")
Back to Journals » Clinical Epidemiology » Volume 12
Diagnosis of Open Tibial Fracture Showed High Positive Predictive Value in the Swedish National Patient Register
Authors Tampe U , Frank S, Weiss RJ, Jansson KÅ
Received 7 July 2020
Accepted for publication 31 August 2020
Published 14 October 2020 Volume 2020:12 Pages 1113—1119
DOI https://doi.org/10.2147/CLEP.S271173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Vera Ehrenstein
Ulrika Tampe, Sonny Frank, Rüdiger J Weiss, Karl-Åke Jansson
Department of Molecular Medicine and Surgery, Section of Orthopaedics and Sports Medicine, Karolinska Institutet at Karolinska University Hospital, Stockholm, Sweden
Correspondence: Ulrika Tampe
Karolinska University Hospital, Solna, Stockholm 171 76, Sweden
Tel +46768188611
Email [email protected]
Introduction: The Swedish National Patient Register was validated only for a few diagnoses in the field of trauma. In this study, we calculated the positive predictive values (PPV) of the diagnosis of open tibial fracture and corresponding E-codes (cause of injury).
Patients and Methods: Out of 2845 cases from a 10-year period (2007– 2016), a random sample of 300 cases was selected for review of medical records. The accuracy of the diagnosis and cause of injury was calculated and presented as PPV. We divided the study population into two subgroups (moderate and severe injury) that were analyzed separately. Severe injury was defined as when a patient had an amputation and/or reconstructive surgical procedures, indicated by corresponding ICD-codes.
Results: The PPV of the diagnosis of open tibial fracture was 87% (95% CI: 86– 88%) overall, 86% (95% CI: 79– 91%) for moderate injuries and 96% (95% CI: 91– 98%) for severe injuries. The PPV for E-codes was 74% (95% CI: 65– 81%). The majority of injuries were caused by falls (47%) or transport accidents (38%). Most of these injuries were caused by high-energy trauma (60%).
Conclusion: The PPV of the diagnosis of open tibial fracture in the Swedish National Patient Register is high (87%). The PPV of E-codes was lower (79%). The results imply that the register is well suited for healthcare evaluation and research purposes regarding trauma diagnoses. Most open tibial fractures are high-energy injuries.
Keywords: cause of injury, diagnosis, open tibial fracture, positive predictive value, register study
Background and Purpose
Open tibial fractures are serious injuries, associated with severe complications like osteomyelitis and amputations. The soft tissue over the tibial bone is sparse and approximately one in ten patients with these fractures requires reconstructive surgery, including multi-professional treatment by plastic reconstructive and orthopedic surgeons. Moreover, the population is heterogeneous and comprises young patients with major traumatic injuries as well as the elderly who are prone to simple falls.1
The Swedish National Patient Register (SNPR) covers 98% of all hospital admissions in Sweden. The coverage and content expanded, and since 1998, the ICD-10 diagnoses for somatic diseases, surgical codes and injuries were used and registered in all Swedish hospitals.2
There are previous validation studies for selected diagnoses.3 However, the number of such studies on traumatic injuries and external causes of injury is limited.4 No validation of the diagnosis of open tibial fracture has been previously presented. For every diagnosis of a traumatic injury, there is an associated external cause of injury (E-code). To our knowledge, there are no publications on the validity of E-codes in the SNPR.
The aim of this study was to validate the diagnosis of open tibial fracture and the associated E-codes, by calculating the positive predictive values (PPV). To elucidate possible differences, we performed a validation of the diagnosis on two subpopulations, ie, patients with or without major complications.
Patients and Methods
Patients
Data on demographics, diagnoses, E-codes and surgical procedure codes were collected from the SNPR. We extracted data on all patients with the diagnosis of open tibial fracture, including fractures of the proximal tibia, the shaft and the distal tibia (S82.11, S82.21 and S82.31). The study period was 2007–2016.
