")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 11
Differential pharmacology and clinical utility of dapagliflozin in type 2 diabetes
Authors Papakitsou I, Vougiouklakis G, Elisaf MS , Filippatos TD
Received 20 February 2019
Accepted for publication 8 May 2019
Published 19 September 2019 Volume 2019:11 Pages 133—143
DOI https://doi.org/10.2147/CPAA.S172353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Arthur E. Frankel
Ioanna Papakitsou,1 George Vougiouklakis,1 Moses S Elisaf,2 Theodosios D Filippatos1
1Department of Internal Medicine, School of Medicine, University of Crete, University Hospital of Heraklion, Heraklion, Crete, Greece; 2Department of Internal Medicine, School of Medicine, University of Ioannina, Ioannina, Greece
Correspondence: Theodosios D Filippatos
Department of Internal Medicine, School of Medicine, University of Crete, University Hospital of Heraklion, Voutes, Crete, Heraklion, Crete 71500, Greece
Tel +30 281 340 2817
Email [email protected]
Abstract: Dapagliflozin belongs in the family of sodium-glucose cotransporter 2 (SGLT2) inhibitors and acts by reducing glucose reabsorption in the proximal tubule. The aim of this review is to present the differential pharmacology and clinical utility of dapagliflozin. Dapagliflozin is orally administered, has a long half-life of 12.9 hours and (similar to empagliflozin) is a much weaker SGLT1 inhibitor compared with canagliflozin. Dapagliflozin significantly decreases glycated hemoglobin and fasting glucose levels in patients with type 2 diabetes mellitus (T2DM). The drug improves body weight, blood pressure, uric acid, triglycerides and high-density lipoprotein cholesterol. In the DECLARE-TIMI 58 trial, a large trial of 17,160 T2DM patients with established cardiovascular disease (CVD) or without established CVD but with multiple risk factors, dapagliflozin compared with placebo resulted in a significantly lower rate of the composite outcome of CVD death or hospitalization for heart failure (HHF); this effect was mainly due to a lower rate of HHF in the dapagliflozin group (HR: 0.73; 95%CI: 0.61–0.88), whereas no difference was observed in the rate of CVD death (HR: 0.98; 95%CI: 0.82–1.17). Moreover, dapagliflozin was noninferior to placebo with respect to major adverse CVD events. Dapagliflozin exerts beneficial effects on albuminuria. Additionally, in the DECLARE-TIMI 58 trial it significantly reduced the composite renal endpoint (40% decrease in glomerular filtration rate, end stage renal disease, or renal death) in both patients with established CVD and patients with multiple risk factors (overall HR: 0.53; 95%CI: 0.43–0.66). However dapagliflozin, like the other SGLT2 inhibitors, is associated with an increased risk of genital and urinary tract infections (usually mild mycotic infections) and acute kidney injury in cases of reduced extracellular volume. Dapagliflozin is a useful antidiabetic treatment which also exerts beneficial effects in the management of heart failure and diabetic kidney disease.
Keywords: dapagliflozin, sodium-glucose cotransporter 2, cardiovascular disease, diabetes, kidney, adverse effects
Introduction
Diabetes mellitus (DM) is a multisystemic disease with serious impact on people’s quality of life and financial dynamics worldwide.1 A new class of antidiabetic drugs, the sodium-glucose cotransporter 2 (SGLT2) inhibitors have recently gained great interest. Glucose is absorbed in the urine in the proximal convoluted tubule by the SGLTs, which are energy consuming transporters on the brush border. This is mediated mainly by SGLT2 (90%) and SGLT1 (10%), resulting in reabsorption of 97% of daily filtrated glucose.2 A mechanical model for sodium-coupled sugar transport has been proposed, which suggests that sodium binds first to the extracellular side of the SGLT2 to open the outer gate, then glucose binds inducing a conformational change of the transporter leading to the release of sodium and glucose into the tubular cell interior.3 SGLT2 inhibitors prevent glucose reabsorption in the proximal convoluted tubule.4 Experimental models have shown that dapagliflozin acts specifically on the kidneys, which binds to the external surface of functional SGLT2 in the plasma membrane of proximal tubular cells surrounding the glomeruli, leading to inhibition of glucose binding.3
The aim of this review is to present the differential pharmacology and clinical utility of dapagliflozin, focusing on its effects on glucose regulation and DM management, renal function, blood pressure and body weight, lipid metabolism, and cardiovascular disease (CVD), as well as on adverse effects that have been recognized in clinical trials and postmarketing studies.
Pharmacology
Dapagliflozin is orally administered in doses of 5–10 mg. Peak plasma concentration is achieved in 1.5–2 hours in adults (Table 1).5 Food consumption does not significantly affect the efficacy of dapagliflozin.6 Dapagliflozin is mainly protein-bound and has the largest volume of distribution (118 L) between the SGLT2 inhibitors.5 Dapagliflozin, similar to empagliflozin and canagliflozin, has a long half-life of 12.9 hours, permitting it to be administered in single-dose regimens.7 Regarding SGLT2 inhibition, it is the second most potent agent, after ertugliflozin, with a maximal half-inhibitory concentration of 1.2 nM, followed by canagliflozin (2.7 nM) and empagliflozin (3.1 nM). Both dapagliflozin and empagliflozin are much weaker SGLT1 inhibitors compared with canagliflozin.5
