")
Back to Journals » Open Access Emergency Medicine » Volume 14
Diagnosis and Management of Pediatric Ovarian Torsion in the Emergency Department: Current Insights
Authors Scheier E
Received 7 April 2022
Accepted for publication 17 June 2022
Published 23 June 2022 Volume 2022:14 Pages 283—291
DOI https://doi.org/10.2147/OAEM.S342725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Eric Scheier1,2
1Pediatric Emergency Department, Kaplan Medical Center, Rehovot, Israel; 2Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel
Correspondence: Eric Scheier, Pediatric Emergency Department, Kaplan Medical Center, 1 Pasternak Street, Rehovot, 7661041, Israel, Tel +972 8 944-1275, Fax +972 8 944-1276, Email [email protected]
Abstract: Ovarian torsion is defined as twisting of the ovary around an axis consisting of its vascular pedicle, the infundibulopelvic ligament and the tubo-ovarian ligament, and can occur in females of any age. Torsion can be a result of ovarian mass causing asymmetry and subsequent torsion, or can be spontaneous. While ovarian torsion is a surgical emergency, early diagnosis and treatment can preserve ovarian viability even if necrosis is seen operatively. Presentation classically involves sudden onset severe abdominal pain and vomiting but diagnostic delay can follow subtler presentations. Diagnosis is most commonly based on sonographic findings, but advanced imaging such as CT or MRI may be required if sonography is not diagnostic. Treatment is surgical, with ovarian preservation preferred in almost all cases. In this review, I present the most recent evidence on epidemiology, diagnosis, and management of pediatric ovarian torsion, with a focus on point-of-care ultrasound for the emergency care provider.
Keywords: point-of-care, POCUS, adnexal, ovary
Introduction
Ovarian torsion occurs most frequently during the neonatal period and during adolescence with a mean age of 14.5 years,1 although several series report younger average ages.2–5 Ovarian torsion has an incidence of 4.9 per 100,000 children,1 and up to 4% of PED visits for acute abdominal pain in females are due to ovarian torsion.6 In neonates, ovarian torsion may be asymptomatic representing antenatal torsion.7 In infants, the location of the torsed ovary may be in an inguinal hernia sac (Figure 1).8 In children over a year of age, ovarian torsion comprises 1.3% of acute surgical diagnoses.9
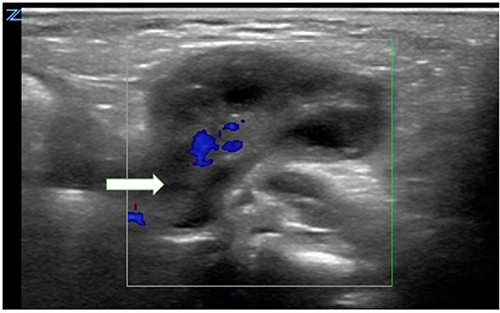 |
Figure 1 An inguinal ovarian hernia. This is a transverse view with a linear high-frequency probe in sagittal orientation over the left inguinal area. The ovarian stalk (arrow) is seen to communicate with the abdomen. Color flow can be seen in the center of the ovary. The ovary is not edematous and is without secondary signs of ischemia such as surrounding free fluid. |
The presentation of ovarian torsion can be non-classic, and diagnostic delay is common. In one series, 38% of premenarchal girls and 20% of postmenarchal girls experienced delay in diagnosis ranging from 12 hours to 4 days,6 with premenarchal girls significantly more likely to have a missed diagnosis on initial evaluation.2 Ovarian necrosis can occur after as little
7 as 10 hours of abdominal pain and in the series authored by Prieto et al 34% of premenarchal and 17% of postmenarchal girls were found to have necrosis of the affected ovary at the time of surgery.6 The time from patient presentation with ovarian torsion to surgery ranges from an average of 16 hours to a median of 101 hours.10–12 While the incidence of pediatric ovarian torsion is similar to that of pediatric testicular torsion, the rate of oophorectomy is approximately one and a half times that of orchiectomy.13 Just as evaluation of abdominal pain in a male requires examination of testes, evaluation of abdominal pain in a female requires consideration of ovarian torsion in the differential diagnosis.
