")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Dilemma of prescribing aripiprazole under the Taiwan health insurance program: a descriptive study
Authors Hsu Y, Chou Y, Chang H, Kao Y, Huang S, Tzeng N
Received 9 October 2014
Accepted for publication 6 January 2015
Published 27 January 2015 Volume 2015:11 Pages 225—232
DOI https://doi.org/10.2147/NDT.S75609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Wai Kwong Tang
Yi-Chien Hsu,1,2 Yu-Ching Chou,3 Hsin-An Chang,1,2,4 Yu-Chen Kao,1,2,5 San-Yuan Huang,1,2 Nian-Sheng Tzeng1,2,4
1Department of Psychiatry, Tri-Service General Hospital, Taipei, Taiwan; 2School of Medicine, 3School of Public Health, 4Student Counseling Center, National Defense Medical Center, Taipei, Taiwan; 5Department of Psychiatry, Tri-Service General Hospital, Song-Shan Branch, Taipei, Taiwan
Objectives: Refractory major depressive disorder (MDD) is a serious problem leading to a heavy economic burden. Antipsychotic augmentation treatment with aripiprazole and quetiapine is approved for MDD patients and can achieve a high remission rate. This study aimed to examine how psychiatrists in Taiwan choose medications and how that choice is influenced by health insurance payments and administrative policy.
Design: Descriptive study.
Outcome measures: Eight questions about the choice of treatment strategy and atypical antipsychotics, and the reason to choose aripiprazole.
Intervention: We designed an augmentation strategy questionnaire for psychiatrists whose patients had a poor response to antidepressants, and handed it out during the annual meeting of the Taiwanese Society of Psychiatry in October 2012. It included eight questions addressing the choice of treatment strategy and atypical antipsychotics, and the reason whether or not to choose aripiprazole as the augmentation antipsychotic.
Results: Choosing antipsychotic augmentation therapy or switching to other antidepressant strategies for MDD patients with an inadequate response to antidepressants was common with a similar probability (76.1% vs 76.4%). The most frequently used antipsychotics were aripiprazole and quetiapine, however a substantial number of psychiatrists chose olanzapine, risperidone, and sulpiride. The major reason for not choosing aripiprazole was cost (52.1%), followed by insurance official policy audit and deletion in the claims review system (30.1%).
Conclusion: The prescribing behavior of Taiwanese psychiatrists for augmentation antipsychotics is affected by health insurance policy.
Keywords: major depressive disorder, aripiprazole, psychiatrists, prescribing behavior, antipsychotic augmentation, National Health Insurance program
Introduction
Major depressive disorder (MDD) is a common and recurrent mental illness with a lifetime prevalence of 5%–12% in adult men and 9%–26% in adult women. In spite of recent advances in psychopharmacology, approximately 60% of patients with MDD do not achieve an adequate response or remission to initial antidepressant therapy (ADT) even with adequate dose and duration.1
Common strategies adopted for nonresponders to ADT include switching to other antidepressants, combining therapy with antidepressants of another class, and augmentation strategies with atypical antipsychotics, lithium, or thyroid hormone.2–4 The United States Food and Drug Administration (FDA) has approved aripiprazole and quetiapine as adjunctive treatment for MDD,5 however few studies have been conducted on the actual choices of psychiatrists for nonresponders to ADT.
The prescribing behavior of physicians is influenced by many factors, including evidence-based medical knowledge, training and continuous education, and largely by health insurance and reimbursement or payment policies.6–8 The aim of this study was to examine how Taiwanese psychiatrists prescribe medication and how they are influenced by health insurance payments and administrative policy.
Methods
This descriptive study used an innovative questionnaire for Taiwanese psychiatrists on augmentation strategy for MDD patients with an inadequate response to ADT. The aim of this questionnaire was to examine the influence of health insurance payments and administrative policy on the prescribing behavior of Taiwanese psychiatrists. The first question asked how many MDD outpatients per month each Taiwanese psychiatrists treated. The second question asked about the percentage of poor responders to ADT, and the third question asked about the remission rate of MDD. The fourth question asked about the strategies used for the poor responders to ADT, and the fifth question asked which antipsychotics were chosen for antipsychotic augmentation therapy. The sixth and seventh questions asked why and why not aripiprazole was chosen as the augmentation antipsychotic. The eighth question asked why augmentation antipsychotics were not chosen. We handed out the questionnaire during the annual meeting of the Taiwanese Society of Psychiatry in October 2012.
