")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Dipeptidyl peptidase-4 inhibitors as add-on therapy to insulin in patients with type 2 diabetes mellitus: a meta-analysis of randomized controlled trials
Authors Wang N , Yang T, Li J, Zhang X
Received 18 January 2019
Accepted for publication 7 June 2019
Published 22 August 2019 Volume 2019:12 Pages 1513—1526
DOI https://doi.org/10.2147/DMSO.S202024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Na Wang,1 Tao Yang,2 Jie Li,2 Xianfeng Zhang2
1Department of Endocrinology, The Affiliated Hospital of Jining Medical University, Jining 272000, People’s Republic of China; 2The 4th Department of Psychiatry, Jining Psychiatric Hospital, Jining 272000, People’s Republic of China
Correspondence: Na Wang
Department of Endocrinology, The Affiliated Hospital of Jining Medical University, No. 89 Guhuai Road, Jining 272000, People’s Republic of China
Tel +86 0 537 290 3399
Fax +86 0 537 290 3399
Email [email protected]
Purpose: Addition of the dipeptidyl peptidase-4 (DPP4) inhibitors to insulin in patients with type 2 diabetes mellitus (T2DM) may achieve better glycemic control. However, results of pilot randomized controlled trials (RCTs) are inconsistent. We aimed to perform a meta-analysis of RCTs to evaluate efficacy and safety of DPP4 inhibitors compared with placebo/no treatment as add-on therapy to insulin in T2DM patients.
Materials and methods: Relevant studies were identified via a search of PubMed, Cochrane Library, and Embase databases. A fixed or random effect model was applied according to the heterogeneity.
Results: Overall, 22 RCTs with 6,957 T2DM patients were included. Addition of DPP4 inhibitors to insulin was associated with significantly reduced HbA1c as compared with controls (weighed mean difference [WMD]: −0.54%, p<0.001). The benefits of DPP4 inhibitors as add-on therapy on HbA1c were independent of study design, follow-up duration, categories of DPP4 inhibitors used, and using of fixed/adjustable insulin doses as indicated by predefined subgroup analyses. Moreover, addition of DPP4 inhibitors to insulin was associated with significantly reduced fasting blood glucose (WMD: −0.47mmol/L, p<0.001), postprandial glucose at 2 hrs (WMD: −2.03 mmol/L, p<0.001), and daily dose of insulin (WMD: −2.73U/d, p<0.001), while body weight (WMD: 0.02 g, p=0.81) or risk of symptomatic hypoglycemia (risk ratio: 0.92, p=0.37) were not affected.
Conclusions: Addition of DPP4 inhibitors to insulin significantly improved the glycemic control in T2DM patients without further increasing the risk of weight gain and hypoglycemia.
Keywords: dipeptidyl peptidase-4 inhibitors, insulin, add-on therapy, diabetes mellitus, meta-analysis
Introduction
The incidence of type 2 diabetes mellitus (T2DM) is increasing rapidly worldwide.1–3 Pathophysiologically, patients with T2DM are characterized by insulin resistance and lack of insulin secretion by the β cells of the pancreatic islet.4,5 Although initial treatment with oral antidiabetic drugs (OADs) is effective for glycemic control in T2DM patients, with the deterioration of the β cells of the pancreatic islet during the progression of the disease, exogenous insulin injection is eventually needed.6,7 Currently, multiple regimens of insulin injections are applied in clinical practice, such as basal insulin treatment, basal and premeal bolus insulin injections, and premix insulin treatments, and with which, satisfying glycemic control can be achieved in most T2DM patients.8–10 However, insulin treatment is associated with adverse events including gain of body weight (BW) and hypoglycemia, which are related to the increase of the daily insulin dose.11,12 Therefore, exploring an optimized add-on therapy to insulin is of clinical significance for the improvement of glycemic control and reducing the risk of adverse events in T2DM patients with insulin injections.
Conventionally, many OADs exert their hypoglycemic efficacies via insulin-dependent mechanisms, such as stimulation of endogenous insulin secretion and improvement of peripheral insulin resistance.13–15 The dipeptidyl peptidase-4 (DPP4) inhibitors are a novel group of OADs which exert hypoglycemic efficacy via inhibiting the degradation of gastrointestinal incretins including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP).16,17 Increased GLP-1 and GIP resulted from DPP4 inhibiting, potentiate glucose-stimulated insulin secretion, which is complementary to the direct insulin injection in T2DM patients.18 Moreover, unlike GLP-1 receptor agonists, DPP4 inhibitors can be orally administered, do not reduce BW, and do not cause serious gastrointestinal adverse reactions.19,20 Therefore, theoretically, combination of DPP4 inhibitors and insulin treatment may exert beneficial effects in T2DM patients compared to intensive insulin therapy. In fact, some pilot randomized controlled trials (RCTs) have evaluated the efficacies of DPP4 inhibitors as add-on therapy to insulin in T2DM patients.21–42 However, the scales of these RCTs are generally small and the results of them are not always consistent. Although two previous meta-analyses were performed to evaluate the efficacy of the addition of DPP4 inhibitors to insulin therapy in T2DM patients, these two studies are with certain methodological flaws.43,44 One of them included RCTs with active OADs in the control arm, which makes it difficult to interpret the results.43 The other one only included RCTs with stable insulin regimens, and studies with insulin dose titration were excluded, leading to the missing of the important study data.44 In addition, some recently published studies were not included in the previous meta-analysis, and the influences of patient and study characteristics on the hypoglycemic efficacy of DPP4 inhibitors added-on to insulin have not been determined. Therefore, we aimed to perform an updated meta-analysis to evaluate the overall effects of DPP4 inhibitors as add-on therapy to insulin in T2DM patients. Furthermore, particular attention will be paid regarding the influences of study design, patient characteristics, and categories of DPP4 inhibitors on the glycemic control efficacy in T2DM patients receiving a combined therapy with DPP4 inhibitors and insulin.
Methods
This meta-analysis was designed and performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses45 and the Cochrane Handbook guidelines.46
Search strategy
We searched the Medline (PubMed), Embase (Ovid), and CENTER (Cochrane Library) databases using the combination of the following terms: (1) “DPP4”, “DPP-4”, “dipeptidyl peptidase-4 inhibitors”, “sitagliptin”, “vildagliptin”, “linagliptin”, “saxagliptin”, “alogliptin”, “dutogliptin”, “aemigliptin”, “anagliptin”, “teneligliptin”, “trelagliptin”, or “omarigliptin”; (2) “insulin”; and (3) “random”, “randomly”, or “randomized”. The date of the final database search was October 18, 2018. We limited the search to clinical studies in humans. The references of related original and review articles were manually searched for potential studies.