Clinical Presentation
Torsion classically presents with sudden onset abdominal pain and vomiting. In one series, 41% of patients with ovarian torsion presented to the PED after two days of abdominal pain, and 33% presented with a visual analog scale (VAS) of 6 or lower. There, three patients who were discharged from the PED the day prior suffered ovarian loss.10 A second series reported that only 51% of premenarchal and 41% of postmenarchal patients presented with non-severe pain, and that pain was present for two days or more in 47% of premenarchal and 52% of postmenarchal patients.11 In a majority of patients, pain is intermittent.14 Constipation or dysuria can be presenting signs of torsion in 7.8% and 5.8%, respectively.2 While one series found fever to be present in 7.3% of pediatric OT,15 a more recent series of 193 cases of ovarian torsion, fever was not found in a single case.14
Laboratory Evaluation
There is no laboratory profile that can predict adnexal torsion. Pyuria can be associated with ovarian torsion.16 There may be mild leukocytosis and elevated CRP.2,17 Leukocytosis has been postulated to result from cortisol release resulting from ovarian ischemia.18 Both leukocytosis and elevated CRP are associated with ovarian ischemia.19
Diagnostic Imaging
The first-line imaging modality in the diagnosis of ovarian torsion is ultrasound.20 Ultrasound has been shown to have higher sensitivity to CT for ovarian torsion without exposure to ionizing radiation.21 A recent meta-analysis showed ultrasound to have a pooled sensitivity of 0.79 and a specificity of 0.76, compared to MRI at 0.81 and 0.91, respectively.22 MRI is the preferred modality to image an ovarian mass that has resulted in torsion, and can be performed after detorsion.23
More recently, contrast-enhanced sonography has been explored as an improved diagnostic modality.24 Machine-learning as well has been applied to develop sonographic algorithms in the identification of ovarian torsion, with a sensitivity of approximately 95% and specificity of 92%.25 Cases with equivocal findings on imaging may require diagnostic laparoscopy.26
Point-of-Care Ultrasound
While ultrasound is traditionally performed by trained sonographers, more recent literature supports POCUS as a diagnostic screening tool in the evaluation of potential ovarian torsion. ACEP 2016 Emergency US Guidelines lists POCUS for adnexal pathology as an Adjunct or Emerging rather than Core POCUS application.27 POCUS for adnexal pathology, using both transabdominal and intracavitary views, in an adult ED resulted in LOS 162 minutes less than those who received radiology performed ultrasound, with no alternative diagnoses in a two-week follow-up period.28 A recent study of adult ED patients examined with point-of-care transvaginal sonography demonstrated that in 79% of patients both ovaries were visualized and that POCUS led to changes in plan in 43% of patients, with a similarly decreased LOS.29 Literature on pediatric ovarian torsion diagnosed with POCUS is currently limited to case reports and a case series.21,30–32
Evaluation of the ovaries and uterus in the pediatric patient is performed with a low-frequency curvilinear probe placed transabdominally, just above the pubic symphysis. A full bladder is helpful to fully image the uterus/ovaries in the transabdominal view (Figure 2). Fanning in transverse and sagittal orientations brings pelvic structures into view. In the transverse orientation, it is often helpful to rock the probe away from the ovary under examination (ie, rock away from the probe indicator to improve the view of the right ovary) using the bladder as an acoustic window between the probe and the ovary. Non-virginal females can be offered the option of transvaginal sonography which increases the quality of the images without requiring a full bladder. However, transvaginal sonography is generally not available as a point of care examination in the PED and will therefore not be further discussed in this review.