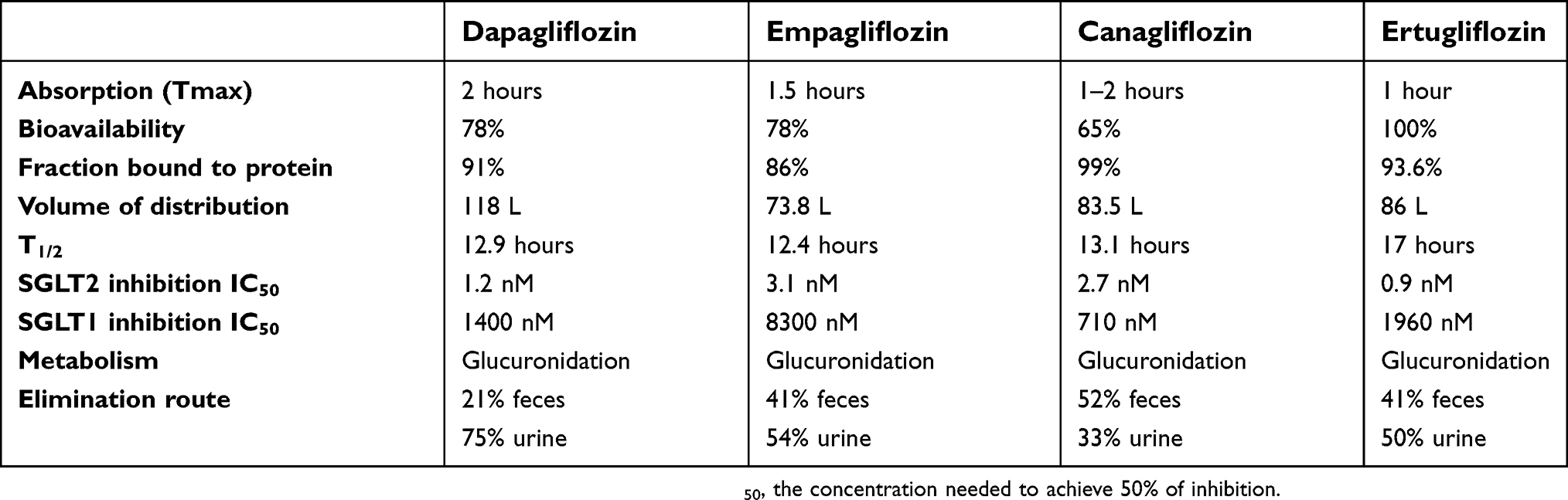 |
Table 1 Pharmacokinetic characteristics of currently approved SGLT2 inhibitors |
Dapagliflozin undergoes glucuronidation to dapagliflozin 3-O-glucoronate in the liver and the kidneys and is excreted in urine (75%) and bile (21%).8,9 Studies have shown increments in blood levels and maximum concentration of dapagliflozin and its metabolite, proportionately to the degree of kidney dysfunction.5 Similar with the other SGLT2 inhibitors, treatment with dapagliflozin should not be initialized in patients with estimated glomerular filtration rate (GFR) <60 mL/minute and discontinued with values <45 mL/minute.5
Effects of dapagliflozin
Effects on urinary glucose excretion, insulin sensitivity, beta cell function and glucagon
Owing to its mechanism of action, dapagliflozin-induced SGLT2 inhibition increases urinary glucose excretion dose-dependently. There is also substantial evidence that dapagliflozin enhances insulin sensitivity.10–13 In a study dapagliflozin was associated with a greater glucose disappearance rate (assessed by hyperinsulinemic and hyperglycemic clamps) compared with placebo. Additionally, the acute (within 10 minutes) insulin response was increased with dapagliflozin but was reduced with placebo.14 Beneficial effects have also been demonstrated in beta-cell function with dapagliflozin. A higher insulin concentration in beta cells was accompanied with reduced variability in glucose and insulin levels.15,16 A two-week dapagliflozin administration increased the area under the curve for c-peptide levels compared with placebo. The increased ratio of c-peptide increments to glucose difference from 0 to 120 minutes, along with an improved euglycemic clamp after treatment, suggested enhanced beta-cell function and improved insulin sensitivity.17 Dapagliflozin may also affect glucose metabolism by increasing glucagon levels, owing to increase of glucagon gene expression, reduction of hepatocyte nuclear factor 4α (HNF4A) and SGLT2 inhibition-induced decreased glucose and sodium influx in alpha-cells causing greater glucagon secretion.18,19
Effects on anthropometric and metabolic variables
Dapagliflozin has been shown to be beneficial regarding body weight, blood pressure and lipid parameters. In type 2 DM (T2DM) subjects with body mass index (BMI) >25 kg/m2 and glycated hemoglobin (HbA1c) >6.5% treated with dapagliflozin 5 mg for 12 weeks, apart from improved glycemic parameters, a reduction in body weight (−4 kg), a significant elevation in adiponectin levels and a reduction in C-reactive protein (CRP) levels were observed.20 Dapagliflozin 10 mg achieved reductions in body weight of 2.6, 4.3 and 4.6 kg after 14–90, 91–180 and beyond 180 days, respectively.21 A study involving 5,828 T2DM subjects showed reductions in body weight by 5 kg and systolic blood pressure by 3.1 mmHg after 12–24 months.22 In a meta-analysis of 55 placebo-controlled trials, dapagliflozin achieved significant weight reduction proportional to its dose. Mean weight loss by 1.30 kg, 1.51 kg, 1.70 kg and 2.24 kg were noted with doses of 2.5, 5, 10 and 20 mg, respectively (P<0.001).23 Indeed, dapagliflozin 5 mg for 24 weeks in T2DM patients induced a significant reduction in total fat mass, which was independently correlated with the improvement of anthropometric parameters (BMI, waist circumference, and waist to hip ratio, all P<0.001), while total body water and lean muscle mass remained unaffected.24
Dapagliflozin exerts beneficial effects on lipid profile.5 In T2DM subjects dapagliflozin significantly reduced triglycerides by 18 mg/dL, increased high-density lipoprotein cholesterol by 2.2 mg/dL, while low-density lipoprotein cholesterol (LDL-C) remained unaffected or slightly increased.25
In a meta-analysis of 62 studies dapagliflozin dose-dependently reduced uric acid levels (P<0.01). This effect persisted after long-term therapy, while it was abolished in patients with chronic kidney disease (CKD; GFR <60 mL/minute/1.73 m2).26 The reduction of serum uric acid levels has been attributed to uricosuria; possibly the SGLT2 inhibition-induced increased glucose levels stimulate uric acid excretion mediated by GLUT9 isoform 2 in the proximal tubule and the collecting duct.27
Utility in patients with DM
A randomized trial lasting 102 weeks showed that dapagliflozin as monotherapy significantly reduces HbA1c (−0.44% with 5 mg and −0.53% with 10 mg) compared with placebo.28 In treatment-naïve patients (baseline HbA1c 9%), dapagliflozin reduced HbA1c (−1.45%) similarly to metformin-XR (−1.44%).29 In another randomized double-blind phase 3 trial dapagliflozin reduced not only mean fasting plasma glucose (FPG) levels but also decreased mean amplitude of glucose excursions after 24 weeks.30
Dapagliflozin has been extensively studied as an adjunct therapy in T2DM patients. In a randomized double blind phase 3 placebo-controlled trial involving 400 patients suboptimally controlled with metformin twice daily, the addition of dapagliflozin 2.5 mg and 5 mg twice daily produced mean HbA1c reductions by −0.52% and −0.65% respectively, along with improvements in FPG and body weight at 16 weeks.31 Dapagliflozin in a triple regimen with metformin and saxagliptin produced greater reductions in FPG and HbA1c levels compared with placebo (−0.82% vs −0.07%) at week 24, while more patients reached the HbA1c goal of <7%.32 These effects were sustained at week 52.33 Dapagliflozin as an adjunct to metformin and sulphonylurea for 52 weeks in a trial involving 218 patients with baseline HbA1c 7–10% produced a relative reduction of HbA1c by −0.8% vs placebo at 52 weeks, while 27.3% and 11.3% of participants achieved the HbA1c goal in the treatment and placebo group, respectively.34
