")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Development of the Chinese Version of the Physician Internalized Occupational Stigma Scale (PIOSS)
Authors Fan Z , Cong X, Tao M , Wu S, Gao P
Received 25 August 2022
Accepted for publication 15 November 2022
Published 29 November 2022 Volume 2022:15 Pages 3445—3459
DOI https://doi.org/10.2147/PRBM.S386724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Zhiguang Fan,1,2 Xiangxin Cong,1 Min Tao,1 Shijia Wu,3 Peng Gao3
1Department of Education, Jilin International Studies University, Changchun City, Jilin Province, People’s Republic of China; 2Department of Marxism, Changchun University of Chinese Medicine, Changchun City, Jilin Province, People’s Republic of China; 3Department of Traditional Chinese Medicine, Changchun University of Chinese Medicine, Changchun City, Jilin Province, People’s Republic of China
Correspondence: Peng Gao, Department of Traditional Chinese Medicine, Changchun University of Chinese Medicine, Boshuo Street 1035, Changchun City, Jilin Province, 130117, People’s Republic of China, Tel +86-431-84924101, Fax +86 1 594-831-4623, Email [email protected]
Background/Objective: Internalized occupational stigma may develop in physicians as a result of their identification with the public negative labels and stereotypes about them, and then internalization of them as a part of their self-concept. This study aims to develop the Physician Internalized Occupational Stigma Scale (PIOSS) and to examine its reliability and validity.
Methods: In study 1, the initial scale was used to investigate 356 physicians. While in study 2, a total of 346 physicians were investigated with the survey tools named the PIOSS, the Career Commitment Scale (CCS), the Workplace Well-Being Scale (WWBS), the Scale for the Doctor with Patient-doctor Relationship (DDPRQ-10), the Intent to Leave Scale (ILS) and the Occupational Disidentification Scale (ODS).
Results: The PIOSS includes 19 items divided into 3 dimensions: label identification, status loss, and career denial. The results of confirmatory factor analysis (CFA) reveal that the three-factor model fitted well (χ2/df=2.574, RMSEA= 0.068, CFI= 0.931, IFI= 0.931, TLI= 0.919, PNFI= 0.762, PCFI= 0.795). The PIOSS total and each dimension scores were significantly negatively correlated with the CCS and the WWBS scores and remarkably positively associated with the DDPRQ-10, the ILS, and the ODS scores. Cronbach’s α coefficients for the PIOSS total scale and dimensions ranged from 0.775 to 0.914, and split-half reliability coefficients ranged from 0.801 to 0.931. In addition, the PIOSS exhibited cross-gender invariance.
Conclusion: Having good reliability and validity, the PIOSS can serve as a valid tool for the assessment of physician internalized occupational stigma.
Keywords: physician, internalized occupational stigma, reliability, validity
Introduction
Medicine shoulders the community responsibility of health maintenance, disease prevention, and illness elimination. It is such a cardinal obligation of all governments and a crucial factor determining public trust and satisfaction with the government that they endeavor for universal access to health care services.1 Physicians are granted high praise in most cultures precisely motivated by the fact that medicine deals directly with the health and well-being of human beings.2 According to Hippocrates, by way of illustration, “Medicine is of all the arts the most noble”. Similarly, it is a well-established concept in Chinese Confucianism that “medicine is the art of benevolence, in which the physician must have a caring heart”. In general, physicians have a high social status and professional prestige and are respected by the people. It is, nevertheless, typical not to be exempted from the stigmatization of almost all professions due to the content and nature of their work, nor are physicians.3 Negative media reports and derogatory remarks about physicians, especially in recent years, have been common in China.4 What is of concern is that physician stigma is a global issue. By way of example, career-related stigma has been found in studies of physicians across different countries such as the United States,5 Spain,6 Bangladesh,7 and Australia.8
Being confronted with a severe physician-patient trust crisis, China is experiencing a high incidence of medical disputes, further exacerbating the stigmatization of health care.9 With the all-around promotion of health care reform by the Chinese government since 2009, the process of marketization, privatization, and industrialization of health care has been progressively deepening, and the proportion of public welfare health care has been gradually decreasing.10 Becoming profit-driven within the process of reform, hospitals have made the excessive pursuit of economic effects while weakening their public welfare attributes.11 Some physicians are guilty of receiving red envelopes and drug kickbacks, and over-checking and treating,12 which has severely damaged the occupational image of physicians and triggered public accusations and criticisms.13 Out of distrust of physicians, ironically, patients mobilized interpersonal networks to send gifts and money to their physicians during consultations to alleviate internal anxiety and panic.14 In addition, what may likewise trigger dissatisfaction of patients are physicians’ lack of communication skills, indifference to patients, and weak awareness of defending patients’ rights and privacy, which could exacerbate the stigma against physicians.15
Occupational stigma, derived from social construction, is the assignment of negative characteristics to a group of people engaging in certain jobs, which generates a loss of social status, discrimination, and exclusion.16 Stigma, as a generalized notion, is amplification by the public of the wrongdoings of a small number of physicians to the entire group, with negative labels for them.17 To be a “Good Doctor” is considered to require a combination of exquisite medical skills and good moral character.18 The stigma attached to physicians may arise from failure to meet public expectations of either professional competence or moral character.19 In this respect, there are three forms of occupational stigma: physically tainted, socially tainted, and morally tainted.20 Taking this as a basis, the classification of professional prestige has been incorporated as a dimension of occupational stigma followed by Ashforth et al, which has been identified into six broad categories: high/low prestige physical stigma, high/low prestige social stigma, and high/low prestige moral stigma.21 By and large, it is acceptable to classify the physician occupational stigma as one of high prestige moral stigma.
Although there are clear differences in the perceptions of doctors and the public regarding the profession of physicians, both sides share the view that the current patient-physician relationship is not harmonious.22 Physicians, traditionally a high prestige profession, nevertheless suffer from more negative evaluations. As occupation is a vital component of an individual’s self-concept, it is possible that occupational stigma can threaten the practitioner’s self-perception.23 Physicians are exposed to a large number of negative statements related to their profession which they identify with and internalize as part of their self-concept, potentially leading to internalized stigma. Occupational stigma negatively shapes physicians’ work attitudes and behaviors.24 By way of example, physicians who subscribe to the negative label of “receiving drug kickbacks” in the belief that most physicians engage in similar behaviors would be more inclined to prescribe medications for financial gain rather than for better treatment outcomes.
According to self-verification theory, individuals with different self-orientations have selective acceptance of external information and integrate it into their self-concept to minimize the discrepancy between external evaluations and their self-concept.25 High public recognition of physicians could positively contribute to the validation of their self-concept, whereas it could be damaged by stigmatizing information.26 Thus, stigma has the power to threaten physicians’ perceptions and evaluations of their profession. In almost all cases, internalized occupational stigma is associated with negative outcomes. Previous studies have identified that occupational stigma is positively associated with practitioners’ intent to leave,27 job burnout,28 feelings of disrespect,23 and defensive medicine,29 but negatively related to feelings of career identification and job worth,30 job satisfaction,31 occupational self-esteem,32 and mental health level.33
As stigma is a complex concept, no academic consensus has been reached on the connotation and dimensional division of occupational stigma. From the perspective of sociology, Link and Phelan have interpreted the concept, origins, matter of degree, and consequences of stigma. Besides, the conceptualizing stigma theory suggests that stigma arises from a power situation.34 A negative stereotype is constituted by the fact that most people in society identify the characteristics of a specific group of people or an occupation, find differences, and assign negative labels to them. Stigma has the power to separate “us” from “them”, giving rise to negative consequences for those stigmatized and making them suffer from status loss, social exclusion, and discrimination. Hence, occupational stigma denotes the burden of negative public evaluations on physicians and the perception of loss of professional status, value, and meaning of their work.
A scale with favorable psychometric properties deserves to be developed given the pronounced negative impact of occupational stigma on the medical and health fields. The stigma consciousness questionnaire for women (SCQ for women), consisting of 10 items, was developed by Pinel to assess women’s stereotypes of their gender.35 A follow-up study by Pinel and Paulin adapted some of the SCQ items to be suitable for assessing the stigma consciousness of service workers.16 Shantz and Booth selected and modified some items of the SCQ to form the Occupational Stigma Consciousness Scale (OSCS),30 a unidimensional structure consisting of six items, which was originally used to assess the call center workers’ perceived public stigma of their work. Although the SCQ and OSCS are currently the most widely used scales for the assessment of stigma consciousness among service workers,36 the origins, the matter of degree, and manifestations of occupational stigma are not identical across occupations due to the wide variation in the content and nature of work. However, the stigma of physicians, who are typically considered to be a high prestige occupation, differs from the traditional “dirty work”. In addition, the SCQ and OSCS assess stigma consciousness rather than the content of stigma and the negative consequences of internalized stigma for a certain occupation.