Study selection
Studies that met the following criteria were included: (1) full-length articles in English; (2) RCTs with a parallel design; (3) included patients with confirmed T2DM; (4) assigned patients to either an oral DPP4 inhibitor intervention group or a placebo or no treatment control group, combined with insulin therapy with or without background OADs; (5) with at least ten patients in each arm; (6) with treatment duration of at least eight weeks; and (7) data of at least one of the following outcomes could be extracted or estimated, including glycosylated hemoglobin (HbA1c), fasting blood glucose (FBG), postprandial glucose at 2 hrs (PPG2h), daily insulin dose, changes of BW, and the incidence of symptomatic hypoglycemia events. We applied no limitations to insulin regimens (basal only, basal and premeal bolus, or premix insulin) in this study. Review articles, preclinical studies, and studies comparing DPP4 inhibitors with other active OADs as add-on therapy to insulin were excluded.
Data extraction and quality assessment
Literature search, data extraction, and quality assessment were performed by two authors independently. Discrepancies were resolved by consensus with a third author. The Cochrane Risk of Bias Tool46 was applied for study quality evaluation.
Statistical analysis
The meta-analysis and statistical analysis were performed with RevMan (Version 5.1; Cochrane Collaboration, Oxford, UK) and Stata (version 12.0; Stata Corporation, College Station, TX) software. The primary outcome of this meta-analysis was the difference between changes of HbA1c from baseline in DPP4 inhibitors and controls. The secondary outcomes included changes of FBG, PPG2h, daily insulin dose, BW, and the incidence of hypoglycemia. The effect of a continuous variable was presented as a weighed mean difference (WMD) with the 95% CI, while for a categorized variable, a risk ratio (RR) with the 95% CI was used. Heterogeneity was evaluated by Cochrane’s Q test,46 and significant heterogeneity was considered if p<0.10. The I2 statistic, indicating the percentage of total variation across studies, was also calculated as a description of heterogeneity.47 A random effect model was used if significant heterogeneity was detected; otherwise, a fixed effect model was applied. For studies with the more than one interventional arm, multiple comparisons were considered and included in the meta-analysis separately. Subgroup analyses were performed to evaluate the potential influence of predefined study and patient characteristics on HbA1c, including study design, sample size, mean age of the patients, follow-up duration, whether titration of insulin dose was applied, and which DPP4 inhibitor was used. Publication bias was assessed by visual inspection of the symmetry of the funnel plot48 and Egger’s regression asymmetry test.46 P-values were two-tailed, and statistical significance was set at P<0.05.
Results
Study selection
The process of study selection is summarized in Figure 1. Briefly, 1,851 studies were obtained via initial database search, and 51 potentially relevant studies were retrieved after selection based on titles and abstracts. Subsequently, 22 studies21–42 were included in the meta-analysis after further excluding of 29 studies based on the following reasons: six were not RCTs, eight were not with addition of DPP4 inhibitors to insulin as intervention, eight were with follow-up durations <8 weeks, one was with <10 patients in each study arm, two were with combination of active OADs (sulfonylureas or glinides) and insulin in controls, and the other four were repeated reports of the included RCTs.
