")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Diagnosing pseudobulbar affect in traumatic brain injury
Authors Engelman W, Hammond F, Malec J
Received 1 March 2014
Accepted for publication 30 April 2014
Published 7 October 2014 Volume 2014:10 Pages 1903—1910
DOI https://doi.org/10.2147/NDT.S63304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
William Engelman,1 Flora M Hammond,2 James F Malec2
1Health Economics and Epidemiology, Evidera, Lexington, MA, 2Indiana University School of Medicine, Rehabilitation Hospital of Indiana, Indianapolis, IN, USA
Abstract: Pseudobulbar affect (PBA) is defined by episodes of involuntary crying and/or laughing as a result of brain injury or other neurological disease. Epidemiology studies show that 5.3%–48.2% of people with traumatic brain injury (TBI) may have symptoms consistent with (or suggestive of) PBA. Yet it is a difficult and often overlooked condition in individuals with TBI, and is easily confused with depression or other mood disorders. As a result, it may be undertreated and persist for longer than it should. This review presents the signs and symptoms of PBA in patients with existing TBI and outlines how to distinguish PBA from other similar conditions. It also compares and contrasts the different diagnostic criteria found in the literature and briefly mentions appropriate treatments. This review follows a composite case with respect to the clinical course and treatment for PBA and presents typical challenges posed to a provider when diagnosing PBA.
Keywords: traumatic brain injury, complications, differential diagnosis, crying, laughing
Composite case report
Patient JC is a 55-year-old married white female with a past history of hypertension and type 2 diabetes mellitus who recently experienced a closed head injury from a motor vehicle accident. The injury was followed by post-traumatic amnesia for 22 days and required surgery for an epidural hematoma and then 3 months in acute care and 3 weeks in inpatient rehabilitation. She subsequently presented for evaluation of affective disturbances after her family members noted episodes of crying occurring suddenly and frequently. Assessment by the patient’s physician found that she was oriented to person, place, and time but had mild attention and memory problems on mental status testing. Routine laboratory chemistry tests were normal. She was diagnosed with depression and started on an antidepressant. At 6-month follow-up, tearful outbursts had not resolved. Although JC denied feeling low, it was still presumed that the crying signified sadness or depression, leading to the addition of an anticonvulsant medication. In spite of this, she continued to have frequent crying episodes, described as brief and uncontrollable “attacks”, that came on suddenly, with minimal provocation, approximately 12 times daily.
Introduction
Traumatic brain injury (TBI) accounts for approximately 50,000 deaths in the USA every year,1,2 and many survivors of the acute event will experience disabling sequelae that impair both daily activities and quality of life.3 Accurately identifying ancillary conditions of TBI is essential to minimizing their impact. However, this can be challenging because the symptoms and signs of common ancillary conditions, as well as those of TBI itself, can have overlapping clinical features. For example, frequent crying and/or laughing episodes following TBI may go undiagnosed or misdiagnosed, particularly in patients who may not be able to accurately communicate their emotions. The composite case above, in which the patient denied having low mood illustrates how an individual with TBI and crying episodes may be misdiagnosed with depression and, thus, correspondingly treated. With this in mind, the following review considers the differential diagnosis and further management of otherwise unexplained crying or laughing episodes after TBI, focusing on a key but frequently overlooked cause of these symptoms, ie, pseudobulbar affect (PBA).
What could the diagnosis be?
The fact that JC does not report low mood and has not responded to antidepressant therapy suggests that she may have a refractory form of depression, or, very likely, that there is an alternative explanation for the crying episodes. The differential diagnosis for inappropriate laughing and crying episodes would include the following (see also Table 1).
