")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 7
Diabetes and sexual dysfunction: current perspectives
Authors Maiorino MI, Bellastella G, Esposito K
Received 4 October 2013
Accepted for publication 5 November 2013
Published 6 March 2014 Volume 2014:7 Pages 95—105
DOI https://doi.org/10.2147/DMSO.S36455
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Maria Ida Maiorino,1 Giuseppe Bellastella,1 Katherine Esposito2
1Department of Medical, Surgical, Neurological, Metabolic and Geriatric Sciences, Second University of Naples, Naples, Italy; 2Department of Clinical and Experimental Medicine, Second University of Naples, Naples, Italy
Abstract: Diabetes mellitus is one of the most common chronic diseases in nearly all countries. It has been associated with sexual dysfunction, both in males and in females. Diabetes is an established risk factor for sexual dysfunction in men, as a threefold increased risk of erectile dysfunction was documented in diabetic men, as compared with nondiabetic men. Among women, evidence regarding the association between diabetes and sexual dysfunction are less conclusive, although most studies have reported a higher prevalence of female sexual dysfunction in diabetic women as compared with nondiabetic women. Female sexual function appears to be more related to social and psychological components than to the physiological consequence of diabetes. Hyperglycemia, which is a main determinant of vascular and microvascular diabetic complications, may participate in the pathogenetic mechanisms of sexual dysfunction in diabetes. Moreover, diabetic people may present several clinical conditions, including hypertension, overweight and obesity, metabolic syndrome, cigarette smoking, and atherogenic dyslipidemia, which are themselves risk factors for sexual dysfunction, both in men and in women. The adoption of healthy lifestyles may reduce insulin resistance, endothelial dysfunction, and oxidative stress – all of which are desirable achievements in diabetic patients. Improved well-being may further contribute to reduce and prevent sexual dysfunction in both sexes.
Keywords: diabetes mellitus, diabetes complications, erectile dysfunction, female sexual dysfunction, lifestyle changes
Introduction
Diabetes mellitus is one of the most common chronic diseases in nearly all countries; it is increasing rapidly in every part of the world, to the extent that it has now assumed epidemic proportions. In 2012, more than 371 million people had diabetes,1 and this is expected to rise to 552 million by 2030,2 rendering previous estimates very conservative.
Several behavioral and environmental factors have contributed to the rise in diabetes incidence in industrialized countries, including overweight (body mass index [BMI], ≥25 kg/m2), obesity (BMI, ≥30 kg/m2), physical inactivity, and increased caloric consumption; these have all been shown to be major risk factors for the development of type 2 diabetes, regardless of age and sex.3
In the US, diabetes is the sixth leading cause of death for women and the fifth leading cause of death for men;4 it is also a leading cause of death in most developed countries.1 However, only a minority of people with diabetes die from diseases that are uniquely related to the condition – about 50% of people with diabetes die of cardiovascular disease (CVD), and 10%–20% die of renal failure.5
Diabetes mellitus is associated with both macrovascular (including CVD) and microvascular (including retinopathy, nephropathy, and neuropathy) complications.6,7 People with diabetes are at a greater risk of developing CVDs, such as heart attack and stroke. The increased risk of CVD results, in part, from CVD risk factors that commonly accompany diabetes mellitus,8 as type 2 diabetes is associated with clustered risk factors for coronary heart diseases (CHD) including hypertension, elevated low-density lipoprotein-cholesterol (LDL), and obesity.9 Diabetic patients also have elevated risk for sight loss, foot and leg amputation, and renal failure, due to microvascular complications, which cause damage to the nerves and blood vessels.10,11
Diabetes has been associated with sexual dysfunction both in men12–14 and in women.15–17 Diabetes is an established risk factor for sexual dysfunction in men; a threefold increased risk of erectile dysfunction (ED) was documented in diabetic compared with nondiabetic men.12,18 Among women, the evidence regarding the association between diabetes and sexual dysfunction is less conclusive,19,20 although most studies have reported a higher prevalence of female sexual dysfunction (FSD) in diabetic women as compared with nondiabetic women.15,16,21
It is still not clear whether hyperglycemia, which is a main determinant of vascular diabetic complications, may participate in the pathogenetic mechanisms of sexual dysfunction in diabetes. On the other hand, diabetic people may present with several clinical conditions, including hypertension, overweight and obesity, metabolic syndrome, cigarette smoking, or atherogenic dyslipidemia, which are themselves risk factors for sexual dysfunction in both sexes.22–27
Erectile dysfunction
ED is defined as the persistent inability to achieve or maintain penile erection for successful sexual intercourse,28 causing decreased quality of life in men.29,30 ED is a common sexual disorder that increases with age. According to a recent analysis of published works on the prevalence of sexual dysfunction by the International Consultation Committee for Sexual Medicine on Definitions/Epidemiology/Risk Factors for Sexual Dysfunction,24 the prevalence of ED was 1%–10% in men younger than 40 years, 2%–9% among men between 40 and 49 years, and it increased to 20%–40% among men between 60–69 years, reaching the highest rate in men older than 70 years (50%–100%). In the Massachusetts male aging study,12 diabetic men showed a threefold probability of having ED than men without diabetes; moreover, the age-adjusted risk of ED was doubled in diabetic men compared with those without diabetes.31 In addition, it has been estimated that the worldwide prevalence of ED will rise to 322 million cases by the year 2025.32,33 Several cross-sectional and longitudinal studies showed an association between ED and most of the cardiovascular risk factors, such as diabetes,12,29,34 smoking,35 hypertension,36 hyperlipidemia,37 metabolic syndrome,23 as well as depression,38 lower urinary tract symptoms,39 and poor health state.29 Moreover, ED is a marker of significantly increased risk of CVD,40 CHD, stroke, and all-cause mortality.41–43 ED can be easily detected by having male patients complete standardized questionnaires investigating their sexual function. One of the most practical questionnaires that is administered is the International Index of Erectile Function (IIEF)-5,44 which consists of items 5, 15, 4, 2, and 7 from the full-scale IIEF-15; a sum score of 21 or less indicates the presence of ED.
