")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Diagnosis and Management of Insect Allergy: Barriers and Facilitators in the United States
Authors Carlson JC , Hajirawala M , Hein N
Received 1 October 2022
Accepted for publication 5 December 2022
Published 15 December 2022 Volume 2022:15 Pages 1773—1781
DOI https://doi.org/10.2147/JAA.S364867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
John C Carlson,1 Monica Hajirawala,2 Nina Hein3
1Department of Pediatrics, Ochsner Health System, New Orleans, LA, USA; 2Department of Pediatric Allergy and Immunology, University of South Florida, St. Petersburg, FL, USA; 3Department of Allergy and Clinical Immunology, Tulane University, New Orleans, LA, USA
Correspondence: John C Carlson, Department of Pediatrics, Ochsner Health System, 1315 Jefferson Hwy, New Orleans, LA, 20121, USA, Tel +1-504-842-3900, Fax +1-504-842-5848, Email [email protected]
Abstract: While guidelines recommend testing and treatment for patients with venom-induced anaphylaxis to prevent morbidity and mortality, significant barriers prevent most patients from receiving the evaluation and treatments that they need. This review examines these barriers in the United States along with the facilitators that can be used to overcome them.
Keywords: insect hypersensitivity, venom, anaphylaxis, immunotherapy, social determinants of health
Introduction
Despite clear guidelines recommending diagnostic testing and desensitization for patients with venom-induced anaphylaxis,1 barriers prevent many patients from receiving these services. In this review, we examine those barriers and the facilitators that promote access to healthcare within the United States. In cases where barriers and facilitators have not been studied explicitly within the field of venom hypersensitivity, we draw on the data from other areas and describe their potential application to venom allergy.
Barriers to Diagnosis
Patients that experience anaphylaxis from an insect sting should be evaluated by an allergist to confirm the diagnosis and determine appropriate treatment. The diagnosis is made with a combination of history, where the diagnosis of anaphylaxis is confirmed and the probable triggers are determined, and by testing the probable trigger(s) via skin testing and/or blood testing to identify venom-specific IgE.1
The largest barrier to the diagnosis and management of venom-induced anaphylaxis may be access to appropriately trained specialists. After a period of contraction, the number of practicing allergists has been growing as training positions have expanded.2 However, the increase in allergists has not kept up with the needs of the growing population.3 Despite persistent predictions of workforce shortages of allergists,2,4 the reform in graduate medical education needed to address the global shortage has not taken place.3
In addition to the need for expanding allergy fellowship training programs, gaps in training within fellowship programs could also be addressed. Fellowship training in Allergy/Immunology includes training in diagnosing and managing venom hypersensitivity,5 however there is no specific requirement for the number of patients tested or desensitized (10 immunotherapy prescriptions are required, but not differentiated between aeroallergen and venom immunotherapy).6 A survey of 253 allergists in the US confirmed that 100% felt that this was an important skill; however, only 84% felt that they gained this competency during their training.7
Immunotherapy is primarily indicated for those with a diagnosis of venom-induced anaphylaxis. An operational consensus definition of anaphylaxis includes the involvement of two or more organ systems after a probable trigger, such as an insect sting.8 This definition will work for most patients but may miss those with clonal mast cell disorder, in which hypotension may be the only symptom.9 Conversely, this definition may over-diagnose patients with vasovagal, psychosomatic, and anxiety-related reactions that can include subjective dyspnea, cough, vomiting and hypotension.10,11 Thus, the expertise of a well-trained allergist is critical to ensure accuracy in diagnosis. Efforts to cultivate experience with venom allergy across training programs are important as we also strive to increase the number of allergists being trained. A formal assessment of training experiences would be useful in order to determine whether variability in training leads to gaps in competency in this less frequently used skill set.
Beyond having a sufficient number of well-trained allergists, there is generally geographic variability to subspecialty care12,13 with evidence that this is also true for allergists.2 Subspecialists are more likely to work within population centers, particularly those with training programs. The challenges in accessing care concentrated within urban centers are especially worrisome for patients with venom allergy. Data examining whether stings are more likely in rural areas are not available in the US, however, are supported by studies in the UK,14 Greece,15 Spain,16 and Australia.17
Telemedicine can address a barrier to care for patients residing in rural communities by promoting access to subspecialty care. Telehealth has been shown to be noninferior to in-person visits for patients with asthma.18–21 A systematic review of school-aged children showed promising outcomes for asthma education delivered via telemedicine in terms of improvement in quality of life, symptom management, and symptom burden.22 A meta-analysis of asthma in adults similarly showed that telehealth is effective in improving quality of life and asthma control.23 The technological advances in digital technology have enhanced access to subspecialists, including allergists.24
While telemedicine holds great promise for the field, a survey of 183 allergists in Turkey found that only 30% of allergists used telemedicine for venom allergy during the COVID epidemic which was lower than those that used telemedicine for other diagnoses.25 The use of skin testing and immunotherapy injections make the use of telemedicine more challenging in a field where procedures are both diagnostic and therapeutic. While telehealth can overcome access to care in a general sense, other mechanisms will be needed to overcome barriers to testing and treatment.