A clinical trial involving T2DM patients suboptimally controlled on insulin with up to two oral antidiabetic drugs showed reductions of HbA1c (−0.40% −0.59% and −0.57% with dapagliflozin 2.5, 5 and 10 mg, respectively) at week 24. Insulin dose was decreased by −7.60 IU, −6.28 IU and −6.82 IU with 2.5 mg, 5 mg and 10 mg respectively, while placebo was correlated with increases of 5.65 IU.35 At 104 weeks, mean reductions of HbA1c levels by −0.6 to −0.8% vs −0.4% with placebo were observed.36 Addition of dapagliflozin in suboptimally treated patients (HbA1c >7.5%) receiving large insulin doses (>30 IU/day) and up to three oral hypoglycemic drugs led to significant Hba1c reductions (−1.8%), as well as reduced total daily insulin dose (overall and individual mean reductions of 10.8 IU and up to 19.9 IU, respectively).37
A meta-analysis of 12 randomized controlled trials supported the above observations by indicating further mean reduction of HbA1c by −0.50% with dapagliflozin in patients receiving any preexisting antiglycemic therapy (P<0.01).38 A post-hoc analysis of pooled trials showed that HbA1c levels were reduced more in patients with baseline glycated hemoglobin (HbA1c) >10% compared with those with baseline HbA1c >9% or those with baseline <8% (0.77% and 1.32% vs 0.72% and 0.75% vs 0.26% and 0.37%, with respective doses of 5 mg and 10 mg) (Table 2).39
The drug’s action is attenuated in patients with compromised renal function. In the DERIVE study, that included patients with moderate renal failure (CKD stage 3a), dapagliflozin 10 mg significantly lowered HbA1c by a median of 0.34% (P<0.001).40 In patients with end-stage renal disease (stage 3b–4), although dapagliflozin significantly lowered blood pressure, body weight and urea-to-creatinine ratio, it did not significantly reduced HbA1c levels.41
Dapagliflozin has also been investigated as a complementary treatment in patients with type 1 DM (T1DM), in whom dose-dependent reductions in average plasma FPG, lower needs in insulin administration and improvement of glycemic parameters have been observed.42 A milestone on this matter is the DEPICT-1 study, a large-scale, multicenter, randomized double-blind phase 3 trial, where 775 T1DM patients inadequately controlled with insulin (mean HbA1c 8.53%) randomized to either dapagliflozin 5 mg, dapagliflozin 10 mg or placebo for 24 weeks. Dapagliflozin 5 mg, 10 mg and placebo induced mean reductions in HbA1c by −0.42%, −0.45%, −0.03%, and total daily insulin dose by −7.74%, −12.6% and +1.16%, respectively. The frequency of ketoacidosis, hypoglycemia and other adverse effects was indifferent between groups.43 Similar results were observed in the large-scale DEPICT-2 trial.44
Effects of dapagliflozin on CVD and heart failure (HF)
T2DM is a major cause of CVD morbidity and mortality worldwide and a risk factor for increased HF morbidity and mortality.45,46 In this context, the results of SGLT2 inhibitor trials are promising in terms of new ways of CVD and HF reduction in T2DM patients.47,48
A retrospective open cohort study, the CVD-REAL study, the first large real-world study of >300,000 patients with T2DM with and without established CVD, showed that the risk of all-cause death and hospitalization for heart failure (HHF) was significantly lower in patients treated with SGLT2 inhibitors compared with other glucose-lowering drugs (P<0.001).49 Dapagliflozin accounted for 42% of the total exposure time in the SGLT2 inhibitors class (Table 3).49 The extended CVD-REAL 2 study confirmed these findings indicating a class effect that may extend to the whole CVD risk continuum.50 Additionally, the CVD-REAL Nordic trial compared SGLT2 inhibitors with other glucose lowering drugs. In this multinational observational analysis the use of dapagliflozin accounted for 94% of the total SGLT2 inhibitor exposure time. Compared with other glucose-lowering drugs, the administration of SGLT2 inhibitors was associated with decreased CVD mortality (HR: 0.53; 95%CI: 0.40–0.71), major adverse CVD events (MACE; HR: 0.78; 95%CI: 0.69–0.87) and HHF (HR: 0.70;, 95%CI: 0.61–0.81; P<0·0001 for all).51
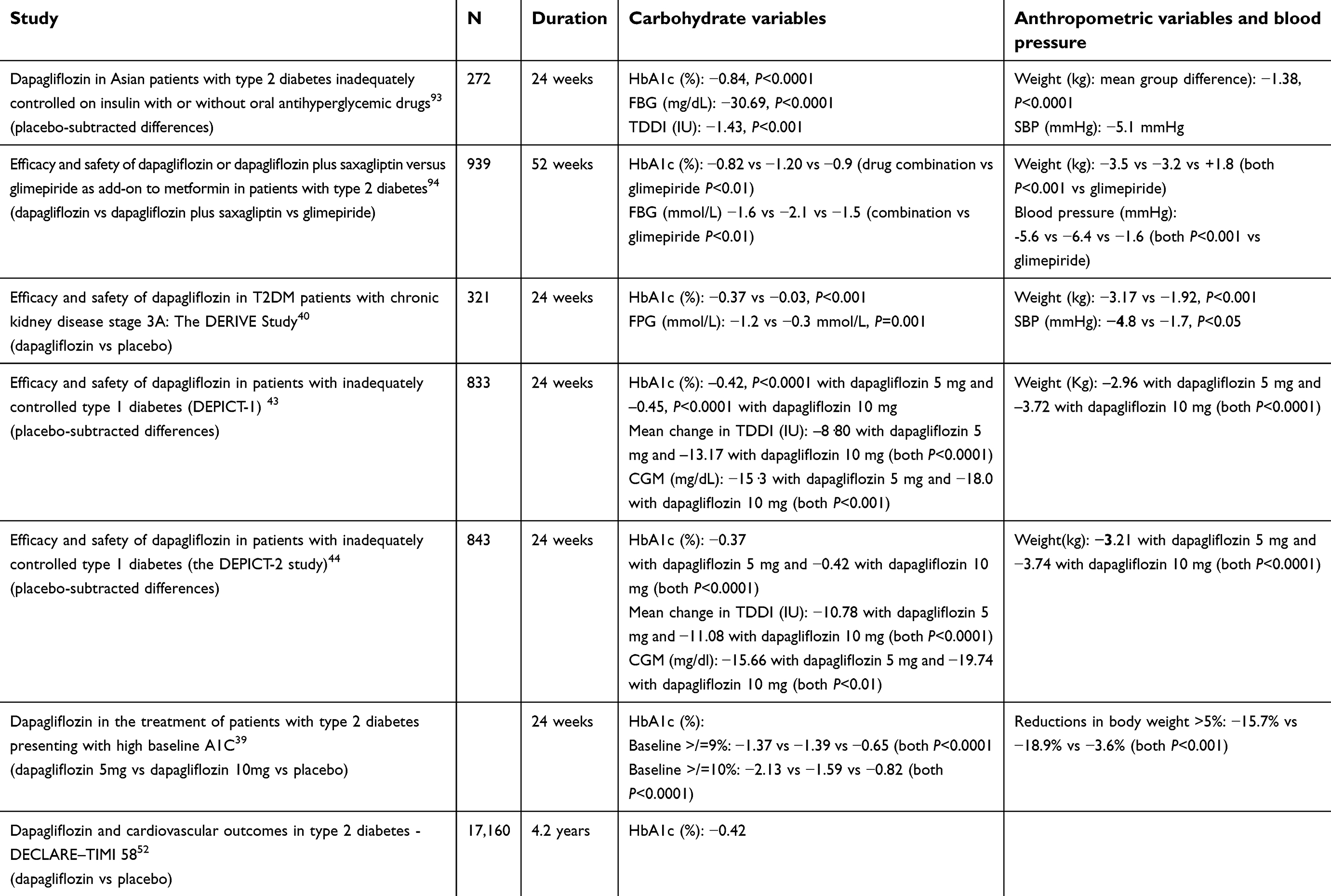 |
Table 2 Effects of dapagliflozin on anthropometric and metabolic variables in patients with type 2 diabetes |
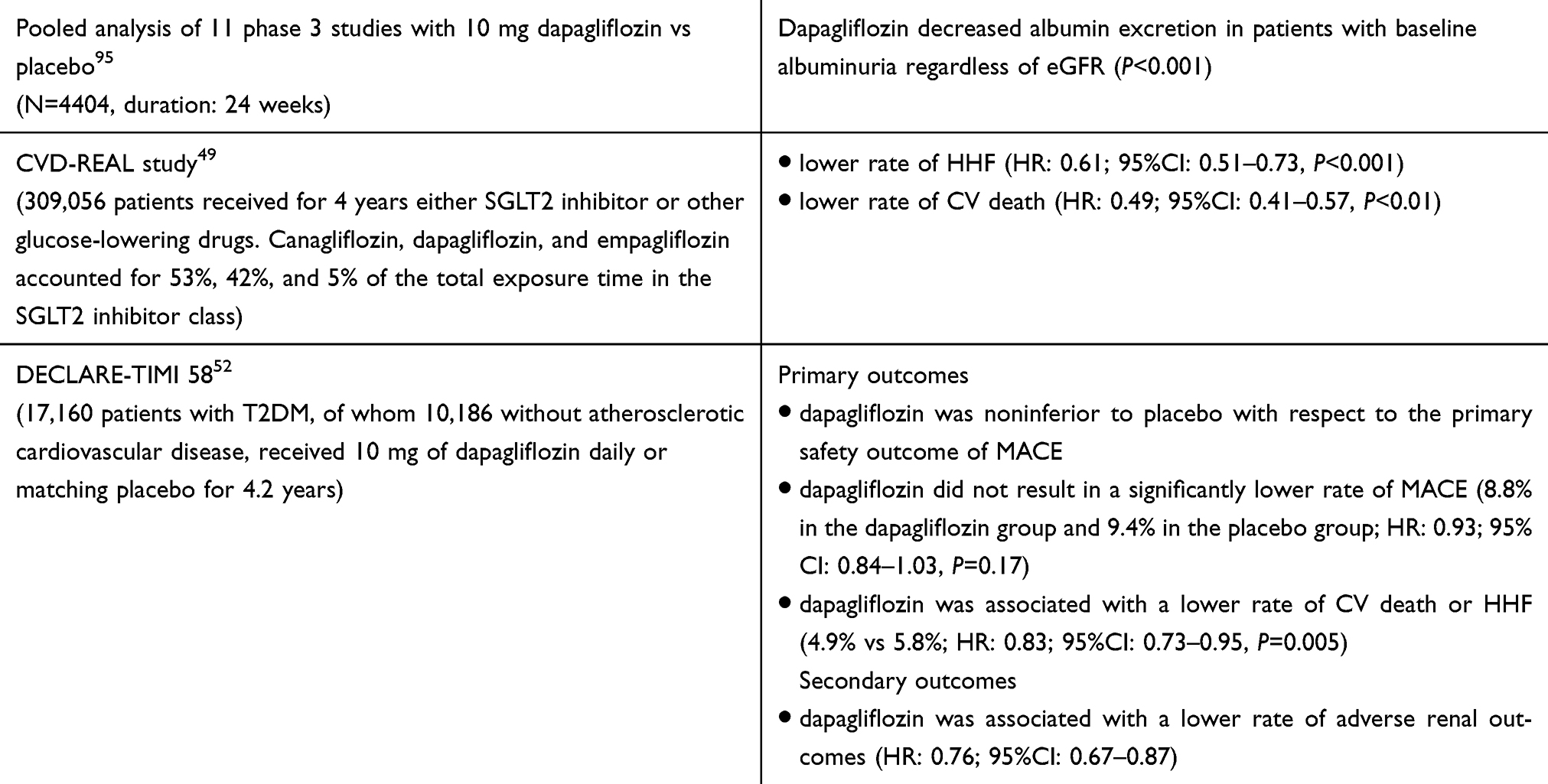 |
Table 3 Effects of dapaliflozin on renal function and cardiovascular events in large prospective trials and meta-analyses |
Recently the DECLARE-TIMI 58 trial assessed CVD outcomes with dapagliflozin in 17,160 T2DM patients with established CVD or without established CVD but with multiple risk factors.52 Dapagliflozin resulted in a lower rate of CVD death or HHF (4.9% vs 5.8%; HR: 0.83; 95%CI: 0.73–0.95, P=0.005), which mainly reflected a lower rate of HHF (HR: 0.73; 95%CI: 0.61–0.88). Dapagliflozin also met the prespecified criterion for noninferiority to placebo with respect to MACE. Mechanisms that may be involved in the cardioprotective properties of dapagliflozin and generally SGLT2 inhibitors include osmotic diuresis and natriuresis, reductions in plasma volume, blood pressure and arterial stifness and beneficial effects on metabolism.5,53–55Additionally, an increase in ketone body formation and oxidation that is observed during SGLT2 inhibitors treatment may have anti-arrhythmogenic properties.56 Furthermore, a direct beneficial effect on ventricular myocytes through a decrease of myocardial intracellular Na+ concentrations via inhibition of the myocardial Na+/H+ exchanger flux leading to a secondary reduction in intracellular and mitochondrial calcium has been also suggested as a potential cardioprotective mechanism of dapagliflozin.53,57,58
