")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Differential Self-Reported Determinants to Antiretroviral Therapy Adherence: Findings from Caregivers of Children Under Five Years Living with Human Immunodeficiency Virus Infection Attending Al-Sabah Hospital, South Sudan
Authors Tong PD, Atuhairwe C , Taremwa IM
Received 2 February 2020
Accepted for publication 24 April 2020
Published 18 May 2020 Volume 2020:12 Pages 175—186
DOI https://doi.org/10.2147/HIV.S248057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Peter Deng Tong, Christine Atuhairwe, Ivan Mugisha Taremwa
Clarke International University, Kampala, Uganda
Correspondence: Ivan Mugisha Taremwa
Tel +256 774346368
Email [email protected]
Aim/Objective: This study explored the caregivers’ self-reported determinants of antiretroviral therapy (ART) adherence among children under five years living with human immunodeficiency virus (HIV) infection attending Al-Sabah Hospital, South Sudan.
Methods: A cross-sectional study of 126 caregivers of HIV-infected children under five years was conducted at Al-Sabah Hospital, South Sudan. Data were collected using an interviewer-administered questionnaire. The self-reported adherence was measured as a binary variable using binary logistic regression. Only variables that were significant at bivariate analysis were analyzed at multivariate level and interpreted using the odds ratios (p< 0.05).
Results: Out of 126 caregivers with HIV-infected children, 38 (30.2%) did not adhere to ART. Of the proportion that adhered to ART (88, 69.8%), 49 (55.7%) were male. Most of the children (52, 59.1%) were above two years, but under five years. Fifty (56.8%) of those who adhered had completed 3 months on ART, and the majority were at WHO stage-1 of HIV infection. Analysis of the determinants indicated that children’s duration on ART (p=0.001), type of ART regimen (single, double or triple therapy) (p=0.065), type of work done by the caregiver to earn a living (p-value 0.003), time a child was initiated on ART (p=0.002), caregiver–child relationship (p=0.002), caregiver-spousal support (p=0.019), type of support obtained whether monetary or not (p=0.000), when the child was started on ART (p=0.004), the person administering ART (p=0.010), the type of ARVs administered (p=0.001), the caregiver detecting ART side effects (p=0.000), types of adverse effects suffered by the child (p=0.043), time of receiving ART (p=0.047), use of western medicine (p=0.043), healthcare cadre (p=0.002), the kind of attention the healthcare provider offered (p=0.015), and improvements in quality of HIV services (p=0.001) were significantly associated with ART adherence.
Conclusion: The study findings indicated that ART adherence among HIV-infected children under five years was suboptimal. This will necessitate continuous engagement and education of caregivers on the prominence of adhering to ART.
Keywords: ART adherence, children under five, HIV, caregivers, Al-Sabah, South Sudan
Background
Globally, the acquired immunodeficiency syndrome (AIDS) epidemic remains devastating to all age groups. By the end of 2018, there were 37.9 million people globally living with HIV/AIDS (human immunodeficiency virus/acquired immunodeficiency syndrome),1 of which 1.7 million were children under 15years.1 In particular, HIV-infection rates remain unacceptably very high in sub-Saharan African countries, where the number of HIV-positive children was reported at 90%.1,2 Statistics by UNAIDS-South Sudan3 indicate that a total of 190 000 people were living with HIV, of whom 19,000 people were newly infected. Furthermore, the HIV prevalence among adults (15–49 years) in South Sudan was 2.7% of which 42% of the new infections were in sex workers and children born by HIV-infected mothers which accounted for 15.7%.3 In Comparison with the 95-95-95 targets, in which by 2030, 95% of people living with HIV/AIDS (PLWHA) ought to be aware of their HIV status, 95% of people aware of their HIV status ought to be on treatment; and 95% of people on treatment ought to achieve a virological suppression; attaining the 95-95-95 target in South Sudan means that 85.5% of PLWHA would be on treatment, and 77.1% of them would have to be virally suppressed.3 Astonishingly in 2018, only 24% of the PLWHA in South Sudan knew their status, and 16% were on ART; and treatment for HIV remains low, with 9% of children aged 0–14 years living with HIV were on ART.3 The burden of HIV-infected children under five is high in South Sudan due to inadequate prevention of mother-to-child transmission (PMTCT) interventions.3 By the end of 2018, only 56% of pregnant women living with HIV were enrolled on prophylaxis to PMTCT.3
As a concerted effort to avert AIDS-related deaths, an estimated at 24.5 million people living with HIV globally had access to antiretroviral therapy (ART) by the end of June 2019,1 however, a very small proportion of these were from South Sudan.3 While 95% ART adherence among people were living with HIV significantly suppresses the HIV virus progression by maintaining a plasma HIV-1 ribose nucleic acid below quantification limits and improves their quality of life,1 this is maximized by early ART initiation and adherence (defined as: the extent to which a person’s behavior related to taking medications corresponds with agreed recommendations from a health care provider).5,6 As a major predictor of survival among PLWHA,1 ART adherence lessens plasma HIV-ribose nucleic acid levels, increases CD4 cell counts, decreases the incidence of opportunistic infections, improves growth and development, and improves the quality of life.5,7,8 On the other hand, poor ART adherence is of critical concern, as this is associated with worsened outcomes such as: limited performance (effect) of ART, repeated hospitalization and increased health care costs, as well as aggravated morbidity and mortality.7,9
ART adherence below 95% increases the risk of a patient developing life-threatening conditions such as multidrug-resistant strains which complicates the limited available treatment options, with eventual mortality.2 Practically, children under five (0–4 years) present a unique ART adherence challenge as they solely depend on their caregivers; a basis for which the caregiver report has been universally utilized to assess pediatric ART adherence.2,5,6 The intricacy of ART adherence in children was even more amplified by the post-conflict era in South Sudan characterized by inadequate healthcare facilities and poor HIV children prevention strategies.3
Despite the scale-up of pediatric ART programs, and proven positive attributes, ART adherence among children under-five remained sub-optimal.9–11 This was as a result of many factors which hinged on the child, caregiver(s) and family, regimen, as well as the society and culture.8 As there was limited data on ART adherence, and determining factors in South Sudan; we reported on the different caregivers’ self-reported determinants of ART adherence among children under five years living with human immunodeficiency virus infection who attended Al-Sabah Hospital.