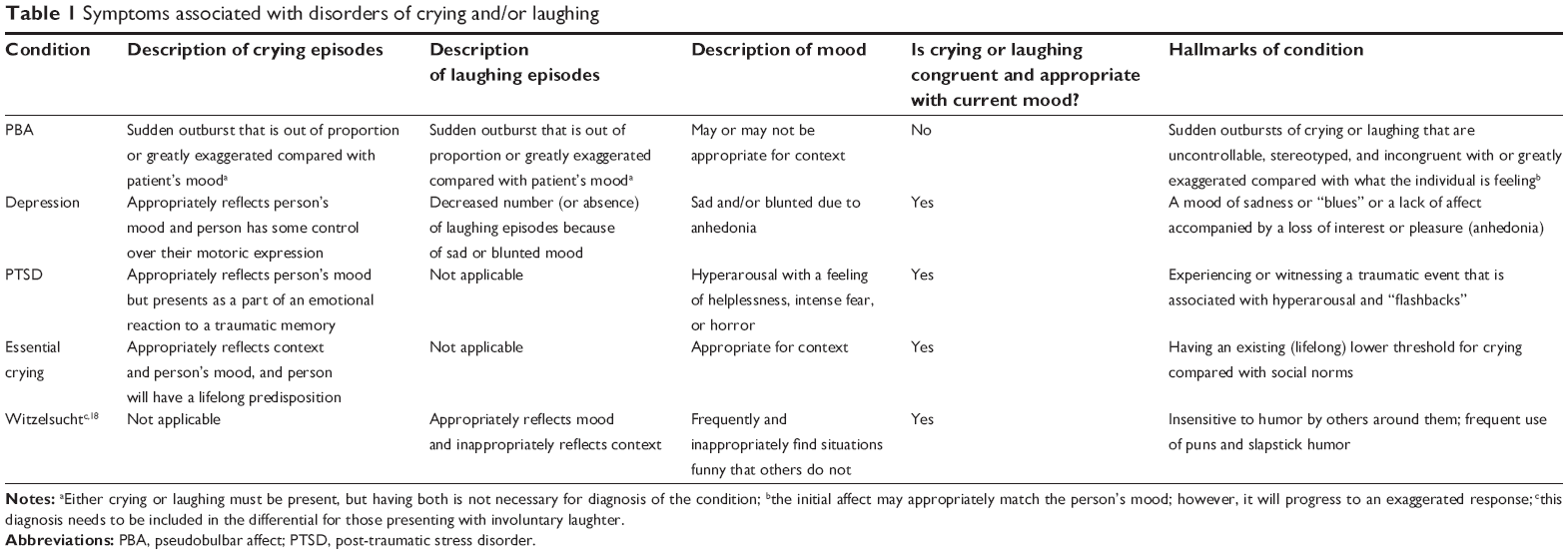 | Table 1 Symptoms associated with disorders of crying and/or laughing |
Depression
JC may have refractory depression that is not responsive to standard therapy. It is important to rule this possibility out, given that estimates suggest 40%–62% of people hospitalized for TBI experience major depression in the years following injury.4–6 Accordingly, many health care providers encountering patients who cry make the understandable assumption that their crying is a symptom of depression. However, this overlooks the fact that not all crying signifies depression or even low mood. In fact, crying in depression has not been well characterized, and the symptom is not a necessary or sufficient criterion for diagnosing depression in the DSM-V (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition).7
The notion that crying automatically indicates depressed mood is further undermined by published evidence. Rottenberg et al found no significant difference between the proportions of depressed and nondepressed individuals who experienced elicited crying when watching a sad film (23.6% versus 18.2%) nor any differences in time to onset or duration of crying among those who did cry.8 Also, in a separate study, Rottenberg et al found that while some people with depression reported increased crying in response to negative emotions, there was no linear relationship between severity of depression and overall proneness to or the frequency or severity of crying.9
Evidence of anhedonia and neurovegetative symptoms is required for a diagnosis of depression.10–12 These features may include disturbances in sleep, disturbances in appetite and weight changes, decreased sexual desire, low energy, psychomotor retardation or agitation, and poor concentration. In addition, some people who are depressed report being unable to cry, which may reflect emotional blunting and anhedonia.9,13
Anxiety disorder
In theory, crying episodes could reflect an underlying anxiety disorder. A key possibility here is post-traumatic stress disorder (PTSD), a common finding in TBI. Studies found that the prevalence of PTSD was 62% in soldiers with mild TBI14 and 27% in people with noncombat-related TBI who were not unconscious for an extended period after the traumatic event.15 However, stereotypical crying episodes are not a cardinal feature of PTSD, which requires one or both of the following to be present in the history:
- Experiencing, witnessing, or being confronted with an event involving serious injury, death, or a threat to a person’s physical integrity16
- A response involving helplessness, intense fear, or horror.16
Also, some individuals with PTSD have outbursts of anger or irritable mood and exaggerated startle responses.16
Essential crying
People with essential crying have a lifelong lower threshold for weeping.17 This phenomenon may be a variant of the emotional domain of temperament and does not imply an underlying neurological disorder. An essential crying diagnosis is uncommon; nonetheless, clinicians should inquire about the person’s threshold for tearfulness before the TBI occurred.
