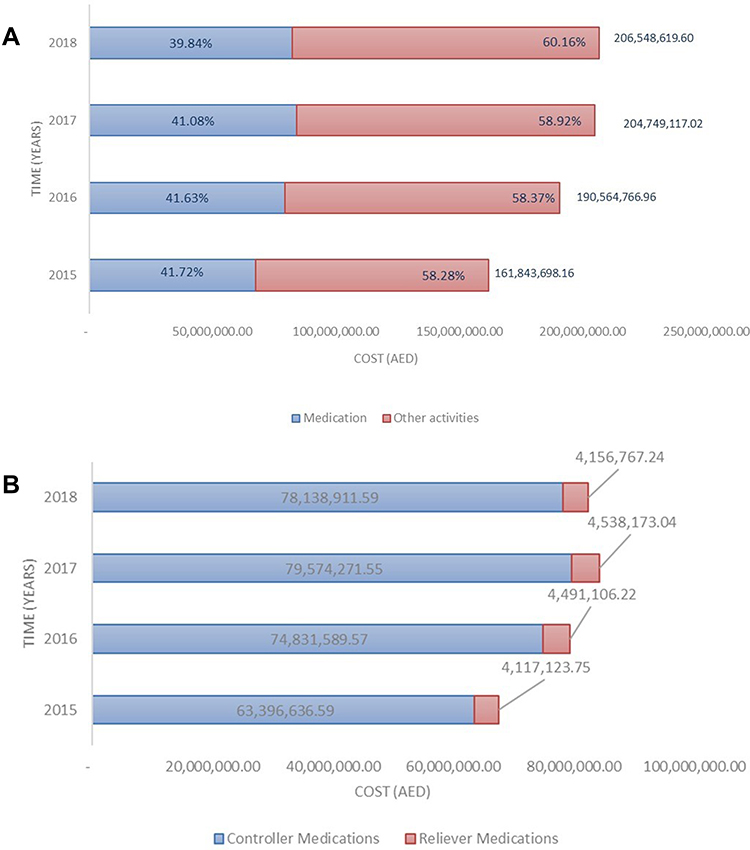 |
Figure 2 Change in medical costs over the study period from 2015 to 2018. (A) Total medical costs per year from 2015 to 2018. (B) Medications cost per year from 2015 to 2018. |
Annual Drug Prescriptions
The above figures are slightly different when the analysis targets the annual number of drug prescriptions instead of the total costs. In this case, we observed an increase in the number of prescribed medications from 2015 to 2016, then a decline in 2017, and a further decline in 2018 (Figure 3). By analyzing the prescribed medications according to the drug type (ie, controller vs reliever medications), the year 2017 has the highest frequency of reliever medication use among all years.
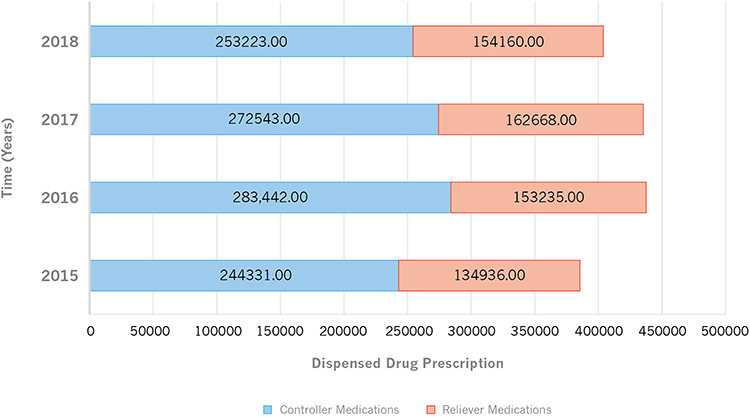 |
Figure 3 Medication use by the number of dispensed prescriptions in different years. |
Annual Costs per Patient
The annual total costs described above resulted from many factors, including the number of patients, drug prices, and the intensity of resources used by each patient. To examine the changes in resources used irrespective of the number of patients and drug price, we calculated the annual costs per patient after adjustment for inflation rate (Table 1). The annual mean cost per patient was AED 1119, 1124, 1158, and 1162 in the years 2015, 2016, 2017, and 2018, respectively.