Current evidence suggests that, if not contraindicated, SGLT2 inhibitors should be the preferred therapy in T2DM patients who have HF.1 However CVD death rates in DECLARE-TIMI 58 trial were not significantly different between dapagliflozin and placebo (HR: 0.98; 95%CI: 0.82–1.17).52 The inclusion of mainly primary prevention patients, who generally have lower CVD risk compared with patients with established CVD, may have played a role in the observed differences in CVD death between DECLARE-TIMI 58 trial and the previous SGLT2 inhibitors trials.
Dapagliflozin and the kidney
DM is strongly related with CKD owing to hyperglycemia and many metabolic and hemodynamic alterations in kidney function.59 The EMPA-REG OUTCOME trial and the CANVAS program demonstrated that empagliflozin and canagliflozin exert significant renoprotective effects.47,48
Dapagliflozin exerts beneficial effects (compared with placebo) on urinary albumin to creatinine ratio in patients with normo-, micro- or macroalbuminuria.41,60–62 This effect is also seen in patients receiving angiotensin converting enzyme inhibitors or angiotensin receptor blockers.63 Additionally, in the DECLARE-TIMI 58 trial dapagliflozin significantly reduced the composite renal endpoint (40% decrease in GFR, end-stage renal disease, or renal death) in patients with established CVD disease (HR: 0.55; 95%CI: 0.41–0.75) and patients with multiple risk factors (HR: 0.51; 95%CI: 0.37–0.69),52 suggesting that nephroprotection is a class effect of SGLT2 inhibitors.
The proposed mechanisms for the cardioprotective and nephroprotective effects of dapagliflozin include64,65 (i) the improvement of hyperglycemia and insulin sensitivity, along with other metabolic effects such as uric acid reduction, (ii) the reduced inflammation, oxidative stress and oxygen‐consuming transport workload owing to reduced sodium and glucose reabsorption in the proximal renal tubules (indeed, it has been demonstrated that dapagliflozin may reduce proximal tubular cell injury),66,67 (iii) the blood pressure lowering effect, (iv) the increase in fasting glucagon,68 (v) the reduction in intraglomerular pressure owing to SGLT2 inhibition-induced increased sodium delivery to the macula densa, leading to constriction of afferent renal arterioles, (vi) the reduction of kidney fat deposition, which is considered ectopic fat that promotes diabetic kidney disease progression,60 (vii) the reversal of hypomagnesemia, which is correlated with a more rapid decline of renal function,69,70 (viii) the increase in erythropoietin levels that exhibits direct renoprotective effects,71 (ix) the increase in the production of ketone bodies, since they can be used as a more efficient energy substrate leading to reduction in renal hypoxia.72
Adverse effects
The adverse effects of dapagliflozin in clinical and postmarketing surveillance trials include:
Genital mycotic infections and urinary tract infections
Genital mycotic infections are the most common adverse effect of SGLT2 inhibitors (approximately 7% in clinical trials).73,74 Similarly with the other SGLT2 inhibitors, treatment with dapagliflozin is associated with a significant increase in genital tract infections compared with placebo (OR: 3.48; 95%CI: 2.33–5.20).75 These infections are observed particularly in women with a previous genital infection and in men with previous balanitis.76,77
Urinary tract infections (UTIs) are the second most common adverse effect in patients receiving SGLT2 inhibitors. The proposed pathophysiologic mechanism is that SGLT2 inhibitors-induced glycosuria provides a positive environment for bacterial growth in the urinary tract.78
A meta-analysis of 52 randomized controlled trials showed a dose-dependent association between dapagliflozin and the risk of UTIs and genital infections, which were more common in females.79 UTIs and genital infections are mostly observed at the beginning of treatment (first 24–26 weeks) with a decreased incidence thereafter.80 These infections are usually mild and usually resolve with conventional treatment (standard oral and topical antifungal therapies).80,81 Severe pyelonephritis has very low incidence and similar frequency with placebo.80
It should be mentioned that, according to the last FDA warnings, 12 cases of Fournier’s gangrene-necrotizing fasciitis of the perineum have been reported in patients on SGLT2 inhibitors since 2013. The rate of genital infections in the DECLARE-TIMI 58 trial was higher in dapagliflozin group compared with placebo, but the rate of Fournier’s gangrene was not (one case in the dapagliflozin group and five in the placebo group). However, clinicians should inform patients regarding the symptoms and signs of a genital infection or a UTI and advise them to seek medical help if they experience such symptoms in order to prevent severe infections of the genital area.
