")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Development of Hypertension and Diabetes Mellitus, and Associated Factors, Among Adult HIV Patients in Ethiopia
Authors Tegene Y , Mengesha S, Putman E, Toma A , Spigt M
Received 14 November 2022
Accepted for publication 14 February 2023
Published 16 February 2023 Volume 2023:15 Pages 41—51
DOI https://doi.org/10.2147/HIV.S397511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Yadessa Tegene,1 Selamawit Mengesha,1 Erin Putman,2 Alemayehu Toma,3 Mark Spigt2,4
1School of Public Health, College of Medicine and Health Science, Hawassa University, Hawassa, Ethiopia; 2School CAPHRI, Department of Family Medicine, Maastricht University, Maastricht, Netherlands; 3School of Medicine, College of Medicine and Health Science, Hawassa University, Hawassa, Ethiopia; 4General Practice Research Unit, Department of Community Medicine, UiT the Arctic University of Norway, Tromsø, Norway
Correspondence: Yadessa Tegene, Master of Science in Nutrition, School of Public Health, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia, Email [email protected]
Background: Medical improvements and increased access to treatment have turned HIV from a highly fatal disease into a treatable and controllable disease. With the improvement in lifespan, HIV patients face increasing morbidity and mortality from chronic comorbidities (hypertension and diabetes mellitus). There is, nevertheless, a paucity of information on the scale of HIV noncommunicable disease comorbidity and its associated factors. This study aimed to investigate the incidence and predictors of chronic comorbidity in HIV patients in a resource-limited setting.
Methods: A prospective cohort study was conducted from 2019 to 2021. We included 520 HIV patients at baseline. Patients without hypertension or diabetes were followed for two years to determine the incidence of developing comorbidities. Nine trained nurses used a pre-tested structured questionnaire to collect data during routine care consultations in three hospitals in southern Ethiopia. To find predictors of these chronic comorbidities, a multivariable logistic regression analysis was used.
Results: After two years, 54 out of 377 participants, or 14%, had chronic comorbidity, which is defined as having diabetes and/or hypertension. Hypertension (12%) and diabetes (4%), respectively, were observed. When compared to those who were not overweight, the risk of developing chronic comorbidity was three times higher in overweight people [AOR = 3.45, 95% CI: (1.04, 11.45), P = 0.045]. Older participants were about 6 times more likely than younger participants to have chronic comorbidity [AOR = 4.93, 95% CI: (1.56, 15.57), P = 0.007]. Those who did not engage in regular physical activity were twice as likely to develop chronic comorbidity [AOR = 2.16, 95% CI: (1.09, 4.29), P = 0.027].
Conclusion: The incidence of chronic comorbidity was high in the study population. Targeted screening for early signs of chronic comorbidity, nutritional counseling, and awareness creation in regular physical activity programs should be integrated into HIV care to prevent and control chronic comorbidity in resource-limited settings.
Keywords: chronic comorbidity, people living with HIV, nutritional status, antiretroviral therapy, South Ethiopia
Introduction
With 37.7 million people infected in 2020, the Human Immunodeficiency Virus (HIV) is a major worldwide concern.1 Approximately 20 million people living with HIV (PLHIV) reside in East and South Africa in 2019.2 Ethiopia is one of the countries with the highest HIV burden worldwide, with an estimated prevalence of 613,000 in 2017.3,4 Medical improvements and increased access to HIV treatment, such as combination antiretroviral therapy (ART), have led to a shift from a highly fatal to a treatable and controllable disease.5–9 With the improvement in lifespan, PLHIV faces increasing morbidity and mortality from non-communicable diseases (NCD) like diabetes mellitus and cardiovascular disease.10 This double burden of HIV and chronic comorbidity is particularly challenging for resource-limited countries, such as Ethiopia, with already constrained health care systems.11
HIV care in resource-limited settings is often not organized with care facilities for NCDs, resulting in unnecessary morbidity and mortality.5 Consequently, the rising incidence of NCDs in PLHIV may even set back the impressive health gains achieved over the past decade.5,12–14 Lifelong HIV treatment causes a complex interaction between HIV-specific factors, ART, and specific chronic disease risk factors.12 More than three-quarters of all NCD fatalities worldwide—31.4 million—occur in low- and middle-income countries, which are disproportionately affected by NCDs.15 In sub-Saharan Africa, including Ethiopia, the epidemiologic intersection between NCDs and HIV and the effects of NCDs-HIV comorbidity are expected to be significant.16,17
The World Health Organization (WHO) warns of a rise in chronic disease rates in resource-limited areas, due to an increase in risk factors, including overweight and obesity.18 Whereas initially a pattern of underweight was seen in PLHIV, the prevalence of overweight and obesity seems to be gradually increasing.19 Over nutrition is a major risk factor for developing chronic diseases, including diabetes mellitus and cardiovascular disease.6 This trend of increasing overweight is also found in Ethiopia. A hospital-based, cross-sectional study of 252 HIV patients found a prevalence of overweight of 21%.18 Another study, performed in Addis Ababa, Ethiopia, found a prevalence of 27.9% of PLHIV being overweight.20 Physical inactivity is also another risk factor for developing chronic diseases.21 The previous study in the current study area, with the same study population, shows a high level of physical inactivity.22 HIV-positive patients may have a number of NCD risk factors. Tobacco use, alcohol abuse, and poor diets (high intake of fat, salt, and processed carbs) are a few of these.21 It is important to promote appropriate nutrition among HIV patients since optimal nutrition is crucial for the prevention of NCDs.6 Existing studies on chronic comorbidity in PLHIV residing in a low-income setting, however, are scarce and often have a small sample size and a cross-sectional design.12,13,23
There is a need for more research on the incidence of chronic comorbidity in HIV patients residing in low-income settings, as research on this specific population is scarce. More insight into the occurrence and predictive factors of chronic comorbidity in HIV patients from a low-income setting provides valuable information that can ultimately be used to reduce chronic comorbidity. The aim of this research was to determine the incidence and identify predictive factors of chronic comorbidity in HIV patients living in a low-income setting.
