")
Back to Journals » Patient Preference and Adherence » Volume 10
Development of a new diabetes medication self-efficacy scale and its association with both reported problems in using diabetes medications and self-reported adherence
Authors Sleath B, Carpenter D, Blalock S, Davis S , Hickson R, Lee C, Ferreri S , Scott J, Rodebaugh L, Cummings D
Received 26 November 2015
Accepted for publication 9 March 2016
Published 7 June 2016 Volume 2016:10 Pages 1003—1010
DOI https://doi.org/10.2147/PPA.S101349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Betsy Sleath,1,2 Delesha M Carpenter,1 Susan J Blalock,1 Scott A Davis,1 Ryan P Hickson,1 Charles Lee,3 Stefanie P Ferreri,4 Jennifer E Scott,5 Lisa B Rodebaugh,6 Doyle M Cummings6,7
1Division of Pharmaceutical Outcomes and Policy, UNC Eshelman School of Pharmacy, The University of North Carolina at Chapel Hill, Chapel Hill, 2Cecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill, Chapel Hill, 3Polyglot Systems, Inc., Morrisville, 4Division of Practice Advancement and Clinical Education, UNC Eshelman School of Pharmacy, 5Consortium for Implementation Science, Department of Health Policy and Management, Gillings School of Global Public Health, The University of North Carolina at Chapel Hill, Chapel Hill, 6Department of Family Medicine, Brody School of Medicine, East Carolina University, Greenville, 7Department of Public Health, Brody School of Medicine, East Carolina University, Greenville, NC, USA
Background: Although there are several different general diabetes self-efficacy scales, there is a need to develop a self-efficacy scale that providers can use to assess patient’s self-efficacy regarding medication use. The purpose of this study was to: 1) develop a new diabetes medication self-efficacy scale and 2) examine how diabetes medication self-efficacy is associated with patient-reported problems in using diabetes medications and self-reported adherence.
Patients and methods: Adult English-speaking patients with type 2 diabetes were recruited from a family medicine clinic and a pharmacy in Eastern North Carolina, USA. The patients were eligible if they reported being nonadherent to their diabetes medicines on a visual analog scale. Multivariable regression was used to examine the relationship between self-efficacy and the number of reported diabetes medication problems and adherence.
Results: The diabetes medication self-efficacy scale had strong reliability (Cronbach’s alpha =0.86). Among a sample (N=51) of mostly African-American female patients, diabetes medication problems were common (6.1±3.1) and a greater number of diabetes medications were associated with lower medication adherence (odds ratio: 0.35; 95% confidence interval: 0.13, 0.89). Higher medication self-efficacy was significantly related to medication adherence (odds ratio: 1.17; 95% confidence interval: 1.05, 1.30) and inversely related to the number of self-reported medication problems (β=–0.13; P=0.006).
Conclusion: Higher diabetes medication self-efficacy was associated with fewer patient-reported medication problems and better medication adherence. Assessing medication-specific self-efficacy may help to identify medication-related problems that providers can help the patients address, potentially improving adherence and patient outcomes.
Keywords: diabetes, adherence, self-efficacy, literacy
Background
Diabetes is a significant public health problem that affects 9.3% of the population in America.1 African-American adults are twice as likely as non-Hispanic White adults to have been diagnosed with diabetes.2,3 Medication management is a critical self-management skill for individuals living with diabetes who cannot control their disease with diet and exercise. Poor medication understanding and adherence are common among the diabetes patients.4,5 Research has shown that the African-American patients worry more about side effects and medication dependency and are less likely to adhere to their diabetes medications than the White patients.6–8 Adherence to diabetes medications is important because better medication adherence has been associated with improved diabetes control.9
Prior research in glaucoma and hypertension has found that medication self-efficacy is significantly associated with medication adherence.10–13 Self-efficacy is one of the key constructs in social cognitive theory.14 Self-efficacy is defined as individuals’ personal beliefs regarding their capabilities to carry out a specific task to achieve a desired outcome.14 According to social cognitive theory, if individuals have higher self-efficacy that they can perform a certain behavior, such as taking a medication, they are more likely to perform the behavior and exert greater effort to overcome obstacles that are encountered. In diabetes, self-efficacy is important because interventions that improve self-efficacy have been associated with improved glycemic control.15 Self-efficacy appears to influence the performance of self-care behaviors, including medication use, which in turn affects glycemic control.16–18 The effect of self-efficacy on diabetes self-care is consistent across races, ethnic groups, and health literacy levels.19