Testing Barriers
The current US stinging insect hypersensitivity practice parameter recommends skin testing as the initial choice in testing1 based on data suggesting higher sensitivity with skin testing when compared with serum testing.26 It is important to note that there have been significant advances in serum testing compared with the RAST testing used in this study, and a more recent analysis27 noted higher sensitivity using modern ImmunoCAP testing compared with standard intradermal testing. In an accompanying editorial to this paper, Tracy28 notes that access to testing would also be improved using this approach by reducing the potential number of visits needed to make a diagnosis and decreasing the costs associated with intradermal testing incurred by allergists.28 In many areas around the world, serum testing is used in place of skin testing due to barriers accessing venom for testing.29
Skin testing barriers include the venom (cost and access) and the procedure itself, which is time-consuming and less than desirable for patients. Difficulty with access to venom led to notable gaps in access in 2016–2017.30 The cost of the venom itself relative to reimbursement may deter some allergists from routine use of venom skin testing.28 Venom skin testing is time-consuming due to the number of intradermal concentrations being tested. Skin testing for children and others averse to the process of sequential intradermal tests can also be challenging.
Additional barriers to the use of skin testing for venom allergy are the number of antihistaminergic medications that inhibit the wheal-and-flare reaction needed to signify a positive reaction. In addition to first- and second-generation antihistamines, tricyclic antidepressants, sedatives,31 and atypical antipsychotics may suppress immediate skin tests.32 Serum testing is not generally affected by the use of medications but may be affected by monoclonal antibodies. Serum testing may be an effective alternative when testing would otherwise be deferred.
The common practice of delaying tests for six weeks following an anaphylactic reaction can become a barrier to testing. This practice is based on data from Goldberg et al,26 which identified a potential refractory phase, resulting in false negative test results within 6 weeks of an anaphylactic event. It is important to note that in the conclusions of this paper the authors do not suggest delaying allergy testing, but rather repeating negative tests if the initial tests were conducted within this time frame.26 The potential for false negatives with earlier testing is only a theoretical barrier, and this common practice warrants additional study to determine whether it causes unnecessary delay in initiation of immunotherapy for patients.
Identification of the Relevant Venom
Based on a single multisite survey of patients,33 current guidelines recommend not using patient history for identification of the stinging insect triggering an anaphylactic reaction. The results focused on the insects themselves rather than nests that are unique to each genus and excluded other factors that may influence reliability (eg, entomologists and beekeepers may be more reliable in genus determination). In addition, fire ants that produce a pathognomonic sterile pustule due to the activation of neutrophils by the venom alkaloids34 and the presence of these lesions 24 hours after an anaphylactic event is considered diagnostic. In some cases, knowledge of species distribution may be useful in narrowing down the incriminating insect.35 Additional research is warranted to determine the reliability of particular aspects of the history which may reduce the number of extracts used, thereby increasing accessibility for venom immunotherapy.
It can be difficult to identify the offending insect for flying Hymenoptera-induced anaphylaxis based on history alone. As a result, allergists are typically forced to perform venom-specific IgE testing to a range of insects rather than selecting a single type of venom based on history. This often results in more than one positive test result and subsequent choice in selecting the relevant venom extracts to use for desensitization. Without a reliable history, allergists often desensitize patients to all venom types that produce positive test results, increasing cost, time, and potentially risk to patients if clinically irrelevant venoms are used. The current stinging insect hypersensitivity practice parameters1 recommend skin testing prior to serum testing based on increased sensitivity using older serum testing processes.26 In comparing sensitivity of serum testing versus skin testing, Park et al27 conclude that serum testing is more sensitive. Similar to food-specific IgE, clinically irrelevant sensitization to venom is common in the general population. The presence of venom-specific IgE does not reliably indicate that a patient will have clinical reaction to that venom.36 An alternate interpretation may be that serum testing identifies cross-reactivity of unknown clinical significance, exacerbating the challenge of obtaining venom and desensitizing patients.36
For those with a clinically relevant sensitization to one venom, clinically irrelevant cross-reactivity to other venom types may be the result of cross-reactive epitopes, such as Cross-reactive Carbohydrate Determinants (CCDs)37 rather than unique sensitizations. IgE-inhibition assays can be useful in determining the primary venom in these cases,38 but are not commercially available. Component testing may also be a useful tool in reducing the types of venom selected for immunotherapy in some cases.37 Conversely, component testing for Api m 10 may also be useful in clarifying an allergy to honeybee venom when history is suggestive of honeybee-induced anaphylaxis, but whole venom testing is negative due to the loss of Api m 10 in conventional extracting processes.39,40
Clinically relevant cross-sensitization may be present in patients that react to one species of Vespidae,41 where treatment with the primary sensitizing insect should result in tolerance to cross-reactive species.42 Identifying the insect responsible for the primary sensitization within this family is challenging. Fortunately, Vespula and Dolichovespula venom can be purchased together as a Mixed Vespid extract. While the cost of this extract is higher than the selection of the individual venom types, the ability to use a single rush-induction phase provides substantial time savings for patients with cross-reactivity among the Vespidae. Of note, Polistes are also members of the Vespidae, and therefore do result in cross-reactive positivity but is not included in the Mixed Vespid product.
Identification is even more limited with current commercially available extracts which do not contain many species present in the US. This includes imported species (one species of Polistes, three species of Vespa) and native species (Bombus, Solenopsis). Serum testing is available for some, but not all, of these species (Table 1).