Increase in creatinine
An acute reversible decrease in GFR after the initiation of SGLT2 inhibitors treatment is usually observed, which is attributed to extracellular volume depletion along with the restoration of tubuloglomerular balance, both leading to a reduction of intraglomerular pressure.64,65,73,82,83 Thus, dapagliflozin should be administered very cautiously or even avoided in patients with hypovolemia, in patients receiving high doses of furosemide or other diuretics or drugs affecting renal hemodynamics such as renin angiotensin aldosterone system blockers or nonsteroidal anti-inflammatory agents.
Changes in lipid profile
SGLT2 inhibitors may induce a mild dose dependent increase in LDL-C, which appears to be a class effect of these drugs.5 However a single center, open-label, randomized, prospective study that included 80 T2DM patients showed that dapagliflozin markedly decreased the levels of the very atherogenic small dence LDL-C, whereas it increased the concentration of the less atherogenic lbLDL-C.84
Orthostatic hypotension
SGLT2 inhibitors block glucose reabsorption in the proximal convoluted tubule and have a diuretic effect that causes plasma volume contraction increasing the risk of hypotension.73,85 According to 13 placebo-controlled studies a slightly higher proportion of patients (~2%) receiving dapagliflozin compared with placebo experienced any measured orthostatic reaction over the entire 24-week observation period irrespective of baseline blood pressure category.86 Clinicians should evaluate thoroughly the patients’ volume status and the presence of risk factors when prescribing SGLT2 inhibitors.
Diabetic ketoacidosis
SGLT2 inhibitors have been related with a specific form of diabetic ketoacidosis (DKA), the so-called euglycemic DKA, which is defined as DKA without marked hyperglycemia. SGLT2 inhibitors induce glucagon release and reduce insulin resistance leading to an increased glucagon/insulin ratio that induces ketone reabsorption in the renal tubules, thus increasing the concentration of ketone bodies.11,87 This mild increase in ketone levels possibly represents a mechanism of cardioprotection and nephroprotection of SGLT2 inhibitors, based on the fact that ketones are energy efficient-substrates.53,64,72 In this context, mild ketonemia during dapagliflozin treatment had no clinical consequences but was significantly associated with improved insulin sensitivity.25 Euglycemic DKA is a severe metabolic complication related to insulin deficiency and lack of glucose utilization, which may be rarely developed in some patients receiving SGLT2 inhibitors in the setting of severe illness and a reduction in food intake and/or insulin doses or any factor that may increase insulin demand, such as stress or excessive alcohol intake.73,88–90
Conclusion
Dapagliflozin used as monotherapy or as add-on treatment in T2DM patients significantly decreases HbA1c and FPG levels and significantly improves body weight, blood pressure, uric acid, triglycerides and high-density lipoprotein cholesterol. Based on the results of the DECLARE-TIMI 58 trial, dapagliflozin is noninferior to placebo with respect to MACE and is associated with lower HHF risk. Dapagliflozin exerts beneficial effects on albuminuria and significantly reduces the progression of diabetic kidney disease. Dapagliflozin was not associated with increased risk of bone fractures or amputation.91 However, dapagliflozin increases the incidence of genital mycotic infections and UTIs, which are usually mild to moderate and respond to standard antimicrobial treatment. Attention is needed in patients receiving dapagliflozin who are prone to plasma volume reduction, in order to avoid acute kidney injury and orthostatic hypotension.
Based on the current evidence, dapagliflozin is promising for the management of HF and kidney disease even in the nondiabetic population, but we have to wait for the results of ongoing trials in such populations. The possible mechanisms of dapagliflozin-induced cardioprotection and nephroprotection need to be elucidated since they may reveal new treatment targets. In addition, dapagliflozin has been shown to affect other variables not directly related to DM; for example, in animal models it seems to have presumptive neuroprotective effects such as reductions in cognitive decline and preservation of synaptic plasticity.92 Further research is required to expand our understanding concerning the effects of dapagliflozin on the aforementioned parameters.
Disclosure
Dr Moses S. Elisaf reports personal fees from Astra-Zeneca, grants and personal fees from MSD, personal fees from Pfizer, Abbott, Sanofi-Aventis, Boehringer Ingelheim, Eli-Lilly and GSK. Dr Theodosios D. Filippatos reports lecture honoraria from Boehringer Ingelheim and Mylan. The authors report no other conflicts of interest in this work.
References
1. Davies MJ, D'Alessio DA, Fradkin J, et al. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2018;61(12):2461–2498. doi: 10.1007/s00125-018-4729-5
2. Hummel CS, Lu C, Loo DD, Hirayama BA, Voss AA, Wright EM. Glucose transport by human renal Na+/D-glucose cotransporters SGLT1 and SGLT2. Am J Physiol Cell Physiol. 2011;300(1):C14–21. doi: 10.1152/ajpcell.00388.2010
3. Ghezzi C, Loo DDF, Wright EM. Physiology of renal glucose handling via SGLT1, SGLT2 and GLUT2. Diabetologia. 2018;61(10):2087–2097. doi: 10.1007/s00125-018-4656-5
4. Whaley JM, Tirmenstein M, Reilly TP, et al. Targeting the kidney and glucose excretion with dapagliflozin: preclinical and clinical evidence for SGLT2 inhibition as a new option for treatment of type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2012;5:135–148. doi: 10.2147/dmso.s22503
5. Filippas-Ntekouan S, Tsimihodimos V, Filippatos T, Dimitriou T, Elisaf M. SGLT-2 inhibitors: pharmacokinetics characteristics and effects on lipids. Expert Opin Drug Metab Toxicol. 2018;14(11):1113–1121. doi: 10.1080/17425255.2018.1541348
6. Kasichayanula S, Liu X, Zhang W, et al. Effect of a high-fat meal on the pharmacokinetics of dapagliflozin, a selective SGLT2 inhibitor, in healthy subjects. Diabetes Obes Metab. 2011;13(8):770–773. doi: 10.1111/j.1463-1326.2011.01397.x
7. Tang W, Reele S, Hamer-Maansson JE, Parikh S, de Bruin TW. Dapagliflozin twice daily or once daily: effect on pharmacokinetics and urinary glucose excretion in healthy subjects. Diabetes Obes Metab. 2015;17(4):423–425. doi: 10.1111/dom.12425
8. Kasichayanula S, Liu X, Lacreta F, Griffen SC, Boulton DW. Clinical pharmacokinetics and pharmacodynamics of dapagliflozin, a selective inhibitor of sodium-glucose co-transporter type 2. Clin Pharmacokinet. 2014;53(1):17–27. doi: 10.1007/s40262-013-0104-3
