")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Differences in etiological beliefs about schizophrenia among patients, family, and medical staff
Authors Tarakita N, Yoshida K, Sugawara N , Kubo K, Furukori H, Fujii A, Nakamura K, Yasui-Furukori N
Received 27 August 2018
Accepted for publication 10 December 2018
Published 27 December 2018 Volume 2019:15 Pages 137—142
DOI https://doi.org/10.2147/NDT.S185483
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Natsumi Tarakita,1,2 Kazutaka Yoshida,1 Norio Sugawara,3 Kazutoshi Kubo,1,4 Hanako Furukori,5 Akira Fujii,2 Kazuhiko Nakamura,1 Norio Yasui-Furukori1
1Department of Neuropsychiatry, Graduate School of Medicine, Hirosaki University, Hirosaki, Japan; 2Department of Mental Health, Mutsu City Hospital, Mutsu, Japan; 3Department of Clinical Epidemiology, Translational Medical Center, National Center of Neurology and Psychiatry, Kodaira, Tokyo, Japan; 4Department of Neuropsychiatry, Hirosaki-Aiseikai Hospital, Hirosaki, Japan; 5Department of Neuropsychiatry, Kuroishi-Akebono Hospital, Kuroishi, Japan
Objectives: To determine whether etiological beliefs are different among schizophrenia patients, their family, and medical staff.
Patients and methods: A cross-sectional study was performed at five hospitals and one mental clinic and included 212 patients, 144 family members, and 347 medical staff other than psychiatrists. A questionnaire about the possible etiological causes of schizophrenia was used.
Results: There were significant differences in response scores among the three groups on using Angermeyer’s and Goulding’s classifications. Factor analyses revealed the following four subscales: Psychosocial, Biological, Environmental, and Cultural connotations. The structure varied among patients, family, and medical staff.
Conclusion: The perspectives of schizophrenia etiology were different among patients, family, and medical staff.
Keywords: schizophrenia, etiology, perception, family, caregivers, beliefs, etiological causes, patients, medical staff
Introduction
Schizophrenia is the most common psychiatric disorder, and it negatively impacts not only the general population but also patients and their families. Our understanding of schizophrenia has progressed through advances in epidemiology and neuroimaging; but for over four decades, the dopamine hypothesis has remained the leading pathoetiologic theory of schizophrenia.1–3 Additionally, schizophrenia represents complex and multidimensional phenotypes with high heritability rates, exceeding 80% in twin studies.4–6 On the other hand, numerous environmental factors have been found to play an important role in the causality of schizophrenia. Factors that have been found to increase the risk of schizophrenia7,8 include cannabis use,9 chronic psychosocial stressors, including childhood adversity,10 migration/ethnic minority status,11 and urbanicity.12 Furthermore, acute stress plays a role in triggering psychotic symptoms,13,14 and impaired stress tolerance is associated with prodromal symptoms.15
Beliefs about pathoetiology are associated with attitudes toward persons with mental illnesses.16 Pathways to accessing health care are believed to be influenced by the beliefs of family members about the cause of the illness.17,18 In Western countries, biological and psychosocial causes are more common than supernatural causes.19–21 In contrast, non-Western cultures tend to endorse supernatural causes.22,23 However, there was no information on beliefs regarding schizophrenia in Japan, which is a developed country but is not fully influenced by Western culture. In fact, the major difference in beliefs about the causes of illness in the general population was that Australians were more likely to believe that illnesses were caused by viruses, infections, or allergies, or that they were inherited or genetic, while the Japanese were more likely to fault a nervous personality or weakness of character.24
A Cochrane review of hospital-based studies of limited quality concluded that psychoeducation for schizophrenia seems to reduce relapse and readmission and encourage medication compliance, as well as reduce the length of hospital stay.25 Psychoeducation may be defined as educating a person with a psychiatric disorder in subject areas that serve treatment and rehabilitation goals. This definition implies that there is a focus on knowledge and etiological beliefs surrounding schizophrenia.
Beliefs about the pathoetiology of schizophrenia have been shown to influence the perceptions of those affected and their likelihood to seek treatment.26–28 This study investigated the beliefs and knowledge of patients and family regarding the causes or etiology of schizophrenia. The study setting was in Aomori, which is in the countryside of Japan. Aomori is famous for its culture, which is a unique combination of Shamanism and Buddhism.29 Additionally, the objective of this study was to examine the differences in the factor structure of a 30-item list of possible causes of schizophrenia as perceived by patients, family, and medical staff.
