")
Back to Journals » Cancer Management and Research » Volume 13
Diagnosis and Treatment of Renal Cell Carcinoma During Pregnancy
Received 20 October 2021
Accepted for publication 23 December 2021
Published 29 December 2021 Volume 2021:13 Pages 9423—9428
DOI https://doi.org/10.2147/CMAR.S345309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alexandra R. Fernandes
Hainan Xu,1 Shutao Tan2
1Department of Obstetrics and Gynecology, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China; 2Department of Urology, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Shutao Tan Tel +86 18940252862
Email [email protected]
Abstract: Renal cell carcinoma during pregnancy is extremely rare, but it is the commonest urological malignancy reported in pregnancy. Currently, no uniform domestic or international diagnostic or treatment criteria exist for these patients, so their diagnosis and treatment are challenging for urologists. The health and reproductive needs of these patients have improved in recent years because of the continuous development of medical technology. This article reviews the epidemiology, risk factors, diagnosis, treatment, and prognosis of renal cell carcinoma during pregnancy.
Keywords: pregnancy, renal cell carcinoma, diagnosis, treatment
Introduction
Renal cell carcinoma (RCC) is a malignant cancer of the kidney, and it has been rarely described in pregnant women. Regardless of whether it is a primary occurrence of cancer in a pregnant woman or an unexpected pregnancy during cancer treatment, the diagnosis and treatment of such patients can be difficult. Meanwhile, the treatment of malignant cancers during pregnancy and the fertility needs of patients with malignant cancers have received an increasing amount of attention. Surgical resection of the lesions is currently the primary treatment for RCC. Novel targeted drugs have proven efficacious in patients with metastatic RCC, but there have been few studies on the safety of these treatments for the fetus. This article reviews the epidemiology, risk factors, diagnosis, treatment, and prognosis of RCC during pregnancy, with the aim of providing better diagnosis and treatment strategies. A MEDLINE search of the peer reviewed literature on diagnosis and case reports of RCC during pregnancy, published in English, was done through March 1, 2021 using the words: “renal cancer”, “pregnancy”, “gestation”, “diagnosis”, “treatment”, and “management”. A total of 109 documented cases of all renal malignancies during pregnancy were evaluated for this review (Table 1).
