")
Back to Journals » Clinical Ophthalmology » Volume 8
Diagnosis of dry eye disease and emerging technologies
Authors Zeev MS, Miller D, Latkany R
Received 14 January 2014
Accepted for publication 3 March 2014
Published 20 March 2014 Volume 2014:8 Pages 581—590
DOI https://doi.org/10.2147/OPTH.S45444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Maya Salomon-Ben Zeev,1 Darby Douglas Miller,2,3 Robert Latkany1,2
1The Dry Eye Center at Physician Eyecare of New York, 2New York Eye and Ear Infirmary, 3Laser and Corneal Surgery Associates, New York, NY, USA
Abstract: Dry eye is one of the most commonly encountered problems in ophthalmology. Signs can include punctate epithelial erosions, hyperemia, low tear lakes, rapid tear break-up time, and meibomian gland disease. Current methods of diagnosis include a slit-lamp examination with and without different stains, including fluorescein, rose bengal, and lissamine green. Other methods are the Schirmer test, tear function index, tear break-up time, and functional visual acuity. Emerging technologies include meniscometry, optical coherence tomography, tear film stability analysis, interferometry, tear osmolarity, the tear film normalization test, ocular surface thermography, and tear biomarkers. Patient-specific considerations involve relevant history of autoimmune disease, refractive surgery or use of oral medications, and allergies or rosacea. Other patient considerations include clinical examination for lid margin disease and presence of lagophthalmos or blink abnormalities. Given a complex presentation and a variety of signs and symptoms, it would be beneficial if there was an inexpensive, readily available, and reproducible diagnostic test for dry eye.
Keywords: cornea, dry eye, tear film, stain
Introduction
Dry eye disease is one of the most common reasons why a patient visits an eye care professional. It is challenging to define due to a wide spectrum of abnormalities to the ocular surface and a variety of presenting symptoms that can change from day to day and from patient to patient.1 What makes it even more puzzling is that there is no consistent, well accepted, diagnostic test that is both readily available and reproducible.
The Latin term “keratoconjunctivitis sicca” refers to dry eye disease or dry inflammation of the cornea and conjunctiva. The term was coined by Henrik SC Sjogren, a Swedish ophthalmologist, and in 1950 reintroduced by Andrew De Roetth as “dry eye”.2,3 Historically, dry eye disease was defined as reduction of the aqueous phase of tear film. In 1995, the definition was modified to include medical and ocular diseases that reduce tear production and/or increase tear evaporation.4 In 2007, the International Dry Eye Workshop updated the original definition and classified dry eye as: “a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage of the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface”.5
Increasing age, perimenopausal stages in women, hormonal diseases, and certain medications are just a few factors that can result in dryness on the ocular surface.6–9 Other factors include long-term contact lens wear, smoking, and laser refractive eye surgery.10–12 Activities like extended computer use, watching television, and reading can trigger and/or exacerbate dry eye symptoms.13 Low relative humidity, such as an office environment and air-conditioned areas, can be detrimental to the tear film.14 Coexisting autoimmune diseases, allergies, or rosacea can also contribute to dry eye-related symptoms.15
Ocular manifestations
Patients who have dry eye often complain of eye irritation, a gritty or foreign body sensation, burning, tearing, photophobia, stinging, or intermittent sharp pain. Blurry vision that improves with blinking or instillation of nonviscous artificial tears, albeit temporarily, is also common. Dry eye patients may have all, some, or none of these symptoms. A careful history-taking contributes greatly to a correct diagnosis. For example, if a patient complains of discomfort upon awakening, this may indicate nocturnal lagophthalmos. The clinician can then look for inferior punctate corneal erosions and poor lid closure after asking the patient to close their lids like they do when they sleep at night. The patient history can guide a more focused slit-lamp examination helping to identify certain ocular manifestations.
A thorough slit-lamp examination should be done before performing any other tests, which may alter or mask some of the relevant findings on examination, resulting in a possible misdiagnosis. Dry eye signs identified on slit-lamp examination include superficial corneal erosions, inadequate tear lake volume, early tear film break-up time, conjunctival hyperemia, conjunctival surface irregularities, and meibomian gland dysfunction.
Whether a patient comes in for a routine examination or because of symptoms that may suggest dry eye, the eye care professional may perform various diagnostic tests to determine if the patient has dry eye disease because of aqueous deficiency, evaporative reasons, or both.
Current methods of diagnosis
Schirmer test
First described in 1903 by Schirmer, this test is still one of the most commonly used measures of tear production.2 Variations of the Schirmer test have been created. The Schirmer I test measures total tear secretion, including reflex and basal tears. Without instilling anesthetic drops, the Schirmer strips are inserted into the temporal lower conjunctival sac, avoiding contact with the cornea, and the length of wetting strips is recorded in millimeters after 5 minutes. Normal mean test values range from 8 mm to 33 mm, but an accepted normal value is greater than 10 mm.16,17 In a study comparing Schirmer I with and without anesthesia, with anesthesia was found to be more objective and reliable in terms of diagnosing dry eyes than without anesthesia.18 However, if the clinician chooses to perform the Schirmer I test without anesthesia, it has been found that patients with eyes closed have a more reliable result because the eyelid margin and eyelash stimulation can alter the tear turnover rate.19 A variation is the Schirmer II test, which uses topical anesthesia and only measures reflex tears using stimulation with a cotton tip applicator. A shorter one-minute Schirmer test was found to decrease eye discomfort as well as save time.20 The Schirmer test is more reproducible in more advanced cases of dry eye disease.21 Further, even the position of the eye during the Schirmer test appears to influence the results, with inferior gaze producing a falsely higher result.22 Although the Schirmer test is one of the most widely used tools in diagnosing dry eye, the lengthy nature of the test, the fact that most patients find the test irritating and invasive, and its unreliable and largely irreproducible nature may explain a high risk of underdiagnosis.23
Fluorescein staining
Fluorescein sodium can be used to identify corneal epithelial defects and can be a useful tool in evaluating dry eye. The corneal surface will stain whenever there is a disruption of cell-to-cell junctions. The staining can show corneal superficial punctate epithelial erosions in patterns that are consistent with certain causes of dry eye. Erosions seen in the lower third of the cornea, for example, could signify lid-related exposure issues such as infrequent or inadequate blink or lagophthalmos. Since epithelial erosions can come from other sources like refractive surgery, contact lens use, exposure-related reasons like thyroid orbitopathy, previous eyelid surgeries, or infections, this type of staining cannot show direct proof of dry eye, nor can it be considered a very sensitive or specific measure.24,25
Often, eye care professionals instill a prepared drop of anesthesia mixed with fluorescein. Early in the slit-lamp examination, this large volume could mask corneal staining. Ideally, only 2–5 μL should be instilled using a micropipette. Another issue with the use of fluorescein drops is that, in some offices, the technician instills some version of this drop before hand to check the patient’s intraocular pressure. By the time the patient is examined by the eye doctor, the fluorescein has either evaporated, the preservative caused some surface toxicity, or the means by which the technician checks the intraocular pressure can cause subtle epithelial damage. Ideally, to assess properly whether or not a patient has dry eye, the patient should be evaluated before any drops or testing is done to establish a baseline appearance. The patient may need to be examined at different times of the day in order to compare morning versus late afternoon findings. It is also important to compare examinations on days when the patient is symptomatic versus asymptomatic. One study did find poor repeatability of the presence or absence of inferior corneal staining in dry eye patients.21 Thus, one examination alone may not be sufficient to exclude the diagnosis of dry eye disease. Further, the clinician should ask the patient if symptoms like discomfort or irritation dissipate after instilling an anesthetic eye drop. If the discomfort persists despite anesthesia, it is the author’s opinion that there may be more than ocular surface disease present.
