")
Back to Journals » Patient Preference and Adherence » Volume 13
Differences in the perception of dental sounds: a preliminary study
Authors Karibe H , Koeda M , Aoyagi-Naka K, Kato Y, Tateno A, Suzuki H, Okubo Y
Received 7 February 2019
Accepted for publication 31 May 2019
Published 3 July 2019 Volume 2019:13 Pages 1051—1056
DOI https://doi.org/10.2147/PPA.S204465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hiroyuki Karibe,1 Michihiko Koeda,2 Kyoko Aoyagi-Naka,1 Yuichi Kato,1 Amane Tateno,2 Hidenori Suzuki,3 Yoshiro Okubo2
1Department of Pediatric Dentistry, School of Life Dentistry at Tokyo, Nippon Dental University, Tokyo, Japan; 2Department of Neuropsychiatry, Nippon Medical School, Tokyo, Japan; 3Department of Pharmacology, Nippon Medical School, Tokyo, Japan
Purpose: The sound of dental treatments can evoke anxiety in some dental patients. While women have shown greater dental anxiety than men, little is known about the gender differences in the perception of dental sounds. The purpose of this preliminary study was to evaluate differences in the perception of dental sounds according to the level of dental fear and gender.
Patients and methods: Based on the level of dental fear, 69 adults (39 women, 30 men; average age, 28.1±8.1 years) were categorized into four groups. Three types of sounds were presented to participants: two sounds associated with dental treatment and a neutral sound. All participants rated their emotional reaction to each sound on a visual analog scale.
Results: Significant differences were observed for ratings of valence and disgust for a dental drilling sound among the four groups (p=0.007 and 0.004, respectively). Female participants in the dental fear group rated the dental drilling sound as more negative and disgusting than did female participants in the control group (p=0.002 for both ratings). However, no significant differences were found in ratings between males in the dental fear and control groups.
Conclusion: Perception of dental sounds appears to differ by level of dental fear and by gender. Considering these differences may contribute to reducing fear in dental patients.
Keywords: dental anxiety, adult, auditory stimuli, sound, visual analog scale
Introduction
Fear of dentistry is a widespread problem as 64% of adults report anxiety regarding dental treatment.1 Epidemiological surveys have indicated that approximately 15% of the population suffer from debilitatingly high levels of dental fear and avoidance.2–4 Previous studies have suggested that one of the most anxiety-provoking experiences in dental treatment is dental drilling.5,6 Oosterink et al reported that past negative experiences of having a tooth drilled were a risk factor for dental fear.7 Thus, the sound of dental drilling may evoke fear or anxiety in patients with dental fears.
Recent epidemiological studies reported that in the general population, levels of dental anxiety were significantly higher in women compared to men.8,9 Moreover, studies with populations of children and youth have found more dental anxiety in girls than in boys.10,11 However, little is known about gender differences in the perception of sounds during dental treatment. This preliminary study aimed to evaluate differences in the perception of dental treatment sounds by level of dental fear and by gender. Based on existing research, we hypothesized that level of fear would be associated with negative feelings toward dental sounds and that women with high levels of dental fear would report more negative feelings toward dental sounds than other individuals. Our null hypotheses were that: 1) the level of dental fear would have no effect on the perception of dental treatment sounds; and 2) there would be no differences in the perception of dental sounds between men and women.
Materials and methods
Participants
The protocol of this study was approved by the Ethical Review Boards of the School of Life Dentistry, Nippon Dental University (NDU-T2013-30) and conformed to the guidelines of the Declaration of Helsinki. The sample size was estimated using the G*Power 3.1 statistical program (Heinrich Heine Universität Düsseldorf Experimentelle Psycologie, Düsseldorf, Germany).12 The effect size was estimated as 0.54, based on a pilot study. Power analysis indicated that the required total sample size for the four groups was 44 (11 per group) to detect this effect size with 80% power and a significance level of 5%.