In succession, researchers have developed stigma scales that can be used to assess specific occupations, for example, scales applicable to female sex workers,37 airline cabin crew,38 and nurses.39 It is clear from the retrieval of available literature that there are two main scales related to physician occupational stigma. The Forensic Stigma Scale (FSS) is composed of 12 items divided into two dimensions – Dangerousness/Unpredictability and Responsibility/Blame.40 Although the FSS has good reliability and validity, it was developed only for the occupational stigma of the medical examiner and assesses the public stigma of patients towards physicians. Fan et al, developed the Patient toward Physician Occupational Stigma Scale (PPOSS) based on individual cognitive models.41 The PPOSS is categorized into three dimensions: stereotype, prejudice, and discrimination, respectively, to assess the cognition, emotion, and behavior of stigma. The POSS, nevertheless, also applies merely to assessing patients’ public stigma toward physicians rather than their internalized occupational stigma. Additionally, within the study of the COVID-19 stigma in healthcare, it was conducted with the Bogardus Social Distance Scale,42 which was initially employed to assess the perceived social distance of patients with psychiatric illness rather than specifically occupational stigma.
It is evident from the analysis of the existing literature that there are three main shortcomings in previous studies. First, studies in the field of occupational stigma have focused more on dirty work and only a few studies have involved physicians, yet stigma is not the same across occupations.43 Second, among the studies related to the stigma of physicians, some of them assessed the perceived stigma of physicians rather than internalized occupational stigma. Third, in the assessment of physician occupational stigma, most studies have focused on the public stigma of physicians by patients. However, there is no specific assessment tool for evaluating physician internalized occupational stigma. The lack of tools with good reliability and validity renders it challenging to accurately assess physician internalized occupational stigma, which is a barrier to the development of quantitative studies. This study aims to develop the Physician Internalized Occupational Stigma Scale (PIOSS) using the conceptualizing stigma theory as a theoretical framework, thereby providing a tool to support the accurate assessment of the degree of internalized occupational stigma among physicians, as well as the evaluation of the effectiveness of the evaluation intervention practices. Two studies were performed to achieve this purpose. In Study 1, primarily completed the development of the item pool and the administration of the initial questionnaire, with some items removed via item analysis and exploratory factor analysis. In Study 2, the factor structure of the scale was examined through confirmatory factor analysis. Furthermore, the PIOSS was tested for its criterion validity, internal consistency reliability, split-half reliability, and cross-group invariance. The study hypothesizes that the PIOSS possesses good psychometric characteristics and can be a valid tool for assessing physician internalized occupational stigma.
Study 1
Purpose
The purpose of Study 1 is to prepare items to form an initial questionnaire by combining semi-structured interviews and expert reviews within the framework of conceptualizing stigma theory. After administering the initial questionnaire to perform item analysis and EFA on the resulting data, the official scale was formed upon the removal of some items. The item analysis is designed to examine the discrimination and homogeneity of scale items, while the exploratory factor analysis is conducted to analyze the factor structure of the PIOSS.
Method
Sample Size Calculation
In factor analysis, the minimum sample size is generally required to be 5–10 times the number of items.44 Taking 10 times the number of items as the standard, a minimum sample size of 260 should be applied to the initial questionnaire consisting of 26 items. In addition, for the stability of factor analysis results, it was suggested that the minimum sample size should be no less than 300.45 All factors considered, the minimum sample size for this study was 300.
Participants
To improve the representativeness of the participants, the study covered 18 hospitals in 13 provinces of China. According to the National Bureau of Statistics of China, the country is divided into the eastern, central, western, and northeastern regions. Following this, a total of 5 hospitals in 4 provinces of Jiangsu, Zhejiang, Shandong, and Guangdong in the eastern region, 4 hospitals in 3 provinces of Anhui, Jiangxi, and Hubei in the central region, 5 hospitals in 3 provinces of Gansu, Guizhou, and Inner Mongolia in the western region, and 4 hospitals in 3 provinces of Liaoning, Jilin, and Heilongjiang in the northeastern region were selected for this study. The survey of physicians was conducted in three main ways. First, the researchers went to each department of the hospital and asked the physicians about their attitudes toward participating in this survey. After obtaining their consent, the questionnaire was distributed to them. Second, a snowballing approach was taken to ask the surveyed physicians to recommend potential participants. Third, the researchers used the interval between hospital-organized meetings to ask whether physicians who attended the meetings were willing to participate in this survey. The survey was completed on a one-to-one basis by the researchers. The researchers first explained in detail to the physicians the anonymity, confidentiality, process, and time required for the survey. Physicians who agreed to participate in this survey were required to sign informed consent. The researchers then gave them a link to the online version of the survey, which the physicians answered independently.
A total of 356 participants were investigated in Study 1, of whom 171 were male and 185 were female; 187 were TCM physicians and 169 were Western medicine physicians; education of bachelor and below 213, master 116, and Ph.D. 27; marital status of unmarried 141, married 210, divorced 4, and widowed 1; the professional title of physician 172, attending physician 86, deputy chief physician 68, and chief physician 30; the minimum age is 24 years old, while the maximum is 62 years old, with the average age of 36.54 years old (SD = 9.58).
Item Pool
A group of 14 physicians, including 6 males and 8 females, aged between 33 and 57 years, were selected for semi-structured interviews in the study. A detailed introduction to the concept of internalized occupational stigma was presented to the interviewees with specific examples before the start of the interviews. During the interview, they were guided by the interviewers to honestly express their understanding, perceptions, and reactions to stigma based on their own experiences. Examples of interview outline items: “What do you think are the reasons for the generation of physician occupational stigma?” “What do you think are the common negative labels the public attaches to physicians?” “How do you evaluate the current social status of physicians?” “What do you think are the negative effects of physician internalized occupational stigma?”
The results of the interviews were analyzed by each of the four master’s students in psychology independently to extract typical words associated with internalized occupational stigma. Subsequently, they worked together to discuss, then merged synonyms and near-synonyms, while removing ambiguous words and infrequently used words, and finally retained a total of 83 words related to internalized occupational stigma. The top 10 words are dispute, kickback, red envelope, stress, indifference, violence, fatigue, misunderstanding, risk, and overtreatment.
One associate professor of psychology together with two Ph.D. students in psychology prepared 42 initial items combining the high-frequency words extracted from the interviews within the theoretical framework of conceptualizing stigma theory. Besides, the four students shared a discussion of all the items one by one, excluding those with repetitive content, unclear expressions, and ambiguities, while modifying the representation of some items, with finally 14 items removed and 28 items retained. Subsequently, a small range of pre-tests was conducted among 13 physicians. At the end of the test, participants were invited to discuss their comprehension, sensitivity, and answer feelings about the items. Further revisions of item contents were made based on feedback, with two items removed, leaving a final total of 26 items, which constituted the initial physician internalized occupational stigma scale. It used a 5-point Likert scale (1 means strongly disagree, 5 means strongly agree), in which participants determine the level of agreement with the items in light of their true feelings.