Prior qualitative research has found that the patients often mention in focus groups: 1) the barriers they have to chronic illness medication self-efficacy and 2) that lack of knowledge of their medications can impede their confidence in managing a chronic medical condition such as diabetes.20 Medication self-efficacy scales have been developed for both hypertension and glaucoma, but not for diabetes.10,12,21
There are several different general diabetes self-efficacy scales such as the Diabetes Management Self-Efficacy Scale; the Diabetes Empowerment Scale, which measures diabetes-related psychosocial self-efficacy; and the Perceived Diabetes Self-Management Scale.18,22,23 The scales all assess general diabetes management self-efficacy without a specific focus on medications. Although some of these general diabetes self-efficacy scales have been positively associated with medication adherence, only two of 20 items on the Diabetes Management Self-Efficacy Scale and no items on the other two scales, specifically pertain to medication use.18,22–24
There is also an Insulin Management Diabetes Self-Efficacy Scale, which assesses confidence in managing/taking insulin.25 However, there is a need to develop a diabetes medication self-efficacy scale relevant to all types of medications commonly used to treat diabetes (eg, oral agents, insulin, and other types of injections), because the patients often take more than one type at the same time. A diabetes medication self-efficacy scale could be used to help providers assess patient’s lack of confidence in taking their medications under different circumstances so that they could help the patients to overcome barriers to medication use.
A few studies have investigated patient-articulated barriers to medication use and their potential relationship with medication self-efficacy.26,27 A systematic review of medication problems in the patients with diabetes or cardiovascular disease revealed three major categories of problems: patient-related factors (including socioeconomic and lifestyle factors), medication-related factors (eg, fear of medicine, lack of knowledge), and condition-related factors (eg, lack of knowledge, fear of condition, and complications).26 Within these three broad areas, prior works specifically identified the following patient-reported problems with diabetes medications: cost of medications,27,28 how medications work alongside diet and exercise,28–30 the belief that natural remedies are an alternative to medications,29 forgetting to take medications or inconvenient to take all medications,27,28 side effects,27,30 not wanting to take medications,27 issues understanding medicine labels,27 access issues and lack of support,27,28 and lack of knowledge about their condition.29
In order to take the first steps in developing a new tool that can capture patient-reported information related to diabetes medication problems and associated self-efficacy, the objectives of the current study were to: 1) develop a new diabetes medication self-efficacy scale, and 2) examine how diabetes medication self-efficacy is associated with patient-reported problems in using diabetes medications and self-reported adherence.
Patients and methods
This pilot study was conducted in compliance with the University of North Carolina Institutional Review Board and Office of Human Research Ethics and in accord with the tenets of the Treaty of Helsinki and was Health Insurance Portability and Accountability Act compliant. All patients signed a statement of informed consent.
Procedure
The patients were recruited from a family practice clinic and a pharmacy in Eastern North Carolina, USA. The patients were eligible for the study if they were: 1) at the age of 18 years or older; 2) had been diagnosed with type 2 diabetes; 3) were taking at least one oral and/or injectable medication for diabetes; 4) could speak English; 5) reported being nonadherent to their diabetes medicines on a visual analog scale (VAS); and 6) were African-American or White. The VAS screener we used to determine eligibility asked the patients to put a line on a 10 cm scale indicating how much of the time they use all of their diabetes medications exactly as directed (range is 0= none of the time to 10= all of the time).31,32 The VAS has strong validity and reliability and has been validated against prescription drug refill records.32,33 The patients were eligible for our study if they indicated that they were not always using their diabetes medication exactly as directed (ie, they did not report their adherence as 10).
The interested patients were told about the study by clinic or pharmacy staff and were referred to a research assistant. The patients were consented and then screened to see if they were eligible for the study. The patients who met the eligibility criteria were enrolled. The research associate then interviewed the patient. Patients received US$20 for participating in the study.
Measurement
Demographic and other characteristics
The following demographic and other characteristics were collected: age, sex, race (African-American versus non-African- American), whether the patient is on oral diabetes medicines, whether the patient is on injectable diabetes medicines, and how many diabetes medications the patient is taking.
