")
Back to Journals » Journal of Pain Research » Volume 15
Diagnosis and Treatment of Five Pain-Related Conditions in Urban China: A Population-Based Cross-Sectional National Health and Wellness Survey
Authors Fan B, Li S , Wu B , Zhang J , Zhou J
Received 2 September 2021
Accepted for publication 13 June 2022
Published 23 June 2022 Volume 2022:15 Pages 1787—1796
DOI https://doi.org/10.2147/JPR.S333590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 7
Editor who approved publication: Professor Krishnan Chakravarthy
Bifa Fan,1 Shuiqing Li,2 Baishan Wu,3 Jinghua Zhang,4 Jing Zhou5
1Department of Pain, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 2Department of Pain, Peking University Third Hospital, Beijing, People’s Republic of China; 3Department of Pain, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Department of Pain, Dongfang Hospital of Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 5KANTAR China, Beijing, People’s Republic of China
Correspondence: Bifa Fan, Department of Pain, China-Japan Friendship Hospital, 2 Yinghua East Road, Chaoyang District, Beijing, People’s Republic of China, Tel +86 15010101616, Email [email protected]
Background: While there is an extensive body of research regarding pain and its treatment in developed countries, little research on this topic has been performed in developing countries. This study aimed to investigate the diagnosis, treatment, and treatment satisfaction in individuals with pain in urban China using real-world data.
Methods: All respondents from the 2013, 2015, and 2017 China National Health and Wellness Survey were included in the analysis and were classified into diagnosed and undiagnosed groups according to their self-reported physician diagnosis or experience in the past month. The following five categories of pain were analysed: headache, cancer-associated pain, musculoskeletal pain, neuropathic pain, and fibromyalgia. Rates for diagnosis, treatment, and satisfaction with medication were calculated overall and for each pain type.
Results: A total of 3802 respondents reported experience of at least one type of pain in the past month. Among those, 61.2% were diagnosed with a pain-related condition, the majority of which (84.0%) were receiving treatment. For diagnosed respondents taking over-the-counter and/or prescription medication, 70.3% were satisfied with their treatment. Comparing between pain types, the diagnosis rates for cancer-associated pain (32.7%) and fibromyalgia (22.8%) were relatively low, whereas respondents with musculoskeletal pain has the highest diagnosis rate (61.1%). Respondents with cancer-associated pain had the lowest satisfaction (30.0%) with over-the-counter and prescription medication, while respondents with headache (76.2%) had the highest satisfaction rate with such medications.
Conclusion: Our study highlights the importance of raising awareness for pain management as well as education and training for healthcare providers and patients.
Keywords: pain management, diagnosis, treatment, treatment satisfaction, China
Introduction
Pain is one of the most common reasons for seeking medical care and has been linked to impairments in daily activities, reduced quality of life,1 psychological comorbidities,2 and substantial personal and societal economic burden.3 The prevalence of pain has been reported to be as high as 24% globally,4 and rates between 25.8% to 45.9% have been reported in China, depending on the type of pain and population investigated.5–8
Numerous pain relief treatments are available and the selection of appropriate pain management depends on the intensity, duration, and mechanism of the pain. The pharmacological management of pain comprises analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, anti-depressants and anti-convulsants.9 Non-pharmacological treatment includes surgery and physical or psychological therapy.9 Additionally, traditional Chinese medicine (TCM) is a widely used option in China and encompasses both pharmacological treatments based on herbal medicine and non-pharmacological treatments such as acupuncture and spinal manipulation.10 Due to the complexity of pain, any one treatment is rarely adequate to provide lasting and meaningful pain reduction on its own. Thus, a multimodal treatment strategy offers patients the best possibility for improvement.11
Despite the wide array of treatments available, unrelieved or poorly controlled pain remains a pressing global health issue.12 Poor pain management exacerbates patients’ conditions resulting in consequences for both the individual and the healthcare services.13 Lack of sufficient education of both healthcare providers and patients has been reported as one of the leading obstacles preventing proper pain management.12,14 In this regard, a recent survey of chronic pain in China reported that 24.1% of respondents had never gone to hospital for pain-related symptoms and 36.8% had never received treatment for their pain, owing largely to their perception that chronic pain was not harmful.15
While there is an extensive body of research investigating pain and its treatment in developed countries, only limited studies have been performed in Asia and specifically in China. To address this issue, this study aimed to investigate the diagnosis, treatment, and treatment satisfaction in individuals with pain in urban China using real-world data. The study focused on five categories of pain: headache, cancer-associated pain, musculoskeletal pain, neuropathic pain, and fibromyalgia.