Witzelsucht
This is a rare disorder in which people will inappropriately find situations funny that others do not and are insensitive to humor by others around them. They often will use puns and slapstick humor. Their affect is congruent with their mood.18
PBA disorder
People with PBA experience episodes of involuntary crying and/or laughing as a result of brain injury or other neurological disease. PBA episodes represent a change from typical emotional reactivity and are incongruent or excessive with regard to the individual’s mood or the provoking stimulus. There is sometimes no clear environmental trigger for the episodes. Clinically, people describe PBA as feeling as if they have lost control of their emotions, with some saying that once an episode starts, it is difficult to stop or is something they need to “wait out”. The nature of each patient’s PBA outbursts tends to be the same on each occasion, with Poeck describing them as being “stereotyped” from one episode to the next.19 PBA episodes can cause significant distress or embarrassment, and are likewise distressing or embarrassing for those around the affected person, resulting in social or occupational impairment.20
It is important to take into consideration that an individual may have multiple comorbid conditions as a result of the TBI or injury event. For example, major depression, PTSD, and PBA may co-occur with TBI. Table 1 compares and contrasts the symptoms of various disorders that are associated with crying and/or laughing. Note that Witzelsucht occurs relatively infrequently and is thus not discussed beyond the listing in Table 1.
The description of crying in JC is at odds with that caused by sad mood and is described as “attacks” that are unrelated or greatly out of proportion to any stimulus. This combination of features should raise suspicion for PBA. So what exactly is PBA, and how is it identified and treated?
About PBA
Definition
PBA is one of several terms that have been used to describe sudden, involuntary, uncontrollable episodes of crying and/or laughing that are incongruent or disproportional to the underlying mood state observed in patients with brain injury or other neurological disorder affecting the brain. Other terms also utilized to describe these manifestations include “pathological laughing and crying”, “affective lability”, “emotionalism”, “emotional incontinence”, “involuntary emotional expression disorder”, and “emotional lability”.19–26 The variety of terms and associated clinical descriptions has led to confusion in the literature regarding the scope and nature of the dysregulation of emotional expression. We have used the term “PBA” for this review, to be consistent with terminology adopted by the regulatory agencies in the USA and European Union denoting a neurological condition primarily manifested by loss of control of crying and/or laughing in the context of a neurological disorder. In addition, some of the other terms that have been used to describe this condition, such as “emotionalism” or “emotional incontinence”, suggest a disorder of emotions or mood rather than a disorder of emotional expression.27 As described earlier, PBA is characterized by involuntary, uncontrollable, frequent, and sudden outbursts of crying and/or laughter. It occurs secondary to various neurological conditions, including TBI, multiple sclerosis, amyotrophic lateral sclerosis, Parkinson’s disease, stroke, Alzheimer’s disease, dementia, and other neurological diseases that damage the central nervous system. It has also been reported that PBA may occur concurrently with problems such as anger or frustration28 and depression.
The pathophysiology of PBA has been thoroughly reviewed by Parvizi et al and is believed to result from lesions in the frontal lobes or descending corticobulbar/cerebellar pathways that regulate motor control and coordination of emotional expression.29–31
Burden of disease
Episodes of PBA may result in considerable burden to the affected person or those around him or her. A case-control study conducted by Colamonico et al32 involved patients and caregivers of patients with Alzheimer’s disease, amyotrophic lateral sclerosis, multiple sclerosis, Parkinson’s disease, stroke, or TBI who participated in the Harris Panel Online (HPOL). The HPOL is a representative sample of 6 million US residents and includes 1.5 million persons or caregivers of persons with chronic diseases. From the HPOL cohort with the aformentioned illnesses, 399 cases with symptoms of PBA (265 patients/134 caregivers) and 653 non-PBA controls (413 patients/240 caregivers) were recruited. Individuals with PBA symptoms (defined as having a Center for Neurologic Study-Lability Scale [CNS-LS, a PBA rating scale validated in patients with amyotrophic lateral sclerosis or multiple sclerosis] score of ≥13) and those without such symptoms (ie, CNS-LS score <13) were compared to study the effects on social and occupational function, health status, patient quality of life, and quality of relationships.
Respondents with CNS-LS ≥13 who acknowledged inappropriate or excessive laughing or crying episodes were also asked customized questions about the burden of these episodes. When compared with non-PBA controls, the study results showed that PBA symptoms were associated with significantly worse scores on measures of quality of life, quality of relationships, health status, and social and occupational functioning.32 Also, involuntary episodes of laughing and crying were reported as being the main cause of or contributing greatly to becoming housebound in approximately one of four respondents in the PBA group and to being placed in supervised living for one of ten people.32
Epidemiology of PBA
The prevalence of PBA in TBI is difficult to establish. The few relevant studies found in the literature estimated that 5.3%–48.2%33 of people with TBI have symptoms consistent with, or suggestive of, PBA.28,34,35 This wide range of prevalence results in part from differing methods and symptom thresholds used for diagnosis.