Rapid Estimate of Adult Literacy in Medicine
Each subject completed the Rapid Estimate of Adult Literacy in Medicine (REALM). This is a validated, rapid screening instrument designed to identify the patients who have difficulty reading common medical and lay terms that are routinely used in patient education materials.34 The REALM was chosen because it has high face validity and high criterion validity, it has been well received by the patients, and it takes only 2–3 minutes to administer and score.34 Patient scores on the REALM correspond to literacy levels (score of 0–60= eighth grade and less and 61–66= ninth grade and more).
Patient Health Questionnaire-2
The Patient Health Questionnaire-2 assesses the frequency of depressed mood and anhedonia over the past 2 weeks.35 The scores range from 0 to 6, and a score of 3 is an optimal cut point for screening depressive symptoms.35 Depressive symptoms were measured as a dichotomous variable (0–2= no depressive symptoms and 3–6= depressive symptoms).
Beliefs about medications questionnaire
The four-item concerns and five-item necessities sections of the Beliefs about Medications Questionnaire were administered.36 The scores ranged from 4 to 20 on the concerns subscale and 10 to 25 on the necessities subscale. Higher scores correspond to more positive beliefs (eg, less concerns, strong beliefs in necessity).
Diabetes medication self-efficacy questionnaire development
A new diabetes medication self-efficacy scale was developed. It was modeled after the hypertension medication self-efficacy scale and the glaucoma medication adherence self-efficacy scale.10,12 The scale was modified to be appropriate for the diabetes patients with input from seven diabetes patients and four health care professionals who work closely with the diabetes patients. The final questionnaire that the patients completed included 20 items to assess self-efficacy in overcoming barriers that might interfere with the use of diabetes medications (Figure S1). The response options for the self-efficacy items were not at all confident, somewhat confident, and very confident.
One item was eliminated “confidence in using at work or school” because many individuals left it blank because they were retired. A Cronbach’s alpha was then calculated to assess reliability of the resulting 19-item diabetes medication self-efficacy scale. If there were missing data for an item, the mean score was substituted for the item. Scores on the diabetes medication adherence scale ranged from 19 (lower self-efficacy) to 57 (higher self-efficacy). Our sample was too small to conduct a factor analysis.
Reported problems in using diabetes medicines
Each patient was asked to evaluate the degree to which 14 potential problems or concerns in using diabetes medications affected them (“none”, “a little”, or “a lot”). Each of these were recoded into a dichotomous variable (none versus a little or a lot of problems). The 14 problem areas were also summed to create a nonweighted variable equal to the number of problems or concerns in taking diabetes medications that ranged from 0 to 14.
Self-reported medication adherence
Morisky’s eight-item measure of self-reported adherence, which has a reliability of 0.83, was used to assess adherence.37 The Morisky measure has been used successfully with the diabetes patients.9,38 The eight-item scale is summed after one item (did you take your diabetes medicine yesterday) is reverse coded. The variable was then recoded into the following categories: high or medium adherence (6–8) versus low adherence (0–5).
Analysis
First, the descriptive statistics for the patient characteristics were calculated. Next, the bivariate relationships between patient age, sex, race, REALM score, Patient Health Questionnaire-2 score, medication concerns, medication necessities, diabetes medication self-efficacy and 1) patient-reported problems in using diabetes medicines, and 2) self-reported adherence were examined using Pearson’s correlation coefficients, independent sample t-tests, and chi-square statistics.
Because this was a pilot study and the sample size was small, only variables that were significant in the bivariate analyses were included in the multivariable linear regression, predicting the number of patient-reported problems in using diabetes medications. Similarly, only variables significant in the bivariate analyses were included in the multivariable logistic regression, predicting patient-reported adherence on the Morisky scale.
Results
Table 1 presents patient characteristics (N=51). The sample was 84.3% African-Americans and 80.4% females. One patient who classified himself as White also stated that he was partly Native American. The patients were on an average of 2.1 diabetes medications (standard deviation =0.9, range =1–4), 80.4% of the patients were on oral diabetes medications and 50.9% were on injectable diabetes medications.
