")
Back to Journals » Patient Preference and Adherence » Volume 16
Development of an Electronic Tool to Assess Patient Preferences in Geriatric Polypharmacy (PolyPref)
Authors Eidam A , Roth A, Frick E, Metzner M, Lampert A, Seidling HM, Haefeli WE , Bauer JM
Received 2 March 2022
Accepted for publication 10 June 2022
Published 23 July 2022 Volume 2022:16 Pages 1733—1747
DOI https://doi.org/10.2147/PPA.S364681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Annette Eidam,1 Anja Roth,1 Eduard Frick,2 Michael Metzner,2 Anette Lampert,2,3 Hanna M Seidling,2,3 Walter E Haefeli,2,3 Jürgen M Bauer1,4
1Center for Geriatric Medicine, Heidelberg University, AGAPLESION Bethanien Hospital Heidelberg, Heidelberg, Germany; 2Department of Clinical Pharmacology and Pharmacoepidemiology, Heidelberg University, Heidelberg, Germany; 3Cooperation Unit Clinical Pharmacy, Heidelberg University, Heidelberg, Germany; 4Network Aging Research (NAR), Heidelberg University, Heidelberg, Germany
Correspondence: Annette Eidam, Center for Geriatric Medicine, Heidelberg University, AGAPLESION Bethanien Hospital Heidelberg, Heidelberg, Germany, Tel +49 6221-319-1795, Fax +49 6221-319-1505, Email [email protected]
Purpose: Medical decision-making in older adults with multiple chronic conditions and polypharmacy should include the individual patient’s treatment preferences. We developed and pilot-tested an electronic instrument (PolyPref) to elicit patient preferences in geriatric polypharmacy.
Patients and Methods: PolyPref follows a two-stage direct approach to preference assessment. Stage 1 generates an individual preselection of relevant health outcomes and medication regimen characteristics, followed by stage 2, in which their importance is assessed using the Q-sort methodology. The feasibility of the instrument was tested in adults aged ≥ 70 years with ≥ 2 chronic conditions and regular intake of ≥ 5 medicines. After the assessment with PolyPref, the patients rated the tool with regard to its comprehensibility and usability and assessed the accuracy of the personal result. Evaluators rated the patients’ understanding of the task.
Results: Eighteen short-term health outcomes, 3 long-term health outcomes, and 8 medication regimen characteristics were included in the instrument. The final population for the pilot study comprised 15 inpatients at a clinic for geriatric rehabilitation with a mean age of 80.6 (± 6.0) years, a median score of 28 (range 25– 30) points on the Mini-Mental State Examination, and a mean of 11.6 (± 3.6) regularly taken medicines. Feedback by the patients and the evaluators revealed ratings in favor of understanding and comprehensibility of 86.7% to 100%. The majority of the patients stated that their final result summarized the most important aspects of their pharmacotherapy (93.3%) and that its ranking order reflected their personal opinion (100%). Preference assessment took an average of 35 (± 8.5) min, with the instrument being handled by the evaluator in 14 of the 15 participants.
Conclusion: Preference assessment with PolyPref was feasible in older adults with multiple chronic conditions and polypharmacy, offering a new strategy for the standardized evaluation of patient priorities in geriatric pharmacotherapy.
Keywords: geriatric pharmacotherapy, medication priorities, multimorbidity, multiple chronic conditions, patient-centered, preference assessment
Introduction
In preference-sensitive medical situations, there is more than one valid therapeutic approach and choice should be based on the values of the individual patient.1 The pharmacotherapy of frail older adults with multiple chronic conditions is characterized by preference-sensitive treatment decisions.2 The American Geriatrics Society has defined the elicitation and incorporation of patient preferences into medical decision-making as a guiding principle for the care of older adults with multimorbidity.3 Including the individual health priorities of older patients can reduce treatment burden, support deprescribing, and might address underuse.4
To date, instruments that measure medication preferences in older patients have primarily targeted disease-specific contexts such as age-related macular degeneration,5 osteoporosis,6 or anticoagulation treatment in atrial fibrillation.7 Few measurement instruments have assessed medication preferences in the context of geriatric multimorbidity.8 Examples include a discrete choice experiment evaluating the trade-offs between the risk of fall injury, symptomatic side effects, and the preventive benefits of antihypertensive drug therapy,9 and a scenario-based approach to measure the patients’ willingness to take medication for the prevention of cardiovascular disease.10 The so-called Outcome Prioritization Tool, which allows for prioritizing between four universal health outcomes, has been used in several different studies and employed as a starting point to propose medication changes in primary care patients.11 Moreover, two separate research groups have developed strategies to deliver pharmacist-led medication reviews that focus on the individual goals of older adults with multiple chronic conditions.12–14 The Drug use Reconsidered in the Elderly using goal Attainment scales during Medication Review (DREAMeR) study evaluated an intervention focused on a patient-centered comprehensive medication review. The medication review, amongst others, explored common health complaints and their relation to the patient’s medicines, practical issues of medication use, as well as possible adverse drug reactions, and helped the patient define health-related goals using goal attainment scales.12,15 In the intervention group health-related quality of life as measured with the EuroQol-Visual Analogue Scale improved and the number of health complaints impacting daily life decreased 3 and 6 months after the baseline assessment.15
Elaborate medication reviews are time-consuming and might not be feasible in every setting. Computerized assessment instruments based on a thorough evaluation of the actual characteristics as well as benefit and risks of the numerous medicines commonly used in geriatric polypharmacy could be valuable in introducing preference-focused prescribing into routine patient care. Both preventive medicines and drugs for the relief of physical symptoms contribute to polypharmacy,16 and point to a variety of short-term and long-term health outcomes that may be modified by tailoring pharmacotherapy. Symptom burden is high in geriatric multimorbidity and a mean number of 8.5 symptoms has been reported for older patients with multiple chronic conditions.17 Because polypharmacy is associated with an increased risk for adverse drug reactions,18 symptoms might not only be pharmacologically alleviated, but also triggered or aggravated by a given drug. In addition to therapeutic outcome goals, the evaluation of preferences in polypharmacy should also include the patient’s attitude toward the practical implementation of the medication regimen.19
Therefore, the aim of our research project was to develop an instrument for the collection of patient preferences in geriatric pharmacotherapy that reflects the complexity of the context by considering the most relevant drug-related health outcomes as well as medication regimen characteristics. To enable an individual preference assessment in this multi-variable setting, we developed a software-based instrument and investigated its feasibility in the target population.
Materials and Methods
Development of PolyPref
Structure of the Instrument
PolyPref is an electronic instrument that can be presented to the patient on a stationary or portable computer. The layout of the software allows patients to complete preference assessment independently or with the assistance of a healthcare worker. Questioning during preference assessment adapts to the answers of the individual patient. The design of PolyPref was based on a direct, two-stage self-explicated approach of preference elicitation. Figure 1 depicts the basic structure of the instrument. In stage 1, the respondent is guided through a comprehensive list of health outcomes and medication regimen characteristics and asked to make an individual pre-selection of the most relevant aspects. Stage 2 finalizes the preference assessment with the importance rating of the previously selected attributes.