Zeilig et al reported that the prevalence of pathological laughing and crying (consistent with PBA) was 5.3% (16 of 301) among people with closed TBI admitted to a rehabilitation hospital affiliated with a regional trauma center, with the condition being identified independently by two experienced attending physicians, board-certified in neurology and psychiatry.35
Tateno et al reported the prevalence of pathological laughing and crying as 10.9% during the first year after a diagnosis of TBI among 92 individuals with a closed head injury in a hospital setting. Pathological laughing and crying was identified based on occurrence of sudden episodes of uncontrollable, emotional expression that were elicited by nonspecific stimuli or were out of proportion to the stimulus and did not have a clear association with the prevailing mood state.34
Work et al reported PBA symptom prevalence to be as high as 48.2% among participants registered in the HPOL panel with TBI polled using an Internet survey. Screening for PBA was done using the Pathological Laughing and Crying Scale (PLACS), a PBA rating scale validated in stroke patients,28 and the CNS-LS. The prevalence of the condition’s symptoms was estimated at various rating-scale thresholds: a PLACS score of ≥13; a CNS-LS score of ≥13; and a more stringent CNS-LS cut-off of ≥21. The proportion of participants with PLACS ≥13 was 17.4%; with CNS-LS ≥13, 48.2%; and with CNS-LS ≥21, 15.5%. Similarly, Brooks et al reported the estimated prevalence of PBA symptoms from the PBA Registry Series (PRISM) – a PBA screening study. This study also measured PBA symptoms using the CNS-LS, but was conducted in a clinic sample of patients in physician offices. PRISM included 590 individuals with TBI and found a PBA symptom prevalence of 52.4% using a CNS-LS ≥13 and 16.4% using a CNS-LS threshold of ≥21.33
In considering these data, it is important to note that the CNS-LS is not diagnostic and has been validated for identifying PBA in people with amyotrophic lateral sclerosis and multiple sclerosis, but not TBI.28 With regards to the much higher prevalence estimate obtained using a CNS-LS cut-off of ≥13, it is unclear whether this threshold is picking up less severe symptoms that might not be reported to physicians or whether the scale itself is less able to discriminate PBA from other causes of laughing and crying in the patients in question. It is also important to note that although the prevalence estimates using the PLACS cut-off score of ≥13 and the CNS-LS score of ≥21 are more consistent with other estimates in the literature, they are still significantly higher. This was probably because the samples taken were a convenience sample and a clinic sample, respectively, and likely attracted people with TBI who were still experiencing difficulties as opposed to an assessment of a population of people with TBI who were assessed or followed.
Clinical criteria for PBA in TBI
One of the difficulties in accurately identifying PBA is the low awareness of the condition among patients and physicians.28 This is exemplified in the study by Work et al in which 74% of people with PBA symptoms reported laughing or crying symptoms to their health care provider. Of those patients who discussed symptoms, 41% were given a specific diagnosis, but in no case was a diagnosis of PBA (or a similarly termed condition) given. Instead, these patients’ symptoms were categorized as depression (in 33% of cases), PTSD (9%), bipolar disorder (13%), or just a “part of their condition”.28 Having a low awareness for PBA typically reflects unfamiliarity with the diagnostic criteria for this condition. The most widely known descriptions are by Poeck and by Cummings et al.
Poeck criteria
In 1969, Poeck published criteria for recognizing PBA that included the presence of inappropriate laughing and crying that “…may arise in cerebral diseases of the most diverse etiology and location…”19 and the following four associated features:
- episodes are inappropriate to the situation and can be precipitated by nonspecific stimuli, such as contraction of facial muscles, removal of bedcovers, or the approach of someone toward the patient
- there is no close correlation between the patient’s emotional expression and how he or she is feeling
- Episodes are relatively stereotyped in that each episode follows a similar pattern of building up paroxysmally or stepwise to a maximum peak, then decreasing slowly, and it is difficult for patients or others to control their extent or duration
- there are no episodic mood changes corresponding to the episodes and no sense of relief as the affects are expressed.
