")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Dietary Patterns and Hypertensive Disorders Among Pregnant Women Attending Antenatal and Delivery Care in Public Hospitals of Jimma Zone, Southwest Ethiopia
Authors Kidane R , Eshete T , Sintayehu T, Belachew T
Received 10 May 2022
Accepted for publication 18 July 2022
Published 30 July 2022 Volume 2022:15 Pages 1645—1656
DOI https://doi.org/10.2147/JMDH.S373749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rediet Kidane,1 Tewodros Eshete,2 Tsion Sintayehu,3 Tefera Belachew1
1Department of Human Nutrition and Dietetics, Institution of Public Health Sciences, Jimma University, Jimma, Ethiopia; 2Department of Public Health, Debre Markos University, Debre Markos, Ethiopia; 3Department of Public Health, Wachemo University, Hosanna, Ethiopia
Correspondence: Tewodros Eshete, Email [email protected]
Purpose: Hypertensive disorders of pregnancy are a major contributor to maternal morbidity and mortality. Dietary pattern is one of the modifiable determinants of hypertension. However, there is a research gap on dietary patterns and hypertensive disorders among pregnant women in Ethiopia. Therefore, this study aimed to identify dietary pattern of hypertensive disorders of pregnant women attending antenatal and delivery care.
Methods: Institution-based unmatched case control study was conducted among a total of 333 participants (111 cases and 222 controls). Data were collected using an interviewer administered questionnaire and analyzed using SPSS version 20. Principal component analysis was used to identify wealth tertile and cluster analysis was used to derive dietary pattern. Adjusted odds ratio with 95% confidence interval and variables with P-value < 0.05 were declared as statistically significant. Model of fitness was tested using Hosmer–Lemeshow goodness-of-fit test.
Results: On multivariable analysis, plant source food based dietary pattern [AOR=0.36 95% CI: 0.15– 0.82], balanced type of dietary pattern [AOR=0.24 95% CI: 0.11– 0.51] and folate intake [AOR=0.17 95% CI: 0.06– 0.48] were found to be significant protective factors from hypertensive disorders of pregnancy. Previous history of pregnancy induced hypertension [AOR=3.76 95% CI: 1.67– 8.37], twin pregnancy [AOR=3.69 95% CI: 1.52– 8.96], history of abortion [AOR=2.37 95% CI: 1.10– 5.12], presence of anemia at the first visit [AOR=7.12 95% CI:2.30– 21.98], gestational diabetes [AOR=3.12 95% CI: 1.002– 9.72] and highest wealth index [AOR=4.17 95% CI: 1.27– 13.66] were found to be significant risk factors for hypertensive disorders during pregnancy.
Conclusion: Balanced food based dietary pattern and plant-based food pattern had direct protective relationship with development of hypertension during pregnancy. This implies the need for promoting consumption of balanced diets and plant source foods high in fruit and vegetables. Mothers with twin pregnancies, anemia at first visit, previous history of pregnancy induced hypertension, and advanced age groups should be prioritized.
Keywords: dietary pattern, hypertensive disorders, Ethiopia, pregnant women
Introduction
Hypertensive disorders of pregnancy (HDP) refer to a continuum of conditions characterized by high blood pressure (systolic blood pressure greater than or equal to 140 mmHg and/or diastolic blood pressure greater than or equal to 90 mmHg in two measurements of at least 6 hours apart)1 and defined as chronic hypertension (of any cause diagnosed before 20 weeks of gestation), gestational hypertension, chronic hypertension with superimposed preeclampsia and preeclampsia – eclampsia syndrome.2
The global prevalence of hypertensive disorders during pregnancy ranges from 5.82 to 8.2%, being the second most common direct cause of maternal mortality worldwide.3 In Africa, HDP affects about one in ten pregnancies.4 In Ethiopia, hypertensive disorders of pregnancy complicate around 6% of pregnancies and are responsible for 19% of all maternal deaths.5,6
Consequences of hypertensive disorders of pregnancy include placental abruption, pulmonary edema, thrombocytopenia, hemolytic anemia, stroke, recurrent seizure, kidney damage, and liver injury.7 Perinatal death is also high in women with preeclampsia/eclampsia syndrome and shows a three- to five-fold increase.8 By the end of 2016, the perinatal mortality rate in Ethiopia was 33 per 1000 pregnancies.9 The study indicates a significant association of perinatal death with maternal death and eclampsia.10
Studies indicated that there is an association between dietary pattern and HDP.11–15 But to the best search of literature, there is an evidence gap in Ethiopia to see the association between dietary patterns and hypertensive disorders of pregnancy. Thus, the current study aimed to assess dietary determinants of hypertensive disorders of pregnancy in public health hospitals of Jimma zone, Southwest Ethiopia, to generate evidence that is most relevant to support health policies and strategies to prevent hypertensive disorders of pregnancy.
Methods
Study Setting and Subjects
Institution-based unmatched case-control study was conducted from April 15 to July 10, 2020, in Jimma zone public hospitals, Southwest Ethiopia. All pregnant women attending antenatal and delivery care in public hospitals in Jimma zone were the source population. In addition, selected pregnant women diagnosed to have hypertensive disorders, with inclusion criteria who are in gestational age of 20 weeks and above, were study population for cases, and selected pregnant women who are not hypertensive (normotensive), with inclusion criteria who are in gestational age of 20 and above, were in a control group. Mothers with a history of confirmed chronic hypertension or diagnosed before 20 weeks of gestation which is greater than or equal to 140/90 mmHg and without superimposed preeclampsia, and those who are critically ill and unable to communicate were excluded from the study.