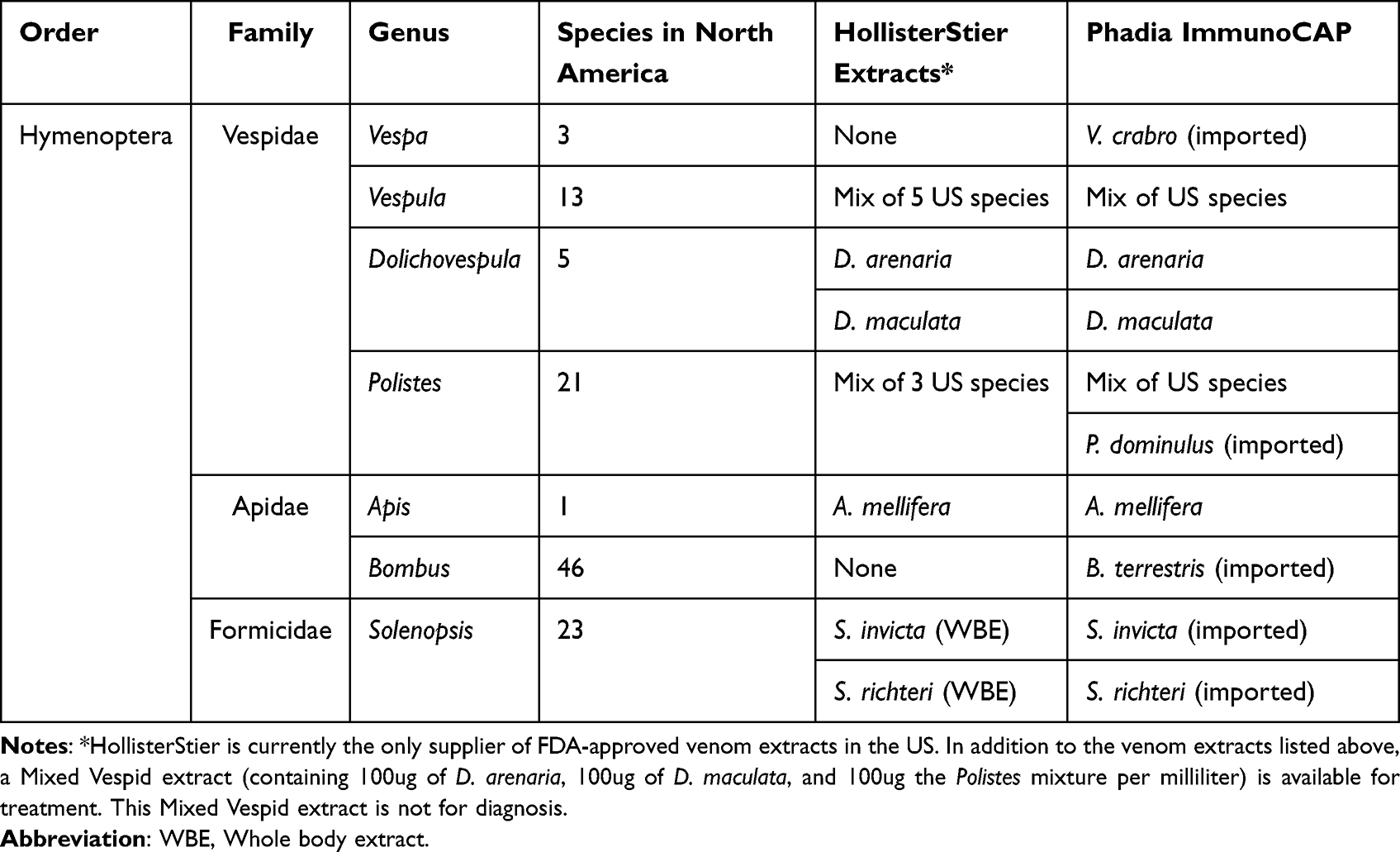 |
Table 1 Testing Options for Venom-Specific IgE Available in the United States |
Barriers to Auto Injectable Epinephrine
Access, training, and cost, are barriers to epinephrine auto injectors (EAI). Identification by providers of when to prescribe epinephrine is the first step to patient access to an EAI. A study of 208 patients diagnosed with anaphylaxis in the Emergency Room (ER) identified that most patients (36.6%) did not receive an EAI prescription nor an allergist referral (31.3%).43 Inadequate training of EAI by healthcare workers poses another hurdle and was found in a study of 697 patients, where only 31.1% of patients demonstrated correct use of the EAI.44
In addition to barriers in access and training, there are barriers in using EAIs by patients. When evaluating patient-driven barriers to prompt epinephrine administration during an event, a study of 66 patients who had been prescribed an EAI at an Allergy and Immunology clinic at a VA medical Center revealed that 92% of patients knew how to use their EAI properly but only 58% consistently carried their device.45 Cost to the patient may also hinder access. In a survey of 917 patients in the US who had been prescribed an EAI, 89% reported filling prescriptions; however, of the ones who did not, 25% cited that cost as the reason.46
Lack of EAI availability and anaphylaxis training is more prevalent in rural and low-income schools. In a survey of school nurses and aides from 1000 schools, 105 rural schools were least likely to have an undesignated EAI available compared to urban and suburban schools and less likely to have a written anaphylaxis plan in the event of a severe allergic reaction (59.4% at rural schools vs 81.7% suburban vs 71.9% urban).47 This is important in venom allergy where most of the fatal outcomes in venom anaphylaxis appear to occur with first reactions.48 The use of stock epinephrine in schools can increase access to EAIs in resource-limited settings.49
The availability of stock epinephrine should be promoted in schools and other public spaces. As with other causes of fatal anaphylaxis, most patients will not have a history of anaphylaxis to draw upon to predict the need for avoidance, auto-injectable epinephrine, or desensitization.50,51 The rapidness with which fatal reactions proceed suggests that epinephrine must be immediately available to prevent this outcome.