We identified 2845 patients, each given a unique code number. We characterized the injuries as moderate or severe. Severe injuries were defined as patients that sustained injuries associated with major complications, indicated as patients that had an amputation and/or reconstructive surgical procedures. These were identified in the Register as having an ICD-coded surgical procedure for reconstructive surgery (ZZS pedicled flap, ZZQ free flap and ZZA skin graft) and/or amputation (NGQ19 below-knee amputation, NGQ09 knee disarticulation and NFQ19 above-knee amputation). Open tibial fractures without such procedure codes were considered moderate injuries. This resulted in two groups: (A) moderate injuries (n=2515) and (B) severe injuries (n=330). From each group, a random sample of 150 cases was selected for review, using a computerized uniform randomization procedure (Figure 1). The size of the random samples was chosen with regard to a previous study of 3777 patients from the same register.1 From that study, we knew that out of 3777 cases during a 13-year period, 9% had a reconstructive procedure and 2% had an amputation. We estimated that 150 from each group would give a representative sample for both subgroups and from an ethical point of view, not too many reviews. The patients’ code numbers were converted to their unique Swedish personal identification numbers by the National Board of Health and Welfare. Thereafter, we collected files for these patients from 50 Swedish hospitals.
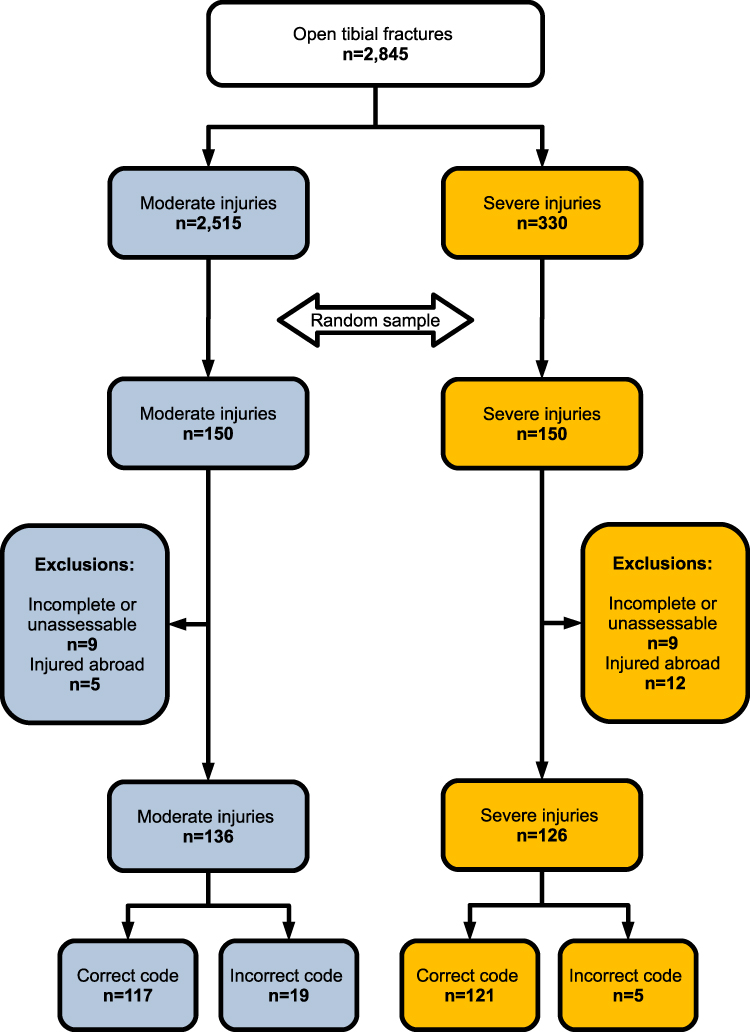 |
Figure 1 Flowchart. Original study population, division in subgroups, random samples for review of medical records and exclusions. Final remaining incorrect and correct diagnosis codes for calculation of PPV. |
Review of Patient Records and Analysis
All patient records were reviewed by a consultant orthopedic surgeon including notes of hospital admission, surgical reports, x-ray reports and discharge summaries. If any information indicated an open fracture, the diagnosis was assumed to be correct. Consequently, if there was no information on any open fracture in the available records or if the anatomical location was incorrect, the diagnosis was assumed to be false. Closed fractures and ankle fractures were considered incorrect. All causes of injury and the E-codes were reviewed correspondingly. E-codes consist of five positions. The fourth and fifth position define the location and the activity. The results for E-codes were grouped as correct, incorrect or unspecified. It is not uncommon that unspecific codes are used, even when specific and detailed information is available in the medical records. Therefore, unspecific codes were grouped separately. We calculated the PPV of E-codes based on the number of completely correct codes. Unspecific codes were considered correct when the necessary information was absent.