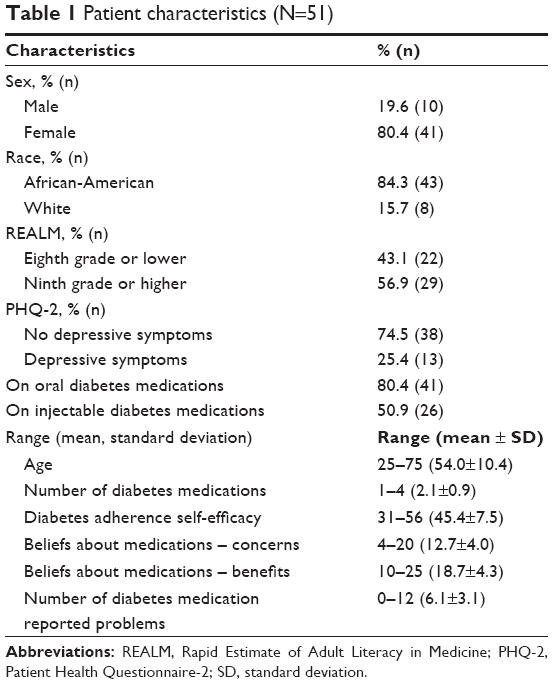 | Table 1 Patient characteristics (N=51) |
Table 2 presents patients’ responses on the 19-item diabetes medication self-efficacy scale. The situations where the patients reported that they were not at all sure they could take their diabetes medications were when the medications cost a lot of money (31.4%), the patients come home late from work or other activities (23.5%), the patients are confused (21.6%), the medications cause some side effects (19.6%), the medications sometimes make the patients tired (19.6%), and the medications make the patient shaky or jittery (19.6%). The measured reliability of the self-efficacy scale was a Cronbach’s alpha of 0.86.
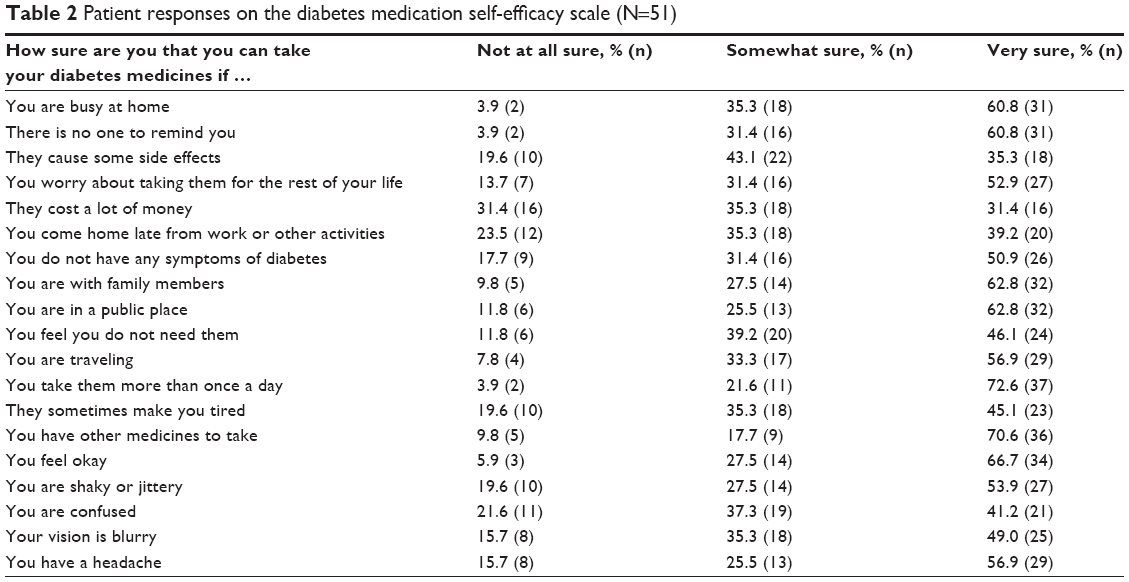 | Table 2 Patient responses on the diabetes medication self-efficacy scale (N=51) |
The patients reported an average of 6.1 problems with their diabetes medications (standard deviation =3.1, range =0–12). The most commonly reported problems were as follows: worried about health problems from diabetes (74.5%), side effects from diabetes medicines (70.6%), hard to pay for glucose monitoring supplies (64.7%), forgot to take medicines (54.9%), and hard to pay for diabetes pills (54.9%).
The African-American patients were significantly more likely to report more diabetes medication problems than the non-African-American patients (t-test =2.66, P=0.01). The patients with depressive symptoms were significantly more likely to report more diabetes medication problems (t-test =2.57, P=0.013). The patients with higher scores on the beliefs about medications concerns scale were significantly more likely to report more diabetes medication problems (Pearson’s correlation =0.47, P=0.0005). The beliefs about medications concerns subscale had a Cronbach’s alpha of 0.77, and the necessities subscale had a Cronbach’s alpha of 0.82.