Methods
Data Source
Data were obtained from the 2013, 2015, and 2017 China National Health and Wellness Survey (NHWS) which is a sample of 64,991 adults (18+ years). The NHWS is an annual, self-administered, internet-based survey managed by Kantar Health. The survey is provided in the Chinese language and is completed nationwide by residents in urban settlements. The survey has been shown to provide reliable results in the Chinese population.16 The sample is stratified by gender, age, and region to represent the demographic composition of the urban adult population in China. Representativeness of the data has been validated and weighted against the official Chinese Statistical Yearbook. The questionnaire for the NHWS were approved by the Pearl Institutional Review Board (Indianapolis, USA). All individuals who completed the survey provided informed consent.
Potential respondents to the NHWS were identified through an existing web-based consumer panel, Lightspeed Research (LSR). Panel members explicitly agreed to join the LSR panel and received periodic invitations to participate in online surveys (not just health related). Members of the panel were recruited through a variety of means including co-registration with other internet panels, e-newsletter campaigns, and banner placements. Respondents were selected using a quota sampling framework based on age and gender.
Respondent Groups
Respondents were classified into two groups according to their self-reported physician diagnosis or experience: 1) diagnosed group, respondents who have experienced pain in the past month and have a diagnosis of the corresponding pain-related disease, and 2) undiagnosed group, respondents who experienced pain in the past month but do not have a diagnosis of the corresponding pain-related disease. Undiagnosed respondents who may or may not have sought a diagnosis from a physician.
Pain Categorization
Five types of pain were analyzed separately in this study, 1) headache (migraine or headache), 2) cancer-associated pain, 3) musculoskeletal pain (arthritis or joint pain [including bursitis, knee, foot, but not shoulder, hip or neck], or lower back pain [lumbar area]), 4) neuropathic pain (neuropathic pain, or phantom limb pain [neuropathic pain following amputation], post herpetic neuralgia, spinal disk [ruptured/herniated/bulging/degenerative]), and 5) fibromyalgia.
Demographics and Health Characteristics
Respondents reported sociodemographic information including age, sex, marital status, employment status, education, and health insurance. General health characteristics included exercise behavior, alcohol use, self-reported pain severity, and body mass index (BMI). All respondents were requested to report whether they had a physician diagnosis of any disease. This information was used to examine the Charlson Comorbidity Index (CCI).17 CCI was derived by weighting the presence of the following conditions (self-reported diagnosis) and summing the result (see Supplementary Table S1): Human immunodeficiency virus/acquired immunodeficiency syndrome, metastatic tumor, lymphoma, leukemia, any tumor, moderate/severe renal disease, mild liver disease, ulcer disease, connective tissue disease, chronic pulmonary disease, dementia, cerebrovascular disease, peripheral vascular disease, myocardial infarction, congestive heart failure, and diabetes with end organ damage. A score of zero would indicate that no comorbidities were identified. The greater the total index score, the greater the comorbid burden on the respondent.
Respondents with a diagnosed pain condition were asked whether they were currently undergoing treatment for their condition, and if yes, to specify the treatment type(s). Response choices included self-administered and non-self-administered treatments. Self-administered treatments included over the counter (OTC) medication, prescription medication, and/or TCM oral remedies. Non-self-administered treatment included steroid injections, surgery, physical therapy, electrical stimulation, ultrasound, spinal simulation, and/or alternative medicine approaches such as herbal therapy, aromatherapy, biofeedback, hypnosis, etc.
The satisfaction rates of respondents with a diagnosed pain condition and who were currently taking OTC and/or prescription medication were assessed. Satisfaction related to the overall experience a respondent had with a medication. A respondent’s satisfaction for each medication treatment was obtained using a self-reported satisfaction score on a scale of 1 to 7 (ie, 1 = extremely dissatisfied, 2 = very dissatisfied, 3 = somewhat dissatisfied, 4 = neither dissatisfied nor satisfied, 5 = somewhat satisfied, 6 = very satisfied, 7 = extremely satisfied). For each medication, reported scores < 5 were considered as unsatisfied, and scores ≥ 5 or above were considered as satisfied. If taking multiple medications, respondents were classified as satisfied with their overall medication if the number of satisfactory medications was greater than the number of unsatisfactory medications. Respondents were classified as unsatisfied with their overall medication if the number of satisfactory medications was equal to or less than the number of unsatisfactory medications.