We characterized all injuries as being caused by high or low energy. Low energy was defined as falls from standing height, from stairs or lower height, sports injuries and low-energy vehicle accidents. High energy was defined as falls from height, crush injuries, gunshot injuries and high-energy road traffic accidents.
We grouped the causes of injury in three main groups: falls, transport accidents and others. These were further divided into detailed subgroups. The term unprotected road users refers to the subgroups of cyclists, motorcyclists and pedestrians.
The PPV (expressed as percentage) was calculated as the number of correct diagnoses divided by the sum of correct and incorrect diagnoses.
The presence of a classification system of open fracture in the medical records was noted. Classification is not a variable reported to the SNPR. Classification systems are used to characterize injuries. They provide guidance for doctors regarding, for example, treatment options and risk factors for complications. The only classification system used by Swedish orthopedic surgeons in this study was Gustilo Anderson et al.5
We analyzed the two subgroups separately. Regarding PPV and energy level, we calculated an estimate for the total study population based on the results from both subgroups. The reason for this calculation was to take into account that severe injuries, according to our definition, represented only 12% of the study population, whereas the majority were moderate injuries.
Exclusion Criteria
We excluded all patients who had their injury abroad, as we had no access to records from foreign hospitals (n=17). We also excluded patients that had incomplete files due to various reasons (n=21). This left us with 262 cases (87%) for the final analysis of PPV (Figure 1).
For E-codes, only records with correct primary diagnoses were examined (n=238, 79%).
Statistics
We used the free software R, available at www.r-project.org. Welsh-2 t-test was used for comparisons between subgroups for continuous variables (age).
Fisher’s exact test was used to calculate differences in percentages for the subgroups regarding PPVs, proportion of high-energy injuries and the use of Gustilo classification. Odds ratios (OR) and the associated 95% confidence intervals (CI) are presented.
Fisher’s exact test was also used to calculate differences in proportions regarding cause of injury in the subgroups.
Ethics
The study was approved by the Ethical Board in Stockholm (Dnr 2009/837-31/3, 2017/1652-32).
Results
Characteristics of the Study Population
The majority of patients in the study population of 2845 individuals were male (64%). The mean age was 47 years (range 0–99). According to our definition, the majority had a moderate injury (n=2515, 88%). There were 330 patients with severe injuries. Females were older than males in the subgroups as well as in the total study population. The proportion of high-energy injuries was higher among severe (78%) compared with moderate (58%) injuries (OR 0.4 (CI=0.2–0.7)) (Table 1).