While the availability of stock epinephrine is important, desensitization substantially decreases the risk of anaphylaxis, making EAIs less critical for patients with known venom allergy. Venom immunotherapy is more effective for Vespula (yellow jacket) venom (9% react with subsequent sting challenge) than for honeybee venom (23% react with subsequent sting challenge).52 For those with a diagnosis of venom-induced anaphylaxis, venom immunotherapy is a critical intervention. This is especially true for patients without access to autoinjectable epinephrine.
Barriers to Venom Immunotherapy
A study by Patel et al53 described two chart reviews for patients prescribed an EAI and having a diagnosis of venom allergy based on VA medical records from Los Angeles. Time constraints were a common reason for patients not pursuing venom immunotherapy in this study. From 2002 to 2003, 60 patients with reaction to insect venom were identified, of which only 20 were evaluated by an allergist. Review of the allergists’ notes verified anaphylaxis in 12 patients of whom none initiated immunotherapy. In their review of cases in 2012–2013, 193 patients with EAI were identified with a diagnosis of venom allergy and only 20 of these were evaluated by an allergist. Fourteen patients seen by an allergist had a confirmed diagnosis of anaphylaxis. Only one of these patients initiated immunotherapy. The authors noted that time constraints were a motivation for not pursuing immunotherapy in both time periods that were reviewed.
The time investment for patients undergoing venom immunotherapy can be reduced, facilitating initiation. The induction phase of immunotherapy can be reduced from 4 months with conventional build-up dosing to 2 months with modified rush protocols, to 2–3 days with rush protocols and to 4–6 hours using ultrarush induction protocols. Rapid induction immunotherapy protocols appear to be safer than slower induction protocols.54 The use of rush-induction protocols increases completion rates reaching maintenance doses for aeroallergen immunotherapy therapy.55 However, paradoxically, fewer patients stayed on aeroallergen immunotherapy for three years after rush-induction compared with patients that initiate therapy using conventional weekly build-up schedules56 and data suggest that this is also true for fire ant immunotherapy.57
Safety comparison between different build-up schedules has been historically difficult as there are different definitions and end points for rush and ultrarush protocols. The best estimates provided by the most recent practice parameters are systemic reaction rates of 5–10% with rush regimens and 0–28% with ultrarush regimens. They concluded that although the risk of a systemic reaction is higher with ultrarush protocols, the risk associated with rush protocols is similar to conventional protocols.1 Honeybee venom immunotherapy does incur a higher risk (up to 41% with systemic reactions) in comparison to other venoms (up to 25% with yellow jacket venom).52
While the use of pre-medications is common, simplification to the use of H1 blockers as the only premedication, given on the day of flying Hymenoptera immunotherapy, appears sufficiently effective.58,59 Thus, it is possible to initiate venom immunotherapy on the day of diagnosis. Ultrarush protocols for fire ant immunotherapy, however, may be safer with more extensive premedication regimens.60
As with aeroallergen immunotherapy, a buildup phase is done to reach maintenance dosing which is then continued to sustain unresponsiveness with subsequent exposures to the triggering insect. After reaching the maintenance phase, there are further barriers in adherence with immunotherapy, which is discussed more in the literature with aeroallergen immunotherapy. A systematic review by Park et al of subcutaneous immunotherapy (SCIT) reviewed studies regarding persistence (continuing with immunotherapy) and adherence (persisting with prescribed immunotherapy) with SCIT in the real world. Persistence rates in aeroallergen SCIT were found to be 16–93.7%, and adherence rates were 15.1%–99%. Five of the studies reviewed with a total of 416 patients cited “inconvenience” as the primary reason for discontinuation.61
Kiel et al62 studied levels and predictors of compliance and persistence of aeroallergen SCIT in the Netherlands from 1994 to 2009. Only 23% of patients completed the recommended minimum 3 years of maintenance aeroallergen SCIT in that period. Factors that were associated with an increased rate of persistence included older age, prescription by a general practitioner rather than a specialist, more than one allergen in the immunotherapy, and higher socioeconomic class. The authors considered distance as a likely reason for higher persistence with general practitioners as specialists tend to be about 7 times further in distance.62
A real-life study of adherence for both aeroallergen and venom SCIT in a tertiary care center included 124 patients, 39 of which had venom allergy.63 Their total adherence rate was 56.25%, which increases to 69% when assessing venom SCIT specifically. They evaluated for age, gender, where they lived, type of extract, comorbid disease, induction protocol (clustered vs conventional), frequency of systemic or local reactions, and need for pre-medications. Interestingly, of all the factors considered, the only factor associated with nonadherence was from dose modifications required due to systemic/local reactions or due to missed visits. Depot extracts for venom are available elsewhere but not in the US. These formulations are associated with fewer local reactions in the build-up and maintenance phase of venom immunotherapy and therefore may be more effective at retaining patients on venom immunotherapy when available.64
Barriers to adherence to venom and aeroallergen SCIT in the military were evaluated in a study by More et al65 77.4% of 381 patients on SCIT at a single military center were compliant with immunotherapy. Factors resulting in nonadherence included inconvenience (34.5%), precluding medical condition (18.2%), and adverse systemic reaction to immunotherapy (16.4%).65 In 2013, a study of 76 patients in a single military center revealed 35% adherence to fire ant immunotherapy at 1-year follow-up.66 More recently, Park et al completed a military multi-site study of patients who underwent fire ant SCIT and postulated that lack of adherence could be due to this population’s high relocation rate and barriers associated with transition of care.61 More active monitoring and system-level facilitation of venom immunotherapy may be needed.