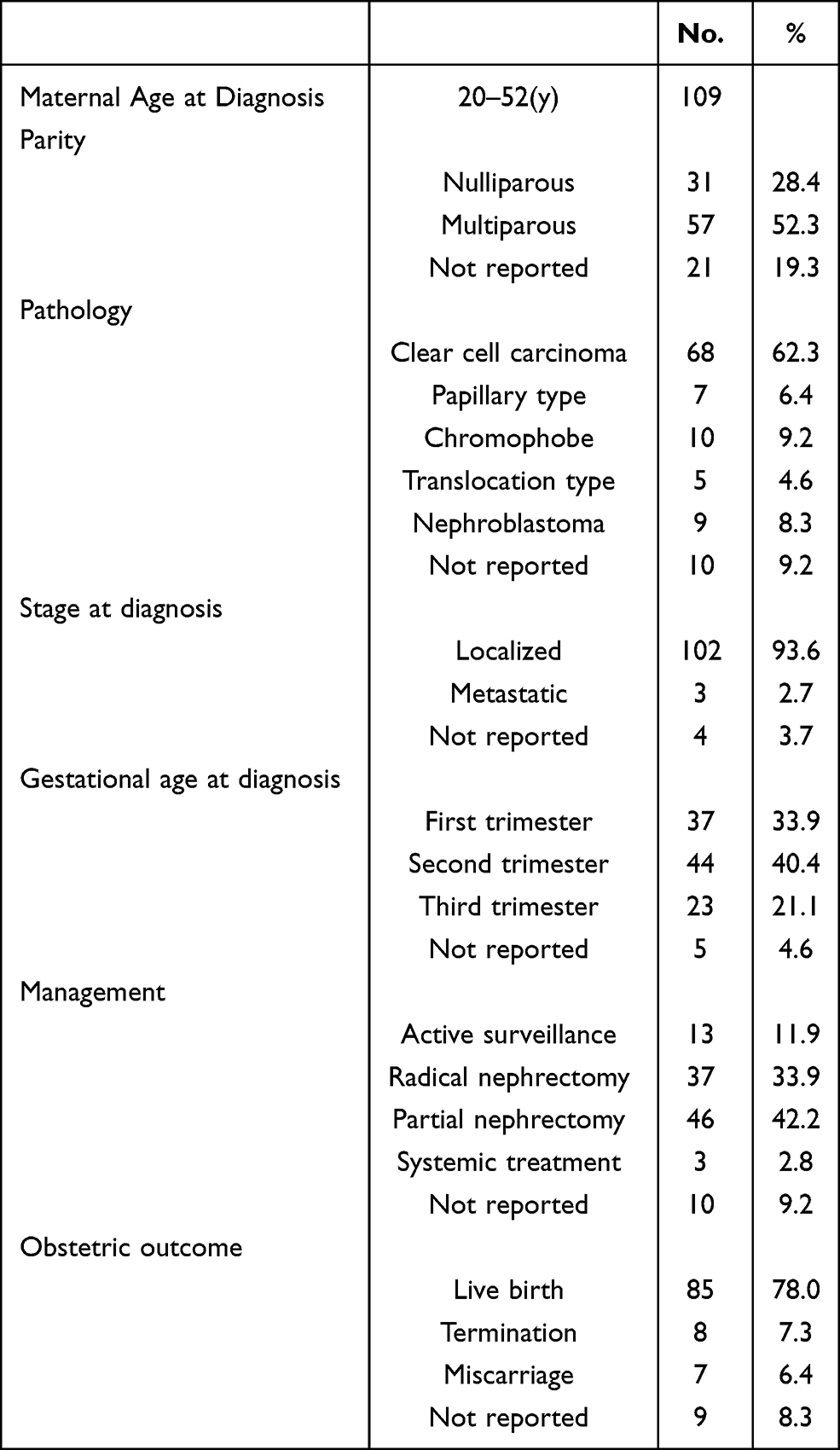 |
Table 1 Characteristics of Patients with RCC During Pregnancy |
Epidemiology and Risk Factors
RCC accounts for approximately 3% of malignant cancers in adults, with a male-to-female ratio of 2:1.1 Malignant cancers during pregnancy are rare, with approximately 1 in 1000 pregnant women diagnosed with cancer before delivery.2 The most common tumors diagnosed during pregnancy are breast cancer, melanoma, cervical cancer, and lymphomas. Urinary tract cancers during pregnancy are even rarer, and RCC is the most common urinary tract malignancy during pregnancy.3
Obesity, smoking, analgesics, environmental factors, hypertension, diabetes, chronic kidney diseases, and reproductive and hormonal factors are established risk factors for RCC.4 During pregnancy, estrogen and progesterone reach to a high peak. High parity (≥5 pregnancies lasting for more than 4 months) was associated with almost doubling of risk for RCC in comparison with nulliparous women. A meta-analysis including 14 studies (5 cohort studies, one nested case control, and 8 case control studies) that were published in 2013 concluded that ever parity, ie with a history of at least one pregnancy and increased parity numbers are associated with an increased risk of kidney cancer.5 However, the correlation between hormonal factors and the development of RCC during pregnancy and its underlying mechanisms are not fully understood.
Clinical Presentation
RCC during pregnancy is usually discovered incidentally during prenatal check-ups. To date, the primary clinical symptoms are pain (50%), hematuria (47%), hypertension (18%), and the classic triad (back pain, mass, hematuria) (26%)6 Other rare clinical manifestations include hemolytic anemia, hypercalcemia, and tumor rupture. The clinical manifestations of RCC during pregnancy are atypical because common complications of pregnancy, such as abdominal pain, abdominal distension, and urinary tract irritation, as well as the patient’s increasing abdominal circumference, can easily obscure these clinical manifestations.