Data Analysis
Using SPSS 20.0 software, the data were subjected to EFA and item analysis, in which the critical ratio values, item-total correlation coefficient, and Cronbach’s α coefficient were calculated separately.46 First, to calculate the total score of the initial questionnaire, divided into the high group of the top 27% and the low group of the bottom 27%, with an independent sample t-test to examine the critical ratio value of all items. The items with insignificant differences (p > 0.05) between the high and low groups were removed. Next, to calculate the item-total correlations, and remove those whose correlation coefficients were less than 0.40.44 Finally, to calculate the Cronbach’s α coefficient of the initial questionnaire. If the Cronbach’s α coefficient of the questionnaire increases after deleting an item, it should be removed.47
In EFA, the KMO value and the p value of Bartlett’s chi-square need to be calculated first. It indicates that the data are suitable for EFA if the KMO value is higher than 0.60 and the p value of Bartlett’s chi-square is less than 0.05.48 The approach of orthogonal rotation forces the factors to be uncorrelated with each other, while the oblique rotation is without such constraint. In studies of social sciences, there is often a degree of correlation between factors. Therefore, most statistical experts suggest that oblique rotation should be taken.49 In addition, the principal axis factoring (PAF) method yields the most stable results compared to other factor extraction methods.50 Hence, in this study, PAF was employed for factor extraction (extraction)45 and the Promax method for oblique rotation50 to determine the number of factors with eigenvalues greater than 1.51 The item should be deleted provided that any of the following conditions are met: (1) the factor loadings are less than 0.40; (2) the communalities of the items are less than 0.30; (3) there are cross-loadings; (4) Lack of theoretical connection between items and factors; (5) Dimensions with less than three items.44
Results
The results of the item analysis are illustrated in Table 1. The critical ratio value of each item of the initial questionnaire ranged from 3.41 to 20.42, with all high group scores considerably higher than those of the low group (p < 0.01). The scores of each item were remarkably positively correlated with the total score. The correlation coefficients of the items with the total score ranged from 0.47 to 0.79, except for item 26, “I would deal with the relationship with patients carefully”, whose correlation coefficient with the total score was 0.30, less than the standard of 0.40. The Cronbach’s α coefficient of the initial questionnaire was 0.936, whereas it is 0.938 after the deletion of item 26. The Cronbach’s α coefficient did not increase significantly after the removal of other items. Consequently, item 26 should be deleted at this stage to preserve the remaining items.
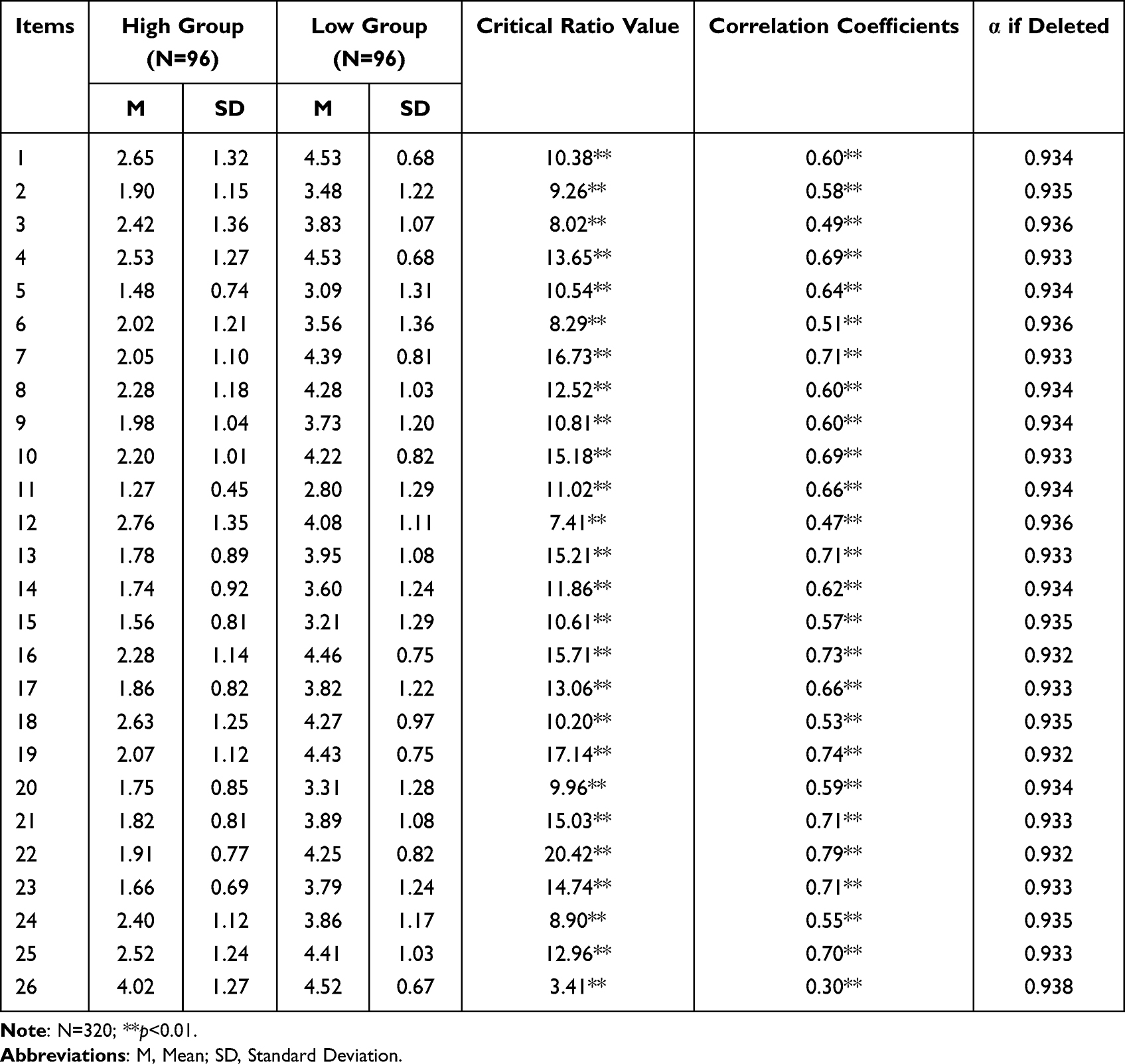 |
Table 1 Item Analysis Results of the PIOSS |
Exploratory Factor Analysis
The value of KMO of the initial questionnaire and Bartlett’s test of sphericity are 0.934 and 4928.94 separately (df=300, p<0.001), suggesting that the data is suitable for EFA. The results of EFA revealed that some items with factor loadings less than 0.40 were deleted, as follows, item 8 “I would not allow my children in medical work”, item 13 “I believe that physicians are in opposition to the public”, item 18 “I believe that the work of physicians is often exposed to death”, and item 12 “I believe that the work of physicians requires frequent access to dirty objects (eg, vomit, urine)”. In addition, there is a separate dimension including item 17, “I believe that it is difficult for me to meet the standards of a ‘good physician’” and item 21, “I believe that it is reasonable that physicians would have difficulty maintaining their passion for patients”, but it was removed given that there were fewer than three items.
When the above items were removed one by one, the remaining 19 items were subjected to EFA again, which revealed (see Table 2) that a total of 3 factors with eigenvalues greater than 1 were extracted, cumulatively explaining 61.21% of the total variance. The factor loadings ranged from 0.539 to 0.941, with communalities from 0.388 to 0.724. Factor 1 includes 8 items named status loss, factor 2 includes 6 items named career denial, and factor 3 includes 5 items named label identification.