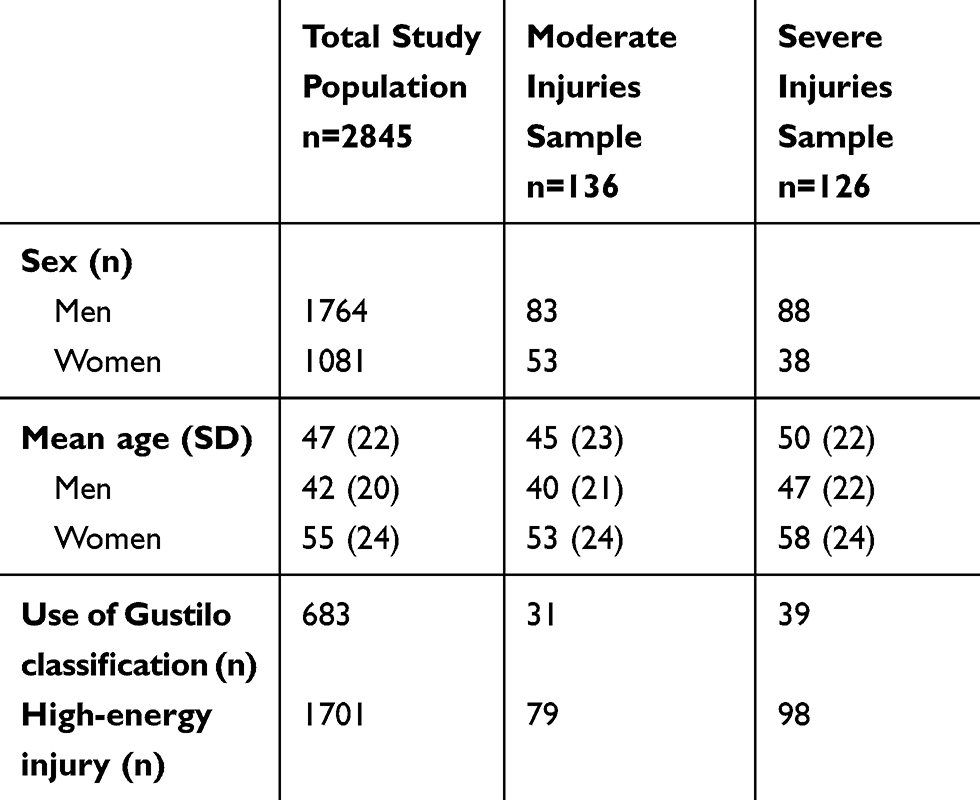 |
Table 1 Characteristics of the Total Study Population and Random Samples of Moderate and Severe Injuries. The Number of Gustilo Classifications and High-Energy Injuries in the Total Population is an Estimate |
Positive Predictive Value
Overall, the PPV was 87% (95% CI: 86–88%) for the diagnosis of open tibial fracture. In the subgroups, PPV differed. PPV was 86% (95% CI: 79–91%) for moderate injuries and 96% (95% CI: 91–98%) for severe injuries (OR 0.3 (CI=0.1–0.7)) (Table 2).
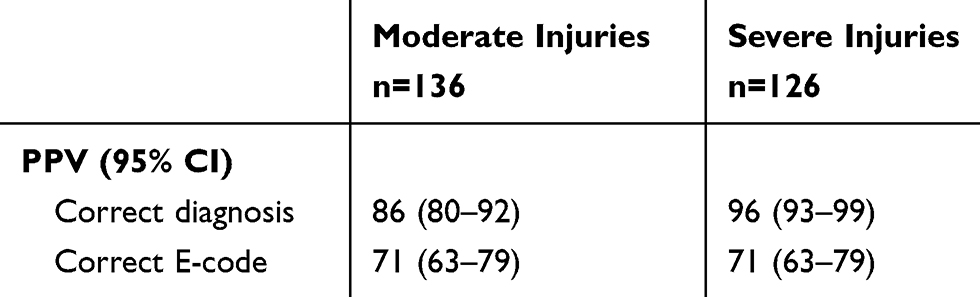 |
Table 2 PPV of Diagnosis and E-Codes, Comparison Between the Subgroups Moderate and Severe Injuries |
For 22 cases, the diagnosis was not accurate. Among those, 17 were closed tibial fractures and 5 were ankle fractures (Figure 1).