Statistical Analysis
Descriptive analyses were used for sociodemographic measures, diagnosis rate, treatment rate, and satisfaction rate for each type of pain. The diagnosis rate was defined as the percentage of participants who were diagnosed with a pain-related condition relative to all those who experienced pain in the past month (ie, both undiagnosed and diagnosed). The treatment rate was calculated as the percentage of diagnosed respondents who received treatment. The satisfaction rate of medication was calculated as the percentage of diagnosed respondents who were satisfied with overall medications among those taking OTC and/or prescription medication.
Independent samples t-tests and chi-square tests were performed between comparison groups for continuous variables and categorical variables, respectively, to understand the baseline differences between the groups in terms of demographic and general health characteristics.
For all analyses, p-values <0.05 were considered statistically significant. All statistical analyses were performed using SPSS Version 18 or Version 20.
Results
Diagnosis Rate
Out of 64,991 respondents, a total of 3802 respondents reported experiencing at least one type of pain in the past month. Among those, 2326 (61.2%) were diagnosed with a pain-related condition by physician. Figure 1 shows the diagnosis rate by pain type. The lowest diagnosis rates were observed for fibromyalgia (22.8%) and cancer-associated pain (32.7%). Respondents with musculoskeletal pain had the highest diagnosis rate (61.1%), and just over half of respondents who reported experiencing neuropathic pain or headache were diagnosed.
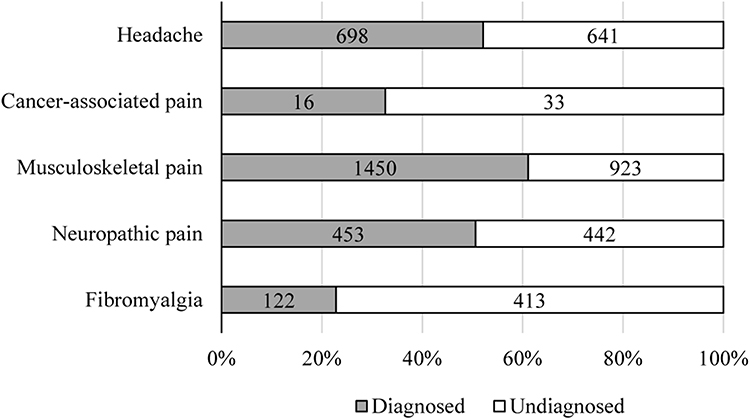 |
Figure 1 Diagnosis rates across pain types. |