Statistical analysis
Outpatient visits per month, percentage of poor responders to ADT, remission rate, the strategies used for the poor responders to ADT, and choice of augmentation antipsychotics were presented with numbers and percentages. The answers to questions 4–8 according to the number of MDD outpatients per month were compared using chi-square and Fisher’s exact tests. Analysis of covariance (ANCOVA) was used to analyze the relationship between the answers to questions 4–8 and the number of MDD outpatients per month after including poor response proportion and remission rate as covariates. Multiple logistic regression was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the correlate variables associated with aripiprazole and quetiapine. The IBM SPSS Statistics version 22 (IBM® SPSS® Statistics 22, IBM, New York, NY, USA) was used for statistical analysis, and the significance level (P-value) was set at 0.05.
Results
We collected 324 questionnaires with complete data. The most common strategies for treating MDD patients with an inadequate response to ADT were switching to antidepressants with different mechanisms (76.4%), augmentation with antipsychotics (76.1%), combination with other antidepressants (35.4%), and electroconvulsive therapy (14.6%) (Table 1).
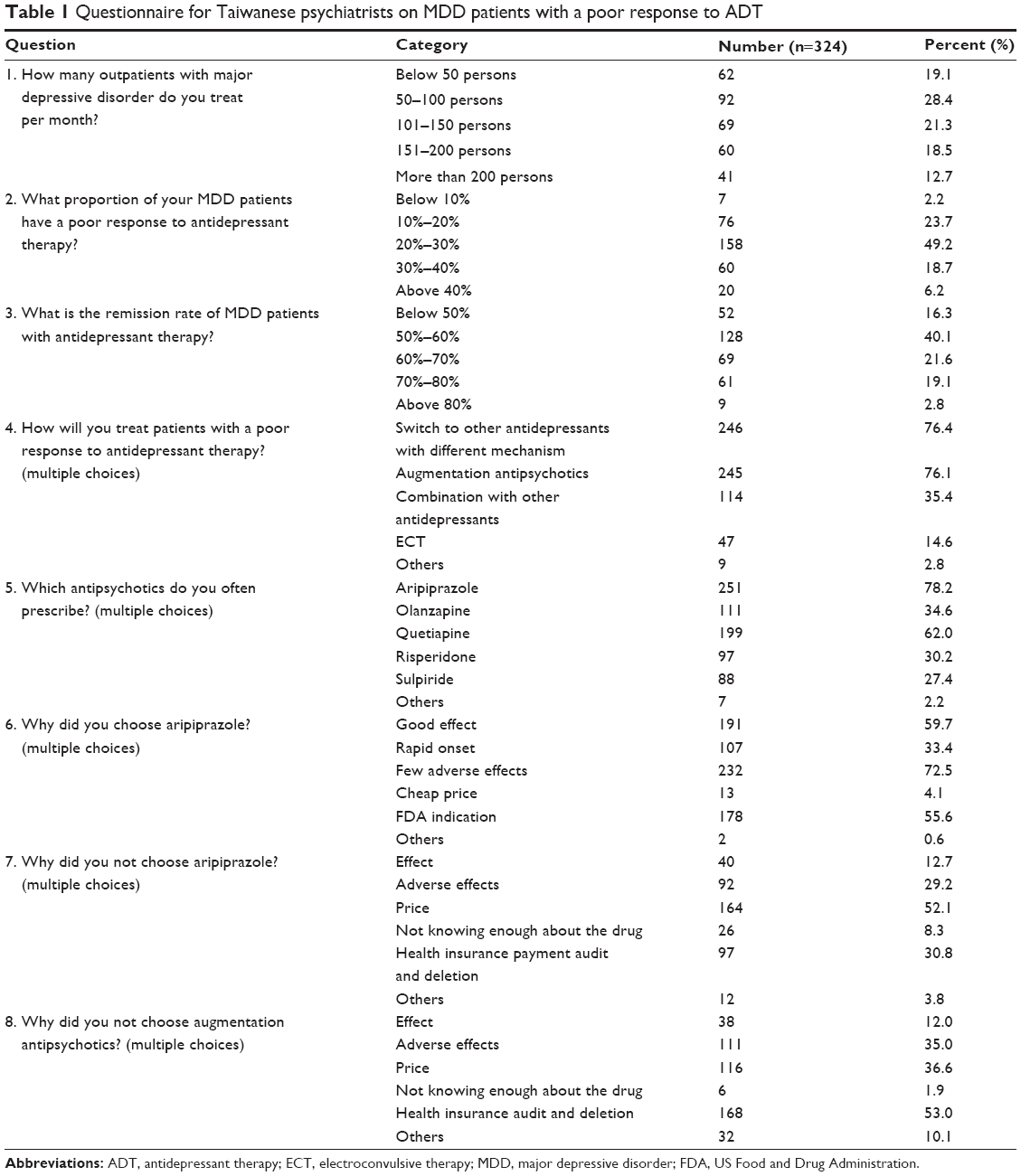 | Table 1 Questionnaire for Taiwanese psychiatrists on MDD patients with a poor response to ADT |
The antipsychotics used for MDD were aripiprazole (78.2%), quetiapine (62%), olanzapine (34.6%), risperidone (30.2%), and sulpiride (27.4%). The reasons psychiatrists chose aripiprazole for augmentation included fewer adverse effects (72.5%), good response (59.7%), FDA indication (55.6%), and rapid onset of action (33.4%). The psychiatrists who chose not to prescribe aripiprazole as the augmentation antipsychotic did so because of price (52.1%), official insurance policy audit and deletion of payments (30.8%), adverse effects (29.2%), response (12.7%), and not knowing enough about the drug (8.3%). Concerns when considering augmentation antipsychotics were insurance audit and deletion (53%), price (36.6%), side effects (35%), response (12%), and not knowing enough about the drug (1.9%) (Table 1).
The data in Table 2 reveals several statistical differences among groups of those who treated different numbers of MDD patients per month (<100, 101–200, and >200), in the antipsychotics chosen, the reasons why they did not choose aripiprazole, and the reasons why they did not choose antipsychotics for augmentation. For example, the reason why psychiatrists in the group of 101–200 treated patients/month, chose not to augment with antipsychotics due to “health insurance payment audit and deletion”, is significantly higher than other groups (76 in 129, 59.4%, P<0.001 in ANCOVA) (Table 2).