The last criterion gives the impression that the episodes appear from nowhere and are out of context with any outside stimuli. However, this is often not the case, and the stimuli inducing the response may be appropriate but trigger an exaggerated response.36
Criteria formulated by Cummings et al
Cummings et al have published criteria for involuntary emotional expression disorder (IEED), a term aimed at encompassing a broader set of disruptions of emotional expressions beyond simply laughing and crying; the term IEED also tried to clarify the distinction between mood and affect (expression of emotions).20 The following are the IEED criteria:
- episodes of involuntary or exaggerated emotional expression that result from a brain disorder, including episodes of laughing, crying, or related emotional displays, with the associated features of episodes representing a change from the person’s usual emotional reactivity; episodes may be inconsistent with the person’s mood or in excess of the corresponding mood state; and episodes are independent or in excess of any provoking stimulus (ie, crying regardless of whether the person is currently sad, happy, or other)
- repetitive episodic disturbances cause clinically significant distress or impairment in social or occupational functioning
- symptoms are not better accounted for by another neurological or psychiatric disorder (eg, gelastic or dacrystic epilepsy, facial dystonia, facial or vocal tics, facial dyskinesias, mania, depression, panic disorder, psychosis)
- the symptoms are not the direct physiological effect of a substance (eg, drug of abuse or medication).
Cummings et al also detailed descriptive characteristics of and observations supporting a diagnosis of IEED. In a subsequent publication, Rosen and Cummings emphasized three major criteria for PBA:
- Episodes that are inconsistent with or are greatly exaggerated compared with what the patient is feeling
- Episodes with a paroxysmal quality at onset and that often occur in an inappropriate context
- A “wait-out” period that must occur before the patient can return to his or her pre-episode activities (typically a few seconds or minutes).36
Comparing and contrasting criteria
Many publications on criteria for PBA, including Poeck’s, suggest that no specific incident provokes episodes of PBA. However, this notion is controversial, and several authors, including Rosen and Cummings, suggest that triggers may be present.36 In a study by McGrath, approximately half of the individuals reporting laughing or crying episodes following acquired brain injury were able to name precipitants for the episodes. These included separation from and thoughts of family, films or television, talking about the situation, acts of kindness, religion, and frustration.37 Regardless of whether the episodes are contextually appropriate or not, when the response is extreme and represents a new, lowered and uncontrolled threshold for laughing and crying, it should be considered pathological.31,36
The lack of consensus on the exact role of triggers in PBA should not overshadow the fact that there are several key diagnostic criteria on which authors agree. These include that episodes are involuntary, are unpredictable, and come on suddenly, possibly without warning signs. In addition, the episodes are excessive, exaggerated, stereotypical, or not appropriate to any provoking stimuli.
Distinguishing PBA from other consequences of TBI
PBA symptoms may coexist or be confused with other symptoms and conditions that can occur in those with TBI. While collectively these constitute significant diagnostic challenges, a thorough and accurate history should make identification of PBA straightforward.
Distinguishing PBA from depression
Depression is a common misdiagnosis of PBA, since crying may be automatically assumed to be a symptom of depression. A crucial diagnostic point in this regard is that affect (eg, crying) in depression is proportional to and consistent with pervasive feelings of sadness or low mood.27
Crying episodes in depression are typically not described as having the sudden, frequent, involuntary, and out of control nature of PBA crying episodes. Unlike depression, mood changes associated with PBA episodes do not typically extend beyond the outburst itself. In some cases, the PBA crying (and/or laughter) may be triggered by a physical or emotional event (eg, by a health care provider’s questions about previous episodes) rather than the patient’s mood.19 Also, in PBA the crying event may be described as something that the patient has to “wait out”36 and is typically brief. In contrast with depression, people with PBA often communicate a sense of bewilderment, aggravation, or lack of control regarding their laughing or crying with resulting embarrassment or frustration.
The essential features of depression are a persistently depressed mood or sustained loss of interest or pleasure. However, the clinical picture in patients after TBI may be complicated if they also have had other symptoms commonly associated with both TBI and depression, such as cognitive impairment, apathy, sleep impairment, and social withdrawal. In addition, PBA and depression may coexist, and the presence of depressive symptoms by no means rules out the possibility of PBA.
Distinguishing PBA from PTSD
Signs of PBA may be confused with those of PTSD due to the sudden loss of emotional control occurring in both conditions. However, major signs suggesting PTSD are the presence of fear, flashbacks, and persistent re-experiencing of the traumatic event, avoidance, hypervigilance/hyperarousal, and nightmares.16 A person may report that they saw something (or someone) that reminded them of the traumatic event, which, in turn, triggered the emotional outburst. With PTSD, the person should communicate having a clear connection between their subjective emotional reactions and the outburst. With PBA, this connection is typically absent. Often, the person may not have any emotional reason for the outburst of laughing or crying.
