")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Development and Validation of Psychological Contract Scale for Hospital Pharmacists
Authors Zhang T, Yin C, Geng Y, Zhou Y, Sun S , Tang F
Received 30 June 2020
Accepted for publication 23 September 2020
Published 2 November 2020 Volume 2020:13 Pages 1433—1442
DOI https://doi.org/10.2147/JMDH.S270030
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ting Zhang,1– 4,* Chengchen Yin,1– 3,* Yongchen Geng,1– 3 Yan Zhou,1– 3 Shusen Sun,5 Fushan Tang1– 3
1Department of Clinical Pharmacy, School of Pharmacy, Zunyi Medical University, Zunyi 563006, People’s Republic of China; 2Key Laboratory of Basic Pharmacology of Ministry of Education and Joint International Research Laboratory of Ethnomedicine of Ministry of Education, Zunyi Medical University, Zunyi 563006, People’s Republic of China; 3The Key Laboratory of Clinical Pharmacy in Zunyi City, Zunyi Medical University, Zunyi 563006, People’s Republic of China; 4Department of Pharmacy, Guiyang Hospital of Stomatology, Guiyang 550000, People’s Republic of China; 5College of Pharmacy and Health Sciences, Western New England University, Springfield, MA 01119, USA
*These authors contributed equally to this work
Correspondence: Fushan Tang
Department of Clinical Pharmacy, School of Pharmacy, Zunyi Medical University, Zunyi 563006, People’s Republic of China
Tel/ Fax +86 851 2864 2334
Email [email protected]
Objective: To set up a psychological contract scale for hospital pharmacists to strengthen the management of pharmacists and improve the occupational health of pharmacists.
Methods: A psychological contract scale for hospital pharmacists with structured questionnaires was designed according to the professional characteristics of hospital pharmacists and validated through the investigation of pharmacists in 77 public medical institutions in Zunyi, China, which were included through stratified random sampling. Kaiser-Meyer-Olkin (KMO) Measure of Sampling Adequacy and Bartlett’s Test of Sphericity were used to assess the suitability of the sample for factor analysis. Validity of the dimensions was investigated with exploratory factor analysis. The principal component analysis and varimax rotation methods were used to identify the factor structure. The internal consistency was assessed by the Cronbach’s alpha coefficient.
Results: The psychological contract scale for hospital pharmacists was composed of pharmacists’ perceptions regarding the hospital, pharmacists themselves, and government/society responsibility. The KMO values of the three perceptions were 0.957, 0.930 and 0.917, respectively, all greater than 0.6. The significance probability of the Bartlett spherical test was 0.000, indicating good structural validity. The Cronbach’s alpha coefficient and half coefficient of the responsibilities in three sub-scales were all greater than 0.6, indicating good internal reliability of the scale. The average scores of the pharmacist responsibility, the hospital responsibility and the government/society responsibility in the pharmacists’ perception were 5.42± 0.637, 4.64± 1.069 and 4.49± 1.134, respectively. In the pharmacists’ perception, their own responsibility has been better fulfilled than those of hospitals and government/society.
Conclusion: The psychological contract scale for hospital pharmacists can be a useful tool to evaluate the psychological contract of hospital pharmacists for research and occupational health assessments and management in the area of hospital pharmacy.
Keywords: pharmacist, psychological contract, questionnaire
Introduction
A psychological contract, first proposed by Argyris, is used to describe the objective understanding and cognition of the mutual obligations in the exchange relationship between organizations and individuals.1,2 These consist of a series of unwritten expectations between employees and managers.3 Compared to written contracts, a psychological contract can better reflect mutual expectations between employees and organizations. The realization of these expectations affects inner feelings, work attitude, and performance of employees.4,5 Maintaining a satisfactory psychological contract can not only promote internal communication between employers and employees, but improve working atmosphere, employee performance and management efficiency.