Tables 1 and 2 show the health and social characteristics of respondents. Over all pain types, diagnosed respondents were older than undiagnosed respondents, and more diagnosed respondents were married or living with a partner. Diagnosis was significantly associated with higher CCI scores, with the exception of neuropathic pain, where undiagnosed and diagnosed respondents had the same score. With the exception of cancer-associated pain, significantly more diagnosed than undiagnosed respondents described their pain as severe. A clear association between diagnosis and exercise was not observed. For headache and musculoskeletal pain, significantly more diagnosed than undiagnosed respondents exercised. However, the converse was observed for cancer-associated pain and neuropathic pain. For musculoskeletal and neuropathic pain, significantly more undiagnosed than diagnosed respondents were obese.
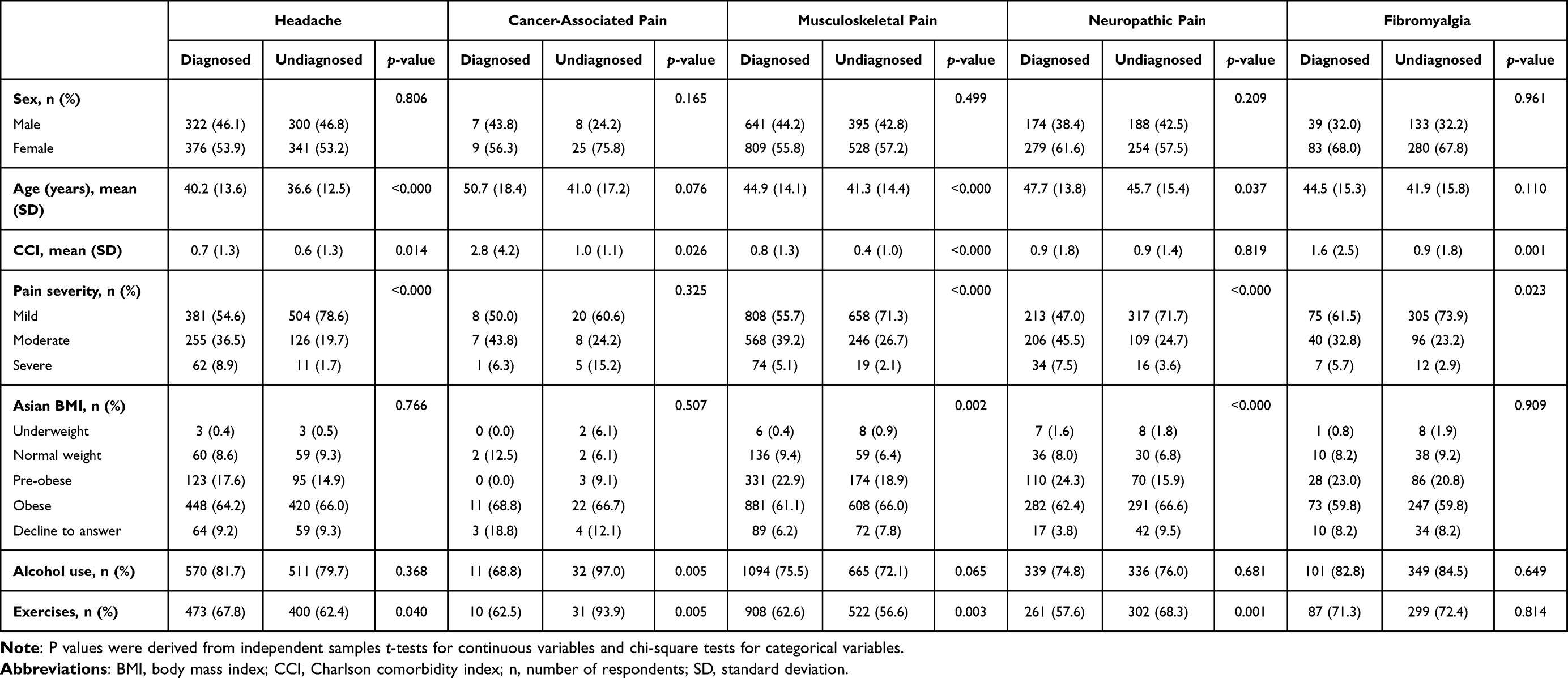 |
Table 1 Health Characteristics for Diagnosed and Undiagnosed Respondents Across Pain Types |
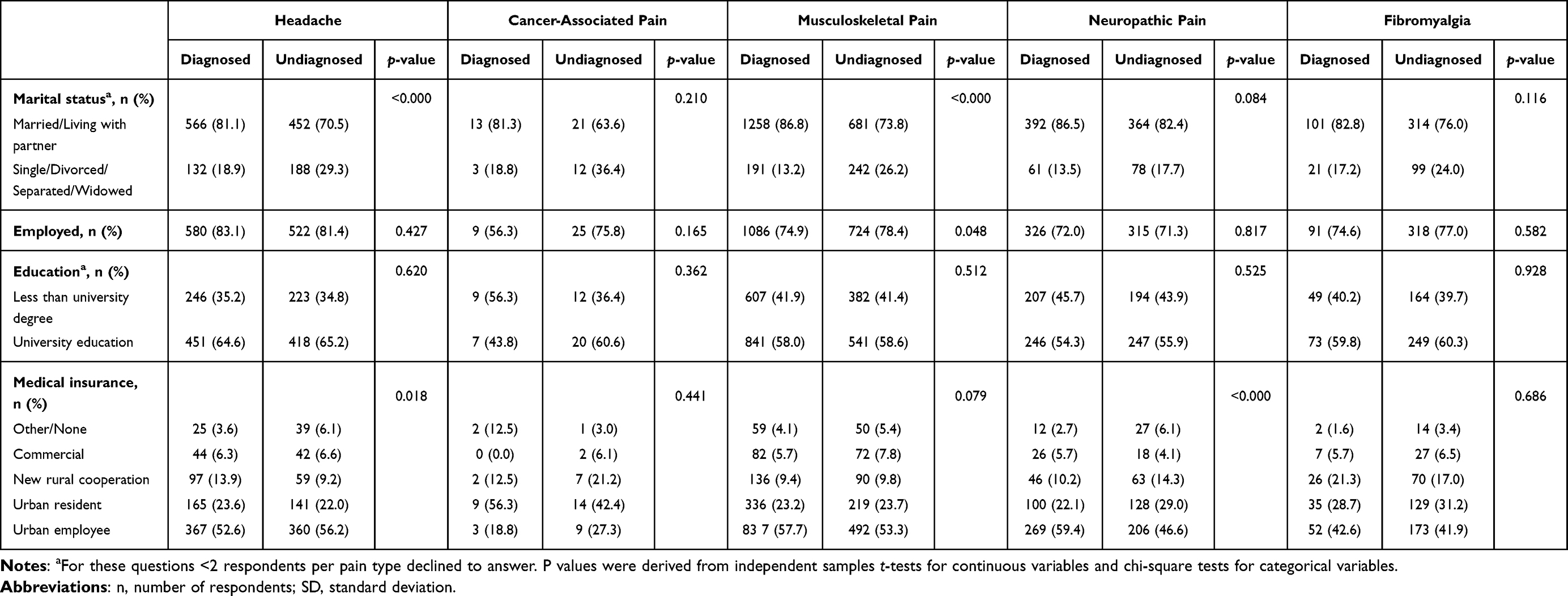 |
Table 2 Social Characteristicsfor Diagnosed and Undiagnosed Respondents Across Pain Types |
Treatment Rate
Out of the diagnosed respondents, 1953 (84.0%) were receiving treatment for their pain. The treatment rate for each pain type is shown in Figure 2. The rate of non-self-administered treatment ranged from 64.6% for headache to 87.5% for cancer-associated pain. The overall rate of self-administered treatment, incorporating OTC, prescription medication and oral TCM, was 67.5%, ranging from 65.1% for musculoskeletal pain to 93.8% for cancer-associated pain. Each self-administered treatment was also analyzed individually. The overall rate of OTC medication was 35.7%, and was the highest for cancer-associated pain (56.3%), followed by headache (40.4%), with the other pain types having similar rates. The overall rate of prescription medication was 27.8%. Only a small percentage of respondents with cancer-associated pain (6.3%) were taking prescription medication. For the remaining pain types, the treatment rate of prescription medication ranged from 25.6% for neuropathic pain to 34.2% for headache. Treatment with oral TCM was most common among respondents with cancer-associated pain (50.0%) and fibromyalgia (44.3%), and least common for musculoskeletal pain (29.4%).
