")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 7
Differences in sexual behavior, health, and history of child abuse among school students who had and had not engaged in sexual activity by the age of 18 years: a cross-sectional study
Authors Kastbom A, Sydsjö G , Bladh M, Priebe G, Svedin CG
Received 31 August 2015
Accepted for publication 8 October 2015
Published 8 January 2016 Volume 2016:7 Pages 1—11
DOI https://doi.org/10.2147/AHMT.S95493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Steven Youngentob
Åsa A Kastbom,1,2 Gunilla Sydsjö,3 Marie Bladh,3 Gisela Priebe,4,5 Carl Göran Svedin2
1Child and Adolescent Psychiatry, Linköping University Hospital, 2Division of Child and Adolescent Psychiatry and Department of Clinical and Experimental Medicine, Medical Faculty, Linköping University, Linköping, 3Department of Obstetrics and Gynecology, and Department of Clinical and Experimental Medicine, Medical Faculty, Linköping University, Linköping, 4Department of Psychology, Linnæus University, Växjö, 5Department of Child and Adolescent Psychiatry, Lund University, Lund, Sweden
Background: Empirical research about late sexual debut and its consequences is limited, and further research is needed.
Objective: To explore how students who had not had intercourse by the age of 18 years differed in terms of sociodemographic factors, physical and psychological health, sexual behavior, and history of sexual abuse from those who had.
Materials and methods: This is a cross-sectional survey involving 3,380 Swedish 18-year-olds. Descriptive analyses were used to investigate different types of sexual behavior. Ordinal data concerning alcohol consumption, self-esteem, sexual and physical abuse, parental relationships, sense of coherence, and health were analyzed, and multiple regression was carried out to identify the most important factors associated with no sexual debut.
Results: Just under a quarter of the adolescents had not had oral, anal, or vaginal sex by the age of 18 years, and they comprised the index group. They were characterized by being more likely to have caring fathers, parents born outside Europe, lower pornography consumption, lower alcohol and tobacco consumption, less antisocial behavior, and above all lower sexual desire (sometimes, adjusted odds ratio [aOR] 3.8; never/seldom, aOR 13.3) and fewer experiences of sexual abuse (aOR 25.5). Family structure and culture matters when it comes to the age of sexual debut.
Conclusion: Adolescents with no sexual debut at 18 years of age seemed to live a more stable and cautious life than more sexual experienced peers, exemplified by fewer antisocial acts, less smoking and alcohol/drug consumption, less sexual desire, and less experience of sexual abuse.
Keywords: adolescents, sexual abuse, sexual behavior, late sexual debut
Background
Empirical research about late sexual debut and its consequences is limited. Studies have tended to focus on early sexual debut and/or the consequences associated with sexual activities, such as unplanned pregnancies and sexually transmitted infections. Several studies have described relationships between early sexual debut and risky behavior, such as alcohol and drug consumption,1,2 antisocial behavior,3,4 and negative outcomes, such as sexually transmitted infections.3 Studies have also reported risk factors, such as poor parental relationships,5 low parental education,6 low academic achievement,7 less positive attitudes toward school,1 and living in a broken home.7 Much has been written about both the short-term and long-term risks of an early sexual debut, but there has been very little written about the factors associated with a late sexual debut. Sandfort et al analyzed data from the 1996 National Health Survey, a cross-sectional population study of adult Americans. They found that people who postponed their first sexual experience were less likely to have risky sexual partners or have sex under the influence of alcohol and drugs.8
To improve our understanding of sexual behavior among adolescents, it is important to look at both protective factors and risk factors. Sexual behavior in adolescence seems to depend on various factors, such as personality, gender, religiosity, ethnicity, family stability, onset of puberty, and experience of abuse. Baams et al described a relationship between sexual development and personality types that they split into three groups: resilient, undercontrollers, and overcontrollers. They showed that undercontrollers, defined as adolescents with low levels of impulse control, tended to be early sexual developers who engaged in more casual, advanced, and risky sexual behavior than others. Overcontrollers, defined as adolescents with low levels of emotional stability who were less open to experiences and extroverted behavior, engaged in fewer sexual experiences than others,9 and had more trouble engaging in social relations in general10 and in romantic and intimate relations in particular.11
The average age of a person’s sexual debut also differs according to religiosity and ethnicity. Religiosity had a protective association with sexual activity and number of partners among Latin American females in the US.12 Another American study that included both men and women aged between 15 and 21 years showed that those who viewed religion as very important were less likely to have made their sexual debut and had significantly fewer partners.13 Cavazos-Rehg et al studied racial and ethnic differences in sexual debut among high school students in grades 9–12 in 1999–2007 in the US. They found that like earlier studies, African-American males had the earliest debut, while Asian males and females had the latest.14
Landsford et al described a number of predictors of the timing of sexual debut. Family factors included race, parental monitoring knowledge, parent and peer relationships, and child characteristics, including IQ, association with deviant peers, and level of internalizing problems. They also claimed that biological factors, such as when puberty started, could predict sexual debut.4 Hormones and neurotransmitters such as dopamine and serotonin also played an important role in sexual behavior, sexual arousal, and satisfaction.15 Dopamine has been associated with motivation and reward-related behaviors, with high levels increasing sexual motivation and sexual behavior,16 while the release of serotonin has been reported to have an inhibitory influence on sexual behavior and libido.17 A well-known side effect of antidepressant selective serotonin-reuptake inhibitors is the decrease in both sexual desire and sexual functioning.18 Earlier research has found associations between experience of sexual and physical abuse and an early voluntary sexual debut, as well as alcohol intoxication being associated with that sexual debut.19,20
The aim of this study was to explore how students who had not initiated sexual activities – voluntary vaginal, oral, or anal sex – by the age of 18 years differed from those who had made their sexual debut, investigating such factors as sociodemographic background, sexual behavior, physical and psychological health, health behavior, self-esteem, sense of coherence, and experience of child sexual and/or physical abuse.