Other diagnostic challenges
Identification of PBA and the clinical features that distinguish it from other symptoms or comorbidities in TBI obviously relies heavily on the patient’s ability to communicate. For example, some individuals with severe TBI may not be able to recognize and describe their mood in order to differentiate whether the episodes of crying or laughing are appropriate or inappropriate. Also, identification of PBA in some individuals with TBI may be complicated by symptoms of PBA first emerging or being recognized some months after the initial injury.
Particular diagnostic challenges are posed by those patients who have outbursts of laughter inappropriately or out of proportion to any stimuli. While this can certainly be a clue to the presence of PBA, inappropriate laughing may also suggest Witzelsucht, a rare condition following frontal lobe damage in which the affected person finds situations inappropriately funny when others do not, makes puns, and commonly presents with hypersexuality (see Table 1).38 Inappropriate laughter in PBA could also be misinterpreted as indicating the patient is “cheerful” and coping with or making light of their problems, with consequent delays in diagnosis.
Treatment
If PBA is present and symptoms cause significant stress or social impairment for the patient, then treatment may be warranted. Although antidepressants have been used traditionally as treatment for PBA, currently dextromethorphan and quinidine (DMQ; marketed as Nuedexta®, Avanir Pharmaceuticals, Inc, Aliso Viejo, CA, USA) is the only pharmaceutical that is approved by the US Food and Drug Administration and European Medicines Agency for the treatment of the condition.
In the principal randomized controlled trial of DMQ, daily PBA episode rates were reduced by nearly 50% over placebo and by 76% over baseline. PBA remission was also significantly higher when compared with placebo (51% and 29%, respectively).39,40 In clinical trials of patients with multiple sclerosis or amyotrophic lateral sclerosis, the most frequently reported adverse events occurring with an incidence of at least 10% and at least twice that seen with placebo were diarrhea (13%) and dizziness (10%).39
Although the 10 mg quinidine dose in DMQ is well below the antiarrhythmic dose, the drug can cause mild QT prolongation. An electrocardiogram is recommended in patients with cardiovascular risk factors (such as left ventricular hypertrophy or dysfunction), in those taking other drugs that prolong QT interval, and for those taking cytochrome P450 3A4 inhibitors that could elevate quinidine levels.
Antidepressants have also shown some benefits as treatment for PBA, but none have been formally studied for US Food and Drug Administration approval. In small, placebo-controlled trials (≤28 participants), the use of selective serotonin reuptake inhibitors and/or tricyclic/heterocyclic antidepressants have shown benefits. However, there is currently only one larger-scale study by Choi-Kwon et al (n=91) showing improvement (measured by a decreased score on the visual analog scale) in excessive or inappropriate laughing or crying in patients having post-stroke emotional incontinence with the use of fluoxetine.41 These patients were followed for 6 months, and it was reported that those taking fluoxetine dropped out more often because of adverse events when compared with placebo.
Returning to the case of JC, a diagnosis of PBA is likely present. Arriving at an accurate diagnosis would be expected to influence the selection of a management strategy tailored for this condition (eg, patient education, use of therapy), which may influence the effectiveness of the treatment and patient adjustment.
Conclusion
TBI is common and may have complex, life-changing consequences for those who survive the acute event. Many may develop depression or PTSD, and it is understandable that these well described and widely recognized conditions are often automatically assumed to explain frequent episodic crying in such individuals. However, this risks overlooking or mismanaging the significant proportion of patients who develop PBA following TBI.
Health care professionals must maintain awareness of this treatable condition in evaluating clinical scenarios where there may be multiple post-TBI complications with potentially overlapping symptoms. The list of key differential diagnoses in this setting is short, and there are useful practical steps that clinicians can take when assessing patients with such episodes. Foremost of these is to listen carefully to what the patients say, if they are able to describe their symptoms. Where, for example, their description (given either spontaneously or in response to direct questioning) includes the patient’s consistent and clear denial of having symptoms of low mood before or during the episodes, PBA needs to be considered as a possibility. Furthermore, this diagnosis has to be formally ruled out where a patient with confirmed or suspected depression experiences no improvement in the crying episodes when given antidepressant drug therapy.
Recognition of PBA may help patients and families in dealing with and seeking appropriate treatment for what can be frustrating and embarrassing symptoms. On the other hand, failure to identify PBA in the context of TBI through inadequate assessment means that the condition can continue to have major detrimental effects on the individual’s functioning, relationships, and quality of life, compounding the already considerable clinical and humanistic burden associated with TBI.