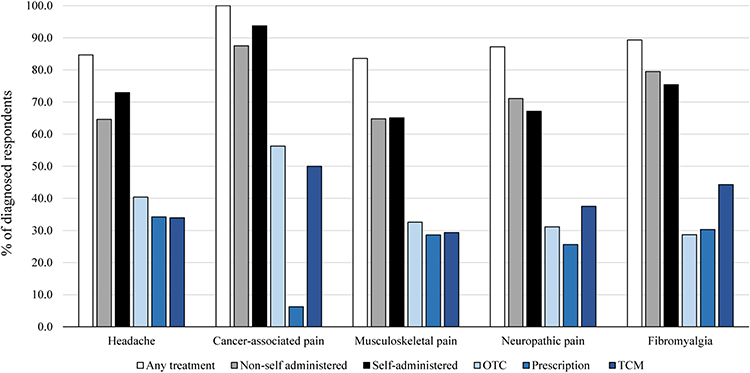 |
Figure 2 Treatment rates among diagnosed respondents across pain types. |
In comparison to respondents not taking medication (OTC/prescription/oral TCM), a greater number of respondents treated with medication had severe pain for the pain types of headache (10.6% vs 4.2%, p<0.000), musculoskeletal pain (5.9% vs 3.6%, p<0.000), and neuropathic pain (9.5% vs 3.4%, p=0.005). Furthermore, for these pain types, more respondents taking medication consumed alcohol: headache (83.9% vs 75.7%, p=0.013), musculoskeletal pain (77.7% vs 71.3%, p=0.008), and neuropathic pain (79.9% vs 64.4, p<0.000). Although the same trend was observed for treated respondents with fibromyalgia, it was not statistically significant. Respondents taking medication for musculoskeletal pain were also more likely to be employed (76.9% vs 71.2%, p=0.016), to exercise (65.4% vs 57.5%, p<0.000), and had higher CCI scores (0.9 vs 0.6, p<0.000) than those not taking medication.
Considering the low number of untreated respondents with cancer-associated pain (n=1), statistical testing was not performed. The complete results of bivariate analysis can be found in Supplementary Table S2. Additionally, bivariate analysis of demographic and clinical characteristics between treated and untreated respondents with any kind of treatment can be found in Supplementary Table S3 and described in Supplementary Results section.
Satisfaction Rate
Of the 1240 diagnosed respondents taking OTC and/or prescription medication, 872 (70.3%) were satisfied with their treatment. Satisfaction rates for each pain type are shown in Figure 3. Satisfaction rates of OTC and/or prescription medication were lowest for cancer-associated pain (30.0%) and highest for headache (76.2%).