Rose bengal staining
Rose bengal (RB) staining occurs in areas on the cornea or conjunctiva that lack membrane-associated mucins.26 RB is an important tool in evaluating dry eye, but it is best used as an adjunct due to its lack of sensitivity and specificity.27 RB staining can occur in asymptomatic patients and there is no clearly defined relationship between ocular surface damage specific to dry eye diagnosis and a patient’s symptoms.28 It is important to note that RB is toxic to the corneal epithelium.29 RB without concurrent anesthesia can cause discomfort upon instillation and is therefore less commonly used than fluorescein.
Lissamine green staining
Lissamine green (LG) is another dye similar to RB that stains the ocular surface. Both types of dyes have similar staining patterns and can be interchangeable. But unlike RB, LG is not toxic to the corneal epithelium, and is better tolerated.30 Ten microliters of 1% LG was found to give the best reliability, especially when using a red filter.31 There is at least moderate within-grader and between-grader reliability when evaluating LG staining.32 There are several grading systems that evaluate ocular surface staining, including the Oxford Scheme, the van Bijsterveld system, and the National Eye Institute/Industry Workshop guidelines.4,33,34 However, there are no published studies that show one is superior to another.
Tear function index
The tear function index is another method of analyzing tear production and is similar to the anesthetized Schirmer test. Five minutes after instilling a 10 μL drop of fluorescein, the length of the wetted area is measured and its intensity is compared with a standard color strip. The tear clearance rate is based on the rate at which the color of the fluorescein dye fades. The tear function index is then determined by dividing the value of the Schirmer test with anesthesia, which reflects the tear drainage, by the tear clearance rate.35 An index score less than 96 indicates dry eyes and an index score less than 34 signifies Sjogren’s syndrome.36 A disadvantage of this test is that it fails to account for evaporation of tear fluid. In addition, instillation of fluorescein increases the tear volume and could act as a stimulant because of its potential to cause irritation and tear stimulation.37 However, the tear function index has been shown to improve sensitivity and specificity in diagnosing dry eyes compared with the standard Schirmer measure or tear clearance rate alone.36 Although the tear function index is relatively simple and inexpensive, it is time-consuming and subjective, which limits its practical application in an office setting.
Fluorescein clearance test
To test a combination of tear secretion and drainage, the fluorescein clearance test can be done as a modification of the Schirmer test. The fluorescein clearance test includes the use of Schirmer paper and application of proparacaine and 5 μL of Fluoress® (0.25% fluorescein with 0.4% benoxinate hydrochloride).38 The wetting of the strip and the disappearance of dye are both measured in 10-minute increments. A value of 3 mm or greater at the first 10-minute interval is the standard for normal. At the 20-minute interval, if the dye cannot be detected, then clearance is normal. This dynamic test analyzes basal and reflex tears and clearance. Since the fluorescein clearance test uses Schirmer paper and readily available drops, it is easily performed and inexpensive. However, like the Schirmer test, it is time-consuming, irritating, and not reproducible.17 A device called the CytoFluor II fluorophotometer (Applied Biosystems, Framingham, MA, USA) is another means of measuring fluorescein clearance and was shown to have a greater predictive value for ocular irritation compared with the Schirmer I test.39 The technology, however, is expensive and time-consuming.
Tear break-up time
The tear break-up time (TBUT) measures stability of the tear film. With fluorescein instilled, TBUT is the time interval after a patient blinks to the first appearance of dryness in the tear film.40–43 A patient is asked not to blink after instillation of fluorescein. The patient has dry eye if a dry area appears before 10 seconds. The TBUT can be used to evaluate an unstable tear film, leaving the physician to investigate further the cause of the instability and look for surface irregularities or lid margin disease. Although this test is inexpensive, rapid to perform, and uses readily available supplies, it is not reproducible and it is inaccurate.44,45 The average score of two separate TBUT measurements, however, helps increase its repeatability.21 TBUT should be done with 5 μL fluorescein drops alone without the anesthetic, although many eye care professionals assess TBUT with combination eye drops or strips doused with anesthetic eye drops.
Functional visual acuity
A common complaint of patients who have dry eye is decreased visual acuity. Activities that require concentration, such as reading, driving, and computer work, cause the blinking rate to be suppressed.46 Patients who have an unstable tear film can show decreased visual acuity especially at these times of prolonged concentration.47 Functional visual acuity reflects performance in relation to specific daily activities involving visual tasks. Eyes can become more dry when normal blinking is suppressed during gazing activities. The functional visual acuity was initially measured by manually raising patients’ upper eyelids for 10–20 seconds.48 The system was improved by development of a device that allows continuous monocular visual acuity measurement during a 30-second blink-free period. Functional visual acuity was significantly lower in dry eye patients compared with controls.49 There are no restraints of blinking in this new system that measures functional visual acuity at 10-second intervals, 5 minutes after the instillation of topical anesthesia. Functional visual acuity in patients with dry eyes has significantly worse results than in patients who have punctal plugs.50 Although functional visual acuity testing, when not using a particular device, is inexpensive and the materials are readily available, it is time-consuming and subjective.