Subjects and methods
The study was conducted between July and December 2015 in six separate mental clinics and psychiatric hospitals in Aomori, Japan. This study was approved by the ethical committees of Hirosaki University and each hospital. All participants provided written informed consent, and this study was conducted in accordance with the Declaration of Helsinki. Patients and family members were recruited from the same facilities. Medical staff, including pharmacists, psychologists, psychiatric nurses, clerks, psychiatric social workers, and staff who cooked and delivered hospital meals, were recruited from two psychiatric hospitals (Kuroishi-Akebono Hospital and Hirosaki-Aiseikai Hospital) and the Department of Neuropsychiatry, Mutsu General Hospital; all of the staff came into contact with schizophrenia patients. Questionnaires were hand delivered in envelopes to the staff. The questionnaires were collected by mail. The recovery rates were 72% for patients, 68% for family members, and 89% for the medical staff.
For each sample of patients, basic demographic information such as age, gender, education level, and duration of illness were collected. Each sample provided data on etiological beliefs, obtained using the 30-item list of the possible causes of schizophrenia, which was measured on a 4-point Likert scale.30,31 For each of the 30 causes, patients were asked, “Is this a cause of your disease?”; families were asked, “Is this a cause of your family’s disease?”; and medical staff were asked, “Is this a cause of schizophrenia?”. All participants were instructed to select either “no”, “possibly”, “likely”, or “very likely”. Participants who left >5 of the 30 items blank were excluded from the analyses, resulting in a final sample size of n=214, 145, and 347, respectively.
All analyses were performed using SPSS 25.0 (IBM Corporation, Tokyo, Japan). Answers of “no”, “possibly”, “likely”, and “very likely” were scored 1, 2, 3, and 4, respectively. Factor analysis was performed using the principal axis factoring method with oblique (promax) rotation. This factor analysis was performed within the medical staff group alone. ANOVA was performed followed by Tukey’s test to detect differences among patients, family, and medical staff. P<0.05 was considered significant.
Results
The mean age (years) of patients, family members, and medical staff was 46.0±11.7, 44.1±12.6, and 37.8±8.1, respectively. There were significant differences in response scores among the three groups. Using Angermeyer’s classification, which is the five conceptually based categories proposed by the list developers,30 the scores for Biological, Personality, Family, and Societal causes among medical staff were significantly higher than they were among patients and family (Table 1). Using Goulding’s classification based on the first examination of the latent or factorial structure,32 the scores for Personality/family/social stressors and External/environmental insults to the brain were significantly higher among medical staff than among patients or families, which is consistent with the modern biological conceptions of medical staff (Table 1).