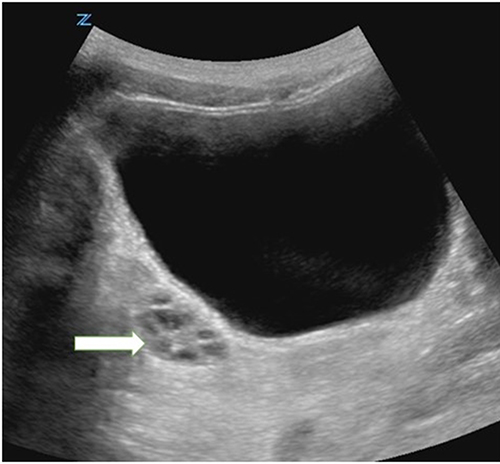 |
Figure 2 Transverse view with a curvilinear low-frequency probe. A normal right ovary (arrow) is seen beneath the full bladder. |
An ovarian diameter over four centimeters has been reported to be the most sensitive marker of torsion, with a majority of torsed ovaries presenting in a medial location (Figure 3).33 In an adult ED, sensitivity, specificity of three centimeter mean ovarian diameters were 100% and 30% (Figure 4) and for five centimeter mean ovarian diameter 91% and 92%.34 Ovarian asymmetry can be the first clue of ovarian torsion, with a 50% increase in ovarian volume compared to the unaffected side highly specific for ovarian torsion in premenarchal girls.35 A recent series of pediatric patients found a median 5.57X difference in volume between affected and unaffected ovaries.14
 |
Figure 3 A torsed ovary in a medial location. Transverse view with a curvilinear low-frequency probe. A hyperechoic torsed right ovary (arrow) is seen close to midline beneath the full bladder. |
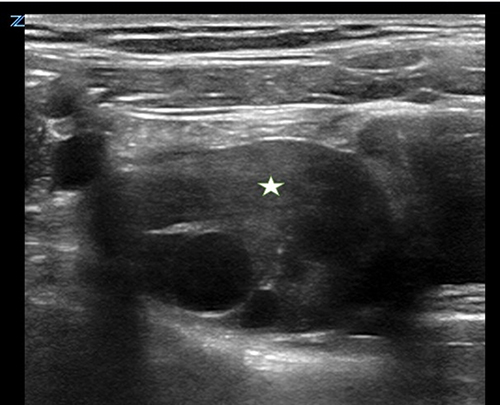 |
Figure 4 Enlarged ovary (star) without secondary signs of torsion. This is a transverse view with a linear high-frequency probe. This ovary was found in an 11-year-old right presenting with ipsilateral lower abdominal pain. The diameter measured 3.6 centimeters. It lacks increased echogenicity indicative of edema, perifollicular enhancement. Gynecology evaluation found normal blood flow to the ovary. |
Venous congestion and ischemia lead to edema and hemorrhage, causing increased echogenicity in the torsed ovary when compared with the healthy ovary. The follicular ring sign, indicating perifollicular edema, is an early indication of torsion and can be seen in 74% of cases (Figure 5).36 The affected ovary may have peripherally located follicles, but this is not specific for torsion and can be found bilaterally in polycystic ovaries, without signs of edema.37 Similarly, medial location of the ovary is found in 1.2% of females without torsion and free fluid in the pelvis is frequently found in females without torsion.25 In a torsed ovary, medial location of the ovary and uterine deviation toward the affected ovary are due to mass effect.23 The most specific sign of torsion, the whirlpool sign indicating twisted vasculature, is infrequently identified even by experienced sonographers.16 The “double bladder” sign characterizes a large, anechoic ovarian cyst that may be mistaken for bladder (Figure 6).38 This cyst is associated with a medially located, enlarged, torsed ovary and is not bordered posteriorly by uterus.