ED and diabetes: risk factors and association
Epidemiological studies suggest that both type 1 and type 2 diabetes are associated with an increased risk of ED, which is reported to occur in ≥50% of men with diabetes worldwide.36,45 In the Massachusetts male aging study,12 diabetic men showed a threefold probability of having ED when compared to men without diabetes; moreover, the age-adjusted risk of ED doubled in diabetic men when compared to those without diabetes.31 Most of the studies that described the prevalence of ED in diabetes did not distinguish between type 1 and type 2 diabetes. Two studies46,47 reported a similar likelihood of having ED among both type 1 and type 2 diabetic men, whereas another report48 showed a higher risk of developing ED in men with type 1 diabetes. The occurrence of ED is 10–15 years earlier in men with diabetes;12 moreover, ED is more severe13 and less responsive to oral drugs49,50 in diabetes, leading to reduced quality of life.13,30
Advanced age and longer duration of diabetes have been associated with an increased risk of ED in diabetic patients.18,24,48 Whether hyperglycemia is a risk factor for the development of ED in diabetic men is still not clear. Some observational studies have shown an association between poor glycemic control, expressed by elevated levels of glycated hemoglobin (HbA1c), and ED,13,18 whereas other studies did not report any association.51,52 The different methodological approaches used in the different studies may explain, at least in part, these divergent results. Moreover, diabetes is commonly associated with hypertension, hyperlipidemia, overweight and obesity, metabolic syndrome, smoking, sedentary lifestyles, and autonomic neuropathy, which are recognized as risk factors for ED.34–37,53 Both microvascular51,54,55 and macrovascular48,56,57 diabetic complications also increase the risk of ED in diabetic men. The use of several medications frequently assumed by diabetic patients, such use of antihypertensive drugs (β-blockers, thiazide diuretics, and spironolactone), psychotropic drugs (antidepressants), and certain fibrates, have all been associated with an additive deleterious effect on diabetic ED.58,59 A moderate consumption of alcohol (not more than 5% of the total daily caloric intake, or ≤7 alcoholic drinks per week) may exert a protective effect on ED in both the general population and in diabetic men.37,47
Pathogenesis of ED in diabetes
The pathogenesis of ED in diabetes is multifactorial, as it depends on both psychological and organic factors (which play major roles in ED), as well as psychological and relationship issues, which often coexist. The proposed mechanisms of ED in diabetic patients are represented by vasculopathy, neuropathy, visceral adiposity, insulin resistance, and hypogonadism.
Diabetic vasculopathy concerns macroangiopathy, microangiopathy, and endothelial dysfunction. Macrovascular disease in diabetes corresponds to the atherosclerotic damage in the blood vessels, which limits blood flow to the penis. As mentioned, several cardiovascular risk factors associated with diabetes contribute to the genesis of penile arterial insufficiency: 23,35,36 all of them converge on endothelial dysfunction, which represents the common denominator leading to vascular ED.
The chronic insult of hyperglycemia on the endothelium results in endothelial dysfunction, which has been suggested as the link between ED and CVD.60 A diagnosis of ED may be seen as a sentinel event that should prompt the investigation of coronary artery disease (CAD) in asymptomatic diabetic men.61 Endothelial dysfunction in diabetes is manifested as the decreased bioavailability of nitric oxide (NO), resulting in insufficient relaxation of the vascular smooth muscle of the corpora cavernosa. The potential mechanisms involved in endothelial dysfunction include the accumulation of advanced glycation end products; increased levels of oxygen free radicals that reduce the bioavailability of NO; impaired endothelial and neuronal NO synthesis, expression, and activity; and an imbalance between the vasoconstrictive and vasorelaxant intracellular pathways favoring increased vasoconstriction.45,62 Esposito et al63 observed an increase in circulating endothelial microparticles – an emergent marker of endothelial dysfunction – in diabetic men with ED, as compared with nondiabetic men.
Microvascular disease determines ischemic damage in the distal circulation and autonomic and peripheral neuropathy. Both somatic and autonomic neuropathies may contribute to diabetes-induced ED due to the impairment of sensory impulses from the penis to the reflexogenic erectile center,64 and reduced or absent parasympathetic activity necessary for relaxation of the smooth muscle of the corpus cavernosum.65
Insulin resistance and visceral adiposity, which are both distinctive clinical traits of type 2 diabetes, are associated with a proinflammatory state that results in the decreased availability and activity of NO, leading to ED in overweight and obese diabetic men.66
Subnormal testosterone concentrations have been found in 25% of men with type 2 diabetes in association with inappropriately low luteinizing hormone (LH) and follicle-stimulating hormone (FSH) concentrations.67,68 Testosterone regulates nearly every component of erectile function, from pelvic ganglions to smooth muscle, and to the endothelial cells of the corpora cavernosa. It also modulates the timing of the erectile process, which occurs as a function of sexual desire, coordinating penile erection with sex. It is still unclear what level of testosterone is needed for good erectile function; however, evidence derived from clinical and molecular studies supports the use of testosterone replacement in hypogonadal patients with ED, although the benefit–risk ratio is uncertain in advanced age.69,70 The mechanisms involved in testosterone deficiency in diabetes include low levels of the sex hormone-binding globulin due to insulin resistance, increased aromatase activity in visceral adipose tissue leading to an augmented conversion of testosterone in estradiol, leptin resistance causing reduced secretion of LH and testosterone, and increased levels of inflammatory mediators, which may suppress the secretion of gonadotropin-releasing hormone and LH.62,71 Bellastella et al72 suggested a possible autoimmune pathogenesis of hypogonadotropic hypogonadism in type 2 diabetic patients, as indicated by the presence of antipituitary antibodies at high titers, as compared with age-matched controls.
Treatment of ED
As a consequence of its multifactorial etiology, the treatment of ED in diabetic men requires a global approach. The first step is to correct the modifiable risk factors and to promote lifestyle changes, whereas the use of phosphodiesterase 5 (PDE5) inhibitors represents first-line pharmacologic therapy (Table 1).
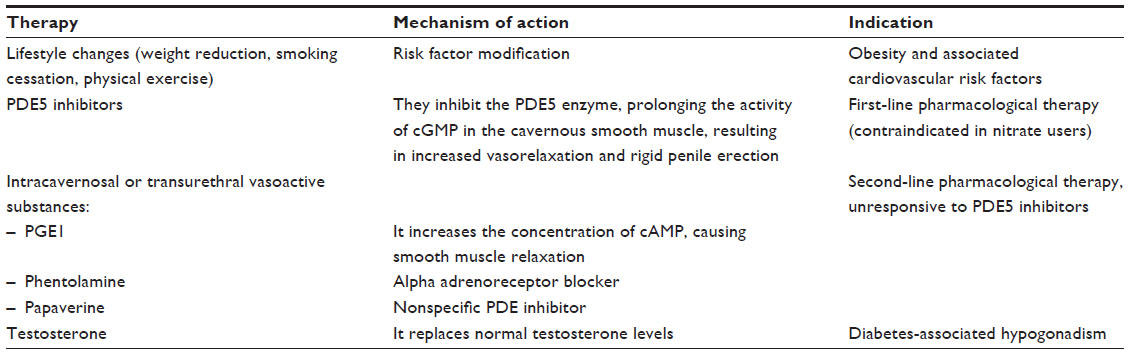 | Table 1 Summary of the behavioral and pharmacological therapies of erectile dysfunction in diabetes |
Glycemic control and lifestyle modifications
Tight glycemic control, so as to maintain an HbA1c concentration <7%, is recommended for all nonpregnant adults with diabetes to minimize the risk of long-term microvascular complications.73 Although several studies demonstrate an association between poor glycemic control and the risk of ED, it is still not clear whether intensive glycemic control may have beneficial effects on erectile function. Many cross-sectional studies have shown that better glycemic control is associated with improved erectile function.74,75 In an ancillary study of the Epidemiology of Diabetes Intervention and Complication Study (EDIC),76 a period of intensive therapy significantly reduced the prevalence of ED among men suffering from diabetes for 10 years or more and microvascular complications, compared with those with a 1- to 5-year history of disease, but without complications. In type 2 diabetic men, limited data have been reported on risk reduction interventions for ED, and these have had conflicting results.77,78 Further studies, including adequate sample size and validated ED measurements, are needed to clarify whether intensive glycemic control may produce benefits for erectile function in men with poor glycemic control.