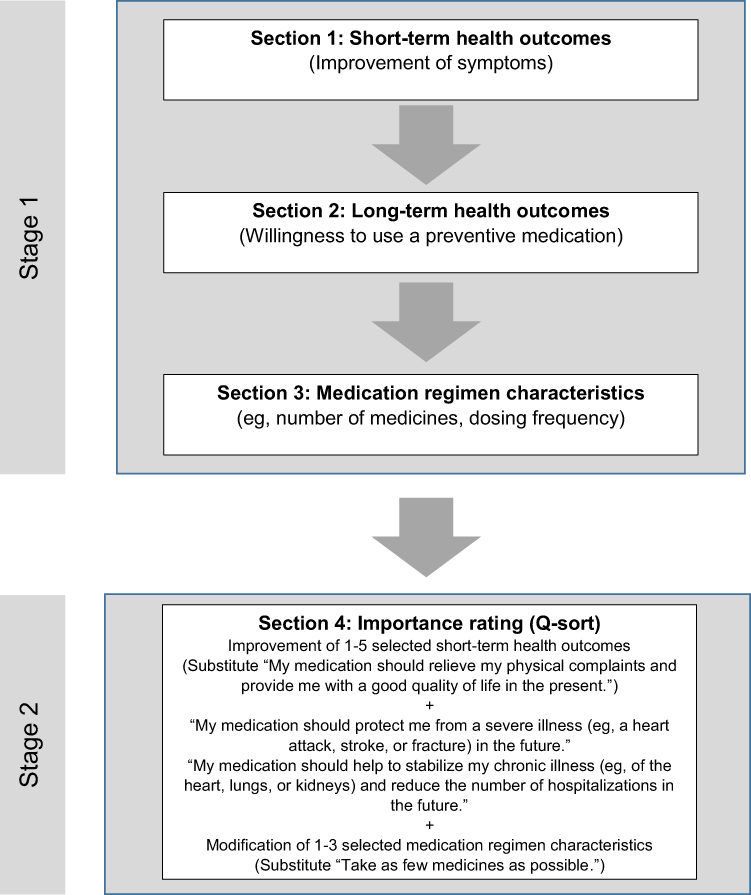 |
Figure 1 Basic structure of PolyPref, an electronic tool to elicit patient preferences regarding their drug treatment in geriatric patients with polypharmacy. Notes: In stage 1, the respondent is presented with a comprehensive list of health outcomes and medication regimen characteristics and asked to make an individual preselection of the most relevant aspects. Stage 2 produces the final result of the preference assessment using the Q-sort methodology. The respondent is requested to give importance ratings for the previously selected short-term health outcomes and medication regimen characteristics and two long-term health outcomes. |
Stage 1 – Section 1: Selection of Short-Term Health Outcomes
Stage 1 was divided into three consecutive sections. In section 1 “Short-term health outcomes” we aimed to confront the respondent with an extensive range of medical symptoms that may affect the immediate quality of life and functionality of older patients and may be relieved by the addition or withdrawal of certain medicines. To ensure that the medical symptoms included in the tool were drug-related, we analyzed a set of approximately 50 medicines commonly used in geriatric medicine with regard to associated favorable short-term health effects, ie, symptoms that the medicine is intended to control, and unfavorable health effects, ie, symptoms possibly caused by the medicine. These medicines were taken from the A (indispensable) and B (beneficial) rating categories of the Fit fOR The Aged (FORTA) classification.20 We complemented the list with additional medicines frequently used at our geriatric center. Adverse drug reactions were then identified for these medicines with the help of the respective United States Food and Drug Administration (FDA) drug labels. We considered adverse reactions that occurred with an incidence of ≥ 1% and more frequently than in the placebo group. For medicines not approved by the FDA as well as for indications and usage we referred to the German summary of product characteristics. We focused on adverse drug reactions directly affecting a patient’s health-related quality of life while omitting adverse but asymptomatic changes in laboratory values.
All symptoms were listed and provisionally categorized into symptom groups based on common health complaints in older adults.21,22 We also added the category “gait instability and fear of falling” to reflect the property of certain medicines to increase fall risk in older adults.23 The list was reviewed and validated by an expert group (3 geriatricians, 2 clinical pharmacists, and 1 clinical pharmacologist). These experts were asked to verify that all symptom groups are prevalent in geriatric medicine and relevant for the health-related quality of life of older patients, that they are pharmacologically modifiable, and that no relevant symptoms were omitted.
PolyPref respondents are asked to rate how strongly they are affected by the respective symptoms on a 5-point Likert scale (Figure 2). In case respondents select more than five symptom groups as at least partly relevant (midpoint on Likert scale), they are asked to choose the five most relevant groups in an additional intermediate step.
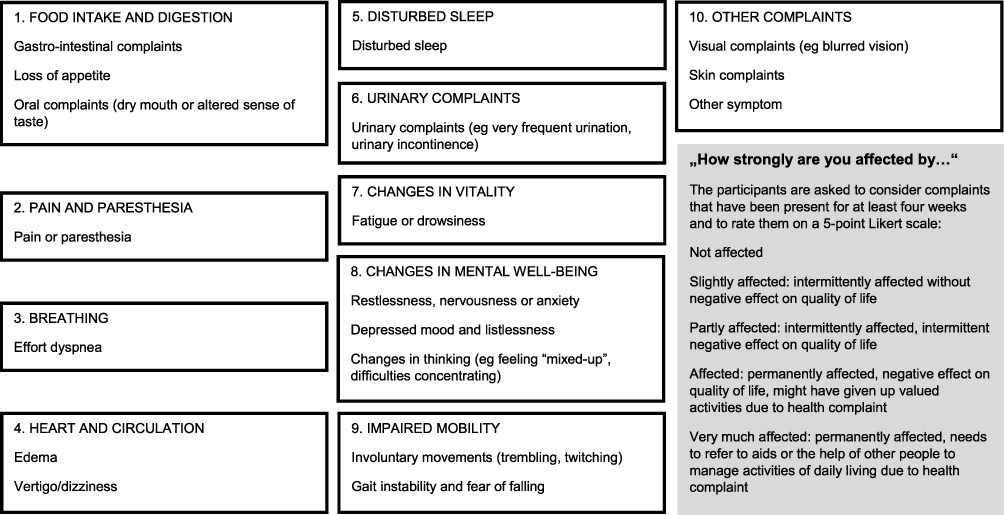 |
Figure 2 Symptom groups included in section 1 (stage 1) of PolyPref. |
Stage 1 – Section 2: Long-Term Health Outcomes
Section 2 was designed to familiarize the patient with the topic of preventive medication. Based on previously published research assessing the willingness of older patients to take medication for the prevention of cardiovascular disease and hip fractures,10,24,25 we created three medication scenarios. In each scenario the respondents are asked if they are willing to take a hypothetical medicine (for the prevention of cardiovascular events, osteoporotic fractures, and for the stabilization of chronic, eg, cardiovascular disease) and if they are willing to accept mild adverse drug reactions (ie, adverse drug reactions not affecting daily life) for the benefit of prevention.
Stage 1 – Section 3: Medication Regimen Characteristics
For section 3 we made use of a comprehensive list of complexity characteristics of treatment regimens from a previous study26,27 and selected those characteristics that could be favorably influenced by medication changes (eg, number of medicines, dosing frequency, splitting of tablets). Respondents are requested to rate how strongly they are bothered by each of the characteristics on a 5-point Likert scale. In case respondents select more than three medication regimen characteristics as at least partly applicable (midpoint on Likert scale), they are asked to choose the three most important characteristics in an additional intermediate step.