The PPV for E-codes was 71% (95% CI: 69–73%) for the total population, and also 71% (95% CI: 65–81%) for moderate as well as for severe injuries (Table 2).
Cause of Injury
In the group of patients with moderate injuries, a larger proportion of the fractures were caused by falls (n=52, 44%) compared with the group of patients with severe injuries (n=36, 30%, OR 1.9 (CI=1.1–3.3)) (Table 3). The majority were low-energy falls in both severe and moderate injury groups (n= 19, 53% and n=36, 69%, respectively). Transport accidents were more common in the group of severe injuries compared with moderate injuries (n=67, 55% vs n= 42, 36%, OR 0.5 (CI=0.3–0.8)). Among those, the largest subgroup (n= 32, 48%) was motorbike accidents (Table 2). Accidents with pedestrians were more common among severe (n=12, 18%) than moderate (n=5, 12%) injuries (Table 3).
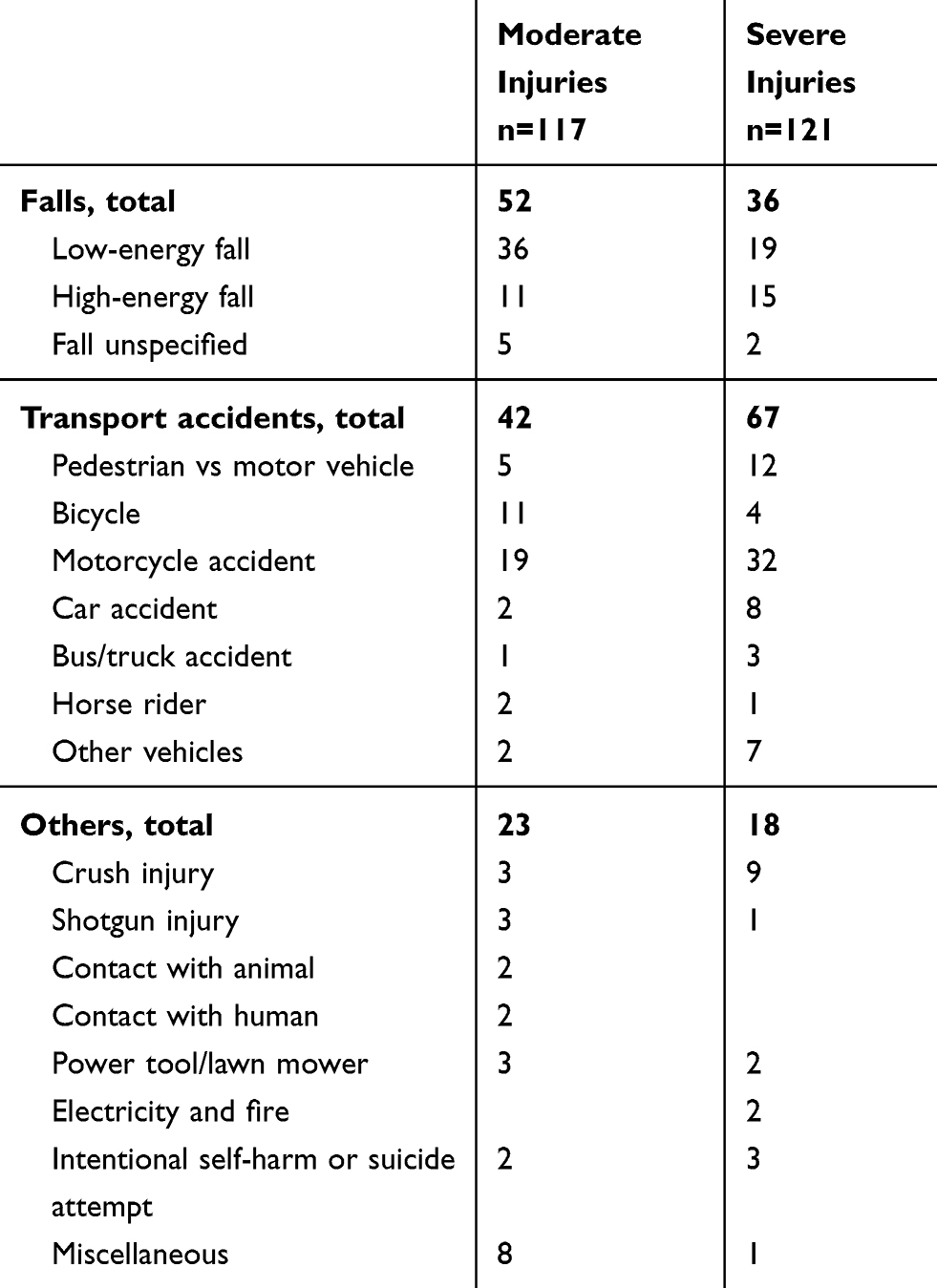 |
Table 3 Distribution of Causes of Injury Among Patients with Open Tibial Fractures. Comparison Between Moderate and Severe Injuries. Causes of Injury are Divided into Three Main Groups: Falls, Transport Accidents and Others |
Discussion
In this validation study of the Swedish National Patient Register, we found that the positive predictive value (PPV) of the diagnosis of open tibial fracture was high (87%). The validity of E-codes was lower (71%).
To validate diagnoses in patient registers, the preferred method is control of input data through a review of patient records. For this study, we reviewed medical records from 50 hospitals in Sweden. In a Finnish validation study performed in three trauma centers on the diagnosis of trochanteric fracture, the authors found an accurate diagnosis for 96% of the cases. The accuracy of E-code was also high (90%).6 In a recent validation study of the Danish registers, the authors evaluated hip fracture diagnoses for different subtypes and codes for surgical procedures. The PPV of the diagnosis trochanteric fracture was 92% and of subtrochanteric fracture 83%, ie, results that are comparable to our numbers.7
Through a detailed analysis of the cases in our study, we found that the most common misdiagnosis was a closed instead of an open fracture. This differentiation between open and closed fracture is on the 3-digit-level where 0 defines a closed fracture and 1 defines an open fracture according to ICD-10. Conversely, in this set-up, we did not examine the population of patients with closed tibial fractures to estimate the number of open fractures that were misclassified as closed.