To facilitate maintenance dose injections, the time between injections can be extended. The FDA-approved package insert for venom extracts recommends maintenance dosing every four weeks. However, intervals of six to eight weeks between injections appear to be safe,67 allowing for lower over-all time commitments prospectively, or safely administering doses after missed injections if used retrospectively. After several years of immunotherapy, doses may be spaced to every three months while maintaining safety and effectiveness of the immunotherapy.68 While the FDA-approved label is for indefinite use of venom immunotherapy, most patients will have long-lasting protection after three to five years of therapy.69 Five years may offer more protection,69,70 and indefinite immunotherapy is recommended for those with higher risk factors for subsequent fatal reactions.1
There is a paucity of information on the role that cost plays in providing access to diagnosis and management of insect hypersensitivity. A study conducted in Portugal examined the consequences of reimbursement cessation for venom immunotherapy; 74% of patients responding to the survey reported stopping VIT due to cost.71 Additional research to clarify the nature of cost as a barrier to care is needed. Presumably, this barrier would be faced by health insurers that have variable practices and policies, costs directly to the patient, and to physician practices if services are not fully reimbursed.72,73 Anecdotally, we know of practices that incur financial losses when providing venom immunotherapy for insured patients. We have also provided extracts to patients that have lacked insurance in our practice; these patients would otherwise have been unable to receive care. Financial barriers faced by physicians could limit their willingness to provide services to patients, adding to the difficulty in accessing physicians with the expertise to diagnose and manage insect hypersensitivity.
Conclusion
Insect hypersensitivity reactions cause significant morbidity and mortality; appropriate diagnosis and management are essential to alleviating them. The primary barrier to diagnosis of insect hypercreativity is difficulty in accessing a trained allergist. Telehealth has the capacity to facilitate access to subspecialists for diagnosis. This does not address the barriers to provision of immunotherapy for patients. Serum testing and component testing may reduce the amount of venom needed for testing and treatment of patients. Use of ultrarush induction protocols for build-up and increasing the spacing interval of maintenance injections may reduce time constraints for those needing immunotherapy while maintaining similar safety profiles as conventional build-up and maintenance dosing. Additional research is needed to better understand the barriers facing those with venom hypersensitivity and how to facilitate the healthcare for these patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Golden DB, Demain J, Freeman T, et al. Stinging insect hypersensitivity: a practice parameter update 2016. Ann Allergy Asthma Immunol. 2017;118:28–54. doi:10.1016/j.anai.2016.10.031
2. Marshall GD; American Academy of Allergy Association, Immunology Workforce Committee. The status of US allergy/immunology physicians in the 21st century: a report from the American Academy of Allergy, Asthma & Immunology Workforce Committee. J Allergy Clin Immunol. 2007;119:802–807. doi:10.1016/j.jaci.2007.01.040
3. Malick A, Meadows JA. Allergy and immunology physician workforce: where do we stand today? Ann Allergy Asthma Immunol. 2021;127:522–523. doi:10.1016/j.anai.2021.06.008
4. de Asis ML. The future physician workforce: an allergy-immunology specialist perspective. Ann Allergy Asthma Immunol. 1999;83:99–103. doi:10.1016/S1081-1206(10)62619-1
5. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in allergy and immunology. 2022.