Tear meniscus assessment
The meniscus, or tear lake, is the amount of tears resting at the junction of the bulbar conjunctiva and the lower eyelid margin. Measurements of the tear meniscus height and curvature are used to determine the presence or absence of dry eye.51 A photograph is taken of the tear meniscus after a small amount of fluorescein is instilled and the photographs are evaluated using a computer analysis program. Without such a device, the meniscus can also be measured by using a slit-lamp that is capable of measuring micrometers. Although lower tear meniscus height can be reliably measured by slit-lamp biomicroscopy without staining, measurements are more repeatable with Tearscope-Plus (Keeler Ltd, Windsor, UK).52,53
Whichever method is used to obtain measurements of the tear lake, a patient normally has a tear meniscus height of 0.2–0.5 mm, but in a patient with dry eye, it is usually less than 0.2 mm.54–56 Very often, by the time the eye doctor sees the patient, other drops have already been instilled in the eyes, resulting in an artificially higher tear lake. While these aforementioned methods of assessing the tear meniscus are straightforward, some patients with a low tear lake do not necessarily have dry eye.54 Thus, tear meniscus assessment should be utilized in conjunction with other tests.
Emerging technologies for diagnosis
Reflective meniscometry
Reflective meniscometry (Table 1) is a noninvasive technique providing quantitative information about tear meniscus shape and volume.57 A new, portable, slit-lamp mounted digital meniscometer was found to produce measurements of the tear meniscus radius similar to those obtained by ocular coherence tomography (OCT).58,59 Although there are limited studies with this new technology, it shows promise and is less expensive than OCT.
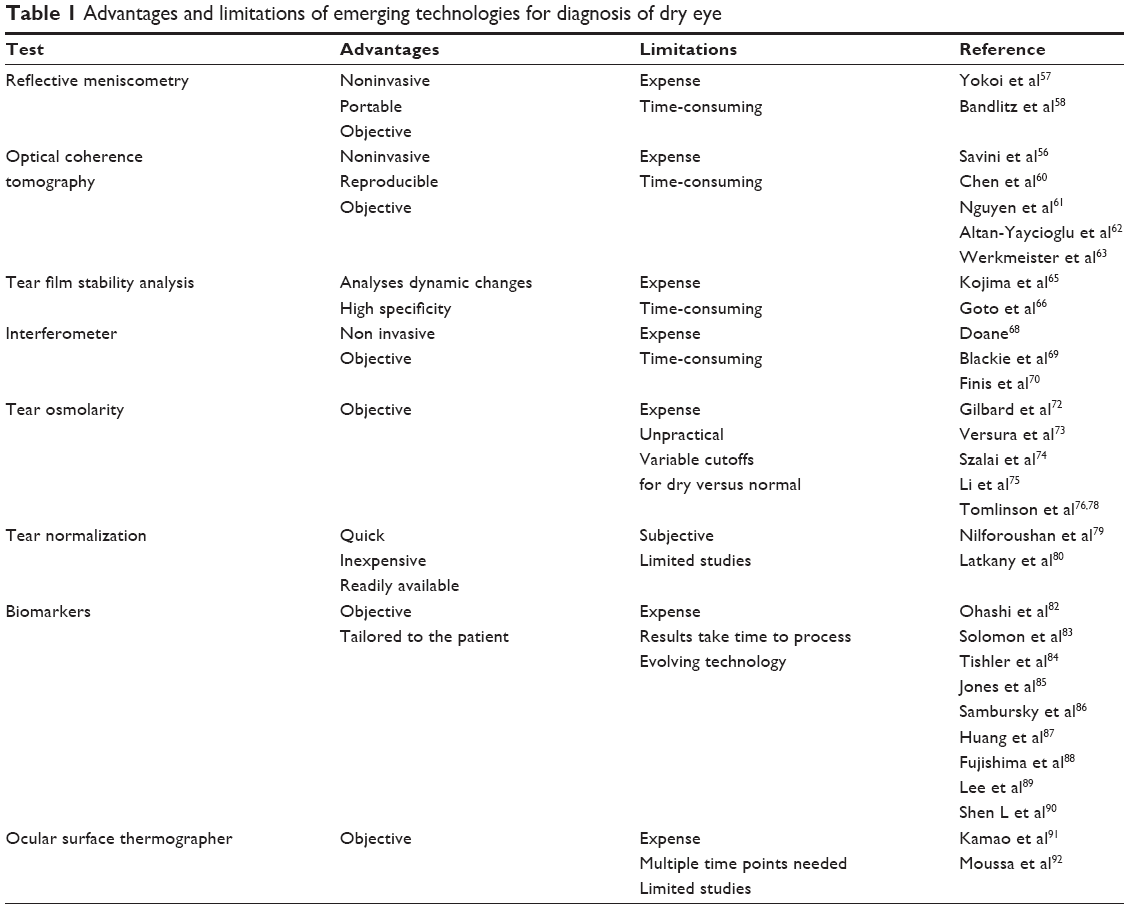 | Table 1 Advantages and limitations of emerging technologies for diagnosis of dry eye |
Optical coherence tomography
Another way to measure the tear lake is by OCT. Tear meniscus heights were found to be significantly lower in aqueous-deficient dry eye patients compared with controls using OCT.56 In another study, the tear meniscus volume was measured with OCT after punctal occlusion.60 The results showed that dry eye patients with punctal plugs have higher tear meniscus heights. Studies have shown that OCT is a reproducible, objective, and noninvasive instrument for measuring the tear lake.61,62 Of interesting potential value is the ability to measure tear film thickness using OCT. One study found highly reproducible measurements using ultrahigh resolution OCT. The average central tear film thickness was 4.79±0.88 μm, with an intraclass correlation coefficient of 0.97.63 OCT could not only aid in the diagnosis of dry eyes but could also gauge the success of particular therapies based on before and after measurements.
OCT is gaining in popularity now that many practices have machines (two examples are Optovue, Freemont, CA, USA, and Zeiss Cirrus, Carl Zeiss Meditec AG, Jena, Germany) with anterior segment imaging capabilities. However, the technology is expensive, time-consuming, and often not reimbursed. In addition, further studies need to be performed in larger patient populations to assess the sensitivity and specificity of OCT in diagnosis of dry eye. With OCT, the tear lake can be captured in a single moment in time, but whether that single measurement represents the true volume of the tear film throughout the day is questionable because there can be intraday variations.64 Serial OCT measurements may need to be done to establish a mean tear lake volume and tear film thickness.