Sample Size Determination
The sample size of the study was determined using Epi Info 7 STAT CALC for unmatched case-control study using the following assumptions: 95% CI, 80% power, percent of controls exposed (39.6%), percent of cases exposed (57.3) with a minimum detectable odds ratio of 2.05 from the study conducted in Tigray.16 By taking the ratio of case to control (m) 1:2, the maximum sample size of 101 cases and 202 controls is obtained. After adding a 10% contingency for non-response, the total sample size of the study was 333 (111 cases and 222 controls).
Sampling Techniques
From the total of eight public hospitals found in Jimma zone, four of them (Limugenet, Seka, Agaro, and Jimma university medical center) were randomly selected to get adequate cases and controls in the specified study period. The calculated sample size was proportionally allocated to the selected four hospitals based on the previous average quarterly report. A total of 189 pregnant women were diagnosed with hypertensive disorder monthly in selected hospitals. Hence, the calculated sample was proportionally allocated to the selected four hospitals based on the number of cases reported at each facility by taking 189 as the denominator. Based on this calculation, the allocated sample was 28, 21, 40, and 22 for Limugenet, Seka, JUMC and Agaro hospital, respectively. All cases that fulfill the eligibility criteria were consecutively included until the desired sample size was obtained. For every case included, two controls were identified and studied.
Data Collection Tool and Measurement
The interviewer-administered structured and pretested questionnaire was used to collect data. The questionnaire was initially prepared in English and translated to Amharic and Affan Oromo by experts after a thorough review of literature from different sources. The questionnaire was designed to capture the socio-demographic, family, nutritional, behavioral and life style variables, obstetrics and medical-related variables. In addition to the questionnaire, patient medical records were reviewed to abstract relevant variables related with laboratory, clinical and obstetrics data. Trained diploma midwives collected data after the case confirmation by physicians using the diagnosis criteria.
Anthropometric Measurement
Mid Upper Arm Circumference (MUAC) was measured at the nearest 0.1 cm at the midpoint between the tip of the acromion and the olecranon process on the back of the arm while the subject was holding the forearm in a horizontal position. The measurement was performed on the subject’s left arm hanging freely along the trunk using inextensible MUAC tape.
Dietary Data
A food frequency questionnaire (FFQ) composed of 45 previously developed items and used in studies conducted in the same study area was used to assess the dietary pattern of pregnant mothers for the last year.17 The 24-hour recall method was conducted on 20 pregnant women who came for antenatal and delivery services at Shenen Gibe hospital. The 24-hour recall method aimed to modify the food frequency questionnaire based on commonly consumed food items. Participants were asked to recall their usual frequency of intake over the past year.
Data Analysis Procedure
Data were coded and entered using Epi data version 3.1 and exported to SPSS version 20 for analysis. Both bivariate and multivariable analysis was done to see the association between dependent and independent variables. Variance inflation factor (VIF) was checked for possible multicollinearity between variables and model fitness was checked using Hosmer–Lemeshow goodness-of-fit test. Variables in the bivariate model with p-value <0.25 were selected as candidate variable for multivariable analysis. Finally, variables with P-value <0.05 were declared as significantly associated variables with the dependent variable. Principal component analysis (PCA) was used to identify wealth index and cluster analysis to derive dietary pattern. To verify whether it is possible to apply the PCA, the Kaiser–Meyer–Olkin (KMO) test, Bartlett’s test of sphericity, anti-image, communality and presence of a variable with complex structure was checked.
Dietary Pattern
Dietary pattern was derived using K means cluster analysis. After converting frequency of intake to week, base individual food items were grouped into 10 major groups and 4 optional food groups by using FANTA III (minimum dietary diversity for women). Individuals were grouped into three clusters based on the Euclidian distance of each frequency of consumption from the centroid of each cluster. The three patterns derived by K mean cluster analysis are animal source food based pattern (meat, poultry, dairy, eggs and organ meats), plant-based foods (Vitamin A rich vegetables and fruits, other fruit and vegetables, grains, dark green leafy vegetables and fruits) and balanced food pattern (both plant and animal source food).
Ethical Considerations
Ethical approval was obtained from Jimma University Ethical Review Board (IRB) with the letter reference number of IRB 00085/2020, and permission was obtained from administrative office of each hospital. Written informed consent was taken, and confidentiality of information was ensured for each study participant, and participation in this research was fully voluntary.
Results
Socio-Demographic Characteristics
A total of 104 cases and 208 controls participated in the study, with a response rate of 93.7%. The mean and standard deviation of age of the study participants was 29.08 ± 6.423 years. Majority of respondents were married and Muslim religion followers. Rural residents were higher among cases (43.3%) as compared to controls (23.6%). Similarly, the proportion of older age mothers was found to be higher among cases (38.5%) as compared to controls (9.1%). Regarding household wealth, 27 (25.96%) cases and 35 (16.83%) controls were in the highest wealth quintiles (Table 1).