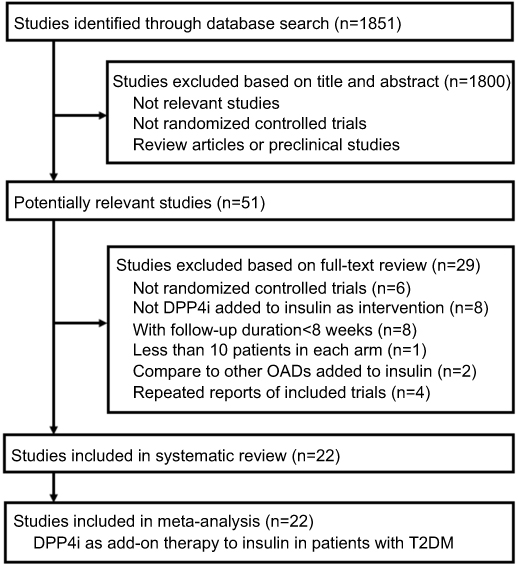 |
Figure 1 Summarized flowchart of literature search. |
Study characteristics and quality evaluation
Overall, 22 RCTs with 6,957 T2DM patients were included in the meta-analysis.21–42 One study22 included two intervention arms with alogliptin 12.5 mg/d and 25 mg/d, respectively, and two comparisons were considered for this study, which were included for analysis separately. The characteristics of the included RCTs are shown in Table 1. Briefly, the mean ages of the included patients varied from 51.0 to 69.1 years, and the baseline HbA1c ranged between 7.5% and 9.3%. Sitagliptin was the most frequently used DPP4 inhibitors in these studies, followed by vildagliptin, alogliptin, saxagliptin, linagliptin, and teneligliptin. Most of the included studies included patients with various regimens of insulins, while two studies only included patients with basal insulin32,35 and another study31 included patients with premix insulin (BIAsp30) only. The follow-up durations varied from 12 to 104 weeks. The doses of insulin were maintained stable in both arms in most of the included RCTs except for eight studies, in which the titration of insulin dose was allowed according to predefined algorithms.30,31,34–36,38,39,42 The summary of quality evaluation via a Cochrane’s Risk of Bias Tool is shown in Table 2. Overall, the quality of the included studies was moderate. Fourteen studies were double-blinded and placebo-controlled RCTs.21–24,26–30,32,37,39,40,42 Methods of random sequence generation were reported in seven studies,23,26,28,36,38–40 while the strategies for allocation concealment were only reported in one study.40
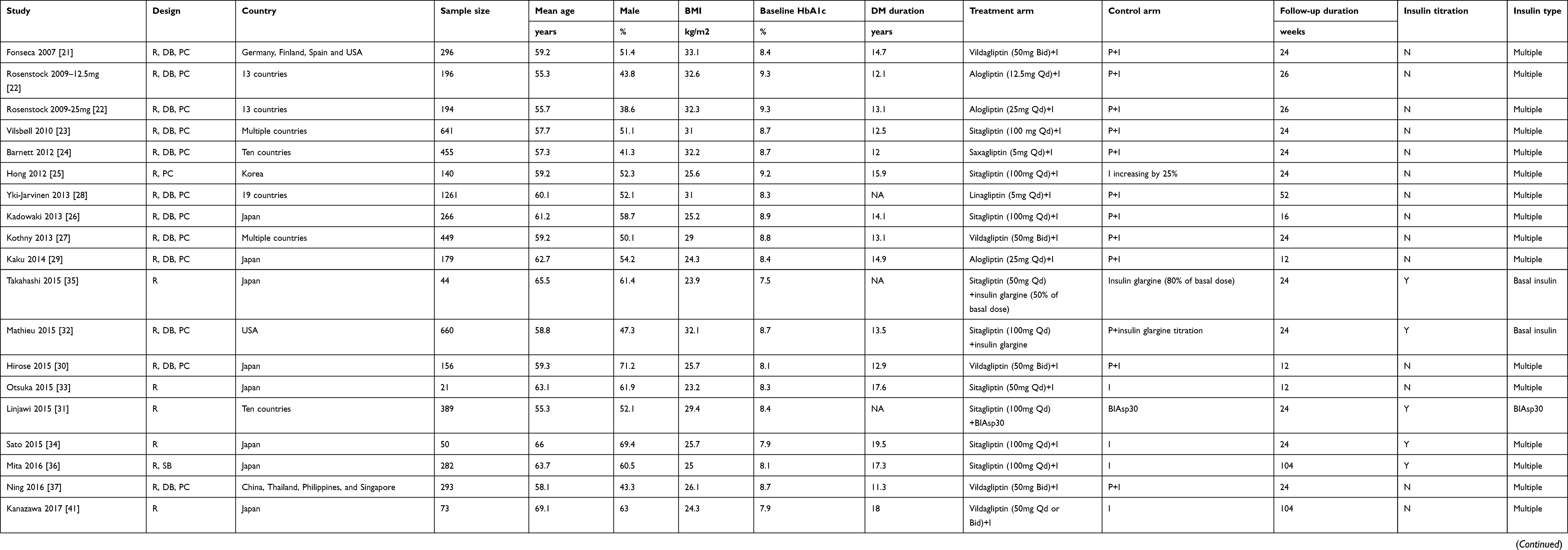 |
Table 1 Characteristics of the included RCTs |
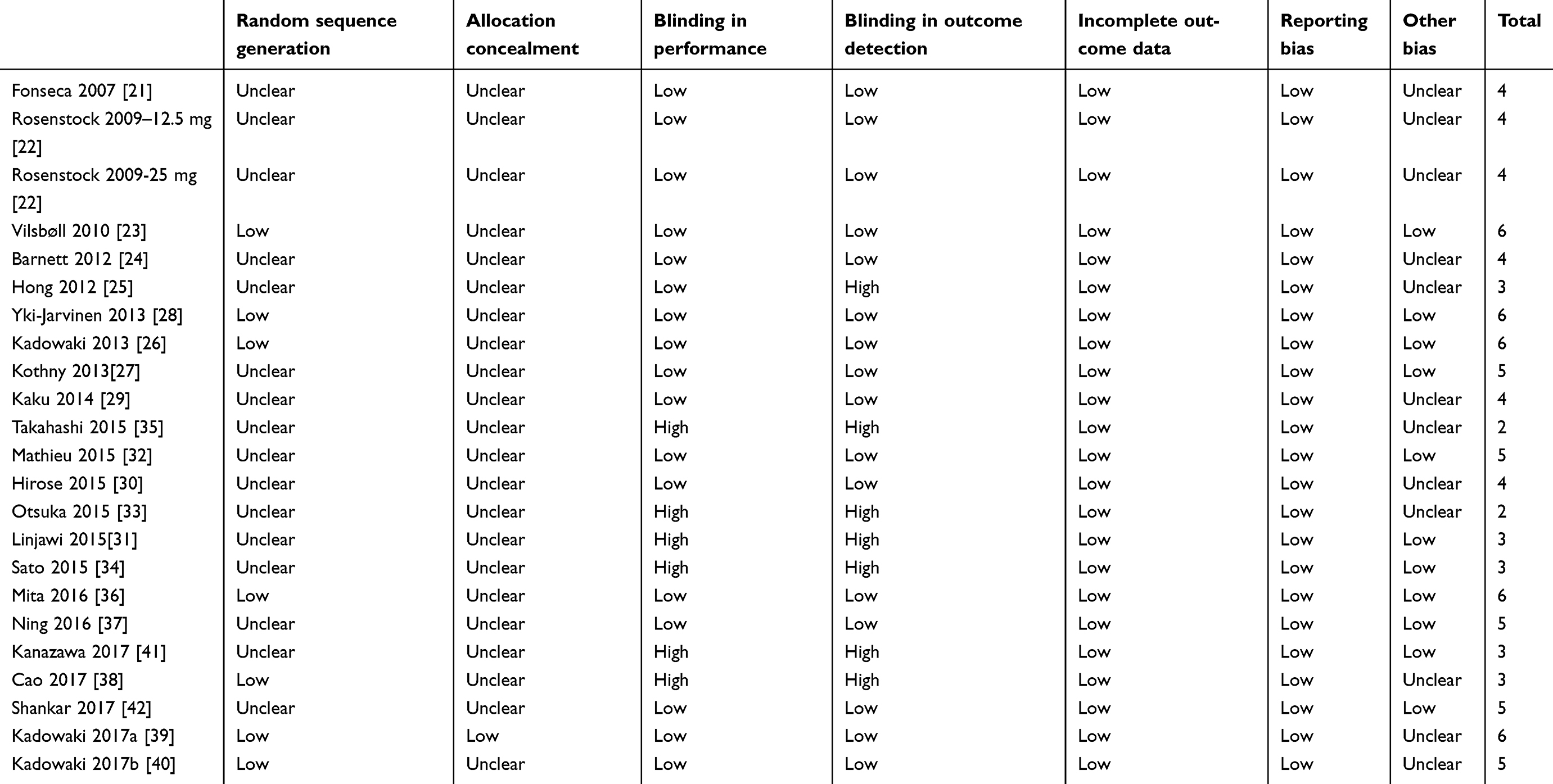 |
Table 2 Quality evaluation of the included RCTs via Cochrane’s risk of bias tool |
Effects of addition of DPP4 inhibitors to insulin on HbA1c
Meta-analysis with 22 studies showed that addition of DPP4 inhibitors to insulin was associated with significantly reduced HbA1c as compared with controls (WMD: −0.54%, 95% CI: −0.66 to −0.42, p<0.001; Figure 2A) with significant heterogeneity (I2=82%, p for Cochrane’s Q test <0.001). Subsequent results of subgroup analyses showed that the effects of addition DPP4 inhibitors to insulin on HbA1c were consistent regardless of the study design characteristics, sample sizes of the RCTs, mean ages of the patients, follow-up durations of the studies, categories of the DPP4 inhibitors, or whether a stable or an up-titrated insulin dose was applied (Table 3). Interestingly, we found that the benefit of addition of DPP4 inhibitors to insulin on HbA1c was more remarkable in double-blinded, placebo-controlled RCTs, indicating the robustness of the findings. Moreover, trends could be observed that benefits of addition of DPP4 inhibitors to insulin on HbA1c may be more remarkable in short-term studies (<24 weeks) as compared with long-term studies (>24 weeks, p for subgroup difference =0.06), and in studies with stable insulin dose as compared with those with insulin dose titration (p for subgroup difference =0.05).