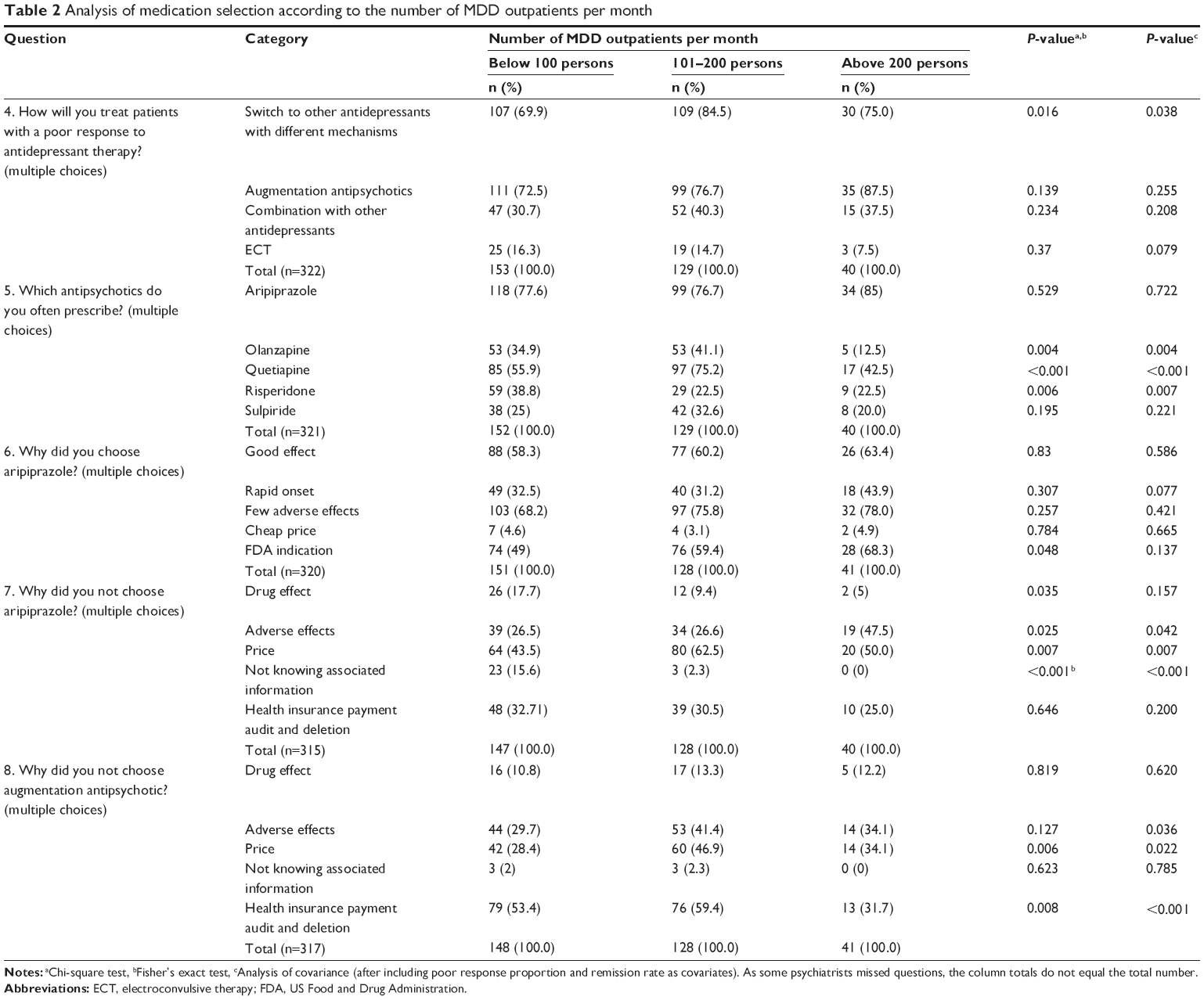 | Table 2 Analysis of medication selection according to the number of MDD outpatients per month |
In further analysis by the number of patients the psychiatrists treated per month, those who saw 101–200 persons/month were more likely to choose quetiapine and olanzapine as augmentation strategy, but those who saw more than 200 persons/month were less likely to choose quetiapine and olanzapine as augmentation strategy. There was no difference in choosing aripiprazole as the augmentation strategy between the groups (Table 3).
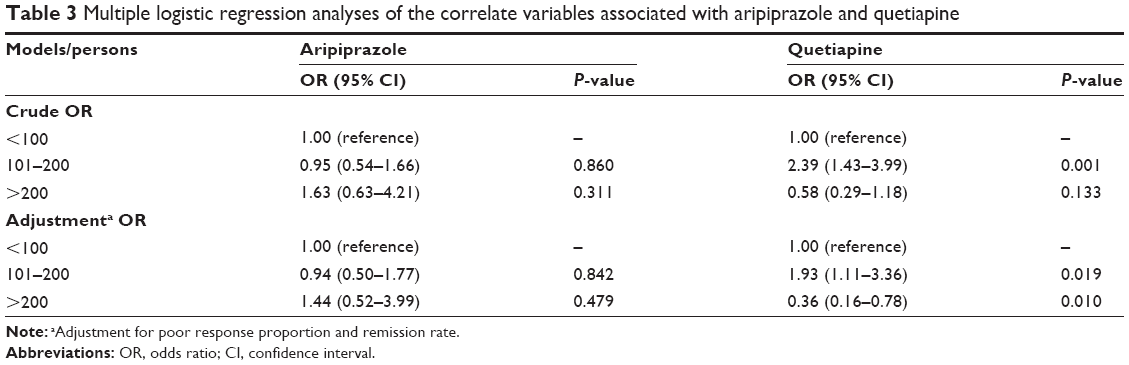 | Table 3 Multiple logistic regression analyses of the correlate variables associated with aripiprazole and quetiapine |
Discussion
Treatment-resistant depression is associated with extensive use of general and psychiatric medical services, which poses substantial economic burden and work loss costs.9,10 The prescribing behavior of psychiatrists may influence the outcomes of refractory MDD and cause a delay in the use of adequate antipsychotic augmentation therapy. It is important therefore for health policy makers to understand the prescribing behaviors and modify the insurance policy accordingly.