 |
Figure 5 A torsed ovary with perifollicular edema. This is a sagittal view with a curvilinear low frequency probe of a torsed ovary in an 8-year-old. The ovary (star) is located to the left of the hypoechoic bladder. Perifollicular edema is represented by a hyperechoic ring (arrow) on the right side of the ovary. |
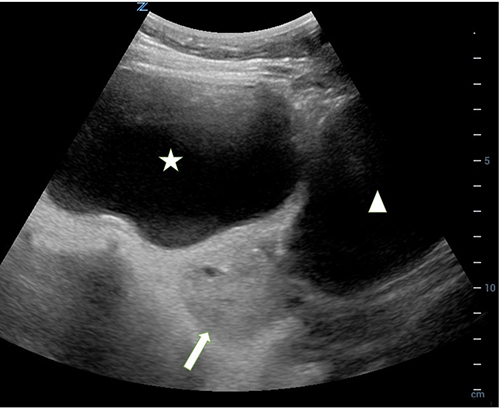 |
Figure 6 The double bubble sign. Transverse suprapubic view with a low frequency probe. The hyperechoic torsed ovary (arrow) sits between the bladder to the left (star) and the large ovarian cyst to the right (triangle). |
Presence of follicle peripheralization and the presence of free fluid in the abdomen on ultrasound are predictors of a higher degree of torsion in children.39 In girls undergoing surgical treatment of paraovarian cysts, torsion was frequently found, with no difference in rate of preoperative sonographic detection of paraovarian cysts, or mean cyst diameter between children with and without torsion.40 Therefore, POCUS must assess the need for further or expedited gynecological evaluation.
There is controversy regarding the utility of Doppler flow in the evaluation of ovarian torsion, as absence of flow may be due to sonographer inexperience or young patient age. The ovary has a dual blood supply and presence of flow to an edematous ovary can be seen in early or incomplete torsion and a torsed ovary can present with normal arterial flow in almost one-third of cases.14,35,41,42 Prieto et al report that only 38% of torsed ovaries were found to have lack of Doppler flow.6
While absence of an enlarged ovary without a full bladder has been suggested to exclude ovarian torsion,43 bowel gas can obscure the torsed ovary32 and a rapid intravenous fluid bolus prior to sonography can increase diagnostic accuracy.
A hemorrhagic corpus luteum ovarian cyst, occurring after ovulation, can present similarly to ovarian torsion44 and can be similar to torsion on sonography (Figures 7 and 8). Isolated torsion of the fallopian tube is a rare entity in children and can present sonographically with normal ovaries and a paraovarian mass representing fallopian tube enlargement along with free intraperitoneal fluid.45
 |
Figure 7 Involuting corpus luteum. This ovary (arrow) was seen in a 14-year-old with ipsilateral lower abdominal pain, and was thought on POCUS to be torsed despite the presence of flow and isoechogenicity with the unaffected ovary. The structure demonstrated asymmetry in size when compared with the unaffected ovary, peripheralized follicles (arrowheads), and surrounding free fluid (triangle). |
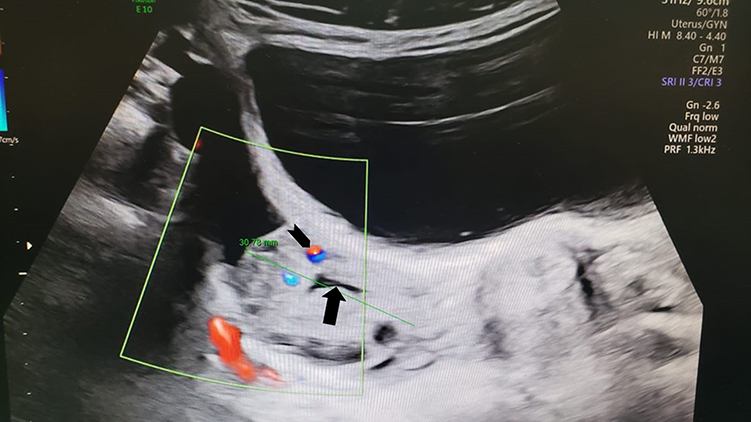 |
Figure 8 Involuting corpus luteum. On gynecology evaluation of the patient presented in Figure 7, a hypoechoic linear structure (involuting fibrin core, arrow) in the presence of low-resistance blood flow (arrowhead) was suggestive of involuting corpus luteum rather than torsion, as was the patient’s quick resolution of abdominal pain. |
Management
Through the first decade of the 21st century, oophorectomy was performed on pediatric patients with torsion in 78% of cases in the United States, and a majority of cases in France and Canada.3,4,46 From 2012 to 2017, pediatric oophorectomy rates in the United States dropped from 36% to 18%.47
In contrast to ovarian torsion in the adult population, malignant masses are rarely associated with pediatric ovarian torsion, and ovarian salvage is generally preferred to oophorectomy. 0.4% to 1.4% of pediatric ovarian torsion is associated with malignancy.1,5 The majority of paraovarian masses are comprised of benign mass or cyst. Prieto et al describe a mass or cyst in 18 of 32 cases of ovarian torsion and Ashwal et al report that 41% of premenarchal torsion was associated with a benign mass or cyst.6,12 Due to hormonal influences, enlarged functional cysts cause torsion almost exclusively in post-menarchal patients.