Diagnosis
There are three main difficulties in the diagnosis of RCC during pregnancy: 1) the clinical symptoms are atypical; 2) auxiliary examination methods are limited; and 3) diagnosis causes significant mental stress to the patient and family members. The ionizing radiation from radiography and computed tomography (CT) examinations may cause fetal congenital malformations, central nervous system damage, intrauterine growth restriction, or stillbirth. Therefore, such examinations should be avoided in early pregnancy.7 For pregnant patients who must undergo these imaging examinations, the radiation dose should be <0.1 Gy, and the examination should be conducted with the abdomen shielded to ensure the fetus is safe.8 CT and magnetic resonance imaging (MRI) are the preferred imaging examinations for diagnosing RCC. Clinically the safest imaging examinations during pregnancy are ultrasonography and MRI.7 Ultrasonography is often used for routine prenatal examinations. The ultrasonography and CT detection rates for renal tumors ≥3 cm in diameter are similar, but the sensitivity of ultrasonography for tumors <3 cm or small lesions that do not change the contour of the kidney is significantly lower than that of CT.9 MRI can accurately identify the size, location, and progression of the tumor, and its diagnostic accuracy for RCC is the same as that of CT.10
It is generally believed that imaging examination is sufficient for diagnostic confirmation, so preoperative biopsy of lesions among pregnant patients is rarely reported in the literature.6 Preoperative histological examination can significantly increase the diagnostic accuracy and guide adjuvant treatment decisions.11 A small renal mass is not always a cancer. If we cannot tell it is benignant or malignant, biopsy is needed. In other cases, biopsy of suspected lesions is an option for patients with unclear tumor tissue origin, local ablative therapies (ie radiofrequency ablation and cryosurgery), patients with a solitary kidney, and patients with metastatic disease before initiating targeted therapies.12
Treatment
RCC during pregnancy is extremely rare, and no uniform treatment standard exists. We should make a treatment plan based on the guidelines and the actual situation of the patient. However, surgical resection of the lesion is still the primary treatment option for these patients. Some patients with a small renal mass may not undergo surgery temporarily and try active surveillance. Ethical concerns should be the first consideration in the treatment process. Some researchers generally consider the treatment of the pregnant woman as the focus, not only addressing potential physiological problems but also providing psychological counseling, followed by ensuring the normal development and health of the fetus.11 Standardized guidelines for management are unavailable due to the rarity of this diagnosis and the decision is individualized for each case, putting in consideration the welfare of mother and fetus. In addition, given the complex physiological and pathological conditions of RCC during pregnancy, a multidisciplinary team of urologists, obstetricians, anesthesiologists, radiologists, pediatricians, psychologists, and genetic counselors should be involved in the treatment and consultation of these patients to achieve the best possible outcome.11 Further, an individualized treatment plan should be formulated based on the clinical manifestations, gestational age, tumor site and stage, whether complications are present, and the wishes of the patient and family members. Full communication with the patient and family is necessary when time-limited surgery, watchful waiting, or termination of pregnancy are considered.13
Timing of Surgery
Currently, termination of pregnancy is generally not recommended for pregnant RCC patients and should only be extremely carefully considered in patients with metastatic tumors whose body cannot continue to tolerate the pregnancy.14 The patient’s general condition, gestational age, tumor size and progression, and the status of fetal development are the primary factors guiding the timing of surgery.6
Many researchers believe that RCC resection can be performed in the early, middle, and late stages of pregnancy, although the consensus is that early pregnancy is the safest time for surgery.15 There is still controversy as to whether surgery should be performed in the second trimester. Some researchers recommend that surgical operation may cause uterine contraction and miscarriage and that hypotension caused by intraoperative blood loss may cause fetal hypoxia and recommend that operation be postponed until 32 weeks of gestation or even after delivery due to improved fetal lung development and maturity.16 However, others believe that the difficulty of surgical intervention gradually increases with uterine size and that surgery during the second trimester is safe and feasible.17 Therefore, surgical treatment of RCC in the second trimester requires a comprehensive assessment of the impact of invasive surgery on the mother and fetus and the risk of delayed surgery.18