Method
Study Design and Setting
The study was conducted at three selected hospitals in southern Ethiopia from May 2019 to June 2021 using a prospective cohort study design. The Hawassa University Comprehensive Specialized Hospital (HUCSH) is a tertiary-level specialized hospital that serves as a referral center for general hospitals. Adare and Yirgalem General Hospitals provide secondary-level health care, including preventive and curative services that require diagnostic and therapeutic intervention. HUCSH and Adare Hospital are located in Hawassa, 275 km from Addis Ababa, whereas Yirgalem Hospital is 45 kilometers away from Hawassa. At the commencement of the study on May 7, 2019, HUCSH, Adare, and Yirgalem General Hospital each provided ART treatment to 2553, 1821, and 1476 HIV patients, respectively.
Study Population and Sample Size
Adult HIV patients (≥18 years) enrolled on ART and visiting the three hospitals during the study period made up the study sample. The study had two rounds of follow-up over a 24-month period. For this analysis, we used data from both the baseline and the last round of follow-up. At the start of the study, all 520 eligible patients were assessed cross-sectionally. The baseline data from the same study population were used to assess the physical activity level and associated factors among our study participants, (https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-022-07120-z). In the base line, diabetes affected 1.5% of the population (8/520), while hypertension affected 9% of the population (49/520). The remaining 465 patients (referred to as “the cohort”) were prospectively followed at the ART clinic for the development of the outcomes of interest, namely hyperglycemia and hypertension. At the end of the second year, 377 patients were left in the cohort (Figure 1).
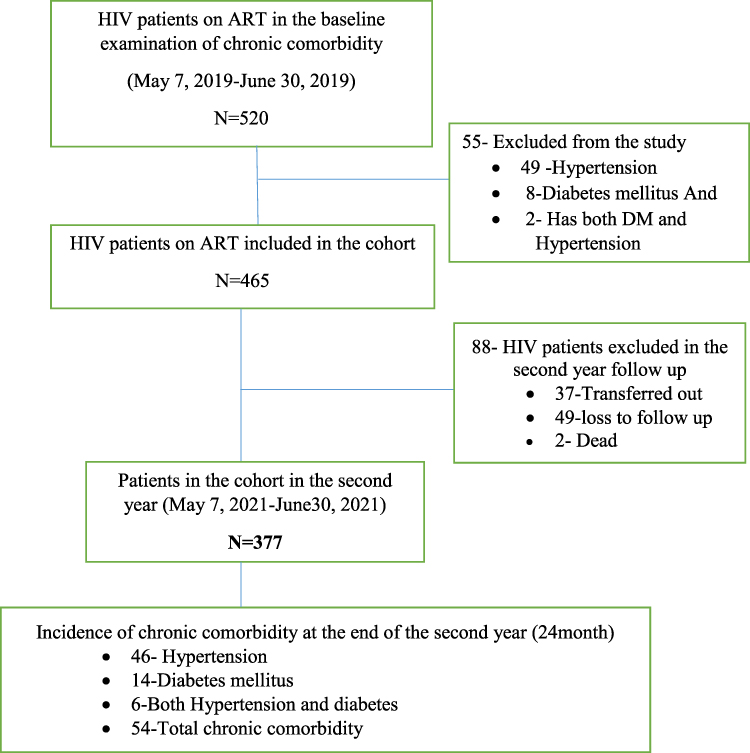 |
Figure 1 Flowchart diagram of the study profile of the participants in the three selected hospitals of South Ethiopia. |
Data Collection Methods and Procedures
Data from the participants was collected during routine consultations at the hospitals. The baseline measurement was performed in 2019 and the follow-up measurement two years later, in 2021. The data collectors, consisting of nine clinical nurses and three supervisors, attended a training course on data collection methods for three days to ensure that the data were collected in a consistent and correct manner. The questionnaire administered consisted of several aspects to elicit the sociodemographic, health, behavioral, physical activity, and nutrition-related factors of the participants. To avoid a language barrier, the questionnaire was first prepared in English and then translated into Amharic, so that the participants could complete the questionnaire in their own language. Afterwards, the completed questionnaire was translated back into English to check for consistency.
The Household Food Insecurity Access Scale (HFIAS) was used to get insight into the level of food insecurity of the participants.24 This scale consists of nine items that measure the degree of food insecurity in the past four weeks. On each item of the scale, the participants are asked how frequently the situation occurs (1 = rarely, 2 = sometimes, 3 = often). The scores on the items together will result in the participant being categorized as either secure or insecure. Data on dietary diversity was collected using the Household Dietary Diversity Score (HDDS).25 The dietary diversity score is based on different food groups, including grains; legumes; roots or tubers; fruits; vegetables; meat; milk products; eggs; fish; oil, fat, or butter; sugar or honey; and other foods such as condiments, coffee, and tea. First, the categorization of individual food scores was made into terciles as, Low IDDS (1–3 food groups); Medium IDDS (4–5 food groups); and High IDDS (≥6 food groups). Further, this score was dichotomized into two categories as low dietary diversity scores, having 0–4 and high dietary diversity scores.26
Furthermore, a calibrated digital Seca® scale was used to measure the participants’ weight in kilograms (kg). This scale measured weight to the nearest 0.1 kg. The height of the participants was measured using a stadiometer (Seca Germany). Participants were positioned at the Frankfurt plane to measure their height to the nearest 0.1 cm. To increase the reliability of the measurements, all anthropometric measurements were performed twice, with the average of the two measurements being used for further analysis. The BMI of the participants was calculated as the ratio of weight (kg) to the square of height (m) and is used to determine the nutritional status. BMI was then used to classify the participants as underweight, normal weight, and overweight. Underweight was defined as having a BMI of 18.5 kg/m2, normal weight as having a BMI of 18.5–24.9 kg/m2, and overweight as having a BMI of 25 kg/m2.27
The Fia Biomed Blood Glucose Meter (Glucometer) Salut was used to determine random blood glucose levels via finger puncture. Fasting plasma glucose levels of ≥ 126 mg/dL, 2 hour plasma glucose of ≥ 200 mg/dL during an oral glucose tolerance test, hemoglobin A1C of ≥ 6.5%, and a random plasma glucose of ≥ 200 mg/dL in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis are all considered diabetes by the American Diabetes Association.28 The participants’ blood pressure at rest was measured on the left arm using an automated sphygmomanometer. The blood pressure was measured three times in total at five-minute intervals, with the average of the last two measurements used for further analysis. The diagnosis of high BP (hypertension) was made according to the WHO criteria as systolic BP ≥ 140 mmHg or diastolic BP ≥ 90 mmHg.29 Participants were classified as having chronic comorbidity if they had either diabetes or hypertension, or both. When a participant was newly diagnosed with hypertension or diabetes, the participant was immediately referred to a specialist for further diagnosis and treatment.