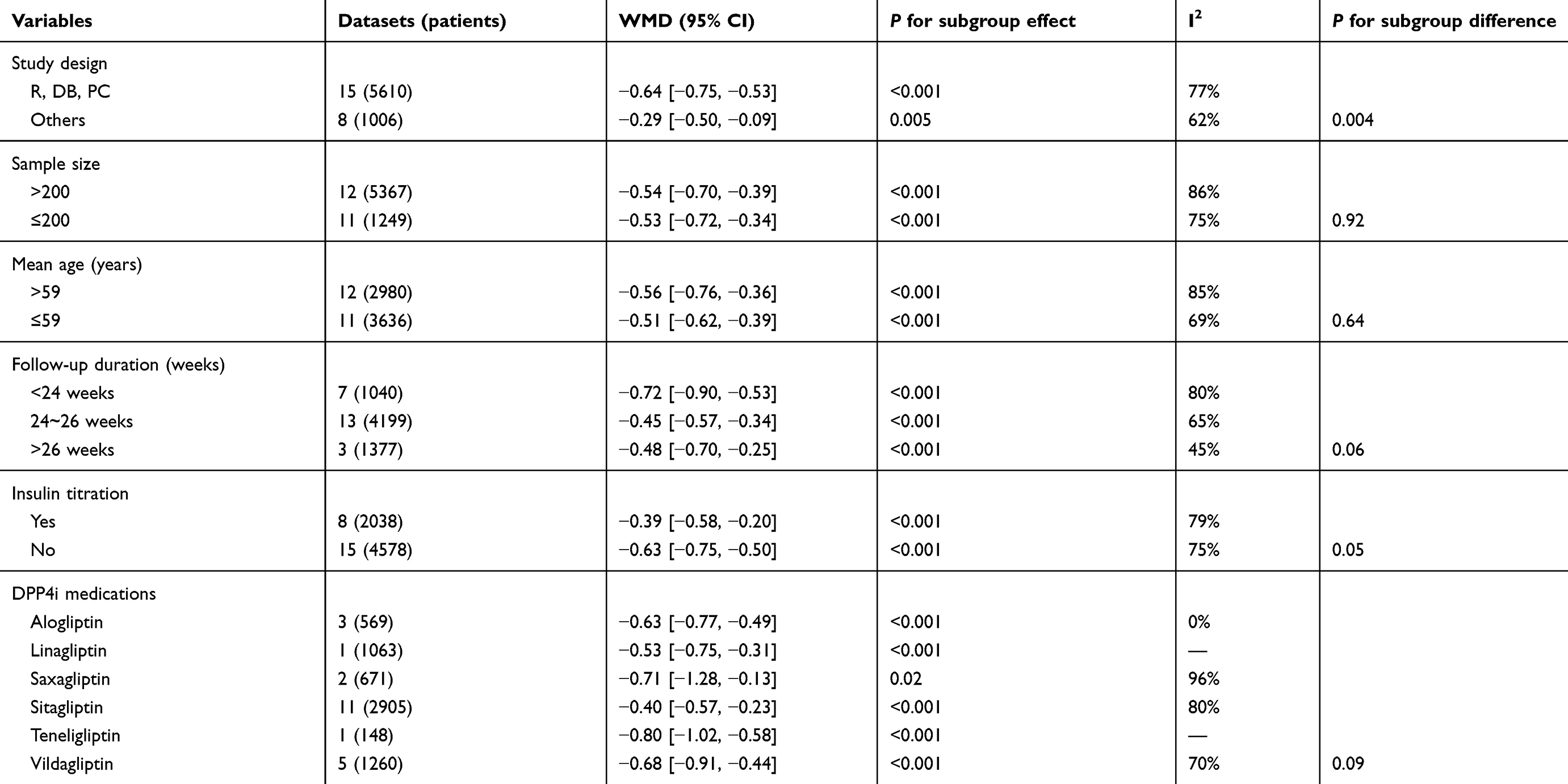 |
Table 3 Subgroup analysis for the effects of DPP4i combined with insulin on HbA1c |
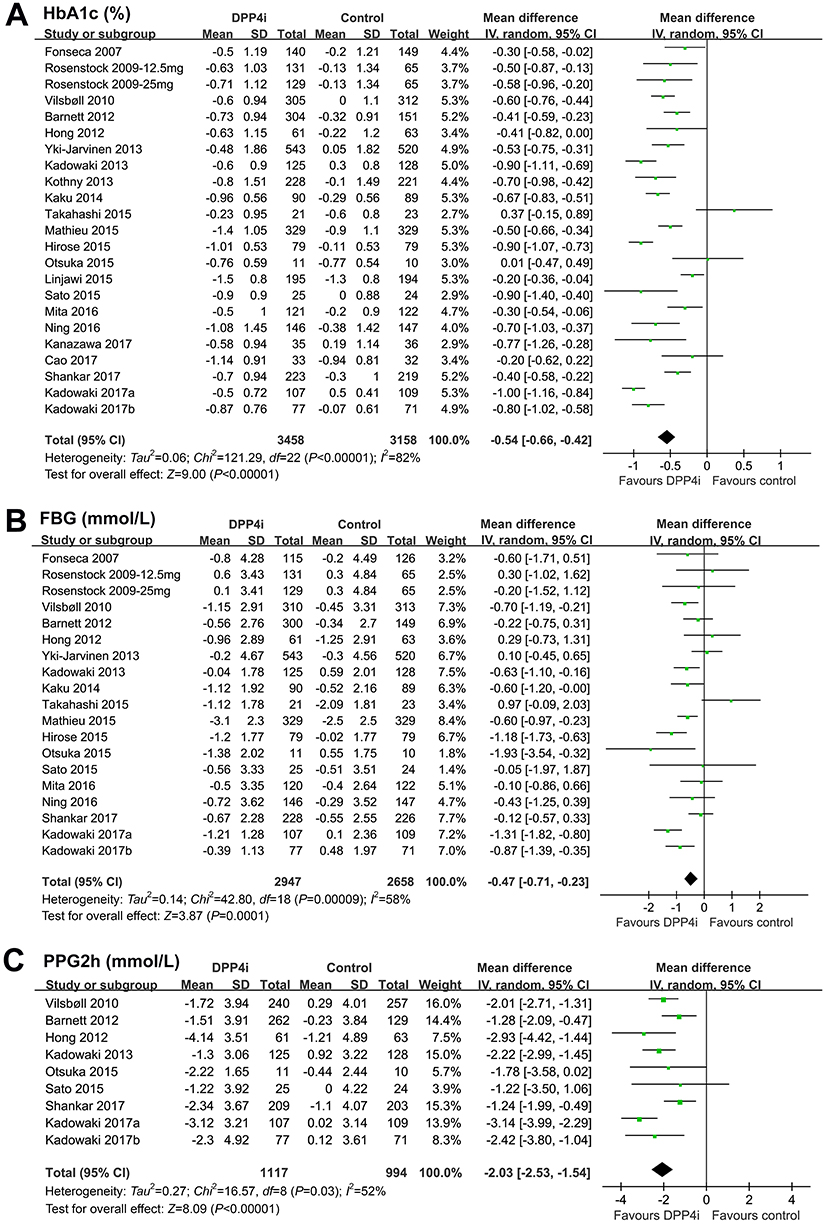 |
Figure 2 Forest plots for the meta-analyses of addition of the dipeptidyl peptidase-4 inhibitors to insulin on glycemic control in patients with type 2 diabetes mellitus. (A) HbA1c (%); (B) fasting blood glucose (mmol/L); and (C) postprandial glucose at 2 hrs. |
Effects of addition of DPP4 inhibitors to insulin on FBG and PPG2h
The pooled results showed that addition of DPP4 inhibitors to insulin was associated with significantly reduced FBG (WMD: −0.47 mmol/L, 95% CI: −0.71 to −0.23, p<0.001; I2=58%; Figure 2B) and PPG2h (WMD: −2.03 mmol/L, 95% CI: −2.53 to −1.54, p<0.001; I2=52%; Figure 2C) as compared with controls.