Lifestyle changes, such as increased physical activity, a Mediterranean diet, and reduced caloric intake, have been associated with the amelioration of erectile function in the general male population. Esposito et al79 used their database of subjects participating in randomized controlled trials to evaluate whether improvements in erectile function were related to success in achieving lifestyle changes. After ranking men according to their success in achieving the goals of intervention (weight loss, low intake of saturated fat, high consumption of monounsaturated fat and fiber, and moderate physical activity), a strong correlation was observed between the success score and the restoration of erectile function. Moreover, at the 2-year examination point, the number of men without ED was significantly higher in the group randomized to intensive lifestyle changes compared with that of men in the control group. Wing et al80 evaluated 1-year changes in erectile function in 306 overweight men with type 2 diabetes mellitus participating in the Look AHEAD (Action for Health in Diabetes) trial; from baseline to 1 year, 8% of men assigned to the intensive lifestyle intervention reported a worsening of erectile function compared to 22% of the control participants. Moreover, the overall IIEF score improved from 17.3 to 18.6 (P=0.04 and P=0.06, after adjusting for baseline differences) in the intervention group. The suggested mechanisms by which weight loss, healthy diet, and physical exercise can improve erectile function include the amelioration of endothelial dysfunction, insulin-resistance, and low-grade inflammatory state associated with diabetes and metabolic diseases – all of which are risk factors for ED.81 In this vein, the resulting improved inflammatory status may help contribute to reduce the burden of sexual dysfunction in diabetic men.
Pharmacological therapy
Oral PDE5 inhibitors are considered the first-line treatment for ED.82,83 These drugs promote erection by inhibiting the PDE5 enzyme, which is responsible for the degradation of cyclic guanosine monophosphate (cGMP) in the cavernous smooth muscle. This inhibition leads to the prolonged activity of cGMP which, in turn, reduces intracellular calcium concentrations, maintains smooth muscle relaxation, and results in rigid penile erections. Sildenafil, vardenafil, and tadalafil are commercially available worldwide, while udenafil and mirodenafil are actually only used in Korea. These drugs differ in their time to onset and in their duration of action, but they show the same efficacy and safety profile. All of them have shown their efficacy in diabetic patients,84 although it has been reported that diabetic men with ED are less responsive to PDE5 inhibitors when compared with nondiabetic men with ED.85 A randomized, placebo controlled trial, involving 268 diabetic men with ED, reported improved erections in 56% of patients taking sildenafil in a dose-dependent manner, compared with 10% of those in the control group.86 In two other multicenter, placebo-controlled studies,87,88 treatment with vardenafil (10 mg and 20 mg), or tadalafil (10 mg and 20 mg), improved erections in 57% and 72%, and 56% and 64% of patients, respectively, as compared with improvements in 13% and 25% among those in the placebo arms. Diminished NO generation in the penile nerves and/or endothelium, as well as the low testosterone levels of diabetics, may be responsible for the reduced responsiveness to PDE5 inhibitor therapy.85 Moreover, findings from both experimental and clinical studies reported that chronic or daily use of PDE5 inhibitors for ED may significantly improve endothelial dysfunction.89–91 CHD is not an absolute contraindication for PDE5 inhibitors therapy, but particular caution has to be paid in cases of unstable and severe angina pectoris, recent myocardial infarction, certain arrhythmias, poorly controlled hypertension, and concomitant use of nitrates or nitrate donors: before starting therapy with PDE5 inhibitors, diabetic patients should undergo an overall cardiovascular examination.92
Intracavernosal injection of papaverine, phentolamine, and prostaglandin E1 (PGE1) (alone or in combination), as well as the intraurethral administration of PGE1, are good alternatives for patients who do not respond to PDE5 inhibitors. Both of these two treatment modalities have demonstrated efficacy in ameliorating erectile function in diabetic patients.93–95
Testosterone replacement therapy is recommended in men with ED who show low levels of testosterone.95 Different formulations are available, such as gels, patches, tablets, implants, and injections. In a prospective, randomized, double-blind, placebo-controlled study, transdermal testosterone replacement therapy was associated with beneficial effects on sexual function in men with type 2 diabetes.96
Female sexual dysfunction
FSD is a complex condition that affects women of all ages and races. It is characterized by disturbances in the psychophysiological changes associated with the sexual response cycle in women, and it includes disorders of sexual desire, arousal, orgasm, and pain.97 In 2010, the Third International Consensus of Sexual Medicine accepted revised definitions of FSD, emphasizing a model based on a circular pattern of the sexual female response, in which different phases of sexual function can overlap.98
More recently, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) released newer and revised definitions, in which sexual desire and arousal disorders have been combined into the “female sexual interest/arousal disorder” category, and vaginismus and dyspareunia have been grouped into the “genito-pelvic pain/penetration disorder” category.99 Moreover, all of the sexual dysfunctions outlined in the DSM-5 require a minimum duration of approximately 6 months, and more precise severity criteria must be met in order to provide useful thresholds for making a diagnosis and for distinguishing transient sexual difficulties from more persistent sexual dysfunction.99
Sexual difficulties in women appear to be widespread in society, as they are influenced by both health-related and psychosocial factors; they are also associated with impaired quality of life and interpersonal relationships. Based on data of the National Health and Social Life Survey,33 which examined a cohort of adults in the US in 1992, the prevalence of FSD has, for many years, been estimated at 43%, which is higher than the rate reported in men (31%). Large epidemiological studies reported that the prevalence of FSD ranges from 40%–60%,100–102 with the highest values observed in postmenopausal women.101
There are common risk factor categories associated with sexual dysfunction in women; these include aging,102 diabetes mellitus,16,21 CVD,103 hypertension,104 concurrence of genitourinary disease,24 psychiatric/psychological disorders,101 cancer,105 and other chronic diseases.106,107 Moreover, limited social relations, financial difficulties, employment status, religious beliefs, educational background, and lack of exercise represent the sociocultural risk factors of FSD.97
FSD and diabetes: risk factors and association
FSD have been described in diabetic women since the early 1980s. Sexual disorders reported in women with diabetes include the reduction or loss of sexual interest or desire, arousal or lubrication difficulties, dyspareunia, and loss of the ability to reach orgasm.108,109
FSD has been associated with both type 115,19 and type 2 diabetes.16–18 A recent meta-analysis110 that included 26 studies, 3,168 diabetic women, and 2,823 controls showed that FSD is more frequent, and is associated with a lower Female Sexual Function Index (FSFI) score in diabetic women than in controls. In particular, the risk for FSD was 2.27 (95% confidence interval [CI]: 1.23–4.16) and 2.49 (95% CI: 1.55–3.99) in type 1 and type 2 diabetic women, respectively. Furthermore, the risk for FSD was 2.02 (CI: 1.49–2.72) when considering “any diabetes” (which represented the two forms of diabetes together). Interestingly, an increased risk of FSD was found in premenopausal women with “any diabetes”, but not in postmenopausal women. Moreover, at meta-regression, among the independent variables, only BMI was significantly associated with the FSFI effect size (P=0.005), suggesting that the higher frequency of FSD and lower FSFI score found in diabetic women may be related to body weight. Several studies have already shown an increased prevalence of FSD in women affected by obesity111–113 and metabolic syndrome.27,114 Studies that have focused on type 1 diabetic women have provided a valid opportunity to investigate the role of diabetes on sexual function, independent of other associated comorbidities. In type 1 diabetic women, FSD appears to be correlated mainly to psychological factors, such as depression, anxiety, and marital status.15,19 Results from a large prospective study of 625 women with type 1 diabetes15 showed that depression was the major predictor of sexual dysfunction.