Tear film stability analysis
Tear film stability is important to take into account when diagnosing dry eye. The tear film stability analysis system (TSAS), developed in Japan, is a sensitive videokeratographer.65,66 Instability of tear film is found in meibomian gland dysfunction, conjunctivochalasis, and aqueous tear dysfunction states. The TSAS uses videokeratography to take ten topographic images at one-second intervals of the corneal surface. The TSAS quantitatively analyzes dynamic changes in tear stability over 10 seconds by measuring areas of irregularity. Patients who have more irregularities have more severe dry eye disease. Two measures that can be used for this test include the surface regularity index and the surface asymmetry index.65 The system is commercially available (RT-6000; Tomey Corporation, Nagoya, Japan), but the technology is expensive and time-consuming, and studies are limited. Another option, for clinicians who may already have a wavefront aberrometer, is to evaluate higher order aberrations. Dry eye patients showed greater optical aberrations compared with normal control eyes as a result of increased tear film irregularity.67
Interferometer
The lipid layer of the tear film can be analyzed visually using a tear film interferometer.68 Grades are assigned after comparing the images for uniformity and color. This evaluation allows dryness to be measured based on analysis of the precorneal tear lipid layer and possible correlation of meibomian gland dysfunction. LipiView (TearScience Inc., Morrisville, NC, USA) is an example of this technology. A strong correlation was found between dry eye symptoms and thin lipid layers (less than 60 nm) and between a lack of dry eye symptoms and thick lipid layers (more than 75 nm).69 More recently, patients with low lipid layer thicknesses were found to have a higher probability of meibomian gland dysfunction, which can cause and/or exacerbate dry eye symptoms.70 Another advantage of LipiView is that it records a video of the patient blinking, so the clinician can determine if the patient is a partial blinker. A different example, the Keratograph 5M (Oculus, Wetzlar, Germany) evaluates meibography which allows easy visualization of the meibomian glands.71 Although this precision is promising, the disadvantages of expense, time, and reimbursement are apparent.
Tear osmolarity
Patients with dry eyes have been found to have an increased level of tear osmolarity. An abnormal tear osmolarity shows failure of homeostatic regularity, which can lead to increased damage to the ocular surface and more inflammation.72 The TearLab osmolarity system (TearLab Corporation, San Diego, CA, USA) can be used to quantify osmolarity numbers and help in diagnosis of dry eye.73 The TearLab marks hyperosmolarity as a key factor of dry eye disease, but osmolarity measurements with the TearLab showed no ability to distinguish between healthy individuals and patients with dry eye.74 Also, tear osmolarity measurements were found to vary on average by 21.9 mOsm/L in dry eye patients during the day.75 An osmolarity value greater than 308 mOsm/L is generally indicative of dry eye.74 Another study noted a cutoff value of 315 mOsm/L for healthy eyes and dry eyes.76 The technology provides a quantifiable means of diagnosing dry eye, but the inability to distinguish between dry eye and healthy patients is problematic. Again, the technology is expensive and time-consuming. It is, however, potentially reimbursable.77 This instrument can be better evaluated with larger sample studies.
Another way to evaluate tear osmolarity is to study the freezing temperatures of tear samples (Clifton Osmometer; Clifton Technical Physics, Hartford, NY, USA). Diluted samples will freeze at higher temperatures than concentrated samples, meaning that the lower the freezing temperature, the more likely the patient has dry eye. This test must be completed quickly to avoid any evaporation of the tear sample. Although reproducible, this test is difficult to perform in a clinic setting. The newer technology in the TearLab osmolarity system uses electrical impedance and correlates well with the Clifton osmometer.78 Although promising, further studies need to be performed.
Tear normalization test
Nonviscous artificial tears provide a temporary but significant improvement of visual acuity in symptomatic and asymptomatic dry eye patients.79 The tear normalization test takes advantage of this fact. It works best by examining a patient before any drops are instilled in their eyes. Near or distance visual acuity is checked and stopped at the line where the patient is blurry. Their vision is retested after instillation of a 0.5% carboxymethylcellulose drop, such as Refresh Plus® (Allergan, Irvine, CA, USA) or any other nonviscous artificial tear drop. If their vision does not improve, then they most likely do not have dry eye. However, if their vision improves, if only for a few seconds, then they most likely have dry eye. Two lines or more of improvement was 82.5% sensitive and 100% specific for dry eye.80 In addition, it is the authors’ opinion that if vision improves substantially, this usually indicates a more severe variety of dry eye. This test has the benefit of being inexpensive and available in all doctors’ offices, and can be performed by a technician. However, there are no independent studies assessing reproducibility, and the test should be performed before any other eye drops are instilled.
Biomarkers
Analyzing tear protein patterns in patients is another way dryness can be evaluated. Patients with early dry eye characteristically have lower protein content compared with patients who do not have dry eye.81 Specifically, patients with dry eye do not contain as many protective proteins and have more proinflammatory markers when compared with patients without dry eye.82–85 High levels of the inflammatory biomarker, matrix metalloproteinase 9, may lead to an earlier diagnosis of dry eye using an office test called the InflammaDry Detector (Rapid Pathogen Screening Inc, Sarasota, FL, USA), which showed 85% sensitivity and 94% specificity in diagnosing dry eye.86 Another study looked at tear fluid collected at day 0 and day 7, and measured concentrations of 43 protein markers. The protein markers interleukin-1Ra and interleukin-8 have also been reported in patients with dry eye.87
Another diagnostic tool is the TearScan MicroAssay System (Advanced Tear Diagnostics, Birmingham, AL, USA). The relationship between allergy and dry eye has long been established, so technology that can quantify dry eye and allergy biomarkers like lactoferrin and immunoglobulin E in the tear film will be very helpful.88 Other technologies include EyePrim (OPIA Technologies, Paris, France), which can procure cells from the ocular surface for biological testing. The device allows quick and painless sampling of conjunctival cells, which can then be analyzed for dry eye biomarkers. Further studies will clarify its sensitivity and specificity in diagnosing different types of ocular surface disease. Another study using a multiplex immunobead assay of tear samples found elevated cytokine levels of interleukin-17, interleukin-6, and tumor necrosis factor-alpha in patients with dry eye and Sjogren syndrome compared with patients with dry eye without Sjogren syndrome and controls.89 A new laboratory test known as Sjö (Nicox, Sophia Antipolis, France) looks at novel proprietary biomarkers in Sjogren syndrome, including salivary gland protein 1, parotid secretory protein, and carbonic anhydrase 6. These autoantibodies occurred earlier in the course of the disease than antibodies to Ro or La.90
The study of biomarkers may lead to developments in medications that can help treat dry eye disease. However, although promising, its use is limited in current clinical practice due to the expense and lack of insurance reimbursement.