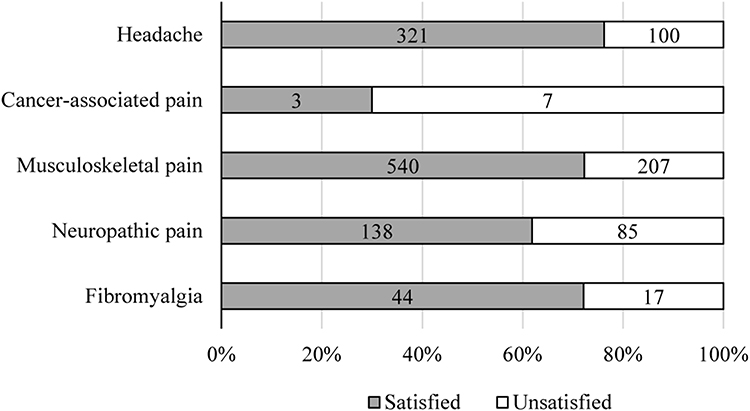 |
Figure 3 Satisfaction rates of medication (OTC and/or prescription) among diagnosed respondents, across pain types. |
For headache, more respondents who were satisfied with OTC and/or prescription medications, were older (41.5 years vs 38.7 years, p=0.070), married or living with partner (86.6% vs 74.0%, p=0.003), currently consumed alcohol (86.3% vs 77.0%, p=0.027), currently exercised (71.7% vs 57.0%, p=0.006), and had urban employee medical insurance (58.9% vs 43.0%, p=0.005) compared to those unsatisfied with such medications. For musculoskeletal pain, a greater proportion of those respondents who were satisfied with OTC and/or prescription medications were married or living with partner than patient who were unsatisfied with their treatment (92.2% vs 81.6%, p<0.000). For neuropathic pain, respondents who were satisfied with OTC and/or prescription medications were more frequently male (39.9% vs 25.9%, p=0.033), and currently employed (83.3% vs 65.9%, p=0.003) compared with respondents who were unsatisfied with such medications.
There were no significant differences between respondents regarding medication satisfaction in terms of demographic and clinical characteristics for cancer-associated pain and fibromyalgia. The complete results of covariate analysis can be found in Supplemental Table S4.
Discussion
This study aimed to investigate the diagnosis, treatment, and treatment satisfaction in individuals with pain in urban China using real-world data. Diagnosed respondents were generally older, with higher CCI scores and a greater percentage reporting severe pain than undiagnosed respondents. The highest diagnosis rates were observed for musculoskeletal pain, headache, and neuropathic pain. In these pain types, taking medication was associated with severe pain, and among those taking medication, the majority (>60%) were satisfied. While these rates are favourable, the diagnosis of headache and neuropathic pain could be improved. Given the association of diagnosis with greater pain intensity, undiagnosed respondents may consider that medical attention is not necessary for mild pain, or their pain may have gone undiagnosed due its mild nature. In any case, patients and healthcare providers should be educated to encourage the recognition of even mild pain so that it can be properly managed.
The diagnosis rates for cancer-associated pain (32.7%) and fibromyalgia (22.8%) were relatively poor. The low diagnosis rate of cancer-associated pain is somewhat surprising as previous survey studies in China have found that the majority of physicians frequently screen their cancer patients for pain using a standardized pain scale.18,19 Considering that opioids are the recommended treatment for moderate to severe cancer pain, it is noteworthy that respondents with cancer pain had the lowest treatment rate for prescription medication. Numerous studies in China have reported that physicians and cancer patients are reluctant to prescribe/take opioids due to fears over opioid addiction and adverse effects.18–20 The greater reliance on OTC medication in the current sample is likely a contributor to the low satisfaction rate observed for respondents with cancer-associated pain. Although NSAIDs and analgesics that are available OTC are used in the management of cancer-associated pain, when taken on their own, they are recommended to treat mild pain only, and are more frequently used as adjuvants to opioid treatment.21,22 In the current study, the low satisfaction rate with “Western” medication may partly account for the high treatment rate with oral TCM in respondents with cancer-associated pain. The lower satisfaction rate of cancer treatment could also be explained with the clinical perspectives on cancer. The pathologic and neurologic mechanisms of cancer pain is complicated such as cancer-induced pain often involves background pain, spontaneous pain and incidence or movement-evoked pain.23–25 Also, the side effects, cost, and long period of cancer treatment can influence patients’ therapeutic adhesion and satisfaction.26,27
Due to the diversity of symptoms and phenotypes, the diagnosis of fibromyalgia can be difficult,28 and a survey of Chinese patients with fibromyalgia reported that most patients were diagnosed about two years after symptom onset.29 Previous studies in China have shown that nearly 30% of rheumatologists believed that fibromyalgia was only a psychological disorder, less than 20% of rheumatologists have ever knowingly treated a patient with fibromyalgia, and nearly 80% stated they had difficulties in treating fibromyalgia patients.30 These findings suggest that physicians often miss the diagnosis of fibromyalgia in part due to lack of knowledge about the disease.