Data Management and Analysis
IBM SPSS for Windows version 26.0 (IBM, USA) was used to enter, clean, code and analyze the data. Descriptive statistics were performed to describe the data with the use of proportions for categorical variables and mean ± standard deviation (SD) for continuous variables. Multivariate logistic regression analysis was run to identify predictors of chronic comorbidity in the study population. First, a binary analysis was performed to determine predictors associated with chronic comorbidity. Next, the variables were included in the multivariable logistic regression analysis. Adjusted odds ratio (AOR) with 95% Confidence Interval (CI) were calculated to assess the strength of the associations that are found. Results were considered statistical significance at a p-value <0.05.
Results
Baseline Characteristics
The majority of the study participants (63%) were female, and the prevalence of being overweight was much higher in females (29%) than in males (15%), and it was found to have a significant association with nutritional status. The age group 35–54 years constituted a larger proportion of the whole sample (61%) than the other age groups, with a mean age of 38.01±8.81 years. Most participants were single (45%) and resided in urban areas (93%). Overweight was more than twice as common among participants in urban areas (25%) than in rural areas (12%). The participants’ most common religion (50%) was Orthodox, and slightly more than half (52%) had a low income. Finally, participants with a high income (32%), compared to those with a low income (17%), were more likely to be overweight, and income level has shown a significant association with nutritional status (Table 1).
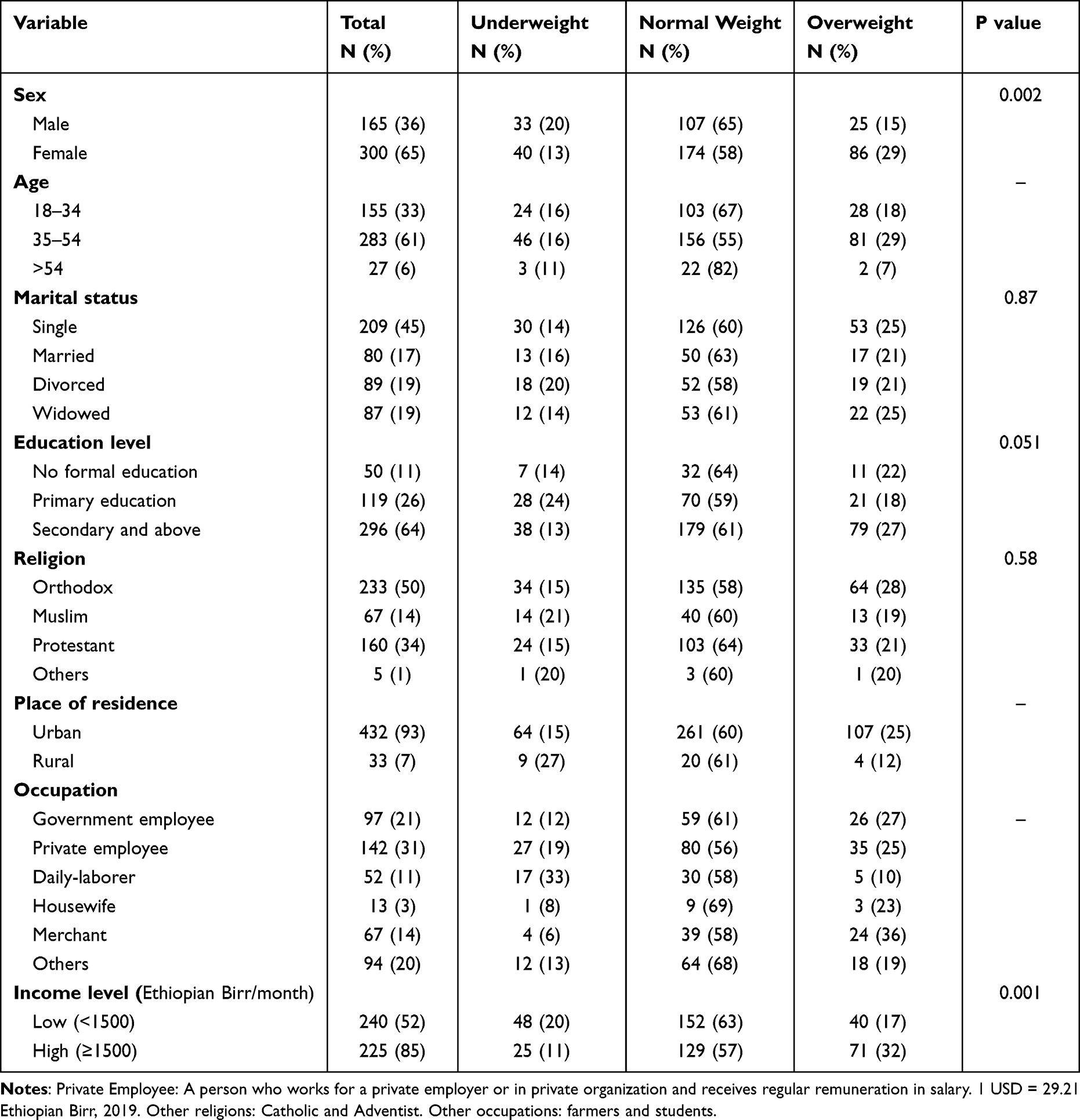 |
Table 1 Sociodemographic Characteristics of Adult HIV Patients (Baseline Cohort N = 465) |
Health and Nutrition Related Factors of the Study Participants
The majority of the participants had been treated with ART for more than 24 months (72%), with the most common regimen being TDF-3TC-EFV (53%). Most participants were not regularly physically active (53%), and the prevalence of smoking and alcohol consumption was low, at 1% and 12%, respectively. Overweight was most prevalent in participants with WHO clinical stage I (25%) and among participants with a history of alcohol consumption (39%). Alcohol consumption was found to have a significant association with nutritional status. In addition, most participants had a low dietary diversity score (56%) and were often food insecure (79%) (Table 2).