If RCC is found in the third trimester, the timing of surgery is relatively simple. First, if tumor progression is limited, watchful waiting until surgical treatment 1 week after delivery is appropriate.19 Second, if the patient has a strong desire for treatment or has other organ dysfunctions, surgical treatment can be performed after inducing delivery. Fetal lung is mature after gestational week 32. Then early delivery followed by kidney surgery or systemic therapy for metastatic disease is an option.11,16 If RCC is found close to the expected date of delivery, surgical treatment can be delayed until the expected date of delivery, and cesarean section and radical nephrectomy can be performed simultaneously.20
Because the doubling time of RCC is relatively slow (300–500 days),21 the growth rate is 0.4 cm/year on average within T1 stage,22 so watchful waiting depending on physical condition and disease progression is recommended for patients in whom surgery would be difficult or who are concerned about the safety of the fetus. In addition, treatment after delivery is also a feasible treatment plan.4
Selection of Surgical Procedure
Some researchers recommend that laparoscopic surgery should be avoided during pregnancy because of concerns about uterine injury, miscarriage, malformations, premature delivery, hypercapnia, and other surgical complications.23 However, laparoscopic surgery and robot-assisted laparoscopic surgery are becoming more common with improvements in surgical technologies.24 With respect to the impact on pregnant women, laparoscopic surgery has advantages over open surgery in terms of average hospital stay, administration of antispasmodic drugs, postoperative pain, and intestinal recovery time.25 Further, there is no statistically significant difference in gestational age, birth weight, or Apgar score in women undergoing these two surgical techniques.
Laparoscopic radical nephrectomy and nephron-sparing surgery have become common procedures for the treatment of RCC during pregnancy, but there are still differences of opinion regarding the optimal treatment approach. In the transabdominal approach, the operation space is large, but because the intestine is compressed by the enlarged uterus, the kidney and renal pedicle are not well exposed, and there is greater irritation of the uterus.26,27 This method is appropriate for tumors of the anterior and lateral kidney. Conversely, in the retroperitoneal approach, the operation space is narrow, but the kidney and renal blood vessels are directly exposed, there is little irritation of the uterus, and there is little impact on the patient’s systemic circulation.17,23 This method is often performed for tumors of the posterior, posteromedial, or posterolateral kidney. As few cases have been described, it is not yet possible to compare the specific effects of the two approaches, so the selection of approach depends on the operator’s experience with laparoscopic surgery, the size of the uterus, and the location and size of the kidney tumor.27 For the right (left) kidney masses, placing the patient in a left (right) lateral decubitus position will shift the uterus off the vena cava, improving venous return and cardiac output. Surgery during pregnancy requires maintenance of stable maternal hemodynamic parameters to provide adequate uteroplacental circulation, and avoidance of preterm labor.
Several precautions for laparoscopic surgery in the treatment of RCC during pregnancy must be kept in mind. First, to avoid uterine damage and reduce uterine irritation, the Hasson technique is the most reliable for placing the first laparoscopic trocar with an open field of view. The position of each cannula should be moved upward in the abdomen corresponding to increases in the uterine volume.27 Second, intra-abdominal pressure should be maintained at <12 mmHg. Excessive intra-abdominal pressure will cause the cardiac index to decrease and the systemic vascular resistance to increase, which can result in increased intrauterine pressure and decreased uteroplacental perfusion.24 Last, in order to prevent hypercapnia, hyperventilation of the patient during anesthesia is recommended to maintain end-tidal CO2 at a concentration of ≤35 mmHg.28
Treatment of Metastatic RCC
Current first-line treatment strategies for metastatic RCC are immune checkpoint inhibitors based combination therapies. The combination of pembrolizumab and axitinib as well as nivolumab and ipilimumab is the standard of care in all risk groups. Alternatives are VEGFR-TKIs when immune checkpoint inhibitors are not available or contra-indicated.29 The safety of these drugs during pregnancy is poorly studied; However, there have been few studies on the safety of these drugs during pregnancy; data are available only from animal studies.30 The United States Food and Drug Administration lists these drugs as Class D drugs that should be avoided during pregnancy.6 Therefore, systemic treatment is not recommended after radical tumor resection for pregnant RCC patients who do not have metastasis, whereas systemic treatment can be considered after termination of pregnancy for patients with distant metastases.