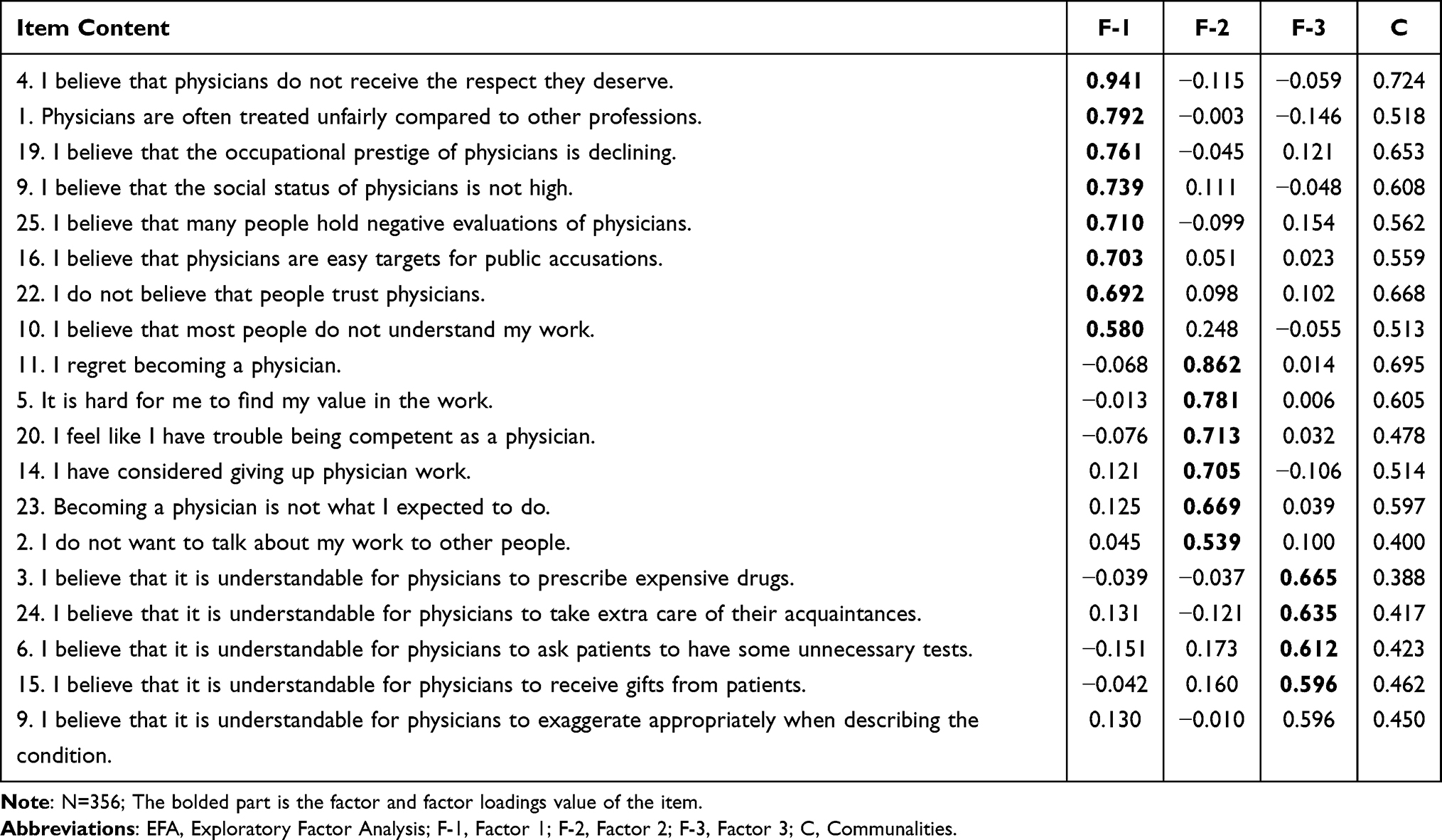 |
Table 2 EFA Results of the PIOSS |
Study 2
Purpose
A formal scale of 19 items was formed in study 1 with the removal of 7 items following item analysis and EFA. The purpose of study 2 is to further examine the reliability and validity of the scale, including the following four parts: First, the rationality of the three-factor structured PIOSS was examined through confirmatory factor analysis. Second, to conduct a test of the criterion validity. The CCS, the WWBS, the DDPRQ-10, the ILS, and the ODS were selected as tools to be administered simultaneously with the PIOSS. The conservation of resources theory asserts that individuals strive to acquire and develop new resources while also trying to avoid attrition.52 More resourceful individuals possess a greater ability to resist and repair stress, whereas continuous resource depletion hurts individuals’ cognition, attitudes, and behaviors.53 Stigma, as a typical pressure source, provokes a depletion of practitioner resources, leading to low occupational identification, decreased well-being, and higher intent to leave.54,55 Accordingly, it was hypothesized that individual physician occupational stigma was capable of a reduction in occupational commitment, workplace well-being, and evaluation of the patient-doctor relationship, while an increase in the intent to leave and occupational disidentification. Third, the reliability of the scale was examined via the calculation of Cronbach’s α coefficient and split-half reliability. Fourth, it was tested whether the PIOSS exhibited cross-gender invariance.
Participants
Study 2 was identical to Study 1 in terms of the calculation of the minimum sample size, the selection of the survey participants, and the survey process, with the investigation of a total of 17 hospitals in 12 provinces. The sampling area covered three provinces in the Chinese eastern region of Guangdong, Zhejiang, and Jiangsu; three provinces in the central region of Hubei, Henan, and Anhui; the western region, including Inner Mongolia and provinces of Yunnan, and Gansu; and three provinces in the northeastern region of Liaoning, Jilin, and Heilongjiang. Informed consent was obtained from the physicians and they signed the informed consent form before starting the survey.
A total of 346 participants were investigated in Study 2, of whom 154 were male and 192 were female; 170 were TCM physicians and 176 were Western medicine physicians; 239 were educated with a bachelor’s degree or less, 98 with master’s degree, and 9 to doctorate degree; 70 were unmarried, 270 were married, 5 were divorced, and 1 was widowed; 144 had the title of physician, 122 were attending physicians, 61 were deputy chief physicians, and 19 were chief physicians; the minimum age was 25 years old, while the maximum age was 59 years old, with an average age of 37.71 years old (SD = 8.28).
Measurements
The Physician Internalized Occupational Stigma Scale (PIOSS). The PIOSS, developed for this study, consists of 19 items divided into 3 dimensions: label identification, status loss, and career denial, which is rated on a 5-point scale ranging from “1 means strongly disagree” to “5 means strongly agree”. Scores for each item are summed into the total score, with the higher the score, the higher the degree of physician internalized occupational stigma.
The Career Commitment Scale (CCS). The Chinese version of the CCS, a unidimensional structure consisting of 8 items, is selected as the survey instrument56 to assess individuals’ attitudes toward their careers, which is based on a 5-point scale ranging from “1 means strongly disagree” to “5 means strongly agree”. Items 1, 3, and 7 are reverse scored, where the sum of the scores of each item is the total score, indicating that the higher the score, the more positive the individual’s attitude toward their career as well as the more inclined to continue in their current career. The Cronbach’s α coefficient of the scale in this study is 0.843.
The Workplace Well-Being Scale (WWBS). The Employee Well-being Scale (EWBS) is a valid tool for the assessment of employee well-being within the context of Chinese society, including three subscales of the Life Well-Being Scale, the Workplace Well-Being Scale, and the Psychological Well-Being Scale. The WWBS subscale was selected as the survey instrument,57 comprising 6 items on a 7-point scale ranging from “1 means strongly disagree” to “7 means strongly agree”. The sum of the scores of each item is the total score, whereas the higher the score, the higher the level of job satisfaction and well-being of the individual. The Cronbach’s α coefficient of the scale in this study is 0.939.
The Scale for the doctor with patient-doctor relationship (DDPRQ-10). The Chinese version of the DDPRQ-10 is selected as the survey instrument,58 consisting of 10 items, categorized into 3 dimensions of the Physician’s Subjective Experience, Quasi-Objective Questions About the Patient’s Behavior, and Symptoms-Combines Elements of the Patient’s Behavior and of the Physician’s Subjective Response, which is based on a 6-point scale from “1 means not at all” to “6 means a great deal”. Items 1, 7, and 9 are reverse scored, and the sum of the scores of each item is the total score. The Cronbach’s α coefficient for the scale in this study is 0.779.
The Intent to Leave Scale (ILS). The Chinese version of the ILS, a unidimensional structure with 4 items, is used as a survey instrument,59 using a 5-point scale ranging from “1 means strongly disagree” to “5 means strongly agree”. Item 4 is reverse scored and the sum of the scores of each item is the total score, thus the higher the score, the higher the intent to leave. The Cronbach’s α coefficient of the scale in this study is 0.792.
The Occupational Disidentification Scale (ODS). The Chinese version of the ODS is adopted as the survey instrument,60 which is a unidimensional structure consisting of 3 items, rated on a 7-point scale ranging from “1 means not at all” to “7 means fully”. The sum of the scores of each item is the total score, and the higher the score, the higher the level of disidentification with one’s own career. The Cronbach’s α coefficient of the scale in this study is 0.709.
Data Analysis
Data from Study 2 were used for tests of CFA, criterion validity analysis, reliability, and cross-group invariance. First, CFA using AMOS 24.0 indicated that a good model fit provided the following conditions were met: χ2/df < 3, RMSEA < 0.08, CFI, IFI, TLI > 0.90, PNFI, PCFI > 0.50.61 Second, Pearson correlation analysis was conducted to calculate the relevance of the PIOSS to career commitment, workplace well-being, the doctor with patient-doctor relationship, intent to leave, and occupational disidentification. Third, the reliability of the PIOSS was assessed utilizing Cronbach’s α coefficient and split-half reliability, suggesting that the reliability of the scale would be high in the event of the reliability coefficient being greater than 0.70.62 Fourth, the test of cross-gender invariance was performed using AMOS 24.0 to build the four models sequentially, namely the configural invariance model (M1), and the weak invariance model (M2), the strong invariance model (M3), and the strict invariance model (M4). M1 was the same for males and females in terms of the number and affiliation of items, without any added restrictions. M2 was to set factor loadings equal on the basis of M1, M3 was to set intercept equal on the basis of M2, and M4 was to set error variances equal on the basis of M3. The differences in CFI and RMSEA between M2 and M1, M3 and M2, and M4 and M3 were calculated sequentially, with ΔCFI<0.01 and ΔRMSEA<0.01 as the standard for invariance to hold.63
Results
Confirmatory Factor Analysis (CFA)
It is demonstrated by the CFA results that the three-factor model fits well with each fit indices of χ2/df=2.574, RMSEA=0.068, CFI=0.931, IFI=0.931, TLI=0.919, PNFI=0.762, and PCFI=0.795.