Sixty-nine Japanese adults (39 women, 30 men; average age, 28.1±8.1 years; range, 18–50) were recruited from patients who visited the Nippon Dental University Hospital, Tokyo, Japan, and via an advertisement for this study in the surrounding community. All participants included in this study had previously visited a dental clinic, had received dental treatment, and were above 18 years of age. All participants had normal vision and hearing. None had a history of psychiatric disorder, significant physical illness, neurological disorder, or severe sensory-motor impairment. To avoid selection bias, we excluded participants who were engaged in the dental profession. After the procedures had been fully explained to the participants, written informed consent was obtained.
Psychological assessment
The level of dental fear was assessed using the self-report Dental Fear Survey (DFS).5 We used the Japanese version of the questionnaire in this study, for which the validity and reliability have been verified, and Cronbach’s alpha values have ranged from 0.94 to 0.96.13 The questionnaire addresses anxiety-provoking situations associated with dental treatment. It consists of 20 questions, rated on a five-point Likert scale ranging from 1 to 5, summed to give total scores between 20 and 100. The population mean score was estimated at 37.4 (standard deviation [SD] =14.1) for Japanese individuals.13 Based on a threshold score above 52 on the DFS (Japanese mean score +1 SD), participants were categorized into four groups. Twenty-four participants (13 women, 11 men) scored between 52 and 82 on the questionnaire and were therefore placed in the female dental fear (FF) and male dental fear (MF) groups. The remaining 45 participants (26 women, 19 men), with <52 points, were placed in the female control (FC) and male control (MC) groups.
Level of dental anxiety was evaluated with the Dental Anxiety Scale (DAS).14 The DAS consists of four items that assess self-reported anxiety to imagined dental situations. Responses are rated on a scale ranging from 1 to 5, with total scores ranging from 4 to 20. High scores indicate high anxiety.
To assess trait and state anxiety levels, participants completed the State-Trait Anxiety Inventory-Trait (STAI-T) and STAI-State (STAI-S).15 Level of depression was evaluated with the Self-Rating Depression Scale (SDS).16
Subjective ratings
Two sounds associated with dental treatment and a neutral sound were presented to participants. From among various dental treatments, we chose cavity preparation as the anxiety-evoking stimulus.17 As cavity preparation consists of dental drilling with a high-speed dental handpiece and vacuum suction, we employed dental drilling sounds using a high-speed dental handpiece (D1) and a vacuum suction sound (D2) as the dental treatment sounds, and a 2000 Hz pure tone (N) as a neutral sound. These sounds (all 80 dB) were randomly presented to participants for 5 seconds via noise-canceling headphone. Participants were able to listen to these sounds repeatedly as needed. Then, all participants rated their affective reaction regarding each sound on a 0–100 mm visual analog scale (VAS) for the emotional dimensions of valence (0 [very negative], 50 [neutral], 100 [very positive]) and disgust (from 0 [not at all] to 100 [extremely]).18 For these two ratings, the participants specified their level of agreement to each statement (ie, valence/disgust) by selecting a position along a 100 mm continuous line between two end-points. One examiner (K-AN) measured subjective ratings of participants on the 0–100 mm VAS.
Intra- and inter-examiner reliability
To test the intra- and inter-examiner reliability of the subjective ratings, we randomly selected 30 subjective ratings from five individuals. To evaluate the intra-examiner reliability, the measurements of subjective ratings were repeated by one examiner (K-AN) at least two weeks after the first measurement in a blinded and random order. To assess the inter-examiner reliability, the subjective ratings for each of the randomly selected samples were measured by another examiner (HK). We used these data to calculate Spearman’s rank correlation coefficient for the intra- and inter-examiner agreement. The measurements of subjective ratings were found to demonstrate excellent intra- and inter-examiner reliability (Spearman’s rank correlation coefficient, 0.998 and 0.995, respectively).