Prognosis
Most pregnant RCC patients have a good prognosis and can deliver healthy newborns. Moreover, stage of patients who are diagnosed with RCC during pregnancy is significantly lower than that of common patients with RCC.6 This may be related to tumors being found earlier at regular physical examinations during pregnancy. However, there have been no relevant reports on the prognosis of pregnant patients with metastatic RCC.
Conclusion
Pregnant RCC patients are a unique population in which the safety of the fetus must be considered in addition to the condition of the patient. No uniform domestic or international diagnostic or treatment criteria exist, so these patients require a multidisciplinary team for diagnosis, treatment, and comprehensive clinical management. Moreover, an individualized treatment plan should be formulated based on the patient’s condition and the development of the fetus. Currently, laparoscopic radical nephrectomy or nephron-sparing surgery are the primary treatment for RCC during pregnancy. Although laparoscopic surgery has many advantages over open surgery, there are details that require careful consideration by the surgeon. Targeted drug therapy is recommended for metastatic RCC, but it should be avoided during pregnancy and lactation. Currently, the overall prognosis of these patients is good, but further investigation of specific pathogenic mechanisms and safer anticancer drugs is still necessary to reduce the risk to the pregnant RCC patient and the fetus.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82103679) and the 345 Talent Project of Shengjing Hospital of China Medical University (Grant No. M0339).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Maggen C, Linssen J, Gziri MM, et al. Renal and bladder cancer during pregnancy: a review of 47 cases and literature-based recommendations for management. Urology. 2021;151:118–128. doi:10.1016/j.urology.2020.08.084
2. Maggen C, Wolters VERA, Cardonick E, et al. Pregnancy and cancer: the INCIP Project. Curr Oncol Rep. 2020;22:17. doi:10.1007/s11912-020-0862-7
3. Pavlidis N. Cancer and pregnancy: what should we know about the management with systemic treatment of pregnant women with cancer. Eur J Cancer. 2011;47(Suppl 3):S348–352. doi:10.1016/S0959-8049(11)70199-X
4. Yilmaz E, Oguz F, Tuncay G, et al. Renal cell carcinoma diagnosed during pregnancy: a case report and literature review. J Int Med Res. 2018;46:3422–3426. doi:10.1177/0300060518776744
5. Guan HB, Wu QJ, Gong TT. Parity and kidney cancer risk: evidence from epidemiologic studies. Cancer Epidemiol Biomarkers Prev. 2013;22:2345–2353. doi:10.1158/1055-9965.EPI-13-0759-T
6. Khaled H, Lahloubi NA, Rashad N. Review on renal cell carcinoma and pregnancy: a challenging situation. J Adv Res. 2016;7:575–580. doi:10.1016/j.jare.2016.03.007
7. Jain C. ACOG Committee Opinion No. 723: guidelines for diagnostic imaging during pregnancy and lactation. Obstet Gynecol. 2019;133:186. doi:10.1097/AOG.0000000000003049
8. Saltybaeva N, Platon A, Poletti PA, et al. Radiation dose to the fetus from computed tomography of pregnant patients-development and validation of a web-based tool. Invest Radiol. 2020;55(12):762–768. doi:10.1097/RLI.0000000000000701
9. Guo F, Hu B, Chen L, et al. Clinical application of contrast-enhanced ultrasound after percutaneous renal tumor ablation. Br J Radiol. 2019;92(1103):20190183. doi:10.1259/bjr.20190183
10. Chu JS, Wang ZJ. Protocol optimization for renal mass detection and characterization. Radiol Clin North Am. 2020;58(5):851–873. doi:10.1016/j.rcl.2020.05.003
11. Chys B, Dumont S, Van Calsteren K, et al. Renal neoplasm during pregnancy: a single center experience. Clin Genitourin Cancer. 2018;16:e501–e507. doi:10.1016/j.clgc.2018.02.018
12. Muglia VF, Prando A. Renal cell carcinoma: histological classification and correlation with imaging findings. Radiol Bras. 2015;48:166–174. doi:10.1590/0100-3984.2013.1927
13. Boere I, Lok C, Vandenbroucke T, et al. Cancer in pregnancy: safety and efficacy of systemic therapies. Curr Opin Oncol. 2017;29:328–334. doi:10.1097/CCO.0000000000000386
14. David RA, Idowu B, Akindiose C, et al. Peculiarities and management challenges of advanced renal cell carcinoma incidentally discovered in pregnancy. Clin Case Rep. 2018;6:863–866. doi:10.1002/ccr3.1485
15. Balinskaite V, Bottle A, Sodhi V, et al. The risk of adverse pregnancy outcomes following nonobstetric surgery during pregnancy: estimates from a retrospective cohort study of 6.5 million pregnancies. Ann Surg. 2017;266:260–266. doi:10.1097/SLA.0000000000001976
16. Tiang KW, Ng KL, Vega-Vega A, et al. Rapidly enlarging renal tumor during pregnancy: diagnostic and management dilemma. J Kidney Cancer VHL. 2014;1:12–16. doi:10.15586/jkcvhl.2014.6
17. Petrut B, Hogea M, Tat T, et al. Literature review on the feasibility of laparoscopic partial nephrectomy for renal cancer during pregnancy: a propos of a case. J BUON. 2018;23:872–876.