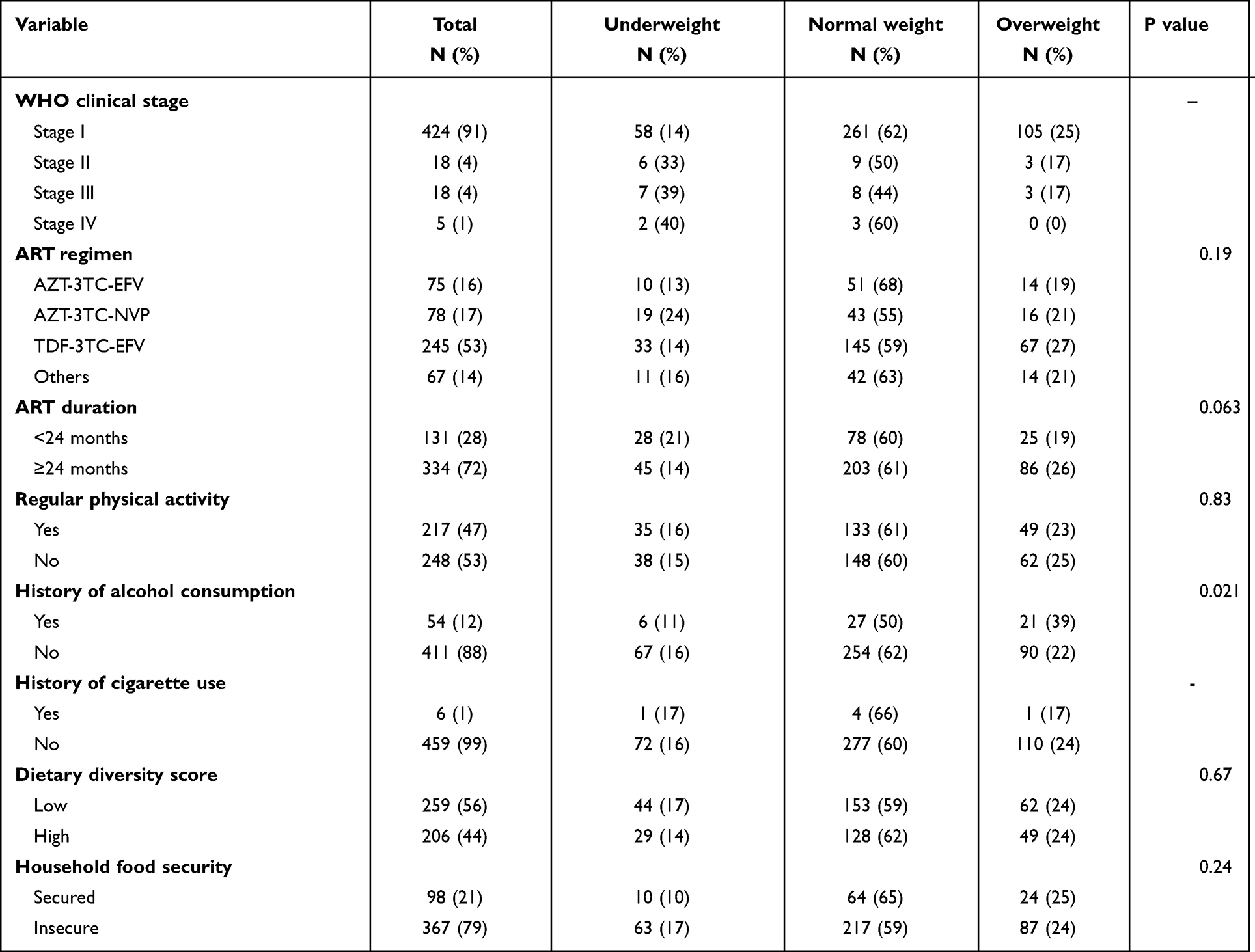 |
Table 2 Health and Nutrition Related Factors of Adult HIV Patients (Baseline Cohort N = 465) |
Chronic Comorbidity Among the Study Participants
During the two-year follow-up period, 54 out of 377 participants (14%) developed chronic comorbidity. The incidence of chronic comorbidity consisted of both hypertension (N = 46 (12%)) and diabetes (N = 14 (4%)). Six participants (2%) developed both hypertension and diabetes.
Predictors of Chronic Comorbidity in HIV Patients
In a bivariate analysis, overweight, old age, economic level, ART duration, and inadequate physical activity were all associated with the development of chronic comorbidity in adult HIV patients. These associations were analyzed further using multivariable logistic analysis, and chronic comorbidity was found to be strongly associated with being overweight, age, and a lack of regular physical activity. Participants with a BMI of ≥25 kg/m2 had a 3 times higher risk of developing chronic comorbidity than those with a normal weight (BMI 18.5–24.9 kg/m2) [AOR = 3.45, 95% CI: (1.04, 11.45), P = 0.045]. Chronic comorbidity was found to be five times more common in older (54-year-old) participants than in younger participants [AOR = 4.93, 95% CI: (1.56, 15, 57), P = 0.007]. Another characteristic that has been associated with chronic comorbidity is regular physical activity. Those who did not engage in regular physical activity were twice as likely as their counterparts to develop chronic comorbidity [AOR = 2.16, 95% CI: (1.09, 4.29), P = 0.027]. (Table 3).
