")
Back to Journals » Infection and Drug Resistance » Volume 16
Diagnosis of Rare Bone Infection Caused by Nocardia by 16S rRNA Gene Sequencing
Authors Li S, Shi Y, Xiong Y, Liu Y
Received 5 October 2022
Accepted for publication 30 December 2022
Published 20 January 2023 Volume 2023:16 Pages 347—353
DOI https://doi.org/10.2147/IDR.S392342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Video abstract of "Rare bone infection caused by Nocardia" [ID 392342].
Views: 157
Shaozeng Li,1,* Yu Shi,1,* Yulin Xiong,1 Yali Liu2
1Department of Clinical Laboratory, the Fourth Medical Center of PLA General Hospital, Beijing, 100037, People’s Republic of China; 2Department of Clinical Laboratory, Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yali Liu, Email [email protected]
Abstract: Nocardia is an aerobic actinomycete that causes serious opportunistic infections in immunocompromised individuals. Gene sequencing is the gold standard for pathogenic bacteria diagnosis. This study uses 16S rRNA gene sequencing to diagnose three cases of bone infections caused by Nocardia, including one rare case (N. cyriacigeorgica), and the clinial features, etiological characteristics, treatment, and prognosis of the patients.
Keywords: Nocardia, 16S rRNA gene sequencing, bone infection, clinical features
Introduction
A Nocardia infection is an acute, sub-acute or chronic rare disease caused by gram-positive, modified positive-staining acid-fast bacteria that can occur in skin, lung, and disseminated (eg. brain and meninges) infections.1 Bone infections caused by Nocardia are relatively rare, and their clinical features are atypical, which should attract the attention of clinicians and docimasters. This study analyses the clinical manifestations and pathogenic characteristics of three patients with Nocardia bone infections who were admitted to the Fourth Medical Center of PLA General Hospital from September 2019 to November 2021.
Case Information
Case 1 was a 62-year-old female with a duration of 33 years who was admitted to our hospital for amputation to eliminate pain due to a crush injury on the right leg caused by a car accident, which had resulted in massive avulsion and infection of the soft tissue and protracted wound healing of the affected limb. After multiple transfers and surgeries, the bacterial cultures were all negative. A physical examination showed several sinus tracts of approximately 0.3 cm in diameter on the anterior and medial sides of the right thigh, a small amount of yellowish exudation, and local tenderness, as shown in Figure 1A. Laboratory tests showed the following: erythrocyte sedimentation rate: 2 mL/h; high-sensitivity C-reactive protein: 0.5 mg/L; blood routine white blood cells: 6.1×109/L; neutrophil: 62.6%; pro-B-type natriuretic peptide: 436.4 pg/mL; and urine routine white blood cells: 11.88/µL. The magnetic resonance imaging (MRI) results showed discontinuous signal intensity in the right femoral bone, local cortical thickening, a less uniform signal intensity in the medullary cavity, a dot-like slightly long T2 signal, and an abnormal shape and signal intensity in the right femur, which is consistent with the chronic osteomyelitis findings shown in Figure 1B.
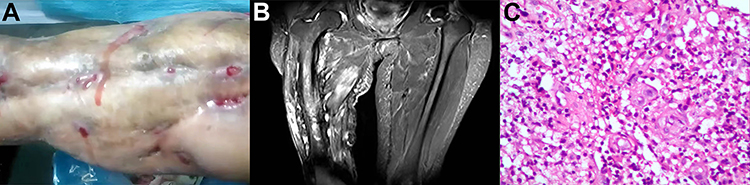 |
Figure 1 Three images of the affected area in case 1. (A), Features of osteomyelitis caused by Nocardia otitidiscaviarum; (B), Magnetic resonance imaging manifestation of chronic osteomyelitis; (C), Pathological examination of septic changes under a 10*20x microscope. |
On July 5th, 2019, vascular nerve exploration for the debridement of the right-thigh lesion was performed under general anaesthesia. Antibacterial bone cement was used to fill the bone defect site, with resection of the right-iliac mass and external fixation vacuum aspiration. During the operation, tissues and pus were removed and sent for pathological examination and microbial culture. The pathology results showed acute and chronic inflammatory cell infiltration in the fibroadipose tissue of the mass, with small vessel hyperplasia, which is consistent with suppurative inflammatory changes, as shown in Figure 1C. The submitted tissue was identified as N. otitidiscaviarum by 16S rRNA gene sequencing after 9 days’ microbial culture. The patient was discharged after their inflammatory parameters and symptoms had improved with a change in empirical medication gentamicin injection (480,000 units/day), moxifloxacin hydrochloride injection (0.4 g/day) and oral trimethoprim–sulfamethoxazole (0.96 g/day) for symptomatic treatment. Sequential oral trimethoprim–sulfamethoxazole (0.96 g/day) was administered orally, and the patient recovered 12 months later.
