")
Back to Journals » International Journal of General Medicine » Volume 14
Diabetes Mellitus and Marital Status: Evidence from the National Longitudinal Mortality Study on the Effect of Marital Dissolution and the Death of a Spouse
Authors Kposowa AJ , Aly Ezzat D, Breault K
Received 26 February 2021
Accepted for publication 12 April 2021
Published 17 May 2021 Volume 2021:14 Pages 1881—1888
DOI https://doi.org/10.2147/IJGM.S307436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Augustine J Kposowa,1 Dina Aly Ezzat,2,3 Kevin Breault4
1Department of Sociology, University of California, Riverside, CA, 92521, USA; 2Department of Sociology, California State University, San Bernardino, CA, 92407, USA; 3Department of Sociology, Assiut University, Assiut, Republic of Egypt; 4Department of Sociology, Middle Tennessee State University, Murfreesboro, TN, 37132, USA
Correspondence: Augustine J Kposowa
Department of Sociology, University of California, Riverside, CA, 92521, USA
Tel +1-951-456-5425
Email [email protected]
Purpose: This study evaluates the full impact of marital status on diabetes mellitus by stratifying the analysis by gender, including socioeconomic covariates and, unlike most studies, extending marital status by separating out previously conflated status categories.
Methods: Release 5 of the National Longitudinal Mortality Study (NLMS) was used for the data. Logistic regression was applied to the data from 1990 to 2011. The effective sample size consists of 1,384,507 individuals age 18 and above recruited into the study (via the Current Population Surveys), 3,955 of whom had died of diabetes mellitus by 2011.
Results: For minority men and non-Hispanic white men, divorced/separated status was significantly related to diabetes mortality, respectively (OR=1.318, CI=1.010, 1.719; and OR=1.283, CI=1.054, 1.562). For minority women and non-Hispanic white women, widowed status was related to diabetes mortality, respectively (OR=1.349, CI=1.107, 1.643; and OR=1.262, CI=1.113, 1.431).
Conclusion: Contrary to recent epidemiological studies in which divorced/separated and widowed status were combined into one covariate, this United States study finds that divorced/separated men and widowed women are at increased risk for diabetes mellitus mortality, and that among these populations at risk, minorities are at higher risk than whites. The study highlights the importance of marital status and gender differences in the risk of death from diabetes.
Keywords: diabetes, gender, divorced, widowed, socioeconomic disparities
Introduction
Diabetes Mellitus is one of the top ten causes of death in the United States. Thirty-four million people had the disease in 2017, and it is estimated that the annual cost of diabetes in the US is 327 billion dollars.1 In addition, the risk of early death among adults with diabetes is 60% higher than those without the condition, 88 million people in the United States have prediabetes, and more than 80% of them do not know they have the disease.1,2 Moreover, diabetes is a growing worldwide concern with the most rapid increase among low- and middle-income countries.3 Among other factors, genetics, being overweight or obese, and stress in the form of socioeconomic disparities have been implicated as causes.1,2 Notably in the US, while 7.5% of non-Hispanic whites have diabetes, non-Hispanic African Americans, Hispanics, and American Indians/Alaskan Natives are between 56 and 96% more likely to be affected.2 Less understood is the role of marital status in the disease and as a cause of death. Specifically, divorce/separated and widowed status are viewed as among the most stressful of life events but have not been fully explored with diabetes mortality.4,5 This study evaluates the relationship between marital status and diabetes mellitus mortality by stratifying gender, and including socioeconomic covariates.