Methods
Study Area and Setting
The study was carried out at Al-Sabah Hospital, the main children’s hospital in Juba state, South Sudan. It is a state and referral children’s hospital with a capacity of 144 beds. The hospital is located in Juba, the capital city of South Sudan. South Sudan had a generalized HIV epidemic that was geographically concentrated in the former Equatorial States which comprised an estimated 47% (88,720 people living with HIV) of the National 2018 estimate. Initiated under Country Operational Plan 2017 (COP17), Test and Treat is being implemented in all President’s Emergency Plan for AIDS Relief (PEPFAR) intervention sites.3
Study Design
This study followed a cross-sectional study design, between July and October 2019.
Study Population, Sample Size Estimation, Sampling and Recruitment
The study population comprised adult caregivers of HIV-infected children under five years of age, who had consented. We defined a caregiver as a parent, or guardian, or person who was charged with administering ART medicines to the HIV-positive child. Using the Leslie Kish 1965 formula,12 a total of 126 caregivers with HIV-infected children were considered sufficient for the study. This study could not carry out sampling because there were few caregivers with HIV-infected children that came for refills at the facility. Inclusion criteria for caregivers with HIV-infected children in the study were those with children that had taken ART for at least 12 weeks, and were aged six to 59 months. Participants were selected on the basis of their ability to understand and communicate in any of the two languages, ie Arabic and English. The study excluded children who were receiving only cotrimoxazole prophylaxis.
Study Variables
The dependent variable was ART adherence which was categorized into two: adhered (self-reported) and non-adhered. ART adherence was defined according to the WHO guidelines,5 HIV adherence was based on caregiver self-report of ≥95% administered ART, while non-adherence was assessed based on reportedly missed pills that aggregately was less than 95% in the 7 days prior to the date of interview.
Data Collection Tool
Data were collected using an interviewer-administered questionnaire (Figure 1). The questionnaire comprised: demographic characteristics (age, sex); clinical factors (ART regimen, ART side effect, baseline CD4 count, WHO stages, oral therapy, clinical visits and hospital checkup, waiting time and distances); caregivers/family factors (age, gender, education, religious affiliation, occupation and support groups); societal factors (society may support or discourage ART, alternative medicines, discrimination, stigma, social isolation, HIV disclosure). Also, data on the child and caregiver factors; how ART was administered to the child, health facility and societal factors were collected. The research team with the help of the health workers looked at the patients’ medical forms to triangulate the information collected through the interview. The questionnaires were in the language of the participants’ choice (English or Arabic), and were administered in a suitable private room where the caregivers would talk freely. To enhance the accuracy of the translation, the questionnaire was originally developed in English, then translated into Arabic, and translated back to English. The questionnaire items were reviewed by five experts on pediatric HIV care who knew both English and Arabic. Also, prior to the commencement of the study, two research assistants proficient in both English and Arabic languages were trained to help selected caregivers understand each question. The questionnaire was pre-tested with the help of 20 caregivers to ensure clarity and accuracy among South Sudanese seeking ART care at Kisugu Health Centre IV, in Kampala (Uganda), and modifications were made to the effect.
 |
Figure 1 Continued. |
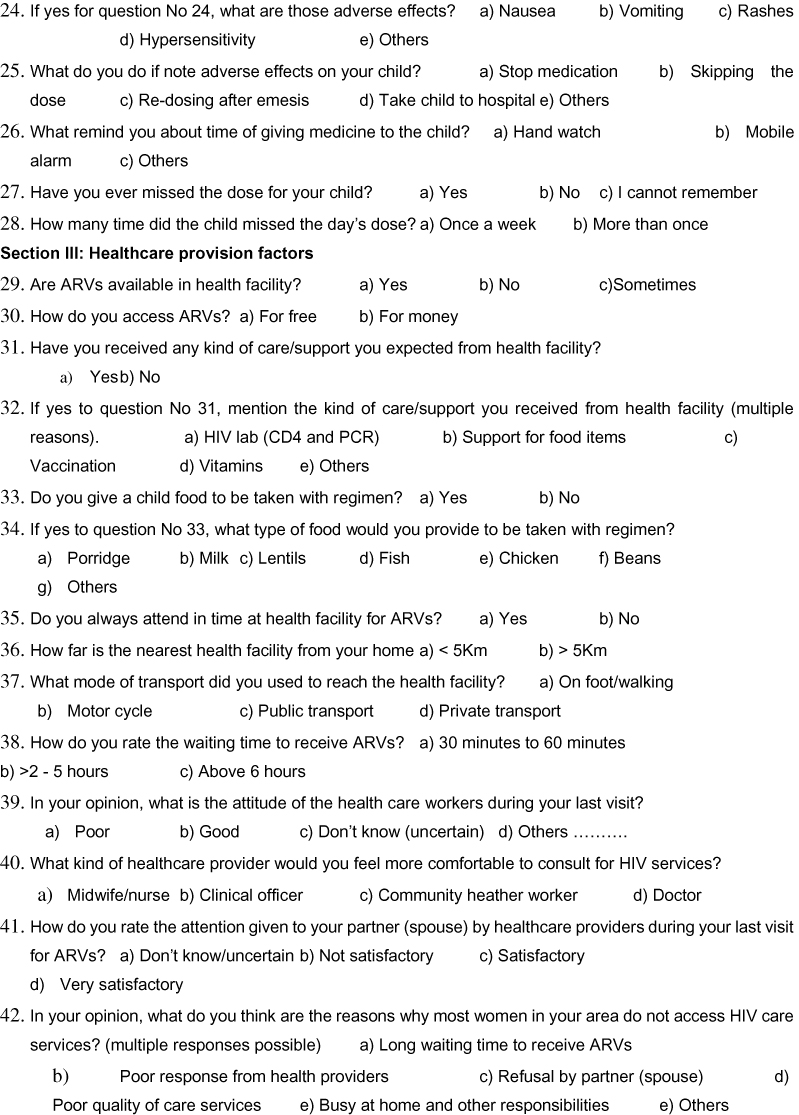 |
Figure 1 Continued. |
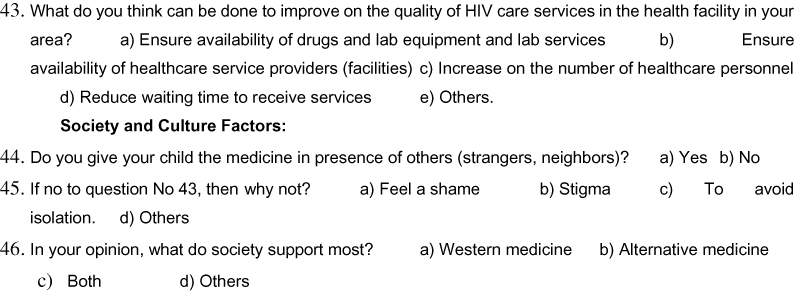 |
Figure 1 Interviewer-administered questionnaire. |
Data Collection Process
The caregivers were interviewed on exit from the HIV clinic. The research assistants were positioned at the exit of the HIV clinic and followed the interview protocol procedures to obtain the required information. Information regarding the CD4 cell count, type of ARVs, laboratory and prescriptions given to the child was verified from the child’s medical records, while the other information was received for the study participants (caregivers).