Limitations
Limitations of the current study include that data from the China NHWS is cross-sectional and mainly answered by respondents with internet access who were also subscribed members of a web-based consumer panel. Thus, while the NHWS is broadly representative of the Chinese urban adult population, the extent to which study respondents are representative of the larger population is unknown. Respondents self-reported all data in the NHWS, and verification of these data could not be performed and recall bias could not be excluded. Furthermore, the reliance on self-reported data likely underestimates conditions defined by clinical measures that the patient may not be aware of (eg, neuropathic pain and fibromyalgia).
Conclusion
In conclusion, the current study found variations in diagnosis, treatment, and satisfaction rates among different types of pain and has particularly highlighted the need to improve disease awareness and diagnosis for fibromyalgia and cancer pain. In addition, the prescription medication rate is low and satisfaction rate of treatment for complex pain, such as cancer pain, still needs to be improved. This study highlights the importance of raising awareness for pain management and further education for healthcare providers and patients.
Abbreviations
BMI, body mass index; CCI, Charlson comorbidity index; LSR, lightspeed research; n, number of respondents; NHWS, National Health and Wellness Survey; NSAIDs, nonsteroidal anti-inflammatory drugs; OTC, over-the-counter; SD, standard deviation; TCM, traditional Chinese medicine.
Significance
This article provides important information regarding diagnosis and treatment of five types of pain conditions in urban China. This research can be used to inform public health policy regarding pain conditions.
Data Sharing Statement
Data are available on reasonable request.
Ethics Approval and Informed Consent
The 2017 and 2015 National Health and Wellness Survey (NHWS) was approved by the Pearl Pathways Institutional Review Board (Indianapolis, Indiana, USA; 2017 NHWS: Protocol #17-KANT-147; 2015 NHWS: Protocol #15-KAN-121), while the 2013 NHWS was approved by Essex Institutional Review Board (Lebanon, NJ, USA; 2013 NHWS: Protocol# KH-NHWS-CH2012-3895). All respondents provided informed consent prior to participating.
Consent for Publication
The authors confirm and provide consent for the contents in this article to be published.
Acknowledgment
The authors acknowledge Dr. Ann-Marie Waldron, on behalf of Kantar Health, for her assistance with medical writing.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All authors have no conflicts of interest in relation to this work to declare.
References
1. Dueñas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457–467. doi:10.2147/JPR.S105892
2. Hooten WM. Chronic pain and mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin Proc. 2016;91(7):955–970. doi:10.1016/j.mayocp.2016.04.029
3. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
4. Mansfield KE, Sim J, Jordan JL, Jordan KP. A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain. 2016;157(1):55–64. doi:10.1097/j.pain.0000000000000314
5. Chen B, Li L, Donovan C, et al. Prevalence and characteristics of chronic body pain in China: a national study. SpringerPlus. 2016;5(1):938. doi:10.1186/s40064-016-2581-y
6. Chung JWY, Wong TKS. prevalence of pain in a community population. Pain Med. 2007;8(3):235–242. doi:10.1111/j.1526-4637.2006.00205.x
7. Jackson T, Chen H, Iezzi T, Yee M, Chen F. Prevalence and correlates of chronic pain in a random population study of adults in Chongqing, China. Clin J Pain. 2014;30(4):346–352. doi:10.1097/AJP.0b013e31829ea1e3
8. Qiu Y, Li H, Yang Z, et al. The prevalence and economic burden of pain on middle-aged and elderly Chinese people: results from the China health and retirement longitudinal study. BMC Health Serv Res. 2020;20(1):600. doi:10.1186/s12913-020-05461-6