Ocular surface thermographer
The use of a device to measure the temperature of the tear film called the Ocular Surface Thermographer (Tomey Corporation) has been shown to be fairly sensitive and specific when comparing dry eye patients with healthy controls.91 Measurements of ocular surface temperature 10 seconds after eye opening may prove to be a repeatable, quantifiable measurement for dry eyes but further multicenter trials need to be performed. It was recently found that corneal surface temperature does not change diurnally in healthy subjects.92 This leads to the assumption that diurnal changes in corneal temperature may indicate ocular surface abnormality or corneal pathology. Ocular surface thermography shows promise in diagnosing dry eye, although its use may be limited due to expense.
Patient-specific considerations of dry eye disease
Lid margin assessment
Evaporative dry eye can occur in patients with meibomian gland dysfunction. Different scales are used to grade meibomian gland dysfunction. The International Workshop on meibomian gland dysfunction published a grading scale in 2011 that evaluates the ducts, acini, and secretions on a scale from 1 to 3.93 Regardless of the classification used, it is important that the glands be examined at the slit-lamp by pulling down on the lower lid and up on the upper lid. The glands should be expressed, and the consistency and contents of the glands evaluated. The lid margin assessment should also include evaluation of gland dropout, telangiectasias, meibomian gland plugging, collarettes, and chalazia. Although quick and easy to perform, there is no commonly accepted grading scale. It is likely that there is also a fair amount of variability from examiner to examiner, and there is poor repeatability of meibomian gland dysfunction classification.21
Patient questionnaires
Questionnaires can help detect cases of dry eye that are subclinical and help practitioners comprehend how having dry eye can affect everyday activities. If a patient is not asked whether certain dryness symptoms are present, they may never tell you. This is important before laser refractive surgery or premium intraocular lens insertion. It is important to treat dry eyes before any high visual expectation surgeries. Thus, questionnaires may have value in detecting an otherwise unrecognizable dry eye patient, such as in contact lens wearers.94 The Standard Patient Evaluation of Eye Dryness questionnaire is a repeatable and effective measure that can help identify a patient’s symptoms.95 This survey uses a scale ranging from 0 to 4 to focus on frequency and severity of symptoms. Another questionnaire is the Ocular Surface Disease Index.96 This survey grades on a scale ranging from 0 to 100, with higher scores signifying higher disability. The Ocular Surface Disease Index helps to differentiate the sensitivity and specificity values between dry eye and healthy patients. The Ocular Surface Disease Index questionnaire has been reported to show reliable results in measuring the severity of a patient’s dry eye. Other questionnaires such as the Dry Eye Questionnaire and its variations (DEQ, DEQ-8, Contact Lens Dry Eye Questionnaire), the National Eye Institute Visual Functioning Questionnaire, and the Impact of Dry Eye on Everyday Life Questionnaire can help distinguish between symptomatic and asymptomatic patients.97–99 A recent study showed that only the Ocular Surface Disease Index and Impact of Dry Eye on Everyday Life questionnaires are validated while others have not been tested for reliability.100 It is important to remember that there is moderate repeatability, with patients’ subjectively reporting symptoms of dryness from one examination day to another.1 Questionnaires can be completed while the patient is in the waiting room, but interpreting the data still takes time.
Lagophthalmos and blink evaluation
Lagophthalmos is the inability to completely close the eyelids. Patients affected by this condition can have dry eye symptoms. Importantly, however, not all lagophthalmos patients have dry eye signs or symptoms. While some patients already know that they sleep with their eyes open, many go undetected. If there is no history of reported nocturnal lagophthalmos, an eye care professional can ask the patient to gently close their eyes as if they are asleep during a slit-lamp examination, and then observe the patient as they are closing their lids and examine if any lagophthalmos is present. A case of obvious lagophthalmos will already be known to the patient, or easily detected on slit-lamp examination. However, cases of eyelash obstructed or overhang lagophthalmos are subtle and can often be missed on examination.101
A complete eyelid blink is important in maintaining a stable tear film and a healthy ocular surface. Prolonged use of a video display terminal reduced blink rates by half compared with baseline levels and increased the percentage of incomplete blinks.46,102,103 While machines can be used to measure blink rates in patients, it is also possible to simply observe patients during clinical history-taking and make note of the frequency and quality of their blink.
Conclusion
Given its complex and varied presentation, it is no wonder that dry eye disease often tends to be misdiagnosed. With poorly correlating signs and symptoms, extreme variability with season and time of day, and even variability between eye care professional examinations, it is an intricate disease process, and we are only beginning to understand its complexity. It does not help that patients with dry eye disease have high pain sensitivity and low pain tolerance,104 which can take up a considerable amount of chair time. What would help are simple, inexpensive, and highly sensitive and specific tests that can reliably aid in the diagnosis of dry eye. This will then lead to more specific treatments for dry eye disease that could target the source of the dryness. For now, we are unfortunately left with numerous diagnostic tests that are not yet widely accepted and are often not reproducible. It would help if there were more multicenter, nonsponsored clinical trials comparing the currently available tests to determine which should be considered the gold standard for dry eye diagnostic testing. Until then, it is critical to rely heavily on careful clinical history-taking, a detailed slit-lamp examination, and utilization of the tests above, such as TBUT, fluorescein staining, and eyelid margin assessment. If further workup is needed, consider referral to an ocular surface specialist.
Disclosure
The authors report no conflicts of interest in this work.