Studies examining FSD in individuals with type 2 diabetes are less conclusive and are limited by small study sizes;17,111 the determinants of sexual function in type 2 diabetes include age, duration of diabetes, menopause, microvascular complications, and psychological complaints. In one large study16 that evaluated 613 diabetic women and 524 controls, it was found that the longer duration of diabetes, older age, higher BMI, the presence of CVD, and the presence of diabetic complications was significantly associated with worse sexual function. In a study by Esposito et al,21 it was found that metabolic syndrome and atherogenic dyslipidemia were independent predictors of FSD in 595 type 2 diabetic women, although only depression and marital status were the strongest independent factors associated with FSD.
In conclusion, psychological concerns may play a significant role in the development of FSD in both type 1 and type 2 diabetes. This is in line with the complex nature of female sexuality, which is largely dependent on psychological and cultural factors, even more so than male sexuality.
Pathogenesis of FSD in diabetes
The normal female sexual response needs the integrity of the sensory and autonomic nervous systems in order to respond to erotic stimuli, as well as of the vascular districts that supply blood to the external genitalia and vagina. Both the smooth muscle relaxation of female genitalia erectile tissue and the enhancement of genital blood flow are dependent upon the action of nonadrenergic/noncholinergic neurotransmitters, such as vasoactive intestinal polypeptide (VIP) and NO. The regulation of blood flow and clitoral erectile function is governed by the same NO/cGMP pathway in women as that involved in erectile function is in men. NO and PDE5 have been identified in human clitoral smooth muscle,115,116 indicating a key role of NO in female sexual function. Normal levels of various hormones are also required for physiologic sexual activity. Diabetes may affect all of these integrated systems, leading to sexual dysfunction. The mechanisms involved include hyperglycemia, infections, vascular and neurological damage, and hormonal disorders.117
Hyperglycemia reduces the hydration of the vaginal mucus membranes, producing poor vaginal lubrication and dyspareunia.118 Moreover, hyperglycemia increases the risk of genitourinary infections which, in turn, may lead to vaginal discomfort and dyspareunia.119
Diabetes-induced vascular and nerve dysfunctions may impair the sexual response by producing structural and functional changes in the female genitalia. Studies in animals showed that diabetes may affect arousal and orgasmic sexual responses by inducing impaired relaxation responses of the vaginal tissue to almost all transmitter systems,120 decreasing nerve-stimulated clitoral and vaginal blood flow, producing diffuse fibrosis of the clitoris and vaginal tissues, and reducing the muscular layer and epithelial thickness in the vagina.121–123 Vascular abnormalities, including atherosclerotic damage and diabetes-induced endothelial dysfunction, may be responsible for reducing the engorgement of the clitoris and for reducing lubrication of the vagina, leading to decreased arousal and dyspareunia during sexual intercourse.121 Diabetic neuropathy may further contribute to the pathogenesis of sexual dysfunctions by altering both the normal transduction of sexual stimuli and the triggered sexual response.124,125
It has been hypothesized that FSD may be the consequence of an imbalance in the hormonal levels of diabetic women, as indicated by epidemiological studies showing a correlation between alterations in the levels of androgens, estrogens, as well as sex hormone-binding globulin and sexual problems in diabetic women.126 Moreover, several endocrinological pathologies that may be associated with diabetes, such as thyroid disorders, hypothalamic–pituitary dysfunctions, and polycystic ovarian syndrome, may further contribute to sexual dysfunctions in these women.107
Depression is strongly associated with diabetes.127 Most epidemiological studies showed that psychosocial factors are the main contributors to sexual dysfunctions in both type 115,19 and type 2 diabetes.21,101 Depression seems to be the principally established determinant of sexual dysfunction in women with diabetes.15,19,99,128 Diabetic complications may also affect health and relationship status, quality of life, and a woman’s self-image, generating a vicious cycle that may have detrimental effects on sexual performance.15,16,129
To conclude, FSD pathogenesis in diabetes is complex, and current studies have not yet clarified all of the pathological pathways involved; these studies are limited by small sample sizes, lack of standardized definitions of sexual dysfunction, and inadequate characterization of diabetes with regard to glycemic control, the presence of complications, and the presence of depression. In contrast to what is described in men, female sexual function appears to be more related to social and psychological components than to the physiological consequence of diabetes.
Treatment of FSD
At present, no specific guidelines are currently available for the treatment of FSD in diabetes; therefore, therapeutic possibilities for sexual dysfunction in diabetic women refer to lifestyle changes, optimal diabetic control, psychotherapy, and selected medications when appropriate (Table 2).
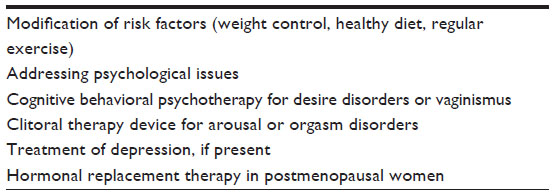 | Table 2 Summary of the available therapies for female sexual dysfunction |
Major health organizations recommend that individuals adopt a healthy lifestyle (including engaging in physical activity and adopting a Mediterranean-style diet for the prevention of cardiovascular risk factors), and screen for and treat depression.25 Giugliano et al130 found a positive association between one’s adherence to a Mediterranean diet and FSFI score in 595 type 2 diabetic women; women with the highest level of adherence to a Mediterranean diet had the lowest prevalence of sexual dysfunction. The same group evaluated the effect of a Mediterranean diet on sexual function in 59 women with metabolic syndrome.131 Thirty-one women with a diagnosis of FSD and metabolic syndrome were assigned to the Mediterranean-style diet and 28 to a standard control diet. After 2 years, sexual function improved in the intervention group, and remained stable in the control group. The Look AHEAD Sexual Dysfunction Ancillary study132 examined the effects of an intensive lifestyle intervention when compared with a control group (which received diabetes support and education) in 229 sexually active type 2 diabetic women. After 1 year, among women with FSD at baseline, those in the intensive lifestyle intervention group reported greater improvements in their total FSFI scores and across most of the FSFI domains, and they were also more likely to experience a resolution in FSD, as compared with those in the diabetes support and education group. The adoption of healthy lifestyles may reduce insulin resistance, endothelial dysfunction, and oxidative stress, all of which are desirable achievements for diabetic patients. The resulting improved well-being may further help reduce and prevent sexual dysfunction in women.
Sexual dysfunction in diabetic women may benefit from both the resolution of psychological issues and the treatment of depression with specific medical therapy. Moreover, achieving adequate glycemic control is of paramount importance for diabetic women, in order to help reduce the risk of genitourinary infections and avoid complications.