Ovarian neoplasm greater than five centimeters in diameter is associated with a two times increased likelihood of ovarian torsion. However, the rates of malignancy are lower in those with mass and torsion.48
Literature shows a high rate of follicle development in salvaged ovaries, with one series demonstrating preservation of normal anatomy and folliculogenesis in all 42 torsed ovaries within 12 weeks of detorsion. In a second series, 74% of pediatric patients had follicles visualized at a median of 18.7 weeks after detorsion, with an oophorectomy rate of 2%.13,49 Cystectomy at the time of detorsion is not shown to have an effect on the post-operative sonographic morphology of the affected ovary.50
Torsion of an ovary with underlying mass has been shown to have a better prognosis than torsion of an otherwise healthy ovary and postpubescent torsion is more likely than prepubescent torsion to be associated with an ovarian mass.51 Some suggest that diagnostic delay associated with prepubescent torsion, together with a less favorable prepubertal hormonal profile may make prepubescent torsion more susceptible to ovarian atrophy.51 Pediatric patients are found to have multiple twists in the adnexa in 43% of cases, indicating a high level of chronicity or recurrence of torsion. In that study, 22.7% of patients were found to have between 24 hours and four weeks of abdominal pain, and 44% had multiple discrete episodes of pain.44
Asynchronous bilateral torsion is a rare entity in children, having been reported only 30 times in the literature.52 History of prior torsion is a risk factor for subsequent ipsilateral or contralateral torsion, and some authors suggest that oophoropexy should be considered in all cases of pediatric torsion.53 The overall rate of recurrent torsion is 0.2% with no difference seen between ovarian preservation surgery and oophorectomy.54 The strongest indication for oophoropexy is a normal ovary on intraoperative inspection, as this suggests a long infundibulopelvic or tubo-ovarian ligament and significantly increased risk of recurrence.23
While some studies have shown a difference in management between pediatric surgery and between gynecology,4,47,55 a recent study suggests that there may not be a difference in the rates of oophoropexy, cystectomy, oophorectomy, and intra-operative time whether managed by pediatric surgery or by gynecology.56
Conclusion
Pediatric ovarian torsion is a surgical emergency that can occur at any age, and diagnostic delay can threaten viability of the ovary and fertility. Ovarian torsion may present with non-severe abdominal pain or with pain that is intermittent or subacute and therefore the physician must have a high index of suspicion for this diagnosis. POCUS is an invaluable tool that can assist the physician to assess the risk for adnexal torsion. Definitive diagnosis may be based on sonographic findings or may require advanced imaging. In contrast with adult-onset torsion, the incidence of ovarian malignancy causing torsion is exceedingly low and therefore surgical treatment aims for ovarian preservation in the majority of cases.