9. Ghezzi C, Yu AS, Hirayama BA, et al. Dapagliflozin binds specifically to sodium-glucose cotransporter 2 in the proximal renal tubule. J Am Soc Nephrol. 2017;28(3):802–810. doi: 10.1681/asn.2016050510
10. Merovci A, Abdul-Ghani M, Mari A, et al. Effect of dapagliflozin with and without acipimox on insulin sensitivity and insulin secretion in T2DM males. J Clin Endocrinol Metab. 2016;101(3):1249–1256. doi: 10.1210/jc.2015-2597
11. Merovci A, Solis-Herrera C, Daniele G, et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J Clin Invest. 2014;124(2):509–514. doi: 10.1172/jci70704
12. Ramirez-Rodriguez AM, Gonzalez-Ortiz M, Martinez-Abundis E. Effect of dapagliflozin on insulin secretion and insulin sensitivity in patients with prediabetes. Exp Clin Endocrinol Diabetes. 2018:Epub ahead of print. doi: 10.1055/a-0664-7583
13. Gonzalez-Ortiz M, Mendez-Del Villar M, Martinez-Abundis E, Ramirez-Rodriguez AM. Effect of dapagliflozin administration on metabolic syndrome, insulin sensitivity, and insulin secretion. Minerva Endocrinol. 2018;43(3):229–235. doi: 10.23736/s0391-1977.16.02550-5
14. Mudaliar S, Henry RR, Boden G, et al. Changes in insulin sensitivity and insulin secretion with the sodium glucose cotransporter 2 inhibitor dapagliflozin. Diabetes Technol Ther. 2014;16(3):137–144. doi: 10.1089/dia.2013.0167
15. Joannides CN, Mangiafico SP, Waters MF, Lamont BJ, Andrikopoulos S. Dapagliflozin improves insulin resistance and glucose intolerance in a novel transgenic rat model of chronic glucose overproduction and glucose toxicity. Diabetes Obes Metab. 2017;19(8):1135–1146. doi: 10.1111/dom.12923
16. Tahara A, Takasu T, Yokono M, Imamura M, Kurosaki E. Characterization and comparison of sodium-glucose cotransporter 2 inhibitors: Part 2. Antidiabetic effects in type 2 diabetic mice. J Pharmacol Sci. 2016;131(3):198–208. doi: 10.1016/j.jphs.2016.06.004
17. Merovci A, Mari A, Solis-Herrera C, et al. Dapagliflozin lowers plasma glucose concentration and improves beta-cell function. J Clin Endocrinol Metab. 2015;100(5):1927–1932. doi: 10.1210/jc.2014-3472
18. Bonner C, Kerr-Conte J, Gmyr V, et al. Inhibition of the glucose transporter SGLT2 with dapagliflozin in pancreatic alpha cells triggers glucagon secretion. Nat Med. 2015;21(5):512–517. doi: 10.1038/nm.3828
19. Pedersen MG, Ahlstedt I, El Hachmane MF, Gopel SO. Dapagliflozin stimulates glucagon secretion at high glucose: experiments and mathematical simulations of human A-cells. Sci Rep. 2016;6:31214. doi: 10.1038/srep31214
20. Okamoto A, Yokokawa H, Sanada H, Naito T. Changes in levels of biomarkers associated with adipocyte function and insulin and glucagon kinetics during treatment with dapagliflozin among obese type 2 diabetes mellitus patients. Drugs R D. 2016;16(3):255–261. doi: 10.1007/s40268-016-0137-9
21. Wilding J, Bailey C, Rigney U, Blak B, Beekman W, Emmas C. Glycated hemoglobin, body weight and blood pressure in type 2 diabetes patients initiating dapagliflozin treatment in primary care: A retrospective study. Diabetes Ther. 2016;7(4):695–711. doi: 10.1007/s13300-016-0193-8
22. Wilding J, Bailey C, Rigney U, Blak B, Kok M, Emmas C. Dapagliflozin therapy for type 2 diabetes in primary care: Changes in HbA1c, weight and blood pressure over 2 years follow-up. Prim Care Diabetes. 2017;11(5):437–444. doi: 10.1016/j.pcd.2017.04.004
23. Cai X, Yang W, Gao X, et al. The association between the dosage of SGLT2 inhibitor and weight reduction in type 2 diabetes patients: A meta-Analysis. Obesity (Silver Spring). 2018;26(1):70–80. doi: 10.1002/oby.22066
24. Tobita H, Sato S, Miyake T, Ishihara S, Kinoshita Y. Effects of dapagliflozin on body composition and liver tests in patients with nonalcoholic steatohepatitis associated with type 2 diabetes mellitus: A prospective, open-label, uncontrolled study. Curr Ther Res Clin Exp. 2017;87:13–19. doi: 10.1016/j.curtheres.2017.07.002
25. Min SH, Oh TJ, Baek SI, et al. Degree of ketonaemia and its association with insulin resistance after dapagliflozin treatment in type 2 diabetes. Diabetes Metab. 2018;44(1):73–76. doi: 10.1016/j.diabet.2017.09.006
26. Zhao Y, Xu L, Tian D, et al. Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on serum uric acid level: A meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2018;20(2):458–462. doi: 10.1111/dom.13101
27. Chino Y, Samukawa Y, Sakai S, et al. SGLT2 inhibitor lowers serum uric acid through alteration of uric acid transport activity in renal tubule by increased glycosuria. Biopharm Drug Dispos. 2014;35(7):391–404. doi: 10.1002/bdd.1909
28. Bailey CJ, Morales Villegas EC, Woo V, Tang W, Ptaszynska A, List JF. Efficacy and safety of dapagliflozin monotherapy in people with Type 2 diabetes: a randomized double-blind placebo-controlled 102-week trial. Diabet Med. 2015;32(4):531–541. doi: 10.1111/dme.12624
29. Parikh S, Wilding J, Jabbour S, Hardy E. Dapagliflozin in type 2 diabetes: effectiveness across the spectrum of disease and over time. Int J Clin Pract. 2015;69(2):186–198. doi: 10.1111/ijcp.12531
30. Li FF, Gao G, Li Q, et al. Influence of dapagliflozin on glycemic variations in patients with newly diagnosed type 2 diabetes mellitus. J Diabetes Res. 2016;2016:5347262. doi: 10.1155/2016/5347262
31. Schumm-Draeger PM, Burgess L, Koranyi L, Hruba V, Hamer-Maansson JE, de Bruin TW. Twice-daily dapagliflozin co-administered with metformin in type 2 diabetes: a 16-week randomized, placebo-controlled clinical trial. Diabetes Obes Metab. 2015;17(1):42–51. doi: 10.1111/dom.12387
32. Mathieu C, Ranetti AE, Li D, et al. Randomized, double-blind, phase 3 trial of triple therapy with dapagliflozin add-on to saxagliptin plus metformin in type 2 diabetes. Diabetes Care. 2015;38(11):2009–2017. doi: 10.2337/dc15-0779
33. Mathieu C, Herrera Marmolejo M, Gonzalez Gonzalez JG, et al. Efficacy and safety of triple therapy with dapagliflozin add-on to saxagliptin plus metformin over 52 weeks in patients with type 2 diabetes. Diabetes Obes Metab. 2016;18(11):1134–1137. doi: 10.1111/dom.12737
34. Matthaei S, Bowering K, Rohwedder K, Grohl A, Parikh S. Dapagliflozin improves glycemic control and reduces body weight as add-on therapy to metformin plus sulfonylurea: a 24-week randomized, double-blind clinical trial. Diabetes Care. 2015;38(3):365–372. doi: 10.2337/dc14-0666
35. Wilding JP, Woo V, Soler NG, et al. [Long-term efficacy of dapagliflozin in patients with type 2 diabetes mellitus receiving high doses of insulin]. Dtsch Med Wochenschr. 2013;138 Suppl 1: S27-38. doi: 10.1055/s-0032-1305284