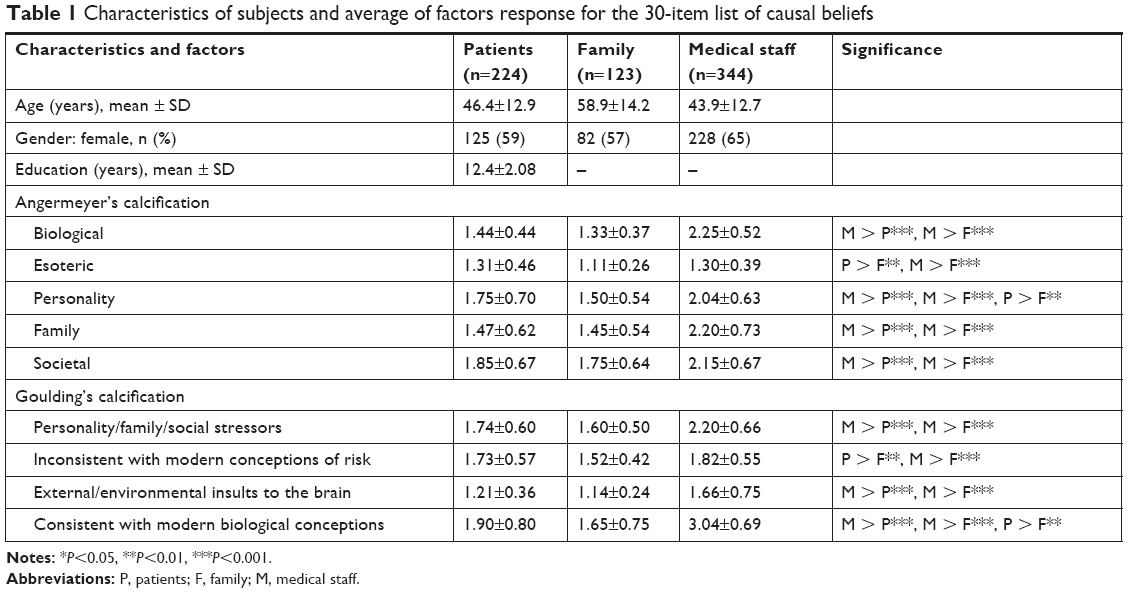 | Table 1 Characteristics of subjects and average of factors response for the 30-item list of causal beliefs |
The Kaiser–Meyer–Olkin (KMO) measure was 0.934, and Bartlett’s test of sphericity was significant (χ2=9,044, degrees of freedom [df] =435, P<0.001) in all subjects. Although the initial principal axis factoring method yielded nine factors with eigenvalues >1.0, explaining 52.5% of the cumulative variance, the point where the slope of the curve clearly leveled off was 4. Accordingly, we created the following four subscales: Psychosocial, Biological, Environmental, and Cultural connotations (Table 2). The KMO measure was 0.804, 0.699, and 0.928 and Bartlett’s test of sphericity was significant for patients (χ2=1,902, df =435, P<0.001), family (χ2=1,325, df =435, P<0.001), and medical staff (χ2=5,773, df =435, P<0.001), respectively. The structure varied among patients, family, and medical staff (Table 2).
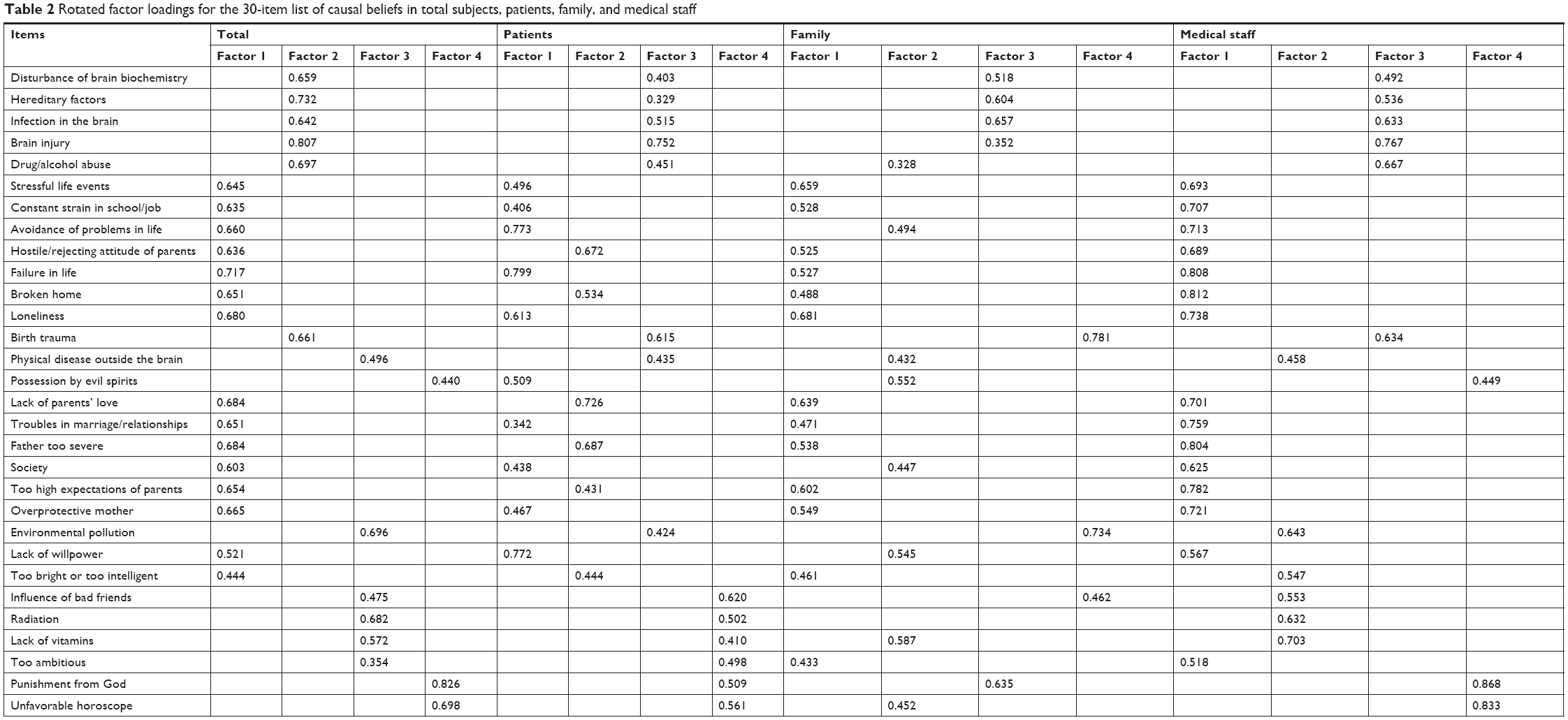 | Table 2 Rotated factor loadings for the 30-item list of causal beliefs in total subjects, patients, family, and medical staff |
Discussion
In our sample, the good internal consistency of the overall 30-item list of the possible causes of schizophrenia (a=0.925) indicated that this scale can be used as a reliable screening tool. The results of this exploratory factor analysis revealed four factors, which were used to create four subscales, termed Psychosocial (15 items), Biological (6 items), Environmental (6 items), and Cultural connotations (3 items). Because the structure varied among patients, family, and medical staff, the etiological beliefs about schizophrenia were different among them.
Using Angermeyer’s classification, Psychosocial, Biological, Societal, and Personality were the predominant causes perceived by medical staff. Using Goulding’s classification, modern biological conceptions were the most predominant cause considered by medical staff, while Personality/family/social stressors and Inconsistent with modern conceptions of risk were comparable in patients and family. This finding suggests that etiological beliefs about schizophrenia among patients and their families may be complex. It is necessary to keep in mind that beliefs regarding the psychosocial causes of schizophrenia, such as failure, avoidance of problems, stressful life events, constant strain in school/jobs, and difficulty in marriage/relationships, are as common as beliefs about inherited causes and chemical imbalances among patients and their families.