Stage 2: Importance Rating with Q-Sort Methodology
The so-called “Q-sort methodology” forces the respondent to trade-off between different attributes by sorting them into importance categories, the latter mimicking a normal distribution. For instance, with a total of ten attributes the respondent is first asked to select the most important attribute, followed by the two second most important attributes. In the next step, the respondent is asked to select the least important attribute and finally the two second least important attributes, resulting in five importance categories with 1:2:4:2:1 attributes.28 Based on the individual choices made in stage 1 and the number of relevant attributes selected, respondents give importance ratings for 4 to 10 pharmacologically achievable health outcomes and modifications of medication regimen characteristics in stage 2 of PolyPref. In case respondents do not select any relevant short-term health outcomes or medication regimen characteristics in sections 1 and 3 of stage 1 of the tool, they are presented with a substitute attribute for each section (Figure 1). To ensure the representation of the three different categories of attributes during the final importance ratings, we decided to confront every respondent – irrespective of the answers given in stage 1 – with the same two long-term health outcomes in the Q-sort exercise (Figure 1). The result of the Q-sort exercise yields the final result of the preference assessment with PolyPref.
Programming
The tool was developed as a Windows Forms application, written in the C# programming language (.NET Framework version 4.6.1). The output of the surveys was exported to a comma-separated values (CSV) file.
Pretest
A preliminary prototype for the PolyPref tool was pretested anonymously in a convenience sample of 9 older patients maintained on ≥ 5 regular medicines (Center for Geriatric Medicine, Clinic of geriatric rehabilitation, Agaplesion Bethanien Hospital, Heidelberg, Germany). Additionally, the prototype was presented during a meeting of the interdisciplinary Medication and Quality of Life (MedQoL) research group to obtain expert feedback.29 Slight modifications and minor rephrasing of the wording were carried out based on the feedback from both the pretest and the presentation.
Final Version of PolyPref
Stage 1 of the final version of PolyPref comprised 29 questions: 18 questions targeting medical symptoms were included in section 1 (Figure 2), three hypothetical medications in section 2, and 8 medication regimen characteristics in section 3. Screenshots of the different sections and the final result of the task can be found in the Electronic Supplementary Material Figures S1–S5 .
Pilot Study
The study was approved by the responsible Ethics Committee of the Medical Faculty of Heidelberg University (S-766/2018) and registered with the German Clinical Trials Register (DRKS00016728) before inclusion of the first participant. All study procedures were carried out in accordance with the Declaration of Helsinki.
Study Population
Eligible patients were aged ≥ 70 years, with ≥ 2 chronic conditions, and polypharmacy defined as the regular intake of ≥ 5 medicines. They were mentally and physically fit to participate in the study as judged by a medical member of the study group or the attending physician. Exclusion criteria comprised a score of ≤ 23 points on the Mini-Mental State Examination (MMSE),30 a formal diagnosis of dementia, insufficient knowledge of the German language, and missing written informed consent.
Study Objectives and Procedures
We aimed to assess the feasibility of preference elicitation with PolyPref by examining its usability and comprehensibility as well as the effort imposed on the older respondents during the assessment. We also asked whether the participants found the individual preference evaluation with PolyPref beneficial and appropriate.
After giving written informed consent, the participant’s comorbidities, medication, and score on the MMSE were noted from the patient’s file. The completeness of the recorded medication was verified with the participants and they were asked to provide their sociodemographic data. Prior to performing the preference assessment, we collected a set of additional questionnaires. The 15-item Geriatric Depression Scale (GDS)31 was used to characterize the participants’ affective status. With the consent of the license holder (IQVIA, Durham, NC, USA), we modified the German version of the “Treatment Satisfaction Questionnaire for Medication” (TSQM),32 usually directed towards therapy with a single specific drug, to assess the participants’ satisfaction with their current medication. We developed an unofficial, paper-based German translation of the Now vs Later tool33 to evaluate the relative importance that the participants attributed to their present versus their future quality of life.
Preference assessment with PolyPref was carried out during an interview with a trained research associate (AE or AR), and monitoring by the second interviewer was mandatory during the first five assessments. The electronic tool was presented on a laptop, and the participants could opt to navigate the software themselves or to have it operated by the interviewer. In either case, participants were placed in front of the laptop monitor and asked to follow along while the interviewer read the textual content on the screen (explanatory information, instructions) to them. After completion of the preference task, both the participant and the interviewer filled in a feedback questionnaire, rating the comprehensibility, usability, benefit, and effort of the task (respondent) as well as the understanding and handling of the instrument by the participant (interviewer). To collect further information regarding the validity of preference assessment with PolyPref, the participants were asked to evaluate the congruence of their individual results with their actual preferences. Participants gave their feedback on a 5-point rating scale of 1 (= agreement) to 5 (= disagreement). Interviewers gave their feedback on a 3-point rating scale.
Analysis
We used descriptive statistics to present the characteristics of the participants as well as the results of the feedback questionnaires and the preference task. The participants’ feedback was summarized as “favors agreement” (rating categories 1 and 2) and “favors disagreement” (rating categories 4 and 5). The results of the assessment with the Now vs Later tool were categorized (1 = focus on present health, −1 = focus on future health, 0 = equally important) and compared to the responses regarding the importance of short-term and long-term health outcomes during the interview with PolyPref. Differences in mean age between participants who chose a long-term health outcome as most important and those who chose a short-term health outcome as most important were assessed using a two-tailed unpaired t-test. A two-sided p-value ≤ 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics version 27 (IBM Deutschland GmbH, Ehningen, Germany).
Results
Study Population
From April to August 2019, we recruited a convenience sample of 18 inpatients at the clinic of geriatric rehabilitation at Agaplesion Bethanien Hospital (Heidelberg, Germany), and 15 participants were ultimately included in the analyses. One participant decided to drop out of the study after partial completion of the additional questionnaires. Two participants were excluded because they were confronted with an incorrect sequence of the Q-sort exercise (initial software error).
The characteristics of the final study population are listed in Table 1. We included eight women (53.3%) and seven men (46.7%) with a mean age of 80.6 (± 6.0) years and a median score of 28 points on the MMSE. They took a mean of 11.6 (± 3.6) regular medicines and 66.7% (n = 10) had a medical history of severe cardiovascular events (stroke, myocardial infarction, decompensated heart failure) and/or osteoporotic fractures. All 15 participants indicated that they were at least somewhat satisfied with their current medication (TSQM item 14). Forty percent (n = 6) rated their present quality of life as more important than their future quality of life one year from now.