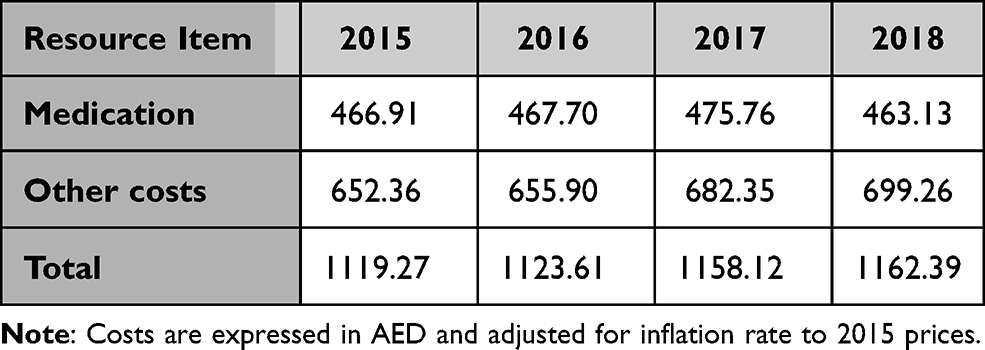 |
Table 1 Adjusted Mean Cost per Patient per Year (2015 to 2018) |
The log-transformed results of these data are presented in Figure 4. It showed a continuous annual increase in total costs per patient every year with an increase of all health-care services, except medications (Figure 4A and B). The adjusted cost of medications per patient increased each year before it exhibits a decline in 2018, as shown in Figure 4C.
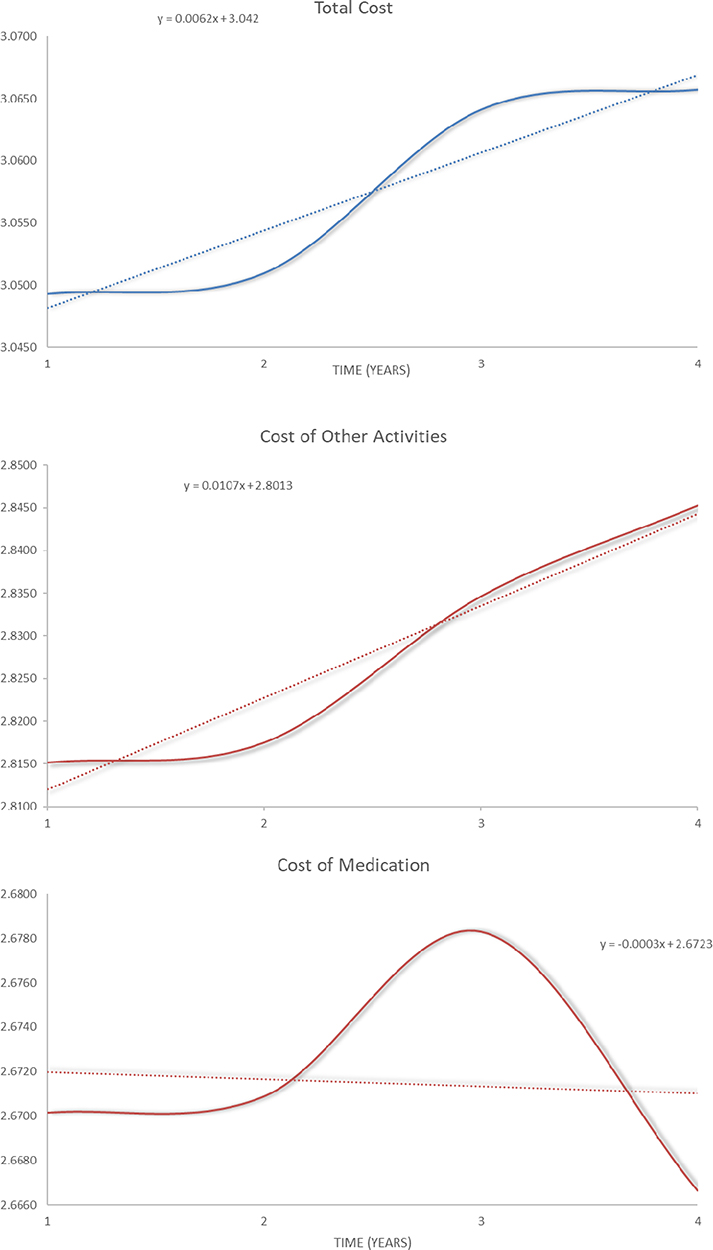 |
Figure 4 Trend analysis for medical costs using log transformed data. (A) Trend analysis for total medical costs. (B) Trend analysis for medical costs other than medications. (C) Trend analysis for medication cost. |
Frequency of Prescribed Medications by Class
All patients with prescribed medications in 2018 were analyzed according to the prescribed drug class (Figure 5). The analysis revealed that the combination of long-acting beta-agonists (LABA) and inhaled corticosteroids (ICS) were the most prescribed, followed by the short-acting beta-agonists (SABA), then leukotriene modifiers. Anti-immunoglobulin E (IgE), single use of LABA, and theophylline were the least prescribed medications.