The national health care system in Taiwan, known as the National Health Insurance (NHI) program, was instituted in 1995. The NHI program is a single-payer compulsory social insurance plan which centralizes the disbursement of health care funds.11,12 The system promises equal access to health care for all citizens, and the population coverage had reached 99% by the end of 2004.13,14 Although patient satisfaction with the NHI program was reported to be more than 80% in 2011,15 doctors have reported dissatisfaction because of instability in NHI regulations, a complicated medical claims system, and excessive working hours.16 Doctors can be heavily penalized for a wide variety of reasons such as seeing too many patients or offering too many services even if they were appropriate under a budget-reduction scenario and reduced-payment physician payment policy and claims review system.17
In Taiwan, the NHI payment policy adopts a unique way in the denial of prescriptions payment, which is called “insurance policy audit and deletion of payments”. The auditors act by “post-hoc” denial, or deletion, of payment for the medications. For example, while some health care providers (including psychiatrists) prescribe medications costlier than those prescribed daily by other peer health care providers, auditors could delete the payment for these medications. This doesn’t just mean that the NHI denied the payment per se, but also means a 100-fold penalty, that is, 100-fold of the price of the denied medications must be paid back to the NHI by the health care providers.18–20 The sampling rate of cases for auditing is one-fifteenth (6.67%) of the medical cases submitted monthly by individual health care providers.21
MDD is one of the major mental illnesses treated by Taiwanese psychiatrists, many of whom agree that an inadequate poor response to ADT is common. Although 50%–60% of patients respond to first-line treatment, only 35%–40% of patients were reported to experience a remission of symptoms during an initial 8-week trial.1 In Taiwan, the inadequate response rate has been reported to be 30%. Most psychiatrists in Taiwan agree that around 60% of MDD patients can achieve remission, which is close to that reported with venlafaxine (59.3%), and higher than that reported in previous studies with conventional antidepressants (ie, paroxetine, citalopram, sertraline, fluoxetine, mirtazapine, or other treatments),22 which may imply that Taiwanese psychiatrists overestimate the MDD remission rate.
Other than medical knowledge and training, physician prescribing behavior is largely influenced by pharmaceutical promotions,23 health insurance payments, and administrative policy. As previously reported, health insurance policy can jeopardize patient benefits when physicians are required to conform to the finance-driven regulatory rules of health insurance companies.7,8,24 Switching to venlafaxine, for example, has been shown to have a higher response rate after selective serotonin reuptake inhibitor (SSRI) failure.22 However, in Taiwan, approximately the same number of psychiatrists choose switching as choose augmentation.