Data Management and Analysis
Data were pre-coded and entered using Epi-data and analyzed using SPSS version 21. After univariate analysis, the results were presented using frequencies and percentages. For bivariate analysis, each predictor was cross-tabulated with the dependent variable (ART adherence) to establish possible associations using the chi-square test statistic at a 5% level of significance. For the multivariate level of analysis, the binary logistic regression was used and interpreted using the odds ratios.
Ethics Approval and Consent to Participate
Ethical approval was obtained from Clarke International University. Thereafter, administrative permission was obtained from Al-Sabah Hospital and written informed consent was sought from each caregiver before the questionnaire was administered. This study was conducted in accordance with the Declaration of Helsinki.
Consent forms were translated into the languages of English and Arabic, the language most commonly used then in South Sudan. Consent forms were read aloud to caregivers by trained research assistants. Caregiver participation was strictly voluntary, and caregivers’ withdraw did not carry any consequences to their children’s ART care. Also, the confidentiality of information, privacy, non-coercion and respect to their autonomy was observed. Anonymity was ensured by keeping data secure at all times.
Results
The study enrolled 126 caregivers with HIV-infected children. Of these, 69 (54.8%) were male child participants, and 78 (61.9%) of the child participants were aged 2–5 years. The characteristics of the participants are presented in Table 1.
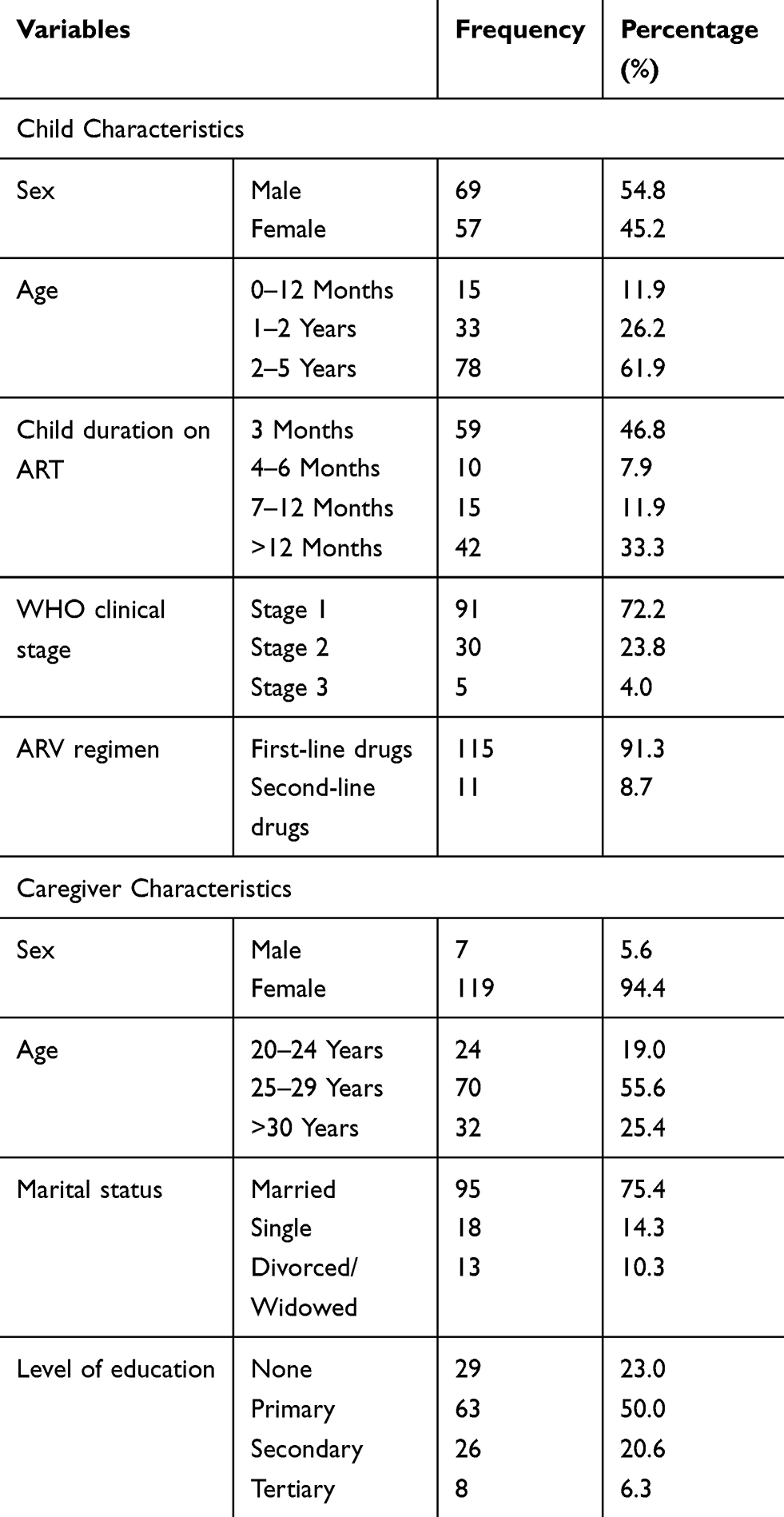 |
Table 1 Child Characteristics of the Participants |