Case 2 was a 2-year-old male who presented with ulceration and exudation of the left index finger for more than 1 month caused by a knife cut. The physical examination showed that the wound of the index finger was approximately 1 cm long, with a small amount of bleeding and pain. Laboratory tests revealed the following: erythrocyte sedimentation rate: 15 mL/h; alkaline phosphatase: 275 U/L; high-sensitivity C-reactive protein: 0.7 mg/L; white blood cells 11.9×109/L; neutrophil: 36.7%; and platelets: 403×109/L. The MRI results showed soft tissue swelling around the left index finger with slightly long T1 and T2 signal shadows. Additionally, the middle phalanx lost its normal shape in T1WI, the normal signal intensity of the middle and distal bone marrow disappeared, and the middle phalanx of the left index finger was consistent with osteomyelitic changes. On Aug. 30th 2019, the patient underwent debridement of the lesion in the left index finger and Kirschner wire fixation with vacuum aspiration under general anaesthesia. Intraoperative secretions were removed and sent for pathology, which showed inflammatory cell infiltration in the second bone block, fibrous connective tissue, and immature bone tissue of the left index finger. The secretion was cultured in a Columbia blood plate for 9 days, and the colony was identified as N. cyriacigeorgica by 16S rRNA gene sequencing. The patient was given symptomatic treatment with ceftriaxone sodium (0.5 g/day) by injection and discharged 7 days later. On September 23, the erythrocyte sedimentation rate, C-reactive protein, and white blood cell count returned to normal. The patient was discharged and followed up for 12 months and recovered.
Case 3 was a 56-year-old female who underwent endoscope-assisted L2-5 interbody release and interbody fusion cage implantation using a lateral anterior lumbar approach under general anaesthesia on Sep. 8th 2020 due to scoliosis deformity and lumbar spinal stenosis. A posterior route percutaneous minimally invasive pedicle screw system internal fixation was performed. Three months after lumbar surgery, the incision ruptured intermittently during the preceding 1 month and showed significant granulation tissue proliferation, a small amount of yellowish exudation, no redness or swelling around the incision, and normal local skin temperature. Laboratory tests revealed the following: leukocytes: 7.6×109 /L; procalcitonin: 0.020 ng/mL; high-sensitivity C-reactive protein: 3.3 mg/L; erythrocyte sedimentation rate: 13 mL/h; and D-dimer: 223 ng/mL. The MRI results showed metal fixation shadows in the L2-5 vertebral body and corresponding intervertebral space, a heterogeneous T2WI signal of the intervertebral disc, and an uneven soft tissue signal in the lower back, suggestive of postoperative changes.
On Jan. 5th 2021, the patient underwent lumbar debridement, sinus tract resection, and closed lavage under general anaesthesia. Sinus secretions were cultured for 9 days and were identified as N. farcinica by 16S rRNA sequencing. The patient had a history of a sulphonamide allergy and was discharged with anti-infective treatment with the sensitive antibacterial drug linezolid (600 mg/day) + imipenem and cilastatin sodium (1000 mg/day) until the wound healed well and the inflammatory parameters were normal.