At present, there are no Food and Drug Administration-approved transdermal or oral androgen therapies for FSD, whereas hormonal replacement therapy is approved for postmenopausal women. Acting on NO-mediated smooth muscle relaxation to increase vasodilatation, PDE5 inhibitors might theoretically improve vaginal lubrication and vulvar engorgement. In contrast, few successes have been reported for the use of these agents in the treatment of sexual arousal problems in women; this is likely due to the inconsistencies observed between the physiological and psychological factors on sexual response,133 or the low PDE5 levels noted in the female reproductive system.134
Further research is needed in order to investigate the effects of diabetes on female sexual function, and hence to provide effective therapeutic opportunities for these women.
Conclusion
Diabetes mellitus is a growing public health concern, leading to cardiovascular, psychological, and sexual dysfunctions. Diabetes is a well-known cause of ED, with prevalence rates approaching 50% in both type 1 and type 2 diabetes. The determinants of ED in diabetic men include glycemic control and most of the principal cardiovascular risk factors, such as hypertension, hyperlipidemia, overweight and obesity, metabolic syndrome, smoking, and sedentary lifestyles. Moreover, ED is an independent risk factor for the new onset of CVD, and it is an important predictor of the development of major cardiovascular events in diabetic patients with known CAD. The debate as to whether FSD should be classified as a dysfunction similar to ED or whether it should be considered a pathologic condition at all is not ended. Although diabetic women suffer from the same neurovascular complications that contribute to the pathogenesis of ED in men, results of sexual functioning of diabetic women are less conclusive. However, a high prevalence of FSD has been described in both type 1 and type 2 diabetic women as compared with non-diabetic women, with most studies reporting psychosocial issues as a main determinant of FSD. Although ED in men has been recognized as a powerful predictor of major cardiovascular events, it is still not clear whether FSD may be indicated as a risk factor for CVD. Based on the current limited data, it seems as though an association between female sexual health and vascular risk factors (hypertension, hyperlipidemia, metabolic syndrome/obesity, diabetes, and CAD) exists; however, at the present time, there are no data supporting the idea that FSD can be indicated as a predictor of future cardiovascular events.25 The promotion of a healthful lifestyle, including the adoption of a healthy diet and engaging in exercise, for the prevention and treatment of cardiovascular risk factors among individuals of all ages yields great benefits and reduces the burden of chronic diseases. Extending beyond the specific effects on sexual dysfunction in men and women, the adoption of these measures promotes a healthier life and increased well-being, which in turn, may help to reduce the burden of sexual dysfunction.
Acknowledgment
The authors thank Dr Elisabetta Della Volpe and Dr Laura Olita for their technical help and writing assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
International Diabetes Federation. IDF Diabetes Atlas, 5th edition. Update. Brussels, Belgium: International Diabetes Federation, 2012. | |
Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053. | |
Kopelman PG. Obesity as a medical problem. Nature. 2000;404(6778):635–643. | |
Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics – 2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6–e245. | |
International Diabetes Federation. Diabetes Atlas. 5th ed. Brussels, Belgium: International Diabetes Federation; 2011. | |
Campos C. Chronic hyperglycemia and glucose toxicity: pathology and clinical sequelae. Postgrad Med. 2012;124(6):90–97. | |
Rahman S, Rahman T, Ismail AA, Rashid AR. Diabetes-associated macrovasculopathy: pathophysiology and pathogenesis. Diabetes Obes Metab. 2007;9(6):767–780. | |
Fox CS, Coady S, Sorlie PD, et al. Increasing cardiovascular disease burden due to diabetes mellitus: the Framingham Heart Study. Circulation. 2007;115(12):1544–1550. | |
Preis SR, Pencina MJ, Hwang SJ, et al. Trends in cardiovascular disease risk factors in individuals with and without diabetes mellitus in the Framingham Heart Study. Circulation. 2009;120(3):212–220. | |
The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329(14):977–986. | |
Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321(7258):405–412. | |
Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151(1):54–61. | |
Penson DF, Latini DM, Lubeck DP, Wallace KL, Henning JM, Lue TF; Comprehensive Evaluation of Erectile Dysfunction (ExCEED) database. Do impotent men with diabetes have more severe erectile dysfunction and worse quality of life than the general population of impotent patients? Results from the Exploratory Comprehensive Evaluation of Erectile Dysfunction (ExCEED) database. Diabetes Care. 2003;26(4):1093–1099. | |
Lu CC, Jiann BP, Sun CC, Lam HC, Chu CH, Lee JK. Association of glycemic control with risk of erectile dysfunction in men with type 2 diabetes. J Sex Med. 2009;6(6):1719–1728. | |
Enzlin P, Rosen R, Wiegel M, et al; DCCT/EDIC Research Group. Sexual dysfunction in women with type 1 diabetes: long-term findings from the DCCT/EDIC study cohort. Diabetes Care. 2009;32(5):780–785. | |
Abu Ali RM, Al Hajeri RM, Khader YS, Shegem NS, Ajlouni KM. Sexual dysfunction in Jordanian diabetic women. Diabetes Care. 2008;31(8):1580–1581. | |
Olarinoye J, Olarinoye A. Determinants of sexual function among women with type 2 diabetes in a Nigerian population. J Sex Med. 2008;5(4):878–886. | |
Giugliano F, Maiorino M, Bellastella G, Gicchino M, Giugliano D, Esposito K. Determinants of erectile dysfunction in type 2 diabetes. Int J Impot Res. 2010;22(3):204–209. | |
Enzlin P, Mathieu C, Van Den Bruel A, Vanderschueren D, Demyttenaere K. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes Care. 2003;26(2):409–414. | |
Salonia A, Lanzi R, Scavini M, et al. Sexual function and endocrine profile in fertile women with type 1 diabetes. Diabetes Care. 2006;29(2):312–316. | |
Esposito K, Maiorino MI, Bellastella G, Giugliano F, Romano M, Giugliano D. Determinants of female sexual dysfunction in type 2 diabetes. Int J Impot Res. 2010;22(3):179–184. | |
Seftel AD, Sun P, Swindle R. The prevalence of hypertension, hyperlipidemia, diabetes mellitus and depression in men with erectile dysfunction. J Urol. 2004;171(6 Pt 1):2341–2345. | |