At least as far back as 1897, martial statuses different from the married have been implicated in morbidity and mortality.6 More recent data has extended the research with the finding that social support, influence and regulation work to reduce the morbidity and mortality of those who are married.7,8 While research on marital status and some forms of morbidity and mortality has employed the full range of marital statuses,9,10 that generally has not been the case with diabetes research. In addition, work on marital status and diabetes has been mixed. In diabetes research in the United States, socioeconomic status has been strongly related to mortality when divorced/separated and widowed statuses were combined into one covariate.11 Similarly, single status was related to diabetes morbidity among African American women and diabetes mortality in African American men without separating out divorced/separated from widowed status.12
In two recent studies based on samples from Iran, single status and a combined covariate of divorced and widowed statuses were not related to the prevalence of diabetes in a group of variables that included gender and educational attainment;13 and in research on diabetes, hypertension, cardiovascular disease and all-cause mortality, widowed women had a lower risk of diabetes mortality.14 Finally, in a recent study based on a population in Brazil that included race and socioeconomic factors, only a combined covariate of divorce and the widowed was significantly related to the incidence of diabetes.15 More generally, it is common in the morbidity, mortality and obesity literature for researchers to combine divorced/separated and widowed status into one covariate.
Materials and Methods
Sample
Data were obtained from version 5 of the NLMS released in October 2015, a mortality study involving non-institutionalized persons in the United States.16 Sponsored by the US Census Bureau and the National Center for Health Statistics, the National Longitudinal Mortality Study (NLMS) is a database established to study demographic and socioeconomic disparities among causes of mortality in the US A multistage stratified sample, it includes data from the Current Population Surveys (CPS) and the Annual Social and Economic Supplements (ASES). The data comprise almost 1.4 million records and 160,750 cases of all-cause mortality. Full information about the CPS and ASES has been previously presented.17,18
We use the NLMS Public Use Microdata Sample (PUMS) which is an extract of the full NLMS for purposes of analyses and ensuring the confidentiality of respondents.16 Death certificates from April 1, 1990 to April 30, 2011 were used and link those in the CPS to mortality information available in the National Death Index (NDI) of the National Center for Health Statistics. The NDI includes deaths happening in the United States and gives researchers a way of providing mortality data in epidemiological studies. Complete information on the NDI has been previously discussed in detail.19 Mortality was studied from 1990 to 2011, and the follow-up period included 4,018 days or 11 years, 2000–2011. Only those 18 years old and older were studied because that is the age at which all can legally marry in the US. The age restriction led to 1,384,507 individuals at the outset, 3,955 of whom died of diabetes mellitus during the follow-up time. To estimate mortality risk from diabetes, those alive after 4,018 days of follow-up, and those who died of different causes were considered right censored observations. All individuals including cases of all-cause mortality and the 3,955 who died of diabetes mellitus were included in the study. Only persons below the age 18 were excluded.
Measurements
The dependent variable was diabetes mellitus, identified by codes E08, E11, and E13 from the International Statistical Classification of Diseases, ie, death from diabetes mellitus (E11), with specified underlying conditions such as cancer and pancreatitis (E080), and other specified diabetes mellitus conditions including genetic defects (E11), obtained from the CDC standardized death certificate form.20 Dummy variables were used. Marital status was measured by divorce/separated, single/never married, and widowed. Race/ethnicity included non-Hispanic African Americans, Non-Hispanic Asians, Non-Hispanic Native Americans, and Hispanics. For some analyses, to avoid the problem of small cell size, the race and ethnic groups were collapsed into Non-Hispanic White Men, Minority Men, Non-Hispanic White Women and Minority Women. Place of Residence was measured by those living in cities and suburban areas within SMSAs. Housing Tenure was measured by whether the respondent owned or rented. Educational Attainment was measured by those with less than high school education, and some colleges or higher. Annual Family Income adjusted for inflation included those below $20,000, $20,000–29,999, $30,000–39,999, $50,000–59,999, and family income greater than $59,999. Age was measured by those 45–64 years, and 65 years and above. Independent variables were measured at baseline, and follow-up effects on diabetes mortality were estimated.
Statistical Analysis
Parameters were estimated with the use of logistic regression, and estimates were exponentiated to arrive at odds ratios along with 95% confidence intervals. The LOGISTIC procedure in SAS version 9.4 was utilized.21 In the case of logistic and Cox proportional hazards regression on longitudinal data, if the variables are related to the follow-up period, results for the procedures may be different.22,23 In these data, there were no relevant relationships between the variables and follow-up, and in the analyses reported here the logistic model was used. However, similar proportional hazards results are available upon request.