Materials and methods
Procedure and participants
This study emanated from a larger survey – Youth, Sex and the Internet – that was conducted in 2009 on behalf of the Swedish National Board for Youth Affairs and the Swedish government.21 A representative sample of Swedish high school seniors was selected by Statistics Sweden (gathers official statistics in Sweden) based on the information from the Swedish School Register. The sampling frame consisted of all students in the grade before the last grade of high school at schools with at least ten students. In total, there were 123,551 students at 754 schools in 2007. The sampling frame was stratified for number of students enroled at each school (10–190, 191–360, and more than 360 students) and educational programs (20 programs). A random sample that included at least one program at 150 schools was selected (7,700 students), and 119 schools chose to participate. Of the 5,792 enroled students at these schools, 3,503 participated in the study, resulting in a response rate of 60.5%. The sampling procedure, from the first information letter and two reminders to the schools, took 7 weeks (January–April), and there was no time for replacements of schools during the spring semester of 2009.
Information letters and questionnaires were mailed to the head teacher and teachers at each participating school. The students received written information about the study, and provided informed consent by choosing to answer the questionnaire. Parental consent was not required, according to the Swedish act concerning the ethical review of research involving humans, as the students were over the age of 15 years. The anonymous pen-and-paper questionnaire was distributed by school staff and completed in the classroom during school hours. It took the students 45–60 minutes to complete the questionnaires and return it in an unmarked envelope by post. Each school was offered €120 as compensation for the extra time it took for the school staff to handle, distribute, and collect the questionnaires, but the participants did not receive any personal incentives. The schools sent the completed questionnaires to Statistics Sweden. The adolescents were given information about where they could seek counseling if they needed support because of the issues raised by the questionnaire. A total of 3,503 students answered the questionnaire, a response rate of 60.5%. Five students were excluded from the sample, due to unserious or incomplete responses. The 38 participants who did not answer the question about their sexual debut and another 28 who did not identify themselves as either male or female were not included, because it was our intention to study gender differences. Finally, 52 students did not answer the questions about their experience of voluntary oral, anal, or vaginal sex. As a result, the sample used in this study consisted of 3,380 students – 1,566 (46.3%) male and 1,814 (53.7%) female – with a mean age of 18.3±0.6 years. The index questions in the questionnaire were whether they had ever had voluntary oral, anal, or vaginal sex with a teenager or an adult who was their own sex or the opposite sex. Of the total sample, the 830 (24.6%) who answered no to all the index questions formed the final index group. This group is compared throughout the entire paper with the comparison group of 2,550 students who had made their sexual debut.
The schools and students that did not participate did not skew the material in any direction. The only difference was that 22% of the sample had an immigrant background, compared to 19% of the general Swedish population (Sweden Statistics).
Measures
A questionnaire that included five well-known instruments was used to measure such factors as parental bonding (Parental Bonding Instrument [PBI]),22 rape-myth acceptance (Illinois Rape Myth Acceptance [IRMA] scale),23 sense of coherence (Sense of Coherence [SOC] scale),24 self-esteem (Rosenberg Self-Esteem Scale),25 and physical and psychological symptoms (Symptom Checklist [SCL]-25).26,27
Study-specific questions were divided into four categories. The first was background and sociodemographics, including parental bonding, love and consensual sexual experience, attitudes including rape-myth acceptance, health and health behavior, and factors related to abuse, including sense of coherence, self-esteem, and physical and psychological symptoms. Background and sociodemographic data referred to whether the adolescents were living with their parents or not, whether they were undertaking a theoretical, practical, or individual study program, whether they were born in Sweden or not, and whether their parents were employed or unemployed. “Employed” was defined as having a job, being on parental leave, or studying, and “unemployed” as not having a job or being a pensioner. Love and consensual sexual experience and attitudes were measured by sexual identification (heterosexual, homosexual, bisexual, or not sure), experience of sexual intercourse, and sexual desire (never/seldom, sometimes, or often/almost all the time). The adolescents were also asked if they ever watched pornography, defined as images or movies where one or more people are having sex with themselves or each other. In the category “health and health behavior”, the use of cigarettes, alcohol, and other drugs and different kinds of antisocial behaviors were measured. Antisocial behaviors included whether they had ever been away from home without their parents’ knowledge, been in a fight or hurt someone, hit or hurt an animal, been violent toward a teacher, or threatened or bullied someone. The number of antisocial acts – divided into zero to two incidents and three to five incidents – was measured. The questions about abuse included sexual abuse, sexual exploitation, and experience of physical abuse. Adolescents were asked if they had ever experienced sexual abuse. This was defined as someone touching their genitals or breasts against their will, trying to undress them to have sex with them, or making them masturbate or have vaginal, oral, or anal sex. To measure sexual exploitation, there was a question about whether the adolescent had ever sold sexual services.
Physical abuse by an adult was measured by asking the students if they had ever been pushed or shaken by an adult, if an adult had ever thrown something at them, hit them with their hand, fist or an object, or kicked, bitten, burnt, scalded, or tried to strangle them.