References
Nichols KK, Nichols JJ, Mitchen GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004;23(8):762–770. | ||
Schirmer O. Studien zur physiologie und pathologie der tranen-absonderung und tranenabfuhr. Graefes Arch Clin Exp Ophthalmol. 1903;56:197–291. German. | ||
De Roetth A. Lacrimation in normal eyes. Arch Ophthalmol. 1953;49(2):185–189. | ||
Lemp MA. Report of the National Eye Institute/Industry workshop on the Clinical Trials in Dry Eyes. CLAO J. 1995;21(4):221–232. | ||
[No authors listed]. Dry Eye Workshop. The definition and classification of dry eye disease: report of the definition and classification subcommittee of the International Dry Eye Workshop. Ocul Surf. 2007;5(2):75–92. | ||
Hashemi H, Khabazkhoob M, Kheirkhah A, et al. Prevalence of dry eye syndrome in an adult population. Clin Experiment Ophthalmol. August 8, 2013. [Epub ahead of print]. | ||
Scuderi G, Contestabile MT, Gagliano C, Iacovello D, Scuderi L, Avitabile T. Effects of phytoestrogen in postmenopausal women with dry eye syndrome: a randomized clinical trial. Can J Ophthalmol. 2012;47(6):489–492. | ||
Rocha EM, Mantelli F, Nominato, Bonini S. Hormones and dry eye syndrome: an update on what we do and don’t know. Curr Opin Ophthalmol. 2013;24(4):348–355. | ||
Wong J, Lan W, Ong LM, Tong L. Non-hormonal systemic medications and dry eye. Ocul Surf. 2011;9(4):212–226. | ||
Farris RL. The dry eye: its mechanism and therapy, with evidence that contact lens is a cause. CLAO J. 1986;12(4):234–246. | ||
Grus FH, Sabuncuo P, Augustin A, Pfeiffer N. Effect of smoking on tear proteins. Graefes Arch Clin Exp Ophthalmol. 2002;240(11):889–892. | ||
Quinto GG, Camacho W, Behrens A. Postrefractive surgery dry eye. Curr Opin Ophthalmol. 2008;19(4):335–341. | ||
Moschos MM, Chatziralli IP, Siasou G, Papazisis L. [Visual problems in young adults due to computer use]. Klin Monbl Augenheilkd. 2012;229(4):379–381. German. | ||
Abusharha AA, Pearce EI. The effect of low humidity on the human tear film. Cornea. 2013;32(4):429–434. | ||
Palmowski AM, Ruprecht KW. The cornea and systemic diseases. Curr Opin Ophthalmol. 1995;6(4):17–20. | ||
Shapiro A, Merin S. Schirmer test and break-up time of tear film in normal subjects. Am J Ophthalmol. 1979;88(4):752–757. | ||
Jordan A, Baum J. Basic tear flow. Does it exist? Ophthalmology. 1980;87:920–930. | ||
Li N, Deng XG, He MF. Comparison of the Schirmer I test with and without topical anesthesia for diagnosing dry eye. Int J Ophthalmol. 2012;5(4):478–481. | ||
Serin D, Karsloglu S, Kyan A, Alagoz G. A simple approach to the repeatability of the Schirmer test without anesthesia: eyes open or closed. Cornea. 2007;26(8):903–906. | ||
Kashkouli MB, Pakdel F, Amani A, Asefi M, Aghai GH, Falavarjani KG. A modified Schirmer test in dry eye and normal subjects: open versus closed eye and 1-minute versus 5-minutes tests. Cornea. 2010;29(4):384–387. | ||
Nichols KK, Mitchell GL, Zadnik K. The repeatability of clinical measurements of dry eye. Cornea. 2004;23(3):272–285. | ||
Bitton E, Wittich W. Influence of eye position on the Schirmer tear test. Cont Lens Anterior Eye. December 18, 2013. [Epub ahead of print]. | ||
Feldman F, Wood MM. Evaluation of the Schirmer tear test. Can J Ophthalmol. 1979;14(4):257–259. | ||
Yoon KC, Im SK, Kim HG, You IC. Usefulness of double vital staining with 1% fluorescein and 1% lissamine green in patients with dry eye syndrome. Cornea. 2011;30(9):972–976. | ||
Savini G, Barboni P, Zanini M. The incidence and risk factors for developing dry eye after myopic LASIK. Am J Ophthalmol. 2006;142(2):355–356. | ||
Feenstra RP, Tseng SC. What is actually stained by rose bengal? Arch Ophthalmol. 1992;110(7):984–993. | ||
Schein OD, Tielsch JM, Munõz B, Bandeen-Roche K, West S. Relation between signs and symptoms of dry eye in the elderly: a population-based perspective. Ophthalmology. 1997;104(9):1395–1401. | ||
Khan-Lim D, Berry M. Still confused about rose bengal? Curr Eye Res. 2004;29(4–5):311–317. | ||
Kim J, Foulks GN. Evaluation of the effect of lissamine green and rose bengal on human corneal epitheliual cells. Cornea. 1999;18(3):328–332. | ||
Machado LM, Castro RS, Fontes BM. Staining patterns in dry eye syndrome: rose bengal versus lissamine green. Cornea. 2009;28(7):732–734. | ||
Hamrah P, Alipour F, Jiang S, Sohn JH, Foulks GN. Optimizing evaluation of lissamine green parameters for ocular surface staining. Eye (Lond). 2011;25(11):1429–1434. | ||
Berntsen DA, Mitchell GL, Nichols JJ. Reliability of grading lissamine green conjunctival staining. Cornea. 2006;25(6):695–700. | ||
Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650. | ||
Van Bijsterveld OP. Diagnostic tests in the sicca syndrome. Arch Ophthalmol. 1969;82:10–14. | ||
Savini G, Prabhawasat P, Kojima T, Grueterich M, Espana E, Goto E. The challenge of dry eye diagnosis. Clin Ophthalmol. 2008;2(1):31–55. | ||
Xu KP, Yagi Y, Toda I, Tsubota K. Tear function index: a new measure of dry eye. Arch Ophthalmol. 1995;113(1):84–88. | ||
Kaye SB, Sims G, Willoughby C, Field AE, Longman L, Brown MC. Modification of the tear function index and its use in the diagnosis of Sjogren’s syndrome. Br J Ophthalmol. 2001;85(2):193–199. | ||
Prabhasawat P, Tseng SC. Frequent association of delayed tear clearance in ocular irritation. Br J Ophthalmol. 1998;82(6):666–675. | ||