6. Accreditation Council for Graduate Medical Education. Case log procedures for allergy and immunology programs. 2019.
7. Li JT, Stoll DA, Smith JE, Lin JJ, Swing SR. Graduates’ perceptions of their clinical competencies in allergy and immunology: results of a survey. Acad Med. 2003;78:933–938. doi:10.1097/00001888-200309000-00021
8. Sampson HA, Munoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report--second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. Ann Emerg Med. 2006;47:373–380. doi:10.1016/j.annemergmed.2006.01.018
9. Zanotti R, Lombardo C, Passalacqua G, et al. Clonal mast cell disorders in patients with severe hymenoptera venom allergy and normal serum tryptase levels. J Allergy Clin Immunol. 2015;136:135–139. doi:10.1016/j.jaci.2014.11.035
10. Rosloff DA, Patel K, Feustel PJ, Celestin J. Criteria positive and criteria negative anaphylaxis, with a focus on undifferentiated somatoform idiopathic anaphylaxis: a review and case series. Allergy Asthma Proc. 2020;41:436–441. doi:10.2500/aap.2020.41.200076
11. Choy AC, Patterson R, Patterson DR, et al. Undifferentiated somatoform idiopathic anaphylaxis: nonorganic symptoms mimicking idiopathic anaphylaxis. J Allergy Clin Immunol. 1995;96:893–900. doi:10.1016/S0091-6749(95)70225-3
12. Mayer ML. Disparities in geographic access to pediatric subspecialty care. Matern Child Health J. 2008;12:624–632. doi:10.1007/s10995-007-0275-3
13. Turner A, Ricketts T, Leslie LK. Comparison of number and geographic distribution of pediatric subspecialists and patient proximity to specialized care in the US between 2003 and 2019. JAMA Pediatr. 2020;174:852–860. doi:10.1001/jamapediatrics.2020.1124
14. Perez-Pimiento A, Prieto-Lastra L, Rodriguez-Cabreros M, Reano-Martos M, Garcia-Cubero A, Garcia-Loria J. Work-related anaphylaxis to wasp sting. Occup Med. 2007;57:602–604. doi:10.1093/occmed/kqm054
15. Grigoreas C, Galatas ID, Kiamouris C, Papaioannou D. Insect-venom allergy in Greek adults. Allergy. 1997;52:51–57. doi:10.1111/j.1398-9995.1997.tb02545.x
16. Fernandez J, Blanca M, Soriano V, Sanchez J, Juarez C. Epidemiological study of the prevalence of allergic reactions to Hymenoptera in a rural population in the Mediterranean area. Clin Exp Allergy. 1999;29:1069–1074. doi:10.1046/j.1365-2222.1999.00614.x
17. Brown SG, Franks RW, Baldo BA, Heddle RJ. Prevalence, severity, and natural history of jack jumper ant venom allergy in Tasmania. J Allergy Clin Immunol. 2003;111:187–192. doi:10.1067/mai.2003.48
18. Kew KM, Cates CJ. Remote versus face-to-face check-ups for asthma. Cochrane Database Syst Rev. 2016;4:CD011715. doi:10.1002/14651858.CD011715.pub2
19. Portnoy JM, Waller M, De Lurgio S, Dinakar C. Telemedicine is as effective as in-person visits for patients with asthma. Ann Allergy Asthma Immunol. 2016;117:241–245. doi:10.1016/j.anai.2016.07.012
20. Perry TT, Halterman JS, Brown RH, et al. Results of an asthma education program delivered via telemedicine in rural schools. Ann Allergy Asthma Immunol. 2018;120:401–408. doi:10.1016/j.anai.2018.02.013
21. Zhao J, Zhai YK, Zhu WJ, Sun DX. Effectiveness of telemedicine for controlling asthma symptoms: a systematic review and meta-analysis. Telemed J E Health. 2015;21:484–492. doi:10.1089/tmj.2014.0119
22. Culmer N, Smith T, Stager C, et al. Telemedical asthma education and health care outcomes for school-age children: a systematic review. J Allergy Clin Immunol Pract. 2020;8:1908–1918. doi:10.1016/j.jaip.2020.02.005
23. Chongmelaxme B, Lee S, Dhippayom T, Saokaew S, Chaiyakunapruk N, Dilokthornsakul P. The effects of telemedicine on asthma control and patients’ quality of life in adults: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2019;7:199–216 e111. doi:10.1016/j.jaip.2018.07.015
24. Bajowala SS, Shih J, Varshney P, Elliott T. The future of telehealth for allergic disease. J Allergy Clin Immunol Pract. 2022;10:2514–2523. doi:10.1016/j.jaip.2022.08.022
25. Ozturk AB, Baccioglu A, Soyer O, Civelek E, Sekerel BE, Bavbek S. Change in allergy practice during the COVID-19 pandemic. Int Arch Allergy Immunol. 2021;182:49–52. doi:10.1159/000512079
26. Goldberg A, Confino-Cohen R. Timing of venom skin tests and IgE determinations after insect sting anaphylaxis. J Allergy Clin Immunol. 1997;100:182–184. doi:10.1016/S0091-6749(97)70222-7
27. Park HJ, Brooks DI, Chavarria CS, Wu RL, Mikita CP, Beakes DE. Combining discordant serum IgE and skin testing improves diagnostic and therapeutic accuracy for hymenoptera venom hypersensitivity immunotherapy. J Allergy Clin Immunol Pract. 2022;10:837–843 e833. doi:10.1016/j.jaip.2021.08.037
28. Tracy JM. Testing for venom allergy: should we change testing order? J Allergy Clin Immunol Pract. 2022;10:844–845. doi:10.1016/j.jaip.2021.12.028