Effects of addition of DPP4 inhibitors to insulin on daily insulin dose, BW, and hypoglycemic events
Addition of DPP4 inhibitors to insulin was found to be associated with a significantly reduced daily dose of insulin (WMD: −2.73U/d, 95% CI: −3.96 to −1.51, p<0.001; I2=70%; Figure 3A) as compared with controls. Moreover, addition of DPP4 inhibitors to insulin did not significantly affect BW (WMD: 0.02 Kg, 95% CI: −0.16 to 0.20, p=0.81; I2=32%; Figure 3B) or risk of symptomatic hypoglycemia (RR: 0.92, 95% CI: 0.78 to 1.10, p=0.37; I2=60%; Figure 3C) as compared with controls.
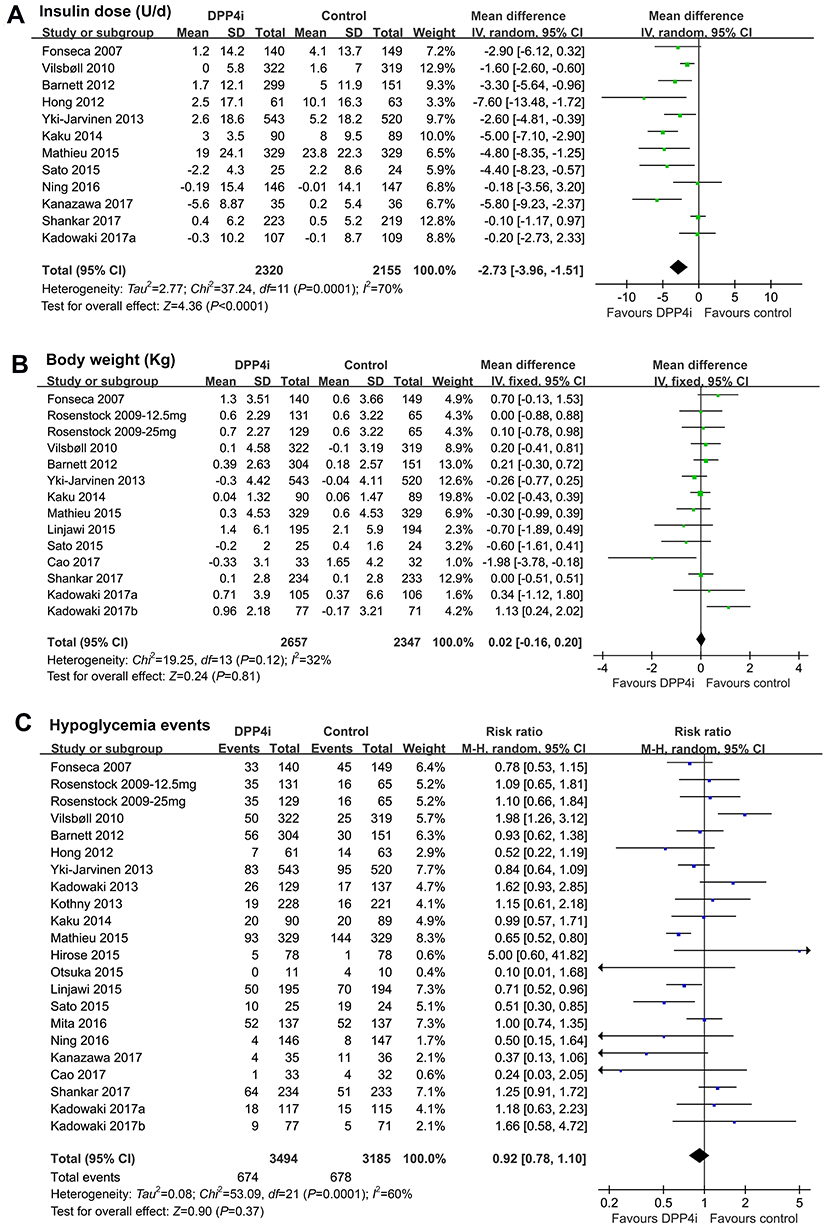 |
Figure 3 Forest plots for the meta-analyses of addition of the dipeptidyl peptidase-4 inhibitors to insulin on daily insulin dose and safety outcomes. (A) daily insulin dose (U/d); (B) body weight (kg); and (C) incidence of systematic hypoglycemia. |
Publication bias
The funnel plots for the effects of DPP4 inhibitors as add-on therapy to insulin compared with controls on HbA1c, FBG, PPG2h, daily insulin dose, BW, and incidence of symptomatic hypoglycemic events are shown in Figure 4A–F, which were all symmetrical on visual inspection symmetrical on visual inspection, suggesting no significant publication biases. These findings were further supported by the results of Egger’s regression tests (p=0.312, 0.432, 0.237, 0.539, 0.418, and 0.602, respectively).