36. Wilding JP, Woo V, Rohwedder K, Sugg J, Parikh S. Dapagliflozin in patients with type 2 diabetes receiving high doses of insulin: efficacy and safety over 2 years. Diabetes Obes Metab. 2014;16(2):124–136. doi: 10.1111/dom.12187
37. Das G, Surya A, Abusahmin H. Use of dapagliflozin as an add-on to insulin therapy in patients with suboptimally controlled type 2 diabetes. Ther Adv Endocrinol Metab. 2018;9(8):269–270. doi: 10.1177/2042018818771434
38. Sun YN, Zhou Y, Chen X, Che WS, Leung SW. The efficacy of dapagliflozin combined with hypoglycaemic drugs in treating type 2 diabetes mellitus: meta-analysis of randomised controlled trials. BMJ Open. 2014;4(4):e004619. doi: 10.1136/bmjopen-2013-004619
39. Skolnik N, Bonnes H, Yeh H, Katz A. Dapagliflozin in the treatment of patients with type 2 diabetes presenting with high baseline A1C. Postgrad Med. 2016;128(4):356–363. doi: 10.1080/00325481.2016.1173514
40. Fioretto P, Del Prato S, Buse JB, et al. Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): The DERIVE Study. Diabetes Obes Metab. 2018;20(11):2532–2540. doi: 10.1111/dom.13413
41. Dekkers CCJ, Wheeler DC, Sjostrom CD, Stefansson BV, Cain V, Heerspink HJL. Effects of the sodium-glucose co-transporter 2 inhibitor dapagliflozin in patients with type 2 diabetes and Stages 3b-4 chronic kidney disease. Nephrol Dial Transplant. 2018;33(11):2005–2011. doi: 10.1093/ndt/gfx350
42. Henry RR, Rosenstock J, Edelman S, et al. Exploring the potential of the SGLT2 inhibitor dapagliflozin in type 1 diabetes: a randomized, double-blind, placebo-controlled pilot study. Diabetes Care. 2015;38(3):412–419. doi: 10.2337/dc13-2955
43. Dandona P, Mathieu C, Phillip M, et al. Efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (DEPICT-1): 24 week results from a multicentre, double-blind, phase 3, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(11):864–876. doi: 10.1016/S2213-8587(17)30308-X
44. Mathieu C, Dandona P, Gillard P, et al. Efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (the DEPICT-2 study): 24-Week results from a randomized controlled trial. Diabetes Care. 2018;41(9):1938–1946. doi: 10.2337/dc18-0623
45. Tancredi M, Rosengren A, Svensson AM, et al. Excess mortality among persons with type 2 diabetes. N Engl J Med. 2015;373(18):1720–1732. doi: 10.1056/NEJMoa1504347
46. Cavender MA, Steg PG, Smith SC,
47. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi: 10.1056/NEJMoa1504720
48. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi: 10.1056/NEJMoa1611925
49. Kosiborod M, Cavender MA, Fu AZ, et al. Lower risk of heart failure and death in patients initiated on sodium-glucose cotransporter-2 inhibitors versus other glucose-lowering drugs: The CVD-REAL study (Comparative Effectiveness of Cardiovascular Outcomes in New Users of Sodium-Glucose Cotransporter-2 Inhibitors). Circulation. 2017;136(3):249–259. doi: 10.1161/circulationaha.117.029190
50. Kosiborod M, Lam CSP, Kohsaka S, et al. Cardiovascular events associated with SGLT-2 inhibitors versus other glucose-lowering drugs: The CVD-REAL 2 study. J Am Coll Cardiol. 2018;71(23):2628–2639. doi: 10.1016/j.jacc.2018.03.009
51. Birkeland KI, Jorgensen ME, Carstensen B, et al. Cardiovascular mortality and morbidity in patients with type 2 diabetes following initiation of sodium-glucose co-transporter-2 inhibitors versus other glucose-lowering drugs (CVD-REAL Nordic): a multinational observational analysis. Diabetes Obes Metab. 2017;5(9):709–717. doi: 10.1111/dom.13081
52. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi: 10.1056/NEJMoa1812389
53. Filippatos TD, Liontos A, Papakitsou I, Elisaf MS. SGLT2 inhibitors and cardioprotection: a matter of debate and multiple hypotheses. Postgrad Med. 2019;131(2):82–88. doi: 10.1080/00325481.2019.1581971
54. Filippatos TD, Liberopoulos EN, Elisaf MS. Dapagliflozin in patients with type 2 diabetes mellitus. Ther Adv Endocrinol Metab. 2015;6(1):29–41. doi: 10.1177/2042018814558243
55. Filippatos TD, Tsimihodimos V, Elisaf MS. Mechanisms of blood pressure reduction with sodium-glucose co-transporter 2 (SGLT2) inhibitors. Expert Opin Pharmacother. 2016;17(12):1581–1583. doi: 10.1080/14656566.2016.1201073
56. Snorek M, Hodyc D, Sedivy V, et al. Short-term fasting reduces the extent of myocardial infarction and incidence of reperfusion arrhythmias in rats. Physiol Res. 2012;61(6):567–574.
57. Packer M, Anker SD, Butler J, Filippatos G, Zannad F. Effects of sodium-glucose cotransporter 2 inhibitors for the treatment of patients with heart failure: Proposalof a novel mechanism of action. JAMA Cardiol. 2017;2(9):1025–1029. doi: 10.1001/jamacardio.2017.2275
58. Baartscheer A, Schumacher CA, Wust RC, et al. Empagliflozin decreases myocardial cytoplasmic Na(+) through inhibition of the cardiac Na(+)/H(+) exchanger in rats and rabbits. Diabetologia. 2017;60(3):568–573. doi: 10.1007/s00125-016-4134-x
59. Soldatos G, Cooper ME. Diabetic nephropathy: important pathophysiologic mechanisms. Diabetes Res Clin Pract. 2008;82 Suppl 1:S75–79. doi: 10.1016/j.diabres.2008.09.042
60. Nixon A, Jaber L, Sugiyama S, et al. Impact of dapagliflozin therapy on renal protection and kidney morphology in patients with uncontrolled type 2 diabetes mellitus. Clin Pharmacol Drug Dev. 2018;10(6):466–477. doi: 10.1002/cpdd.461
61. Fioretto P, Stefansson BV, Johnsson E, Cain VA, Sjostrom CD. Dapagliflozin reduces albuminuria over 2 years in patients with type 2 diabetes mellitus and renal impairment. Diabetologia. 2016;59(9):2036–2039. doi: 10.1007/s00125-016-4017-1
62. Petrykiv SI, Laverman GD, de Zeeuw D, Heerspink HJL. The albuminuria-lowering response to dapagliflozin is variable and reproducible among individual patients. Diabetes Obes Metab. 2017;19(10):1363–1370. doi: 10.1111/dom.12936
63. Heerspink HJ, Johnsson E, Gause-Nilsson I, Cain VA, Sjostrom CD. Dapagliflozin reduces albuminuria in patients with diabetes and hypertension receiving renin-angiotensin blockers. Diabetes Obes Metab. 2016;18(6):590–597. doi: 10.1111/dom.12654
64. Tsimihodimos V, Filippatos TD, Elisaf MS. SGLT2 inhibitors and the kidney: Effects and mechanisms. Diabetes Metab Syndr. 2018;12(6):1117–1123. doi: 10.1016/j.dsx.2018.06.003
65. Tsimihodimos V, Filippatos TD, Filippas-Ntekouan S, Elisaf M. Renoprotective effects of SGLT2 inhibitors: Beyond glucose reabsorption inhibition. Curr Vasc Pharmacol. 2017;15(2):96–102. doi: 10.2174/1570161114666161007163426
66. Lin Q, Chen Y, Lv J, et al. Kidney injury molecule-1 expression in IgA nephropathy and its correlation with hypoxia and tubulointerstitial inflammation. Am J Physiol Renal Physiol. 2014;306(8):F885–895. doi: 10.1152/ajprenal.00331.2013