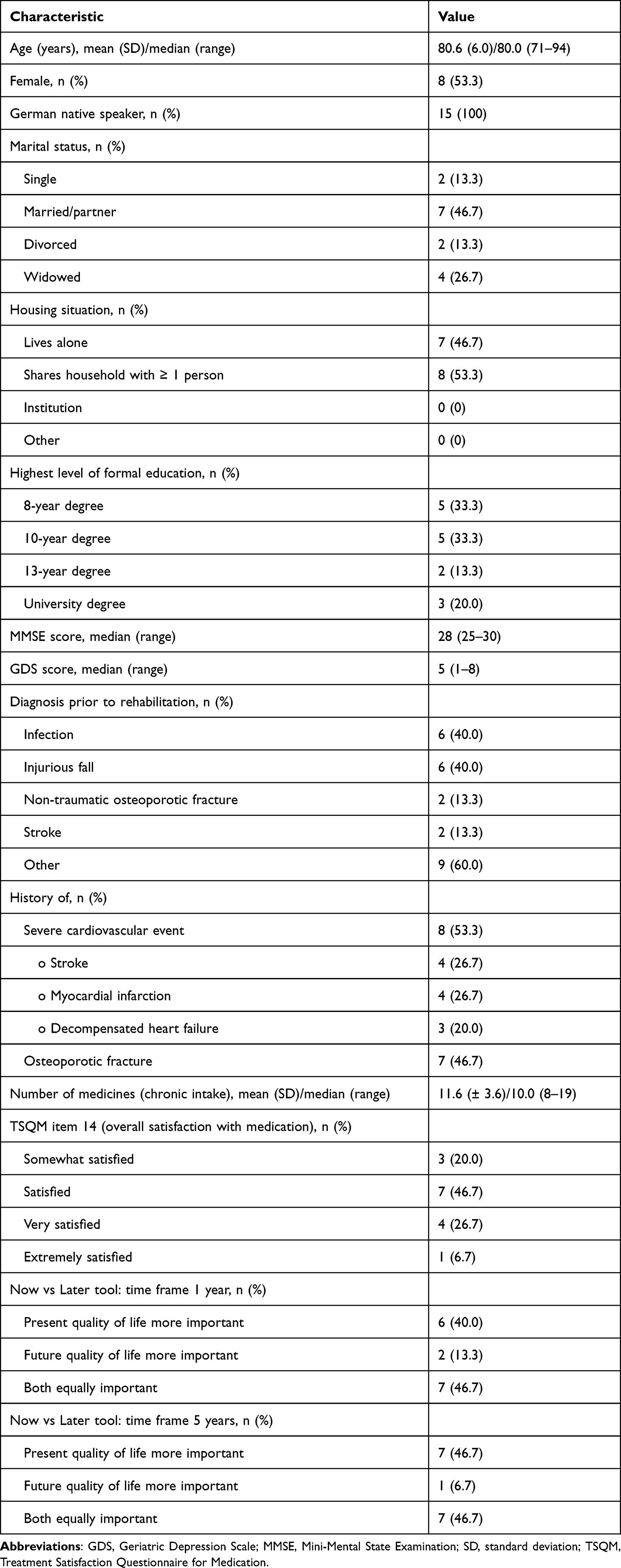 |
Table 1 Characteristics of the Study Population (n = 15) |
Preference Assessment with PolyPref
The interview with PolyPref took on average 35 (± 8.5) min to complete, with a range of 19 to 47 min. Only one participant chose to operate the software without assistance. The minimum number of attributes in stage 2 (Q-sort exercise) was 6 (n = 1), the maximum number 10 (n = 9).
Table 2 details the feedback of the interviewers and the respondents. Using seven different evaluation criteria, the interviewers found, depending on the respective criterion, 86.7% (n = 13) to 100% (n = 15) of the respondents to have unimpaired understanding. Thirteen patients (86.7%) gave consistent answers throughout the interview, and all participants but one showed a thorough understanding of the requirements of the different sections of the tool (n = 14; 93.3%). Because the software was operated by the interviewer in 93.3% of the assessments (n = 14), we did not list any ratings for the handling of the instrument.
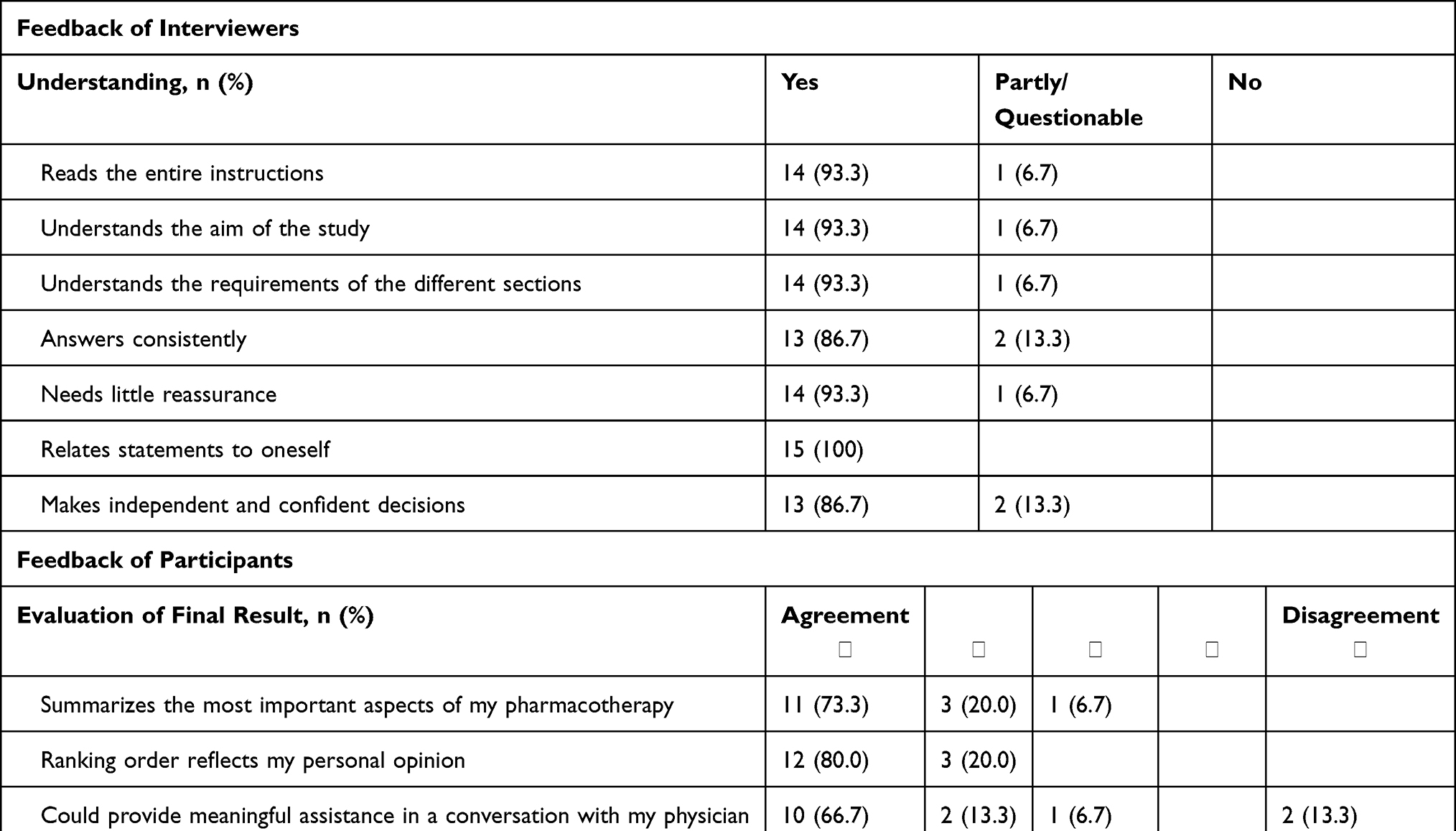 |
Table 2 Feasibility and Validity of Preference Elicitation with PolyPref – Feedback of Interviewers and Participants |
The majority of the respondents confirmed that the instrument was well understandable: all participants found that the text was phrased intelligibly and questioning logical, and 13 participants (86.7%) rated the instructions to be unambiguous (Table 2). With regard to the usability of the tool, 12 respondents (80.0%) confirmed the readability of the textual content and 13 respondents (86.7%) found the visual design to be clear. Concerning the effort required for the task, 86.7% (n = 13) did not consider the assessment with the instrument to be exhausting, and only one participant reported becoming tired during the course of the survey. Most respondents (n = 13; 86.7%) considered the topic of the study to be important. As far as the evaluation of the individual final result was concerned, 93.3% of the respondents (n = 14) stated that their final result summarized the most important aspects of their pharmacotherapy, and all participants confirmed that the ranking order in their final result properly reflected their personal opinion. Eighty percent (n = 12) agreed that their personal results could enrich the conversation with their physician.