Results
As may be seen in Table 1, which is based on the descriptive statistics from the entire sample, divorce/separated and widowed status were significantly related to diabetes mortality, respectively (OR=1.147 [95%] CI=1.026, 1.282; and OR=1.262, CI=1.159, 1.374). As expected, the socioeconomic covariates, renting housing tenure, less than high school, high school educational attainment, and family income were consistent with the existing literature. Similarly, the race/ethnicity covariates of non-Hispanic African American, non-Hispanic American Indian/Alaskan Native, and Hispanic were significantly related to diabetes mortality.
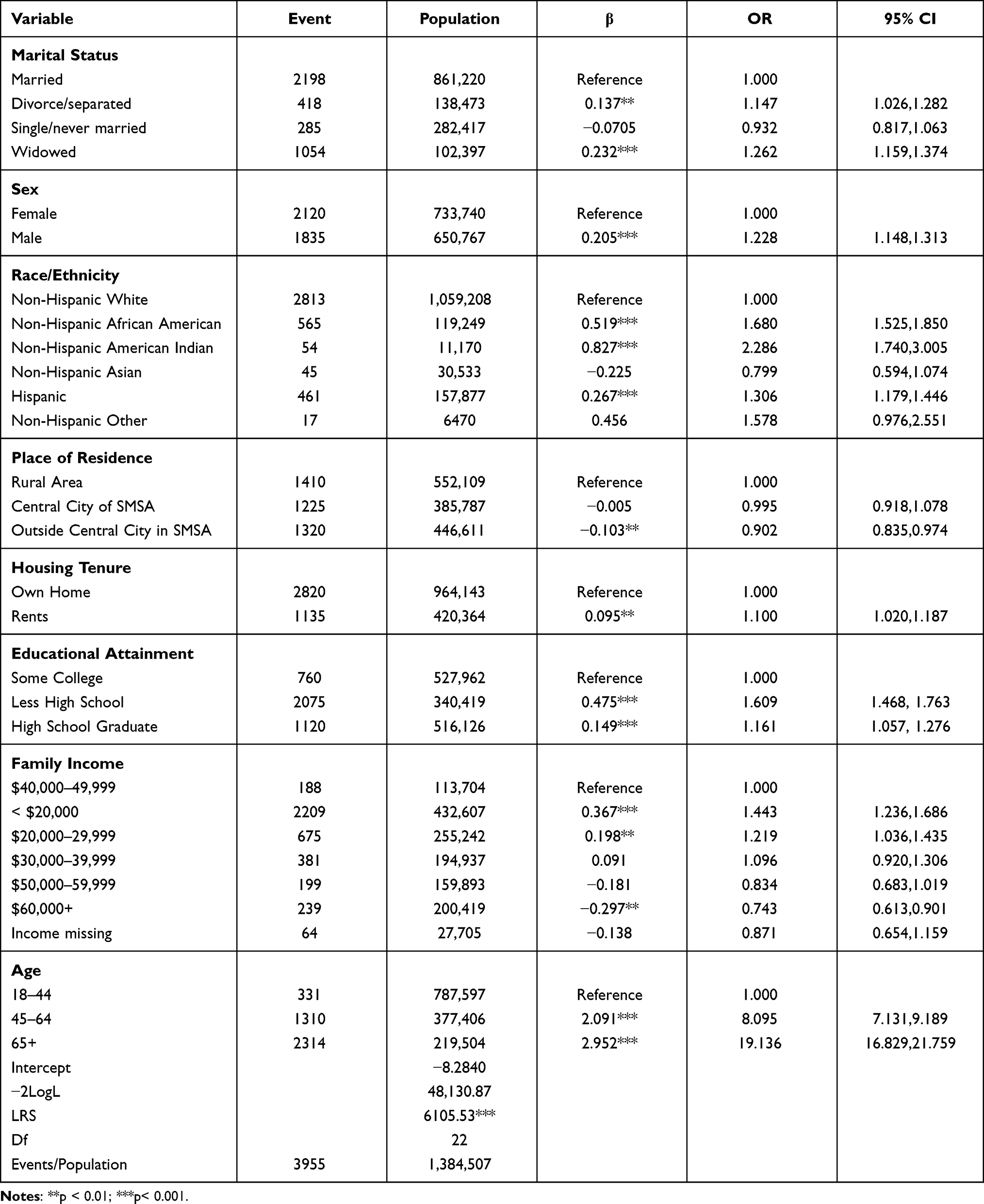 |
Table 1 Descriptive Statistics and the Effect of Marital Status on Diabetes Mellitus, Entire Sample, National Longitudinal Mortality Study, 1990–2011 |
Tables 2 and 3 stratify the analysis by gender and separate minority from non-Hispanic white men and women. For minority men and non-Hispanic white men (Table 2), the divorced/separated were significantly related to diabetes mortality, respectively (OR=1.318 [95%] CI =1.010, 1.19; and OR=1.283, CI=1.054, 1.562). For minority women and non-Hispanic white women (Table 3), the widowed had significant risks for mortality, respectively (OR=1.349, [95%] CI=1.107, 1.643; and OR=1.262, CI=1.113, 1.431, respectively). The socioeconomic covariates in the stratified samples (Tables 2 and 3) were comparable with those in the entire sample (Table 1) with some exceptions. Renting as opposed to owning was only significant for non-Hispanic white women; high school attainment was only significant for minority men; and minority men and women compared to white men and women in the highest family income category were not significantly less likely to die of diabetes.
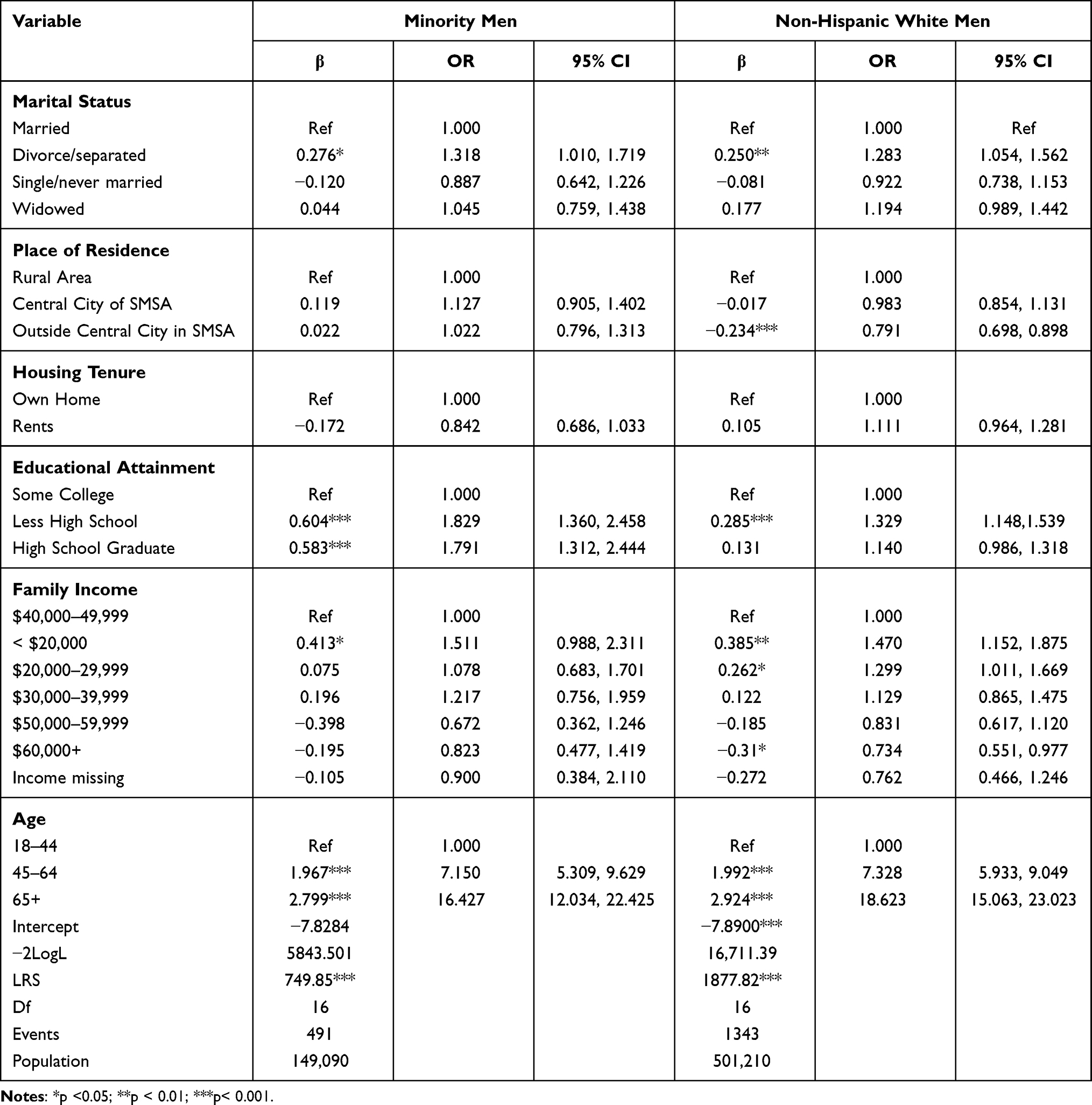 |
Table 2 Minority Men and Non-Hispanic White Men: Effect of Marital Status on Diabetes |
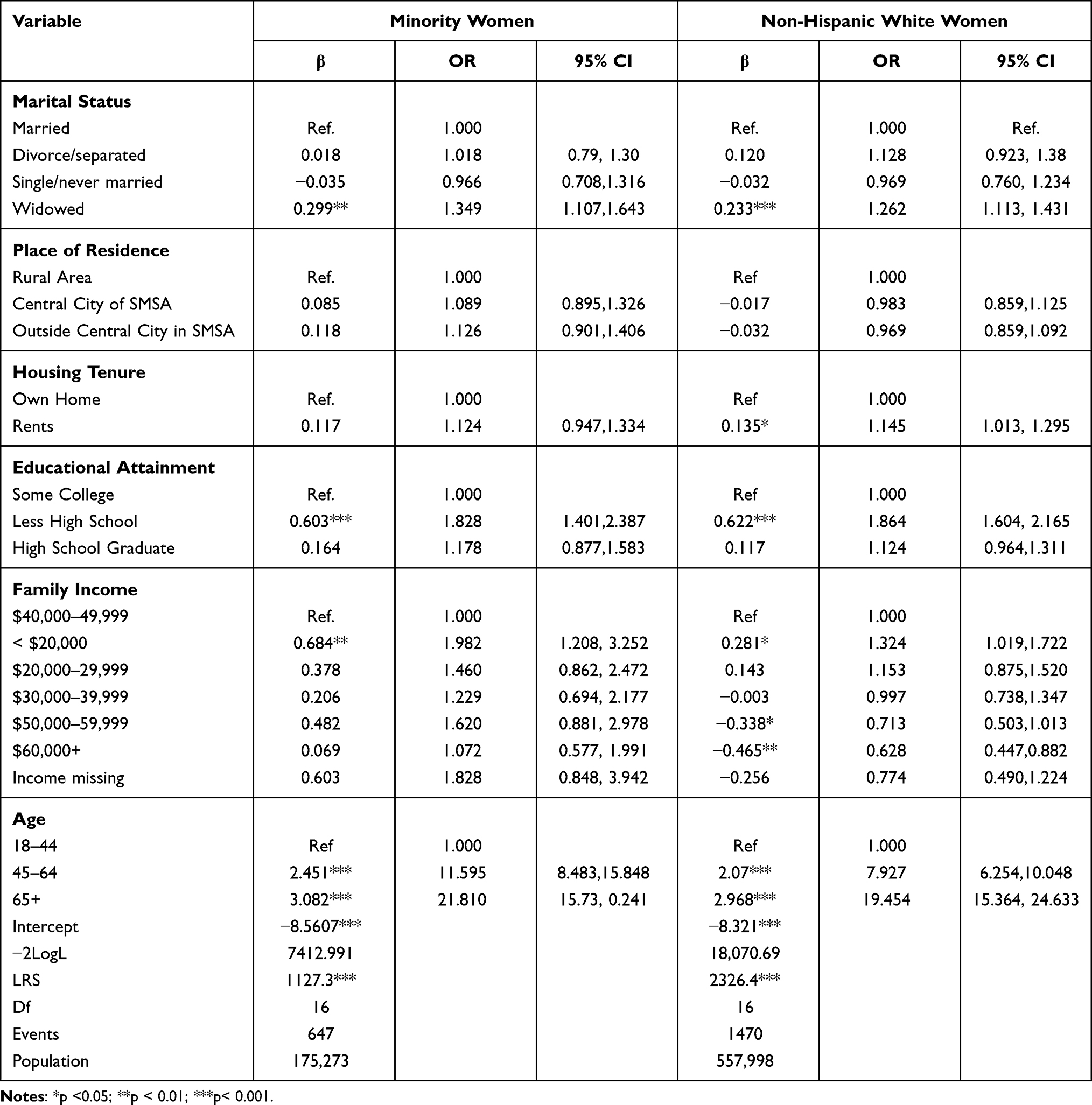 |
Table 3 Minority Women and Non-Hispanic White Women: Effect of Marital Status on Diabetes |
Discussion
This study shows that it is important to separate out marital status into at least four categories: married, single/never married, divorced/separated and widowed, and to stratify by gender. The different marital status findings by gender in this study were unexpected and novel. It is especially important to separate out the divorce/separated from the widowed because the ages of the two statuses tend to be different. For example, in the United