The patients who had a literacy level of ninth grade or more were significantly less likely to report diabetes medication problems than those who had eighth grade or less (t-test =−3.15, P=0.003). The patients with higher diabetes medication self-efficacy were significantly less likely to report diabetes medication problems (Pearson’s correlation =−0.52, P<0.0001). No other patient characteristics were significantly associated with the number of diabetes medication problems.
Table 3 presents the linear regression predicting the number of patient-reported problems in using diabetes medications. Having depressive symptoms was not significant in the multivariable analysis (β=0.26, P=0.750). African- Americans (β=2.24, P=0.016) and the patients who had more concerns about using their medications (β=0.29, P=0.003) reported significantly more problems in using their diabetes medications. The patients with higher diabetes medication self-efficacy (β=−0.13, P=0.006) and higher health literacy (β=−1.51, P=0.036) reported significantly fewer problems.
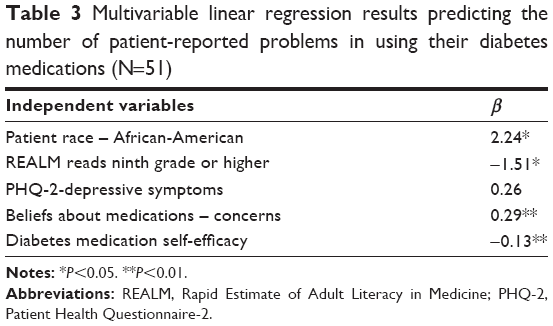 | Table 3 Multivariable linear regression results predicting the number of patient-reported problems in using their diabetes medications (N=51) |
The patients with higher diabetes medication self-efficacy were significantly more likely to report being adherent to their diabetes medications (t-test =−3.30, P=0.002). The patients with higher scores on the beliefs about medications concerns scale were significantly less likely to report being adherent to their diabetes medications (t-test =3.36, P=0.0015). The patients on more diabetes medications were significantly less likely to be adherent to their diabetes medications (t-test =2.36, P=0.02). No other patient characteristics were significantly associated with adherence.
Table 4 presents the logistic regression predicting patient self-reported diabetes medication adherence. Beliefs about medications concerns were not included in the final regression because they were significantly correlated with the number of medications (Pearson’s correlation =−0.28, P=0.04) and diabetes medications self-efficacy (Pearson’s correlation =0.30, P=0.03). The patients with higher diabetes medication self-efficacy scores were significantly more adherent to their medications than the patients with lower self-efficacy (odds ratio =1.17; 95% confidence interval: 1.05, 1.30). The patients on more diabetes medications were significantly less adherent to their medications (odds ratio =0.35; 95% confidence interval: 0.13, 0.89). No other patient characteristics were significantly associated with adherence.
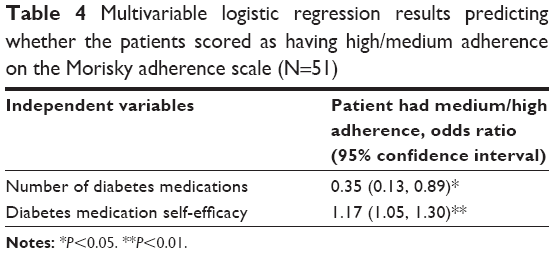 | Table 4 Multivariable logistic regression results predicting whether the patients scored as having high/medium adherence on the Morisky adherence scale (N=51) |
Discussion
This study reports on the development and evaluation of a diabetes medication self-efficacy scale. The scale had strong reliability and was significantly associated with patient self-reported diabetes medication adherence, which suggests good construct validity. Diabetes medication self-efficacy was also strongly associated with the number of diabetes medication problems that the patients reported having.
The diabetes medication self-efficacy scale could be used to screen patients with low self-efficacy, so that providers such as physicians, nurse practitioners, pharmacists, and diabetes educators could educate patients and attempt to improve their diabetes medication self-efficacy. This would then hopefully result in fewer patient problems in using their diabetes medications and improved medication adherence.
Additionally, the patients with higher scores on the beliefs about medication concerns scale were found to report more problems in using their diabetes medications and lower adherence. This suggests that providers should work with the patients to help them overcome any concerns they have in using diabetes medications. African-Americans reported significantly more problems in using their diabetes medications than Whites, which is similar to the previous research that found that African-Americans were more worried about side effects and medication dependency than Whites.7 Providers should work closely with the African-American patients to address or manage any problems they have in using their diabetes medications.