Table 3 depicts the results of the preference assessment. Eight participants (53.3%) rated one of the two long-term health outcomes as the most important goal to achieve with their medication, seven participants (46.7%) rated a short-term health outcome as most important. Participants who rated a long-term health outcome as most important (mean age 82.9 ± 6.6 years) and participants who rated a short-term health outcome as most important (mean age 78.0 ± 4.2 years) did not differ in mean age (p = 0.118). Three respondents (20.0%) mentioned only short-term health outcomes and none of the long-term health outcomes within their first two importance categories. Only one participant rated a characteristic of the medication regimen – the number of the medicines taken – in the first two categories.
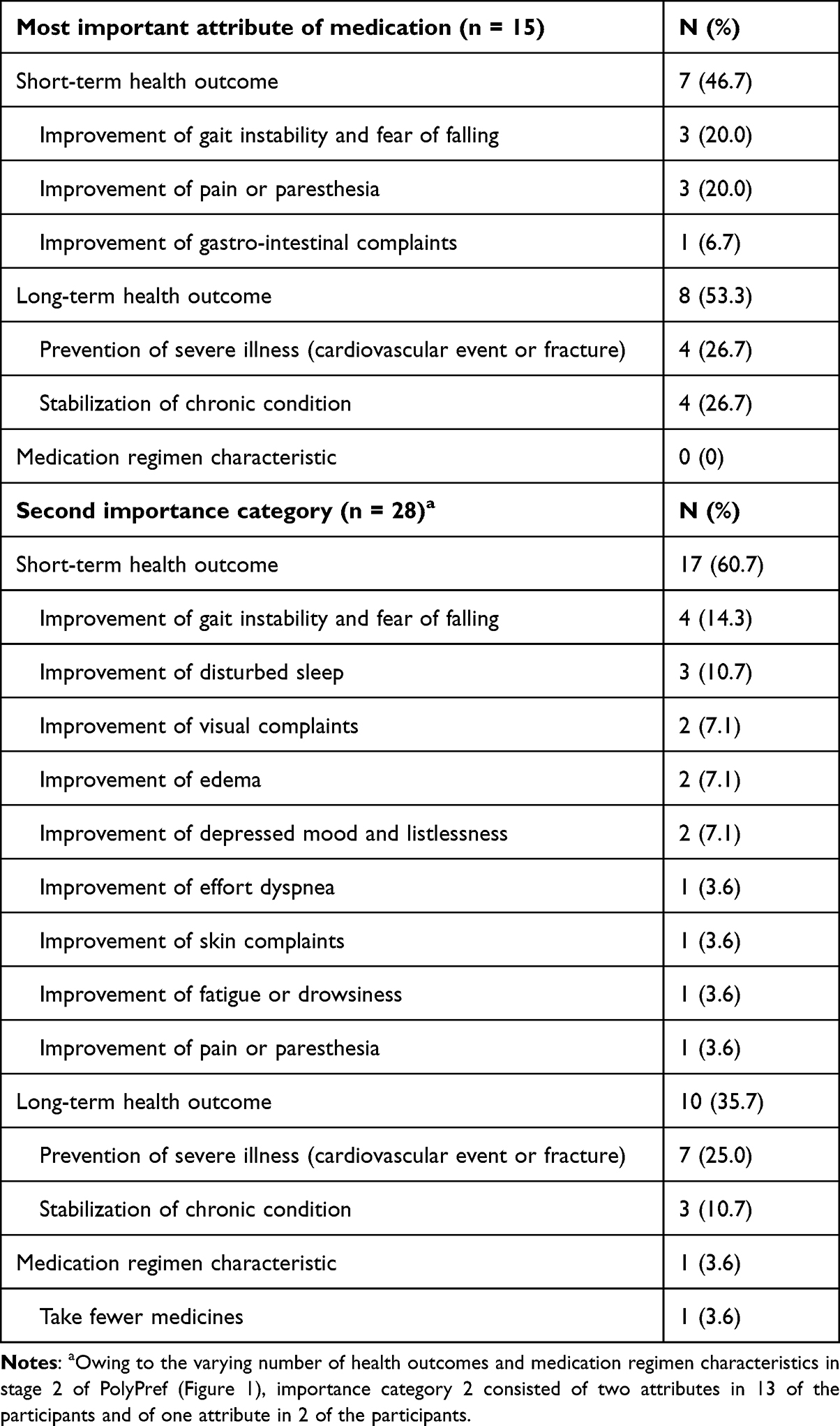 |
Table 3 Importance Ratings of Health Outcomes and Medication Regimen Characteristics in the First Two Importance Categories of the Q-Sort Exercise |
On the Now vs Later tool, all of the eight participants who chose a long-term health outcome as their primary goal valued their present quality of life as either more important than or equally important as their quality of life one year into the future. Seven of these eight participants had a prior diagnosis of severe cardiovascular event or osteoporotic fracture.
Discussion
Despite explicit recommendations by organizations such as the American Geriatrics Society to include the priorities of older patients with multiple chronic conditions in the decision-making process, there is still a lack of validated standardized assessments for the collection of medication-related patient preferences in this context. The electronic tool PolyPref pursues a novel approach for the detailed evaluation of patient preferences in geriatric polypharmacy.
In our study population, preference assessment with PolyPref could be accomplished within an adequate time frame. Understanding and comprehensibility were rated as good by interviewers and respondents, and all but one participant showed no difficulty in mastering the Q-sort exercise and switching between the choice of the most important and the least important attributes. This agrees with previous findings that reported that Q-sorting tasks can be successfully completed by older adults with unimpaired cognitive function.34,35
However, independent handling was not generally possible, and 14 of the 15 participants declined to operate the software themselves. In a 2011 sample of Medicare beneficiaries, 50.3% of adults aged 70 to 74 years reported using the internet in the past month, compared to 26.4% in the 80 to 84-year-old age group.36 Limitations in physical capacities such as the handling of small objects reduced internet usage.36 In a study examining the usability of a tablet computer questionnaire that addressed quality of life and symptom severity in cancer patients, participants aged ≥ 65 years reported lower ease of use than younger participants.37 Nevertheless, the ease of use of the application was rated as positive by the older participants.37 Yet, in an emergency department-based study in adults aged ≥ 65 years, only a minority of individuals willing to complete a tablet-based questionnaire were able to do so without assistance.38 While computer literacy and the ease of operating technology are expected to increase in the older population over the next few years, electronic preference assessment will need to account for the associated challenges and provide an appropriate time budget for recording preferences. The mean duration of assessment with PolyPref was 35 min, which likely offers time-saving advantages over preference assessment in individual patient interviews without the support of comprehensive lists of drug-related health outcomes and standardized trade-off techniques. Moreover, contrary to medication reviews during patient-centered interviews, the preference assessment with PolyPref does not have to be conducted by a physician or clinical pharmacist, but could be carried out by an assistant trained in the handling of the software. The final result of the preference assessment could then provide the background for individual conversations between patients and their primary care physicians or geriatricians and help initiate preference-based modifications to the patients’ medication.