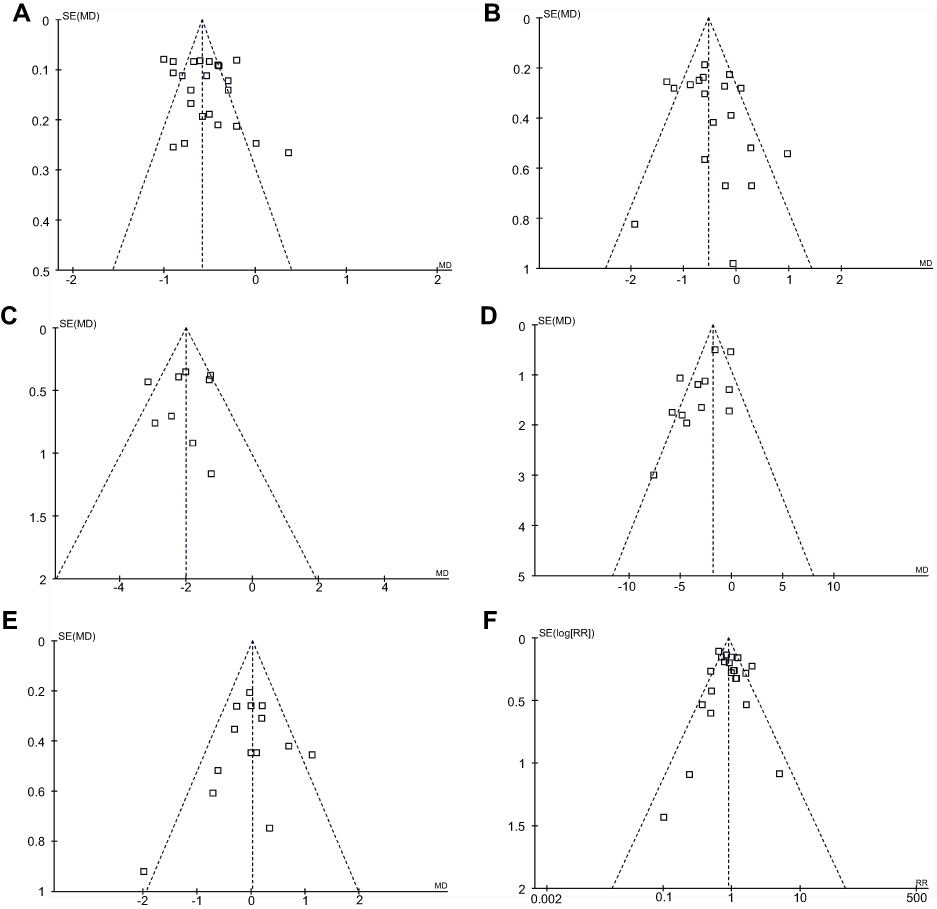 |
Figure 4 Funnel plots for the meta-analyses. (A) HbA1c (%); (B) fasting blood glucose (mmol/L); (C) postprandial glucose at 2 hrs; (D) daily insulin dose (U/d); (E) body weight (kg); and (F) incidence of systematic hypoglycemia. |
Discussion
In this meta-analysis of RCTs, we found that addition of DPP4 inhibitors to insulin significantly improved the glycemic control in T2DM patients as compared with placebo/no treatment to insulin. Moreover, the benefits of DPP4 inhibitors as an add-on therapy to insulin on glycemic control were consistent regardless of the study design, follow-up duration, and categories of DPP4 inhibitors used. In addition, the benefits of DPP4 inhibitors as an add-on therapy to insulin on glycemic control were observed not only in studies with stable insulin dose, but also in studies with insulin dose titration. Besides, the addition of DPP4 inhibitors to insulin significantly reduced daily insulin dose, without significant influences on BW or risk of hypoglycemia. These results suggested that DPP4 inhibitors as an add-on therapy to insulin improved glycemic control without further increasing the risk of weight gain and hypoglycemia in patients with T2DM.
Previously, two meta-analyses performed by Chen et al43 and Kim et al44 have been published concerning the efficacy of DPP4 inhibitors as add-on therapy to insulin. Our study is different from the previous two meta-analyses in the following aspects. Firstly, the meta-analysis by Chen et al included RCTs comparing the effect between DPP4 inhibitors and placebo/no treatment/active OADs as add-on therapies to insulin.43 The various regimens of controls in this meta-analysis may confound the results. In the meta-analysis by Kim et al, the authors focused on studies with stable insulin dose, while the potential glycemic benefits of addition of DPP4 inhibitors to insulin with adjustable dose therefore cannot be confirmed.44 However, in our meta-analysis, we included all RCTs comparing the effect of DPP4 inhibitors and placebo/no treatment controls as add-on therapies to insulin in T2DM patients, and the dose of insulin in the included RCTs could be stable or adjustable (titration) during the study periods. Secondly, the numbers of included RCTs (seven in meta-analysis of Chen et al, nine in meta-analysis of Kim et al, and 22 in our meta-analysis) and the overall patients (3,384 in meta-analysis of Chen et al, 4,464 in meta-analysis of Kim et al, and 6,957 in our meta-analysis) were much larger in our study than the previous ones, which makes our study with larger statistical power to show a significantly improved FBG and PPG2h in DPP4 inhibitor groups. Thirdly, the large scale of the current meta-analysis allowed us to perform subgroup analysis for the influence of the combined treatment with DPP4 inhibitors and insulin on HbA1c. Generally, the results of our meta-analysis are consistent with the previous two meta-analyses,43,44 which showed that addition of DPP4 inhibitors to insulin improved glycemic control in T2DM patients. Moreover, results of our subgroup analyses showed that the benefits of DPP4 inhibitors as an add-on therapy to insulin on glycemic control were consistent regardless of the study design, follow-up duration, and categories of DPP4 inhibitors used. Finally, we found that benefits of DPP4 inhibitors as an add-on therapy to insulin on glycemic control were observed not only in studies with stable insulin dose, but also in studies with insulin dose titration. These results implied that in T2DM patients that are inadequately controlled by insulin, adding DPP4 inhibitors to insulin may be superior in glycemic control as compared with the up-titration of the insulin dose.
The synergetic effect of the addition of DPP4 inhibitors to insulin therapy on glycemic control may be explained by the potential insulin-independent hypoglycemic effect of DPP4 inhibitors. The DPP4 inhibitors prevent the degradation of gastrointestinal incretins including GLP-1and GIPs, thereby improving glycemic control via various mechanisms besides stimulation of insulin secretion, such as glucagon suppression.49 The complementary actions of DPP4 inhibitors to insulin therapy may be the fundamental reasons for the benefits of combined therapy on glycemic control. This is also reflected by one of the findings from our meta-analysis which showed a significantly reduced daily insulin dose in patients receiving combined therapy with DPP4 inhibitors and insulin. Moreover, our meta-analysis showed that addition of DPP4 inhibitors to insulin did not the risks of BW gain and hypoglycemia. This is not surprising since DPP4 inhibitors are confirmed to have no significant influence on BW and with low risk of hypoglycemic events.19 Additionally, patients from the combined therapy group had lower daily insulin dose than controls as evidenced by the results of our meta-analysis, which may also be a potential reason that the combined treatment did not significantly increase the risk of adverse events such as weight gain and hypoglycemia.
Our study has limitations. Firstly, our study is a study-level-based meta-analysis. Results of subgroup analysis according to the study or patient characteristics (such as mean ages, and follow-up duration) should be interpreted with caution since we did perform the stratified analyses based on the individual patient data. Secondly, significant heterogeneity remains in some outcomes of our meta-analysis, and differences in the regimens of insulin treatment of the included RCTs may contribute to the heterogeneity. However, subgroup analyses according to the regimens of insulin treatment could not be performed since most of the RCTs included patients with mixed insulin regimens, while stratified data were rarely available. In one of the included RCTs, addition of sitagliptin various regimens of insulin, including premixed, immediate-acting, and long-acting insulin showed similar efficacies on HbA1c reduction in T2DM patients.23 Similarly, a recent post-hoc analysis of two clinical trials showed that sitagliptin in combination with premixed insulin achieved better glycemic control than premixed insulin alone.50 Therefore, whether addition of DPP4 inhibitors to different regimens of insulin treatment confers similar benefits remains to be determined. Thirdly, the comparative efficacies between DPP4 inhibitors and other active OADs as add-on therapies to insulin cannot be determined based on our results, and direct comparative RCTs are lacking. Previous meta-analyses based on indirect comparisons showed that DPP4 inhibitors may be inferior to sodium glucose cotransporter 2 inhibitors,51 but similar to thiazolidinedione and GLP-1 receptor agonists in glycemic control as add-on therapies to insulin in T2DM patients.52 However, these results should be validated in head-to-head RCTs. Fourthly, whether addition of DPP4 inhibitors to insulin improves the clinical outcome should be evaluated in future studies.