Three randomized controlled trials demonstrated that aripiprazole augmentation is useful for antidepressant nonresponders, and that it should be reserved for nonresponders after 6 weeks of adequate ADT.25,26 There is currently no consensus on the duration of aripiprazole augmentation, however current American Psychiatric Association MDD guidelines recommend the same dose used for the acute phase as in the continuation and maintenance phases.27 The most common adverse effect of aripiprazole is akathisia, which occurs in about 23.1% of the patients treated with aripiprazole,25 and can be treated with propranolol. Many Taiwanese psychiatrists choose aripiprazole and quetiapine as augmentation antipsychotics, however up to 30% of Taiwanese psychiatrists still choose off-label olanzapine (34.6%), risperidone (30.2%), and sulpiride (27.4%). In Taiwan, psychiatrists are allowed to prescribe medications for off-label use,28–31 but off-label use of prescriptions are one of the exclusion criteria for drug relief in the Taiwan Drug Hazard Relief Act, which was enacted in 2000.32,33
The main reasons why psychiatrists do not choose aripiprazole are price, insurance audit and deletion, and adverse effects. Aripiprazole costs US$0.33 per mg in Taiwan, and therefore a dose ranging from 2–10 mg/d costs US$0.66–3.30 per day. Whereas, antidepressants cost US$0.14–0.95 per tablet for SSRI, and US$0.90–1.07 per tablet for (serotonin-norepinephrine reuptake inhibitor) SNRI. So an adequate dose of SSRI costs US$0.14–0.95 per day and US$2.70–3.20 per day for SNRI.34
The switching strategy is cheaper than augmentation strategy. In 2004, the average daily drug price for depressive outpatients in Taiwan was estimated to be US$1.3±1.316.35 Insurance payment is an important concern for Taiwan psychiatrists. If the prescription is audited and deleted in outpatients, the penalty is up to 100-fold the medication price.20 We speculate that insurance audit and deletion is the main reason why Taiwanese psychiatrists do not choose aripiprazole as an augmentation strategy. In contrast to the American Psychiatric Association’s willingness to sue insurers over American Medical Association’s Current Procedural Terminology code violations,36 the Taiwanese Society of Psychiatry has taken little action against insurance audit and deletion.
Few previous studies have discussed psychiatrists’ decision-making. In one study concerning the prescription of benzodiazepines, the decision-making was found to be influenced by concerns of fear of supply, initiating substance abuse, or even diversions in patients, especially when facing time limits and patient manipulation, however insurance coverage issues were not mentioned.37 Similar to a study which reported that the prescription of non-steroid anti-inflammatory drugs (NSAIDs) or NSAIDs with gastroprotective therapy to the elderly with osteoarthritis was influenced by the reimbursement policy in Canada,7 the prescribing behavior by Taiwanese psychiatrists for antipsychotic augmentation seems to be affected by health insurance payment policy.
The response to placebo in antidepressant drug trials for MDD is highly variable and has increased significantly in recent years.38 Two main mechanisms underlie the effect of placebo administration: conditioned reflexes, which are subconscious, and the patient’s expectations, which are conscious. Other factors in placebo administration relate to the doctor’s influence on the patient’s attitude to his or her disease. This can be referred to as the “context effect”.39 Placebo effects may explain why off-label use of atypical antipsychotics is common among Taiwanese psychiatrists.
The main limitation of this study is lack of demographic data, for most of the psychiatrists did not offer their detailed personal information. However, the total numbers of psychiatrists was nearly 1,436 in the year of the study, 2012,40 therefore, nearly one in every five (22.56%) Taiwan psychiatrists responded to this questionnaire, which could be representative of this group.
Conclusion
Antipsychotic augmentation with aripiprazole and quetiapine is recommended for MDD patients with a poor response to ADT, however many Taiwanese psychiatrists still choose a switching strategy. Price and insurance audit and deletion affected the intention to prescribe aripiprazole. We suggest that prescribing behavior by Taiwan psychiatrists for antipsychotic augmentation is affected by health insurance policy.