Out of 126 caregivers of HIV-infected children, 38 (30.2%) did not adhere to ART. Of the proportion that adhered to ART (88, 69.8%), 49 (55.7%) were male 11 of the children (12.5%) were below 1-year-old, while 25 (28.4%) were aged between 1 and 2 years, and 52 (59.1%) were between ages of 2–5 years old. With regard to ART duration, 50 (56.8%) of those who adhered had completed 3 months, 7 (8.0%) had spent 4–6 months, 5 (5.7%) had spent 7–12 months and 26 (29.5%) had spent above 12 months. According to WHO clinical staging, 64 (72.7%), 21 (23.9%) and 3 (3.4%) were in stages 1, 2 and 3, respectively. Also, 83 (94.3%) of the children that adhered were on first-line ART regimen, while 5 (5.7%) were on second line. Bivariate analysis showed that: child’s duration on ART (χ2= 16.970, p=0.001), ARV regimen (single, double or triple therapy) (χ2=3.403, p=0.065) was significantly associated with ART adherence, as given in (Table 2).
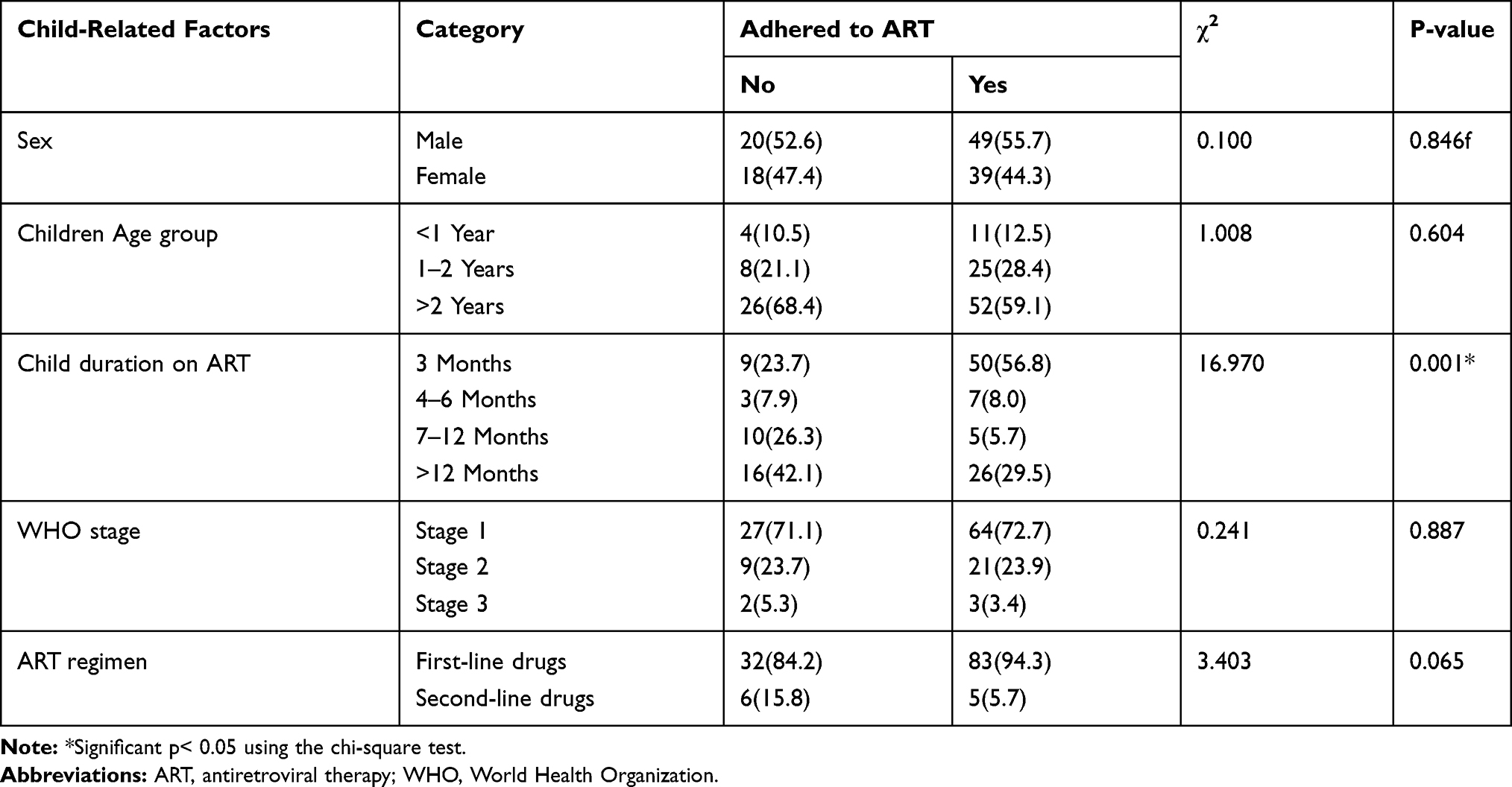 |
Table 2 Child-Related Factors and ART Adherence Among Children |
The caregiver factors; most (65, 73.9%) caregivers were housewives, 5 (5.7%) were peasants, 5 (5.7%) were traders, and 13 (14.8%) used other means to earn a living. Seventy-eight (88.6%) of the caregivers earned below 10,000 South Sudan Pound (SSP), while 10 (11.4%) earned between 10,001 and 50,000 SSP. There were 61 (69.3%) caregivers who received support from their spouse/family in the form of money (55, 90.2%), and food supplies (N=5, 8.2%). Bivariate analysis showed that: type of work done to earn a living (χ2=14.286, p=0.003), time a child was initiated on ART (χ2= 9.681, p=0.002), caregiver–child relationship (χ2=9.567, p=0.002), caregiver-spousal support (χ2 = 5.467, p=0.019), and the type of support (χ2= 16.768, p=0.000) were significantly associated with ART adherence, as shown in (Table 3).