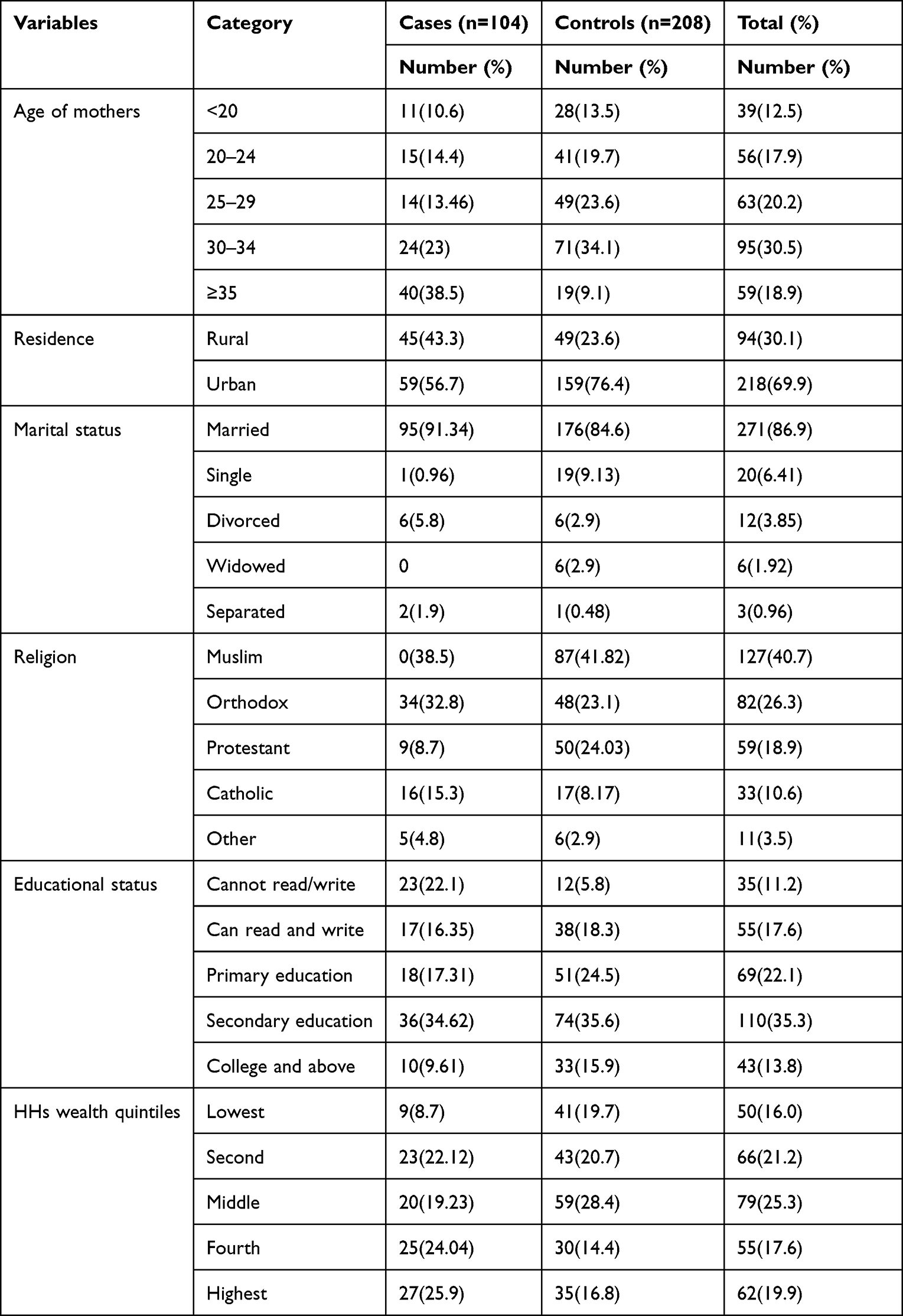 |
Table 1 Socio-Demographic Characteristics of Cases and Controls Attending Antenatal Follow Up or Delivery Care in Jimma Zone, Ethiopia, 2020 (N=312) |
Obstetrics and Gynecologic Characteristics of the Participants
The proportion of twin pregnancy was higher among cases (23.1) as compared to controls (9.6%). Accordingly, having previous history of pregnancy induced hypertension was also found to be higher among cases (26.9%) as compared to controls (18.3%). Of total participants, 26.9% of cases and 18.7% of controls reported a history of abortion. Besides, as compared to controls the proportion having anemia at the first visit was found to be higher among cases (3.8% vs 17.3%). Regarding iron folate intake, 80.7% of cases and 94.7% of controls reported that they take iron folate during pregnancy (Table 2).
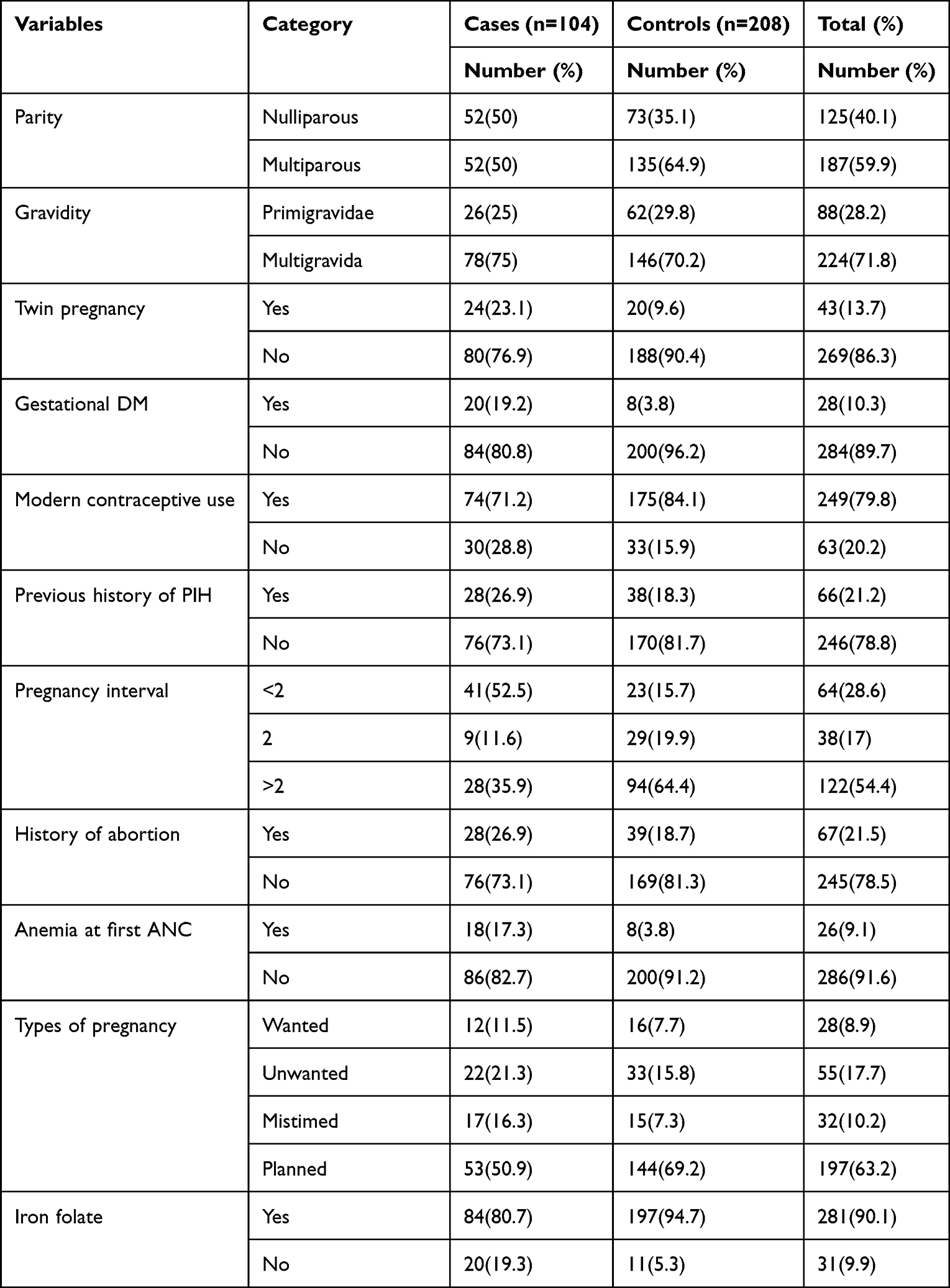 |
Table 2 Obstetrics and Gynecologic Characteristics of Cases and Controls Attending Antenatal Follow Up or Delivery Care in Jimma Zone, Ethiopia, 2020 (N=312) |
Behavioral, Lifestyle and Nutritional Characteristics of the Study Participants