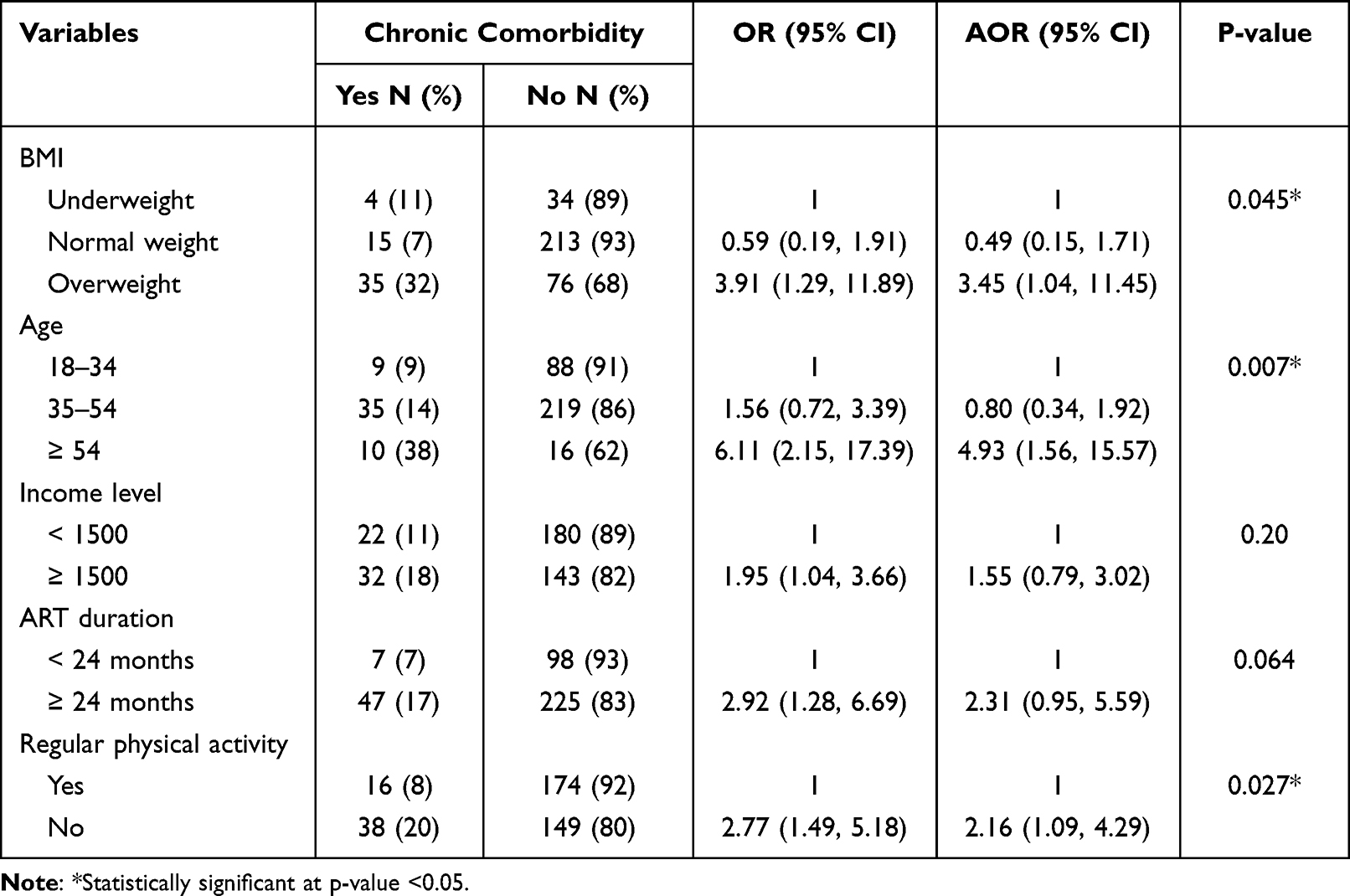 |
Table 3 Follow-Up Data on the Predictors of the Development of Chronic Comorbidity Among HIV Patients (N=377) |
Discussion
The aim of this research was to determine the incidence and identify predictive factors of chronic comorbidity in HIV patients living in a low-income setting. The results of the study show that, within a follow-up period of two years, 14% of the HIV cohort developed chronic comorbidity, where hypertension (12%) was more prevalent than diabetes (4%). The findings also show that, with a prevalence of 30%, being overweight was prevalent in the study population. Overweight was more common in females (77%), and participants with a high income (64%). Chronic comorbidity seemed especially prevalent among overweight patients, participants with a longer ART duration, those with a high income, and those who had low physical activity. After adjusting for possible confounding effects, the predictors of overweight (BMI ≥ 25 kg/m2), age (≥ 54 years), and absence of regular physical activity were found to be significantly associated with the development of chronic comorbidity. This result indicates that being overweight, having an older age, or the absence of regular physical activity increases the risk of chronic comorbidity in HIV-patients.
In the current study, 14% of the HIV cohort developed chronic comorbidity within two years. There are very few studies assessing the incidence of chronic comorbidity in HIV patients in a low-income setting. One comparable study was found in which a retrospective longitudinal study was conducted among adult HIV patients in Kenya.30 In this study population of 3170 participants, 39% developed chronic comorbidity in a five-year follow-up period. Given the longer follow-up period, the incidence observed in our study appears to be comparable. In contrast to longitudinal studies, many cross-sectional studies have been conducted on the prevalence of chronic comorbidity in HIV patients in low-income settings. One study in Bahir Dar City, Ethiopia, showed a prevalence of chronic comorbidity (hypertension and/or diabetes) of 20% in a study population of 560 adult HIV patients.12 Other studies among HIV patients in low-income settings found a similar prevalence of 22% and 27% in South Africa and Malawi, respectively.21,31 The development of chronic comorbidity in HIV patients complicates the treatment of HIV patients and therefore poses a threat to the health gains achieved with HIV treatment. With a high prevalence of HIV patients in low-resource settings, many individuals residing in those areas are vulnerable to developing chronic comorbidity. It could therefore be recommended to carefully monitor the development of comorbidity in HIV patients.
During the follow-up period, 4% of the HIV cohort developed diabetes mellitus. In the study by Achwoka et al, diabetes mellitus was detected in 2% of the HIV-cohort after a five-year follow-up period (2019). Other longitudinal studies in low-income settings, including one in Southern Africa (3%) and Zimbabwe (12%), found a comparable incidence of diabetes mellitus in HIV patients after one and nine years of follow-up.32,33 It is known that diabetes mellitus is a common comorbidity in PLHIV.10,13,14,34 Particularly in areas of the world where the prevalence of HIV is high, many cases of comorbidity with diabetes mellitus are reported.13 As a result, all ART patients should have their blood glucose levels checked on a regular basis, and this should be considered standard procedure in all ART clinics.
After a two-year follow-up period, 12% of the present HIV cohort developed hypertension. Other longitudinal studies performed in a similar setting found comparable incidences, including a prospective cohort study performed in South Africa where 13% of the HIV cohort developed hypertension after one year.35 The incidence of hypertension among 834 HIV patients residing in rural Tanzania was 10% after a follow-up period of six months.36 Additionally, a retrospective cohort study among HIV patients conducted in Zimbabwe showed an incidence of 27% after five years.33 Considering these differences in follow-up duration, the observed incidence in our study seems comparable. Hypertension as a predominant risk factor for cardiovascular disease (CVD) is a growing problem as it is one of the leading causes of morbidity and mortality in PLHIV.11 Evidence suggests that PLHIV, particularly individuals using ART, have an increased risk of developing CVD.12,37 A recent meta-analysis reported that HIV patients receiving ART show higher rates of hypertension as compared to HIV-negative individuals, respectively 35% and 30%.38 A possible explanation for the increased risk of CVD in PLHIV could be due to additional HIV-related risk factors such as immune reconstitution inflammatory syndrome induced by ART, which increases inflammation.10,12 Cumulative exposure to ART is supported in the literature to have a significant relationship with the occurrence of chronic diseases.11,23,39 This is a cause of concern given that PLHIV are exposed to ART for the remainder of their lives, and it highlights the need for the integration of hypertension screening into HIV care.