The patients on more medications were significantly less adherent to their diabetes medications, which is similar to the results of other studies in different therapeutic areas.39 This suggests that, when possible, providers should simplify the patients’ medication regimens and prescribe fewer medications for the patient’s condition.
The patients who had a literacy level of eighth grade or less were significantly more likely to report more diabetes medication problems. Prior works in diabetes have found lower literate patients to have worse adherence and more hypoglycemia.8,40 Our findings suggest that providers might want to spend more time with less literate patients to help them overcome any problems they might have in using their diabetes medications.
The patients with more medication concerns reported significantly more problems in using their diabetes medications and lower adherence. Providers need to help the diabetes patients overcome negative views or concerns they have about using diabetes medications so that they will take medications to help control their blood sugar.
Limitations
The study has many limitations. First, as the patients were recruited from one pharmacy and one family medicine clinic in the Eastern part of North Carolina, the results may not be generalizable to other geographic areas. Second, this was a pilot study with a small sample size. Future research should test the psychometric properties of the diabetes medication self-efficacy scale with larger and more diverse patient samples.
Conclusion
Despite the limitations, this study provides new information on the development of a diabetes medication self-efficacy scale. An association between diabetes medication self-efficacy and both patient-reported problems in using diabetes medications and self-reported adherence was identified in this study. Future research in larger and more diverse patient populations needs to be conducted to determine if an intervention to improve self-efficacy longitudinally is associated with 1) objective changes in adherence measured by medication refills or electronic monitoring, and 2) improved hemoglobin A1C. If successful, identifying the diabetes patients with low medication self-efficacy in a clinical setting may allow providers to address medication-related problems and potentially improve adherence. As diabetes management can be improved through better medication adherence,9 the diabetes medication self-efficacy scale has the potential to allow providers to augment patient self-efficacy in taking their diabetes medications in areas where they report difficulties.
Acknowledgments
This study was supported by the UNC Center for Diabetes Translation Research to Reduce Health Disparities, supported by Grant Number P30DK093002 from the National Institute of Diabetes and Digestive and Kidney Diseases and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant Award Number 1UL1TR001111. Ryan P Hickson is supported by the American Foundation for Pharmaceutical Education as the 2015 Phi Lambda Sigma First Year Graduate School Fellow. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Disclosure
The authors report no conflicts of interest in this work, participated fully in the project, and take full responsibility for the content of this article.
References
Cdc.gov [webpage on the Internet]. Atlanta: Centers for Disease Control and Prevention; 2014 [updated May 15, 2015; cited March 3, 2016]. Available from: http://www.cdc.gov/diabetes/data/statistics/2014statisticsreport.html. Accessed March 3, 2016. | ||