Out of total respondents, 46 (80.7%) cases and 61 (63.5%) controls have reported that they drink alcohol in the past 12 months. Of total of 91 women who reported to have history of khat chewing in the past 12 months, 30 (100%) cases and 53 (86.8%) controls chew khat during recent pregnancy. Twenty (19.2%) cases and 79 (37.9%) controls reported that they had engaged in moderate physical exercise during their pregnancy; out of them, 56 (70.9%) controls and 12 (60%) cases are physically active. Based on self-report of the study participants, 86 (82.7%) cases and 167 (80.3%) controls reported that they drink coffee during pregnancy; out of them, 77 (89.55%) cases and 167 (100%) controls drink less than 4 cups of coffee per day (Table 3).
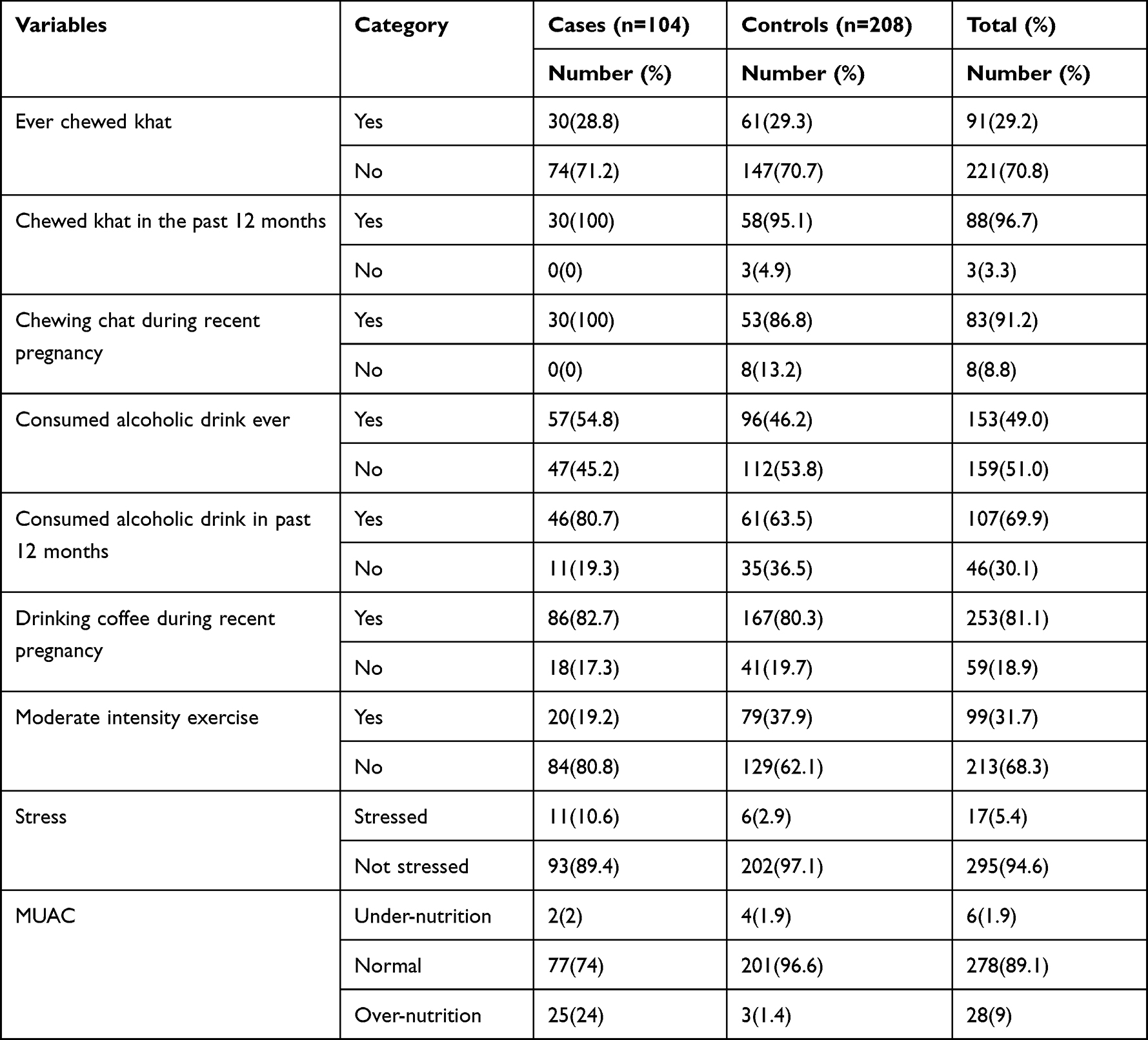 |
Table 3 Behavioral, Life Style and Nutritional Characteristics of Cases and Controls Attending Antenatal Follow Up or Delivery Care in Jimma Zone, Ethiopia, 2020 |
Dietary Pattern
The proportion of following balanced dietary pattern is found to be high among controls as compared to cases (46.1% and 34.6%, respectively). Similarly, as compared to cases (19.2%) following plant source food based dietary pattern was found to be high among controls (30.8%). In contrast, following animal source food based dietary pattern was found to be high among cases (46.2%) as compared to controls (23.1%) (Figure 1).