Chronic comorbidity was more prevalent among older participants in the current study. This result shows consistency with other studies reporting an increased risk of chronic comorbidity as age increases.40–43 The global availability of ART has significantly reduced the number of deaths from AIDS-related causes, transforming HIV into a chronic disease which remains present for the rest of the patient’s life.10 This implies that the majority of HIV patients, given that they have access to ART, are very likely to reach an age well above 50 years. This aging, however, comes with a number of problems for the health of HIV patients, since age is associated with several comorbidities, independently of HIV.43 In addition, for the remainder of their lives, PLHIV are bound to ART, which is another risk factor for chronic comorbidity.14,23 And third, the HIV virus itself is yet another independent risk factor for the development of chronic comorbidity.43
The present study showed that being overweight is a predictor of developing chronic comorbidity, which is in line with studies in HIV patients performed in Botswana, Nigeria, and Zambia.27,44,45 Moreover, an analysis of the Veterans Aging Cohort Study showed that the risk of diabetes mellitus due to weight gain is greater for PLHIV than for uninfected controls.46 The study showed that for every 5 pounds gained, the risk of diabetes increased by 14% in PLHIV, compared with 8% in uninfected controls. A possible explanation for this finding was offered by the study by Bailin et al, who suggested that ART may not fully normalize systemic inflammation and that weight gain coupled with ART may worsen this inflammation.10 It is therefore a matter of concern that an increasing trend of overweight people is being observed in PLHIV.10,47 Remarkably, this trend is also slowly starting to emerge in resource-limited, developing countries.18,47 These countries are experiencing urbanization, and this transition from rural to urban is often accompanied by a shift to energy-dense food consumption, leading to increasing levels of overweight.48,49 This transition, however, takes place slowly, and a large proportion remains undernourished, resulting in a double burden of undernutrition and overweight among PLHIV in these countries.4,19,49–51
A lack of regular physical activity is another factor that has been associated with chronic comorbidity. Physical activity has been found to be a significant factor in reducing a number of chronic comorbidities, including hypertension, type 2 diabetes, hypercholesterolemia, asthma, and other comorbidities, according to research undertaken in various parts of the world.52–55 According to another meta-analysis study, exercise-based intervention is just as effective as pharmacological intervention in preventing chronic comorbidities.56 In addition, the previous study conducted in the current study area indicates that there is a low level of physical activity among PLWH.22 Therefore, the health care providers working in the ART clinic should consider creating awareness about the importance of regular physical exercise among HIV patients.
The strength of our study lies in the fact that we conducted a follow-up study over a period of two years. Until now, there has not been a long-term study carried out on the same study subjects (among adult PLHIV) in the current study area. The results of this longitudinal study provide policymakers with a clearer picture of the incidence of chronic comorbidities (hypertension and diabetes) in PLHIV.
Limitations
The focus of this research was to investigate the occurrence of two common chronic comorbidities in PLHIV: diabetes mellitus and hypertension. To better understand the incidence of chronic co-morbidity in this particular population, chronic comorbidities such as liver disease, cancer, and respiratory disease should be included. Due to a lack of additional resources (financial and material) to diagnose the remaining chronic diseases, we were not able to address the aforementioned chronic comorbidities.
Conclusion
In conclusion, the incidence of chronic comorbidity among adult HIV patients in a resource-limited setting was high. Age, nutritional status, and regular physical exercise seem to be important predictors of chronic comorbidity. There is a need for more longitudinal studies with a longer follow-up period to further investigate and establish this causal relationship between the risk factors of HIV patients and chronic comorbidity in a resource-limited setting. To prevent and control chronic comorbidity, targeted screening for early signs of chronic comorbidity, nutritional counseling, and awareness-creation about regular physical exercise should be integrated into HIV care.
Abbreviation
AIDS, Acquired Immune Deficiency Virus; ART, Antiretroviral Therapy; AOR, Adjusted Odds Ratio; BMI, Body Mass Index; BP, Blood Pressure; CI, Confidence Interval; CVD, Cardiovascular Disease; HDDS, Household Dietary Diversity Score; HFIAS, Household Food Insecurity Access Scale; HIV, Human Immunodeficiency Virus; HUCSH, Hawassa University Comprehensive Specialized Hospital; IDDS, Individual Dietary Diversity Score; NRTI, Nucleotide Reverse Transcriptase Inhibitors; NCD, Non-communicable diseases; OR, Odds Ratio; PI, Protein Inhibitors; PLHIV, People Living with HIV; SPSS, Statistical Package for The Social Sciences; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed as part of this study are available from the corresponding author upon reasonable request.
Ethical Consideration
To comply with the Declaration of Helsinki (1964) and the Population Screening Act, ethical approval for the study was obtained from the institutional review board of Hawassa University College of Medicine and Health Sciences (IRB/216/2019). Ethical clearance was granted on May 7, 2019. Informed verbal consent was obtained from each study participant prior to data collection. The data were collected and analyzed anonymously.
Acknowledgments
We would like to thank Hawassa University, College of Medicine and Health Sciences for providing fund for the study. We would also like to thank Maastricht University for the collaboration of the authors. Finally, we thank the data collectors and the study participants.
Author Contributions
All authors have made a substantial contribution to the work reported, be it in conception, design, conduct, acquisition of data, analysis and interpretation, or all of these; they have participated in drafting, revising, or critically reviewing the article; they have given final approval of the version to be published; they have agreed to submit the article to the journal; and they have agreed to take responsibility for all aspects of the work.
Funding
Hawassa University, Ethiopia, financed the study. The funder did not have any involvement in the design, collection, analysis, publish or preparation of the manuscript of this study.
Disclosure
The authors have declared that there are no competing interests in this work.
References
1. Latest H. Estimates and Updates on HIV Policies Uptake. World Health Organization; 2020:11.
2. Cattaneo U, Licata M, Montefiori M. The Impact of HIV on Care Work and the Care Workforce. International Labour Organization; 2019.