Pathogenesis-Related Tests
Identification
All three strains of Nocardia were sent to the microbiology laboratory for bacterial culture from the samples taken during surgery and were grown on blood culture dishes for 9 days before 16S rRNA gene sequencing. Each Nocardia strain was identified by 16S rRNA gene sequencing (1465 bp), primers were the bacterial 16S rRNA universal primer pairs, 27F and 1492R (5’AGAGTTTGATCATGGCTC3’, 5’TAGGGTTACCTTGTTACGACTT3’). NCBI GenBank BLAST analysis was used in this study.
(http://www.ncbi.nlm.nih.gov/blast, identification accuracy >99.5%), which detected N. otitidiscaviarum, as shown in Figure 2A. The colony growth was characterised by dryness, an asteroid appearance and a hard texture, as shown in Figure 2B. The colony growth of N. cyriacigeorgica, as shown in Figure 2C, was characterized by white limestone (in colours and shapes), as shown in Figure 2D. The colony growth of the case of N. farcinica, as shown in Figure 2E, was characterised by yellowish soft and central convex colonies, as shown in Figure 2F. The three strains tested positive for modified acid-fast staining (the staining solution was purchased from BASO DIAGNOSTICS INC. ZHUHAI. Address: No.286, Tongchang Road, Xiangzhou District, Zhuhai City 519,000, Guangdong Province, China).
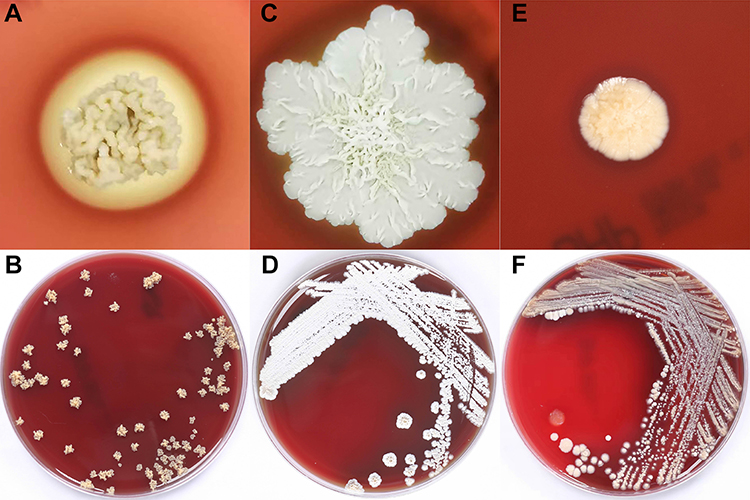 |
Figure 2 Colony morphology of three Nocardia species after 9 days of Columbia blood agar culture. (A and B), Nocardia otitidiscaviarum; (C and D), Nocardia cyriacigeorgica; (E and F), Nocardia farcinica. |
Results of Antimicrobial Susceptibility Testing
Eleven antimicrobial agents, including trimethoprim–sulfamethoxazole, linezolid, ciprofloxacin, imipenem, moxifloxacin, cefepime, amikacin, ceftriaxone, minocycline, tobramycin, and clarithromycin, were tested for antimicrobial susceptibility, using broth microdilution. The clinical breakpoints were interpreted with reference to the Clinical and Laboratory Standards Institute M24-2A standards for susceptibility. The antimicrobial susceptibility testing results are shown in Table 1.