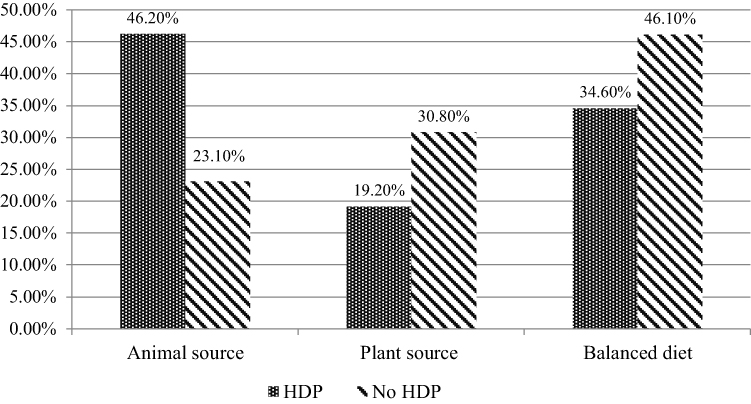 |
Figure 1 Dietary pattern of cases and controls attending antenatal follow up or delivery care in Jimma zone, Ethiopia, 2020. |
Determinants of Hypertension During Pregnancy
Bivariate logistic regression analysis was conducted to identify risk factors associated with hypertensive disorders of pregnancy. Accordingly, dietary pattern, previous history of pregnancy-induced hypertension, rural residence, multiple pregnancies, history of abortion, presence of anemia at first visit, folate intake, gestational diabetes mellitus, wealth index, presence of mental stress, parity and age were identified as risk factors. Variables which were found to be associated with the outcome variable in the bivariate analysis (P <0.25) were taken to multivariable analysis. On multivariable analysis after adjusting for confounders, dietary pattern, previous history of pregnancy-induced hypertension (AOR=3.76 95% CI 1.69–8.37), rural residence (AOR= 5.14 95% CI 2.45–10.79), twin pregnancy (AOR=3.69 95% CI 1.52–8.96), history of abortion (AOR=2.37 95% CI 1.1–5.12), presence of anemia at first visit (AOR= 7.12 95% CI 2.30–21.98), folate intake (AOR= 0.17 95 CI 0.06–0.48), advanced age (AOR=4.44 95% CI 1.52–12.97), gestational diabetes mellitus (AOR=3.12 95% CI 1.002–9.72) and wealth index were found to be significantly associated with hypertensive disorders during pregnancy.
Those pregnant women who follow dietary pattern characterized by balanced food consumption have 0.24 times lower odds of developing hypertension during pregnancy as compared to those who follow dietary pattern high in animal source foods (AOR=0.24 95% CI 0.11–0.51). The odds of developing hypertension during pregnancy were 0.36 times lower (AOR=0.36 95% CI 0.15–0.82) among pregnant women follow plant based dietary pattern as compared to those who follow animal source food based dietary pattern (Table 4).
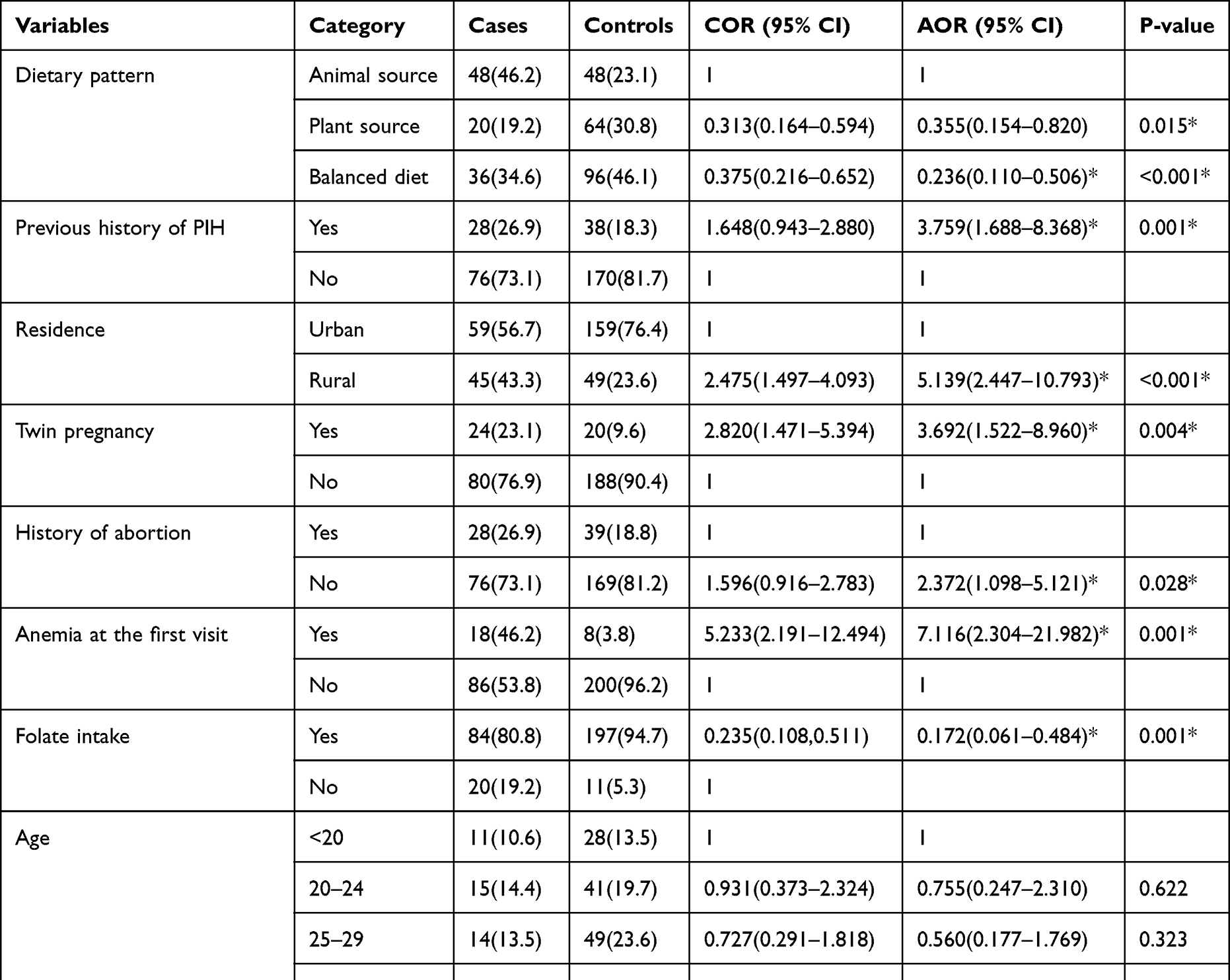 |
Table 4 Bivariate and Multivariable Analysis for the Predictors of Hypertensive Disorders of Pregnancy Among Pregnant Women Attending Antenatal Follow Up or Delivery Care in Jimma Zone, Southwest Ethiopia, 2020 |
Discussion
The findings of this study identify that dietary patterns, previous history of pregnancy-induced hypertension, place of residence, multiple pregnancies, history of abortion, presence of anemia at first visit, folate intake, advanced maternal age, gestational diabetes, and wealth index are predictor variables for hypertensive disorders of pregnancy.
Dietary pattern derived by K mean cluster analysis identifies three dietary patterns, namely: animal source food-based pattern (meat, poultry, dairy, eggs and organ meats); plant-based foods (Vitamin A-rich vegetables and fruits, other fruit and vegetables, grains, dark green leafy vegetables, and fruits); and balanced food pattern (fruit and vegetables, dairy, poultry, fish, meat, eggs, grains, and pulses).