3. Aynalem YA, Shibabaw Shiferaw W, Woldiye Z. Prevalence of anemia and its associated factors in antiretroviral-treated HIV/AIDS-positive adults from 2013 to 2018 at Debre Berhan Referral Hospital, Ethiopia. Adv Hematol. 2020;2020:2513578.
4. Daka DW, Ergiba MS. Prevalence of malnutrition and associated factors among adult patients on antiretroviral therapy follow-up care in Jimma Medical Center, Southwest Ethiopia. PLoS One. 2020;15(3):e0229883.
5. Narayan KM, Miotti PG, Anand NP, et al. HIV and noncommunicable disease comorbidities in the era of antiretroviral therapy: a vital agenda for research in low- and middle-income country settings. J Acquir Immune Defic Syndr. 2014;67(Suppl 1):S2–S7.
6. Thuppal SV, Jun S, Cowan A, Bailey RL. The nutritional status of HIV-infected US adults. Curr Dev Nutr. 2017;1(10):e001636.
7. Cruciani M, Martí‐Carvajal AJ, Mengoli C, Serpelloni G, Bovo C, Moyle G. Abacavir versus other nucleoside reverse transcriptase inhibitor (NRTI) backbone therapies for treatment of HIV infection. Cochrane Database Syst Rev. 2018;2018:2.
8. Friis-Møller N, Weber R, Reiss P, et al. Cardiovascular disease risk factors in HIV patients--association with antiretroviral therapy. Results from the DAD study. Aids. 2003;17(8):1179–1193.
9. Castro Ade C, Silveira EA, Falco Mde O, Nery MW, Turchi MD. Overweight and abdominal obesity in adults living with HIV/AIDS. Rev Assoc Med Bras. 2016;62(4):353–360.
10. Bailin SS, Gabriel CL, Wanjalla CN, Koethe JR. Obesity and Weight Gain in Persons with HIV. Curr HIV/AIDS Rep. 2020;17(2):138–150. doi:10.1007/s11904-020-00483-5
11. Melaku T, Chelkeba L, Mekonnen Z. Clinical care & blood pressure control among hypertensive people living with human immune deficiency virus: prospective cohort study. Ann Med Surg. 2020;54:114–124. doi:10.1016/j.amsu.2020.04.017
12. Getahun Z, Azage M, Abuhay T, Abebe F. Comorbidity of HIV, hypertension, and diabetes and associated factors among people receiving antiretroviral therapy in Bahir Dar city, Ethiopia. J Comorb. 2020;10:2235042x19899319. doi:10.1177/2235042X19899319
13. Abebe SM, Getachew A, Fasika S, Bayisa M, Girma Demisse A, Mesfin N. Diabetes mellitus among HIV-infected individuals in follow-up care at University of Gondar Hospital, Northwest Ethiopia. BMJ Open. 2016;6(8):e011175. doi:10.1136/bmjopen-2016-011175
14. Duguma F, Gebisa W, Mamo A, Tamiru D, Woyesa S. Diabetes mellitus and associated factors among adult HIV patients on highly active anti-retroviral treatment. HIV AIDS. 2020;12:657–665.
15. Boore C, Mutiso VM, Obonyo V. Use of ehealth and big data in management of non communicable diseases in developing Countries; the Kenyan healthcare sector; 2021.
16. Ananworanich J, Avihingsanon A. HIV and noncommunicable diseases: the Asian perspective. JAIDS. 2014;67:S99–S103. doi:10.1097/QAI.0000000000000262
17. Bigna JJR, Sime PSD, Koulla-Shiro S. HIV related pulmonary arterial hypertension: epidemiology in Africa, physiopathology, and role of antiretroviral treatment. AIDS Res Ther. 2015;12(1):1–8. doi:10.1186/s12981-015-0078-3
18. Yitbarek GY, Engidaw MT, Ayele BA, Tiruneh SA, Alamir MT. Magnitude of obesity/overweight and its associated factors among HIV/AIDS patients on antiretroviral therapy in Jimma Zone Hospitals, South West Ethiopia: hospital-Based Cross-Sectional Study. Diabetes Metab Syndr Obes. 2020;13:1251–1258.
19. Mahlangu K, Modjadji P, Madiba S. The nutritional status of adult antiretroviral therapy recipients with a recent HIV diagnosis; a cross-sectional study in primary health facilities in Gauteng, South Africa. Healthcare. 2020;8:3.
20. Feleke D, Yemanebrhane N, Gebretsadik D. Nutritional status and CD4 cell counts in HIV. AIDS patients under highly active antiretroviral therapy in Addis Ababa, Ethiopia; 2017:8.
21. Oni T, Youngblood E, Boulle A, McGrath N, Wilkinson RJ, Levitt NS. Patterns of HIV, TB, and non-communicable disease multi-morbidity in peri-urban South Africa-a cross sectional study. BMC Infect Dis. 2015;15(1):1–8.
22. Tegene Y, Mengesha S, van der Starre C, Lako S, Toma A, Spigt M. Physical activity level and associated factors among adult HIV patients in Ethiopia. BMC Infect Dis. 2022;22(1):1–8.
23. Fiseha T, Belete AG, Dereje H, Dires A. Hypertension in HIV-infected patients receiving antiretroviral therapy in Northeast Ethiopia. Int J Hypertens. 2019;2019:4103604.
24. Coates J, Swindale A, Bilinsky P. Household Food Insecurity Access Scale (HFIAS) for measurement of food access: indicator guide. Version. 2007;3:5.
25. Swindale A, Bilinsky P. Development of a universally applicable household food insecurity measurement tool: process, current status, and outstanding issues. J Nutr. 2006;136(5):1449S–52S.
26. Woldemariam A, Yusuf M, Beyen T, Yenit M. Factors associated with dietary diversity among HIV positive adults (≥ 18 years) attending ART clinic at Mettema Hospital, Northwest Ethiopia: cross-sectional study. J AIDS Clin Res. 2015;6(8):490.
27. Sabir AA, Balarabe S, Sani AA, et al. Prevalence of diabetes mellitus and its risk factors among the suburban population of Northwest Nigeria. Sahel Med J. 2017;20(4):168.
28. Association AD. 2. Classification and diagnosis of diabetes: standards of Medical Care in Diabetes—2020. Diabetes Care. 2020;43(Supplement_1):S14–S31.