18. Bettez M, Carmel M, Temmar R, et al. Fatal fast-growing renal cell carcinoma during pregnancy. J Obstet Gynaecol Can. 2011;33:258–261. doi:10.1016/S1701-2163(16)34827-7
19. Yin L, Zhang D, Teng J, et al. Retroperitoneal laparoscopic radical nephrectomy for renal cell carcinoma during pregnancy. Urol Int. 2013;90(4):487–489. doi:10.1159/000346334
20. Pertia A, Gagua D, Managadze L, et al. Treatment of renal cell carcinoma in pregnancy: simultaneous nephron-sparing surgery and Caesarian section (case report). Georgian Med News. 2011;201:7–10.
21. Kay K, Dolcy K, Bies R, et al. Estimation of solid tumor doubling times from progression-free survival plots using a novel statistical approach. AAPS J. 2019;21(2):27. doi:10.1208/s12248-019-0302-5
22. Lee SW, Sung HH, Jeon HG, et al. Size and volumetric growth kinetics of renal masses in patients with renal cell carcinoma. Urology. 2016;90:119–124. doi:10.1016/j.urology.2015.10.051
23. Akin Y, Ciftci H, Karahan MA, et al. Laparoscopic retroperitoneal radical nephrectomy in a pregnant woman with retrocaval artery. Int Urol Nephrol. 2015;47:469–471. doi:10.1007/s11255-014-0906-8
24. Ramirez D, Maurice MJ, Seager C, et al. Robotic partial nephrectomy during pregnancy: case report and special considerations. Urology. 2016;92:1–5. doi:10.1016/j.urology.2015.11.037
25. O’Shea M. Nonobstetric surgery during pregnancy. Obstet Gynecol. 2018;132:1506. doi:10.1097/AOG.0000000000002993
26. Fan X, Xu K, Lin T, et al. Comparison of transperitoneal and retroperitoneal laparoscopic nephrectomy for renal cell carcinoma: a systematic review and meta-analysis. BJU Int. 2013;111:611–621. doi:10.1111/j.1464-410X.2012.11598.x
27. Dell’Atti L, Borghi C, Galosi AB. Laparoscopic approach in management of renal cell carcinoma during pregnancy: state of the art. Clin Genitourin Cancer. 2019;17:e822–e830. doi:10.1016/j.clgc.2019.05.025
28. Brandon MT, Sarah SM, Rachael MP, et al. Diagnosis and management of obesity hypoventilation syndrome during labor. Case Rep Anesthesiol. 2021;2021:8096212. doi:10.1155/2021/8096212
29. Goebell PJ, Ivanyi P, Bedke J, et al. Consensus paper: current state of first- and second-line therapy in advanced clear-cell renal cell carcinoma. Future Oncol. 2020;16(29):2307–2328. doi:10.2217/fon-2020-0403
30. Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27:v58–v68. doi:10.1093/annonc/mdw328
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.