As compared to those who are following an animal source food pattern, those who are followinging a healthy balanced diet are at 0.24 times lower odds of developing hypertension during pregnancy. This result is supported by studies conducted in Canada and Iran, which show lower odds of preeclampsia with increased intake of a healthy diet.12,15 This could be explained by the intake of a variety of foods that are a good source of all nutrients which are needed for a normal pregnancy. Additionally, a nutritious and well-balanced diet may enhance functionality and efficiency of maternal and fetal metabolism through substrate availability, reductive capacity, immunologic mechanisms, insulin sensitivity and the metabolic stress induced by disturbed placentation.
As compared to animal source food based patterns, those who are following plant-based food patterns have 0.36 times lower odds of developing hypertension during pregnancy. This might be due to the high intake of fruit and vegetable consumption as seen in plant-based food pattern. This result is supported by studies conducted in Australia, Norway, Denmark, Addis Ababa, Tigray and Bahirdar,10,11,13,14,16,18,19 which show the inverse association between high intake of fruit and vegetables and the occurrence of hypertension during pregnancy. This might be explained by a diet rich in vegetables and fruit that is rich in micronutrients such as antioxidants, vitamins, minerals and dietary fiber. A diet rich in fruit and vegetables decreased the risk of hyperhomocysteinemia, which is one of the risk factors for the occurrence of hypertension during pregnancy.
The odds of developing hypertension during pregnancy is 3.8 times higher among participants who have a previous history of pregnancy-induced hypertension (PIH) as compared to those who do not. This result is supported by studies conducted in Nigeria, Kombolcha, and Derashe.20–22 This might be due to the existence of non-modifiable risk factors and the severe consequences of preeclampsia.
The current study indicated that those who are rural residents have 5 times higher odds of developing hypertension during pregnancy as compared to urban residents. This result is supported by studies conducted in Nekemete and Tigray.16,23 This could be due to the fact that women from rural areas can start antenatal care follow-up later in pregnancy, which can be associated with a delay in healthcare-seeking behavior of rural women who are prone to economic, social, and cultural problems. Additionally, a range of variables, such as disparities in risk factor levels (such as obesity and tobacco use) and upstream socioeconomic determinants of health (eg, poverty rates, access to care, education and health literacy, food insecurity), may be behind the rural–urban disparity in pregnant hypertension. Particularly in rural areas, significantly reduced access to obstetric services may further amplify unfavorable maternal risk for hypertension.
In addition, odds of developing hypertension during pregnancy are 3.7 times higher among pregnant women with multiple gestations as compared to a singleton pregnancy. This result is supported by a study conducted in Nekemete and Tigray.16,23 This might be due to larger placental mass or relative placental ischemia in twin gestations compared with singletons. Moreover, relative placental hypoxia due to the increased size of the placenta is thought to play an important role for increased secretion of circulating anti-angiogenic particles, which could play a role in the increased risk of hypertensive disorders of pregnancy (HDP) in twin pregnancies.