29. Korosec P, Jakob T, Harb H, et al. Worldwide perspectives on venom allergy. World Allergy Organ J. 2019;12:100067. doi:10.1016/j.waojou.2019.100067
30. Golden DB, Bernstein DI, Freeman TM, Tracy JM, Lang DM, Nicklas RA. AAAAI/ACAAI joint venom extract shortage task force report. Ann Allergy Asthma Immunol. 2017;118:283–285. doi:10.1016/j.anai.2017.02.001
31. Bernstein IL, Li JT, Bernstein DI, et al. Allergy diagnostic testing: an updated practice parameter. Ann Allergy Asthma Immunol. 2008;100:S1–148. doi:10.1016/s1081-1206(10)60305-5
32. Kjaer HF, Mortz CG, Bindslev-Jensen C. Does treatment with antidepressants, antipsychotics, or benzodiazepines hamper allergy skin testing? Clin Transl Allergy. 2021;11:e12060. doi:10.1002/clt2.12060
33. Baker TW, Forester JP, Johnson ML, Stolfi A, Stahl MC. The HIT study: hymenoptera identification test--how accurate are people at identifying stinging insects? Ann Allergy Asthma Immunol. 2014;113:267–270. doi:10.1016/j.anai.2014.05.029
34. Javors MA, Zhou W, Maas JW, Han S, Keenan RW. Effects of fire ant venom alkaloids on platelet and neutrophil function. Life Sci. 1993;53:1105–1112. doi:10.1016/0024-3205(93)90546-F
35. Carlson JC, Fox MS. Exposure to species of Vespidae in the urbanized areas of New Orleans, Louisiana. Ann Allergy Asthma Immunol. 2021;127:384–386. doi:10.1016/j.anai.2021.05.014
36. Sturm GJ, Kranzelbinder B, Schuster C, et al. Sensitization to Hymenoptera venoms is common, but systemic sting reactions are rare. J Allergy Clin Immunol. 2014;133:1635–1643 e1631. doi:10.1016/j.jaci.2013.10.046
37. Blank S, Bilo MB, Ollert M. Component-resolved diagnostics to direct in venom immunotherapy: important steps towards precision medicine. Clin Exp Allergy. 2018;48:354–364. doi:10.1111/cea.13090
38. Holzweber F, Svehla E, Fellner W, et al. Inhibition of IgE binding to cross-reactive carbohydrate determinants enhances diagnostic selectivity. Allergy. 2013;68:1269–1277. doi:10.1111/all.12229
39. Blank S, Etzold S, Darsow U, et al. Component-resolved evaluation of the content of major allergens in therapeutic extracts for specific immunotherapy of honeybee venom allergy. Hum Vaccin Immunother. 2017;13:2482–2489. doi:10.1080/21645515.2017.1323603
40. Jakob T, Rauber MM, Perez-Riverol A, Spillner E, Blank S. The honeybee venom major allergen Api m 10 (Icarapin) and its role in diagnostics and treatment of hymenoptera venom allergy. Curr Allergy Asthma Rep. 2020;20:48. doi:10.1007/s11882-020-00943-3
41. Blank S, Bazon ML, Grosch J, et al. Antigen 5 allergens of hymenoptera venoms and their role in diagnosis and therapy of venom allergy. Curr Allergy Asthma Rep. 2020;20:58. doi:10.1007/s11882-020-00954-0
42. Kosnik M, Korosec P, Silar M, Music E, Erzen R. Wasp venom is appropriate for immunotherapy of patients with allergic reaction to the European hornet sting. Croat Med J. 2002;43:25–27.
43. Campbell RL, Luke A, Weaver AL, et al. Prescriptions for self-injectable epinephrine and follow-up referral in emergency department patients presenting with anaphylaxis. Ann Allergy Asthma Immunol. 2008;101:631–636. doi:10.1016/S1081-1206(10)60227-X
44. Arga M, Topal E, Yilmaz S, Erdemli PC, Bicakci K, Bakirtas A. Healthcare workers` knowledge level regarding anaphylaxis and usage of epinephrine auto-injectors. Turk J Pediatr. 2021;63:372–383. doi:10.24953/turkjped.2021.03.004
45. Amirzadeh A, Verma P, Lee S, Klaustermeyer W. Epinephrine auto-injector use and demographics in a Veterans Administration population. Allergy Asthma Proc. 2010;31:304–307. doi:10.2500/aap.2010.31.3351
46. Warren CM, Zaslavsky JM, Kan K, Spergel JM, Gupta RS. Epinephrine auto-injector carriage and use practices among US children, adolescents, and adults. Ann Allergy Asthma Immunol. 2018;121:479–489 e472. doi:10.1016/j.anai.2018.06.010
47. Szychlinski C, Schmeissing KA, Fuleihan Z, et al. Food allergy emergency preparedness in Illinois schools: rural disparity in guideline implementation. J Allergy Clin Immunol Pract. 2015;3:805–807 e808. doi:10.1016/j.jaip.2015.04.017
48. Barnard JH. Studies of 400 Hymenoptera sting deaths in the United States. J Allergy Clin Immunol. 1973;52:259–264. doi:10.1016/0091-6749(73)90044-4
49. Neupert KB, Huntwork MP, Udemgba C, Carlson JC. Implementation of stock epinephrine in chartered versus unchartered public-school districts. J Sch Health. 2022;92:812–814. doi:10.1111/josh.13159
50. Pumphrey R. Anaphylaxis: can we tell who is at risk of a fatal reaction? Curr Opin Allergy Clin Immunol. 2004;4:285–290. doi:10.1097/01.all.0000136762.89313.0b
51. Pumphrey RS. Lessons for management of anaphylaxis from a study of fatal reactions. Clin Exp Allergy. 2000;30:1144–1150. doi:10.1046/j.1365-2222.2000.00864.x