Parental Bonding Instrument
The PBI is a self-reporting measure of fundamental parental styles, which comprises two scales called care and overprotection or control, as perceived by the child.22 The measure is retrospective, meaning that people over 16 years of age complete the measure based on how they remember their parents’ behavior toward them during their first 16 years. The measure is completed separately for mothers and fathers. There are 25 questions, including 12 care items and 13 overprotection items. Each item is scored on a 4-point scale, where 3 is “very likely”, 2 is “moderately likely”, 1 is “moderately unlikely”, and 0 is “very unlikely”. High scores indicate a high level of care and overprotection. The PBI has been established as having good internal consistency and test–retest reliability and satisfactory construct and convergent validity.22 The Swedish-translated version of the instrument has been found to be reliable.21 Cronbach’s α for this study was 0.93.
Rape myths
The IRMA scale is used to explore attitudes toward sexual violence, and originally consisted of 45 questions. However, we used the shorter Swedish-translated version of 22 questions called the IRMA Short Form.23 The IRMA scale consists of both a general myth component and seven subcomponents. In this study, only the general myth component was used. Each item is scored on a 7-point scale, where 1 is “not at all” and 7 is “completely”. High scores indicate high acceptance of sexual violence and rape myths. The cutoff for high acceptance of sexual violence and rape myths is 80. Cronbach’s α for this study was 0.84.
Sense of Coherence scale
The SOC scale measures the individual’s sense of coherence, which is a global orientation that expresses the extent to which a person has a pervasive, enduring, and dynamic feeling of confidence.24 The SOC scale has been used in a number of previous studies, and has been shown to be valid and reliable.28 The Swedish version used in this study consisted of 13 items, each of which can be rated on a 7-point scale. A total score based on all items is calculated, and ranges between 13 and 91. High values indicate a strong sense of coherence. In this study, a weak sense of coherence was defined as values in the lowest quartile, with a score of ≤50. Cronbach’s α was 0.85 in this study.
Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale is translated to Swedish, and consists of ten items ranging from 0 for “strongly disagree” to 3 for “strongly agree”. The total score ranges from 0 to 30, with high values indicating high self-esteem.25 The cutoff was set at the 20th percentile, with values ≤16 indicating low self-esteem. Cronbach’s α was 0.89 in this study.
Symptom Checklist 25
The SCL-25 was developed from the SCL-90,26,27 translated into Swedish, and measures occurrence of psychiatric symptoms, mainly depression and anxiety, during the previous week. The measure consists of 25 items with a 4-point scale ranging from 1 for “not at all” to 4 for “extremely”. A total score ranging from 25 to 100 is calculated, with high values indicating a high symptom score. The cutoff was set at the 80th percentile, with values ≥53 indicating poor mental health. The SCL-25 has been shown to have acceptable reliability and validity.29 Cronbach’s α was 0.93 in this study. The adolescents in this study who had not made their sexual debut were called the index group and the adolescents who had made their sexual debut were called the comparison group.
Ethics
This study was approved by the Regional Ethical Review Board in Linköping, Sweden (220-08).
Data analysis
Statistical analyses were performed using SPSS version 22.0. Descriptive analyses were used to investigate the different types of sexual behavior among the adolescents, and are presented as percentages. The differences between male and female participants were investigated with Pearson’s χ2 using 95% confidence intervals. Ordinal data concerning alcohol consumption, self-esteem, sexual and physical abuse, parental relationships, sense of coherence, and health were analyzed by using Pearson’s χ2. The data were arranged into four different domains – socioeconomics, sexual experience, health factors, and abuse – categorized into no sexual debut and sexual debut, and then stratified by gender (Tables 1–4).