Afonso AA, Monroy D, Stern ME, Feuer WJ, Tseng SC, Pflugfelder SC. Correlation of tear fluorescein clearance and Schirmer test scores with ocular irritation symptoms. Ophthalmology. 1999;106(4):803–810. | ||
Lemp MA. Breakup of the tear film. Int Ophthalmol Clin. 1973;13(1):97–102. | ||
Lemp MA, Hamill JR. Factors affecting tear film breakup in normal eyes. Arch Ophthalmol. 1973;89(2):103–105. | ||
Norn MS. Desiccation of the precorneal film. I. Cornea wetting-time. Acta Ophthalmol (Copenh). 1969;47(4):865–880. | ||
Norn MS. Desiccation of the precorneal film. II. Permanent discontinuity and dellen. Acta Ophthalmol (Copenh). 1969;47(4):881–889. | ||
Vanley GT, Leopold IH, Gregg TH. Interpretation of tear film breakup. Arch Ophthalmol. 1977;95(3):445–448. | ||
Lin YY, Carrel H, Wang IJ, et al. Effect of tear film break-up on higher order aberrations of the anterior cornea in normal, dry, and post-LASIK eyes. J Refract Surg. 2005;21(5):S525–S529. | ||
Tsubota K, Nakamori K. Dry eyes and video display terminals. N Engl J Med. 1993;328(8):584. | ||
Rieger G. The importance of the precorneal tear film for the quality of optical imaging. Br J Ophthalmol. 1992;76(3):157–158. | ||
Goto E, Yagi Y, Matsumoto Y, et al. Impaired functional visual acuity of dry eye patients. Am J Ophthalmol. 2002;133(2):181–186. | ||
Ishida R, Kojima T, Dogru R, et al. The application of a new continuous functional visual acuity measurement system in dry eye syndromes. Am J Ophthalmol. 2005;139(2):253–258. | ||
Kaido M, Dogru M, Ishida R, Tsubota K. Concept of functional visual acuity and its application. Cornea. 2007;26(9 Suppl 1):S29–S35. | ||
Mainstone JC, Bruce AS, Golding TR. Tear meniscus measurement in the diagnosis of dry eye. Curr Eye Res. 1996;15(6):653–661. | ||
Guillon JP. Non-invasive Tearscope Plus routine for contact lens fitting. Cont Lens Anterior Eye. 1998;21 Suppl 1:S31–S40. | ||
Fodor E, Hagyó K, Resch M, Somodi D, Németh J. Comparison of Tearscope Plus versus slit lamp measurements of the inferior tear meniscus height in normal individuals. Eur J Ophthalmol. 2010;20(5):819–824. | ||
Lamberts DW, Foster CS, Perry HD. Schirmer test after topical anesthesia and the tear meniscus height in normal eyes. Arch Ophthalmol. 1979;97(6):1082–1085. | ||
Miller WL, Doughty MJ, Narayanan S, et al. A comparison of tear volume (by tear meniscus height and phenol red thread test) and tear fluid osmolality measures in non-lens wearers and in contact lens wearers. Eye Contact Lens. 2004;30(3):132–137. | ||
Savini G, Barboni P, Zanini M. Tear meniscus evaluation by optical coherence tomography. Ophthalmic Surg Lasers Imaging. 2006;37(2):112–118. | ||
Yokoi N, Bron A, Tiffany J, Brown N, Hsuan J, Fowler C. Reflective meniscometry: a non-invasive method to measure tear meniscus curvature. Br J Ophthalmol. 1999;83(1):92–97. | ||
Bandlitz S, Purslow C, Murphy PJ, Pult H. Comparison of a new portable digital meniscometer and optical coherence tomography in tear meniscus radius measurement. Acta Ophthalmol. October 7, 2013. [Epub ahead of print]. | ||
Bandlitz S, Purslow C, Murphy PJ, Pult H, Bron AJ. A new portable digital meniscometer. Optom Vis Sci. 2014;91(1):e1–e8. | ||
Chen F, Shen M, Chen W, et al. Tear meniscus volume in dry eye after punctal occlusion. Invest Ophthalmol Vis Sci. 2010;51(4):1965–1969. | ||
Nguyen P, Huang D, Li Y, et al. Correlation between optical coherence tomography-derived assessments of lower tear meniscus parameters and clinical features of dry eye disease. Cornea. 2012;31(6):680–685. | ||
Altan-Yaycioglu R, Sizmas S, Canan H, Coban-Karatas M. Optical coherence tomography for measuring the tear film meniscus: correlation with Schirmer test and tear-film breakup time. Curr Eye Res. 2013;38(7):736–742. | ||
Werkmeister RM, Alex A, Kaya S, et al. Measurement of tear film thickness using ultrahigh-resolution optical coherence tomography. Invest Ophthalmol Vis Sci. 2013;54(8):5578–5583. | ||
Garcia N, Teson M, Enriquez-de-Salamanca A, et al. Basal values, intra-day and inter-day variations in tear film osmolarity and tear fluorescein clearance. Curr Eye Res. January 8, 2014. [Epub ahead of print]. | ||
Kojima T, Ishida R, Dogru M, et al. A new noninvasive tear stability analysis system for the assessment of dry eyes. Invest Ophthalmol Vis Sci. 2004;45(5):1369–1374. | ||
Goto T, Zheng X, Klyce SD, et al. A new method for tear film stability analysis using videokeratography. Am J Ophthalmol. 2003;135(5):607–612. | ||
Montes-Mico R, Caliz A, Alio JL. Wavefront analysis of higher order aberrations in dry eye patients. J Refract Surg. 2004;20(3):243–247. | ||
Doane MG. An instrument for in vivo tear film interferometry. Optom Vis Sci. 1989;66(6):383–388. | ||
Blackie CA, Solomon JD, Scaffidi RC, Greiner JV, Lemp MA, Korb DR. The relationship between dry eye symptoms and lipid layer thickness. Cornea. 2009;28(7):789–794. | ||
Finis D, Pischel N, Schrader S, et al. Evaluation of lipid layer thickness measurement of the tear film as a diagnostic tool for Meibomian gland dysfunction. Cornea. 2013;32(12):1549–1553. | ||
Kent C. Dry-eye diagnosis: 21st-century tools. Review of Ophthalmology. October 2013. Available from: http://www.revophth.com/content/t/dry_eye/c/44198/.Accessed March 4, 2014. | ||
Gilbard JP, Farris RL, Santamaria J 2nd. Osmolarity of tear microvolumes in keratoconjunctivitis sicca. Arch Ophthalmol. 1978;96(4):677–681. | ||
Versura P, Campos EC. TearLab osmolarity system for diagnosing dry eye. Expert Rev Mol Diagn. 2013;13(2):119–129. | ||