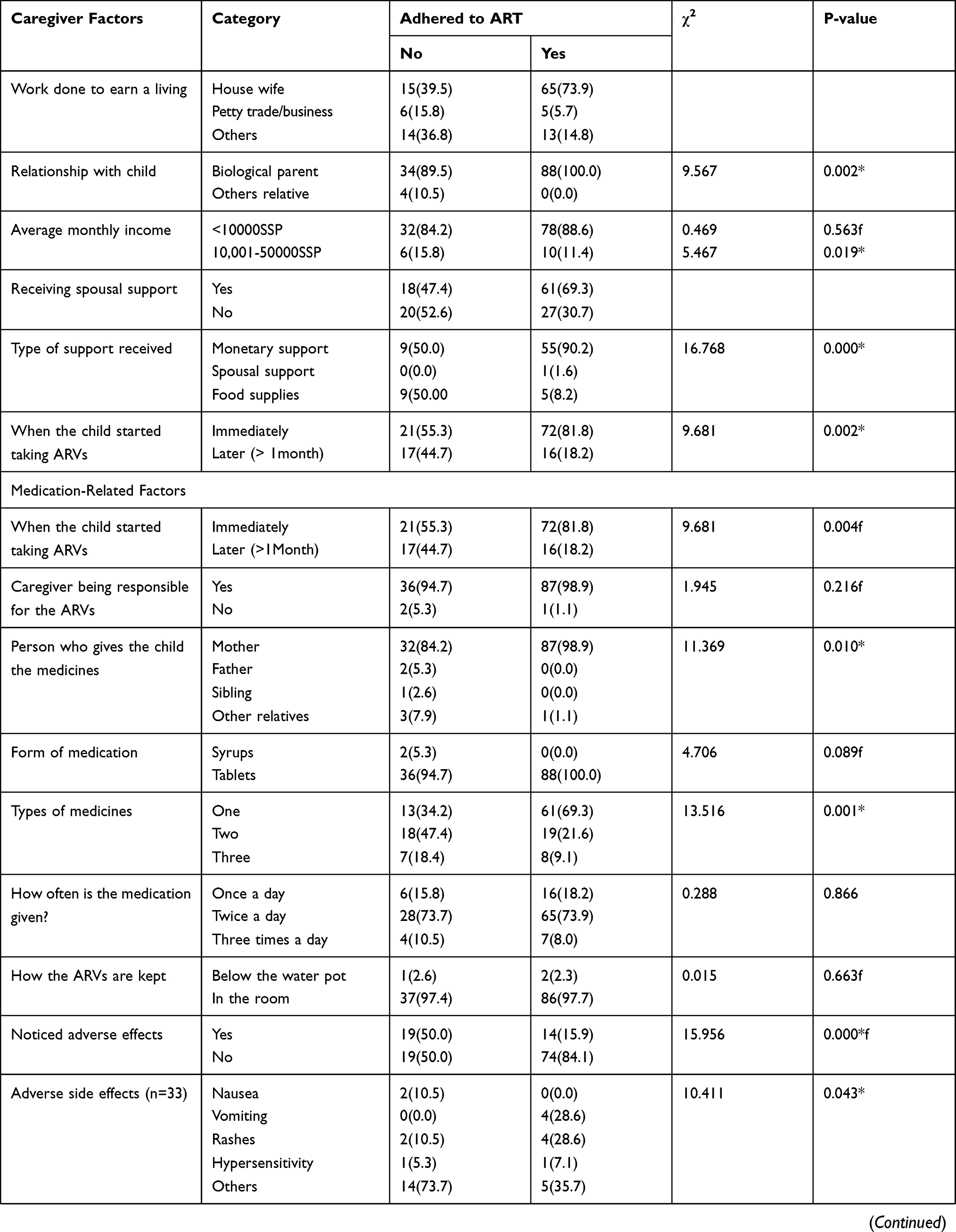 |  |  |
Table 3 Predictors of ART Adherence Among Children |
To explore how the medication was administered to children, 72 (81.8%) of the children that adhered had been initiated on ART instantly after diagnosis, while 16 (18.2%) had started a month later. Also, more children (87, 98.9%) had their mothers in charge of medication. All the children who adhered were taking tablets; and ART was given as one type (61, 69.3%), two types (19, 21.6%), or three types (8, 9.1%). Sixteen (18.2%) were on a single daily dose, 65 (73.9%) received a double-doze, and 7 (8.0%) were on triple dose. ART adverse effects were reported to occur among 14 (15.9%), and these manifested as nausea, vomiting, and rashes; which had prompted the caregivers to either skip a day’s dose, or take the child to a health facility. Bivariate analysis found that: when the child was started on ART (χ2= 9.681, p=0.004), the person administering ART (χ2= 11.369, p=0.010), the type of ARVs administered (χ2= 13.516, p=0.001), the caregiver detecting ART side effects (χ2= 15.956, p=0.000), and types of adverse effects suffered by the child (χ2= 10.411, p=0.043) were significantly associated with ART adherence, as presented in (Table 3).