Abbreviations
CT, computed tomography; MRI, magnetic resonance imaging; POCUS, point of care ultrasound; PED, pediatric emergency department; VAS, visual analog scale; CRP, C-reactive protein; ACEP, American College of Emergency Physicians; ED, emergency department; LOS, length of stay.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Dasgupta R, Renaud E, Goldin AB, et al. Ovarian torsion in pediatric and adolescent patients: a systematic review. J Pediatr Surg. 2018;53(7):1387–1391. doi:10.1016/j.jpedsurg.2017.10.053
2. Chang YJ, Yan DC, Kong MS, et al. Adnexal torsion in children. Pediatr Emerg Care. 2008;24(8):534–537.
3. Rousseau V, Massicot R, Darwish AA, et al. Emergency management and conservative surgery of ovarian torsion in children: a report of 40 cases. J Pediatr Adolesc Gynecol. 2008;21(4):201–206.
4. Aziz D, Davis V, Allen L, Langer JC. Ovarian torsion in children: is oophorectomy necessary? J Pediatr Surg. 2004;39(5):750–753.
5. Oltmann SC, Fischer A, Barber R, et al. Cannot exclude torsion–a 15-year review. J Pediatr Surg. 2009;44(6):1212–1216.
6. Prieto JM, Kling KM, Ignacio RC, et al. Premenarchal patients present differently: a twist on the typical patient presenting with ovarian torsion. J Pediatr Surg. 2019;54(12):2614–2616.
7. Bagolan P, Rivosecchi M, Giorlandino C, et al. Prenatal diagnosis and clinical outcome of ovarian cysts. J Pediatr Surg. 1992;27:879Y881.
8. Scheier E. Inguinal ovarian hernia on point of care ultrasound: case reports and review of the literature. Emerg Radiol. 2022;29(1):215–217.
9. Tseng Y-C, Lee M-S, Chang Y-J, Wu H-P. Acute abdomen in pediatric patients admitted to the pediatric emergency department. Pediatr Neonatol. 2008;49(4):126–134.
10. Rey-Bellet Gasser C, Gehri M, Joseph J-M, et al. Is it ovarian torsion? A systematic literature review and evaluation of prediction signs. Pediatr Emerg Care. 2016;32(4):256–261. doi:10.1097/PEC.0000000000000621
11. Schuh AM, Klein EJ, Allred RJ, et al. Pediatric adnexal torsion: not just a postmenarchal problem. J Emerg Med. 2018;54(1):131–132.
12. Ashwal E, Hiersch L, Krissi H, et al. Characteristics and management of ovarian torsion in premenarchal compared with postmenarchal patients. Obstet Gynecol. 2015;126(3):514–520.
13. Walker SK, Lal DR, Boyd KP, et al. Management of pediatric ovarian torsion: evidence of follicular development after ovarian preservation. Surgery. 2018;163(3):547–552.
14. Sims M, Price A, Hirsig L, et al. Pediatric ovarian torsion should you go with the flow? Pediatr Emerg Care. 2022.
15. Melcer Y, Sarig-Meth T, Maymon R, et al. Similar but different: a comparison of adnexal torsion in pediatric, adolescent, and pregnant and reproductive-age women. J Womens Health. 2016;25(4):391–396.
16. Appelbaum H, Abraham C, Choi-Rosen J, et al. Key clinical predictors in the early diagnosis of adnexal torsion in children. J Pediatr Adolesc Gynecol. 2013;26(3):167–170.
17. Bolli P, Schädelin S, Holland-Cunz S, Zimmermann P. Ovarian torsion in children: development of a predictive score. Medicine. 2017;96(43):e8299.
18. Yilmaz M, Cimilli G, Saritemur M, et al. Diagnostic accuracy of neutrophil/lymphocyte ratio, red cell distribution width and platelet distribution width in ovarian torsion. J Obstet Gynaecol. 2016;36(2):218–222.
19. Tsai J, Lai J-Y, Lin Y-H, et al. Characteristics and risk factors for ischemic ovary torsion in children. Children. 2022;9(2):206.