Esposito K, Giugliano F, Martedì E, et al. High proportions of erectile dysfunction in men with the metabolic syndrome. Diabetes Care. 2005;28(5):1201–1203. | |
Lewis RW, Fugl-Meyer KS, Corona G, et al. Definitions/epidemiology/risk factors for sexual dysfunction. J Sex Med. 2010;7(4 Pt 2):1598–1607. | |
Miner M, Esposito K, Guay A, Montorsi P, Goldstein I. Cardiometabolic risk and female sexual health: the Princeton III summary. J Sex Med. 2012;9(3):641–651; quiz 652. | |
Esposito K, Ciotola M, Maiorino MI, et al. Hyperlipidemia and sexual function in premenopausal women. J Sex Med. 2009;6(6):1696–1703. | |
Esposito K, Ciotola M, Marfella R, Di Tommaso D, Cobellis L, Giugliano D. Sexual dysfunction in women with the metabolic syndrome. Diabetes Care. 2005;28(3):756. | |
NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA. 1993;270(1):83–90. | |
Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA. 1999;281(6):537–544. | |
De Berardis G, Franciosi M, Belfiglio M, et al; Quality of Care and Outcomes in Type 2 Diabetes (QuED) Study Group. Erectile dysfunction and quality of life in type 2 diabetic patients: a serious problem too often overlooked. Diabetes Care. 2002;25(2):284–291. | |
Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, McKinlay JB. Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts male aging study. J Urol. 2000;163(2):460–463. | |
Bacon CG, Mittleman MA, Kawachi I, Giovannucci E, Glasser DB, Rimm EB. Sexual function in men older than 50 years of age: results from the health professionals follow-up study. Ann Intern Med. 2003;139(3):161–168. | |
Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999;84(1):50–56. | |
Ponholzer A, Temml C, Mock K, Marszalek M, Obermayr R, Madersbacher S. Prevalence and risk factors for erectile dysfunction in 2869 men using a validated questionnaire. Eur Urol. 2005;47(1):80–85; discussion 85–86. | |
Bortolotti A, Fedele D, Chatenoud L, et al. Cigarette smoking: a risk factor for erectile dysfunction in diabetics. Eur Urol. 2001;40(4):392–396; discussion 397. | |
Giuliano FA, Leriche A, Jaudinot EO, de Gendre AS. Prevalence of erectile dysfunction among 7689 patients with diabetes or hypertension, or both. Urology. 2004;64(6):1196–1201. | |
Nicolosi A, Moreira ED, Shirai M, Bin Mohd Tambi MI, Glasser DB. Epidemiology of erectile dysfunction in four countries: cross-national study of the prevalence and correlates of erectile dysfunction. Urology. 2003;61(1):201–206. | |
De Berardis G, Pellegrini F, Franciosi M, et al; QuED Study Group. Clinical and psychological predictors of incidence of self-reported erectile dysfunction in patients with type 2 diabetes. J Urol. 2007;177(1):252–257. | |
Demir O, Akgul K, Akar Z, et al. Association between severity of lower urinary tract symptoms, erectile dysfunction and metabolic syndrome. Aging Male. 2009;12(1):29–34. | |
Turek SJ, Hastings SM, Sun JK, King GL, Keenan HA. Sexual dysfunction as a marker of cardiovascular disease in males with 50 or more years of type 1 diabetes. Diabetes Care. 2013;36(10):3222–3226. | |
Dong JY, Zhang YH, Qin LQ. Erectile dysfunction and risk of cardiovascular disease: meta-analysis of prospective cohort studies. J Am Coll Cardiol. 2011;58(13):1378–1385. | |
Ponholzer A, Temml C, Obermayr R, Wehrberger C, Madersbacher S. Is erectile dysfunction an indicator for increased risk of coronary heart disease and stroke? Eur Urol. 2005;48(3):512–518; discussion 517–518. | |
Araujo AB, Travison TG, Ganz P, et al. Erectile dysfunction and mortality. J Sex Med. 2009;6(9):2445–2454. | |
Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):319–326. | |
Thorve VS, Kshirsagar AD, Vyawahare NS, Joshi VS, Ingale KG, Mohite RJ. Diabetes-induced erectile dysfunction: epidemiology, pathophysiology and management. J Diabetes Complications. 2011;25(2):129–136. | |
Bacon CG, Hu FB, Giovannucci E, Glasser DB, Mittleman MA, Rimm EB. Association of type and duration of diabetes with erectile dysfunction in a large cohort of men. Diabetes Care. 2002;25(8):1458–1463. | |
Kalter-Leibovici O, Wainstein J, Ziv A, Harman-Bohem I, Murad H, Raz I; Israel Diabetes Research Group (IDRG) Investigators. Clinical, socioeconomic, and lifestyle parameters associated with erectile dysfunction among diabetic men. Diabetes Care. 2005;28(7):1739–1744. | |
Fedele D, Coscelli C, Santeusanio F, et al. Erectile dysfunction in diabetic subjects in Italy. Gruppo Italiano Studio Deficit Erettile nei Diabetici. Diabetes Care. 1998;21(11):1973–1977. | |
Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N Engl J Med. 1998;338(20):1397–1404. | |
Corona G, Giorda CB, Cucinotta D, Guida P, Nada E; Gruppo di studio SUBITO-DE. The SUBITO-DE study: sexual dysfunction in newly diagnosed type 2 diabetes male patients. J Endocrinol Invest. 2013;36(10):864–868. | |
Siu SC, Lo SK, Wong KW, Ip KM, Wong YS. Prevalence of and risk factors for erectile dysfunction in Hong Kong diabetic patients. Diabet Med. 2001;18(9):732–738. | |
Al-Hunayan A, Al-Mutar M, Kehinde EO, Thalib L, Al-Ghorory M. The prevalence and predictors of erectile dysfunction in men with newly diagnosed with type 2 diabetes mellitus. BJU Int. 2007;99(1):130–134. | |
Rosen RC, Wing RR, Schneider S, et al. Erectile dysfunction in type 2 diabetic men: relationship to exercise fitness and cardiovascular risk factors in the Look AHEAD trial. J Sex Med. 2009;6(5):1414–1422. | |
Vinik AI, Maser RE, Mitchell BD, Freeman R. Diabetic autonomic neuropathy. Diabetes Care. 2003;26(5):1553–1579. | |
Chew SKh, Taouk Y, Xie J, et al. Relationship between diabetic retinopathy, diabetic macular oedema and erectile dysfunction in type 2 diabetics. Clin Experiment Ophthalmol. 2013;41(7):683–689. | |
Heruti RJ, Uri I, Arbel Y, Swartzon M, Galor S, Justo D. Erectile dysfunction severity might be associated with poor cardiovascular prognosis in diabetic men. J Sex Med. 2007;4(2):465–471. | |
Chew KK, Bremner A, Jamrozik K, Earle C, Stuckey B. Male erectile dysfunction and cardiovascular disease: is there an intimate nexus? J Sex Med. 2008;5(4):928–934. | |
Rosen RC. Sexual dysfunction as an obstacle to compliance with antihypertensive therapy. Blood Press Suppl. 1997;1:47–51. | |
Foresta C, Caretta N, Corona G, et al. Clinical and metabolic evaluation of subjects with erectile dysfunction: a review with a proposal flowchart. Int J Androl. 2009;32(3):198–211. | |
Guay AT. ED2: erectile dysfunction = endothelial dysfunction. Endocrinol Metab Clin North Am. 2007;36(2):453–463. | |
