")
Back to Journals » Integrated Blood Pressure Control » Volume 14
Dietary and Behavioral Risk Factors of Ischemic Heart Disease Among Patients of Medical Outpatient Departments in Southern Ethiopia: Unmatched Case-Control Study
Authors Gebremedhin MH, Gebrekirstos LG
Received 11 June 2021
Accepted for publication 8 September 2021
Published 22 September 2021 Volume 2021:14 Pages 123—132
DOI https://doi.org/10.2147/IBPC.S322663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Turgay Celik
Meron Hadis Gebremedhin,1 Lielt Gebreselassie Gebrekirstos2
1School of medicine, College of health science and medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2Department of maternity and reproductive health, College of health science and medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Meron Hadis Gebremedhin Tel +251 9-1639-7836
Email [email protected]
Background: Worldwide mortality due to cardiovascular disease is the dominant cause of death, and ischemic heart disease is the leading one. Though risk factors for Ischemic heart diseases are modifiable and preventable, it is not well investigated in the local context. Thus, this study aimed to assess the dietary and behavioral risk factors for ischemic heart disease among patients in medical outpatient departments in Southern, Ethiopia.
Methods: A facility-based unmatched case-control study was conducted from November 16 to March 20, 2020, among patients with ischemic heart disease and those patients who visited the three hospitals of the Wolaita Zone. A convenient sampling method was used and the data were entered using Epi data version 3.1 and exported to SPSS version 21 for analysis, a p-value < 0.05, were considered statistically significant.
Results: A total of 557 study participants (140 cases and 417 controls) were included in a ratio of 1:3. The adjusted odds ratio for having no formal education (AOR = 3.18; 95% CI: 1.59, 6.34), previous history of hypertension (AOR= 2.84; 95% CI: 1.73, 4.66), physical inactivity (AOR= 2.23; 95% CI: 1.32, 3.76), inadequate intake of fruit and vegetable consumption (AOR= 2.43; 95% CI; 1.40, 4,22), palm oil use for food preparation (AOR= 2.12; 95% CI: 1.23, 3.63) and obesity (AOR= 5.68; 95% CI: 2.63, 12.23) increased the occurrence of the disease.
Conclusion: Although ischemic heart disease is preventable, using relatively simple and inexpensive lifestyle changes, it is projected to cause preventable loss of life. So, expanding health education and healthy life styles including exercise is recommended.
Keywords: behavioral, ischemic heart disease, case-control, logistic regression, Ethiopia
Background
Globally among the non-communicable diseases, cardiovascular-related death accounts more than 70% of mortality worldwide.1 Among this, ischemic heart disease is the most dominant one. It is caused by imbalance in supply and demand of oxygen to some parts of the myocardium leading to formation of atherosclerosis. Most people do not have symptoms at an early age.2 Depending on the severity of arterial narrowing and myocardial response angina pectoris (chest pain), sudden cardiac death, acute myocardial infarction, and chronic ischemic heart disease were detected.3,4
The magnitude of deaths from non-communicable diseases alone surpasses all other combined causes, where it is anticipated to increase from 38 million in 2012 to 52 million by 2030.5,6 A lot of patients of ischemic heart disease present with heart failure and cardiomegaly due to ischemic damage of the left ventricle.7–9
A study in China showed that around 17 million people died because of cardiovascular diseases in 2016, which occupied 31% of all deaths.10 NCDs including CVDs share various modifiable behavioral risk factors such as unhealthy diet, tobacco use, excess alcohol consumption and physical inactivity which lead to metabolic syndromes.11–13 In older people, IHD is already the leading cause of death and the second leading cause of death in men and women in the African region, respectively.14,15 This shift is more common in urban and high-income individuals with higher incomes and alternative lifestyles.16 In both gender, IHD ranked 8th among the leading causes of death in Africa following cerebrovascular diseases.
These continued to be a persistent major public health problem all over the world including our country Ethiopia where mortality due to NCD is over three-quarters.17–19 In Ethiopia, ischaemic heart disease is one of the top three prevalent CVDs. The reduction in the mortality rate due to CVDs is slower than for communicable diseases and other causes of mortality.20 Another study in Addis Ababa, Ethiopia showed IHD occupied a 7.4% of death.21 Also, a study in Jimma showed from admitted IHD patients 61.25% were diagnosed with chronic ischemic heart disease.9 In Ethiopia, unlike the majority of previous studies which assessed risk factors, it was hard to reach enough studies having a case-control association of risk factors to the disease. Empirical findings also indicated socio-demographic, nutritional, and behavioral factors with different study designs. Thus, this study aimed to identify the modifiable dietary and behavioral risk factors in the study area. These findings urge Ethiopia and the local community to consider IHD as a priority public health problem.
Materials and Methods
Study Setting and Study Period
The study was conducted from November 16, 2019, to March 20, 2020, in selected public and non-governmental hospitals in southern Ethiopia. There are seven hospitals in Wolaita zone from these three hospitals were selected purposively. These hospitals were Wolaita Sodo University referral hospital (governmental), Sodo Christian Hospital, and St. Mary Dubo Hospital (non-governmental hospitals), primarily serving the catchment. Wolaita Sodo University referral hospital is a referral hospital serving around 2 million people in the catchment area, including the neighboring Kambata Tambaro, Gamogofa and Dawuro zones.
Study Design
A hospital-based unmatched case-control study was employed.
Study Population
The study population for cases included all adult patients above 18 years of age admitted and on follow-up to the medical wards of Wolaita Sodo University referral hospital, St Mary Dubo Hospital and Sodo Christian Hospitals with a diagnosis of IHD. For selection of controls, a person’s prior history regarding cardiovascular disease was asked and it was assured that they had no history of hospital admission or taken treatment for CVDs.
Inclusion and Exclusion Criteria
Inclusion Criteria for Cases
- All adult patients who met the diagnosis of ischemic heart disease with electrocardiogram, cardiac biomarkers or echocardiography during the study period.