Test of Criterion-Related Validity
The results of the correlation analysis (see Table 3) reveal that the total PIOSS score and each dimension score are notably negatively associated with the CCS and the WWBS (p<0.01), with correlation coefficients ranging from −0.25 to −0.60, and they are significantly positively related to the DDPRQ-10, the ILS, and the ODS (p<0.01), with correlation coefficients ranging from 0.31 to 0.73.
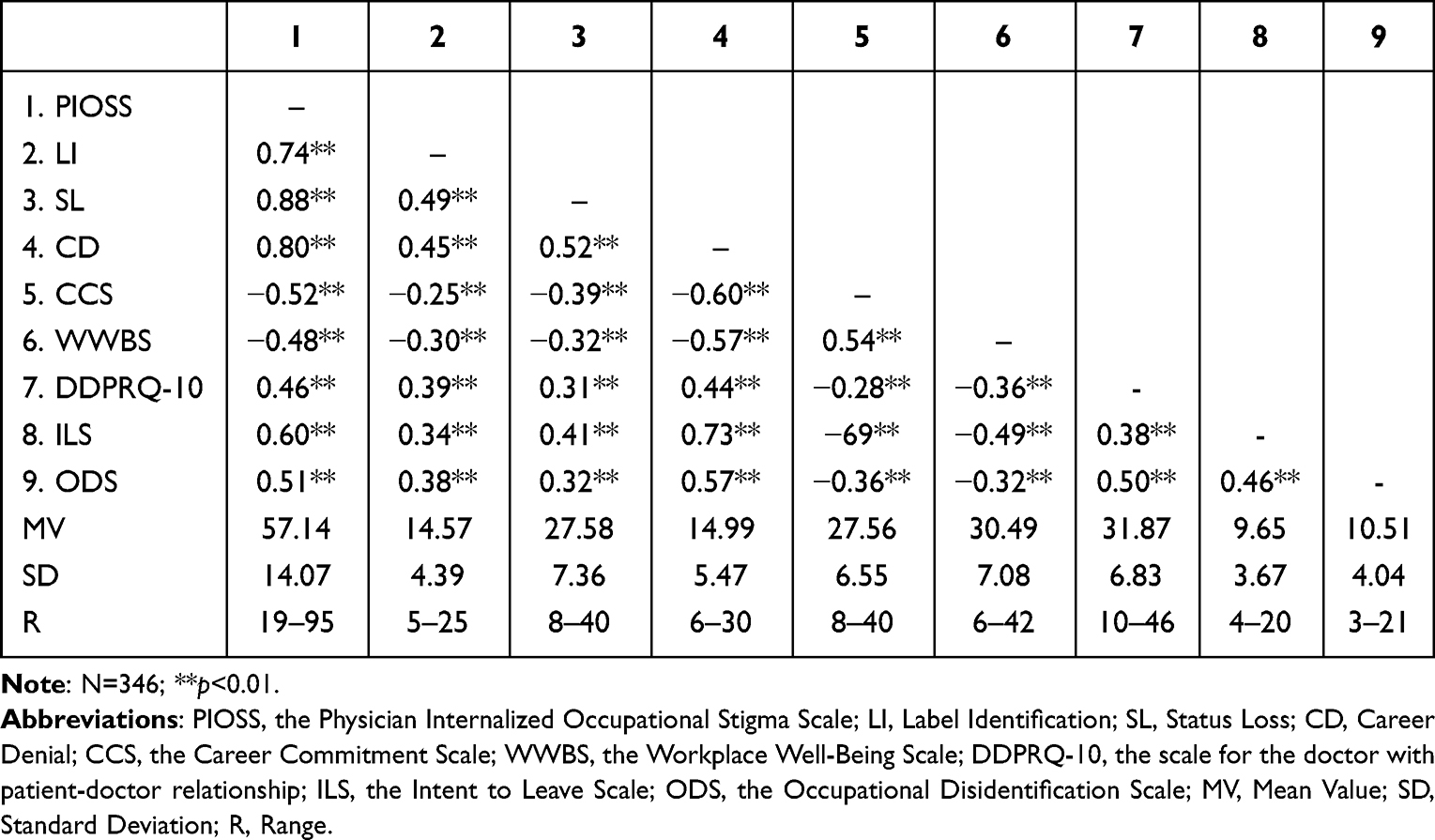 |
Table 3 Criterion Validity Test of the PIOSS |
Reliability Test
The Cronbach’s α coefficients for the PIOSS total scale and dimensions range from 0.775 to 0.914, with split-half reliability coefficients ranging from 0.801 to 0.931, all of which are above the standard of 0.70 (see Table 4).
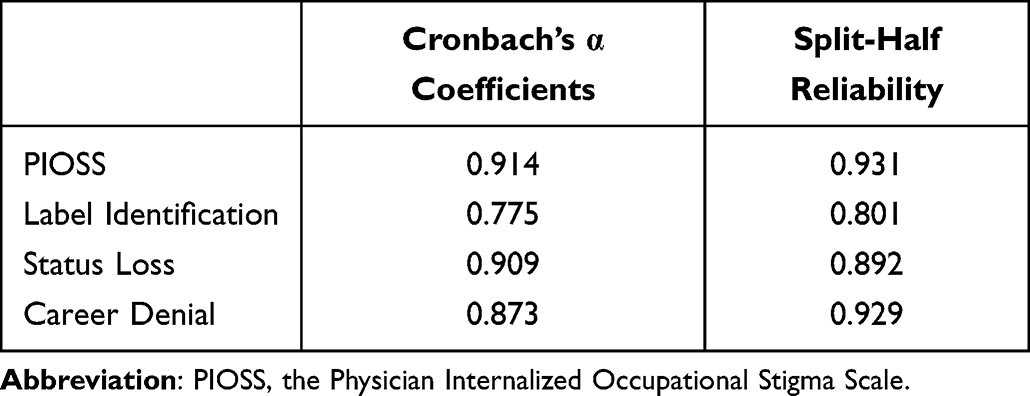 |
Table 4 Reliability Test of the PIOSS |
Cross-Gender Invariance Test
The results of the cross-gender invariance test are shown in Table 5. In the M1, M2, M3, and M4, all fit indices satisfy the requirements of psychometrics and the prerequisites for equivalence testing. CFI and RMSEA were compared between M2 and M1, M3 and M2, and M4 and M3, respectively, with ∆CFI and ∆RMSEA less than the criterion of 0.01, illustrating that the PIOSS exhibits cross-gender invariance.
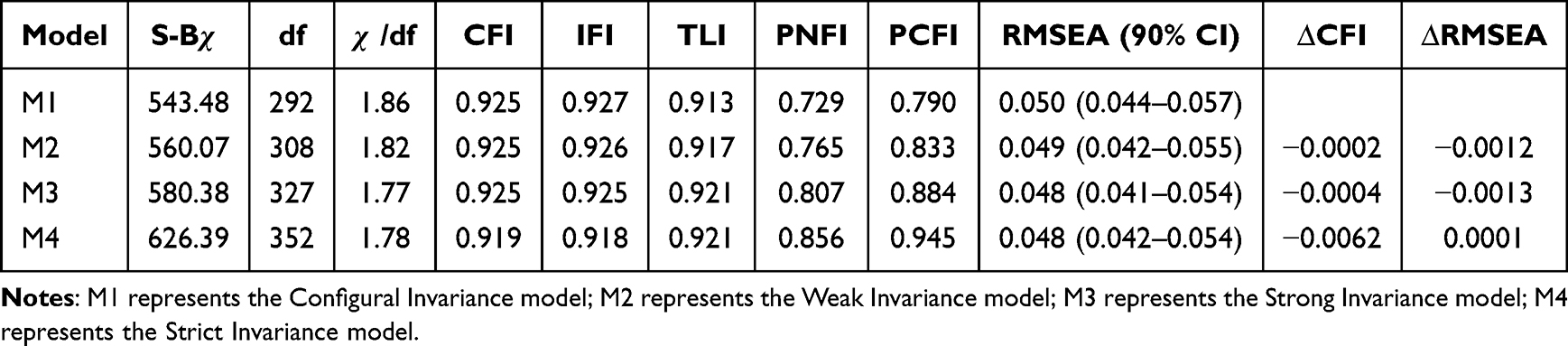 |
Table 5 Comparative Results of Nested Models for Cross-Gender Invariance Analysis of the PIOSS |
General Discussion
As physicians perceive stigmatizing comments and remarks related to their profession, they will engage in different coping strategies, where confronting or counting perceptions and behaviors and occupational ideologies are adaptive coping strategies while internalizing stigma is a maladaptive strategy.64 Physician stigma is currently increasingly prevalent which is seriously threatening their occupational development and the construction of a physician-patient trust relationship. Although it is undeniable that stigma is difficult to eliminate, it can be dramatically reduced with positive interventions.65 It is urgent to develop a scale with good reliability and validity in order to assess the effectiveness of the intervention. To this end, following the requirements of psychometrics using conceptualizing stigma theory as the theoretical framework, the present study combined semi-structured interviews and expert reviews to develop an initial questionnaire with 26 items. The 7 items were deleted after item analysis and EFA, leaving 19 items divided into 3 dimensions of label identification, status loss, and career denial, for which CFA verified the rationality of the three-factor structure.