 |
Figure 5 Number of patients according to the prescription frequency of each drug class during 2018. Abbreviations: ICS, inhaled corticosteroids; IGE, immunoglobulin; LABA, long acting beta agonists; OCS, oral corticosteroids; SABA, short acting beta agonists. |
Indirect Costs
Work Absenteeism
The total number of sick leaves in days in 2019 for asthma patients (above 18 years) was estimated to be 30,948 days. The average income per day per employee was calculated as AED 888.02 per day. Indirect costs for 2019 due to work absenteeism related to asthma were estimated by multiplying the number of off days by the average income per day per employee. It was found that in 2019, the total indirect cost due to work absenteeism related to asthma was AED 27,482,319.
Similarly, the average daily earnings per employee for 2018 was calculated as AED 856.22, resulting in a total indirect cost due to work absenteeism related to the asthma of AED 35,809,014. Sick leaves for patients younger than 18 years were not used in the calculation due to the assumption that these patients are school-going and not contributing to the workforce.
Asthma Related Death
The number of deaths for each year from 2015 to 2018 due to respiratory diseases and asthma are shown in Table 2. According to the available data, all over the four years, a total of 15 fatality cases were attributable to asthma. These numbers represented a small percentage of all respiratory deaths (2.1%). Although the total number of respiratory deaths was highest in 2018 (195 cases), the same year witnessed the lowest asthma-related deaths (no. =2 cases), representing 1% of the total respiratory-related death.
 |
Table 2 Number of Respiratory Disease Deaths for Each Year and Death Cases Attributable to Asthma |
Discussion
Asthma has a sizeable economic impact on the healthcare system in Abu Dhabi. Our study aimed to estimate both direct and indirect costs of asthma in Abu Dhabi over four years from 2015 to 2018. Previous research conducted in this area was a study collecting data back in 2011 limited to the one-year duration and focused only on direct costs.16 This study makes a unique contribution to our understanding of the financial burden of the disease throughout many years.
-We demonstrated that more than 206 million AED ($56 million in 2015) was expensed on direct medical costs for asthma treatment in 2018. While productivity loss due to work absenteeism was estimated to cause more than 27 million AED ($7.4 million in 2015) lost income in 2019. These findings revealed a high economic burden imposed by asthma on the healthcare system in Abu Dhabi in terms of both direct and indirect costs, as documented in the national claims database.
Medical costs for asthma management estimated in the study can be compared to previous studies conducted in Abu Dhabi and other Emirates in the UAE. Our findings revealed that the total medical cost incurred in 2018 was AED 206,548,620 ($56,238,265 in 2105) resulting from an average annual per-patient cost of nearly AED 1162 ($316 in 2015). In the previous study conducted in Abu Dhabi in 2011, the total annual costs were about AED 105 million ($31 million in 2015) for 139,000 patients.16 The annual per-patient cost was around AED 750 ($220 in 2015). These figures are much lower than the calculated costs in our study. This difference can be partly attributed to the involvement of other activities in the e-claims database that were not captured in the previous years, such as outpatients’ visits and hospitalizations. However, the difference is too large to be explained by the inclusion of these items. In the current study, the trend analysis of medical costs, over the study duration, revealed a continuous increase in total and per-patient costs every year, even after adjusting for the inflation rate. The adjusted annual per-patient costs increased from AED 1119 ($305 in 2015) in 2015 to AED 1162 ($316 in 2015) in 2018. Interpreting these figures together raises a number of questions to address the exact causes for this small but continuous increase. The increase might suggest an increased number of uncontrolled asthma patients requiring more considerable healthcare expenditure. The other possible explanation is the overuse of health-care resources in terms of outpatient visits, hospitalizations, or medication use. National efforts should be directed to evaluate health-care professionals’ compliance and facilities to treatment guidelines.