Statistical analysis
Before performing any multiple group comparisons, homogeneity of variance was assessed by the Levene test. Since the Levene test revealed no significant differences among the groups, one-way analysis of variance (ANOVA) was used to analyze group differences in age, DFS, DAS, STAI-T, STAI-S, and SDS scores. A p-value<0.05 was considered statistically significant. When one-way ANOVA revealed a significant difference among groups, Tukey’s honestly significant difference post-hoc test was used to identify group differences accounting for the significant p-value.
While the Levene test revealed significant differences in the subjective ratings among groups and sounds, the Kruskal-Wallis test was used to analyze group and sound differences. If a significant difference was found, the Mann-Whitney U-test was used with a pair of variables in the groups and sounds. Since six and three tests were performed for groups and sounds, respectively, Bonferroni’s adjustment was applied such that the alpha levels were p=0.0083 (ie, 0.05/6) for groups and p=0.0167 (ie, 0.05/3) for sounds. All analyses were performed using IBM SPSS Statistics for Windows, version 21.0 (IBM Japan, Tokyo, Japan).
Results
Psychological assessment
Table 1 shows the characteristics of the participants. Age, STAI-T, STAI-S, and SDS scores were not significantly different between the groups. Significant differences were observed in DFS and DAS scores between the groups, reflecting the level of dental fear.
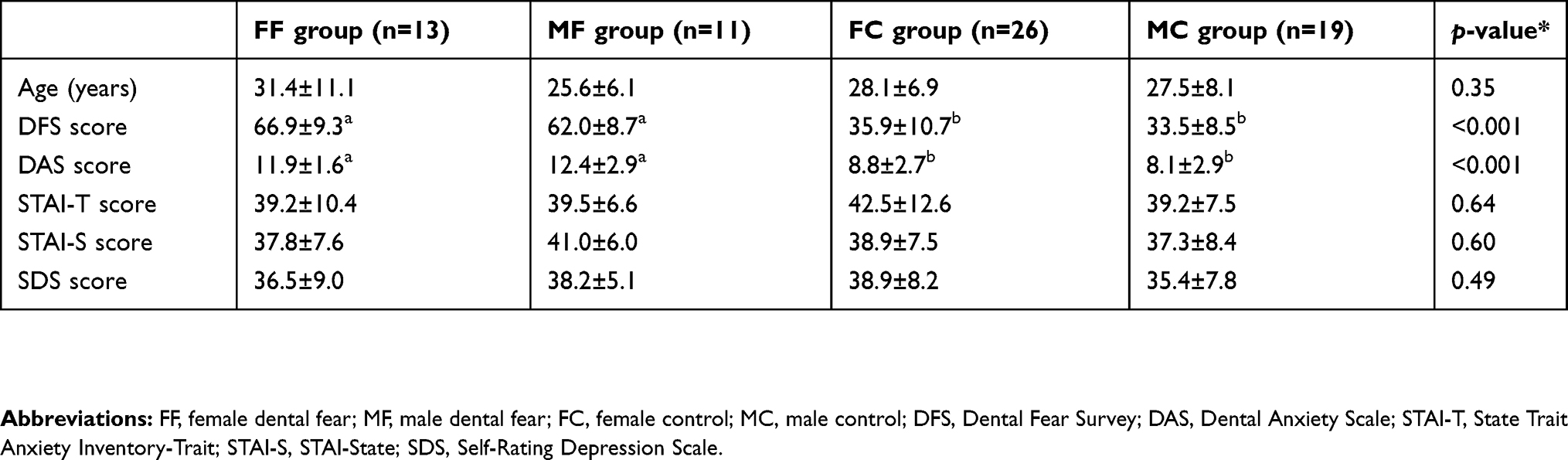 |
Table 1 Characteristics of the participants |
Subjective ratings among groups
Table 2 shows the subjective ratings of dental and neutral sounds in each group. There were significant differences in valence ratings for D1 and D2 and disgust ratings for D1 among the four groups. Participants in the FF group rated D1 more negatively than did those in the FC group (p=0.002), and rated D2 more negatively than did those in the FC and MC groups (p<0.001 and p=0.001, respectively). Participants in the FF group rated D1 as more disgusting than did those in the FC and MC groups (p=0.002 and 0.006, respectively). However, no significant differences were found in ratings between the MF and FC groups or the MF and MC groups. Further, no significant differences were observed for the emotional ratings of the N stimulus among the groups.