States, the average age for divorce is 30, while the mean age for widowhood is 59. The large sample size of the NLMS and its longitudinal nature allows for a better understanding of marital status and provides for relevant socioeconomic covariates.
The different ages for the divorced/separated compared to the widowed are likely responsible for these findings that men (both minority and non-Hispanic whites) who are divorced/separated have increased risk for diabetes, and women (minority and non-Hispanic whites), who are widowed are at increased diabetes risk. Married men may have the social support of their spouses and the social control marriage can provide with regard to eating responsibly; and without that support and control men may be at higher risk for unhealthy eating leading to obesity.24,25 Accordingly, women may be less likely to overeat after divorce because they have been more focused on the importance of healthy eating during marriage. Widowed women have fewer partnering opportunities than the divorced/separated, and they may cope with the loss of a spouse by overeating. Compared to widowed men, women have larger friendship networks that often include social gatherings involving food at which overeating is a risk.26,27 Some widowed men, on the contrary, are more likely to cope with the loss of a spouse by engaging in more dangerous activity leading to early morbidity and mortality related to alcohol and drug use, accidents, homicide and suicide.28,29
Our findings should be viewed in the context of some potential limitations. First, research has generally indicated that diabetes is underreported as a cause of death. Death certificates may not include diabetes as a cause of death because certifying physicians did not know or believe it was a cause, the decedent had other diseases thought to be more causally important, and death certificates have limited space for recording death.30 As with some other causes of death, this evidence suggests that reported diabetes deaths, if not a measure of all diabetes mortality, are nevertheless a good measure of death from the most serious diabetes, and diabetes morbidity that is less complicated by different causal understanding of atherosclerotic and hypertensive cardiovascular disease. More research is needed on the chain of causality in diabetes morbidity. However, it is important to understand that we must not minimize the fact that many people with diabetes die of other causes, especially cardiovascular disease and cancer.