Our findings can also be compared with a study conducted in Dubai (another emirate in UAE) in 2013 using data collected from patient questionnaires. The study estimated an annual per-patient medical cost of about AED 1700 ($493 in 2015). The total economic burden for this year was AED 88 million ($25.5 million in 2015) for treating 52,500 patients.15
Various estimated costs were also reported in the literature from the US, Canada, and Europe. In the US, the estimated annual direct cost per patient from 2008 to 2013 was $3300 (adjusted to 2015 US dollars).22 Studies from Europe generally reported a lower cost for treating asthma patients. According to a recent review, the average cost per patient was estimated to be $1900 ($1840 in 2015) in Europe.5 A report from Ireland documented nearly €700 in 2017 ($770 in 2015) for direct costs per asthma patient.23 The lowest cost was estimated in a Canadian study, in which the cost per patient was $311 in 2012 ($270 in 2015).24
Comparison of the above figures requires some caution. Many factors can affect the estimated costs in each study. Some are related to the disease and its management, such as the severity of cases, the clinical practice, health-care services, and medication costs. Other heterogeneity sources may result from the methodology used in data collection or analysis and the resource items included within the scope of each study. Finally, the perspective and the countries’ insurance system structure impact the estimated costs in different studies.
The primary driver for medical cost in this study was outpatient visits, followed by medication, and hospitalization cost with a contribution of 52.89%, 39.84%, and 7.27%, respectively. Similar results were found in both studies conducted in UAE, in which outpatient care represented the highest cost but with variable share (81% in the previous study in Abu Dhabi and 37% in the Dubai study15,16).
On the contrary, results from the US, UK, and Canada revealed that medication costs made up the highest contribution in the total medical cost.22,24,25 In Canada, for example, medication costs alone accounted for 68.3% of the total costs.24 Notably, outpatient care represented the least costly category in the US and Canada.22,24
Though these findings can reflect, to some extent, how the disease is managed differently in each country, care should be taken as each study might have used different definitions and classification systems for these categories, which may affect the comparability between them. The unit prices of these items in each country should also be considered beside the total cost. Finally, in studies collecting data through patient questionnaires, recall bias can play a role in overestimating specific categories with a special impact on patients, such as hospital stays.
Our study found that a substantial amount of costs was attributed to ER visits and hospitalization. In the first analysis, ER visits represented 10.53% of the total costs. In the second analysis, hospitalization accounted for 7.27% of the total medical cost. These findings suggest a potential for improving asthma management in UAE to minimize such avoidable costs by implementing cost-effective national strategies aiming at better asthma control and improved access to early treatment. For example, in Finland, a nationwide asthma program (1994–2004) and an allergy program (2008–2018) have been implemented to improve asthma management. From 1987 to 2013, the total annual costs decreased by 14%. This reduction was despite the three-fold increase in prevalence. The annual costs per patient decreased by 72%.9
In this study, we estimated a total of AED 27,482,319 ($7,482,780) indirect cost in 2019 attributed to work absenteeism. Similar to our findings, substantial indirect costs were also documented in several studies in the UAE and other countries. In Dubai, the average loss of days due to asthma was four days per year, which results in a loss of about 79,000 workdays annually.15 In Ireland, the indirect costs were estimated to account for 43% of the total asthma costs.23 Another study from the US calculated that asthma was responsible for $3 billion (adjusted to 2015 US dollars) in losses due to missed work and school days during 2008–2013.22
The methodology used in our study has many strengths. It gives us a very close estimate of the real expenditure on medical costs of asthma treatment. Real prices incurred by different health-care providers and paid by different insurers are all reflected in the claims database. There is a low risk of selection bias in our study as the e-claims database represents the national health insurance of Abu Dhabi, which covers 98% of the whole population. The use of the ICD classification system also allowed accurate identification of asthma cases. Another strength of this study is the analysis of changes in costs over multiple years. It gives an overall picture of the nature of changes occurring in the asthma management landscape in Abu Dhabi. It is also worth noting that this is the second study measuring asthma costs in Abu Dhabi, which provides a more extended timeframe for better and more robust insights generation.