Inclusion Criteria for Controls
- Patients attending outpatient clinics for minor complaints from non-cardiac clinics (ophthalmology, ENT, dermatology, and family planning clinic).
Exclusion Criteria for Cases and Controls
Patients who were readmitted after being included in the study with stable IHD were excluded unless they develop ACS of new onset. Among controls, those patients with outcomes that could be related to the same exposure, such as lung cancer, chronic obstructive pulmonary disease, chronic kidney disease, and mentally unstable were excluded. Moreover, we also excluded patients with other metabolic diseases like diabetes mellitus and hypertension since risk factors for these diseases and the cases might be similar.
Measurement Variables
The dependent variable in the study was ischemic heart disease which was diagnosed using ECG, echocardiography and cardiac biomarkers.
- ECG finding with the presence of flat or down-sloping ST-segment depression of 1.0 mm or greater finding on ECG and T-wave inversion.
- Echocardiographic finding which includes dilation of left ventricle, acute severe mitral insufficiency and fall of stroke volume.
- The presence of cardiac biomarkers like elevated level of troponin (above 0.4 ng/mL) within a few hours of heart damage and remains elevated for up to two weeks.22,23
Sample Size and Sampling Technique
Sample Size
The sample size was calculated based on the double proportion formula for case-control study using Epi Info Stat Calc version 7.1, assuming a 95% confidence level, 80% power, and ratio of cases to controls of 1:3. Different dietary and behavioral risk factors of ischemic heart disease from different studies had been used to obtain the largest sample size and a study from South Africa was used with percent of hypercholesterolemia among controls of 7.6% with AOR=2.53, 95% CI (0.92,6.89).24 Finally, by adding a 10% non-response rate, the total sample size for the study was 557 (140 cases and 417 controls).
Sampling Procedure
Wolaita Zone has seven hospitals, among which three hospitals were purposively selected because of high patient flow, availability of ECG machine and Echocardiography and senior clinicians. All cases of IHD within the study period were included until the sample size was achieved. For each case, three hospital-based controls were selected from patients with minor complaints from non-cardiac outpatient clinics or inpatient wards (ophthalmology, ENT, dermatology, family planning clinic) with proportional allocation for each ward.
Data Collection Procedure and Quality Management
Data were collected using pretested interviewer-administered structured questionnaires, which were developed by reviewing different literature25–27 and from the WHO standard tools,28,29 which were related to behavioral and dietary risk factors of ischemic heart disease, and different anthropometric measurements. The questionnaire was translated into the local language (Amharic) and subsequently re-translated back to English by different language experts to check for internal consistency. BSc nurses were recruited from the staff for interview administered questionnaires and anthropometric measurements upon their previous experience and interest in collecting data. The data collectors were trained for one day on the objectives of the study, data collection tools, interviewees approach, interviewing techniques, maintaining confidentiality, privacy and respect of the respondents. To minimize measurement error anthropometric measurements were taken after prerequisites to avoid error that is, Weight was measured after we checked for the scale pointer at zero, and subjects wore light clothed and stood straight and unsupported at the center of a balance platform. Height was also measured after participants were requested to take out their shoes; stood erect being knees straight and position at the plane with feet together. The heels, buttocks and shoulder blades were made straight against the stadiometer’s vertical stand. Instrument calibration and random auditing were performed; measurements were taken twice, and finally, we approximated height to the nearest 0.1 cm and weight to the nearest 0.1kg. Anthropometric measurements (BMI) were translated according to the WHO Steps guidelines as shown below.28
- Underweight: <18.5 kg/m2
- Normal weight: 18.5–24.9 kg/m2
- Overweight 25.0–29.9 kg/m2
- Obesity: >30 kg/m2
The most important and common behavioral risk factors of ischemic heart disease were unhealthy diet, physical inactivity, tobacco use and harmful use of alcohol.10 Since Ethiopian drinks such as “Tella, Areki, Teji, and borde“ were the kind of alcoholic drinks in the study area. Excess alcohol consumption was defined as consumption of these local drinks and standard ones more than six months above WHO recommendation.
Physical activity was considered as at least 150–300 min of moderate-intensity aerobic activity or at least 75–150 min of vigorous-intensity aerobic physical activity or an equivalent combination of moderate and vigorous-intensity activity throughout the.30
To assess the current and previous status of smoking the following questions were asked.
- Do you have history of smoking, if yes duration, frequency and how much pack per one smoking session.
- Ever smoker was defined as, those patients who had ever tried smoking cigarettes in the past.
- Current smoker was defined as those who had smoked cigarettes on one or more days in including the data collection period.
Fruit and Vegetable Consumption
According to WHO recommendation of fruit and vegetables consumption, intake of fruit and, vegetables more than three times per week was considered as adequate while less than three times per week as inadequate. In this study, use of packed oil for food preparation was considered as use of packed oils in the jar “Chef, Hayat, Viking”.
Salt Intake Measurement
Intake of salt is defined according to WHO recommendation of salt consumption. As a result, optimal salt intake is defined as intake of salt below 5 gram per day which is comparable to one teaspoon full. High salt intake was a daily salt consumption of more than one teaspoonful or 5 gram per day.31 We told patients to report their salt intake in terms of gram or teaspoon according to their level of understanding and low was categorized as not taking any salt and very little amount.
Data Processing and Analysis
The data on each coded questionnaire were entered into Epi-data version 3.1 and double entry verification was made and exported to SPSS version 21 for analysis. The data were checked for assumptions and outliers. During analysis, descriptive statistics and bivariate analyses were performed to select variables for multivariate analysis. Significant variables with a p-value of ≤0.25, in bivariate analysis were retained for further consideration in multivariate logistic regression to control for confounders. Lastly, multivariate logistic regression was performed in order to control possible confounding effects of the selected variables. Odds ratios and 95% confidence intervals were computed and a p-value of less than 0.05 was used to determine the cut-off points for statistical significance and final model was checked by Hosmer-Lemeshow goodness of fit test and multi-colinearity and confounders interaction were checked.