Second, because of limitations of the NLMS data, the effects of genetics and health variables could not be estimated in this research. This study, based on the largest US sample, focused on the importance of marital statuses–and the full spectrum of marital statuses–in diabetes mellitus and found high mortality risk for large populations of people: divorced/separated minority and white men, and widowed minority and white women. Going forward, additional work on marital status and diabetes is indicated.
Finally, while we were able to separate out divorced/separated status from the widowed, the data do not allow us to separate the divorced from those who are separated. Divorce is quite distinct from separation. Separation can be of an extended amount of time and be a source of considerable stress. Researchers can also conflate separated and single status when it comes to identifying different marital statuses. As noted, in this study, divorced/separated and single/never married were different covariates.
Conclusion
This study examined diabetes mortality with the findings that the marital statuses of divorce/separated and widowed were differentially related when gender was stratified. Unlike most recent studies in which divorced/separated and widowed status were combined into one covariate, this research on the most recent version of the NLMS covering nearly 1.4 million deaths finds that divorced/separated men and widowed women are at increased risk for diabetes mortality. Specifically, minority men and non-Hispanic white men who were divorced/separated had significantly higher risk for death from diabetes mellitus, a 43 and 28% increase, respectively; and minority women and non-Hispanic white women who were widowed had a similarly high risk for diabetes mortality, a 35 and 26% corresponding increase, respectively. In addition to previous work on socioeconomic disparities, this study highlights the importance of marital status and gender differences in the risk of death from diabetes.
Ethical Approval and Informed Consent
Research for this study did not require an institutional review board or ethics committee. NLMS data are publicly available to researchers on the World Wide Web and all the data are anonymized prior to release. Without identifying information consent was not needed.
Acknowledgments
The US Bureau of the Census and the National Center for Health Statistics are gratefully acknowledged for providing the data for this research. The views and opinions presented in this paper do not necessarily reflect those of these institutions. We also thank the anonymous reviewers for their generous and constructive comments.
Disclosure
The authors report no conflicts of interest in this study.
References
1. American Diabetes Association. Economic costs of diabetes in the U.S. in 2017. Diabetes Care. 2018;41:917–928. doi:10.2337/dci18-0007
2. American Diabetes Association. The cost of diabetes[homepage on the Internet]. Available from: https://www.diabetes.org/resources/statistics/cost-diabetes.
3. World Health Organization [homepage on the Internet]. Available from: http://www.who.int/news-room/fact-sheets/detail/diabetes.
4. Booth A, Amato P. Divorce and psychological stress. J Health Soc Behav. 1991;32:396–407. doi:10.2307/2137106
5. Marks N, Lambert J. Marital status continuity and change among young and midlife adults: longitudinal effects on psychological well-being. J Fam Issues. 1998;19:652–6877. doi:10.1177/019251398019006001