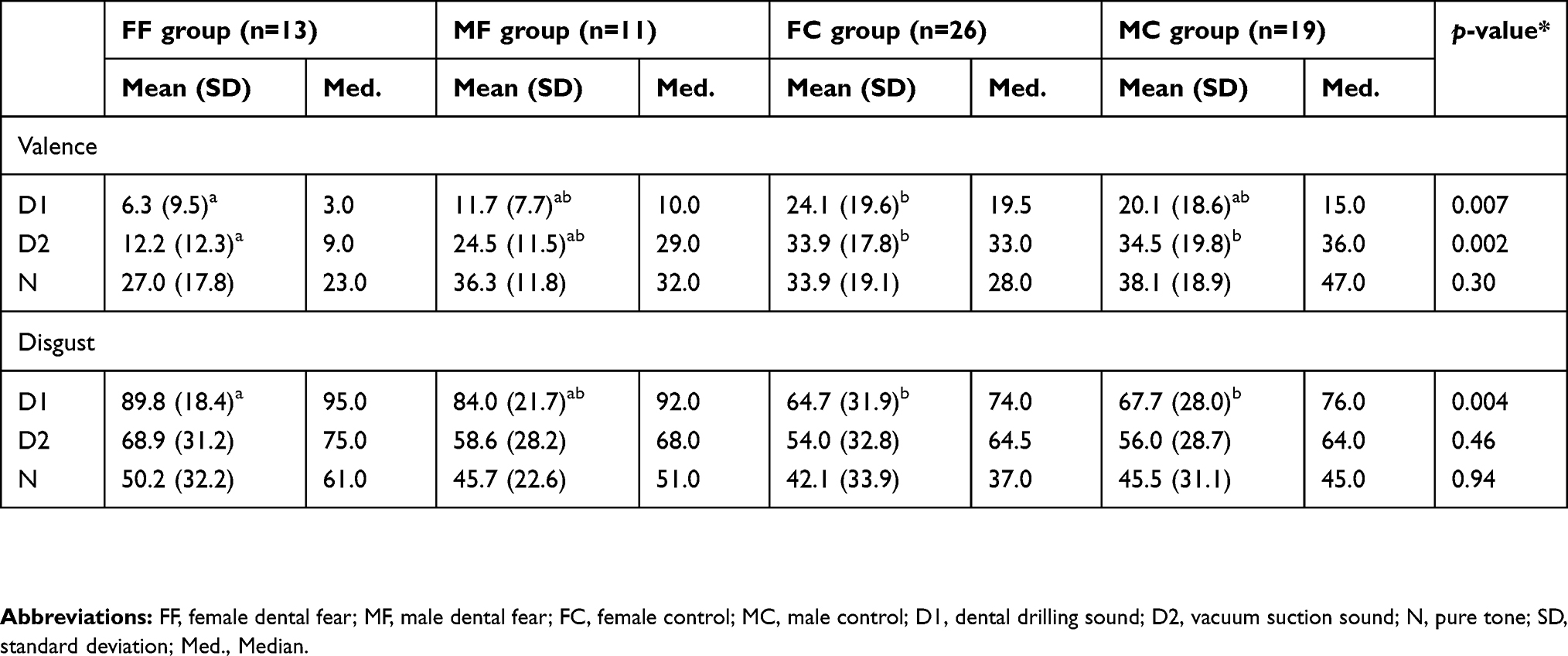 |
Table 2 Subjective ratings of dental and neutral sounds |
Subjective ratings among sounds
Figure 1 presents the differences in the subjective ratings of the three sounds for each group. In the FF and MF groups, significant differences in ratings of valence and disgust were found among the three types of sounds (p=0.002 for valence in FF group, p<0.001 for valence in MF group, and p=0.001 for disgust in both groups). Participants in the FF and MF groups rated D1 as more disgusting than did D2 and N (p=0.016 for D2 and p<0.001 for N in the FF group, p=0.004 for D2 and p<0.001 for N in the MF group, respectively). However, in the FC and MC groups, there was no significant difference in ratings of disgust among the sounds.