Acknowledgment
The authors thank Ms Jessie Wei-Shan Chiang for her help in the administrative work and proofreading of the manuscript.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Fava M. Diagnosis and definition of treatment-resistant depression. Biol Psychiatry. 2003;53(8):649–659. | ||
Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronine augmentation in the treatment of refractory depression. A meta-analysis. Arch Gen Psychiatry. 1996;53(9):842–848. | ||
Bauer M, Forsthoff A, Baethge C, et al. Lithium augmentation therapy in refractory depression-update 2002. Eur Arch Psychiatry Clin Neurosci. 2003;253(3):132–139. | ||
Papakostas GI, Shelton RC, Smith J, Fava M. Augmentation of antidepressants with atypical antipsychotic medications for treatment-resistant major depressive disorder: a meta-analysis. J Clin Psychiatry. 2007;68(6):826–831. | ||
U.S. Food and Drug Administration. Efficacy Supplement Approvals in 2007. Available from: http://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/drugandbiologicapprovalreports/ucm081898.htm#NDAEfficacySupplementsApprovedNSE1-SE7. Accessed November 29, 2014. | ||
DeWitt EM, Glick HA, Albert DA, Joffe MM, Wolfe F. Medicare coverage of tumor necrosis factor alpha inhibitors as an influence on physicians’ prescribing behavior. Arch Intern Med. 2006;166(1):57–63. | ||
Raina PS, Gafni A, Bell S, et al. Is there a tension between clinical practice and reimbursement policy? the case of osteoarthritis prescribing practices in Ontario. Healthc Policy. 2007;3(2):e128–e144. | ||
Virabhak S, Shinogle JA. Physicians’ prescribing responses to a restricted formulary: the impact of Medicaid preferred drug lists in Illinois and Louisiana. Am J Manag Care. 2005;11 Spec No:SP14–SP20. | ||
Greenberg P, Corey-Lisle PK, Birnbaum H, Marynchenko M, Claxton A. Economic implications of treatment-resistant depression among employees. Pharmacoeconomics. 2004;22(6):363–373. | ||
Parikh RM, Lebowitz BD. Current perspectives in the management of treatment-resistant depression. Dialogues Clin Neurosci. 2004;6(1):53–60. | ||
Chiang TL. Taiwan’s 1995 health care reform. Health Policy. 1997;39(3):225–239. | ||
Cheng SH, Chiang TL. The effect of universal health insurance on health care utilization in Taiwan. Results from a natural experiment. JAMA. 1997;278(2):89–93. | ||
Fanchiang C. New IC health insurance card expected to offer many benefits Taiwan. Taiwan J. 2004. Available from http://www.taiwantoday.tw/ct.asp?xItem=20439&CtNode=122. Accessed December 29, 2014. | ||
Liu CT, Yang PT, Yeh YT, Wang BL. The impacts of smart cards on hospital information systems–an investigation of the first phase of the national health insurance smart card project in Taiwan. Int J Med Inform. 2006;75(2):173–181. | ||
National Health Insurance Bureau. National Health Insurance in Taiwan 2011 Annual Report. Available from: http://www.nhi.gov.tw/resource/Webdata/20774_1_NHI%20IN%20TAIWAN%202011%20ANNUAL%20REPORT.pdf. Accessed April 30, 2014. | ||
Lin HC, Chang WY, Tung YC. Factors related to dissatisfaction with the National Health Insurance among primary care physicians in Taiwan. Chang Gung Med J. 2003;26(2):81–90. | ||
Lu JF, Hsiao WC. Does universal health insurance make health care unaffordable? Lessons from Taiwan. Health Aff (Millwood). 2003;22(3):77–88. | ||
Bureau of National Health Insurance. Central Area Liaison Meeting Records. Avialable from: http://sc-dr.com.tw/admin/images/cke/files/03020202.pdf. Accessed November 28, 2014. | ||
Liang JA, Sun LM, Muo CH, Sung FC, Chang SN, Kao CH. The analysis of depression and subsequent cancer risk in Taiwan. Cancer Epidemiol Biomarkers Prev. 2011;20(3):473–475. | ||
Fu HH. A Study on Medical Claim Payments Auditing Procedure in Taiwan National Health Insurance [PhD Thesis]. Kaohsiung, Taiwan: Institute of Business Management, National Sun Yat-sen University; 2004. | ||