However, this study is not without limitations. First, it is supposed that few data, especially from smaller health-care facilities, may not be included in the insurance claims database, which can result in little underestimation of the overall costs. The percent of omitted claims is estimated to be about 10%, according to the DoH. The main objective of the study was to estimate the economic burden of asthma from the health-care system perspective; accordingly, the study did not capture the whole burden of the disease on the society as other important costs are not assessed here, eg, non-medical costs including transportation. For indirect costs also, only work absence was included in our study while other critical aspects were not measured. Such costs include productivity losses due to decreased performance at work, partial absence, reduced working hours, inability to work, early retirement, reduced productivity in performing routine household chores, and the indirect cost of missed school days for children. It was reported in the literature that children with asthma caused higher indirect costs than adult patients because of the parents’ missed workdays who are caring for sick kids.5 Earlier studies that attempted to measure different cost type from a societal perspective found that indirect costs alone represent 35% to 43% of the total disease burden.23,26 Finally, the method used in our study does not allow us to access patient clinical characteristics such as the disease history and severity and relate them with the incurred costs.
Studies measuring the cost of illness are of substantial importance to the decision-makers and researchers. Our findings can inform other economic studies, such as cost-effectiveness studies of newer asthma medications. On the other hand, it can support decision-makers to better allocate resources according to the disease areas that are consuming the highest resources. Unfortunately, up to our knowledge, very few data are generated on the cost of illness of other diseases in the UAE. The only study, which examined the cost of diabetes in UAE in AL-Ain from 2004 to 2005, reported an annual cost per diabetic patient without complications of US $1605 ($1980 in 2015) and $5645 ($6700 in 2015) for patients with complications.27
Future research collecting individual patient data will support and explain findings in our study on the national level. Such clinical details will help us precisely define the causes of resource consumption. It will also facilitate monitoring of care improvement, compliance with guidelines, and the success of national programs. Studying the relationship between medication prescribing habits and the decrease in asthma hospitalizations and ER visits will also be of interest to decision-makers. For indirect costs, future studies can include the indirect costs of school-age patients, which is expected to increase the estimates significantly.
On the global level, more standardized approaches should be developed and adopted to allow for valid inter-country comparisons and help monitor trends in the economic burden on a robust basis.
Conclusion
The economic burden of asthma on the health-care system in Abu Dhabi is very high in terms of both direct and indirect costs. Direct medical costs increased dramatically since the last study conducted in the same region in 2011. Medical costs are primarily derived from outpatient visits, followed by medication and hospitalization. Total and annual costs per patient were constantly increasing over the study period suggesting that asthma management is not moving towards a better status. Though the mortality rate is very low, indirect costs attributed to sick leaves are substantial. Our findings can inform policymakers and suggest the need for implementing better cost-effective disease management programs.
Disclosure
This project is an investigator-initiated project funded by AstraZeneca. The funding sources had no role in the conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The authors report no other conflicts of interest in this work.
References
1. Winer RA, Qin X, Harrington T, Moorman J, Zahran H. Asthma incidence among children and adults: findings from the behavioral risk factor surveillance system asthma Call-Back Survey-United States, 2006–2008. J Asthma. 2012;49(1):16–22. doi:10.3109/02770903.2011.637594
2. Mattiuzzi C, Lippi G. Worldwide asthma epidemiology: insights from the Global Health Data Exchange database. Int Forum Allergy Rhinol. 2020;10(1):75–80. doi:10.1002/alr.22464
3. Vos T, Abajobir AA, Abbafati C, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
4. Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
5. Nunes C, Pereira AM, Morais-Almeida M. Asthma costs and social impact. Asthma Res Pract. 2017;3(1):1–11. doi:10.1186/s40733-016-0029-3
6. Accordini S, Corsico A, Cerveri I, et al. The socio-economic burden of asthma is substantial in Europe. Allergy. 2008;63(1):116–124. doi:10.1111/j.1398-9995.2007.01523.x
7. Accordini S, Bugiani M, Arossa W, et al. Poor control increases the economic cost of asthma. A multicentre population-based study. Int Arch Allergy Immunol. 2006;141(2):189–198. doi:10.1159/000094898
8. Global Initiative for Asthma. 2018 GINA Report: Global Strategy for Asthma Management and Prevention 2018: Global Initiative for Asthma. 2018. doi:10.1002/uog.8947