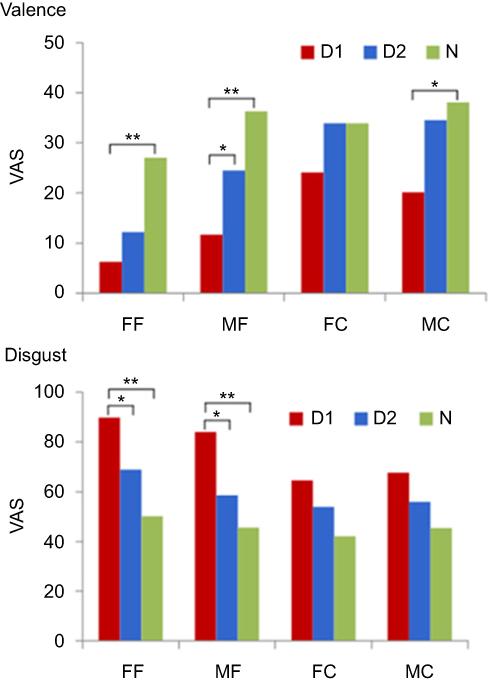 |
Figure 1 Differences in the subjective ratings of the three sounds; *p<0.0167, **p<0.001. Abbreviations: FF, female dental fear; MF, male dental fear; FC, female control; MC, male control; D1, dental drilling sound; D2, vacuum suction sound; N, pure tone; VAS, visual analog scale. |
Discussion
We presented the sounds of dental cavity preparation to participants and examined affective ratings of these sounds by level of dental fear and gender. Our results confirmed that female participants with dental fear rated the sound of dental drilling more negatively and as being more disgusting than did those women without dental fear. However, no significant differences were found in the ratings of the male participants with dental fear and those men without dental fear.
A recent study reported that people with high levels of trait anxiety have an increased likelihood of engaging in oral behaviors.19 Further, gender differences in the presence of oral behaviors have been identified and found to be more common in women. Trait anxiety was also found to be positively correlated with somatosensory amplification, which is related to bodily hypervigilance.19 However, in our study, the results of psychological assessments of participants in the four groups were similar except for those related to the level of dental fear. The mean values of STAI-T and STAI-S in a Japanese population were 38.8±9.7 and 36.6±9.0, respectively, and the mean values of SDS in a Japanese population were 35.7±14.8 in females and 35.1±8.0 in males, respectively.20,21 Thus, the levels of trait and state anxiety and depression in the four groups were within normal limits.
Köchel et al evaluated auditory symptom provocation in 25 female patients with dental phobia and 25 women without phobia, using the sound of a dental drill and pleasant and neutral sounds.22 They reported that patients rated the phobia-relevant sounds as more negative, more arousing, and more fear-eliciting than did the controls. Additionally, valence, arousal, and fear ratings did not differ between the female dental patients with phobia and those without phobia for neutral and pleasant sounds. From our results, we found that female participants with dental fear had greater disgust regarding the sound of dental drilling, and greater negative valence for the sound of vacuum suction than did control participants. However, affective ratings did not differ significantly among the groups for the neutral sound. These results are consistent with those of Köchel.