Only 12% of tibial shaft fractures in Sweden are open.8 As a comparison, 21% were open fractures in a cohort from Edinburgh, and 60% in a recent study from several European trauma centers.9,10 These differences could be due to the fact that patient populations from trauma centers are likely to comprise a larger part of complicated cases. By analyzing moderate and severe injuries separately, we saw that the validity for the diagnosis was higher among severe injuries. This may be explained by the fact that severe open fractures are often obvious with large wounds and dislocations, in contrast to the low-grade injuries with wound size of one centimeter. Also, we saw a tendency towards higher use of classification systems among severely injured patients. We think that Swedish orthopedic surgeons may find classification more important for the cases where there is a higher risk for complications like amputation or lack of soft tissue that may need reconstructive surgery.
To our knowledge, this is the first published validation of E-codes for the SNPR. The PPV for E-codes was lower than for diagnosis (71%). E-codes were somewhat more difficult to assess as the available information in the records was not always complete. Nevertheless, we found that in several cases the information exists in the medical records but was not used for a correct coding. Instead, they were classified as unspecified. We did not perform a specific analysis on these cases, but in our opinion, unspecified codes were used too often and improvement should be possible. As we validated diagnoses and E-codes, we could also examine the causes of injury patterns among patients with open tibial fracture as well as the basic characteristics of the study population. As in other large study populations, the majority of patients sustaining open tibial fractures in Sweden were men (64%), at an average age of 47 years.9,10 In a population from Edinburgh of 1502 patients with open or closed tibial shaft fractures during 1990–1999, men represented 75% at an age of 32 years.11 The higher proportion of men at a younger age in that study may indicate differences in study populations but also that a larger part of trauma patients in recent years are elderly women.