20. Ssi-Yan-Kai G, Rivain AL, Trichot C, et al. What every radiologist should know about adnexal torsion. Emerg Radiol. 2018;25(1):51–59.
21. Valle Alonso J, Ruffino G, Hurdidge E. Abdominal pain in a young female adolescent: point-of-care ultrasound added value. Pediatr Emerg Care. 2020;36(7):355–357.
22. Wattar B, Rimmer M, Rogozinska E, et al. Accuracy of imaging modalities for adnexal torsion: a systematic review and meta-analysis. BJOG. 2021;128(1):37–44.
23. Tielli A, Scala A, Alison M, et al. Ovarian torsion: diagnosis, surgery, and fertility preservation in the pediatric population. Eur J Pediatr. 2022. doi:10.1007/s00431-021-04352-0
24. Trinci M, Danti G, Di Maurizio M, et al. Can contrast enhanced ultrasound (CEUS) be useful in the diagnosis of ovarian torsion in pediatric females? A preliminary monocentric experience. J Ultrasound. 2021;24(4):505–514.
25. Otjen JP, Stanescu AL, Alessio AM, Parisi MT. Ovarian torsion: developing a machine-learned algorithm for diagnosis. Pediatr Radiol. 2020;50(5):706–714.
26. Corre A, Dandekar S, Lau C, Ranasinghe L, Case A. Report of Pediatric Ovarian Torsion: the Importance of Diagnostic Laparoscopy. Clin Pract Cases Emerg Med. 2021;5(1):109–112.
27. Ultrasound Guidelines. Emergency, Point-of-Care and Clinical Ultrasound Guidelines in Medicine. Ann Emerg Med. 2017;69(5):e27–e54.
28. Chiem AT, Chan CH, Ibrahim DY, et al. Pelvic ultrasonography and length of stay in the ED: an observational study. Am J Emerg Med. 2014;32(12):1464–1469.
29. Gelin A, Driver BE, Whitson KL, et al. The feasibility of bedside transvaginal ultrasonography in non-pregnant women in the emergency department. Am J Emerg Med. 2020;1:84.
30. Curry A, Sodhi S, Rempell J, Cheng A. Young girl with abdominal pain. J Am Coll Emerg Physicians Open. 2020;1(6):1731–1733.
31. Scheier E, Balla U. Ovarian torsion identified on point-of-care ultrasound in the paediatric emergency department. Emerg Med Australas. 2019;31(5):905–906.
32. Scheier E, Balla U. Pediatric ovarian torsion on point-of-care ultrasound: a case series. Pediatr Emerg Care. 2022;38(3):e1159–e1163.
33. Yatsenko O, Vlachou PA, Glanc P. Predictive value of single or combined ultrasound signs in the diagnosis of ovarian torsion. J Ultrasound Med. 2020. doi:10.1002/jum.15497
34. Budhram G, Elia T, Dan J, et al. A case-control study of sonographic maximum ovarian diameter as a predictor of ovarian torsion in emergency department females with pelvic pain. Acad Emerg Med. 2019;26(2):152–159.
35. Hartman SJ, Prieto JM, Naheedy JH, et al. Ovarian volume ratio is a reliable predictor of ovarian torsion in girls without an adnexal mass. J Pediatr Surg. 2020. doi:10.1016/j.jpedsurg.2020.09.031
36. Sibal M. Follicular ring sign: a simple sonographic sign for early diagnosis of ovarian torsion. J Ultrasound Med. 2012;31(11):1803–1809.
37. Schmitt ER, Ngai SS, Gausche-Hill M, Renslo R. Twist and shout! Pediatric ovarian torsion clinical update and case discussion. Pediatr Emerg Care. 2013;29(4):518–523.
38. Lin J, Buttar S. Double Bladder Sign: three Cases of an Ultrasonographic Sign that Indicates Ovarian Torsion. Cureus. 2019;11(7):e5134.