In our study, male participants with dental fear reacted to dental sounds similar to the control participants. To the best of our knowledge, few studies have evaluated gender differences in affective ratings of auditory stimulation related to dental procedures. Schienle et al conducted a functional magnetic resonance imaging experiment using pictures depicting dental treatment as visual symptom provocation and provided the first evidence of sex-specific brain activation and structure in patients with dental phobia.23 A future study using neuroimaging is needed to clarify gender differences in affective ratings of dental sounds as auditory symptom provocation.
We also compared subjective ratings of sounds in each group. These findings indicated that all participants with dental fear had more negative and disgust-related feelings regarding the sound of dental drilling compared to the sound of vacuum suction or the neutral sound. These findings are consistent with past studies.2,7,17 However, ratings of disgust did not differ significantly among sounds in control groups. Similarly, using standardized affective sounds in a functional near-infrared spectroscopy (fNIRS) study in healthy individuals, Plichta et al reported that unpleasant stimuli evoked more pronounced auditory cortex activation as compared to neutral stimuli.24 Although Plichta et al did not use dental sounds as unpleasant stimuli in their fNIRS study, enhanced sensory processing of emotional stimuli may objectively indicate levels of dental fear.
Despite our findings, this study does have some limitations. First, because convenience sampling was used, we did not select participants randomly, making it is difficult to generalize our findings to the general adult population of Japan. Second, data were based on the subjective report of the participants. Thus, it is difficult to objectively confirm whether the sound of dental drilling evoked strong aversion in participants. Future studies could include methods, such as neuroimaging to confirm the presence and level of emotional modulation during auditory stimulation. In addition, a larger cohort of participants with dental fear, together with a cohort of control participants is required to validate these results.
Conclusion
This study suggests that affective ratings of dental treatment sounds differ by level of dental fear and gender. In particular, women with dental fear may have a greater susceptibility to the sounds of dental drilling and vacuum suction. To reduce their dental fear, an effective sound masking technique such as using headphones/earphones or the application of dental instruments without sounds such as a spoon excavator could be recommended. Consideration of susceptibility to dental sounds may contribute to lowering dental fear in patients.
Ethics approval and informed consent
The study protocol was reviewed and approved by the Ethical Review Boards of the School of Life Dentistry, Nippon Dental University (NDU-T2013-30), and conformed to the guidelines of the Declaration of Helsinki. The participants provided written informed consent prior to participation.
Acknowledgments
We thank Editage for English language editing. This study was supported by the Japan Society for the Promotions of Science, Grant Numbers 25463266 and 17K12063.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Edmunds R, Buchanan H. Cognitive vulnerability and the aetiology and maintenance of dental anxiety. Community Dent Oral Epidemiol. 2012;40:17–25. doi:10.1111/j.1600-0528.2011.00636.x
2. Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 2013;58:390–407. doi:10.1111/adj.2013.58.issue-4
3. Seligman LD, Hovey JD, Chacon K, Ollendick TH. Dental anxiety: an understudied problem in youth. Clin Psychol Rev. 2017;55:25–40. doi:10.1016/j.cpr.2017.04.004
4. Nicolas E, Collado V, Faulks D, Bullier B, Hennequin M. A national cross-sectional survey of dental anxiety in the French adult population. BMC Oral Health. 2007;7:12. doi:10.1186/1472-6831-7-12