The health facility factors revealed that caregivers had received ART at no cost, and 34 (38.6%) of the caregivers lived less than 5 Kilometers (Km) from a health facility. More (84, 95.5%) of the caregivers reported a positive attitude towards healthcare providers, and 74 (84.1%) of the caregivers were satisfied with the attention given to their children. Bivariate analysis indicated that: time of receiving ART (χ2= 3.944, p=0.047), healthcare cadre (χ2= 18.227, p=0.002), the kind of attention the healthcare provider offered (χ2= 8.429, p=0.015), and improved quality of HIV services (χ2= 19.049, p=0.001) were significantly associated with ART adherence, as shown in (Table 3). Relatedly, societal and cultural factors indicated that the use of western medicine (χ2=8.176, p=0.043) was key as it showed a statistical association with ART adherence (Table 3). A binary regression model was fitted using covariates to ascertain the determinants of ART adherence, and this was associated with such factors as the duration a child spent on ART (COR 2.171; 95% CI: 0.758–6.221), first-line ART regimen (COR 2.199; 95% CI: 0.524–9.230), time a child was initiated on ART (COR 2.494; 95% CI: 0.906–6.868), and time a child had spent on ART (COR 2.171–3.793; 95% CI: 0.758–6221), as shown in (Table 4).
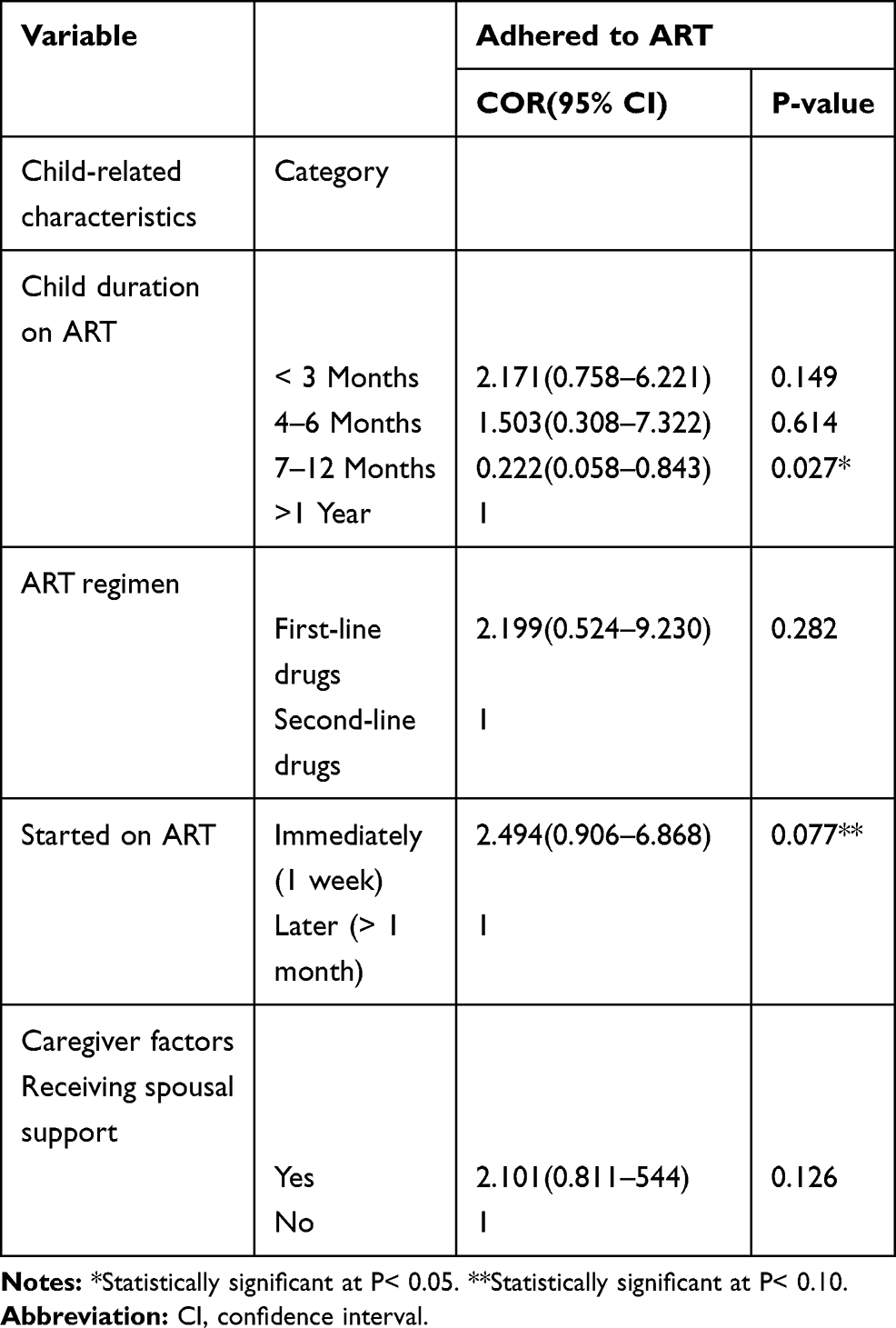 |
Table 4 Factors Associated with ART Adherence Among Children |
Discussion
This study’s findings revealed a 69.8% level of ART adherence among caregivers with HIV-infected children under five years at Al-Sabah children’s hospital in Juba State, South Sudan. This value was lower than the 79% that was reported among caregivers of HIV-infected children in Kabale district, Southwestern Uganda,13 88.7% and 93.3% of caregivers reported adherence from Ethiopia.14,15 However, it was higher than the 62.5% reported from Tanzania11 while 34.8% was based on unannounced home-based pill count reported from Ethiopia.14 The high-edge variance was ascribed to the fact that this was caregiver self-reported data. The caregiver self-report was the mostly used ART adherence assessment method for pediatric HIV care in resource-limited settings, it is prone to error compared to pill counts, pharmacy refill and electronic dose monitoring.7 At the same time, the obtained self-reported ART adherence was moderate, considering the global concerted target of 95-95-95 strategy. In this fast-tracking end HIV/AIDS strategy by 2030, 95% of people living with HIV ought to know their HIV status; 95% of people who know their status would be initiated on treatment; and 95% of people on treatment would have with suppressed viral loads as a surrogate for optimal ART adherence.16 Among the non-adhered, caregivers missed hospital appointments and/or their doses because they were unable to raise money for transport fares. This phenomenon was consistent with data that patients on higher incomes had less difficulty with adherence compared to their counterparts with low-income levels.5,7 Although ART was given free of charge in South Sudan, socio-economic challenges were still a hindrance to optimal ART adherence.7 The barriers to optimal adherence were multifaceted, as previous studies had described,13,14,17,18 and obliged urgent and focused attention to improve ART adherence and reduce HIV-associated childhood morbidity and mortality.