39. Karaca SY, Ileri A. Ovarian Torsion in Adolescents with and without ovarian mass: a Cross-sectional Study. J Pediatr Adolesc Gynecol. 2021;34(6):857–861.
40. Tzur T, Smorgick N, Sharon N, et al. Adnexal torsion with paraovarian cysts in pediatric and adolescent populations: a retrospective study. J Pediatr Surg. 2021;56(2):324–327.
41. Rey-Bellet Gasser C, Gehri M, Joseph JM, et al. Is it ovarian torsion? A systematic literature review and evaluation of prediction signs. Pediatr Emerg Care. 2016;32:256–261.
42. Grunau GL, Harris A, Buckley J, Todd NJ. Diagnosis of Ovarian Torsion: is It Time to Forget About Doppler? J Obstet Gynaecol Can. 2018;40(7):871–875.
43. Shapira-Zaltsberg G, Fleming NA, Karwowska A, et al. Non-visualization of the ovaries on pediatric transabdominal ultrasound with a non-distended bladder: can adnexal torsion be excluded? Pediatr Radiol. 2019;49(10):1313–1319.
44. Joudi N, Adams Hillard PJ. Adnexal torsion in a pediatric population: acute presentation with question of chronicity. Eur J Obstet Gynecol Reprod Biol. 2022;268:82–86.
45. de Matos VL, Pessanha I, David DA, Gante I. Isolated torsion of a fallopian tube: an uncommon cause of abdominal pain in an 11-year-old. BMJ Case Rep. 2021;14(8):e243947.
46. Sola R, Wormer BA, Walters AL, et al. National Trends in the Surgical Treatment of Ovarian Torsion in Children: an Analysis of 2041 Pediatric Patients Utilizing the Nationwide Inpatient Sample. Am Surg. 2015;81(9):844–848.
47. Lipsett SC, Haines L, Monuteaux MC, et al. Variation in Oophorectomy Rates for Children with Ovarian Torsion across US Children’s Hospitals. J Pediatr. 2021;231:269–272.e1.
48. Lawrence AE, Fallat ME, Hewitt G, et al. Factors associated with torsion in pediatric patients with ovarian masses. J Surg Res. 2021;263:110–115.
49. Geimanaite L, Trainavicius K. Pediatric ovarian torsion: follow- up after preservation of ovarian tissue. J Pediatr Surg. 2019;54(7):1453–1456.
50. Murphy NC, Elborno D, Kives S, Allen LM. Postoperative ovarian morphology on ultrasound after ovarian torsion-effect of immediate surgery: a retrospective cohort study. J Pediatr Adolesc Gynecol. 2021;4:5487.
51. Ollivier M, Sfar Mohamed S, Tessier B, et al. Torsion of otherwise healthy ovary Has a worse prognosis than torsion of pathologic ovary in children. J Pediatr Surg. 2019;54(11):2435–2438.
52. Raffaldi I, Guidi C, Di Gianni VR, et al. An insidious cause of abdominal pain in a preschooler girl: the asynchronous bilateral ovarian torsion. Pediatr Emerg Care. 2022;38(1):e61–e62.
53. Ozcan C, Celik A, Ozok G, et al. Adnexal torsion in children may have a catastrophic sequel: asynchronous bilateral torsion. J Pediatr Surg. 2002;37(11):1617–1620.
54. Saberi RA, Gilna GP, Rodriguez C, et al. Ovarian preservation and recurrent torsion in children: both less common than we thought. J Surg Res. 2022;271:67–72.
55. Trotman GE, Cheung H, Tefera EA, et al. Rate of oophorectomy for benign indications in a children’s hospital: influence of a gynecologist. J Pediatr Adolesc Gynecol. 2017;30(2):234–238.
56. Alberto EC, Tashiro J, Zheng Y, et al. Variations in the management of adolescent adnexal torsion at a single institution and the creation of a unified care pathway. Pediatr Surg Int. 2021;37(1):129–135.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.