5. Kleinknecht RA, Klepac RK, Alexander LD. Origins and characteristics of fear of dentistry. J Am Dent Assoc. 1973;86:842–848. doi:10.14219/jada.archive.1973.0165
6. Berggren U, Meynert G. Dental fear and avoidance: causes, symptoms, and consequences. J Am Dent Assoc. 1984;109:247–251. doi:10.14219/jada.archive.1984.0328
7. Oosterink FM, De Jongh A, Aartman IH. Negative events and their potential risk of precipitating pathological forms of dental anxiety. J Anxiety Disord. 2009;23:451–457. doi:10.1016/j.janxdis.2008.09.002
8. Halonen H, Salo T, Hakko H, Räsänen P. Association of dental anxiety to personality traits in a general population sample of Finnish University students. Acta Odontol Scand. 2012;70:96–100. doi:10.3109/00016357.2011.645061
9. Humphris G, Crawford JR, Hill K, Gilbert A, Freeman R. UK population norms for the modified dental anxiety scale with percentile calculator: adult dental health survey 2009 results. BMC Oral Health. 2013;13:29. doi:10.1186/1472-6831-13-43
10. Klingberg G, Broberg AG. Dental fear/anxiety and dental behaviour management problems in children and adolescents: a review of prevalence and concomitant psychological factors. Int J Paediatr Dent. 2007;17:391–406. doi:10.1111/ipd.2007.17.issue-6
11. Katanec T, Singh S, Majstorovic M, Klaric I, Herman NG, Moursi AM. Gender differences in dental anxiety and medical fear in Croatian adolescents. J Clin Pediatr Dent. 2018;42:182–187. doi:10.17796/1053-4628-42.3.3
12. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41:1149–1160. doi:10.3758/BRM.41.3.691
13. Yoshida T, Milgrom P, Mori Y, et al. Reliability and cross-cultural validity of a Japanese version of the Dental Fear Survey. BMC Oral Health. 2009;9:17. doi:10.1186/1472-6831-9-17
14. Moore R, Berggren U, Carlsson SG. Reliability and clinical usefulness of psychometric measures in a self-referred population of odontophobics. Community Dent Oral Epidemiol. 1991;19:347–351. doi:10.1111/j.1600-0528.1991.tb00185.x
15. Spielberger C, Gorsuch R, Lushene R. STAI Manual for the State-Trait Anxiety Inventory (“Self-Evaluation Questionnaire”). Palo Alto, CA: Consulting Psychologists Press; 1970.
16. Thurber S, Snow M, Honts CR. The Zung self-rating depression scale: convergent validity and diagnostic discrimination. Assessment. 2002;9:401–405. doi:10.1177/1073191102238471
17. Oosterink FM, De Jongh A, Aartman IH. What are people afraid of during dental treatment? Anxiety-provoking capacity of 67 stimuli characteristic of the dental setting. Eur J Oral Sci. 2008;116:44–51. doi:10.1111/j.1600-0722.2008.00522.x
18. Lueken U, Hoyer J, Siegert J, Gloster AT, Wittchen HU. Symptom provocation in dental anxiety using cross-phobic video stimulation. Eur J Oral Sci. 2011;119:61–68. doi:10.1111/j.1600-0722.2010.00790.x
19. Chow JC, Cioffi I. Effects of trait anxiety, somatosensory amplification, and facial pain on self-reported oral behaviors. Clin Oral Investig. 2019;23:1653–1661. doi:10.1007/s00784-018-2600-1
20. Nakazato K, Shimonaka Y. The Japanese State-Trait Anxiety Inventory: age and sex differences. Percept Mot Skills. 1989;69:611–617. doi:10.2466/pms.1989.69.2.383
21. Fukuda K, Kobayashi S. A study on a self-rating depression scale. Seishin Shinkeigaku Zasshi. 1973;75:673–679. Japanese.
22. Köchel A, Plichta M, Schäfer A, Schöngassner F, Fallgatter A, Schienle A. Auditory symptom provocation in dental phobia: a near-infrared spectroscopy study. Neurosci Lett. 2011;503:48–51. doi:10.1016/j.neulet.2011.07.058
23. Schienle A, Scharmüller W, Leutgeb V, Schäfer A, Stark R. Sex differences in the functional and structural neuroanatomy of dental phobia. Brain Struct Funct. 2013;218:779–787. doi:10.1007/s00429-012-0428-z
24. Plichta MM, Gerdes AB, Alpers GW, et al. Auditory cortex activation is modulated by emotion: a functional near-infrared spectroscopy (fNIRS) study. Neuroimage. 2011;55:1200–1207. doi:10.1016/j.neuroimage.2011.01.011
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.