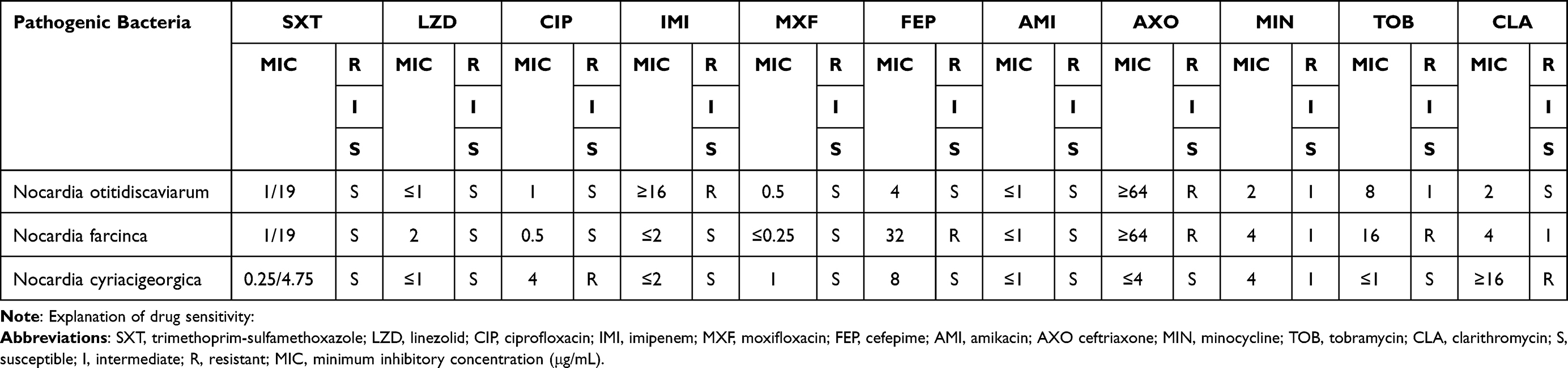 |
Table 1 Antimicrobial Susceptibility Testing Results of Nocardia in Three Patients with Bone Infection |
Discussion
In orthopaedic patients, wound infections are a common and difficult problem encountered in clinical practice. A wound infection can easily lead to difficult wound healing, which may cause problems, such as osteomyelitis, and in severe cases may result in disability or partial loss of function. The most common pathogenic bacteria in orthopaedic patients are Staphylococcus aureus, coagulase-negative Staphylococcus, Pseudomonas aeruginosa, and Escherichia coli.1 Nocardia infections are rare, atypical, and easily confused with tuberculosis, fungal or non-tuberculous mycobacterial infections, which can lead to misdiagnoses. This is a growing concern.2
Nocardia is an aerobic actinomycete that is commonly found in decaying plants, water, and soil. It causes severe opportunistic infections in immunocompromised individuals, such as patients with acquired immunodeficiency syndrome, chronic granulomas, transplants, and long-term high-dose hormone use.3 A Nocardia infection is not thought to be transmitted from person to person and manifests clinically as acute or chronic pyogenic granulomas, often with sinus tract formation, usually occurring in the lungs and skin. According to the three patients in this study who suffered from car accident injury, knife wound, and post-operative orthopaedic infection, respectively, trauma or an invasive operation is a suspected risk factor in the diagnosis of Nocardia in immunocompetent people and should not be ignored. The published literature reports approximately 500–1000 cases of Nocardia infections in the United States every year, most of which are in the lungs, with only 18.7% in the muscles and bones.4 French expert D. Lebeaux et al5 showed in their study that from a total of 793 strains of Nocardia in 2010 and 2015, joint fluid and bone tissue accounted for 20 cases (2.5%). Yashik Bansal et al6 revealed that pulmonary infections accounted for approximately 70% of Nocardia infections, and orthopaedic Nocardia infections accounted for 4% of patients in northern India. Hao Wang et al’s study7 analysed a total of 441 strains of Nocardia collected from 21 provinces, cities, and autonomous regions in China from 2009 to 2021, of which three strains were present in bone-associated infections, accounting for 0.68% of the study.