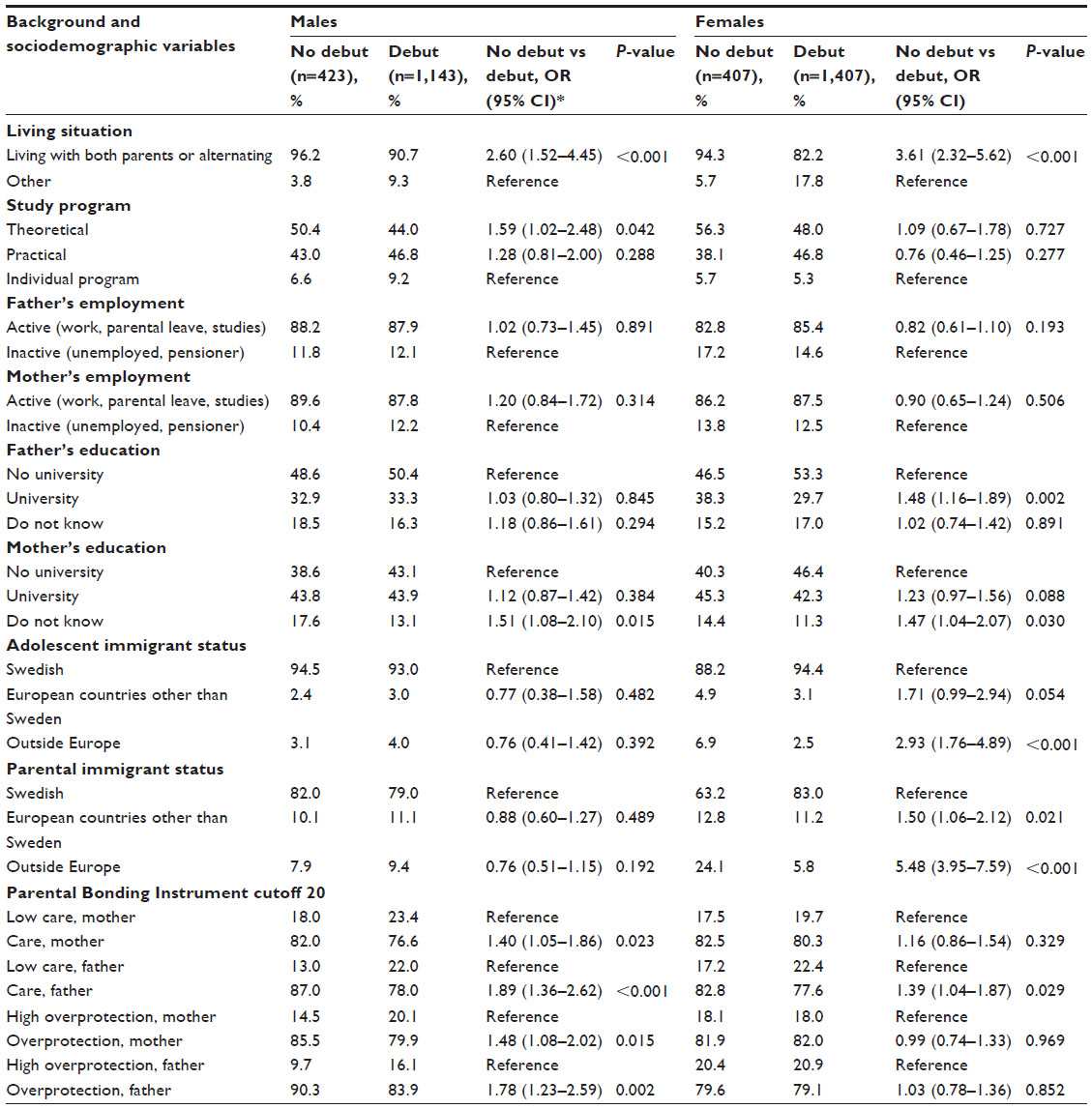 | Table 1 Distribution of background and sociodemographic variables by sexual debut and gender |
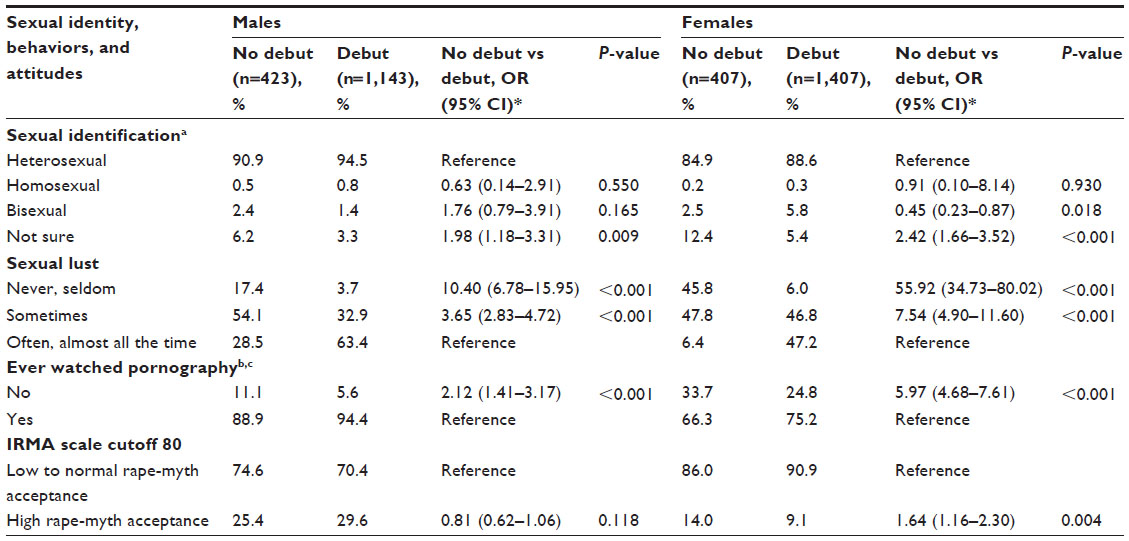 | Table 2 Distribution of sexual behavior and attitudes by sexual debut and gender |
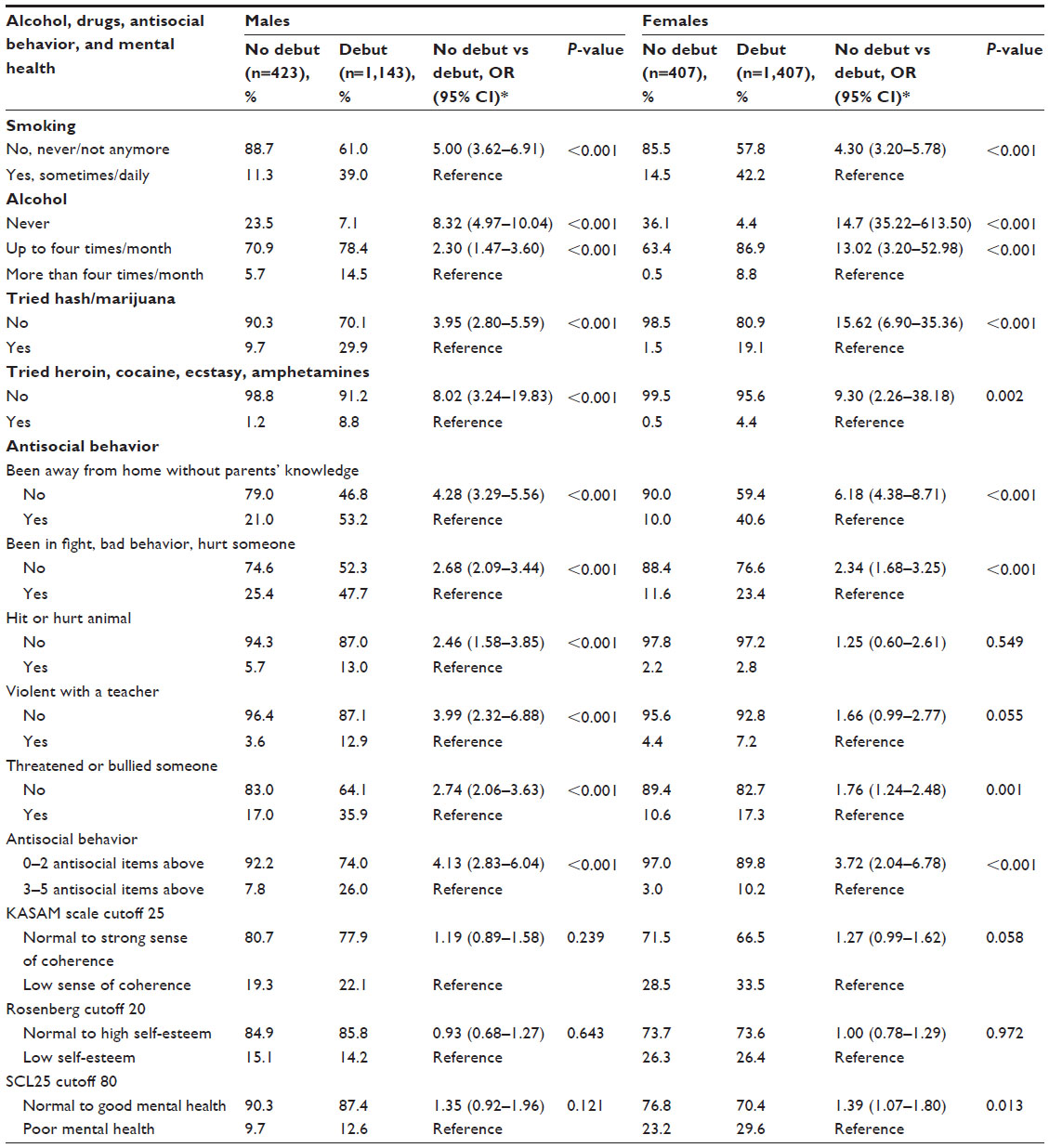 | Table 3 Distribution of health and health-behavior variables by sexual debut and gender |
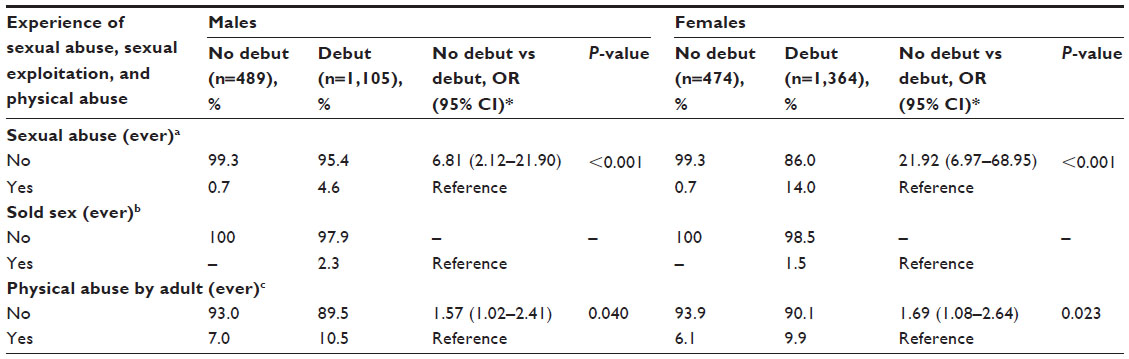 | Table 4 Distribution of sexual abuse, sexual exploitation, and physical abuse by sexual debut and gender |
Univariate analysis was carried out for the variables in Tables 1–4 – socioeconomics, sexual experience, health factors, abuse, and sexual debut age – and then categorized into the two groups, using no sexual debut as the index group and sexual debut as the comparison group. As no sexual debut was set as the index group, all variables entered into the logistic regression models had the least common event as the reference level in order to capture the factors that contributed the most to a later sexual debut. Entering all the statistically significant variables into one model was impossible, as there were too many variables for the multiple logistic analysis to handle. To overcome this problem, we performed multiple logistic regression analyses for each table. The most important variables from each table, ie, those variables that were statistically significant in the multiple logistic regression for each table, were then analyzed in a final multiple logistic regression with all the variables entered into the model. However, this became saturated, and a stepwise multiple regression was also performed.
Only the final model from the stepwise regression is displayed in the “Results” section. In order to accommodate as many of the independent factors as possible in the model, it was decided to collapse males and females into a combined group, and instead include gender as an independent factor. The outcome was the dichotomized variable for the no-debut index group compared to the sexual debut comparison group (Table 5). The number of participants differed between various analyses, as not all of the participants answered all the questions.