Carter EL, Nunlee-Bland G, Callender C. A patient-centric, provider-assisted diabetes telehealth self-management intervention for urban minorities. Perspect Health Inf Manag. 2011;8:1b. | ||
Minorityhealth.hhs.gov [webpage on the Internet]. Rockville, MD: Office of Minority Health; 2011 [updated June 16, 2015; cited March 3, 2016]. Available from: http://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=18. Accessed March 3, 2016. | ||
McDonald HP, Garg AX, Haynes RB. Interventions to enhance patient adherence to medication prescriptions: scientific review. JAMA. 2002;288(22):2868–2879. | ||
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. | ||
Adams AS, Trinacty CM, Zhang F, et al. Medication adherence and racial differences in A1C control. Diabetes Care. 2008;31(5):916–921. | ||
Huang ES, Brown SE, Thakur N, et al. Racial/ethnic differences in concerns about current and future medications among patients with type 2 diabetes. Diabetes Care. 2009;32(2):311–316. | ||
Osborn CY, Cavanaugh K, Wallston KA, et al. Health literacy explains racial disparities in diabetes medication adherence. J Health Commun. 2011;16(suppl 3):268–278. | ||
Krapek K, King K, Warren SS, et al. Medication adherence and associated hemoglobin A1c in type 2 diabetes. Ann Pharmacother. 2004;38(9):1357–1362. | ||
Ogedegbe G, Mancuso CA, Allegrante JP, Charlson ME. Development and evaluation of a medication adherence self-efficacy scale in hypertensive African-American patients. J Clin Epidemiol. 2003;56(6):520–529. | ||
Sleath B, Blalock SJ, Carpenter DM, et al. Ophthalmologist-patient communication, self-efficacy, and glaucoma medication adherence. Ophthalmology. 2015;122(4):748–754. | ||
Sleath B, Blalock SJ, Robin A, et al. Development of an instrument to measure glaucoma medication self-efficacy and outcome expectations. Eye (Lond). 2010;24(4):624–631. | ||
Sleath BL, Blalock SJ, Muir KW, et al. Determinants of self-reported barriers to glaucoma medicine administration and adherence: a multisite study. Ann Pharmacother. 2014;48(7):856–862. | ||
Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. 1st ed. Englewood Cliffs, NJ: Prentice-Hall; 1986. | ||
Ha M, Hu J, Petrini MA, McCoy TP. The effects of an educational self-efficacy intervention on osteoporosis prevention and diabetes self-management among adults with type 2 diabetes mellitus. Biol Res Nurs. 2014;16(4):357–367. | ||
Gao J, Wang J, Zheng P, et al. Effects of self-care, self-efficacy, social support on glycemic control in adults with type 2 diabetes. BMC Fam Pract. 2013;14:66. | ||
King DK, Glasgow RE, Toobert DJ, et al. Self-efficacy, problem solving, and social-environmental support are associated with diabetes self-management behaviors. Diabetes Care. 2010;33(4):751–753. | ||
Walker RJ, Smalls BL, Hernandez-Tejada MA, Campbell JA, Egede LE. Effect of diabetes self-efficacy on glycemic control, medication adherence, self-care behaviors, and quality of life in a predominantly low-income, minority population. Ethn Dis. 2014;24(3):349–355. | ||
Sarkar U, Fisher L, Schillinger D. Is self-efficacy associated with diabetes self-management across race/ethnicity and health literacy? Diabetes Care. 2006;29(4):823–829. | ||
Williams A, Manias E, Cross W, Crawford K. Motivational interviewing to explore culturally and linguistically diverse people’s comorbidity medication self-efficacy. J Clin Nurs. 2014;24(9–10):1269–1279. | ||
Sleath B, Blalock SJ, Stone JL, et al. Validation of a short version of the glaucoma medication self-efficacy questionnaire. Br J Ophthalmol. 2012;96(2):258–262. | ||