In conclusion, results of our meta-analysis showed that addition of DPP4 inhibitors to insulin significantly improved the glycemic control in T2DM patients without further increasing the risk of weight gain and hypoglycemia. The benefits of DPP4 inhibitors as add-on therapy on glycemic control were independent of study design, follow-up duration, categories of DPP4 inhibitors used, and using of fixed/adjustable insulin doses. The DPP4 inhibitors as an add-on therapy to insulin should be considered in T2DM patients in clinical practice.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lascar N, Brown J, Pattison H, Barnett AH, Bailey CJ, Bellary S. Type 2 diabetes in adolescents and young adults. Lancet Diabetes Endocrinol. 2018;6(1):69–80. doi:10.1016/S2213-8587(17)30186-9
2. Yang W, Lu J, Weng J, et al. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362(12):1090–1101. doi:10.1056/NEJMoa0908292
3. Worldwide trends in diabetes since. 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. 2016;387(10027):1513–1530. doi:10.1016/S0140-6736(16)00618-8
4. Czech MP. Insulin action and resistance in obesity and type 2 diabetes. Nat Med. 2017;23(7):804–814. doi:10.1038/nm.4350
5. Valaiyapathi B, Gower B, Ashraf AP. Pathophysiology of type 2 diabetes in children and adolescents. Curr Diabetes Rev. 2018. doi:10.2174/1573399814666180608074510
6. Chamberlain JJ, Herman WH, Leal S, et al. Pharmacologic therapy for type 2 diabetes: synopsis of the 2017 American Diabetes Association Standards of Medical Care in Diabetes. Ann Intern Med. 2017;166(8):572–578. doi:10.7326/M16-2937
7. Weng J, Ji L, Jia W, et al. Standards of care for type 2 diabetes in China. Diabetes Metab Res Rev. 2016;32(5):442–458. doi:10.1002/dmrr.2827
8. Raccah D, Huet D, Dib A, et al. Review of basal-plus insulin regimen options for simpler insulin intensification in people with Type 2 diabetes mellitus. Diabet Med. 2017;34(9):1193–1204. doi:10.1111/dme.13390
9. Giugliano D, Sieradzki J, Stefanski A, Gentilella R. Personalized intensification of insulin therapy in type 2 diabetes – does a basal-bolus regimen suit all patients? Curr Med Res Opin. 2016;32(8):1425–1434. doi:10.1080/03007995.2016.1181051
10. Wang C, Mamza J, Idris I. Biphasic vs basal bolus insulin regimen in Type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabet Med. 2015;32(5):585–594. doi:10.1111/dme.12694
11. Goh SY, Hussein Z, Rudijanto A. Review of insulin-associated hypoglycemia and its impact on the management of diabetes in Southeast Asian countries. J Diabetes Investig. 2017;8(5):635–645. doi:10.1111/jdi.12647
12. Brown A, Guess N, Dornhorst A, Taheri S, Frost G. Insulin-associated weight gain in obese type 2 diabetes mellitus patients: what can be done? Diabetes Obes Metab. 2017;19(12):1655–1668. doi:10.1111/dom.13009
13. Stein SA, Lamos EM, Davis SN. A review of the efficacy and safety of oral antidiabetic drugs. Expert Opin Drug Saf. 2013;12(2):153–175. doi:10.1517/14740338.2013.752813
14. Daniels MA, Kan C, Willmes DM, et al. Pharmacogenomics in type 2 diabetes: oral antidiabetic drugs. Pharmacogenomics J. 2016;16(5):399–410. doi:10.1038/tpj.2016.54
15. Del Prato S, Bianchi C, Marchetti P. beta-cell function and anti-diabetic pharmacotherapy. Diabetes Metab Res Rev. 2007;23(7):518–527. doi:10.1002/dmrr.770
16. Waldrop G, Zhong J, Peters M, Rajagopalan S. Incretin-based therapy for diabetes: what a cardiologist needs to know. J Am Coll Cardiol. 2016;67(12):1488–1496. doi:10.1016/j.jacc.2015.12.058
17. Esposito K, Chiodini P, Maiorino MI, Bellastella G, Capuano A, Giugliano D. Glycaemic durability with dipeptidyl peptidase-4 inhibitors in type 2 diabetes: a systematic review and meta-analysis of long-term randomised controlled trials. BMJ Open. 2014;4(6):e005442. doi:10.1136/bmjopen-2014-005442
18. Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet. 2006;368(9548):1696–1705. doi:10.1016/S0140-6736(06)69705-5
19. Ling J, Cheng P, Ge L, et al. The efficacy and safety of dipeptidyl peptidase-4 inhibitors for type 2 diabetes: a Bayesian network meta-analysis of 58 randomized controlled trials. Acta Diabetol. 2019;56(3):249-272.
20. Ostergaard L, Frandsen CS, Madsbad S. Treatment potential of the GLP-1 receptor agonists in type 2 diabetes mellitus: a review. Expert Rev Clin Pharmacol. 2016;9(2):241–265. doi:10.1586/17512433.2016.1121808
21. Fonseca V, Schweizer A, Albrecht D, Baron MA, Chang I, Dejager S. Addition of vildagliptin to insulin improves glycaemic control in type 2 diabetes. Diabetologia. 2007. 50(6):1148–1155. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/414/CN-00609414/frame.html
22. Rosenstock J, Rendell MS, Gross JL, Fleck PR, Wilson CA, Mekki Q. Alogliptin added to insulin therapy in patients with type 2 diabetes reduces HbA1c without causing weight gain or increased hypoglycaemia. Diabetes Obesity Metab. 2009;11(12):1145–1152. doi:10.1111/dom.2009.11.issue-12
23. Vilsbøll T, Rosenstock J, Yki-Järvinen H, et al. Efficacy and safety of sitagliptin when added to insulin therapy in patients with type 2 diabetes. Diabetes Obes Metab. 2010;12(2):167–177. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/573/CN-00769573/frame.html
24. Barnett AH, Charbonnel B, Donovan M, Fleming D, Chen R. Effect of saxagliptin as add-on therapy in patients with poorly controlled type 2 diabetes on insulin alone or insulin combined with metformin. Curr Med Res Opin. 2012. 28(4):513–523. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/728/CN-00842728/frame.html
25. Hong ES, Khang AR, Yoon JW, et al. Comparison between sitagliptin as add-on therapy to insulin and insulin dose-increase therapy in uncontrolled Korean type 2 diabetes: CSI study. Diabetes Obes Metab. 2012;14(9):795–802. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/500/CN-00842500/frame.html
26. Kadowaki T, Tajima N, Odawara M, et al. Efficacy and safety of sitagliptin add-on therapy in Japanese patients with type 2 diabetes on insulin monotherapy. Diabetol Int. 2013;4(3):160–172. doi:10.1007/s13340-013-0109-z
27. Kothny W, Foley J, Kozlovski P, Shao Q, Gallwitz B, Lukashevich V. Improved glycaemic control with vildagliptin added to insulin, with or without metformin, in patients with type 2 diabetes mellitus. Diabetes Obesity Metab. 2013;15(3):252–257. doi:10.1111/dom.12020