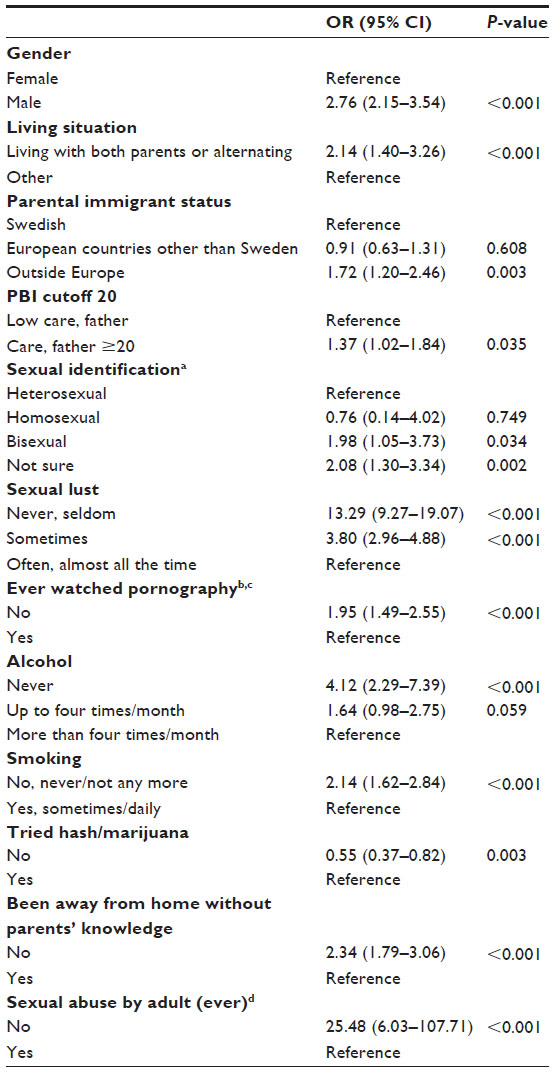 | Table 5 Multiple logistic regression |
Results
Sexual debut
There were 3,380 adolescents in our study, and 830 (24.6%) had not made their sexual debut at the age of 18 years (22.4% females and 27% males). They formed the index group. The remaining 2,550 had made their sexual debut, and they formed the comparison group. The mean age for sexual debut was 15.4 years for the total sample, 15.3 years for the females, and 15.5 years for the males.
Sociodemographic background and parental bonding
Male and female adolescents who had not made their sexual debut were significantly more likely to be living with their biological parents and less likely to be living on their own, in boarding schools, institutions, or foster care (Table 1). Females who were born outside Europe or had parents who were born outside Europe were three to five times less likely to have made their sexual debut (Table 1). There was almost no difference between the groups when it came to females and parental bonding, but the males in the index group were significantly more likely to have relationships with their parents that were based on care and normal control (Table 1).
Sexual behavior and attitudes
Twice as many males and females (odds ratio [OR] 1.98 and 2.42, respectively) in the index group were unsure about their sexual identity than peers who had made their sexual debut (Table 2). The adolescents in the index group reported significantly lower sexual lust and use of pornography than the males and females in the comparison group. The males in the index group were ten times more likely to report that they never or seldom felt sexual desire than the males in the comparison group, and this was 56 times higher among the females in the index group than the females in the comparison group. The OR for never having watched pornography was more than double for the males in the index group and six times higher for the females in the index group (Table 2). There was no difference concerning attitudes toward sexual violence, based on rape-myth acceptance, between the males but the females in the index group were significantly more likely to have tolerant attitudes toward sexual violence than the females in the comparison group, with an increase in OR of 1.64 (Table 2).
Health and health behavior
Males and females in the index group were significantly less likely to smoke or use alcohol and drugs than adolescents in the comparison group, with the adolescents in the index group having increased likelihoods for not having used drugs, alcohol, or tobacco that varied between two and 16 (Table 3). In addition, the index group reported significantly less antisocial behavior. It was more common for the adolescents in the comparison group to stay away from home at night without their parents’ knowledge, be in a fight, demonstrate antisocial behavior, or hurt someone (Table 3). Males in general were more likely to hit or hurt animals and were more violent to teachers than females, but the males in the index group were significantly less likely to demonstrate such behavior than the males in the comparison group (Table 3). No difference in sense of coherence or self-esteem was found between the two groups. Females in the index group had better mental health scores than females who had made their sexual debut (Table 3).
Experience of sexual and/or physical abuse
Experience of child abuse was significantly less common among both males and females in the index group. Those in the comparison group had increased ORs for sexual abuse and physical abuse (Table 4). None of the adolescents in the index group had ever sold sex.
Multiple analyses
Sociodemographics and being male increased the adjusted OR of adolescents not having made their sexual debut at the age of 18 years, as well as living with both biological parents or alternating between them (Table 5).
It was more common for adolescents in the index group to have a parent born outside Europe. Parental bonding style also had an impact. Adolescents whose fathers had normal to high caring parental styles demonstrated a 1.37-fold increase in their adjusted OR (aOR) for not having made their sexual debut by the age of 18 years.
When it came to sexual behavior and attitudes, the multiple analysis showed that it was more common for adolescents in the index group (aOR 2.08) to be unsure about their sexual identity than adolescents who had made their sexual debut. Adolescents in the index group showed little interest in sex, had low (aOR 3.80) or no sexual desire (aOR 13.29), and consumed very little pornography (Table 5).
With respect to health behavior, no sexual debut at 18 years of age positively correlated with no alcohol and tobacco consumption (Table 5). Adolescents in the index group reported significantly less experiences of sexual abuse (aOR 25.48) in relation to the adolescents in the comparison group (Table 5).
Discussion
This study compared adolescents who had not made their sexual debut by the age of 18 years with adolescents of the same age who had become sexually active, against a set of background factors. These were sociodemographics, health behavior, sexual behavior and attitudes, mental health, and experience of sexual and/or physical abuse. The results were summarized into five main findings.
First, adolescents living with both biological parents or alternating between them seemed to postpone their sexual debut. This supported earlier research from both Western and non-Western countries that an intact household or dual-parent family was seen as a protective factor6,13,30 and that family stress or impaired families were associated with risky sexual behavior and early sexual debut.31,32 This family cohesion was also strengthened by the adolescents in the index group, especially males, who perceived their fathers as more caring.
Second, immigration status mattered, especially for females. Females born outside Europe or with a parent born outside Europe were less likely to have made their sexual debut than females born in Sweden. As earlier studies have described, there were considerable racial/ethnic differences linked to the age of sexual debut, presumably depending on social expectations in different cultures and communities.33 However, further research about the age of sexual debut with regard to values, culture, ethnicity, and biological factors would add valuable information.