67. Dekkers CCJ, Petrykiv S, Laverman GD, Cherney DZ, Gansevoort RT, Heerspink HJL. Effects of the SGLT-2 inhibitor dapagliflozin on glomerular and tubular injury markers. Diabetes Obes Metab. 2018;20(8):1988–1993. doi: 10.1111/dom.13301
68. Tsimihodimos V, Filippatos TD, Elisaf MS. Effects of sodium-glucose co-transporter 2 inhibitors on metabolism: unanswered questions and controversies. Expert Opin Drug Metab Toxicol. 2017;13(4):399–408. doi: 10.1080/17425255.2017.1258055
69. Filippatos T, Tzavella E, Rizos C, Elisaf M, Liamis G. Acid-base and electrolyte disorders associated with the use of antidiabetic drugs. Expert Opin Drug Saf. 2017;16(10):1121–1132. doi: 10.1080/14740338.2017.1361400
70. Filippatos TD, Tsimihodimos V, Liamis G, Elisaf MS. SGLT2 inhibitors-induced electrolyte abnormalities: An analysis of the associated mechanisms. Diabetes Metab Syndr. 2018;12(1):59–63. doi: 10.1016/j.dsx.2017.08.003
71. Tsuruya K, Yoshida H, Suehiro T, Fujisaki K, Masutani K, Kitazono T. Erythropoiesis-stimulating agent slows the progression of chronic kidney disease: a possibility of a direct action of erythropoietin. Ren Fail. 2016;38(3):390–396. doi: 10.3109/0886022x.2015.1136874
72. Ferrannini E, Mark M, Mayoux E. CV protection in the EMPA-REG OUTCOME trial: A “thrifty substrate” hypothesis. Diabetes Care. 2016;39(7):1108–1114. doi: 10.2337/dc16-0330
73. Filippas-Ntekouan S, Filippatos TD, Elisaf MS. SGLT2 inhibitors: are they safe? Postgrad Med. 2018;130(1):72–82. doi: 10.1080/00325481.2018.1394152
74. Hussar DA, Purzycki DJ. Dapagliflozin propanediol, avanafil, and conjugated estrogens/bazedoxifene. J Am Pharm Assoc (2003). 2014;54(3):314; 316–318. doi: 10.1331/JAPhA.2014.14517
75. Vasilakou D, Karagiannis T, Athanasiadou E, et al. Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med. 2013;159(4):262–274. doi: 10.7326/0003-4819-159-4-201308200-00007
76. Jabbour S, Seufert J, Scheen A, Bailey CJ, Karup C, Langkilde AM. Dapagliflozin in patients with type 2 diabetes mellitus: A pooled analysis of safety data from phase IIb/III clinical trials. Diabetes Obes Metab. 2018;20(3):620–628. doi: 10.1111/dom.13124
77. Thong KY, Yadagiri M, Barnes DJ, et al. Clinical risk factors predicting genital fungal infections with sodium-glucose cotransporter 2 inhibitor treatment: The ABCD nationwide dapagliflozin audit. Prim Care Diabetes. 2018;12(1):45–50. doi: 10.1016/j.pcd.2017.06.004
78. Arakaki RF. Sodium-glucose cotransporter-2 inhibitors and genital and urinary tract infections in type 2 diabetes. Postgrad Med. 2016;128(4):409–417. doi: 10.1080/00325481.2016.1167570
79. Li D, Wang T, Shen S, Fang Z, Dong Y, Tang H. Urinary tract and genital infections in patients with type 2 diabetes treated with sodium-glucose co-transporter 2 inhibitors: A meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2017;19(3):348–355. doi: 10.1111/dom.12825
80. Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, List JF. Urinary tract infections in patients with diabetes treated with dapagliflozin. J Diabetes Complications. 2013;27(5):473–478. doi: 10.1016/j.jdiacomp.2013.05.004
81. Gadzhanova S, Pratt N, Roughead E. Use of SGLT2 inhibitors for diabetes and risk of infection: Analysis using general practice records from the NPS MedicineWise MedicineInsight program. Diabetes Res Clin Pract. 2017;130:180–185. doi: 10.1016/j.diabres.2017.06.018
82. Szalat A, Perlman A, Muszkat M, Khamaisi M, Abassi Z, Heyman SN. Can SGLT2 Inhibitors cause acute renal failure? Plausible role for altered glomerular hemodynamics and medullary hypoxia. Drug Saf. 2018;41(3):239–252. doi: 10.1007/s40264-017-0602-6
83. Hahn K, Ejaz AA, Kanbay M, Lanaspa MA, Johnson RJ. Acute kidney injury from SGLT2 inhibitors: potential mechanisms. Nat Rev Nephrol. 2016;12(12):711–712. doi: 10.1038/nrneph.2016.159
84. Hayashi T, Fukui T, Nakanishi N, et al. Dapagliflozin decreases small dense low-density lipoprotein-cholesterol and increases high-density lipoprotein 2-cholesterol in patients with type 2 diabetes: comparison with sitagliptin. Cardiovasc Diabetol. 2017;16(1):8. doi: 10.1186/s12933-016-0491-5
85. Halimi S, Verges B. Adverse effects and safety of SGLT-2 inhibitors. Diabetes Metab. 2014;40(6Suppl 1): S28-34. doi: 10.1016/s1262-3636(14)72693-x
86. Sjostrom CD, Johansson P, Ptaszynska A, List J, Johnsson E. Dapagliflozin lowers blood pressure in hypertensive and non-hypertensive patients with type 2 diabetes. Diab Vasc Dis Res. 2015;12(5):352–358. doi: 10.1177/1479164115585298
87. Daniele G, Xiong J, Solis-Herrera C, et al. Dapagliflozin enhances fat oxidation and ketone production in patients with type 2 diabetes. Diabetes Care. 2016;39(11):2036–2041. doi: 10.2337/dc15-2688
88. Chou YM, Seak CJ, Goh ZNL, Seak JC, Seak CK, Lin CC. Euglycemic diabetic ketoacidosis caused by dapagliflozin: A case report. Medicine (Baltimore). 2018;97(25):e11056. doi: 10.1097/MD.0000000000011056
89. Peters AL, Buschur EO, Buse JB, Cohan P, Diner JC, Hirsch IB. Euglycemic diabetic ketoacidosis: A potential complication of treatment with sodium–glucose cotransporter 2 inhibition. Diabetes Care. 2015;38(9):1687–1693. doi: 10.2337/dc15-0843
90. Rosenstock J, Ferrannini E. Euglycemic diabetic ketoacidosis: A predictable, detectable, and preventable safety concern with SGLT2 inhibitors. Diabetes Care. 2015;38(9):1638–1642. doi: 10.2337/dc15-1380
91. Katsiki N, Dimitriadis G, Hahalis G, et al. Sodium-glucose co-transporter-2 inhibitors (SGLT2i) use and risk of amputation: an expert panel overview of the evidence. Metabolism. 2019. doi: 10.1016/j.metabol.2019.04.008
92. Sa-Nguanmoo P, Tanajak P, Kerdphoo S, et al. SGLT2-inhibitor and DPP-4 inhibitor improve brain function via attenuating mitochondrial dysfunction, insulin resistance, inflammation, and apoptosis in HFD-induced obese rats. Toxicol Appl Pharmacol. 2017;333:43–50. doi: 10.1016/j.taap.2017.08.005
93. Yang W, Ma J, Li Y, et al. Dapagliflozin as add-on therapy in Asian patients with type 2 diabetes inadequately controlled on insulin with or without oral antihyperglycemic drugs: A randomized controlled trial. J Diabetes. 2018;10(7):589–599. doi: 10.1111/1753-0407.12634
94. Muller-Wieland D, Kellerer M, Cypryk K, et al. Efficacy and safety of dapagliflozin or dapagliflozin plus saxagliptin versus glimepiride as add-on to metformin in patients with type 2 diabetes. Diabetes Obes Metab. 2018;20(11):2598–2607. doi: 10.1111/dom.13437
95. Petrykiv S, Sjostrom CD, Greasley PJ, Xu J, Persson F, Heerspink HJL. Differential effects of dapagliflozin on cardiovascular risk factors at varying degrees of renal function. Clin J Am Soc Nephrol. 2017;12(5):751–759. doi: 10.2215/CJN.10180916
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.