Data Quality Control
We developed a questionnaire from WHO standard questionnaire and revising different literatures related to risk factors of cardiovascular disease and anthropometric measurements were interpreted according to international guidelines. Finally, it was translated to Amharic from English and back to English. The principal investigator supervised the data collection process, checked for completeness, clarity, consistency and completeness daily.
Results
Socio-Demographic Characteristics of Participants
A total of 557 study participants with (140 cases and 417 controls) were included, with a response rate of 100%. Nearly half of the cases (43.6%) and 42.7% controls were older than 55 years with interquartile range of 20. More than half of the cases, 73 (52.1%) and controls, 218 (52.3%) were male participants. The majority of the cases and controls, 110 (78.6%) and 332 (79.6%) were married. Nearly half of the cases 70 (50.4%) and 113 (27.1%) of controls had no formal education (p= 0.001). Of the study participants, 63.6% of cases had previous history of hypertension (p< 0.001) (Table 1).
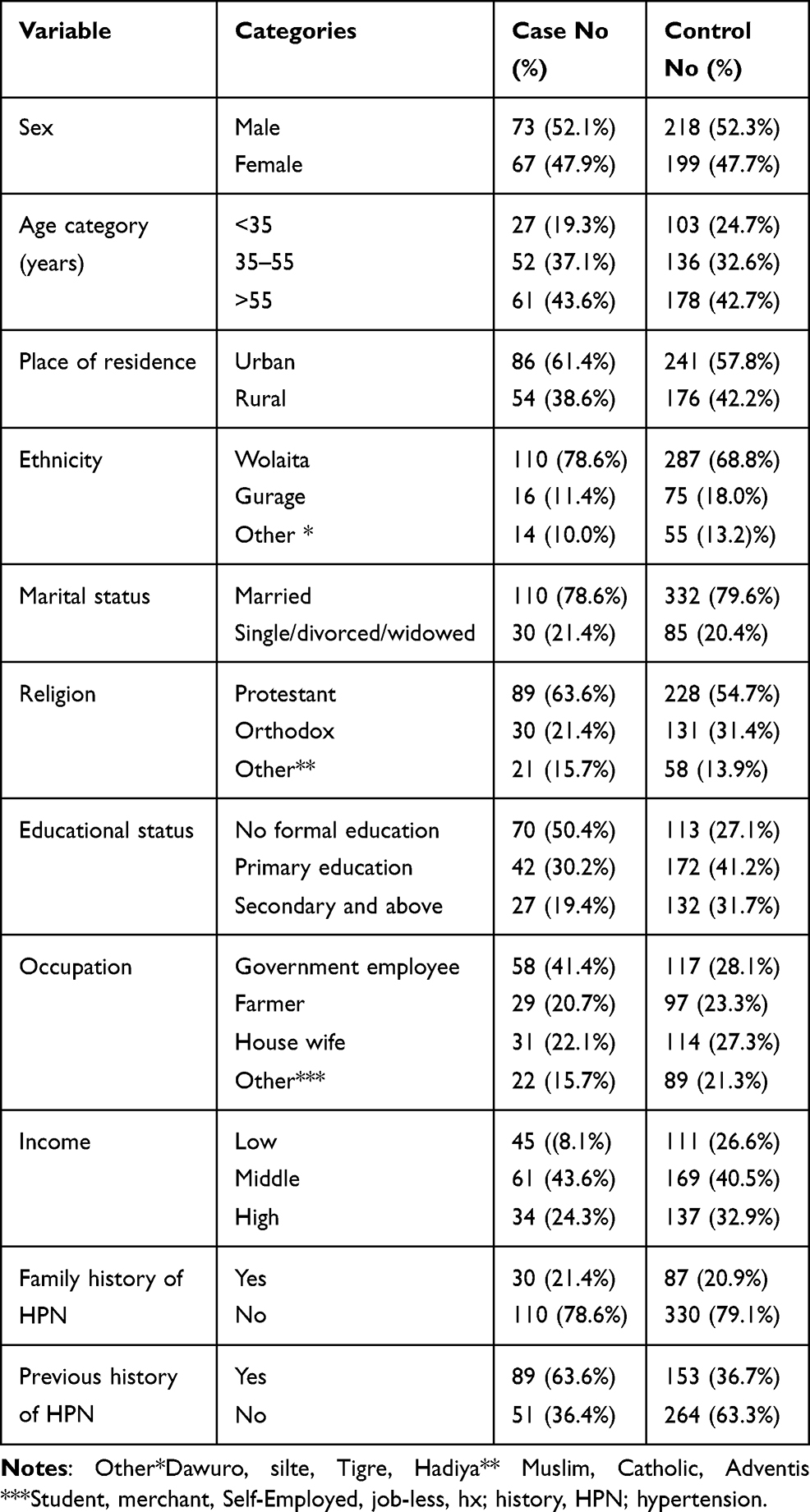 |
Table 1 Socio-Demographic Characteristics of Respondents, Southern Ethiopia, 2020 |
Behavioral, Nutritional and Anthropometric Risk Factors of Ischemic Heart Disease
More than half of the cases had history of alcohol intake (57.1%) of which 31.3% drink daily. And among the controls 31.2% had a history of alcohol intake; among them, 46.4% drank alcohol once a week. Concerning physical inactivity, three-fourth of cases were physically inactive as compared to controls (75.7% vs 53.0%). Regarding the history of khat chewing, 24 (17.1%) and 49 (11.8%) of controls chew khat.