52. Muller U, Helbling A, Berchtold E. Immunotherapy with honeybee venom and yellow jacket venom is different regarding efficacy and safety. J Allergy Clin Immunol. 1992;89:529–535. doi:10.1016/0091-6749(92)90319-W
53. Patel AM, Wang V, Philipp A, Yusin JS. Underuse of allergy services for patients having systemic reactions to Hymenoptera venom stings. Ann Allergy Asthma Immunol. 2017;118:366–367. doi:10.1016/j.anai.2016.11.025
54. Birnbaum J, Charpin D, Vervloet D. Rapid Hymenoptera venom immunotherapy: comparative safety of three protocols. Clin Exp Allergy. 1993;23:226–230. doi:10.1111/j.1365-2222.1993.tb00886.x
55. Teachout J, Vandegrift S, Schafer C, Uekert S, Gell K. Improved patient adherence to subcutaneous allergen immunotherapy using a modified rush immunotherapy protocol. Ann Allergy Asthma Immunol. 2019;122:347–349. doi:10.1016/j.anai.2018.10.005
56. Lee JH, Lee SH, Ban GY, et al. Factors associated with adherence to allergen specific subcutaneous immunotherapy. Yonsei Med J. 2019;60:570–577. doi:10.3349/ymj.2019.60.6.570
57. Neaves BI, Adams KE, White KM, Stokes SC, Sacha J, Quinn JM. Long-term adherence to imported fire ant subcutaneous immunotherapy. Ann Allergy Asthma Immunol. 2022. doi:10.1016/j.anai.2022.09.020
58. Berchtold E, Maibach R, Muller U. Reduction of side effects from rush-immunotherapy with honey bee venom by pretreatment with terfenadine. Clin Exp Allergy. 1992;22:59–65. doi:10.1111/j.1365-2222.1992.tb00115.x
59. Reimers A, Hari Y, Muller U. Reduction of side-effects from ultrarush immunotherapy with honeybee venom by pretreatment with fexofenadine: a double-blind, placebo-controlled trial. Allergy. 2000;55:484–488. doi:10.1034/j.1398-9995.2000.00520.x
60. Arseneau AM, Nesselroad TD, Dietrich JJ, et al. A 1-day imported fire ant rush immunotherapy schedule with and without premedication. Ann Allergy Asthma Immunol. 2013;111:562–566. doi:10.1016/j.anai.2013.08.021
61. Park M, Kapoor S, Yi J, Hura N, Lin S. Systematic review of real-world persistence and adherence in subcutaneous allergen immunotherapy. Int Forum Allergy Rhinol. 2022. doi:10.1002/alr.23078
62. Kiel MA, Roder E, Gerth van Wijk R, Al MJ, Hop WC, Rutten-van Molken MP. Real-life compliance and persistence among users of subcutaneous and sublingual allergen immunotherapy. J Allergy Clin Immunol. 2013;132:353–360 e352. doi:10.1016/j.jaci.2013.03.013
63. Koca Kalkan I, Ates H, Aksu K, et al. Real-life adherence to subcutaneous immunotherapy: what has changed in the era of the COVID-19 pandemic. World Allergy Organ J. 2021;14:100558. doi:10.1016/j.waojou.2021.100558
64. Rueff F, Wolf H, Schnitker J, Ring J, Przybilla B. Specific immunotherapy in honeybee venom allergy: a comparative study using aqueous and aluminium hydroxide adsorbed preparations. Allergy. 2004;59:589–595. doi:10.1111/j.1398-9995.2004.00505.x
65. Moore WC, Meyers DA, Wenzel SE, et al. Identification of asthma phenotypes using cluster analysis in the severe asthma research program. Am J Respir Crit Care Med. 2010;181:315–323. doi:10.1164/rccm.200906-0896OC
66. Stokes SC, Quinn JM, Sacha JJ, White KM. Adherence to imported fire ant subcutaneous immunotherapy. Ann Allergy Asthma Immunol. 2013;110:165–167. doi:10.1016/j.anai.2012.11.010
67. Gadde J, Sobotka A, Valentine M, Lichtenstein L, Golden D. Intervals of 6 and 8 weeks in maintenance venom immunotherapy (MVIT). Ann Allergy. 1985;54:348.
68. Cavallucci E, Ramondo S, Renzetti A, et al. Maintenance venom immunotherapy administered at a 3-month interval preserves safety and efficacy and improves adherence. J Investig Allergol Clin Immunol. 2010;20:63–68.
69. Lerch E, Muller UR. Long-term protection after stopping venom immunotherapy: results of re-stings in 200 patients. J Allergy Clin Immunol. 1998;101:606–612. doi:10.1016/S0091-6749(98)70167-8
70. Keating MU, Kagey-Sobotka A, Hamilton RG, Yunginger JW. Clinical and immunologic follow-up of patients who stop venom immunotherapy. J Allergy Clin Immunol. 1991;88:339–348. doi:10.1016/0091-6749(91)90095-6
71. Carneiro-Leao L, Amaral L, Coimbra A. Reasons for Declining Venom Immunotherapy. Acta Med Port. 2018;31:618–623. doi:10.20344/amp.9695
72. Meadows JA, Golden DBK, Tracy J, Reyes EG, Sublett J. Venom shortages: what’s an allergist to do? Part 1, the issues. Ann Allergy Asthma Immunol. 2019;123:9–10. doi:10.1016/j.anai.2019.03.006
73. Meadows JA, Golden DBK, Tracy J, Reyes EG, Sublett J. Venom shortages: what’s an allergist to do? Part two: potential solutions. Ann Allergy Asthma Immunol. 2019;123:131–132. doi:10.1016/j.anai.2019.03.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.