Cheitlin MD. Erectile dysfunction: the earliest sign of generalized vascular disease? J Am Coll Cardiol. 2004;43(2):185–186. | |
Malavige LS, Levy JC. Erectile dysfunction in diabetes mellitus. J Sex Med. 2009;6(5):1232–1247. | |
Esposito K, Ciotola M, Giugliano F, et al. Endothelial microparticles correlate with erectile dysfunction in diabetic men. Int J Impot Res. 2007;19(2):161–166. | |
Nehra A, Moreland RB. Neurologic erectile dysfunction. Urol Clin North Am. 2001;28(2):289–308. | |
Sáenz de Tejada I, Angulo J, Cellek S, et al. Pathophysiology of erectile dysfunction. J Sex Med. 2005;2(1):26–39. | |
Esposito K, Giugliano D. Obesity, the metabolic syndrome, and sexual dysfunction in men. Clin Pharmacol Ther. 2011;90(1):169–173. | |
Dhindsa S, Prabhakar S, Sethi M, Bandyopadhyay A, Chaudhuri A, Dandona P. Frequent occurrence of hypogonadotropic hypogonadism in type 2 diabetes. J Clin Endocrinol Metab. 2004;89(11):5462–5468. | |
Kapoor D, Aldred H, Clark S, Channer KS, Jones TH. Clinical and biochemical assessment of hypogonadism in men with type 2 diabetes: correlations with bioavailable testosterone and visceral adiposity. Diabetes Care. 2007;30(4):911–917. | |
Shabsigh R, Rajfer J, Aversa A, et al. The evolving role of testosterone in the treatment of erectile dysfunction. Int J Clin Pract. 2006;60(9):1087–1092. | |
Isidori AM, Buvat J, Corona G, et al. A critical analysis of the role of testosterone in erectile function: from pathophysiology to treatment – a systematic review. Eur Urol. 2014;65(1):99–112. | |
Dandona P, Dhindsa S. Update: Hypogonadotropic hypogonadism in type 2 diabetes and obesity. J Clin Endocrinol Metab. 2011;96(9):2643–2651. | |
Bellastella G, Maiorino MI, Olita L, De Bellis A, Giugliano D, Esposito K. Anti-pituitary antibodies and hypogonadotropic hypogonadism in type 2 diabetes: in search of a role. Diabetes Care. 2013;36(8):e116–e117. | |
Skyler JS, Bergenstal R, Bonow RO, et al; American Diabetes Association; American College of Cardiology Foundation; American Heart Association. Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American Diabetes Association and a scientific statement of the American College of Cardiology Foundation and the American Heart Association. Diabetes Care. 2009;32(1):187–192. | |
Roth A, Kalter-Leibovici O, Kerbis Y, et al. Prevalence and risk factors for erectile dysfunction in men with diabetes, hypertension, or both diseases: a community survey among 1,412 Israeli men. Clin Cardiol. 2003;26(1):25–30. | |
Romeo JH, Seftel AD, Madhun ZT, Aron DC. Sexual function in men with diabetes type 2: association with glycemic control. J Urol. 2000;163(3):788–791. | |
Wessells H, Penson DF, Cleary P, et al; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Effect of intensive glycemic therapy on erectile function in men with type 1 diabetes. J Urol. 2011;185(5):1828–1834. | |
Khatana SA, Taveira TH, Miner MM, Eaton CB, Wu WC. Does cardiovascular risk reduction alleviate erectile dysfunction in men with type II diabetes mellitus? Int J Impot Res. 2008;20(5):501–506. | |
Yaman O, Akand M, Gursoy A, Erdogan MF, Anafarta K. The effect of diabetes mellitus treatment and good glycemic control on the erectile function in men with diabetes mellitus-induced erectile dysfunction: a pilot study. J Sex Med. 2006;3(2):344–348. | |
Esposito K, Ciotola M, Giugliano F, et al. Effects of intensive lifestyle changes on erectile dysfunction in men. J Sex Med. 2009;6(1):243–250. | |
Wing RR, Rosen RC, Fava JL, et al. Effects of weight loss intervention on erectile function in older men with type 2 diabetes in the Look AHEAD trial. J Sex Med. 2010;7(1 Pt 1):156–165. | |
Esposito K, Giugliano D. Lifestyle/dietary recommendations for erectile dysfunction and female sexual dysfunction. Urol Clin North Am. 2011;38(3):293–301. | |
Konstantinos G, Petros P. Phosphodiesterase-5 inhibitors: future perspectives. Curr Pharm Des. 2009;15(30):3540–3551. | |
Brant WO, Bella AJ, Lue TF. Treatment options for erectile dysfunction. Endocrinol Metab Clin North Am. 2007;36(2):465–479. | |
Vardi M, Nini A. Phosphodiesterase inhibitors for erectile dysfunction in patients with diabetes mellitus. Cochrane Database Syst Rev. 2007:CD002187. | |
Francis SH, Corbin JD. PDE5 inhibitors: targeting erectile dysfunction in diabetics. Curr Opin Pharmacol. 2011;11(6):683–688. | |
Rendell MS, Rajfer J, Wicker PA, Smith MD. Sildenafil for treatment of erectile dysfunction in men with diabetes: a randomized controlled trial. Sildenafil Diabetes Study Group. JAMA. 1999;281(5):421–426. | |
Goldstein I, Young JM, Fischer J, Bangerter K, Segerson T, Taylor T; Vardenafil Diabetes Study Group. Vardenafil, new phosphodiesterase type 5 inhibitor, in the treatment of erectile dysfunction in men with diabetes: a multicenter double-blind placebo-controlled fixed-dose study. Diabetes Care. 2003;26(3):777–783. | |
Sáenz de Tejada I, Anglin G, Knight JR, Emmick JT. Effects of tadalafil on erectile dysfunction in men with diabetes. Diabetes Care. 2002;25(12):2159–2164. | |
Ferrini MG, Kovanecz I, Sanchez S, et al. Long-term continuous treatment with sildenafil ameliorates aging-related erectile dysfunction and the underlying corporal fibrosis in the rat. Biol Reprod. 2007;76(5):915–923. | |
Porst H, Giuliano F, Glina S, et al. Evaluation of the efficacy and safety of once-a-day dosing of tadalafil 5 mg and 10 mg in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, placebo-controlled trial. Eur Urol. 2006;50(2):351–359. | |
Bella AJ, Deyoung LX, Al-Numi M, Brock GB. Daily administration of phosphodiesterase type 5 inhibitors for urological and nonurological indications. Eur Urol. 2007;52(4):990–1005. | |
Nehra A, Jackson G, Miner M, et al. The Princeton III Consensus recommendations for the management of erectile dysfunction and cardiovascular disease. Mayo Clin Proc. 2012;87(8):766–788. | |
Williams G, Abbou CC, Amar ET, et al. Efficacy and safety of transurethral alprostadil therapy in men with erectile dysfunction. MUSE Study Group. Br J Urol. 1998;81(6):889–894. | |
Padma-Nathan H, Hellstrom WJ, Kaiser FE, et al. Treatment of men with erectile dysfunction with transurethral alprostadil. Medicated Urethral System for Erection (MUSE) Study Group. N Engl J Med. 1997;336(1):1–7. | |
Wang C, Nieschlag E, Swerdloff R, et al. Investigation, treatment and monitoring of late-onset hypogonadism in males: ISA, ISSAM, EAU, EAA and ASA recommendations. Eur J Endocrinol. 2008;159(5):507–514. | |
Jones TH, Arver S, Behre HM, et al; TIMES2 Investigators. Testosterone replacement in hypogonadal men with type 2 diabetes and/or metabolic syndrome (the TIMES2 study). Diabetes Care. 2011;34(4):828–837. | |