Fu HH, Tsai HT, Lin CW, Wei D. Application of a single sampling plan for auditing medical-claim payments made by Taiwan National Health Insurance. Health Policy. 2004;70(2):185–195. | ||
Baldomero EB, Ubago JG, Cercos CL, Ruiloba JV, Calvo CG, Lopez RP. Venlafaxine extended release versus conventional antidepressants in the remission of depressive disorders after previous antidepressant failure: ARGOS study. Depress Anxiety. 2005;22(2):68–76. | ||
King M, Essick C, Bearman P, Ross JS. Medical school gift restriction policies and physician prescribing of newly marketed psychotropic medications: difference-in-differences analysis. BMJ. 2013;346:f264. | ||
Saito S, Mukohara K, Bito S. Japanese practicing physicians’ relationships with pharmaceutical representatives: a national survey. PLoS One. 2010;5(8):e12193. | ||
Berman RM, Marcus RN, Swanink R, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2007;68(6):843–853. | ||
Marcus RN, McQuade RD, Carson WH, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a second multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. 2008;28(2):156–165. | ||
Psychiatryonline.org. Practice Guideline for the Treatment of Patients with Major Depressive Disorder. Available from: http://psychiatryonline.org/data/Books/prac/PG_Depression3rdEd.pdf. Accessed April 21, 2014. | ||
Cheng WM, Lin TP, Lin AT, Chen KK, Chen TJ. A nationwide population study of trazodone use in urology patients. J Chin Med Assoc. 2013;76(8): 432–437. | ||
Hsu SW, Chiang PH, Chang YC, Lin JD, Tung HJ, Chen CY. Trends in the use of psychotropic drugs in people with intellectual disability in Taiwan: a nationwide outpatient service study, 1997–2007. Res Dev Disabil. 2014;35(2):364–372. | ||
Hsu YC, Chien IC, Tan HK, et al. Trends, correlates, and disease patterns of antipsychotic use among children and adolescents in Taiwan. Soc Psychiatry Psychiatr Epidemiol. 2013;48(12):1889–1896. | ||
Huang WF, Lai IC. Patterns of sleep-related medications prescribed to elderly outpatients with insomnia in Taiwan. Drugs Aging. 2005;22(11):957–965. | ||
On AWF, Chi LH, Liu C, Lin KH. A unique drug-injury relief system in Taiwan: comparing drug-injury compensation in different countries. J Pharm Health Serv Res. 2012;3:3–9. | ||
Chih LH, On AWF, Liao WC. A Study of the patterns of off-label use resulting in drug relief applications in Taiwan. Taiwan J Family Med (in traditional Chinese with English abstract). 2012;22(3):119–129. | ||
Ministry of Health and Welfare, National Health Insurance Administration. Taiwan National health drug price query. Available from: http://www.nhi.gov.tw/Query/query1.aspx?menu=20&menu_id=831&WD_ID=831. Accessed November 28, 2014. | ||
Chen CM, Chien CW. [A Study of Resource Utilization on Depressive Disorders in Taiwan]. Taipei, Taiwan: Institute of Hospital and Health Care Administration, National Yang-Ming University; 2006. Avialable from: http://ir.ym.edu.tw/ir/bitstream/987654321/2549/2/GYF120319195.pdf. Accessed January 12, 2015. Chinese. | ||
Brauser D. APA willing to sue insurers over CPT code violations–legal action may be taken when mental health parity law is violated. Medscape. 2013. Available from: http://www.medscape.com/viewarticle/781944. Accessed April 30, 2014. | ||
Marienfeld CB, Tek E, Diaz E, Schottenfeld R, Chawarski M. Psychiatrist decision-making towards prescribing benzodiazepines: the dilemma with substance abusers. Psychiatr Q. 2012;83(4): 521–529. | ||
Walsh BT, Seidman SN, Sysko R, Gould M. Placebo response in studies of major depression: variable, substantial, and growing. JAMA. 2002;287(14):1840–1847. | ||
Breidert M, Hofbauer K. Placebo: misunderstandings and prejudices. Dtsch Arztebl Int. 2009;106(46):751–755. | ||
Taiwan Medical Association. Taiwan Statistics of Practicing Physicians and Medical Organizations in 2012. Available from: http://www.tma.tw/tma_stats_2012/2012_stats.pdf. Accessed November 29, 2014. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.