Third, adolescents in the index group watched less pornography and reported significantly lower sexual desire than the comparison group. This implied that those with low sexual interest and desire might make their sexual debut later than their peers. Since there was no information about their testosterone levels or status or stage of puberty in this study, it was impossible to confirm that testosterone levels correlated with desire, as shown in other research.34 Also, we could not establish any correlations due to other biological factors, such as neurotransmitter levels or medication that interacts with libido.15,18 Since dopamine is associated with reward-related behaviors,16 which can include sexual behaviors, one possible theory could be that the adolescents who had not made their sexual debut had low levels of dopamine or that they had not yet experienced the chemical rewards of sexual activity. Because serotonin has an inhibitory influence on libido,17 it would have been useful to know how many of the adolescents who had not made their sexual debut were on selective serotonin-reuptake inhibitors or had high serotonin levels for other reasons. Another contributing factor toward no sexual debut could have been the fact that adolescents in the index group were more likely to be uncertain about their sexual identity.
Fourth, the adolescents in the index group used less alcohol, tobacco, or other drugs, and showed less antisocial behavior than adolescents of the same age who had already made their sexual debut by the age of 18 years, and especially compared to adolescents with an early debut, defined as voluntary sexual intercourse before the age of 14 years, presented in another paper.35
Finally, adolescents in the index group had significantly less experience of sexual abuse than adolescents who had made their sexual debut by the age of 18 years, which supported findings in previous research.19,20 There was nothing to support the view that sexual abuse early in life could result in a delayed consensual sexual debut.
In consideration of all the information together, adolescents with no sexual debut at the age of 18 years seemed to live a more stable and more cautious life than peers with more sexual experience. The results tended to be similar to the overcontrollers described by Baams et al.9 This was also underlined by the fact that females in the index group seemed to have more balanced mental health, since they expressed a normal to high sense of coherence more often and reported better mental health than females in the comparison group. Since this finding did not belong to any primary aim of the study, we suggest that personality traits need to be explored in future studies of young people with late sexual debut.
Limitations
A limitation of this study was that the questionnaire, which contained a lot of sensitive questions, was distributed by school staff and completed by the adolescents in the classroom, which could have affected the answers. To maintain the integrity of the students, and to minimize the risk of them not answering the questions seriously, the class was optional and the students sat far away from each other. They were also given information about where to turn for counseling afterward. Another limitation is that this study included mostly Swedish and some Nordic and European-born adolescents, but only a few born outside Europe. Finally, the response rate of 60.5%, even if it is acceptable, does point to the need for some caution when interpreting the results. A part of this could be explained by the fact at that on a typical day, more than 10% of youths are absent from school.36 One assumption is that the absent group probably could have accentuated the results, since people dropping out from research more often come from problematic families and are burdened with more psychosocial health issues and lower motivation to participate both in school and in surveys.37
Conclusion
Adolescents who had not made their sexual debut by the age of 18 years seemed to have lived a more stable life than their sexually experienced peers, as they were more likely to live with one or two biological parents and tended to have more conservative attitudes, as they were less likely to consume pornography, alcohol, and tobacco, and reported less antisocial behavior. Culture or immigration status seemed be more important to females, since those who had not made their debut were more likely to have had a parent born outside Europe. The two most significant findings were that adolescents with no sexual debut at the age of 18 years reported significantly lower levels of sexual desire and fewer experiences of sexual abuse. This study provides relevant information in the scientific field of sexual behavior among adolescents, and contributes to earlier knowledge of the age of sexual debut and its associations. Based on this and other studies, early or late sexual debut seems to be the symptom or consequence of several factors during early childhood and adolescence, indicating that preventive measures of various kinds should be directed to families with very young children rather than informing specifically on the issue of sexual debut only.
The results imply that we need to raise awareness among parents and public health care workers about the importance of a stable emotional environment for children while growing up, and how risk behaviors, such as alcohol, tobacco, and drug consumption, antisocial behavior, and such risks as experience of sexual abuse, are just as important to discuss as the time for sexual debut.34,35
Acknowledgment
The authors would like to acknowledge the Swedish National Board for Youth Affairs for its financial support for this project.
Disclosure
The authors report no conflicts of interest in this work.