More controls (39.8%) ate fruit and vegetable (more than three times per week) than cases (21.4%). The majority of cases (79.3%) and controls (56.1%) used palm oil for food preparation. Concerning salt usage, 57.1% of the cases and 25.4% of controls used high amount of salt in their diet. Almost half of the cases 64 (45.7%) vs 35 (8.4%) of controls were obese (Table 2).
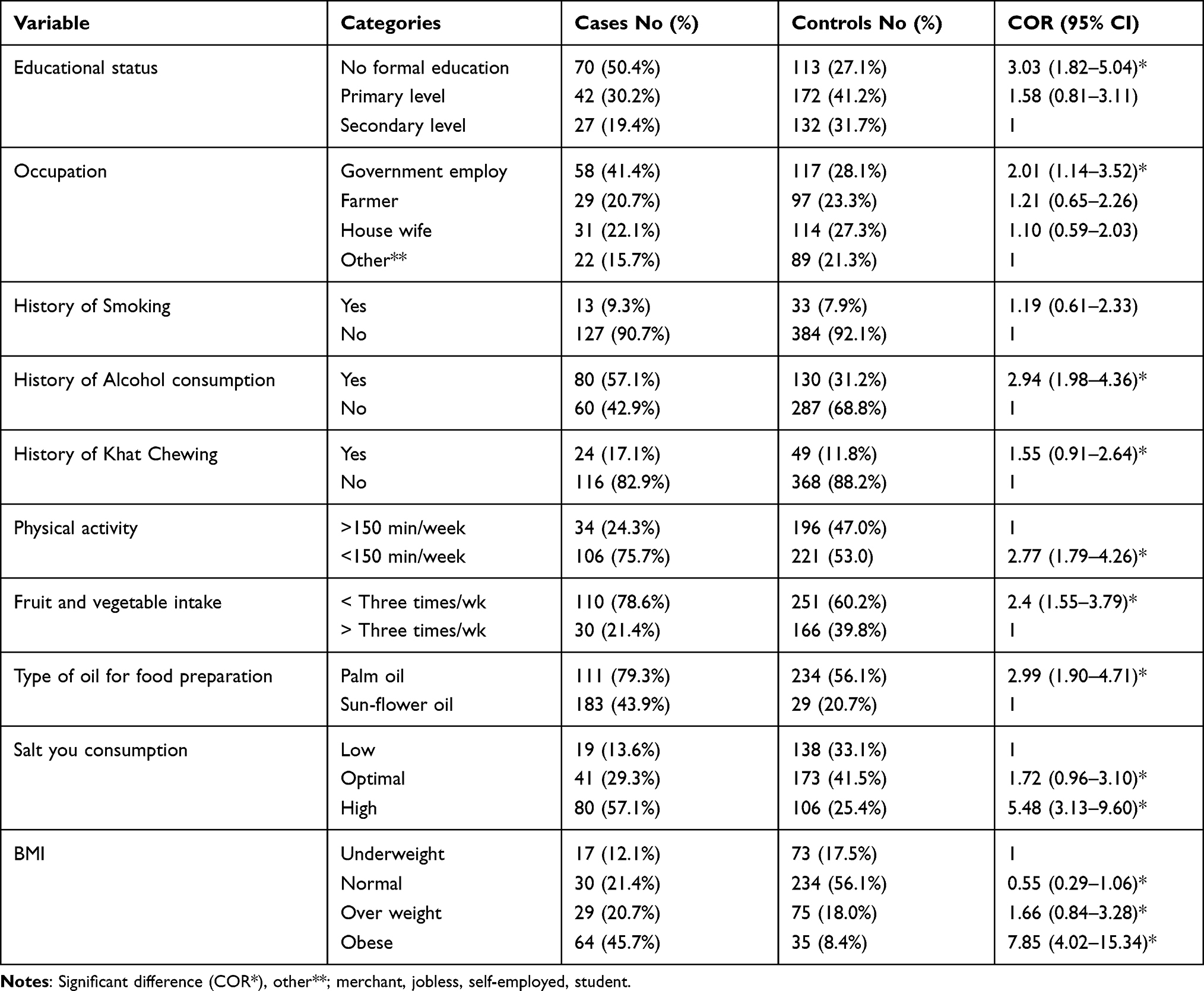 |
Table 2 Bivariate Logistic Regression and Behavioral, Dietary and Anthropometric Risk Factors of Ischemic Heart Disease in Selected Three Hospitals of Wolaita Zone, Ethiopia, 2020 |
Risk Factors of Ischemic Heart Disease
Bivariate logistic regression was performed between cases and controls to check the association between the dependent and independent variables. Variables that were found to be associated with the outcome variable in the bivariate analysis (p≤ 0.25) were included in the multivariate analysis. Accordingly, sex, occupation, educational status, history of alcohol consumption, frequency of alcohol consumption, khat chewing, less amount of fruit and vegetable intake, physical inactivity, and type of oil used for food preparation, amount of salt consumption and obesity were associated in bivariate logistic regression and entered into the multivariate logistic regression model. After adjusting for possible confounding factors, educational status, previous history of hypertension, physical inactivity, type of oil used for food preparation, less amounts of fruit and vegetable consumption per week and obesity were found to be independent predictors of ischemic heart disease. Those with no formal education increased the occurrence of ischemic heart disease by 3.18 times (AOR= 3.18, 95% CI=1.59–6.34) as compared to those who were secondary and above educational status. Those with a previous history of hypertension were 2.84 times more likely to develop as compared to those with no history of hypertension (AOR= 2.84, 95% CI= 1.73, 4.66). The odds of having ischemic heart disease due to lack of physical activity was 2.23 times higher than that of the control group (AOR = 2.23, 95% CI = 1.32–3.76). After adjusting for other variables, unhealthy diets were still more likely to be associated with IHD, such as using palm oil for cooking meals and using fewer amounts of fruit and vegetables in the usual diet. The use of fewer amounts of fruit and vegetables increased by 2.43 times with [AOR = 2.43, 95% CI; (1.40=4.22)] more likely to develop IHD and when compared with the control groups. In those cases who used palm oil for meal preparation increased the risk of developing the disease by two times as compared to [AOR =2.12, 95% CI; (1.23–3.63)] those who used sunflower oil. Those who were obese that is >30 or higher were 5.68 times at risk (AOR = 5.68, 95% CI; 2.63, 12.23) of developing the disease (Table 3). On the other hand, the effect of age, occupation, family history of hypertension, income, excess alcohol drinking, khat chewing and salt consumption disappeared in the multivariate analysis when adjusted for possible confounders.