Acknowledgment
The authors would like to thank Dr Ike Iheanacho for his review and editorial assistance.
Disclosure
This project was commissioned and funded by Avanir Pharmaceuticals, Inc. The authors drafted the manuscript and are responsible for its content. Avanir Pharmaceuticals, Inc., provided editorial comments for author consideration. The authors had final control of the content, and the information presented and any views expressed are those of the authors.
References
Faul M, Xu L, Wald MM, Coronado V. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths, 2002–2006. Atlanta, GA, USA: Centers for Disease Control and Prevention; 2010. Available from: http://www.cdc.gov/traumaticbraininjury/pdf/blue_book.pdf. Accessed May 5, 2014. | ||
Langlois JA, Rutland-Brown W, Thomas KE. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths. Atlanta, GA, USA: Centers for Disease Control and Prevention; 2004. Available from: http://www.cdc.gov/ncipc/pub-res/TBI_in_US_04/TBI-USA_Book-Oct1.pdf. Accessed May 5, 2014. | ||
Rutland-Brown W, Langlois JA, Thomas KE, Xi YL. Incidence of traumatic brain injury in the United States, 2003. J Head Trauma Rehabil. 2006;21(6):544–548. | ||
Bombardier CH, Fann JR, Temkin NR, Esselman PC, Barber J, Dikmen SS. Rates of major depressive disorder and clinical outcomes following traumatic brain injury. JAMA. 2010;303(19):1938–1945. | ||
Hibbard MR, Uysal S, Kepler K, Bogdany J, Silver J. Axis I psychopathology in individuals with traumatic brain injury. J Head Trauma Rehabil. 1998;13(4):24–39. | ||
Jorge RE, Starkstein SE. Pathophysiologic aspects of major depression following traumatic brain injury. J Head Trauma Rehabil. 2005;20(6):475–487. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA, USA: American Psychiatric Publishing; 2013. | ||
Rottenberg J, Gross JJ, Wilhelm FH, Najmi S, Gotlib IH. Crying threshold and intensity in major depressive disorder. J Abnorm Psychol. 2002;111(2):302–312. | ||
Rottenberg J, Cevaal A, Vingerhoets AJ. Do mood disorders alter crying? A pilot investigation. Depress Anxiety. 2008;25(5):E9–E15. | ||
Andrew LB. Depression and suicide. Medscape, 2012. Available from: http://emedicine.medscape.com/article/805459-overview#showall. Accessed March 5, 2013. | ||
Lyness JM. Clinical manifestations and diagnosis of depression. UpToDate, Inc. Wolters Kluwer; 2013. Available from: http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-depression?source=search_result&search=4+neurovegetative&selectedTitle=1 ˜;15. Accessed March 5, 2013. | ||
Press D, Alexander M. Treatment of behavioral symptoms related to dementia. UpToDate, Inc. Wolters Kluwer; 2012. Available from: http://www.uptodate.com/contents/treatment-of-behavioral-symptoms-related-to-dementia?source=see_link. Accessed July 23, 2012. | ||
Vingerhoets AJ, Rottenberg J, Cevaal A, Nelson JK. Is there a relationship between depression and crying? A review. Acta Psychiatr Scand. 2007;115(5):340–351. | ||
Ciechanowski P, Katon W. Posttraumatic stress disorder: epidemiology, pathophysiology, clinical manifestations, and diagnosis. UpToDate, Inc. Wolters Kluwer; 2012. Available from: http://www.uptodate.com/contents/posttraumatic-stress-disorder-epidemiology-pathophysiology-clinical-manifestations-and-diagnosis?source=search_result&search=posttraumatic+stress+disorder&selectedTitle=2~109. Accessed July 24, 2012. | ||
Glaesser J, Neuner F, Lutgehetmann R, Schmidt R, Elbert T. Posttraumatic stress disorder in patients with traumatic brain injury. BMC Psychiatry. 2004;4:5. | ||
American Psychiatric Association. Anxiety disorders. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC, USA: American Psychiatric Association; 2000. | ||
Green RL, McAllister TW, Bernat JL. A study of crying in medically and surgically hospitalized patients. Am J Psychiatry. 1987;144(4):442–447. | ||