The history of abortion was also found to be an independent predictor variable in other studies.23 This is also supported by the current study, which showed that the odds of developing hypertension during pregnancy was 2.4 times higher among pregnant women who had a history of abortion. This might be due to disruption of endothelium by vigorous curettage which may lead to abnormal placentation.
Those who have a history of anemia at first ANC visit have 7 times higher odds of developing hypertension during pregnancy as compared to those who do not. This result is consistent with the study conducted in Bahirdar.10 The susceptibility of pregnant women to anemia could be explained by the occurrence of micronutrient deficiency, which further may lead to the development of hypertension during pregnancy. This might lead to placental hypoperfusion which leads to the development of HDP.
In agreement with a previous study conducted in Bahirdar,10 the current study showed that those who are taking folate during pregnancy have a 0.17 times lower odds of developing hypertension during pregnancy. This might be due to folic acid ability to decrease plasma homocysteine concentrations, which is an amino acid released when the body digests dietary protein. It has been shown that its level increases during HDP, especially during preeclampsia. Excessive homocysteine in pregnancy might damage the vascular endothelium of the developing placenta by promoting oxidative stress, thereby increasing contractile response and the production of procoagulants and vasoconstrictors which lead to the development of preeclampsia.
As compared to lower age groups, those who are >35 years have 4.4 times higher odds of developing hypertension during pregnancy. This result is consistent with studies conducted in Ghana and Derashe,21,24 which show higher odds of hypertension among advanced age groups. This might be explained by women with advanced age group being more likely to develop blood vessel/cardiovascular problems due to the decrement of elasticity of blood vessels mainly related to aging and arterial stiffness.
Those who have gestational diabetes had 3 times higher odds of developing HDP as compared to other groups. This might be due to the reason that elevated glucose level in pregnancy may impair a cascade of vascular development that will predispose to the development of placental vascular compromise, which is one of the explanations for the pathophysiology of HDP.
As compared to lower wealth quintile, those who are at the highest wealth quintile had 4.2 times higher odds of developing HDP. This result is in contrast to the study conducted in India which indicated low socioeconomic status as a risk factor for preeclampsia.25 This difference may be due to differences in study setting and participants. The occurrence of HDP among the highest wealth quintile may be explained by an increment of sedentary behavior and intake of an unhealthy diet.
Unlike previous studies, nulliparity, coffee intake, alcohol intake, exercise, type of pregnancy and stress show no statistical significance with the dependent variable. This might be due to confounding variables, differences in lifestyle habits, study area, and sample size difference.
The above findings have implications for the need for inculcating key messages on nutrition behavior change communications at the ANC contact to emphasize the intake of a healthy balanced diet and plant source foods high in fruit and vegetables. These messages should focus especially on those who are in the advanced age of >35, have a history of anemia at first ANC visit, rural residents, did not take folate during pregnancy, history of previous PIH, gestational DM and history of abortion.
Conclusion and Recommendations
The findings of this study suggest that there are different risk factors and preventive factors for hypertensive disorders during pregnancy. Balanced food pattern and plant source food based food pattern were found to be preventive for the development of hypertension during pregnancy. Additionally, previous history of PIH, rural residence, twin pregnancy, history of abortion, presence of anemia at the first visit, folate intake, advanced age, wealth index and gestational DM were identified as significant predictors of HDP.
Risk factors identified in this study can be used as a screening mechanism for HDP. The following recommendations are forwarded based on the findings of this study, which provide an opportunity for prevention, early diagnosis and management of HDP.
For the general public: Pregnant women should follow healthy balanced dietary pattern and plant source food high in fruit and vegetables.
Healthcare providers: Health professionals should strengthen the counseling they provide to women about the risk factors associated with HDP and the benefits of a healthy and balanced diet, especially focusing on those who are in advanced age of >35, have history of anemia at first ANC visit, rural residents, did not take folate, previous history of PIH, gestational DM and history of abortion.
For government and non-governmental sectors: Multi-sectorial collaboration should be strengthened, especially with the agricultural sector to improve diet of pregnant women by increasing production of a variety of foods to increase access.
Researchers: Further study should be done on HDP in a well-controlled manner and using advanced methodology.
Strength and Limitations of the Study
Even though the major objective of this study is to see the association between diet and risk of developing hypertensive disorders of pregnancy, investigating the effect of multiple risk factors of hypertensive disorders of pregnancy simultaneously to avoid for rival explanations could be the strength of the study.
Cases and controls were recruited at the same facility to control for the context differences in the study participants. Due to the retrospective nature of the study design, the data may be subject to recall bias, especially for food frequency questionnaires. The study was done in a hospital setting which might not be generalized to the general population. Some of the variables may be under-reported since the assessment is self- eported, eg renal disease
Abbreviations
AOR, Adjusted odds ratio; CI, Confidence intervals; COR, Crude odds ratio; HDP, Hypertensive disorders of pregnancy; MNCH, Maternal, Newborn and Child Health.
Data Sharing Statement
The dataset for the current study is available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The ethical review board of Jimma University approved the study and adhered to the declaration of Helsinki. The participants gave written informed consent to be enrolled in the study after they received an adequate briefing on the purpose and procedure of the study. The anonymity of all participating women was ensured by not recording any names or other personal identifiers. Their right not to participate, not to answer any or all questions and to withdraw from the interview at any time they want was respected.