We characterized the two subgroups (moderate and severe injuries) to map the subgroup at risk for complications. Patients with severe injuries were older, to a greater extent male, and more often affected by high-energy accidents. When looking in detail at causes of accidents, we noted that unprotected road-users like motorcyclists, cyclists and pedestrians were most at risk to sustain injuries in transport accidents. This finding is in line with a study from France where the fatality rates for motorized two-wheelers were increased compared with car occupants.12 In a study from European trauma centers, the leading causes of accidents for open fractures were motor vehicle and motorcycle accidents.10 By contrast, moderate injuries were more often due to falls. According to Winkler et al, the number of road traffic accidents (RTAs) as a cause of accident has decreased during 1988–2010.13 In our study from more recent years, the number of falls was higher than RTAs among patients with moderate injuries, who represent 88% of the study population. This is consistent with the trend of improved road safety, and at the same time increasing group of the elderly.
We found that most cases in our study were high-energy injuries. The proportion of high-energy injuries was higher in the subgroup of severe injuries, as expected. Nevertheless, in the subgroup of severe fractures, defined as patients that had an amputation or reconstructive surgery, 22% of the injuries were caused by low-energy trauma. Patient factors like age and co-morbidities as well as extensive contamination of the wound are known as major risk factors for complications.1,14 We conclude that regardless of initial appearance or mechanism of injury, all open fractures should be thoroughly assessed from admission and treated according to recent guidelines.15
The strength of this study is that we analyzed a random sample from a nationwide register where data were verified directly from medical records and surgical reports. The drop out rate was low (13%), which implies that this study provides a reliable calculation of the PPV of the diagnosis of open tibial fracture as well as description of the population of Swedish patients with open tibial fractures. We included all Swedish emergency hospitals to get results applicable to the entire population. As we studied the subpopulations of moderate and severe injury, we acquired specific information on the most complicated injuries that are a challenge for both patients and healthcare providers.
There are limitations with the study. We do not know the actual amount of open tibial fractures in Sweden, as records of patients with closed tibial fractures or ankle fractures were not reviewed. However, we suppose that the number missed is not considerable, and open tibial fractures are not treated in outpatient care. The hospital provided a various amount of information and the records were reviewed by one orthopedic surgeon only. The results would be more reliable when repeated by several orthopedic surgeons.
In Sweden, there are several nationwide registers that gather overlapping information.
Since 2012, the Swedish Fracture Register is used for direct on-line registration of all fractures by orthopedic surgeons and other physicians. Eighty percent of Swedish orthopedic departments participate, and 70–90% of fractures are registered in each department.16 With higher coverage, the fracture register will offer better possibilities of follow-up including patient outcome. A comparison between the SNPR and the Swedish Fracture Register would be valuable.
Regarding cause of injury, the Swedish Transport Agency holds a database that includes all road traffic accidents causing personal injury. This database, STRADA (Swedish Traffic Accident Data Acquisition), has a nationwide coverage since 2016.17 Data are collected from the police as well as the healthcare system. A comparison with E-codes from SNPR would be interesting. In the future, a merging of overlapping registers like these would simplify extraction of data for research purposes as well as information for healthcare providers.
Conclusion
The Swedish National Patient Register is widely used for research purposes. In this study, we conclude that the PPV of the diagnosis of open tibial fracture, a trauma diagnosis, is high, and research data should be interpreted accordingly. The PPV of E-codes is lower, and the improvement of encoding and reporting is a worthwhile objective. Most open tibial fractures in Sweden are caused by high-energy trauma and unprotected road users are especially at risk for complicated injuries.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tampe U, Weiss RJ, Stark B, Sommar P, Al Dabbagh Z, Jansson K-Å. Lower extremity soft tissue reconstruction and amputation rates in patients with open tibial fractures in Sweden during 1998–2010. BMC Surg. 2014;14(1):80. doi:10.1186/1471-2482-14-80
2. The National Board of Health and Welfare, the National Patient Register. Available from: https://www.socialstyrelsen.se/en/statistics-and-data/registers/.
3. Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450. doi:10.1186/1471-2458-11-450
4. Nilsson AC, Spetz CL, Carsjö K, Nightingale R, Smedby B. Reliability of the hospital registry. The diagnostic data are better than their reputation. Läkartidningen. 1994;91:598–605.
5. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24(8):742–746. doi:6471139
6. Huttunen TT, Kannus P, Pihlajamäki H, Mattila VM. Pertrochanteric fracture of the femur in the Finnish National Hospital Discharge Register: validity of procedural coding, external cause for injury and diagnosis. BMC Musculoskelet Disord. 2014;15:98. doi:10.1186/1471-2474-15-98
7. Edwards NM, Kristensen PK, Pedersen AB. The positive predictive value of hip fracture diagnoses and surgical procedure codes in the Danish Multidisciplinary Hip Fracture Registry and the Danish National Patient Registry. Clin Epidemiol. 2020;12:123–131. doi:10.2147/CLEP.S238722
8. Weiss RJ, Montgomery SM, Ehlin A, Al Dabbagh Z, Stark A, Jansson K-A. Decreasing incidence of tibial shaft fractures between 1998 and 2004: information based on 10,627 Swedish inpatients. Acta Orthop. 2008;79(4):526–533. doi:10.1080/17453670710015535
9. Court-Brown CM, Rimmer S, Prakash U, McQueen MM. The epidemiology of open long bone fractures. Injury. 1998;29(7):529–534. doi:10.1016/S0020-1383(98)00125-9
10. Weber CD, Hildebrand F, Kobbe P, Lefering R, Sellei RM, Pape HC. Epidemiology of open tibia fractures in a population-based database: update on current risk factors and clinical implications. Eur J Trauma Emerg Surg. 2019;45(3):445–453. doi:10.1007/s00068-018-0916-9
11. Connelly CL, Bucknall V, Jenkins PJ, Court-Brown CM, McQueen MM, Biant LC. Outcome at 12 to 22 years of 1502 tibial shaft fractures. Bone Joint J. 2014;96B(10):1370–1377. doi:10.1302/0301-620X.96B10.32914
12. Bouaoun L, Haddak MM, Amoros E. Road crash fatality rates in France: a comparison of road user types, taking account of travel practices. Accid Anal Prev. 2015;75:217–225. doi:10.1016/j.aap.2014.10.025
13. Winkler D, Goudie ST, Court-Brown CM. The changing epidemiology of open fractures in vehicle occupants, pedestrians, motorcyclists and cyclists. Injury. 2018;49(2):208–212. doi:10.1016/j.injury.2017.11.009
14. Rajasekaran S, Naresh Babu J, Dheenadhayalan J, et al. A score for predicting salvage and outcome in Gustilo type-IIIA and type-IIIB open tibial fractures. J Bone Joint Surg. 2006;88(10):1351–1360. doi:10.1302/0301-620X.88B10.17631
15. Nanchahal JN, Khan S, Moran U, Barrett C, Sanderson S, Pallister FI. Standards for the Management of Open Fractures of the Lower Limb. London: Royal Society of Medicine Press;2009. Avaiable from: http://www.bapras.org.uk/professionals/clinical-guidance/open-fractures-of-thelower-limb#FullGuide.
16. Wennergren D, Ekholm C, Sandelin, A, Möller M. The Swedish fracture register: 103,000 fractures registered. BMC Musculoskeletal Disorders. 2015;16(1):338. doi:10.1186/s12891-015-0795-8
17. Strada (Swedish Traffic Accident Data Acquisition). Available from: https://www.transportstyrelsen.se/STRADA.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.