Label identification, consisting of five items, is the identification of physicians to the public stigma that is internalized as part of their self-occupational evaluation. Simplistically, it means that physicians accept and endorse externally imposed stigma, with similar stigmatized views of their profession, and act accordingly. While the essence of occupational stigma is a kind of negative stereotype and negative label.66 A fixed stereotype is formed by the public about the behavior of a small number of physicians who do not conform to social norms and violations, which serves as a guideline for the evaluation, analysis, and supervision of the community of physicians. Physicians are gradually forced to identify themselves as “labeled” given the pressure of the social environment in which they view behaviors that are not in line with occupational norms as normal. The higher the score on this dimension, the more individuals identify with the negative labels of their occupation, while the more they tend to believe that it is understandable and acceptable to the prescription of expensive drugs, receipt of gifts from patients, demands for unnecessary medical tests, violation of medical fairness, and exaggeration of medical conditions.
Status loss, comprising eight items, refers to the extent to which physicians perceive their occupation to be devalued and discriminated against. The individuals’ evaluation of their occupational status is directly influenced by the identification with demeaning and humiliating negative labels.34 Physicians are typically a high prestige occupation enjoying superior social status, whereas the cognitive contradiction between occupational stigma and high occupational prestige can exacerbate physicians’ psychological dissonance, thus experiencing a strong sense of unfairness and disrespect, which finally leads to a decline in the evaluation of their occupational status.3 The higher the score on this dimension, the more individuals tend to believe that the public lacks understanding, trust, and respect for physicians and that their frequent blaming, criticism and unfair treatment of physicians are capable of damaging their occupational prestige and decreasing their social status.
Career denial, composed of six items, involves physicians’ denial and disapproval of their occupational values and career options, which is the negative result of label identification and status loss. It is the concern of individuals who are aware of public devaluation and discrimination against the physician community that they will likewise experience similar experiences as members of the physician,67 with this threatening their occupational identification and evaluation, producing impaired self-esteem and reduced quality of life. Consequently, individuals may resort to the denial of the correctness of their career choice, reduction of the evaluation of their occupational value, or even voluntary separation from the career to avoid potential harm. Typically, a negative outcome of decreased sense of occupational value and meaningfulness, and increased occupational disapproval and intent to leave is associated with occupational stigma.68,69 Individuals with high scores on this dimension tend to deny their occupational choices and deem themselves unsuitable for medical work, as well as struggle to derive a sense of value from their work, while they also avoid mentioning their work to others with serious consideration of changing careers.
The results of the correlation analysis reveal that the PIOSS total score and dimensional scores are statistically significantly and negatively correlated with the CCS and the WWBS scores, whereas significantly positively associated with the DDPRQ-10, the ILS, and the ODS scores. That means that physicians with high internalized occupational stigma derive fewer positive emotions and happy experiences from their work, exhibit negative attitudes toward their career and lower career identification, with a higher intent to leave, as well as worse evaluations of the physician-patient relationship. The results are consistent with the study hypothesis, suggesting that not only the PIOSS has good criterion validity, but also the assessment and intervention of physician internalized occupational stigma may be of substantial value to research and practice in health care. Yan et al, found that about half of physicians have the intent to leave, which may contribute to the shortage of physicians and inadequate medical resources.70 Furthermore, the physician-patient relationship problems are manifested not only in patients’ criticism and accusations against physicians, but also in physicians’ dissatisfaction with patients.71 This study illustrates that an approach can be taken from the perspective of the reduction of physician internalized occupational stigma for the improvement of physicians’ evaluation and identification with their career and the physician-patient relationship.
The Cronbach’s α coefficients for the total scale and dimensions of the PIOSS range from 0.775 to 0.914, with split-half reliability coefficients ranging from 0.801 to 0.931, all of which are above the 0.70 standard, indicating that it is the same construct being measured by each item of the scale with good invariance. In addition, the study further tested the cross-gender invariance of the PIOSS with the result of the configural invariance model, the weak invariance model, the strong invariance model, and the strict invariance model of it all being valid, which demonstrated the invariance of the PIOSS for cross-gender comparisons. That is, potential gender differences in physician internalized occupational stigma would be interpreted as practical differences, rather than instrumental inequivalence. In conclusion, the PIOSS developed in the study fulfills the requirements of psychometrics regarding reliability and validity, which is a valid tool to assess physician internalized occupational stigma.
This study is of certain theoretical value. First, the three-factor structure of internalized occupational stigma among physicians extracted from the study is largely compatible with the conceptualizing stigma theory.34 Label identification is an individual’s recognition of the public’s identification and labeling of negative traits of physicians. Status loss and career denial reflect the negative outcomes of stigma, manifesting the relevant contents of devaluation, discrimination, rejection, and exclusion. The conceptualizing stigma theory in previous studies has been mostly used to explain the stigma of the disabled, mental illness, and AIDS. The current study has validated and extended the theory in the field of occupational stigma. Second, the study provided an exploration and validation of the internal structure of internalized occupational stigma among physicians, offering a valid tool for further quantitative research in the future. Third, the factor analysis and criterion-related validity analysis enriched the comprehension of the concept of physician internalized occupational stigma.
The study is of certain practical value. While occupational stigma is one of the career distress that practitioners have to face, internalized occupational stigma may exert a negative influence on practitioners’ career identification, work attitude, performance, career commitment, and psychological well-being. The results of the study serve to provide instrumental support for assessing the degree of physician internalized occupational stigma, probing into the influencing factors and harms of internalized occupational stigma, analyzing the key populations for interventions, and evaluating the effectiveness of interventions. Meanwhile, taking targeted measures to intervene in physician internalized occupational stigma is conducive to easing the increasingly tense physician-patient relationship and improving the trust between physicians and patients.
Limitations and Future Research
Some limitations remain in this study. First, internalized occupational stigma, a complex concept with rich content, is classified into three dimensions: label identification, status loss, and career denial, which is not able to cover all connotations of physician internalized occupational stigma. It is noteworthy that no stigma theory has been widely accepted by most scholars to date. Therefore, more studies should be conducted to verify whether the three-factor structure proposed in this study is the optimal one for physician internalized occupational stigma. Second, there is still insufficient sample representativeness in the absence of a strict random sampling approach, although the study covers different provinces in the eastern, central, western, and northeast regions of China to expand the sampling range. Third, physician internalized occupational stigma was assessed through the self-report, not only making it difficult to avoid the influence of social expectation effects but also potentially generating common method bias. In specific intervention practices, it should be combined with qualitative interviews and an implicit association test (IAT) to be more comprehensive and accurate in the assessment of the effectiveness of interventions. Fourth, the present study was conducted with Chinese physicians only, and whether the PIOSS has good applicability in other cultural contexts still requires more validation. In particular, more empirical evidence is needed to determine whether the PIOSS has cross-cultural invariance. Fifth, the current study does not conduct an examination of the test-retest reliability, and the stability of the PIOSS across time needs to be tested in future studies.