9. Tompkins DA, Hobelmann JG, Compton P. Providing chronic pain management in the “Fifth Vital Sign” era: historical and treatment perspectives on a modern-day medical dilemma. Drug Alcohol Depend. 2017;173(Suppl 1):S11–S21. doi:10.1016/j.drugalcdep.2016.12.002
10. Manheimer E, Wieland S, Kimbrough E, Cheng K, Berman B. Evidence from the Cochrane collaboration for traditional Chinese medicine therapies. J Altern Complement Med. 2009;15(9):1001–1014. doi:10.1089/acm.2008.0414
11. Dale R, Stacey B. Multimodal treatment of chronic pain. Med Clin. 2016;100(1):55–64. doi:10.1016/j.mcna.2015.08.012
12. Bond M. Pain education issues in developing countries and responses to them by the International Association for the study of pain. Pain Res Manag. 2011;16(6):404–406. doi:10.1155/2011/654746
13. Sinatra R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010;11(12):1859–1871. doi:10.1111/j.1526-4637.2010.00983.x
14. Cogan J, Ouimette MF, Vargas-Schaffer G, Yegin Z, Deschamps A, Denault A. Patient attitudes and beliefs regarding pain medication after cardiac surgery: barriers to adequate pain management. Pain Manag Nurs. 2014;15(3):574–579. doi:10.1016/j.pmn.2013.01.003
15. Yongjun Z, Tingjie Z, Xiaoqiu Y, et al. A survey of chronic pain in China. Libyan J Med. 2020;15(1):1730550. doi:10.1080/19932820.2020.1730550
16. DiBonaventura MD, Liu GG, Stankus A. PRM12 evidence for validity of a national patient-reported survey in China: the China national health and wellness survey. Value Health. 2012;15(7):A647. doi:10.1016/j.jval.2012.08.263
17. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
18. Xia Z. Cancer pain management in China: current status and practice implications based on the ACHEON survey. J Pain Res. 2017;10:1943–1952. doi:10.2147/JPR.S128533
19. Zhang Q, Yu C, Feng S, et al. Physicians’ practice, attitudes toward, and knowledge of cancer pain management in China. Pain Med. 2015;16(11):2195–2203. doi:10.1111/pme.12819
20. Yanjun S, Changli W, Ling W, et al. A survey on physician knowledge and attitudes towards clinical use of morphine for cancer pain treatment in China. Support Care Cancer. 2010;18(11):1455–1460. doi:10.1007/s00520-009-0768-2
21. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13(2):e58–e68. doi:10.1016/S1470-2045(12)70040-2
22. Jost L, Roila F. Management of cancer pain: ESMO clinical recommendations. Ann Oncol. 2009;20:iv170–iv173. doi:10.1093/annonc/mdp164
23. Caraceni A, Portenoy RK. An international survey of cancer pain characteristics and syndromes. IASP task force on cancer pain. International Association for the study of pain. Pain. 1999;82(3):263–274. doi:10.1016/s0304-3959(99)00073-1
24. Svendsen KB, Andersen S, Arnason S, et al. Breakthrough pain in malignant and non-malignant diseases: a review of prevalence, characteristics and mechanisms. Eur J Pain. 2005;9(2):195–206. doi:10.1016/j.ejpain.2004.06.001
25. Zeppetella G. Impact and management of breakthrough pain in cancer. Curr Opin Support Palliat Care. 2009;3(1):1–6. doi:10.1097/SPC.0b013e3283260658
26. EL Marnissi B, Abbass F, Charaka H, et al. Evaluation of cancer patient satisfaction: a transversal study in radiotherapy department, Hassan II University Hospital, Fez, Morocco. Adv Public Health. 2019;2019:6430608. doi:10.1155/2019/6430608
27. Schmidt BL, Hamamoto DT, Simone DA, Wilcox GL. Mechanism of cancer pain. Mol Interv. 2010;10(3):164–178. doi:10.1124/mi.10.3.7
28. Bidari A, Ghavidel Parsa B, Ghalehbaghi B. Challenges in fibromyalgia diagnosis: from meaning of symptoms to fibromyalgia labeling. Korean J Pain. 2018;31(3):147–154. doi:10.3344/kjp.2018.31.3.147
29. Zhang Y, Liang D, Jiang R, et al. Clinical, psychological features and quality of life of fibromyalgia patients: a cross-sectional study of Chinese sample. Clin Rheumatol. 2018;37(2):527–537. doi:10.1007/s10067-017-3872-6
30. Mu R, Li C, Zhu J-X, et al. National survey of knowledge, attitude and practice of fibromyalgia among rheumatologists in China. Int J Rheum Dis. 2013;16(3):258–263. doi:10.1111/1756-185X.12055
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.