29. World Health Organization. Guideline for the Pharmacological Treatment of Hypertension in Adults: Web Annex A: Summary of Evidence. World Health Organization; 2021.
30. Achwoka D, Waruru A, Chen TH, et al. Noncommunicable disease burden among HIV patients in care: a national retrospective longitudinal analysis of HIV-treatment outcomes in Kenya, 2003–2013. BMC Public Health. 2019;19(1):372.
31. Divala OH, Amberbir A, Ismail Z, et al. The burden of hypertension, diabetes mellitus, and cardiovascular risk factors among adult Malawians in HIV care: consequences for integrated services. BMC Public Health. 2016;16(1):1243.
32. Karamchand S, Leisegang R, Schomaker M, et al. Risk factors for incident diabetes in a cohort taking first-line nonnucleoside reverse transcriptase inhibitor-based antiretroviral therapy. Medicine. 2016;95:9.
33. Cheza A, Tlou B, Zhou DT. Incidence of non-communicable diseases (NCDs) in HIV patients on ART in a developing country: case of Zimbabwe’s Chitungwiza Central Hospital-A retrospective cohort study (2010–2019). PLoS One. 2021;16(5):e0252180.
34. Kalra S, Agrawal N. Diabetes and HIV: current understanding and future perspectives. Curr Diab Rep. 2013;13(3):419–427.
35. Brennan AT, Jamieson L, Crowther NJ, et al. Prevalence, incidence, predictors, treatment, and control of hypertension among HIV-positive adults on antiretroviral treatment in public sector treatment programs in South Africa. PLoS One. 2018;13(10):e0204020.
36. Rodríguez-Arbolí E, Mwamelo K, Kalinjuma AV, et al. Incidence and risk factors for hypertension among HIV patients in rural Tanzania - A prospective cohort study. PLoS One. 2017;12(3):e0172089.
37. Zanni MV, Schouten J, Grinspoon SK, Reiss P. Risk of coronary heart disease in patients with HIV infection. Nat Rev Cardiol. 2014;11(12):728–741.
38. Xu Y, Chen X, Wang K. Global prevalence of hypertension among people living with HIV: a systematic review and meta-analysis. J Am Soc Hypertens. 2017;11(8):530–540.
39. Bavinger C, Bendavid E, Niehaus K, et al. Risk of cardiovascular disease from antiretroviral therapy for HIV: a systematic review. PLoS One. 2013;8(3):e59551.
40. Cardoso SW, Torres TS, Santini-Oliveira M, Marins LM, Veloso VG, Grinsztejn B. Aging with HIV: a practical review. Braz J Infect Dis. 2013;17(4):464–479.
41. Rasmussen LD, Mathiesen ER, Kronborg G, Pedersen C, Gerstoft J, Obel N. Risk of diabetes mellitus in persons with and without HIV: a Danish nationwide population-based cohort study. PLoS One. 2012;7(9):e44575.
42. Nsakashalo-Senkwe M, Siziya S, Goma FM, Songolo P, Mukonka V, Babaniyi O. Combined prevalence of impaired glucose level or diabetes and its correlates in Lusaka urban district, Zambia: a population based survey. Int Arch Med. 2011;4(1):2.
43. Negin J, Bärnighausen T, Lundgren JD, Mills EJ. Aging with HIV in Africa: the challenges of living longer. Aids. 2012;26(Suppl 1):S1–S5.
44. Dusara P, Bussmann H, Lima C, et al. Predictors of hypertension among HIV infected adults in Botswana, Africa. FASEB J. 2009;23:551.
45. Shankalala P, Jacobs C, Bosomprah S, Vinikoor M, Katayamoyo P, Michelo C. Risk factors for impaired fasting glucose or diabetes among HIV infected patients on ART in the Copperbelt Province of Zambia. J Diabetes Metab Disord. 2017;16:29.
46. Herrin M, Tate JP, Akgün KM, et al. Weight gain and incident diabetes among HIV-infected veterans initiating antiretroviral therapy compared with uninfected individuals. J Acquir Immune Defic Syndr. 2016;73(2):228–236.
47. Koethe JR, Heimburger DC, PrayGod G, Filteau S. From wasting to obesity: the contribution of nutritional status to immune activation in HIV infection. J Infect Dis. 2016;214(Suppl 2):S75–S82.
48. Bipath P, Levay PF, Viljoen M. Tryptophan depletion in context of the inflammatory and general nutritional status of a low-income South African HIV-infected population. J Health Popul Nutr. 2016;35:5.
49. Mashinya F, Alberts M, Cook I, Ntuli S. Determinants of body mass index by gender in the Dikgale Health and Demographic Surveillance System site, South Africa. Glob Health Action. 2018;11(sup2):1537613.
50. Takarinda KC, Mutasa-Apollo T, Madzima B, et al. Malnutrition status and associated factors among HIV-positive patients enrolled in ART clinics in Zimbabwe. BMC Nutrition. 2017;3(1):1–11.
51. Kabalimu TK, Sungwa E, Lwabukuna WC. Malnutrition and associated factors among adults starting on antiretroviral therapy at PASADA Hospital in Temeke District, Tanzania. Tanzan J Health Res. 2018;20:2.
52. Alreshidi FS, Alswayda SHS, Alassaf OM, et al. Association between physical activity and some comorbidity in a series of Saudi volunteers. Int J Med Res Public Health. 2020;9(4):30–35.
53. Francesconi C, Lackinger C, Weitgasser R, Haber P, Niebauer J. Physical activity and exercise training in the prevention and therapy of type 2 diabetes mellitus. Wien Klin Wochenschr. 2016;128:S141–S145.
54. Purba EN, Santosa H, Siregar FA. The relationship of physical activity and obesity with the incidence of hypertension in adults aged 26–45 years in Medan. Open Access Maced J Med Sci. 2019;7(20):3464.
55. Rêgo ML, Cabral DA, Costa EC, Fontes EB. Physical exercise for individuals with hypertension: it is time to emphasize its benefits on the brain and cognition. Clin Med Insights Cardiol. 2019;13:1179546819839411.
56. Rijal A, Nielsen EE, Hemmingsen B, et al. Adding exercise to usual care in patients with hypertension, type 2 diabetes mellitus and/or cardiovascular disease: a protocol for a systematic review with meta-analysis and trial sequential analysis. Syst Rev. 2019;8(1):1–17.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.