28. Yki-Järvinen H, Rosenstock J, Durán-Garcia S, et al. Effects of adding linagliptin to basal insulin regimen for inadequately controlled type 2 diabetes: a ≥52-week randomized, double-blind study. Diabetes Care. 2013;36(12):3875–3881. doi:10.2337/dc12-2718
29. Kaku K, Mori M, Kanoo T, Katou M, Seino Y. Efficacy and safety of alogliptin added to insulin in Japanese patients with type 2 diabetes: a randomized, double-blind, 12-week, placebo-controlled trial followed by an open-label, long-term extension phase. Expert Opin Pharmacother. 2014. 15(15):2121–2130. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/221/CN-01014221/frame.html
30. Hirose T, Suzuki M, Tsumiyama I. Efficacy and safety of vildagliptin as an add-on to insulin with or without metformin in japanese patients with type 2 diabetes mellitus: a 12-week, double-blind, randomized study. Diabetes Ther. 2015. 6(4):559–571. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/281/CN-01125281/frame.html
31. Linjawi S, Sothiratnam R, Sari R, Andersen H, Hiort LC, Rao P. The study of once- and twice-daily biphasic insulin aspart 30 (BIAsp 30) with sitagliptin, and twice-daily BIAsp 30 without sitagliptin, in patients with type 2 diabetes uncontrolled on sitagliptin and metformin - The Sit2Mix trial. Prim Care Diabetes. 2015. 9(5):370–376. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/453/CN-01097453/frame.html
32. Mathieu C, Shankar RR, Lorber D, et al. A randomized clinical trial to evaluate the efficacy and safety of co-administration of sitagliptin with intensively titrated insulin glargine. Diabetes Ther. 2015;6(2):127–142. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/457/CN-01083457/frame.html
33. Otsuka Y, Yamaguchi S, Furukawa A, Kosuda M, Nakazaki M, Ishihara H. Addition of sitagliptin or metformin to insulin monotherapy improves blood glucose control via different effects on insulin and glucagon secretion in hyperglycemic Japanese patients with type 2 diabetes. Endocr J. 2015. 62(2):133–143. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/243/CN-01052243/frame.html
34. Sato S, Saisho Y, Kou K, et al. Efficacy and safety of sitagliptin added to insulin in Japanese patients with type 2 diabetes: the EDIT randomized trial. PLoS One. 2015;10(3):e0121988.
35. Takahashi H, Sakai K, Kawanishi K, et al. Efficacy of switching from premix analog insulin twice daily injection to insulin glargine once daily injection with sitagliptin. Diabetol Int. 2015;6(1):33–38. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/123/CN-01069123/frame.html
36. Mita T, Katakami N, Shiraiwa T, et al. Sitagliptin attenuates the progression of carotid intima-media thickening in insulin-treated patients with type 2 diabetes: the sitagliptin preventive study of intima-media thickness evaluation (SPIKE): a randomized controlled trial. Diabetes Care. 2016;39(3):455–464. doi:10.2337/dc15-2145
37. Ning G, Wang WQ, Li L, et al. Vildagliptin as add-on therapy to insulin improves glycemic control without increasing risk of hypoglycemia in Asian, predominantly Chinese, patients with type 2 diabetes mellitus. J Diabetes. 2016;8(3):345–353. doi:10.1111/1753-0407.12303
38. Cao Y, Gao F, Zhang Q, et al. Efficacy and safety of coadministration of sitagliptin with insulin glargine in type 2 diabetes. J Diabetes. 2017;9(5):502–509. doi:10.1111/1753-0407.12436
39. Kadowaki T, Kondo K, Sasaki N, et al. Efficacy and safety of teneligliptin add-on to insulin monotherapy in Japanese patients with type 2 diabetes mellitus: a 16-week, randomized, double-blind, placebo-controlled trial with an open-label period. Expert Opin Pharmacother. 2017;18(13):1291–1300. doi:10.1080/14656566.2017.1359259
40. Kadowaki T, Muto S, Ouchi Y, Shimazaki R, Seino Y. Efficacy and safety of saxagliptin in combination with insulin in Japanese patients with type 2 diabetes mellitus: a 16-week double-blind randomized controlled trial with a 36-week open-label extension. Expert Opin Pharmacother. 2017;18(18):1903–1919. doi:10.1080/14656566.2017.1379990
41. Kanazawa I, Tanaka KI, Notsu M, et al. Long-term efficacy and safety of vildagliptin add-on therapy in type 2 diabetes mellitus with insulin treatment. Diabetes Res Clin Pract. 2017;123:9–17. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/601/CN-01301601/frame.html
42. Shankar RR, Bao YQ, Han P, et al. Sitagliptin added to stable insulin therapy with or without metformin in Chinese patients with type 2 diabetes. J Diabetes Investig. 2017;8(3):321–329. doi:10.1111/jdi.12585
43. Chen C, Yu Q, Zhang S, Yang P, Wang CY. Assessing the efficacy and safety of combined DPP-4 inhibitor and insulin treatment in patients with type 2 diabetes: a meta-analysis. Int J Clin Exp Pathol. 2015;8(11):14141–14150.
44. Kim YG, Min SH, Hahn S, Oh TJ, Park KS, Cho YM. Efficacy and safety of the addition of a dipeptidyl peptidase-4 inhibitor to insulin therapy in patients with type 2 diabetes: a systematic review and meta-analysis. Diabetes Res Clin Pract. 2016;116:86–95. doi:10.1016/j.diabres.2016.03.011
45. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2651
46. Higgins J, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0. Cochrane Collab. 2011. Available from: www.cochranehandbook.org
47. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
48. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
49. Cho YM, Merchant CE, Kieffer TJ. Targeting the glucagon receptor family for diabetes and obesity therapy. Pharmacol Ther. 2012;135(3):247–278. doi:10.1016/j.pharmthera.2012.05.009
50. Yu M, Shankar RR, Zhang R, et al. Efficacy and safety of sitagliptin added to treatment of patients with type 2 diabetes inadequately controlled with premixed insulin. Diabetes Obes Metab. 2019;21(2):408–411. doi:10.1111/dom.13517
51. Min SH, Yoon JH, Hahn S, Cho YM. Comparison between SGLT2 inhibitors and DPP4 inhibitors added to insulin therapy in type 2 diabetes: a systematic review with indirect comparison meta-analysis. Diabetes Metab Res Rev. 2017;33(1):e2818. doi:10.1002/dmrr.v33.1
52. Yang W, Cai X, Gao X, Chen Y, Chen L, Ji L. Addition of dipeptidyl peptidase-4 inhibitors to insulin treatment in type 2 diabetes patients: a meta-analysis. J Diabetes Investig. 2018;9(4):813–821. doi:10.1111/jdi.12764
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.