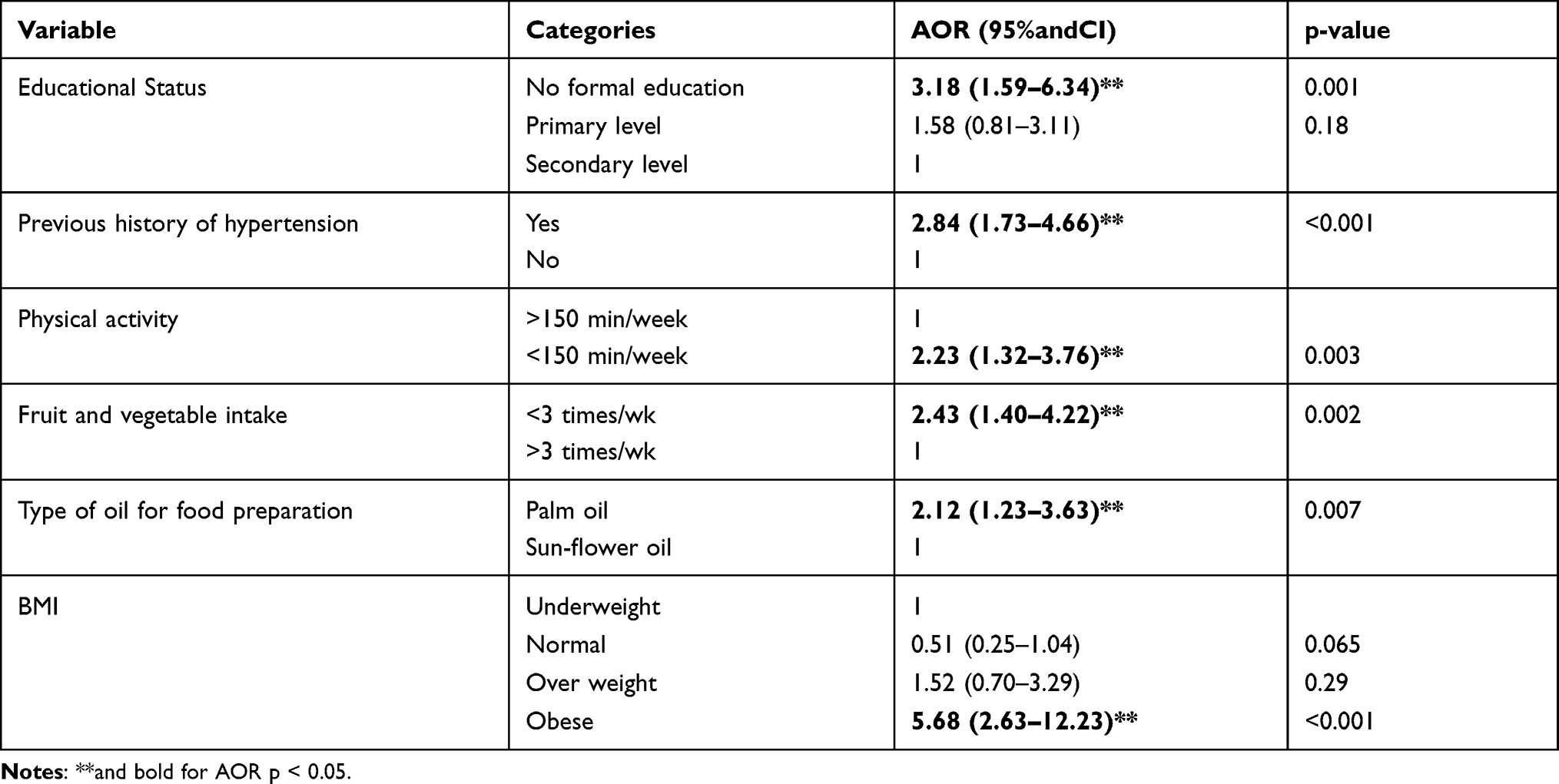 |
Table 3 Factors Associated with Ischemic Heart Disease in Southern Ethiopia, 2020 (N= 557) |
Discussion
Cardiovascular diseases, mainly ischemic heart disease, are the principal causes of global mortality.32 Most of the risk factors were modifiable and preventable, among which dietary and behavioral risk factors were dominant33 This study showed that having no formal education, having previous history of hypertension, physical inactivity, inadequate intake of fruit and vegetable, use of palm oil and being obese, were significant risk factors of ischemic heart disease in Southern, Ethiopia.