References
Makenzius M, Larsson M. Early onset of sexual intercourse is an indicator for hazardous lifestyle and problematic life situation. Scand J Caring Sci. 2013;27:20–26. | |
Cornelius JR, Clark DB, Reynolds M, Kirisci L, Tarter R. Early age of first sexual intercourse and affiliation with deviant peers predict development of SUD: a prospective longitudinal study. Addict Behav. 2007;32:850–854. | |
Ramrakha S, Bell ML, Paul C, Dickson N, Moffitt TE, Caspi A. Childhood behavior problems linked to sexual risk taking in young adulthood: a birth cohort study. J Am Acad Child Adolesc Psychiatry. 2007;46:1272–1279. | |
Lansford JE, Yu T, Erath S, Pettit GS, Bates JE, Dodge KA. Developmental precursors of number of sexual partners from age 16 to 22. J Res Adolesc. 2010;20:651–677. | |
Price MN, Hyde JS. Perceived and observed maternal relationship quality predict sexual debut by age 15. J Youth Adolesc. 2011;40:1595–1606. | |
Cavazos-Rehg PA, Spitznagel EL, Bucholz KK, et al. Predictors of sexual debut at age 16 or younger. Arch Sex Behav. 2010;39:664–673. | |
Price MN, Hyde J. When two isn’t better than one: predictors of early sexual activity in adolescents using a cumulative risk model. J Youth Adolesc. 2009;38:1059–1071. | |
Sandfort TGM, Orr M, Hirsch JS, Santelli J. Long-term health correlates of sexual debut: results from a national US study. Am J Public Health. 2008;98:155–161. | |
Baams L, Overbeek G, Dubas JS, van Aken MA. On early starters and late bloomers: the development of sexual behavior in adolescents across personality types. J Sex Res. 2014;51:754–764. | |
Denissen JJA, Asendorpf JB, van Aken MA. Childhood personality predicts long-term trajectories of shyness and aggressiveness in the context of demographic transitions in emerging childhood. J Pers. 2008;76:67–99. | |
Meeus W, Van de Schoot R, Klimstra T, Branje S. Personality types in adolescence: change and stability and links with adjustment and relationships: a five-wave longitudinal study. Dev Psychol. 2011;47:1181–1195. | |
Edwards LM, Haglund K, Fehring RJ, Pruszynski J. Religiosity and sexual risk behaviors among Latina adolescents: trends from 1995 to 2008. J Womens Health (Larchmt). 2011;20:871–877. | |
Haglund KA, Ferring RJ. The association of religiosity, sexual education, and parental factors with risky sexual behaviors among adolescents and young adults. J Relig Health. 2010;49:460–472. | |
Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, et al. Age of sexual debut among US adolescents. Contraception. 2009;80:158–162. | |
Argiolas A, Melis MR. The neurophysiology of the sexual cycle. J Endocrinol Invest. 2003;26:20–22. | |
Hull EM, Muschamp JW, Sato S. Dopamine and serotonin: influences on male sexual behavior. Physiol Behav. 2004;15:291–307. | |
Hull EM. Sex, drugs and gluttony: how the brain controls motivated behaviors. Physiol Behav. 2011;25:173–177. | |
Cascade E, Kalali AH, Kennedy SH. Real-world data on SSRI antidepressant side effects. Psychiatry (Edgmont). 2009;6:16–18. | |
Dahle T, Dalen HA, Meland E, Breidablik HJ. Uonskede seksuelle erfaringer og helseplager blant ungdom [Unwanted sexual experiences and health complaints among adolescents]. Tidsskr Nor Laegeforen. 2010;130:1912–1916. Norwegian. | |
Valle AK, Røysamb E, Sundby J, Klepp KI. Parental social position, body image, and other psychosocial determinants and first intercourse among 15- and 16-year olds. Adolescence. 2009;44:479–948. | |
Priebe G. Svedin CG. Prevalence, characteristics, and associations of sexual abuse with sociodemographics and consensual sex in a population-based sample of Swedish adolescents. J Child Sex Abus. 2009;18:19–39. | |
Parker G. Parental Overprotection. New York: Grune & Stratton; 1983. | |
Payne DL, Lonsway KA, Fitzgerald LF. Rape myth acceptance: exploration of its structure and its measurement using the Illinois Rape Myth Acceptance Scale. J Res Pers. 1999;33:27–68. | |
Antonovsky A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well. San Francisco: Jossey-Bass; 1987. | |
Rosenberg M. Society and the Adolescent Self-Image. Collingdale (PA): Diane Publishing Co; 1999. | |
Derogatis LR. SCL-90:Administration, Scoring and Procedures Manual-I for the R(evised) Version and Other Instruments of the Psychopathology Rating Series. Baltimore: Johns Hopkins University School of Medicine; 1977. | |
Nettelbladt P, Hansson L, Stefansson CG, Borgquist L, Nordström G. Test characteristics of the Hopkins Symptom Check List-25 (HSCL-25) in Sweden, using the Present State Examination (PSE-9) as a caseness criterion. Soc Psychiaty Psychiatr Epidemiol. 1993;28:130–133. | |
Eriksson M, Lindström B. Validity of Antonovsky´s sense of coherence scale: a systematic review. J Epidemiol Community Health. 2005;59:460–466. | |
Strand BH, Dalgard OS, Tambs K, Rognerud M. Measuring the mental health status of the Norwegian population: a comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nord J Psychiatry. 2003;57:113–118. | |
Lammers C, Ireland M, Resnick M, Blum R. Influences on adolescents’ decision to postpone onset of sexual intercourse: a survival analysis of virginity among youths aged 13 to 18 years. J Adolesc Health. 2000;26:42–48. | |
Tsitsika A, Greydanus D, Konstantoulaki E, et al. Adolescents dealing with sexuality issues: a cross sectional study in Greece. J Pediatr Adolesc Gynecol. 2010;23:298–304. | |
Goldberg RE. Family instability and early initiation of sexual activity in Western Kenya. Demography. 2013;50:725–750. | |
Kinsman SB, Romer D, Furstenberg FF, Schwarz DF. Early sexual initiation: the role of peer norms. Pediatrics. 1998;102:1185–1192. | |
van Anders SM. Testosterone and sexual desire in healthy women and men. Arch Sex Behav. 2012;41:1471–1484. | |
Kastbom AA, Sydsjö G, Bladh M, Priebe G, Svedin CG. Sexual debut before the age of 14 leads to poorer psychosocial health and risky behavior later in life. Acta Paediatr. 2015;104:91–100. | |
Uppsala Municipality. Utvärdering av elevernas övergång från grundskolan till gymnasieskolan. 2014. Utbildnings- och arbetsmarknadsnämnden UAN-2004-0081. | |
Farrington DP, Gallagher B, Morley L, St Ledger RJ, West DJ. Minimizing attrition in longitudinal research: methods of tracing and securing cooperation in a 24-year follow-up study. In: Magnusson D, Bergman LR, editors. Data Quality in Longitudinal Research. Cambridge, UK: Cambridge University Press; 1990:122–147. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.