The scores for the subscales other than Esoteric or Inconsistent with modern conceptions of risk among medical staff were significantly higher than those among patients and their families. Medical staff may form various causal beliefs about schizophrenia from textbooks or from their experiences with many schizophrenic patients, while patients and their families tend to form their specific causal beliefs of schizophrenia through their own experiences. In this study, the scores were significantly higher on the Psychosocial and Biological subscales than on the other subscales among patients. This finding is in line with the results obtained in Western countries.19–21
Medical staff might think that biological treatment, including pharmacotherapy, is greatly beneficial in treating schizophrenia because their etiological beliefs regarding schizophrenia are most predominantly related to biological factors. However, patients and their families hope that psychotherapy focuses on Psychosocial and Familial/temperamental factors in addition to pharmacotherapy.
Mental health nurses as well as psychiatrists regarded antipsychotics as the most helpful for the treatment of schizophrenia in Australia.33 A recent British study showed that ordinary people also believed pharmacotherapy to be more effective than psychotherapy for the treatment of schizophrenia.34 Conversely, Asian people believe that superstitious and religious ideas are more important in relation to the causes and treatments of schizophrenia,35 although our study suggests that a religious or spiritual influence is unlikely for patients and their families. Nakane et al24 reported that Japanese, compared to Australians, were more likely to consider the causes of schizophrenia to be related to a nervous personality or weakness of character, which may well be treated with psychotherapy rather than pharmacotherapy with psychotropic medications. In addition, the general populations of Germany, the Slovak Republic, and Russia all prefer psychotherapy to psychotropic medication.20
In Aomori prefecture, there are shamans called itako or kamisama who make predictions, tell fortunes, and provide medical care through their spiritual or religious power. Out of 670 informants, 232 (34.6%) had experience consulting a shaman. Females had a high tendency to consult shamans, and they went to shamans to address personal illness and family illness. Only 20% of the informants experienced no change. The remaining informants felt healed.29 In the present study, the higher scores for Psychosocial and Familial/temperamental than for Biological might be attributed to this cultural background.