This study revealed that having previous history of hypertension was strongly associated with the occurrence of ischemic heart disease. Those with a previous history of hypertension were two times more likely to have ischemic heart disease than those with no history of hypertension (AOR= 2.84, 95% CI= 1.73, 4.66). A possible reason is that high blood pressure resulting from excess strain on coronary arteries serving the heart to slowly become narrowed from a buildup of fat, cholesterol and other substances. This build-up creates atherosclerosis, which later leads to accumulation of a blood clot or plaque and subsequently blood flow to the myocardium.34,35
Having no formal education increased the occurrence of ischemic heart disease by 3.18times (AOR = 3.18, 95% CI = 1.53, 6.34) than those who had primary and above educational status. This is supported by different reported studies in Australia, London, and Spain.16,36–39 The Number of years spent in school or in educational systems will have a lower risk of developing ischemic heart disease, which is also consistent with the current study and others.40–42 The association might be due to the level of knowledge of different life styles as not selecting what to eat or not understanding unhealthy behavior. In contrast to this study, educational status was not a direct risk factor for ischemic heart disease in a study conducted in Italy; rather, it is related to other chronic illnesses as a secondary complication due to lifestyle risk factor differences in the study population.43
Sedentary life is also the main behavioral risk factor for ischemic heart disease. The results of this study showed that patients who were not engaging in regular physical activity or involved in physical activity for less than three days per week were more likely to develop ischemic heart disease than those who engaged in regular physical activity for more than three days. The odds of having ischemic heart disease due to lack of physical activity were 2.23 times higher than the control groups (AOR = 2.23, 95% CI = 1.32–3.76). This result is comparable with a study in the USA, Saudi Arabia, and Germany.26–28 This might be because the benefits of regular exercise improve myocardial contraction, electrical stability, and an increase in stroke volume and maximal cardiac output. Regular exercise also reduces platelet aggregation and increases fibrinolytic activity.29
Diets high in fruits and vegetables are widely recommended. Fruits and vegetables are important for dietary guidance because of their concentrations of vitamins, minerals, especially electrolytes, dietary fiber and phyto-chemicals. It also improves hemostatic regulation, all of which contribute to the reduction of chronic diseases.44,45 A WHO report of 28 countries from low- and middle-income countries announced that only 18% of individuals consume 400 g/d of fruits and vegetables, which equates to ∼5servings/d.46 In this study, cases with less fruit and vegetable intake in their usual diet per week were 2.43 times at risk of developing ischemic heart disease (AOR = 2.43, 95% CI = 1.40–4.22) than those who eat fruit and vegetables at least three times per week. Another systematic review also showed a positive association with cardiovascular disease.47 In addition, a study in Japan and the UK suggested that consumption of fruits and vegetables alleviates a large percentage of the CVD burden.48,49 In contrast, a study in China showed that for men, no significant association was found, suggesting that a high consumption of fruits may reduce the risk of CHD in Chinese women.50
Due to globalization and import liberalization, different cooking oils are currently available. In this study, those who prepared food using palm oil were 2.12 times at risk to develop ischemic heart disease (AOR = 2.12, 95% CI = 1.23–3.63) than those who prepared food using sunflower oil. A study in Gonder, Ethiopia, disclosed that locally made oil has a higher degree of rancidity because of its higher iodine value compared to the imported oil.51 Another study done in Low- and Middle-Income Countries and in Costa Rica also support this.(52,53) But another systematic review could not establish strong evidence against palm oil consumption as a cardiovascular disease risk factor including IHD.54 This oil has more cholesterol compared to sunflower oil.
This study showed a significant relationship between the risk of ischemic heart disease and body mass index. Being obese was associated with the development of ischemic heart disease by 5.68 times (AOR= 5.68, 95% CI =2.63–12.23). Obesity is one of the main components in the development of metabolic syndrome where it is increased by five-fold in overweight people and by 20 times in obese people in comparison with people with normal body weight.55 In the other way, being obese is associated with a higher incidence of ischemic heart disease, despite their metabolic status.56 A study in Hungary and Brazil showed there is a strong association between obesity and cardiovascular disease.57,58 But another study in Colorado showed a low association between obesity and myocardial infarction rates.59
This study found a significant association between various modifiable risk factors which can be tackled easily. We recommend improving healthy diet with healthy life styles and promoting health education.
Limitations of the Study
As a result of the nature of case-control study, the temporal relationships of events between explanatory variables and IHD cannot be determined. Recall bias and social desirability bias are also potential limitations that might have affected the accuracy of information, especially related to behavioral factors and seasonal variation may affect dietary intake. Moreover, the findings of the current research cannot be generalized to the whole community, because of its institution-based nature.
Conclusion
This study found a significant association between behavioral and dietary factors and IHD in the local context, too. Improving sedentary lifestyles and increasing daily activity to tackle obesity and associated factors such as diet modulation with more fruits and vegetables and using vegetable oils for food preparation and creating health education programs is critical. Therefore, attention needs to be paid to changes in the modifications of risk factors and emphasis to reduce morbidity and mortality either by including to health extension programs or giving health education in different community forums.
Abbreviations
ACS, acute coronary syndrome; AOR; adjusted odds ratio; BMI, body mass index; BSc, Bachelor of Science; COR, crudes odds ratio; CVD, cardiovascular disorder; CI, confidence interval; ECG, electrocardiography; IHD, ischemic heart disease; NCD, non-communicable disease, SPSS, Statistical Package for the Social Sciences; WHO, World Health Organization.
Data Sharing Statement
Data will be available upon reasonable request.
Ethical Approval and Informed Consent
The study was approved by the ethical review committee of Wolaita Sodo University College of Health Science with ERC protocol number CHSM/ERC/92. All study participants were informed about the study, the right to refuse and confidentiality and verbal informed consent was obtained. The study was conducted in accordance with the Declaration of Helsinki. No personal details were recorded or produced on any documentation related to the study and privacy was assured. At the end of each interview and measurement procedure, awareness creation was given to study participants in control groups regarding the risk factors of IHD and the importance of regular checkup and aggravating factors for the cases.
Acknowledgments
We would like to thank Wolaita Sodo University and appreciate all participants who took part and assisted in this study.
Author Contributions
Both authors made significant contribution to the work reported, including conception, study design, execution, acquisition of data, analysis and interpretation of the study, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
Wolaita Sodo University paid per diem for data collectors and supervisors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global status report on noncommunicable diseases. World Heal Organ. 2010;53(9):1689–1699.