Acknowledgments
The authors would like to extend their gratitude to the study participants for their consensual participation. Likewise, the authors would like to thank data collectors and supervisors for their commitment throughout the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no funding from an external source.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. The American College of Obstetricians and Gynecologists. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122(5):1122–1131. doi:10.1097/01.AOG.0000437382.03963.88
2. Lowe SA, Bowyer L, Lust K, et al. SOMANZ guidelines for the management of hypertensive disorders of pregnancy 2014. Aust N Z J Obstet Gynaecol. 2015;55(5):e1–29. doi:10.1111/ajo.12399
3. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–33. doi:10.1016/S2214-109X(14)70227-X
4. Noubiap JJ, Bigna JJ, Nyaga UF, et al. The burden of hypertensive disorders of pregnancy in Africa: a systematic review and meta-analysis. J Clin Hypertens. 2019;21(4):479–488. doi:10.1111/jch.13514
5. Berhe AK, Kassa GM, Fekadu GA, Muche AA. Prevalence of hypertensive disorders of pregnancy in Ethiopia: a systemic review and meta-analysis. BMC Pregnancy Childbirth. 2018;18(1):34. doi:10.1186/s12884-018-1667-7
6. Berhan Y, Berhan A. Causes of maternal mortality in Ethiopia: a significant decline in abortion related death. Ethiop J Health Sci. 2014;24:15–28. doi:10.4314/ejhs.v24i0.3S
7. Ukah UV, De Silva DA, Payne B, et al. Prediction of adverse maternal outcomes from pre-eclampsia and other hypertensive disorders of pregnancy: a systematic review. Pregnancy Hypertens. 2018;11:115–123. doi:10.1016/j.preghy.2017.11.006
8. Abalos E, Cuesta C, Carroli G, et al. Pre‐eclampsia, eclampsia and adverse maternal and perinatal outcomes: a secondary analysis of the W orld H ealth O rganization Multicountry S urvey on M aternal and N ewborn H ealth. BJOG. 2014;121:14–24. doi:10.1111/1471-0528.12629
9. CSA. Ethiopian Demographic and health survey; 2016.
10. Endeshaw M, Ambaw F, Aragaw A, Ayalew A. Effect of maternal nutrition and dietary habits on preeclampsia: a case-control study. Int J Clin Med. 2014;5(21):1405. doi:10.4236/ijcm.2014.521179
11. Schoenaker DA, Soedamah-Muthu SS, Callaway LK, Mishra GD. Prepregnancy dietary patterns and risk of developing hypertensive disorders of pregnancy: results from the Australian longitudinal study on women’s health. Am J Clin Nutr. 2015;102(1):94–101. doi:10.3945/ajcn.114.102475
12. Jarman M, Mathe N, Ramazani F, et al. Dietary patterns prior to pregnancy and associations with pregnancy complications. Nutrients. 2018;10(7):914. doi:10.3390/nu10070914
13. Ikem E, Halldorsson TI, Birgisdottir BE, Rasmussen MA, Olsen SF, Maslova E. Dietary patterns and the risk of pregnancy-associated hypertension in the Danish National Birth Cohort: a prospective longitudinal study. BJOG. 2019;126(5):663–673. doi:10.1111/1471-0528.15593
14. Brantsæter AL, Haugen M, Samuelsen SO, et al. A dietary pattern characterized by high intake of vegetables, fruits, and vegetable oils is associated with reduced risk of preeclampsia in nulliparous pregnant Norwegian women. J Nutr. 2009;139(6):1162–1168. doi:10.3945/jn.109.104968
15. Abbasi R, Bakhshimoghaddam F, Alizadeh M. Major dietary patterns in relation to preeclampsia among Iranian pregnant women: a case–control study. J Matern-Fetal Neonatal Med. 2019;34:1–8.
16. Kahsay HB, Gashe FE, Ayele WM. Risk factors for hypertensive disorders of pregnancy among mothers in Tigray region, Ethiopia: matched case-control study. BMC Pregnancy Childbirth. 2018;18(1):482. doi:10.1186/s12884-018-2106-5
17. Belachew T, Lindstrom D, Hadley C, Gebremariam A, Kasahun W, Kolsteren P. Food insecurity and linear growth of adolescents in Jimma Zone, Southwest Ethiopia. Nutr J. 2013;12(1):55. doi:10.1186/1475-2891-12-55
18. Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 2002;13(1):3–9. doi:10.1097/00041433-200202000-00002
19. Grum T, Hintsa S, Hagos G. Dietary factors associated with preeclampsia or eclampsia among women in delivery care services in Addis Ababa, Ethiopia: a case control study. BMC Res Notes. 2018;11(1):683. doi:10.1186/s13104-018-3793-8
20. Guerrier G, Oluyide B, Keramarou M, Grais RF. Factors associated with severe preeclampsia and eclampsia in Jahun, Nigeria. Int J Womens Health. 2013;5:509. doi:10.2147/IJWH.S47056
21. Ayele G, Lemma S, Agedew E. Factors associated with hypertension during pregnancy in Derashie Woreda South Ethiopia, case control. Qual Prim Care. 2016;24(5):207–213.
22. Temesgen M. Factors associated with hypertensive disorder of pregnancy in Kombolcha. Clinics Mother Child Health. 2017;14:274. doi:10.4172/2090-7214.1000274
23. Hinkosa L, Tamene A, Gebeyehu N. Risk factors associated with hypertensive disorders in pregnancy in Nekemte referral hospital, from July 2015 to June 2017, Ethiopia: case-control study. BMC Pregnancy Childbirth. 2020;20(1):16. doi:10.1186/s12884-019-2693-9
24. Adu-Bonsaffoh K, Obed SA, Seffah JD. Maternal outcomes of hypertensive disorders in pregnancy at Korle Bu Teaching Hospital, Ghana. Int J Gynecol Obstet. 2014;127(3):238–242. doi:10.1016/j.ijgo.2014.06.010
25. Ramesh K, Gandhi S, Rao V. Socio-demographic and other risk factors of pre eclampsia at a tertiary care hospital, Karnataka: case control study. J Clin Diagnostic Res. 2014;8(9):JC01. doi:10.7860/JCDR/2014/10255.4802
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.