Basson R, Berman J, Burnett A, et al. Report of the international consensus development conference on female sexual dysfunction: definitions and classifications. J Urol. 2000;163(3):888–893. | |
Basson R, Wierman ME, van Lankveld J, Brotto L. Summary of the recommendations on sexual dysfunction in women. J Sex Med. 2010; 7(1 Pt 2):314–326. | |
American Psychiatric Association. Appendix. Highlights of changes from DSM-IV to DSM-5. In: Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013. | |
Shifren JL, Monz BU, Russo PA, Segreti A, Johannes CB. Sexual problems and distress in United States women: prevalence and correlates. Obstet Gynecol. 2008;112(5):970–978. | |
Dennerstein L, Randolph J, Taffe J, Dudley E, Burger H. Hormones, mood, sexuality, and the menopausal transition. Fertil Steril. 2002;77 Suppl 4:S42–S48. | |
Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357(8):762–774. | |
Eyada M, Atwa M. Sexual function in female patients with unstable angina or non-ST-elevation myocardial infarction. J Sex Med. 2007;4(5):1373–1380. | |
Doumas M, Tsiodras S, Tsakiris A, et al. Female sexual dysfunction in essential hypertension: a common problem being uncovered. J Hypertens. 2006;24(12):2387–2392. | |
Krychman M, Millheiser LS. Sexual health issues in women with cancer. J Sex Med. 2013;10 Suppl 1:5–15. | |
Peng YS, Chiang CK, Kao TW, et al. Sexual dysfunction in female hemodialysis patients: a multicenter study. Kidney Int. 2005;68(2):760–765. | |
Bhasin S, Enzlin P, Coviello A, Basson R. Sexual dysfunction in men and women with endocrine disorders. Lancet. 2007;369(9561):597–611. | |
Tyrer G, Steel JM, Ewing DJ, Bancroft J, Warner P, Clarke BF. Sexual responsiveness in diabetic women. Diabetologia. 1983;24(3):166–171. | |
Enzlin P, Mathieu C, Vanderschueren D, Demyttenaere K. Diabetes mellitus and female sexuality: a review of 25 years’ research. Diabet Med. 1998;15(10):809–815. | |
Pontiroli AE, Cortelazzi D, Morabito A. Female sexual dysfunction and diabetes: a systematic review and meta-analysis. J Sex Med. 2013;10(4):1044–1051. | |
Veronelli A, Mauri C, Zecchini B, et al. Sexual dysfunction is frequent in premenopausal women with diabetes, obesity, and hypothyroidism, and correlates with markers of increased cardiovascular risk. A preliminary report. J Sex Med. 2009;6(6):1561–1568. | |
Esposito K, Ciotola M, Giugliano F, et al. Association of body weight with sexual function in women. Int J Impot Res. 2007;19(4):353–357. | |
Castellini G, Mannucci E, Mazzei C, et al. Sexual function in obese women with and without binge eating disorder. J Sex Med. 2010;7(12):3969–3978. | |
Martelli V, Valisella S, Moscatiello S, et al. Prevalence of sexual dysfunction among postmenopausal women with and without metabolic syndrome. J Sex Med. 2012;9(2):434–441. | |
Berman JR, Berman LA, Toler SM, Gill J, Haughie S; Sildenafil Study Group. Safety and efficacy of sildenafil citrate for the treatment of female sexual arousal disorder: a double-blind, placebo controlled study. J Urol. 2003;170(6 Pt 1):2333–2338. | |
Min K, Munarriz R, Kim NN, Goldstein I, Traish A. Effects of ovariectomy and estrogen and androgen treatment on sildenafil-mediated changes in female genital blood flow and vaginal lubrication in the animal model. Am J Obstet Gynecol. 2002;187(5):1370–1376. | |
Bargiota A, Dimitropoulos K, Tzortzis V, Koukoulis GN. Sexual dysfunction in diabetic women. Hormones (Athens). 2011;10(3):196–206. | |
Meeking DR, Fosbury JA, Cummings MH. Sexual dysfunction and sexual health concerns in women with diabetes. Practical Diabetes. 2013;30(8):327–331. | |
Muniyappa R, Norton M, Dunn ME, Banerji MA. Diabetes and female sexual dysfunction: moving beyond “benign neglect”. Curr Diab Rep. 2005;5(3):230–236. | |
Giraldi A, Persson K, Werkström V, Alm P, Wagner G, Andersson KE. Effects of diabetes on neurotransmission in rat vaginal smooth muscle. Int J Impot Res. 2001;13(2):58–66. | |
Park K, Ahn K, Chang JS, Lee SE, Ryu SB, Park YI. Diabetes induced alteration of clitoral hemodynamics and structure in the rabbit. J Urol. 2002;168(3):1269–1272. | |
Park K, Ryu SB, Park YI, Ahn K, Lee SN, Nam JH. Diabetes mellitus induces vaginal tissue fibrosis by TGF-beta 1 expression in the rat model. J Sex Marital Ther. 2001;27(5):577–587. | |
Kim NN, Stankovic M, Cushman TT, Goldstein I, Munarriz R, Traish AM. Streptozotocin-induced diabetes in the rat is associated with changes in vaginal hemodynamics, morphology and biochemical markers. BMC Physiol. 2006;6:4. | |
Duby JJ, Campbell RK, Setter SM, White JR, Rasmussen KA. Diabetic neuropathy: an intensive review. Am J Health Syst Pharm. 2004;61(2):160–173; quiz 175. | |
Brown JS, Wessells H, Chancellor MB, et al. Urologic complications of diabetes. Diabetes Care. 2005;28(1):177–185. | |
Feldhaus-Dahir M. The causes and prevalence of hypoactive sexual desire disorder: part I. Urol Nurs. 2009;29(4):259–260, 263. | |
Schram MT, Baan CA, Pouwer F. Depression and quality of life in patients with diabetes: a systematic review from the European depression in diabetes (EDID) research consortium. Curr Diabetes Rev. 2009;5(2):112–119. | |
Rockliffe-Fidler C, Kiemle G. Sexual function in diabetic women: a psychological perspective. Sex Relation Ther. 2003;18(2):143–159. | |
Ogbera AO, Chinenye S, Akinlade A, Eregie A, Awobusuyi J. Frequency and correlates of sexual dysfunction in women with diabetes mellitus. J Sex Med. 2009;6(12):3401–3406. | |
Giugliano F, Maiorino MI, Di Palo C, et al. Adherence to Mediterranean diet and sexual function in women with type 2 diabetes. J Sex Med. 2010;7(5):1883–1890. | |
Esposito K, Ciotola M, Giugliano F, et al. Mediterranean diet improves sexual function in women with the metabolic syndrome. Int J Impot Res. 2007;19(5):486–491. | |
Wing RR, Bond DS, Gendrano IN, et al; Sexual Dysfunction Subgroup of the Look AHEAD Research Group. Effect of intensive lifestyle intervention on sexual dysfunction in women with type 2 diabetes: results from an ancillary Look AHEAD study. Diabetes Care. 2013;36(10):2937–2944. | |
Chivers ML, Rosen RC. Phosphodiesterase type 5 inhibitors and female sexual response: faulty protocols or paradigms? J Sex Med. 2010;7(2 Pt 2):858–872. | |
Uckert S, Ellinghaus P, Albrecht K, Jonas U, Oelke M. Expression of messenger ribonucleic acid encoding for phosphodiesterase isoenzymes in human female genital tissues. J Sex Med. 2007;4(6):1604–1609. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.