2. Yazdanyar A, Newman AB. NIH Public Access. Clin Geriatr Med. 2009;23(1):1–7.
3. Rezende PC, Ribas FF, Vicente C, Jr S, Hueb W. Clinical significance of chronic myocardial ischemia in coronary artery disease patients. J Thoracic Dis. 2019;11(3):1005–1015.
4. Cleveland Clinic. Coronary Artery Disease. Available from: https://my.clevelandclinic.org/health/diseases/16898-coronary-artery-disease. Accessed September 13, 2021.
5. World Health Organization. Global Status Report on Noncommunicable Diseases 2014. World Health Organization; 2014. Available from: http://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf?sequence=1. Accessed September 13, 2021.
6. World Bank Group. The Economic Costs of Noncommunicable Diseases in the Pacific Islands : A Rapid Stocktake of the Situation in Samoa, Tonga, and Vanuatu; 2012. Available from: https://openknowledge.worldbank.org/handle/10986/27219. Accessed September 13, 2021.
7. Adam ME, Garelnabi MEM, Sakin GAE, Omer MAA. Assessment of Ischemic Coronary Arteries Prevalence, Reversibility and Relative Dose Ratio% Using 99MtcSestamibi and 201Tl. Indian J Res. 2016;5(7):394–397.
8. Haque ATME, Yusoff FBM, Bin Ariffin MHS, Hamid M, Hashim S, Haque M. Lipid profile of the Coronary heart disease (CHD) patients admitted in a hospital in Malaysia. J Appl Pharm Sci. 2016;6(5):137–142. doi:10.7324/JAPS.2016.60521
9. Sciences M. Pattern and outcome of ischemic heart disease in patients admitted To Jimma University Specialized Hospital, Southwest Ethiopia. EthiopianJ Health sci. 2015;1–37.
10. Liu MB. Cardiovascular diseases. Chin Med J. 2014;127:6–7.
11. Siddiqi K. Non-communicable diseases. Public Health: an action guide to improving health; Oxford University Press. 2010.
12. Gbadamosi MA, Tlou B. Modifiable risk factors associated with non-communicable diseases among adult outpatients in Manzini, Swaziland: a cross-sectional study. BMC Public Health. 2020;20(1):1–12. doi:10.1186/s12889-020-08816-0
13. Budreviciute A, Damiati S, Sabir DK, et al. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Public Heal. 2020;8(November):1–11.
14. Mensah GA. Ischaemic heart disease in Africa. Heart. 2008;94(7):836–843. doi:10.1136/hrt.2007.136523
15. Article R. NIH Public Access. Bone. 2008;23(1):1–7.
16. Rosengren A, Smyth A, Rangarajan S, et al. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: the Prospective Urban Rural Epidemiologic (PURE) study. Lancet Glob Heal. 2019;7(6):e748–60. doi:10.1016/S2214-109X(19)30045-2
17. Misganaw A, Mariam DH, Ali A, Araya T. Epidemiology of major non-communicable diseases in Ethiopia: a systematic review search strategy. J Health. 2014;32(1):1–13.
18. Dombrovskiy V, Workneh A, Shiferaw F, Small R, Banatvala N. Prevention and control of noncommunicable diseases in Ethiopia: the case for investment, including considerations on the impact of khat. BMC. 2019;1:58.
19. Yosef T. Prevalence and associated factors of chronic non-communicable diseases among cross-country truck drivers. BMC Public Health. 2020;2:1–7.
20. Ali S, Misganaw A, Worku A, Destaw Z, Negash L, Bekele A. The burden of cardiovascular diseases in Ethiopia from 1990 to 2017: evidence from the Global Burden of Disease Study. Int Heal Study. 2020;2021;(September:318–326.
21. Senbeta Guteta Abdissa KO, Feleke Y, Goshu DY, Tafese DMBA. Spectrum of cardiovascular diseases among Ethiopian patients at tikur anbessa specialized university teaching hospital. Ethiop Med J. 2014;52(1):85.
22. Beresford P. Troponin fact sheet for Primary Care. NHS; North Bristol; NHS Trust: 1–4. Available from: https://www.nbt.nhs.uk/sites/default/files/Trop%20w%20%20header.pdf. Accessed September 13, 2021.
23. Venge P, Johnston N, Lindahl B, James S. Normal plasma levels of cardiac troponin i measured by the high-sensitivity cardiac troponin i access prototype assay and the impact on the diagnosis of myocardial ischemia. J Am Coll Cardiol. 2009;54(13):1165–1172. doi:10.1016/j.jacc.2009.05.051
24. Nethononda MR, Essop MR, Mbewu AD, Galpin JS. Coronary artery disease and risk factors in black South Africans - a comparative study. Ethn Dis. 2004;14(4):515–519.
25. Negesa LB, Magarey J, Rasmussen P, Hendriks JML. Patients’ knowledge on cardiovascular risk factors and associated lifestyle behaviour in Ethiopia in 2018: a cross-sectional study. PLoS One. 2020;15(6):1–15. doi:10.1371/journal.pone.0234198
26. Siegel KR, Bullard KM, Imperatore G, et al. Prevalence of major behavioral risk factors for Type 2 diabetes. Diabetes Care. 2018;41(5):1032–1039. doi:10.2337/dc17-1775
27. Chigom E. Non-Communicable Diseases. World Health; 2020.
28. The WHO WHO STEPwise approach to noncommunicable disease risk factor surveillance. Available from: www.who.int/ncds/steps.
29. WHO dietary guideline.pdf.
30. Centers of Disease Control. How much physical activity do adults need? | physical Activity | CDC [Internet]. Centers for Disease Control and Prevention; 2020. Available from: https://www.cdc.gov/physicalactivity/basics/adults/index.htm.
31. WHO. Salt reduction [Internet]; 2016. Available from: https://www.who.int/news-room/fact-sheets/detail/salt-reduction.