Apart from the fact that it is easier to adapt the survey process to each patient’s responses, the computer-based approach of PolyPref could offer further advantages by facilitating the translation of recorded preferences into individualized pharmacotherapy. For example, by using the adverse drug reaction data we relied on to select relevant health outcomes for instrument development and incorporating these data into the software to provide drug-specific information, physicians could learn how likely it is that a particular symptom is caused by a side effect of one of the patient’s medicines. In addition, information on potentially inappropriate medications and potential prescribing omissions could be integrated into the tool, and patient preferences might help to enforce the implementation of these data during the prescribing process.
During the development of the instrument, we focused on the actual characteristics of geriatric pharmacotherapy (drug-related health outcomes, medication regimen characteristics), referring to detailed analyses of the literature as well as expert opinion to achieve comprehensive validity of the content. The validity of the instrument was further confirmed by the feedback of the participants of this pilot study who consistently indicated that the results corresponded well to their own weighting of preferences, and three quarters valued their personal result high enough to regard it as a beneficial addition for their consultation with their physician.
In the absence of a gold standard for measuring patient preferences in polypharmacy, we could not reach a final assessment of the construct validity of the instrument. We used the Now vs Later tool33 to compare the individual significance of present and future quality of life with the importance ratings that were collected for the short-term and long-term health outcomes on PolyPref. Interestingly, participants who rated one of the two preventive attributes of the medication as most important did not display a preference for their future quality of life over their present quality of life on the Now vs Later tool. The majority of study participants were survivors of cardiovascular events or had suffered osteoporotic fractures. Therefore, the included preventive health outcomes might have been considered as present rather than future health goals by these patients.
Only few strategies have been developed and evaluated for the assessment of medication preferences in geriatric multimorbidity.8 In addition to preference instruments focusing specifically on polypharmacy, a number of studies have touched on medication-related patient priorities as part of larger interventions aimed at providing patient-centered care for older individuals with multiple chronic conditions.39–41 Recently, an approach called Patient Priorities Care has been introduced and studied in an ambulatory setting.42 It aims to identify individual health goals and care preferences of older patients through an adapted collaborative goal-setting process43 and to enable care that is aligned with these health priorities.4
In order to evaluate preferences for health outcomes, PolyPref focusses on groups of specific, potentially medication-related symptoms and preventive goals. We refrained from recording preferences to improve conditions such as motor or sensory impairment, which rarely have pharmacological treatment options. Patient Priorities Care uses a broader approach: preferences are assessed in terms of the individual’s key values and patients are encouraged to focus on valued life activities and abilities instead of symptoms.43 Based on the patient’s values, specific health outcome goals and care preferences are then identified.43
Drug therapy may touch on or be intertwined with non-pharmacological approaches to enable successful treatment. Assessment strategies including pharmacological as well as non-pharmacological health priorities, such as Patient Priorities Care, and tools focusing on polypharmacy may complement each other by supporting patient-centeredness across the different domains of health care.
In addition, electronic tools that assess medication preferences in old-age polypharmacy might complement non-preference-based instruments for optimizing drug therapy in older adults. The SENATOR (Software ENgine for the Assessment and optimization of drug and non-drug Therapy in Older peRsons) trial examined the effect of the SENATOR software on the incidence of adverse drug reactions in older adults with multiple chronic conditions in the hospital setting. Physicians attending to these patients were provided with a computerized report detailing potentially inappropriate medications or potential prescribing omissions based on the validated STOPP/START criteria.44 However, uptake of the computerized recommendations by the attending physicians was low and the intervention failed to reduce the incidence of adverse drug reactions.45 Supplementing the SENATOR recommendations with the patient’s individual preferences might substantiate the proposed medication changes and improve the outcome of this intervention as shown in the SPPiRE study, which also used the STOPP/START criteria but supplemented them with an assessment of patient priorities and whose recommendations were well received.46
Besides the small sample size other limitations of our pilot study have to be addressed. Individuals who volunteer to participate in a study may be more open-minded and attentive during preference elicitation than other members of the target group. Owing to the interview setting, participants might have tended towards answers perceived as desired on the feedback questionnaire. In addition, we did not control for framing or order effects. Finally, we exclusively tested the feasibility of our electronic instrument on a laptop computer and did not examine whether a presentation on alternative devices, eg, tablet computers, might improve self-administration and usability.
Despite these limitations, the collected data should encourage the continuing development of PolyPref. Next steps need to further validate the psychometric properties by addressing the test-retest reliability of the tool and to examine the influence of relevant patient characteristics (eg, mild cognitive impairment, level of multimorbidity, or health literacy) on the validity of the instrument. Moreover, strategies to adapt the patients’ medication according to their preferences should now be developed and tested and preferences and their modulators should be assessed over time to define how often the assessment should be repeated to detect relevant preference changes as accurately as possible. Preferences for health outcomes may change in some patients as their health changes,47 and easy-to-use instruments such as PolyPref could offer a feasible method to reassess preferences. In addition, it seems beneficial to evaluate possible strategies for improved self-administration (eg, developing a paper-based training module that is handed to patients prior to administration, navigation of PolyPref via touchscreen) and to compare outcomes of interviewer led and self-administered assessments. A further long-term outlook also includes the evaluation of older adults’ satisfaction with and adherence to their preference-based, individualized pharmacotherapy compared to standard of care management.
Conclusion
In summary, preference elicitation with PolyPref proved feasible in older adults with multimorbidity-related polypharmacy. Based on specific drug-related health outcomes and characteristics of the medication regimen, the instrument introduces a new approach to recording patient priorities in geriatric pharmacotherapy and contributes to the discussion on standardized assessment of patient preferences in this context.
Abbreviations
CSV, comma-separated values; FDA, United States Food and Drug Administration; FORTA, Fit fOR The Aged; GDS, Geriatric Depression Scale; MedQoL, Medication and Quality of Life; MMSE, Mini-Mental State Examination; SD, standard deviation; TSQM, Treatment Satisfaction Questionnaire for Medication.
Data Sharing Statement
Raw data cannot be shared due to data protection regulations.
Ethics Approval and Informed Consent
The study was approved by the responsible Ethics Committee of the Medical Faculty of Heidelberg University, Heidelberg, Germany (reference number S-766/2018). All study participants provided written informed consent before being included in the study.
Acknowledgments
We are grateful to Christian Schlereth (Otto Beisheim School of Management, Vallendar, Germany) and Susanne Hensel-Börner (Hamburg School of Business Administration, Hamburg, Germany) for their expert information on the self-explicated approaches of preference assessment.