Al-Khawaldeh OA, Al-Hassan MA, Froelicher ES. Self-efficacy, self-management, and glycemic control in adults with type 2 diabetes mellitus. J Diabetes Complications. 2012;26(1):10–16. | ||
Hernandez-Tejada MA, Campbell JA, Walker RJ, Smalls BL, Davis KS, Egede LE. Diabetes empowerment, medication adherence and self-care behaviors in adults with type 2 diabetes. Diabetes Technol Ther. 2012;14(7):630–634. | ||
Wallston KA, Rothman RL, Cherrington A. Psychometric properties of the Perceived Diabetes Self-Management Scale (PDSMS). J Behav Med. 2007;30(5):395–401. | ||
Hurley A. Measuring self-care ability in patients with diabetes: the insulin management diabetes self-efficacy scale. In: Waltz C, editor. Measurement of Nursing Outcomes: Measuring Client Self Care and Coping. Vol. 4. New York, NY: Springer; 1990:28–44. | ||
Al Hamid A, Ghaleb M, Aljadhey H, Aslanpour Z. A systematic review of qualitative research on the contributory factors leading to medicine-related problems from the perspectives of adult patients with cardiovascular diseases and diabetes mellitus. BMJ Open. 2014;4(9):e005992. | ||
Odegard PS, Carpinito G, Christensen DB. Medication adherence program: adherence challenges and interventions in type 2 diabetes. J Am Pharm Assoc. 2013;53(3):267–272. | ||
Hu J, Amirehsani K, Wallace DC, Letvak S. Perceptions of barriers in managing diabetes: perspectives of Hispanic immigrant patients and family members. Diabetes Educ. 2013;39(4):494–503. | ||
Coronado GD, Thompson B, Tejeda S, Godina R. Attitudes and beliefs among Mexican Americans about type 2 diabetes. J Health Care Poor Underserved. 2004;15(4):576–588. | ||
Rustveld LO, Pavlik VN, Jibaja-Weiss ML, Kline KN, Gossey JT, Volk RJ. Adherence to diabetes self-care behaviors in English- and Spanish-speaking Hispanic men. Patient Prefer Adherence. 2009;3:123–130. | ||
Amico KR, Fisher WA, Cornman DH, et al. Visual analog scale of ART adherence: association with 3-day self-report and adherence barriers. J Acquir Immune Defic Syndr. 2006;42(4):455–459. | ||
Nau DP, Steinke DT, Williams LK, et al. Adherence analysis using visual analog scale versus claims-based estimation. Ann Pharmacother. 2007;41(11):1792–1797. | ||
McDowell I. Measuring Health: A Guide to Rating Scales and Questionnaires. 3rd ed. New York, NY: Oxford University Press; 2006. | ||
Davis WK, Hess GE, Harrison RV, Hiss RG. Psychosocial adjustment to and control of diabetes mellitus: differences by disease type and treatment. Health Psychol. 1987;6(1):1–14. | ||
Kroenke K, Spitzer RL, Williams JB. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. | ||
Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. | ||
Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich). 2008;10(5):348–354. | ||
Jamous RM, Sweileh WM, Abu-Taha AS, Sawalha AF, Zyoud SH, Morisky DE. Adherence and satisfaction with oral hypoglycemic medications: a pilot study in Palestine. Int J Clin Pharm. 2011;33(6):942–948. | ||
Dailey G, Kim MS, Lian JF. Patient compliance and persistence with antihyperglycemic drug regimens: evaluation of a medicaid patient population with type 2 diabetes mellitus. Clin Ther. 2001;23(8):1311–1320. | ||
Sarkar U, Karter AJ, Liu JY, Moffet HH, Adler NE, Schillinger D. Hypoglycemia is more common among type 2 diabetes patients with limited health literacy: the Diabetes Study of Northern California (DISTANCE). J Gen Intern Med. 2010;25(9):962–968. |
Supplementary material
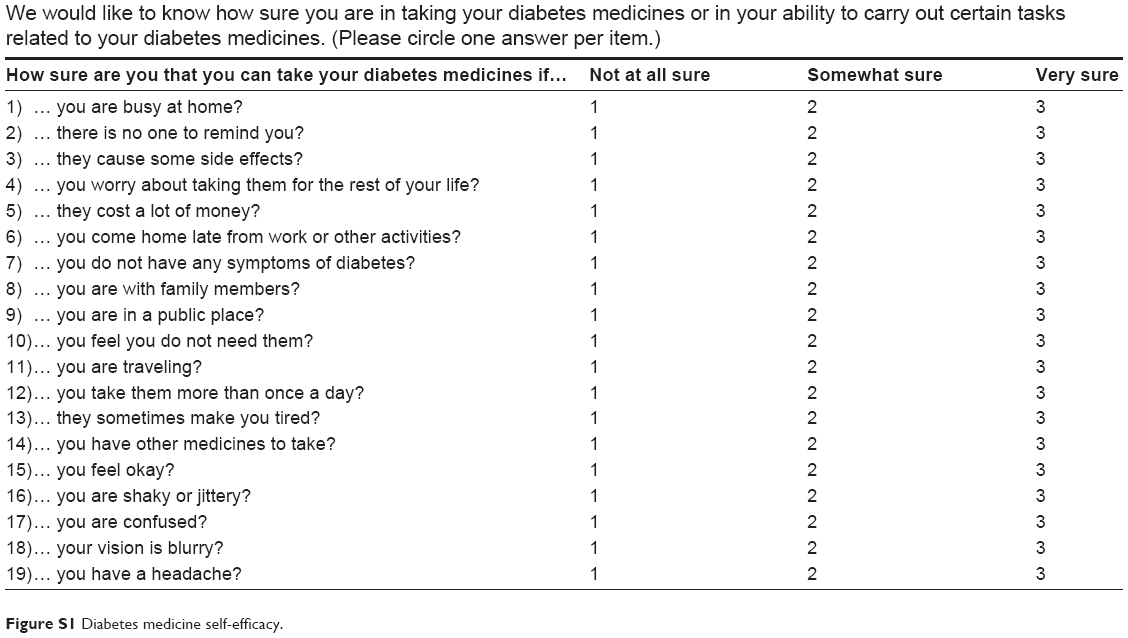 | Figure S1 Diabetes medicine self-efficacy. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.