The child-related factors indicated that a child’s duration on ART, type of regimen (single, double or triple therapy) were significantly associated with ART adherence. These findings are similar to previous studies.14,19 In this context, previous studies indicated that long duration on ART, and multiple dosing that involved unpalatable constitutions affected ART adherence.11,20 These factors highlighted the need for a combined well-tolerated therapy in HIV-infected pediatric population.
The caregivers' self-reported factors indicated that type of work done to earn a living, time a child was initiated on ART, caregiver–child relationship, caregiver-spousal support, and the type of support were significantly associated with ART adherence. These factors in tandem reflected a balance between living conditions and caregiving. While it was a well-known phenomenon that households depended on male partners for survival, this had overtime changed with both partners actively contributing to the family survival. We found that as people’s health improved on ART, some individuals moved to places far from their ART refill clinics in pursuit of work to earn an income that resulted in missed ART refill appointments. The missed ART refill appointments could be due to either busy work schedules, or lack of transport fares, as described by other studies;21,22 and strongly suggested that committed and well-supported biological caregivers are a key determinant to ART adherence as these experienced a stronger connotation to promote adherence.23
Medication-related factors indicated that children who were instantly started on ART after diagnosis were twice more likely to adhere than those started later. While various observational studies had been inconsistent in defining the optimal time to initiate ART, there was substantial evidence that early initiation of ART improved survival and delayed disease progression; a gateway to the “test and treat” strategy.24 This contradicted a previous approach where the urgency to initiate ART was greatest for clients with lower CD4 cell counts in whom there was a high risk of opportunistic infections, and non-AIDS morbidity, and mortality.
The health facility factors included the type of health care cadre preferred by the child’s caregiver which showed a positive influence on ART adherence, which correlated well with a previous study.25 Further, the caregiver detecting ART side effects, and types of adverse effects suffered by the child affected ART adherence. This finding was similar to previous studies.26,27 Additional factors showed that the kind of attention the healthcare provider offered, improved quality of HIV services, and the use of western medicine were pivotal to ART adherence. This was critical as the use of “alternative HIV treatment options” mainly traditional concoctions, holy water, as well as prayers as a cure for HIV had been reported from previous studies;27-30,31 and such beliefs showed the growing demand for improved healthcare services, as well as addressing societal and culture barriers of ART.
While the findings of this study are valid, they ought to be interpreted with caution due to the following limitations: a) the study was only limited to Al-Sabah Children’s Hospital and cannot be generalizable to other health facility, b) also a small sample size of 126 caregiver–child pair was used, c) the use of caregiver self-report may have overrated ART adherence due to recall bias as well as attempt to impress the interviewer and healthcare providers, d) ART adherence was assessed based on missed doses with no regard of correct timing of medication, e) caregiver self-reported adherence relied on their giving rightful information, f) the reported past 7 days of ART adherence was a short time and may not have correlated well with annual adherence levels, and g) the study only used interview data.
Conclusion
ART adherence among children under five years at Al-Sabah children’s hospital was sub-optimal. To these, Interventions to address barriers to ART adherence under HIV-infected children should be integrated into routine HIV-pediatric care in South Sudan.
Abbreviations
ART, antiretroviral therapy; HIV, human immunodeficiency virus; AIDS, acquired immunodeficiency syndrome; PLWHA, people living with HIV/AIDS; OR, odds ratio; ARV, antiretroviral; CI, confidence interval.
Acknowledgments
The authors express our utmost gratitude to our participants who voluntarily responded to our questionnaire, and the research assistants for the field support.
Disclosure
The authors declare no conflict of interest in this work.
References
1. UNAIDS. Global HIV & AIDS statistics 2019 fact sheet. Available from: https://www.unaids.org/en/resources/fact-sheet.
2. Children, HIV and AIDS/Avert. Global information and education on HIV and AIDS. Available from: https://www.avert.org/professionals/hiv-social-issues/key-affected-populations/children.
3. UNAIDS. South Sudan; 2018. Available from: www.unaids.org/en/regionscountries/countries/southsudan.
4. World Health Organization. South Sudan HIV country profile; 2016. Available from: https://www.who.int/hiv/data/Country_profile_South_Sudan.pdf?ua=1.
5. World Health Organization. Children: reducing mortality; 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality.
6. UNICEF. Seventh stocktaking report on children & AIDS; 2016. Available from: https://www.unicef.org/publications/index_93427.html.
7. Haberer J, Mellins C. Pediatric adherence to HIV antiretroviral therapy. Curr HIV/AIDS Rep. 2009;6(4):194–200. doi:10.1007/s11904-009-0026-8
8. World Health Organization. Importance of adherence to ART; 2006. Available from: https://apps.who.int/medicinedocs/en/d/Js13400e/5.html.