Conclusions
The increasing prevalence of stigmatizing statements by physicians is a serious threat to the establishment of a trusting physician-patient relationship. Physicians internalize negative labels related to their profession as part of their self-evaluation, which can lead to the formation of internalized occupational stigma. Meanwhile, internalized occupational stigma has a negative impact on physicians’ career development, professional identity, and mental health. Hence, carrying out quantitative research and intervention studies on physician internalized occupational stigma requires the development of an assessment tool with good reliability and validity. Following psychometric requirements, the current study developed the Physician Internalized Occupational Stigma Scale (PIOSS) by taking conceptualizing stigma theory as the theoretical framework. The PIOSS consists of 19 items divided into 3 dimensions: label identification, status loss, and career denial. The PIOSS features favorable psychometric properties and can be utilized as a valid tool for assessing physician internalized occupational stigma.
Ethics Statement
Both study 1 and study 2 were approved by the Ethics Committee of Jilin International Studies University (Project Number: JY202111001). An anonymous survey was conducted in both studies, and informed consent was obtained from the participants before starting the survey who all signed the informed consent form. Both studies were in accordance with the Declaration of Helsinki.
Acknowledgments
We are very much thankful to all the researchers for data collection and processing. We thank all the survey participants in our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Social Science Research Project of the Education Department of Jilin Province “The research on the influence of the employment view of college students of traditional Chinese medicine on the employment quality” (Project No. JJKH20211014JY).
Disclosure
The authors report no conflicts of interest in this work.
References
1. He AJ, Ma L. Citizen participation, perceived public service performance, and trust in government: evidence from health policy reforms in Hong Kong. Public Perform Manag Rev. 2021;44:471–493. doi:10.1080/15309576.2020.1780138
2. Aparicio M, Centeno C, Robinson C, Arantzamendi M. Gratitude between patients and their families and health professionals: a scoping review. J Nurs Manag. 2019;27(2):286–300. doi:10.1111/jonm.12670
3. Sun T, Wang J, Zhang S, Shi Y, Liu B, Wang X. Status, causes and consequences of physicians’ self-perceived professional reputation damage in China: a cross-sectional survey. BMC Health Serv Res. 2021;21(1):344. doi:10.1186/s12913-021-06306-6
4. Gong W, Guo Q. Framing public opinion on physician-patient conflicts on microblog: a comparative content analysis. Front Public Health. 2022;10:831638. doi:10.3389/fpubh.2022.831638
5. Richmond J, Boynton MH, Ozawa S, Muessig KE, Cykert S, Ribisl KM. Development and validation of the trust in my doctor, trust in doctors in general, and trust in the health care team scales. Soc Sci Med. 2022;298:114827. doi:10.1016/j.socscimed.2022.114827
6. Torales J, González RE, Ríos-González C, et al. Spanish validation of the Stigma of Occupational Stress Scale for Doctors (SOSS-D) and factors associated with physician burnout. Ir J Psychol Med. 2022:1–8. doi:10.1017/ipm.2022.41
7. Khan S, Akter S, Khan T, Shariar G, Awal Miah MA. Psychological distress among Bangladeshi physicians: roles of perceived stigma, fear of infection and resilience in the context of Covid-19 pandemic. J Soc Distress Homeless. 2022;31(1):105–114. doi:10.1080/10530789.2021.1892932
8. Wijeratne C, Johnco C, Draper B, Earl J. Doctors’ reporting of mental health stigma and barriers to help-seeking. Occup Med. 2021;71(8):366–374. doi:10.1093/occmed/kqab119
9. Nie JB, Li L, Gillett G, Tucker JD, Kleinman A. The crisis of patient-physician trust and bioethics: lessons and inspirations from China. Dev World Bioeth. 2018;18(1):56–64. doi:10.1111/dewb.12169
10. Lin J, Zhou J, Wang L. Health care reform in China from the perspective of physicians. Biosci Trends. 2020;14(2):151–155. doi:10.5582/bst.2020.01015
11. Nie JB, Cheng Y, Zou X, et al. The vicious circle of patient-physician mistrust in China: health professionals’ perspectives, institutional conflict of interest, and building trust through medical professionalism. Dev World Bioeth. 2018;18(1):26–36. doi:10.1111/dewb.12170
12. Liang Z, Xu M, Liu G, Zhou Y, Howard PF. Doctors in Chinese public hospitals: demonstration of their professional identities. BMC Med Educ. 2020;20(1):501. doi:10.1186/s12909-020-02339-3
13. Salomon F. Okonomie und Ethik im Klinikalltag - Der Arzt im Spannungsfeld zwischen Patientenwohl und Wirtschaftlichkeit. Economy and ethics in daily hospital routine - physicians in conflict between the well-being of patients and profitability. Anasthesiol Intensivmed Notfallmed Schmerzther. 2010;45(2):128–131. doi:10.1055/s-0030-1248148
14. Chan C, Yao Z. A market of distrust: toward a cultural sociology of unofficial exchanges between patients and doctors in China. Theory Cult Soc. 2018;47:1–36. doi:10.1007/s11186-018-09332-2
15. Wang Q. Doctor-Patient Communication and Patient Satisfaction: A Cross-Cultural Comparative Study Between China and the US. Purdue University; 2012.
16. Pinel EC, Paulin N. Stigma consciousness at work. Basic Appl Soc Psych. 2005;27(4):345–352. doi:10.1207/s15324834basp2704_7
17. Ashford RD, Brown AM, McDaniel J, Curtis B. Biased labels: an experimental study of language and stigma among individuals in recovery and health professionals. Subst Use Misuse. 2019;54(8):1376–1384. doi:10.1080/10826084.2019.1581221
18. Dopelt K, Bachner YG, Urkin J, Yahav Z, Davidovitch N, Barach P. Perceptions of practicing physicians and members of the public on the attributes of a “good doctor”. Healthcare. 2021;10(1):73. doi:10.3390/healthcare10010073
19. Wu QL, Tang L. What satisfies parents of pediatric patients in China: a grounded theory building analysis of online physician reviews. Health Commun. 2022;37(10):1329–1336. doi:10.1080/10410236.2021.1888437
20. Ashforth B, Kreiner G. ”How can you do it?”: dirty work and the challenge of constructing a positive identity. Acad Manage Rev. 1999;24(413). doi:10.2307/259134
21. Ashforth B, Kreiner G, Clark M, Fugate M. Normalizing dirty work: managerial tactics for countering occupational taint. Acad Manage J. 2007;50:149–174. doi:10.5465/AMJ.2007.24162092
22. Sang T, Zhou H, Li M, et al. Investigation of the differences between the medical personnel’s and general population’s view on the doctor-patient relationship in China by a cross-sectional survey. Global Health. 2020;16(1):99. doi:10.1186/s12992-020-00625-9
23. Hansen Löfstrand C, Loftus B, Loader I. Doing ‘dirty work’: stigma and esteem in the private security industry. Eur J Criminol. 2015;13(3):297–314. doi:10.1177/1477370815615624
24. Manchha A, Way K, Tann K, Thai M. The social construction of stigma in aged-care work: implications for health professionals’ work intentions. Gerontologist. 2022;62(1):994–1005. doi:10.1093/geront/gnac002
25. Bosson JK, Swann WB. Self-liking, self-competence, and the quest for self-verification. Pers Soc Psychol Bull. 1999;25(10):1230–1241. doi:10.1177/0146167299258005
26. Zhang H, Liu Y, Shi Y, Zhang N. The effect of customer-initiated support on employee service performance: the self-verification theory perspective. Acta Psychol Sin. 2022;54(4):398–410. doi:10.3724/SP.J.1041.2022.00398
27. Wen LL, Xiang K, Gao F, Zhou J. Occupational stigma perception, emotional exhaustion state, and professional commitment response: understanding the mechanisms underlying hotel interns’ perceptions of career prospects. Front Psychol. 2022;13:798526. doi:10.3389/fpsyg.2022.798526
28. Bianchi R, Verkuilen J, Brisson R, Schonfeld IS, Laurent E. Burnout and depression: label-related stigma, help-seeking, and syndrome overlap. Psychiatry Res. 2016;245:91–98. doi:10.1016/j.psychres.2016.08.025