We would like to thank our collaborating partners within the Medication and Quality of Life (MedQoL) Research Group for their valuable feedback during the development of the PolyPref tool: Christine A. F. von Arnim, Simone Brefka, Dhayana Dallmeier, Michael D. Denkinger, Viktoria Mühlbauer, and Carlos Schönfeldt-Lecuona (University of Ulm, Ulm, Germany), Claudia Bollig, Gabriel Torbahn, and Sebastian Voigt-Radloff (University of Freiburg, Cochrane Germany, Freiburg, Germany), and Stefan Klöppel (University of Bern, Bern, Switzerland).
We are thankful to Marcel Kusch for his feedback on the methods section of this manuscript.
Author Contributions
All author’s (I) made a significant contribution to this work, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, (II) have drafted or written, or substantially revised, or critically reviewed this article, (III) have agreed to submit the article to “Patient Preference and Adherence”, (IV) reviewed the final version of this article and agreed on its publication, and (V) agree to take responsibility and to be accountable for the contents of this article.
Funding
This study was funded by the Baden-Württemberg Ministry of Science, Research and the Arts as part of the project “Medication and circumstances of life in old age” (Verbundvorhaben “Medikation und Lebenssituation im Alter”). The funding source had no role in the design of this study, the collection and interpretation of the data, and the writing of this manuscript.
Disclosure
Dr Anette Lampert reports personal fees from Sanofi, personal fees from Chamber of pharmacists Baden-Wuerttemberg, personal fees from Chamber of pharmacists Hesse, outside the submitted work. Professor Hanna Seidling reports grants from BMG, Chambers of pharmacists Baden-Württemberg, Nordrhein, Hessen and Niedersachsen; Klaus-Tschira-Stiftung, Dosing GmbH, g-BA, BMBF, AOKPlus, Dr. August and Dr. Anni Lesmüller Stiftung, non-financial support from VKliPha; AkdÄ; GSASA, APS e.V., NHS, ESCP, BAK, ÄZQ, SFPC, Dosing GmbH, Karolinska Institutet, University of Bonn, personal fees from Universitätsklinikum Heidelberg IMBI, Govi Verlag, Deutscher Apotheker Verlag, Wissenschaftliche Verlagsgesellschaft Stuttgart, Bundesgesundheitsblatt, personal fees, non-financial support from several chambers of pharmacists and professional organisations, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Wennberg JE. Unwarranted variations in healthcare delivery: implications for academic medical centres. BMJ. 2002;325(7370):961–964. doi:10.1136/bmj.325.7370.961
2. Janssens J, de Kort SJ, Achterberg WP, et al. Medical and moral considerations regarding complex medical decisions in older patients with multimorbidity: a compact deliberation framework. BMC Geriatr. 2018;18(1):25. doi:10.1186/s12877-018-0707-5
3. Boyd C, Smith CD, Masoudi FA, et al. Decision making for older adults with multiple chronic conditions: executive summary for the American Geriatrics Society guiding principles on the care of older adults with multimorbidity. J Am Geriatr Soc. 2019;67(4):665–673. doi:10.1111/jgs.15809
4. Tinetti ME, Naik AD, Dindo L, et al. Association of patient priorities-aligned decision-making with patient outcomes and ambulatory health care burden among older adults with multiple chronic conditions: a nonrandomized clinical trial. JAMA Intern Med. 2019;179(12):1688–1697. doi:10.1001/jamainternmed.2019.4235
5. Vennedey V, Danner M, Evers SM, et al. Using qualitative research to facilitate the interpretation of quantitative results from a discrete choice experiment: insights from a survey in elderly ophthalmologic patients. Patient Prefer Adherence. 2016;10:993–1002. doi:10.2147/PPA.S101584
6. Silverman S, Calderon A, Kaw K, et al. Patient weighting of osteoporosis medication attributes across racial and ethnic groups: a study of osteoporosis medication preferences using conjoint analysis. Osteoporos Int. 2013;24(7):2067–2077. doi:10.1007/s00198-012-2241-1
7. Fuller R, Dudley N, Blacktop J. Avoidance hierarchies and preferences for anticoagulation–semi-qualitative analysis of older patients’ views about stroke prevention and the use of warfarin. Age Ageing. 2004;33(6):608–611. doi:10.1093/ageing/afh202
8. Eidam A, Roth A, Lacroix A, et al. Methods to assess patient preferences in old age pharmacotherapy - a systematic review. Patient Prefer Adherence. 2020;14:467–497. doi:10.2147/PPA.S236964
9. Tinetti ME, McAvay GJ, Fried TR, et al. Development of a tool for eliciting patient priority from among competing cardiovascular disease, medication-symptoms, and fall injury outcomes. J Am Geriatr Soc. 2008;56(4):730–736. doi:10.1111/j.1532-5415.2007.01627.x
10. Fried TR, Tinetti ME, Towle V, O’Leary JR, Iannone L. Effects of benefits and harms on older persons’ willingness to take medication for primary cardiovascular prevention. Arch Intern Med. 2011;171(10):923–928. doi:10.1001/archinternmed.2011.32
11. Stegmann ME, Festen S, Brandenbarg D, et al. Using the Outcome Prioritization Tool (OPT) to assess the preferences of older patients in clinical decision-making: a review. Maturitas. 2019;128:49–52. doi:10.1016/j.maturitas.2019.07.022
12. Verdoorn S, Kwint HF, Blom J, Gussekloo J, Bouvy ML. DREAMeR: Drug use Reconsidered in the Elderly using goal Attainment scales during Medication Review; study protocol of a randomised controlled trial. BMC Geriatr. 2018;18(1):190. doi:10.1186/s12877-018-0877-1
13. Kouladjian O’Donnell L, Gnjidic D, Sawan M, et al. Impact of the Goal-directed Medication Review Electronic Decision Support System on Drug Burden Index: a cluster-randomised clinical trial in primary care. Br J Clin Pharmacol. 2021;87(3):1499–1511. doi:10.1111/bcp.14557
14. Kouladjian O’Donnell L, Reeve E, Hilmer SN. Development, validation and evaluation of the Goal-directed Medication review Electronic Decision Support System (G-MEDSS)(c). Res Social Adm Pharm. 2021;18(7):3174–3183. doi:10.1016/j.sapharm.2021.09.004
15. Verdoorn S, Kwint HF, Blom JW, Gussekloo J, Bouvy ML. Effects of a clinical medication review focused on personal goals, quality of life, and health problems in older persons with polypharmacy: a randomised controlled trial (DREAMeR-study). PLoS Med. 2019;16(5):e1002798. doi:10.1371/journal.pmed.1002798
16. Wastesson JW, Cedazo Minguez A, Fastbom J, Maioli S, Johnell K. The composition of polypharmacy: a register-based study of Swedes aged 75 years and older. PLoS One. 2018;13(3):e0194892. doi:10.1371/journal.pone.0194892
17. Eckerblad J, Theander K, Ekdahl A, et al. Symptom burden in community-dwelling older people with multimorbidity: a cross-sectional study. BMC Geriatr. 2015;15:1. doi:10.1186/1471-2318-15-1