6. Durkheim E. Suicide: A Study in Sociology. New York: Free Press; 1979.
7. Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Soc Sci Med. 2000;51:843–857. doi:10.1016/S0277-9536(00)00065-4
8. Johnson NJ, Backlund E, Sorlie PD, Loveless CA. Marital status and mortality: the national longitudinal mortality study. Ann Epidemiol. 2000;10:224–238. doi:10.1016/S1047-2797(99)00052-6
9. Molloy GJ, Stamatakis E, Randall G, Hamer M. Marital status, gender and cardiovascular mortality: behavioral, psychological distress and metabolic explanations. Soc Sci Med. 2009;69:223–228. doi:10.1016/j.socscimed.2009.05.010
10. Cheung YB. Marital status and mortality in British women: a longitudinal study. Int J Epidemiol. 2000;29:93–99. doi:10.1093/ije/29.1.93
11. Saydah S, Lochner K. Socioeconomic status and risk of diabetes-related mortality in the U.S. Public Health Rep. 2010;125:377–388. doi:10.1177/003335491012500306
12. Schwandt HM, Coresh J, Hindin MJ. Marital status, hypertension, coronary heart disease, diabetes, and death among African American women and men: incidence and prevalence in the Atherosclerosis Risk in Communities (ARIC) study participants. J Fam Issues. 2010;31:1211–1229. doi:10.1177/0192513X10365487
13. Azimi-Nezhad M, Ghayour-Mobarhan M, Parizadeh MR, et al. Prevalence of type 2 diabetes mellitus in Iran and its relationship with gender, urbanization, education, marital status and occupation. Singapore Med J. 2008;49:571–576.
14. Ramezankhani A, Azizi F, Hadaegh F. Associations of marital status with diabetes, hypertension, cardiovascular disease and all-cause mortality: a long term follow-up study. PLoS One. 2019;14:1–15. doi:10.1371/journal.pone.0215593
15. de Oliveira CM, Tureck LV, Alvares D, et al. Relationship between marital status and incidence of type 2 diabetes mellitus in a Brazilian rural population: the Baependi heart study. PLoS One. 2020;15:1–10. doi:10.1371/journal.pone.0236869
16. U.S. Bureau of the Census. Public Use Microdata Sample (PUMS) Release 5 Documentation. Washington: Department of Commerce; 2015.
17. Current Population Survey TP66 [homepage on the Internet]. Washington: U.S. Bureau of the Census; 2006. Available from: http://www.census.gov/prod/2006pubs/tp-66.pdf.
18. Redesign of the Sample for the Current Population Survey [homepage on the Internet]. Washington: U.S. Bureau of the Census; 2014. Available from: https://www.bls.gov/cps/sample_redesign_2014.pdf.
19. National Death Index Data Users’ Guide [homepage on the Internet]. Washington: National Center for Health Statistics; 2017. Available from: http://www.cdc.gov/nchs/ndi/index.htm.
20. World Health Organization. International Statistical Classification of Diseases and Related Health Problems.
21. SAS Institute. SAS/STAT Software. Cary: SAS Institute; 2018.
22. Selvin S. Statistical Analysis of Epidemiological Data. London: Oxford University Press; 1991.
23. Collett D. Modelling Survival Data in Medical Research. London: Chapman and Hall; 2003.
24. Eng PM, Kawachi I, Fitzmaurice G, Rimer EB. Effects of marital transitions on changes in dietary and other health behaviors in U.S. male health professionals. J Epidemiology Community Health. 2005;59:56–62. doi:10.1136/jech.2004.020073
25. Umberson D. Gender, marital status and the social control of health behaviors. Soc Sci Med. 1992;34:907–917. doi:10.1016/0277-9536(92)90259-S
26. Ross CE, Mirowsky J. Explaining the social patterns of depression: control and problem solving—or support and talking. J Health Soc Behav. 1989;30:206–219. doi:10.2307/2137014
27. Tucker JS, Schwartz E, Clark KM, Friedman HS. Age-related changes in the association of social network ties with morbidity risk. Psychol Aging. 1999;14:564–571. doi:10.1037/0882-7974.14.4.564
28. Stroebe MS, Stroebe W. Who suffers more? Sex differences in health risk of the widowed. Psychol Bull. 1983;93:279–301. doi:10.1037/0033-2909.93.2.279
29. Kposowa AJ, Ezzat DA, Breault K. New findings on gender: the effects of employment status on suicide. Int J Wom Health. 2019;11:569–575. doi:10.2147/IJWH.S216504
30. McEven LN, Kim C, Haan M, et al. Diabetes reporting as a cause of death: results from translating research into action for diabetes (TRIAD) study. Diabetes Care. 2006;29:247–253. doi:10.2337/diacare.29.02.06.dc05-0998
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.