9. Iacob SA, Iacob DG, Jugulete G. Improving the adherence to antiretroviral therapy, a difficult but essential task for a successful HIV treatment-clinical points of view and practical considerations. Front Pharmacol. 2017;8:831. doi:10.3389/fphar.2017.00831
10. Bukenya D, Mayanja BN, Nakamanya S, et al. What causes non-adherence among some individuals on long term antiretroviral therapy? Experiences of individuals with poor viral suppression in Uganda. AIDS Res Ther. 2019;16(2). doi:10.1186/s12981-018-0214-y
11. Martelli G, Antonucci R, Mukurasi A, Zepherine H, Nöstlinger C. Adherence to antiretroviral treatment among children and adolescents in Tanzania: comparison between pill count and viral load outcomes in a rural context of Mwanza region. PLoS One. 2019;14(3):e0214014. doi:10.1371/journal.pone.0214014
12. Kish L. Survey Sampling. New York: John Wiley and Sons, Inc; 1965:78–94.
13. Wadunde I, Tuhebwe D, Ediau M, Okure G, Mpimbaza A, Wanyenze RK. Factors associated with adherence to antiretroviral therapy among HIV infected children in Kabale district, Uganda: a cross sectional study. BMC Res Notes. 2018;11(1):466. doi:10.1186/s13104-018-3575-3
14. Biressaw S, Abegaz WE, Abebe M, et al. Adherence to antiretroviral therapy and associated factors among HIV infected children in Ethiopia: unannounced home-based pill count versus caregivers’ report. BMC Pediatric. 2013;13:132. doi:10.1186/1471-2431-13-132
15. Endalamaw A, Tezera N, Eshetie S, Ambachew S, Habtewold TD. Adherence to highly active antiretroviral therapy among children in ethiopia: a systematic review and meta-analysis. AIDS Behav. 2018;22(8):2513–2523. doi:10.1007/s10461-018-2152-z
16. United Nations General Assembly. Resolution no A/RES/70/266, political declaration on HIV and AIDS: on the fast‐track to accelerate the fight against HIV and to end the AIDS epidemic by 2030; 2016. Available from: http://www.unaids.org/sites/default/files/media_asset/2016-political-declaration-HIV-AIDS_en.pdf.
17. Ugwu R, Eneh A. Factors influencing adherence to pediatric antiretroviral therapy in Portharcourt, South South Nigeria. Pan Afr Med J. 2013;16:30. doi:10.11604/pamj.2013.16.30.1877
18. MacCarthy S, Saya U, Samba C, et al. “How am I going to live?”: exploring barriers to ART adherence among adolescents and young adults living with HIV in Uganda. BMC Public Health. 2018;18:1158. doi:10.1186/s12889-018-6048-7
19. Kikuchi K, Poudel KC, Muganda J, et al. High risk of ART non-adherence and delay of ART initiation among HIV positive double orphans in Kigali, Rwanda. PLoS One. 2012;7(7):e41998. doi:10.1371/journal.pone.0041998
20. Vreeman RC, Nyandiko WM, Liu H, et al. Measuring adherence to antiretroviral therapy in children and adolescents in western Kenya. J Int AIDS Soc. 2014;17(1):19227. doi:10.7448/IAS.17.1.19227
21. Ahmed CV, Jolly P, Padilla L, et al. A qualitative analysis of the barriers to antiretroviral therapy initiation among children 2 to 18 months of age in Swaziland. Afr J AIDS Res. 2017;16(4):321–328. doi:10.2989/16085906.2017.1380677
22. Kiplagat J, Mwangi A, Chasela C, et al. Challenges with seeking HIV care services: perspectives of older adults infected with HIV in western Kenya. BMC Public Health. 2019;19:929. doi:10.1186/s12889-019-7283-2
23. Olds PK, Kiwanuka JP, Ware NC, Tsai AC, Haberer JE. Explaining antiretroviral therapy adherence success among HIV-infected children in rural Uganda: a qualitative study. AIDS Behav. 2015;19(4):584–593. doi:10.1007/s10461-014-0924-7
24. Sellers CJ, Wohl DA. Antiretroviral therapy: when to start. Infect Dis Clin North Am. 2014;28(3):403–420. doi:10.1016/j.idc.2014.05.004
25. Kebede A, Wabe NT. Medication adherence and its determinants among patients on concomitant tuberculosis and antiretroviral therapy in South west Ethiopia. N Am J Med Sci. 2012;4(2):67–71. doi:10.4103/1947-2714.93376
26. Abongomera G, Cook A, Musiime V, et al. Improved adherence to antiretroviral therapy observed among HIV-infected children whose caregivers had positive beliefs in medicine in Sub-Saharan Africa. AIDS Behav. 2017;21(2):441–449. doi:10.1007/s10461-016-1582-8
27. Ankomah A, Ganle JK, Lartey MY, et al. ART access-related barriers faced by HIV-positive persons linked to care in southern Ghana: a mixed method study. BMC Infect Dis. 2016;16:738. doi:10.1186/s12879-016-2075-0
28. McKinney O, Modeste NN, Lee JW, Gleason PC, Maynard-Tucker G. Determinants of antiretroviral therapy adherence among women in Southern Malawi: healthcare providers’ perspectives. AIDS Res Treat. 2014;489370.
29. Chirambo L, Valeta M, Banda Kamanga TM, et al. Factors influencing adherence to antiretroviral treatment among adults accessing care from private health facilities in Malawi. BMC Public Health. 2019;19:1382. doi:10.1186/s12889-019-7768-z
30. Umeokonkwo CD, Onoka CA, Agu PA, et al. Retention in care and adherence to HIV and AIDS treatment in Anambra State Nigeria. BMC Infect Dis. 2019;19:654. doi:10.1186/s12879-019-4293-8
31. Azia IN, Mukumbang FC, van Wyk B. Barriers to adherence to antiretroviral treatment in a regional hospital in Vredenburg, Western Cape, South Africa. South Afr J HIV Med. 2016;17(1):476. doi:10.4102/sajhivmed.v17i1.476
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.