18. Olivier P, Bertrand L, Tubery M, Lauque D, Montastruc JL, Lapeyre-Mestre M. Hospitalizations because of adverse drug reactions in elderly patients admitted through the emergency department: a prospective survey. Drugs Aging. 2009;26(6):475–482. doi:10.2165/00002512-200926060-00004
19. Witticke D, Seidling HM, Klimm HD, Haefeli WE. Do we prescribe what patients prefer? Pilot study to assess patient preferences for medication regimen characteristics. Patient Prefer Adherence. 2012;6:679–684. doi:10.2147/PPA.S35950
20. Pazan F, Weiss C, Wehling M, FORTA. The FORTA (Fit fOR The Aged) list 2015: update of a validated clinical tool for improved pharmacotherapy in the elderly. Drugs Aging. 2016;33(6):447–449. doi:10.1007/s40266-016-0371-4
21. Borglin G, Jakobsson U, Edberg AK, Hallberg IR. Self-reported health complaints and their prediction of overall and health-related quality of life among elderly people. Int J Nurs Stud. 2005;42(2):147–158. doi:10.1016/j.ijnurstu.2004.06.003
22. Hellstrom Y, Hallberg IR. Perspectives of elderly people receiving home help on health, care and quality of life. Health Soc Care Community. 2001;9(2):61–71. doi:10.1046/j.1365-2524.2001.00282.x
23. Seppala LJ, Wermelink A, de Vries M, et al. Fall-risk-increasing drugs: a systematic review and meta-analysis: II. psychotropics. J Am Med Dir Assoc. 2018;19(4):
24. Caughey GE, Tait K, Vitry AI, Shakib S. Influence of medication risks and benefits on treatment preferences in older patients with multimorbidity. Patient Prefer Adherence. 2017;11:131–140. doi:10.2147/PPA.S118836
25. Murphy DJ, Gahm GJ, Santilli S, North P, Oliver SC, Shapiro H. Seniors’ preferences for cancer screening and medication use based on absolute risk reduction. J Gerontol A Biol Sci Med Sci. 2002;57(2):M100–105. doi:10.1093/gerona/57.2.M100
26. Wurmbach VS, Lampert A, Schmidt SJ, et al. Komplexe Arzneimitteltherapien vereinfachen. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2018;61(9):1146–1151. German. doi:10.1007/s00103-018-2790-3
27. Schmidt SJ, Wurmbach VS, Lampert A, et al. Individual factors increasing complexity of drug treatment-a narrative review. Eur J Clin Pharmacol. 2020;76(6):745–754. doi:10.1007/s00228-019-02818-7
28. Schlereth C, Eckert C, Schaaf R, Skiera B. Measurement of preferences with self-explicated approaches: a classification and merge of trade-off- and non-trade-off-based evaluation types. Eur J Oper Res. 2014;238:185–198. doi:10.1016/j.ejor.2014.03.010
29. Brefka S, Dallmeier D, Muhlbauer V, et al. A proposal for the retrospective identification and categorization of older people with functional impairments in scientific studies-recommendations of the Medication and Quality of Life in Frail Older Persons (MedQoL) research group. J Am Med Dir Assoc. 2019;20(2):138–146. doi:10.1016/j.jamda.2018.11.008
30. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
31. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5(1–2):165–173. doi:10.1300/J018v05n01_09
32. Atkinson MJ, Sinha A, Hass SL, et al. Validation of a general measure of treatment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a national panel study of chronic disease. Health Qual Life Outcomes. 2004;2:12. doi:10.1186/1477-7525-2-12
33. Case SM, Fried TR, O’Leary J. How to ask: older adults’ preferred tools in health outcome prioritization. Patient Educ Couns. 2013;91(1):29–36. doi:10.1016/j.pec.2012.11.010
34. Huang SF, Huang CM, Chen SF, Lu LT, Guo JL. New partnerships among single older adults: a Q methodology study. BMC Geriatr. 2019;19(1):74. doi:10.1186/s12877-019-1091-5
35. Tielen M, van Exel NJ, van Buren MC, Maasdam L, Weimar W. Attitudes towards medication non-adherence in elderly kidney transplant patients: a Q methodology study. Nephrol Dial Transplant. 2011;26(5):1723–1728. doi:10.1093/ndt/gfq642
36. Gell NM, Rosenberg DE, Demiris G, LaCroix AZ, Patel KV. Patterns of technology use among older adults with and without disabilities. Gerontologist. 2015;55(3):412–421. doi:10.1093/geront/gnt166
37. Fromme EK, Kenworthy-Heinige T, Hribar M. Developing an easy-to-use tablet computer application for assessing patient-reported outcomes in patients with cancer. Support Care Cancer. 2011;19(6):815–822. doi:10.1007/s00520-010-0905-y
38. Brahmandam S, Holland WC, Mangipudi SA, et al. Willingness and ability of older adults in the emergency department to provide clinical information using a tablet computer. J Am Geriatr Soc. 2016;64(11):2362–2367. doi:10.1111/jgs.14366
39. Junius-Walker U, Stolberg D, Steinke P, Theile G, Hummers-Pradier E, Dierks ML. Health and treatment priorities of older patients and their general practitioners: a cross-sectional study. Qual Prim Care. 2011;19(2):67–76.
40. Salisbury C, Man MS, Bower P, et al. Management of multimorbidity using a patient-centred care model: a pragmatic cluster-randomised trial of the 3D approach. Lancet. 2018;392(10141):41–50. doi:10.1016/S0140-6736(18)31308-4
41. Pel-Littel RE, van Weert JCM, Minkman MM, Scholte Op Reimer WJM, van de Pol MH, Buurman BM. The development of the evidence-based SDM(MCC) intervention to improve shared decision making in geriatric outpatients: the DICO study. BMC Med Inform Decis Mak. 2020;20(1):35. doi:10.1186/s12911-020-1022-6
42. Blaum CS, Rosen J, Naik AD, et al. Feasibility of implementing Patient Priorities Care for older adults with multiple chronic conditions. J Am Geriatr Soc. 2018;66(10):2009–2016. doi:10.1111/jgs.15465
43. Naik AD, Dindo LN, Van Liew JR, et al. Development of a clinically feasible process for identifying individual health priorities. J Am Geriatr Soc. 2018;66(10):1872–1879. doi:10.1111/jgs.15437
44. Lavan AH, O’Mahony D, Gallagher P, et al. The effect of SENATOR (Software ENgine for the Assessment and optimisation of drug and non-drug Therapy in Older peRsons) on incident adverse drug reactions (ADRs) in an older hospital cohort – trial protocol. BMC Geriatrics. 2019;19(1):40. doi:10.1186/s12877-019-1047-9
45. O’Mahony D, Gudmundsson A, Soiza RL, et al. Prevention of adverse drug reactions in hospitalized older patients with multi-morbidity and polypharmacy: the SENATOR* randomized controlled clinical trial. Age Ageing. 2020;49(4):605–614. doi:10.1093/ageing/afaa072
46. McCarthy C, Clyne B, Boland F, et al. GP-delivered medication review of polypharmacy, deprescribing, and patient priorities in older people with multimorbidity in Irish primary care (SPPiRE Study): a cluster randomised controlled trial. PLoS Med. 2022;19(1):e1003862. doi:10.1371/journal.pmed.1003862
47. Fried TR, Byers AL, Gallo WT, et al. Prospective study of health status preferences and changes in preferences over time in older adults. Arch Intern Med. 2006;166(8):890–895. doi:10.1001/archinte.166.8.890
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.