Vardi J, Finkelstein Y, Zlotogorski Z, Hod I. L’homme qui rit: inappropriate laughter and release phenomena of the frontal subdominant lobe. Behav Med. 1994;20(1):44–46. | ||
Poeck K. Pathophysiology of emotional disorders associated with brain damage. Handb Clin Neurol. 1969;3:343–367. | ||
Cummings JL, Arciniegas DB, Brooks BR, et al. Defining and diagnosing involuntary emotional expression disorder. CNS Spectr. 2006;11(6):1–7. | ||
House A, Dennis M, Molyneux A, Warlow C, Hawton K. Emotionalism after stroke. BMJ. 1989;298(6679):991–994. | ||
Kim JS, Choi-Kwon S. Poststroke depression and emotional incontinence: correlation with lesion location. Neurology. 2000;54(9):1805–1810. | ||
Moore SR, Gresham LS, Bromberg MB, Kasarkis EJ, Smith RA. A self report measure of affective lability. J Neurol Neurosurg Psychiatry. 1997;63(1):89–93. | ||
Rabins PV, Arciniegas DB. Pathophysiology of involuntary emotional expression disorder. CNS Spectr. 2007;12(4 Suppl 5):17–22. | ||
Sloan RL, Brown KW, Pentland B. Fluoxetine as a treatment for emotional lability after brain injury. Brain Inj. 1992;6(4):315–319. | ||
Wortzel HS, Oster TJ, Anderson CA, Arciniegas DB. Pathological laughing and crying: epidemiology, pathophysiology and treatment. CNS Drugs. 2008;22(7):531–545. | ||
Arciniegas DB, Lauterbach EC, Anderson KE, et al. The differential diagnosis of pseudobulbar affect (PBA). Distinguishing PBA among disorders of mood and affect. Proceedings of a roundtable meeting. CNS Spectr. 2005;10(5):1–14. | ||
Work SS, Colamonico JA, Bradley WG, Kaye RE. Pseudobulbar affect: an under-recognized and under-treated neurological disorder. Adv Ther. 2011;28(7):586–601. | ||
Parvizi J, Coburn KL, Shillcutt SD, Coffey CE, Lauterbach EC, Mendez MF. Neuroanatomy of pathological laughing and crying: a report of the American Neuropsychiatric Association Committee on Research. J Neuropsychiatry Clin Neurosci. 2009;21(1):75–87. | ||
Parvizi J, Anderson SW, Martin CO, Damasio H, Damasio AR. Pathological laughter and crying: a link to the cerebellum. Brain. 2001;124 Pt 9:1708–1719. | ||
Balakrishnan P, Rosen H. The causes and treatment of pseudobulbar affect in ischemic stroke. Curr Treat Options Cardiovasc Med. 2008;10(3):216–222. | ||
Colamonico J, Formella A, Bradley W. Pseudobulbar affect: burden of illness in the USA. Adv Ther. 2012;29(9):775–798. | ||
Brooks BR, Crumpacker D, Fellus J, Kantor D, Kaye RE. PRISM: a novel research tool to assess the prevalence of pseudobulbar affect symptoms across neurological conditions. PLoS One. 2013;8(8):e72232. | ||
Tateno A, Jorge RE, Robinson RG. Pathological laughing and crying following traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2004;16(4):426–434. | ||
Zeilig G, Drubach DA, Katz-Zeilig M, Karatinos J. Pathological laughter and crying in patients with closed traumatic brain injury. Brain Inj. 1996;10(8):591–597. | ||
Rosen HJ, Cummings J. A real reason for patients with pseudobulbar affect to smile. Ann Neurol. 2007;61(2):92–96. | ||
McGrath J. A study of emotionalism in patients undergoing rehabilitation following severe acquired brain injury. Behav Neurol. 2000;12(4):201–207. | ||
Mendez MF. Moria and Witzelsucht from frontotemporal dementia. J Neuropsychiatry Clin Neurosci. 2005;17(3):429–430. | ||
Pioro EP, Brooks BR, Cummings J, et al. Dextromethorphan plus ultra low-dose quinidine reduces pseudobulbar affect. Ann Neurol. 2010;68(5):693–702. | ||
ClinicalTrials.gov. Safety and efficacy of AVP-923 in PBA patients with ALS or MS (STAR). Available from: http://clinicaltrials.gov/ct2/show/results/NCT00573443?term=pseudobulbar&rank=6§=X0125#all. Accessed November 7, 2013. | ||
Choi-Kwon S, Han SW, Kwon SU, Kang DW, Choi JM, Kim JS. Fluoxetine treatment in poststroke depression, emotional incontinence, and anger proneness: a double-blind, placebo-controlled study. Stroke. 2006;37(1):156–161. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.