9. Global Asthma Network. The Global Asthma Report 2018. Global Asthma Network; 2018.
10. Yaghoubi M, Adibi A, Safari A, FitzGerald JM, Sadatsafavi M. The projected economic and health burden of uncontrolled asthma in the United States. Am J Respir Crit Care Med. 2019;200(9):1102–1112. doi:10.1164/rccm.201901-0016OC
11. Tarraf H, Aydin O, Mungan D, et al. Prevalence of asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT program. BMC Pulm Med. 2018;18(1):68. doi:10.1186/s12890-018-0621-9
12. Mungan D, Aydin O, Mahboub B, et al. Burden of disease associated with asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT program. Respir Med. 2018;139(March):55–64. doi:10.1016/j.rmed.2018.03.030
13. Alzaabi A, Idrees M, Behbehani N, et al. Cross-sectional study on asthma insights and management in the Gulf and Russia.
14. Mahboub BHSH, Santhakumar S, Soriano JB, Pawankar R. Asthma insights and reality in the United Arab Emirates. Ann Thorac Med. 2010;5(4):217–221. doi:10.4103/1817-1737.69109
15. Mahboub H. Cost of Asthma in Dubai, United Arab Emirates (UAE). J Pulm Respir Med. 2013;03(2):2–5. doi:10.4172/2161-105x.1000146
16. Alzaabi A, Alseiari M, Mahboub B. Economic burden of asthma in Abu Dhabi: a retrospective study. Clin Outcomes Res. 2014;6:445–450. doi:10.2147/CEOR.S68920
17. World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD): World Health Organization; 2004.
18. Statista Research Department. Consumer price index for medical care in the United Arab Emirates from 2012 to 2019: Statista Research Department; 2021.
19. University of British Columbia. Pacific Exchange Rate Service. Available from: http://fx.sauder.ubc.ca/data.html.
20. International monetary fund. Consumer price index (CPI). Available from: https://data.imf.org/?sk=4FFB52B2-3653-409A-B471-D47B46D904B5&sId=1485878802128.
21. Statistics Centre - Abu Dhabi. Statistical Yearbook. Statistics Centre - Abu Dhabi; 2019.
22. Nurmagambetov T, Kuwahara R, Garbe P. The economic burden of asthma in the United States, 2008–2013. Ann Am Thorac Soc. 2018;15(3):348–356. doi:10.1513/AnnalsATS.201703-259OC
23. Asthma society of Ireland. Easing the Economic Burden of Asthma. Asthma society of Ireland; 2019.
24. Bedouch P, Marra CA, FitzGerald JM, Lynd LD, Sadatsafavi M. Trends in asthma-related direct medical costs from 2002 to 2007 in British Columbia, Canada: a population based-cohort study. PLoS One. 2012;7:12. doi:10.1371/journal.pone.0050949
25. O’Neill S, Sweeney J, Patterson CC, et al. The cost of treating severe refractory asthma in the UK: an economic analysis from the British Thoracic Society Difficult Asthma Registry. Thorax. 2015;70(4):376–378. doi:10.1136/thoraxjnl-2013-204114
26. Cisternas MG, Blanc PD, Yen IH, et al. A comprehensive study of the direct and indirect costs of adult asthma. J Allergy Clin Immunol. 2003;111(6):1212–1218. doi:10.1067/mai.2003.1449
27. Al-Maskari F, El-Sadig M, Nagelkerke N. Assessment of the direct medical costs of diabetes mellitus and its complications in the United Arab Emirates. BMC Public Health. 2010;10(1):679. doi:10.1186/1471-2458-10-679
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.