Szalai E, Berta A, Szekanecz Z, Szucs G, Modis L Jr. Evaluation of tear osmolarity in non-Sjogren and Sjogren syndrome dry eye patients with the TearLab system. Cornea. 2012;31(8):867–871. | ||
Li M, Du C, Zhu D, Shen M, Cui L, Wang J. Daytime variations of tear osmolarity and tear meniscus volume. Eye Contact Lens. 2012;38(5):282–287. | ||
Tomlinson A, Khanal S, Ramaesh K, Diaper C, McFadyen A. Tear film osmolarity: determination of a referent for dry eye diagnosis. Invest Ophthalmol Vis Sci. 2006;47(10):4309–4315. | ||
TearLab. Reimbursement Support Center. Available from: http://www.tearlab.com/products/doctors/reim/reimsuptcenter.htm. Accessed March 4, 2014. | ||
Tomlinson A, McCann LC, Pearce EI. Comparison of human tear film osmolarity measured by electrical impedance and freezing point depression techniques. Cornea. 2010;29(9):1036–1041. | ||
Nilforoushan MR, Latkany RA, Speaker MG. Effect of artificial tears on visual acuity. Am J Ophthalmol. 2005;140(5):830–835. | ||
Latkany R, Lock BG, Speaker M. Tear film normalization test: a new diagnostic test for dry eyes. Cornea. 2006;25(10):1153–1157. | ||
Versura P, Bavelloni A, Grillini M, Fresina M, Campos EC. Diagnostic performance of a tear protein panel in early dry eye. Mol Vis. 2013;19:1247–1257. | ||
Ohashi Y, Ishida R, Kojima T, et al. Abnormal protein profiles in tears with dry eye syndrome. Am J Ophthalmol. 2003;136(2):291–299. | ||
Solomon A, Dursun D, Liu Z, Xie Y, Macri A, Pflugfelder SC. Pro- and anti-inflammatory forms of interleukin-1 in the tear fluid and conjunctiva of patients with dry-eye disease. Invest Ophthalmol Vis Sci. 2001;42(10):2283–2292. | ||
Tishler M, Yaron I, Geyer O, Shirazi I, Naftaliev E, Yaron M. Elevated tear interleukin-6 levels in patients with Sjögren syndrome. Ophthalmology. 1998;105(12):2327–2329. | ||
Jones DT, Monroy D, Ji Z, Atherton SS, Pflugfelder SC. Sjögren’s syndrome: cytokine and Epstein-Barr viral gene expression within the conjunctival epithelium. Invest Ophthalmol Vis Sci. 1994;35(9):3493–3504. | ||
Sambursky R, Davitt WF 3rd, Latkany R, et al. Sensitivity and specificity of a point-of-care matrix metalloproteinase 9 immunoassay for diagnosing inflammation related to dry eye. JAMA Ophthalmol. 2013;131(1):24–28. | ||
Huang JF, Zhang Y, Rittenhouse KD, Pickering EH, McDowell MT. Evaluations of tear protein markers in dry eye disease: repeatability of measurement and correlation with disease. Invest Ophthalmol Vis Sci. 2012;53(8):4556–4564. | ||
Fujishima H, Toda I, Shimazaki J, Tsubota K. Allergic conjunctivitis and dry eye. Br J Ophthalmol. 1996;80(11):994–997. | ||
Lee SY, Han SJ, Nam SM, et al. Analysis of tear cytokines and clinical correlations in Sjogren syndrome dry eye patients and non-Sjogren syndrome dry eye patients. Am J Ophthalmol. 2013;156(2):247–253. | ||
Shen L, Suresh L, Lindemann M, et al. Novel autoantibodies in Sjogren’s syndrome. Clin Immunol. 2012;145(3):251–255. | ||
Kamao T, Yamaguchi M, Kawasaki S, Mizoue S, Shiraishi A, Ohashi Y. Screening for dry eye with newly developed ocular surface thermographer. Am J Ophthalmol. 2011;151(5):782–791. | ||
Moussa S, Eppig T, Pattmoller J, et al. Diurnal and zonal analysis of corneal surface temperature in young healthy adults. Eur J Ophthalmol. 2013;23(5):641–645. | ||
Tomlinson A, Bron AJ, Korb DR, et al. The international workshop on meibomian gland dysfunction: report of the diagnosis subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):2006–2049. | ||
Chalmers RL, Begley CG. Dryness symptoms among an unselected clinical population with and without contact lens wear. Cont Lens Anterior Eye. 2006;29(1):25–30. | ||
Ngo W, Situ P, Keir N, Korb D, Blackie C, Simpson T. Psychometric properties and validation of the Standard Patient Evaluation Of Eye Dryness questionnaire. Cornea. 2013;3(9)2:1204–1210. | ||
Schiffman RH, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the Ocular Surface Disease Index. Arch Ophthalmol. 2000;118(5):615–621. | ||
Begley CG, Chalmers RL, Abetz L, et al. The relationship between habitual patient-reported symptoms and clinical signs among patients with dry eye of varying severity. Invest Ophthalmol Vis Sci. 2003;44(11):4753–4761. | ||
Mangione CM, Lee PP, Pitts J, Gutierrez P, Berry S, Hays RD; for the NEI-VFQ Field Test Investigators. Psychometric properties of the National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 1998;116(11):1496–1504. | ||
Abetz L, Rajagopalan K, Mertzanis P, Begley C, Barnes R, Chalmers R; for the Impact of Dry Eye on Everyday Life (IDEEL) Study Group. Health Qual Life Outcomes. 2011;9:111. | ||
Grubbs JR Jr, Tolleson-Rinehart S, Huynh K, Davis RM. A review of quality of life measures in dry eye questionnaires. Cornea. 2014;33(2):215–218. | ||
Latkany RL, Lock B, Speaker M. Nocturnal lagophthalmos: an overview and classification. Ocul Surf. 2006;4(1):44–53. | ||
Cardona G, García C, Serés C, Vilaseca M, Gispets J. Blink rate, blink amplitude, and tear film integrity during dynamic visual display terminal tasks. Curr Eye Res. 2011;36(3):190–197. | ||
Himebaugh NL, Begley CG, Bradley A, Wilkinson JA. Blinking and tear break-up during four visual tasks. Optom Vis Sci. 2009;86(2):E106–E114. | ||
Vehof J, Kozareva D, Hysi PG, et al. Relationship between dry eye symptoms and pain sensitivity. JAMA Ophthalmol. 2013;131(10):1304–1308. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.