29. Ries NM, Jansen J. Physicians’ views and experiences of defensive medicine: an international review of empirical research. Health Policy. 2021;125(5):634–642. doi:10.1016/j.healthpol.2021.02.005
30. Shantz A, Booth J. Service employees and self-verification: the roles of occupational stigma consciousness and core self-evaluations. Hum Relat. 2014;67(12):1439–1465. doi:10.1177/0018726713519280
31. Baran BE, Rogelberg SG, Carello Lopina E, Allen JA, Spitzmüller C, Bergman M. Shouldering a silent burden: the toll of dirty tasks. Hum Relat. 2012;65(5):597–626. doi:10.1177/0018726712438063
32. Kusluvan H, Akova O, Kusluvan S. Occupational stigma and career commitment: testing mediation and moderation effects of occupational self-esteem. Int J Hosp Manag. 2022;102:103149. doi:10.1016/j.ijhm.2022.103149
33. Hirsch J, Sirois F, Visser P, et al. Perceived stigma and health-related quality of life in the working uninsured: does thwarted belongingness play a role? Stigma Health. 2017;4(1):1–10. doi:10.1037/sah0000116
34. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol. 2001;27(1):363–385. doi:10.1146/annurev.soc.27.1.363
35. Pinel EC. Stigma consciousness: the psychological legacy of social stereotypes. J Pers Soc Psychol. 1999;76(1):114–128. doi:10.1037//0022-3514.76.1.114
36. Zhao Y, Zhan J. Platform riders’ occupational stigma consciousness and workplace deviant behavior: the mediating role of self-depletion. Balt J Manag. 2022;17(2):233–249. doi:10.1108/BJM-06-2021-0215
37. Stockton MA, Kraemer J, Oga E, et al. Validation of a brief internalized sex-work stigma scale among female sex workers in Kenya. J Sex Res. 2021:1–7. doi:10.1080/00224499.2021.1983752
38. Kim HL, Hyun SS. Developing a stigma scale for the workplace: focus on an airline cabin crew. Int J Environ Res Public Health. 2021;18(8). doi:10.3390/ijerph18084003
39. Yang L, Zhang S, Leng J, Fan Z, Luo Y. Development of the nurse occupational stigma scale. Psychol Res Behav Manag. 2022;15:1627–1636. doi:10.2147/prbm.S362709
40. Healey L. The psychometric properties of the Forensic Stigma Scale (FSS). Int J Law Psychiatry. 2022;83:101804. doi:10.1016/j.ijlp.2022.101804
41. Fan Z, Chen H, Wu H, Zhang X. Patient toward physician occupational stigma scale: development of the Chinese version. Psychol Res Behav Manag. 2022;15:2117–2127. doi:10.2147/prbm.S375032
42. Shiu C, Chen WT, Hung CC, Huang EP, Lee TS. COVID-19 stigma associates with burnout among healthcare providers: evidence from Taiwanese physicians and nurses. J Formos Med Assoc. 2022;121(8):1384–1391. doi:10.1016/j.jfma.2021.09.022
43. Zhang R, Wang MS, Toubiana M, Greenwood R. Stigma beyond levels: advancing research on stigmatization. Acad Manag Ann. 2020. doi:10.5465/annals.2019.0031
44. Carpenter S. Ten steps in scale development and reporting: a guide for researchers. Commun Methods Meas. 2018;12(1):25–44. doi:10.1080/19312458.2017.1396583
45. Worthington RL, Whittaker TA. Scale development research: a content analysis and recommendations for best practices. Couns Psychol. 2006;34(6):806–838. doi:10.1177/0011000006288127
46. Gehlbach H, Brinkworth ME. Measure twice, cut down error: a process for enhancing the validity of survey scales. Rev Gen Psychol. 2011;15(4):380–387. doi:10.1037/a0025704
47. McNeish D. Thanks coefficient alpha, we’ll take it from here. Psychol Methods. 2018;23(3):412–433. doi:10.1037/met0000144
48. Henson RK, Roberts JK. Use of exploratory factor analysis in published research: common errors and some comment on improved practice. Educ Psychol Meas. 2006;66(3):393–416. doi:10.1177/0013164405282485
49. Flora D, Flake J. The purpose and practice of exploratory and confirmatory factor analysis in psychological research: decisions for scale development and validation. Can J Behav Sci. 2017;49(2):78–88. doi:10.1037/cbs0000069
50. Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychol Methods. 1999;4(3):272–299. doi:10.1037/1082-989x.4.3.272
51. Morrison JT. Evaluating factor analysis decisions for scale design in communication research. Commun Methods Meas. 2009;3(4):195–215. doi:10.1080/19312450903378917
52. Hobfoll S, Halbesleben J, Neveu J-P, Westman M. Conservation of resources in the organizational context: the reality of resources and their consequences. Annu Rev Organ Psychol Organ Behavr. 2018;5(1):103–128. doi:10.1146/annurev-orgpsych-032117-104640
53. Hobfoll S. Conservation of resource caravans and engaged settings. J Occup Organ Psychol. 2011;84:116–122. doi:10.1111/j.2044-8325.2010.02016.x
54. Fox AB, Quinn DM. Pregnant women at work: the role of stigma in predicting women’s intended exit from the workforce. Psychol Women Q. 2015;39(2):226–242. doi:10.1177/0361684314552653
55. Janiak E, Freeman S, Maurer R, Berkman LF, Goldberg AB, Bartz D. Relationship of job role and clinic type to perceived stigma and occupational stress among abortion workers. Contraception. 2018;98(6):517–521. doi:10.1016/j.contraception.2018.07.003
56. Gary JB. The measurement and prediction of career commitment. J Occup Psychol. 1985;58(4):277–288. doi:10.1111/j.2044-8325.1985.tb00201.x
57. Zheng X, Zhu W, Zhao H, Zhang C. Employee well-being in organizations: theoretical model, scale development, and cross-cultural validation. J Organ Behav. 2015;36:621–644. doi:10.1002/job.1990
58. Hahn SR, Kroenke K, Spitzer RL, et al. The difficult patient: prevalence, psychopathology, and functional impairment. J Gen Intern Med. 1996;11(1):1–8. doi:10.1007/bf02603477
59. O’Reilly C, Chatman J, Caldwell D. People and organizational culture: a profile comparison approach to assessing person-organization fit. Acad Manage J. 1991;34:487–516. doi:10.2307/256404
60. Schaubroeck JM, Lam LW, Lai JYM, Lennard AC, Peng AC, Chan KW. Changing experiences of work dirtiness, occupational disidentification, and employee withdrawal. J Appl Psychol. 2018;103(10):1086–1100. doi:10.1037/apl0000330
61. Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychol Bull. 1980;88(3):588–606. doi:10.1037/0033-2909.88.3.588
62. Viladrich C, Angulo-Brunet A, Doval E. A journey around alpha and omega to estimate internal consistency reliability. An Psicol. 2017;33(3):755–782. doi:10.6018/analesps.33.3.268401
63. Cheung G, Rensvold R. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Modeling. 2002;9(2):233–255. doi:10.1207/S15328007SEM0902_5
64. Bosmans K, Mousaid S, De Cuyper N, Hardonk S, Louckx F, Vanroelen C. Dirty work, dirty worker? Stigmatisation and coping strategies among domestic workers. J Vocat Behav. 2016;92:54–67. doi:10.1016/j.jvb.2015.11.008
65. Carrara BS, Fernandes RHH, Bobbili SJ, Ventura CAA. Health care providers and people with mental illness: an integrative review on anti-stigma interventions. Int J Soc Psychiatry. 2021;67(7):840–853. doi:10.1177/0020764020985891
66. Morrow LC. Cyclical role-playing and stigma: exploring the challenges of stereotype performance among exotic dancers. Deviant Behav. 2012;33(5):357–374. doi:10.1080/01639625.2011.584277
67. Mejia C, Pittman R, Beltramo JMD, Horan K, Grinley A, Shoss MK. Stigma & dirty work: in-group and out-group perceptions of essential service workers during COVID-19. Int J Hosp Manag. 2021;93:102772. doi:10.1016/j.ijhm.2020.102772
68. Huang B, Ma L, Huang L. My work is meaningless: the consequences of perceived occupational stigma for employees in high-prestige occupations. Front Psychol. 2022;13:715188. doi:10.3389/fpsyg.2022.715188
69. Manchha AV, Walker N, Way KA, Dawson D, Tann K, Thai M. Deeply discrediting: a systematic review examining the conceptualizations and consequences of the stigma of working in aged care. Gerontologist. 2021;61(4):129–146. doi:10.1093/geront/gnaa166
70. Yan S, Shen X, Wang R, et al. The prevalence of turnover intention and influencing factors among emergency physicians: a national observation. Hum Resour Health. 2021;19(1):149. doi:10.1186/s12960-021-00688-8
71. Fosnot L, Jones CD, Keniston A, Burden M, Indovina KA, Patel H. Hospitalists’ perspectives on challenging patient encounters and physician well-being: a qualitative study. Patient Educ Couns. 2022;105(5):1209–1215. doi:10.1016/j.pec.2021.08.023
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.