Limitations
This study is associated with several notable limitations. The first limitation is the recruitment strategy used. The assessment of the severity of schizophrenia was not evaluated. The severity of schizophrenia among our participants might be milder than that seen in the general population of people with schizophrenia. Thus, our sampling might not be representative of schizophrenia as a whole. The second limitation is that we did not recruit a community-dwelling population for factor analysis. Third, data on several potential confounding factors were not obtained because of strict ethical considerations and a reluctance to share medical information. This limitation is important because interpersonal relationships between family members and the severity of schizophrenia symptoms may have influenced the results of this study. Finally, this study is limited by its cross-sectional design; thus, we cannot determine the beliefs of the patients before initiating medication.
Conclusion
Most Japanese patients believe that there are multifactorial causes for schizophrenia. Overall, these findings are consistent with the evidence that mental health literacy in Japan has improved with increases in beliefs about both psychosocial and biogenetic causes of illness and decreases in causal beliefs relating to weakness of character.
Acknowledgment
This study was funded by a Grant-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Research JSPS, 15H04754 (Principal Investigator Norio Yasui-Furukori). The funders had no role in the study design, data collection and analysis, the decision to publish, or the preparation of the manuscript.
Disclosure
The authors declare that they have no direct conflicts of interest relevant to this study. Norio Yasui-Furukori has been a speaker for Sumitomo Dainippon Pharma, Mochida Pharmaceutical, Otsuka Pharmaceutical, and Merck Sharp & Dohme in Japan for other studies.
References
Meltzer HY, Stahl SM. The dopamine hypothesis of schizophrenia: a review. Schizophr Bull. 1976;2(1):19–76. | ||
Davis KL, Kahn RS, Ko G, Davidson M. Dopamine in schizophrenia: a review and reconceptualization. Am J Psychiatry. 1991;148:1474–1486. | ||
Howes OD, McCutcheon R, Owen MJ, Murray RM. The role of genes, stress, and dopamine in the development of schizophrenia. Biol Psychiatry. 2017;81(1):9–20. | ||
Cardno AG, Gottesman II. Twin studies of schizophrenia: from bow-and-arrow concordances to star wars Mx and functional genomics. Am J Med Genet. 2000;97(1):12–17. | ||
Cardno AG, Owen MJ. Genetic relationships between schizophrenia, bipolar disorder, and schizoaffective disorder. Schizophr Bull. 2014;40(3):504–515. | ||
Misiak B, Moustafa AA, Kiejna A, Frydecka D. Childhood traumatic events and types of auditory verbal hallucinations in first-episode schizophrenia patients. Compr Psychiatry. 2016;66:17–22. | ||
Dean K, Murray RM. Environmental risk factors for psychosis. Dialogues Clin Neurosci. 2005;7:69–80. | ||
Marangoni C, Hernandez M, Faedda GL. The role of environmental exposures as risk factors for bipolar disorder: a systematic review of longitudinal studies. J Affect Disord. 2016;193:165–174. | ||
Di Forti M, Marconi A, Carra E, et al. Proportion of patients in south London with first-episode psychosis attributable to use of high potency cannabis: a case–control study. Lancet Psychiatry. 2015;2(3):233–238. | ||
Varese F, Smeets F, Drukker M, et al. Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull. 2012;38(4):661–671. | ||
Cantor-Graae E, Selten JP. Schizophrenia and migration: a meta-analysis and review. Am J Psychiatry. 2005;162(1):12–24. | ||
McGrath J, Saari K, Hakko H, et al. Vitamin D supplementation during the first year of life and risk of schizophrenia: a Finnish birth cohort study. Schizophr Res. 2004;67(2–3):237–245. | ||
Day R, Nielsen JA, Korten A, et al. Stressful life events preceding the acute onset of schizophrenia: a cross-national study from the World Health Organization. Cult Med Psychiatry. 1987;11(2):123–205. | ||