32. Brodmann M, Cahill TJ, Hil DP, et al. Global burden of cardiovascular diseases. BMC Public Health. 2020;76:25.
33. World Health Organization. Global Health Risks. World Health Organization; 2009.
34. Chen MA Atherosclerosis: medlinePlus Medical Encyclopedia [Internet]; 2018. Available from: https://medlineplus.gov/ency/article/000171.htm.
35. U.S.Department of Health and Human Services, National Heart Lung an BI, World Health Organization. Heart Attacks and Strokes Don’t be a victim. WHO Libr Cat Publ Data [Internet]; 2005;1–4. Available from: https://apps.who.int/iris/bitstream/handle/10665/43222/9241546727.pdf;jsessionid=F8816FF2956FA3773BDDA5129D37BC82?sequence=1%0Ahttp://www.nlm.nih.gov/medlineplus/ency/article/000195.htm.
36. Australian Institute of Health and Welfare. Stronger evidence, better decisions, improved health and welfare [Internet]; 2019. Available from: https://www.aihw.gov.au/getmedia/f69a0bd9-16f5-48c1-8922-2ef7e904bd14/aihw-cdk-12-fact-sheet.pdf.aspx.
37. Gill D, Efstathiadou A, Cawood K, Tzoulaki I, Dehghan A. Education protects against coronary heart disease and stroke independently of cognitive function: evidence from Mendelian randomization. Int J Epidemiol. 2019;48(5):1468–1477. doi:10.1093/ije/dyz200
38. Psaltopoulou T, Hatzis G, Papageorgiou N, Androulakis E, Briasoulis A, Tousoulis D. Socioeconomic status and risk factors for cardiovascular disease: impact of dietary mediators. Hell J Cardiol. 2017;58(1):32–42. doi:10.1016/j.hjc.2017.01.022
39. Dégano IR, Marrugat J, Grau M, et al. The association between education and cardiovascular disease incidence is mediated by hypertension, diabetes, and body mass index. Sci Rep. 2017;7(1):1–8. doi:10.1038/s41598-017-10775-3
40. Ave H, Ave H. NIH Public Access - education and coronary heart disease. BMJ. 2013;22(4):221–232.
41. Lee JWR, Paultre F, Mosca L. The association between educational level and risk of cardiovascular disease fatality among women with cardiovascular disease. Women’s Heal Issues. 2005;15(2):80–88. doi:10.1016/j.whi.2004.11.004
42. Tillmann T, Vaucher J, Okbay A, et al. Education and coronary heart disease: Mendelian randomisation study. BMJ. 2017;1:358.
43. Tedesco MA, Di SG, Caputo S, et al. Educational level and hypertension: how socioeconomic differences condition health care. J Human Hypertension. 2014;15:727.
44. Slavin JL, Lloyd B. Health benefits of fruits and vegetables 1. Am Soc Nutr. 2012;3:506–516.
45. Maclellan DL, Gottschall-pass KT. Fruit and vegetable consumption: benefits and barriers fruit and vegetable consumption: benefits and barriers MacLellan, Debbie L; Gottschall-Pass, Katherine; Larsen, Roberta. Canadian J Dietetic. 2004;2:786.
46. Siegel KR. Insufficient consumption of fruits and vegetables among individuals 15 years and older in 28 low- and middle-income countries: what can be done? J Nutr Comment. 2019;149:1105–1106. doi:10.1093/jn/nxz123
47. Aune D, Giovannucci E, Boffetta P, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality - a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. 2017;46(3):1029–1056. doi:10.1093/ije/dyw319
48. Mo X, Gai RT, Sawada K, et al. Coronary heart disease and stroke disease burden attributable to fruit and vegetable intake in Japan: projected DALYS to 2060. BMC Public Health. 2019;19(1):1–9. doi:10.1186/s12889-019-7047-z
49. Appleton KM, Krumplevska K, Smith E, Rooney C, McKinley MC, Woodside JV. Low fruit and vegetable consumption is associated with low knowledge of the details of the 5-a-day fruit and vegetable message in the UK: findings from two cross-sectional questionnaire studies. J Hum Nutr Diet. 2018;31(1):121–130. doi:10.1111/jhn.12487
50. Danxia YU. Fruit and vegetable intake and risk of coronary heart disease: results from prospective cohort studies of Chinese adults in Shanghai. Int Soc Differ. 2012;83(2):1–29.
51. Negash YA, Amare DE, Bitew BD, Dagne H. Assessment of quality of edible vegetable oils accessed in Gondar City, Northwest Ethiopia. BMC Res Notes. 2019;5:1–5.
52. Kabagambe EK, Baylin A, Ascherio A, Campos H. The type of oil used for cooking is associated with the risk of nonfatal acute myocardial infarction in Costa Rica. J Nutr. 2005;135(11):2674–2679. doi:10.1093/jn/135.11.2674
53. Susan P. NIH Public Access. Bone. 2005;23(1):1–7.
54. Ismail SR, Maarof SK, Ali SS, Ali A. Systematic review of palm oil consumption and the risk of cardiovascular disease. PLoS One. 2018;13:1–16.
55. Janssen I. Heart disease risk among metabolically healthy obese men and metabolically unhealthy lean men. Cmaj. 2005;172(10):1315–1316.
56. Le ARTIC, Hansen L, Netterstrøm MK, et al. Metabolically healthy obesity and ischemic heart disease: a 10-year follow-up of the inter99 study. J Clinical Endocrinol Metabo. 2017;102(June):1934.
57. Csige I, Ujvárosy D, Szabó Z, et al. Review article the impact of obesity on the cardiovascular system. J Diabetes Res. 2018;2:2018.
58. Cercato C, Fonseca FA. Cardiovascular risk and obesity. Diabetol Metab Syndr. 2019;11(1):1–15. doi:10.1186/s13098-019-0468-0
59. Akil L. Relationships between obesity and cardiovascular diseases in four southern states and Colorado. J Heal Care Poor Underserved. 2015;34(3):474–476.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.