Nocardia grows slowly and generally requires approximately 1 week of culture to form more typical colonies, with some slow-growing colonies requiring at least 2 weeks of culture.8 In contrast, a negative report can be sent in 2–3 days for common bacteria. For rare Nocardia colonies, microbiological testing personnel need to have relatively extensive professional knowledge, and insufficient culture time may be one of the reasons for the missed detection of Nocardia. If there is a mixture of these slow-growing bacteria and common fast-growing bacteria when an infection occurs, the fast-growing bacteria will often completely mask the presence of Nocardia, thus causing misdiagnoses and missed detection. In clinical practice, pathogenic results are often negative in patients with chronic osteomyelitis. To increase the rate of positive culture detection, it is recommended to discontinue antimicrobial drugs for at least 1 to 2 weeks prior to sampling the infected bone tissue.9 When sampling at the site of an implant-associated chronic bone infection, specimens should be taken from at least five sites around the implant to ensure accurate sampling.
From clinical manifestations, the patient in Case 1 in this study, who had a disease duration of up to 33 years, had not been diagnosed after several transfers and surgeries. This patient had the longest duration of Nocardia infection osteomyelitis in the world to be reported in detail. This indicates that the clinical characteristics of patients with this bacterial infection are atypical, the anti-infective treatment is not effective, and the disease is persistent. Case 2 was the youngest patient with Nocardia osteomyelitis reported globally, indicating that Nocardia infections caused in children should not be ignored. Case 3 was postoperative incisional rupture, which suggests the possibility of surgical infection.
Laboratory examinations of patients with a Nocardia bone infection showed that the degree of increase in inflammatory parameters, such as white blood cells, C-reactive protein, procalcitonin, and the erythrocyte sedimentation rate, was not specific to other bacterial infections. Alkaline phosphatase was elevated in one patient with osteomyelitis, which may be associated with osteolytic changes. The pathological examination showed inflammatory cell infiltration and suppurative changes, and MRI has great advantages in indicating abdominal and soft tissue lesions and joint and tendon ligament injuries of the extremities. Moreover, the prognosis and recurrence of the patients could be monitored by follow-up examinations, such as computed tomography or MRI10 scanning.
Nocardia infections remain difficult to diagnose due to the slow growth of the bacteria, and there is no serological method for the clinical diagnosis of this type of infection. Traditional biochemical methods for identifying Nocardia are very time-consuming and can easily lead to a delay in diagnosis.11 Appropriate antimicrobial therapy during the early stage of the disease depends on the early diagnosis of a Nocardia infection and is essential in reducing the mortality rate. Gene sequencing is the gold standard for pathogenic diagnosis, and 16S rRNA has high sensitivity and specificity for the molecular diagnosis and strain identification of Nocardia.12 In this study, this method detected three cases of Nocardia causing a bone infection: N. otitidiscaviarum, N. cyriacigeorgica, and N. farcinica. In addition, antimicrobial susceptibility varies widely between species based on CLSI M24-A13 breakpoints.4 Masahiro Toyokawa et al14 showed that imipenem was 100% resistant to N. otitidiscaviarumand that linezolid had the highest sensitivity in in vitro susceptibility testing. According to the research data of scholars in the United States,15 Japan,16 and France,17 trimethoprim–sulfamethoxazole, linezolid, and amikacin have shown good antibacterial activity against Nocardia. The results of the present study suggest that the use of compound sulphonamide, linezolid, and imipenem also achieves good therapeutic effects.
In summary, it is rare for Nocardia to cause a bone infection. However, to address the poor specificity of clinical manifestations, gene sequencing as the gold standard for pathogenic diagnosis and strong communication between clinicians and laboratory personnel should be improved to facilitate accurate diagnosis and treatment.