Lataster T, Valmaggia L, Lardinois M, van Os J, Myin-Germeys I. Increased stress reactivity: a mechanism specifically associated with the positive symptoms of psychotic disorder. Psychol Med. 2013;43(07):1389–1400. | ||
Reininghaus U, Kempton MJ, Valmaggia L, et al. Stress sensitivity, aberrant salience, and threat anticipation in early psychosis: an experience sampling study. Schizophr Bull. 2016;42(3):712–722. | ||
Gureje O, Olley BO, Olusola EO, Kola L. Do beliefs about causation influence attitudes to mental illness? World Psychiatry. 2006;5:104–107. | ||
Kurihara T, Kato M, Reverger R, Tirta IG. Pathway to psychiatric care in Bali. Psychiatry Clin Neurosci. 2006;60(2):204–210. | ||
Adewuya AO, Ola BA, Mosaku SK, Fatoye FO, Eegunranti AB. Attitude towards antipsychotics among out-patients with schizophrenia in Nigeria. Acta Psychiatr Scand. 2006;113(3):207–211. | ||
Angermeyer MC, Matschinger H. Lay beliefs about mental disorders: a comparison between the western and the eastern parts of Germany. Soc Psychiatry Psychiatr Epidemiol. 1999;34(5):275–281. | ||
Angermeyer MC, Matschinger H. Causal beliefs and attitudes to people with schizophrenia. Trend analysis based on data from two population surveys in Germany. Br J Psychiatry. 2005;186:331–334. | ||
Swami V, Furnham A, Kannan K, Sinniah D. Beliefs about schizophrenia and its treatment in Kota Kinabalu, Malaysia. Int J Soc Psychiatry. 2008;54(2):164–179. | ||
Adewuya AO, Makanjuola RO. Lay beliefs regarding causes of mental illness in Nigeria: pattern and correlates. Soc Psychiatry Psychiatr Epidemiol. 2008;43(4):336–341. | ||
Swami V, Arteche A, Chamorro-Premuzic T, Maakip I, Stanistreet D, Furnham A. Lay perceptions of current and future health, the causes of illness, and the nature of recovery: explaining health and illness in Malaysia. Br J Health Psychol. 2009;14(3):519–540. | ||
Nakane Y, Jorm AF, Yoshioka K, Christensen H, Nakane H, Griffiths KM. Public beliefs about causes and risk factors for mental disorders: a comparison of Japan and Australia. BMC Psychiatry. 2005;5(1):33. | ||
Xia J, Merinder LB, Belgamwar MR. Psychoeducation for schizophrenia. Schizophr Bull. 2011;37(1):21–22. | ||
Link BG. Understanding labeling effects in the area of mental disorders: an assessment of the effects of expectations of rejection. Am Sociol Rev. 1987;52(1):96–112. | ||
Martin JK, Pescosolido BA, Tuch SA. Of fear and loathing: the role of ‘disturbing behavior’, labels, and causal attributions in shaping public attitudes toward people with mental illness. J Health Soc Behav. 2000;41(2):208–223. | ||
Phelan JC, Yang LH, Cruz-Rojas R. Effects of attributing serious mental illnesses to genetic causes on orientations to treatment. Psychiatr Serv. 2006;57(3):382–387. | ||
Fujii H, Yamamoto H, Ohzeki N, et al. Shamanism and mental health in Aomori. J Aomori Univ Health Welf. 2002;4:79–87. | ||
Angermeyer MC, Klusmann D, Walpuski O. The causes of functional psychoses as seen by patients and their relatives. II. The relatives’ point of view. Eur Arch Psychiatry Neurol Sci. 1988;238:55–61. | ||
Matschinger H, Angermeyer MC. Lay beliefs about the causes of mental disorders: a new methodological approach. Soc Psychiatry Psychiatr Epidemiol. 1996;31(6):309–315. | ||
Goulding SM, Broussard B, Demir B, Compton MT. An exploration of the factor structure and development of potentially useful subscales of etiological beliefs about schizophrenia in a general population sample. Soc Psychiatry Psychiatr Epidemiol. 2009;44(11):925–933. | ||
Caldwell TM, Jorm AF. Mental health nurses’ beliefs about interventions for schizophrenia and depression: a comparison with psychiatrists and the public. Aust N Z J Psychiatry. 2000;34(4):602–611. | ||
Furnham A. Psychiatric and psychotherapeutic literacy: attitudes to, and knowledge of, psychotherapy. Int J Soc Psychiatry. 2009;55(6):525–537. | ||
Furnham A, Wong L. A cross-cultural comparison of British and Chinese beliefs about the causes, behaviour manifestations and treatment of schizophrenia. Psychiatry Res. 2007;151(1–2):123–138. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.