Patient Consent and Ethics Statement
Patients have provided informed consent for the case details and images to be published.This study was approved by the Ethics Committee of the Fourth Medical Center of PLA General Hospital, Beijing, China (No. 2022KY130-KS001).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Veis DJ, Cassat JE. Infectious osteomyelitis: marrying bone biology and microbiology to shed new light on a persistent clinical challenge. J Bone Miner Res. 2021;36(4):636–643. doi:10.1002/jbmr.4279
2. Valdezate S, Garrido N, Carrasco G, et al. Epidemiology and susceptibility to antimicrobial agents of the main Nocardia species in Spain. J Antimicrob Chemother. 2017;72(3):754–761. doi:10.1093/jac/dkw489
3. Jiao M, Deng X, Yang H, et al. Case report: a severe and multi-site nocardia farcinica infection rapidly and precisely identified by metagenomic next-generation sequencing. Front Med. 2021;8:669552. doi:10.3389/fmed.2021.669552
4. Hamdi AM, Fida M, Deml SM, et al. Retrospective analysis of antimicrobial susceptibility profiles of nocardia species from a tertiary hospital and reference laboratory, 2011 to 2017. Antimicrob Agents Chemother. 2020;64(3):e01868–19. doi:10.1128/AAC.01868-19
5. Lebeaux D, Bergeron E, Berthet J, et al. Antibiotic susceptibility testing and species identification of Nocardia isolates: a retrospective analysis of data from a French expert laboratory, 2010–2015. Clin Microbiol Infect. 2019;25(4):489–495. doi:10.1016/j.cmi.2018.06.013
6. Bansal Y, Singla N, Butta H, et al. Nocardia infections: ten years experience from a tertiary health care center in North India (2007–2016). Infect Disord Drug Targets. 2021;21(3):445–451. doi:10.2174/1871526520666200516161940
7. Wang H, Zhu Y, Cui Q, et al. Epidemiology and antimicrobial resistance profiles of the nocardia species in China, 2009 to 2021. Microbiol Spectr. 2022;10(2):e0156021. doi:10.1128/spectrum.01560-21
8. Pan L, Wang XH, Meng FQ, et al. Membranous nephropathy complicated with disseminated nocardia farcinica infection: a case report and literature review. Infect Drug Resist. 2021;14:4157–4166. doi:10.2147/IDR.S331737
9. Vemu L, Sudhaharan S, Mamidi N, et al. Need for appropriate specimen for microbiology diagnosis of chronic osteomyelitis. J Lab Physicians. 2018;10(1):21–25. doi:10.4103/JLP.JLP_14_17
10. Weheba I, Abdelsayed A, Alrajhi AA, et al. Nocardiosis at an organ transplant center in Saudi Arabia: 15 years’ experience. J Glob Infect Dis. 2021;13(1):7–12. doi:10.4103/jgid.jgid_66_20
11. Ding J, MA B, Wei X, et al. Detection of Nocardia by 16S Ribosomal RNA Gene PCR and Metagenomic Next-Generation Sequencing (mNGS). Front Cell Infect Microbiol. 2021;11:768613. doi:10.3389/fcimb.2021.768613
12. Weng SS, Zhang HY, Ai JW, et al. Rapid detection of nocardia by next-generation sequencing. Front Cell Infect Microbiol. 2020;10:13. doi:10.3389/fcimb.2020.00013
13. Woods GL, Brown-Elliott BA, CONVILLE PS, et al. CLSI Standards: guidelines for Health Care Excellence [M]. In: Susceptibility Testing of Mycobacteria, Nocardiae, and Other Aerobic Actinomycetes. Wayne (PA): Clinical and Laboratory Standards Institute; 2011.
14. Toyokawa M, Ohana N, Ueda A, et al. Identification and antimicrobial susceptibility profiles of Nocardia species clinically isolated in Japan. Sci Rep. 2021;11(1):16742. doi:10.1038/s41598-021-95870-2
15. Bury DC, Rogers TS, Dickman MM. Osteomyelitis: diagnosis and Treatment. Am Fam Physician. 2021;104(4):395–402.
16. Tripathi S, Meena DS, Rohila AK, et al. Empyema necessitans with osteomyelitis of fifth rib due to Nocardia farcinica: a case report. BMC Infect Dis. 2021;21(1):745. doi:10.1186/s12879-021-06452-6
17. Young P, Riga A, Brunelli J. Nocardia nova infection of tibia tenodesis implant after anterior cruciate ligament reconstruction in an immunocompetent patient. J Am Acad Orthop Surg Glob Res Rev. 2020;4(3):
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.