Most of the existing studies on the management of medical professionals are based on psychological contracts focusing on nurses and doctors. It is believed that the violation of the psychological contract can be negatively related to job satisfaction and emotional organizational commitment, and positively related to the willingness to leave.6 An unsatisfactory psychological contract can make nurses feel disappointed and frustrated, eventually leading to turnover.7 When doctors perceive high levels of fulfillment based on their psychological contract, they are more committed and more active in contributing to their work.8 A high level of agreement on a psychological contract has an essential impact on reducing turnover.9,10 Organizational managers should minimize the negative impact of violating a psychological contract while working to maximize positive opportunities.11–14 This positive utilization of the psychological contract includes recognizing the importance of social exchange within the organization, building trust to ensure that staff are staying,15 and managing expectations through greater participation and leadership. These strong relationships can enhance reciprocity to achieve better management and service.16,17
Hospital pharmacists are unique and growing members of the healthcare team with an indispensable role in rational drug use. The medication intervention of the hospital pharmacists on the patients can not only effectively reduce the medication costs and the incidence of irrational medication use and adverse drug reactions, also significantly increase the medication adherence of the patients.18–22 In our previous study, it was found that maintaining the patients’ psychological contract with the pharmacists can effectively improve patients’ medication adherence and promote the harmonious pharmacist-patient relationship.23 However, reform in the medical care system, suboptimal pharmacist-employer relations and fierce competition inside and outside the hospital pharmacy profession have been adding increasing stress and role-confusion to hospital pharmacists. Thus, hospital pharmacists can also benefit from a well-maintained healthy psychological contract. If the psychological contract of hospital pharmacist is violated, their job burnout and low work motivation may negatively affect patients’ health outcomes. The research and management on a psychological contract for hospital pharmacists is urgently needed for hospital pharmacy administration. Though there were already some psychological contract scales in studies to assess the psychological contract of doctors and nurses,24–26 there is still a lack of research on the psychological contract of hospital pharmacists.
In this paper, we aimed to develop an evaluation scale of the psychological contract for hospital pharmacists and test the validity and reliability of the scale (the scale can be found in the appendix, both in English and Chinese).
Methods
Study Participants
According to the stratified random sampling method, 77 public hospitals at different levels in Zunyi City, China were included in this study. The investigation was carried out from July to September 2018. Pharmacists were invited to participate in an anonymous survey by cluster sampling for each medical institution. Inclusion criteria were 1) a pharmacist qualification certificate, 2) a background in pharmacy and currently working in a pharmacy, and 3) voluntary participation. Pharmacists who were trainees at the institutions were excluded.
Evaluation Tools
The preliminary draft of the hospital pharmacist psychological contract scale was developed by referring to some content in similar scales used for doctors in public hospitals,27 with changes according to professional characteristics of hospital pharmacists after consulting five specialists in the area of hospital pharmacy. The final draft was formed based on the survey feedback conducted at three hospitals. The scale consists of four sub-scales: Pharmacist Basic Information Questionnaire (including 10 items), Hospital Responsibility Questionnaire (17 items), Pharmacist Responsibility Questionnaire (14 items) and Government/Society Responsibility Questionnaire (9 items). There are a total of 50 items in the entire questionnaire. The following seven-level scoring system was adopted in the 3 responsibility questionnaires (a higher score from 0 to 6 means that a perceived responsibility has been better fulfilled in the pharmacists’ perception): “Not the responsibility of the hospital or pharmacist” (0), “the responsibility has not totally been fulfilled” (1), “the responsibility has basically not been fulfilled” (2), “a small part of the responsibility has been fulfilled” (3), “half of the responsibility has been fulfilled” (4), “most of the responsibility has been fulfilled” (5), and “all the responsibility has been fulfilled” (6).28
Statistical Analysis
Epidata 3.1 and SPSS (IBM Statistical Product and Service Solutions) 18.0 were used for data entry and statistical analysis. Both reliability and validity analysis was conducted. The Kaiser-Meyer-Olkin (KMO) Measure of Sampling Adequacy value was used to judge the number of factors extracted, validity of the dimensions were investigated with exploratory factor analysis. The principal component analysis and varimax rotation methods were used to identify the factor structure.29 Reliability analysis was carried out to verify internal consistency among items of the scale by using Cronbach’s alpha coefficient and half coefficient.30,31
Results
606 respondents’ questionnaires were collected from 77 medical institutions and evaluated. The demographics of pharmacists are listed in Table 1.
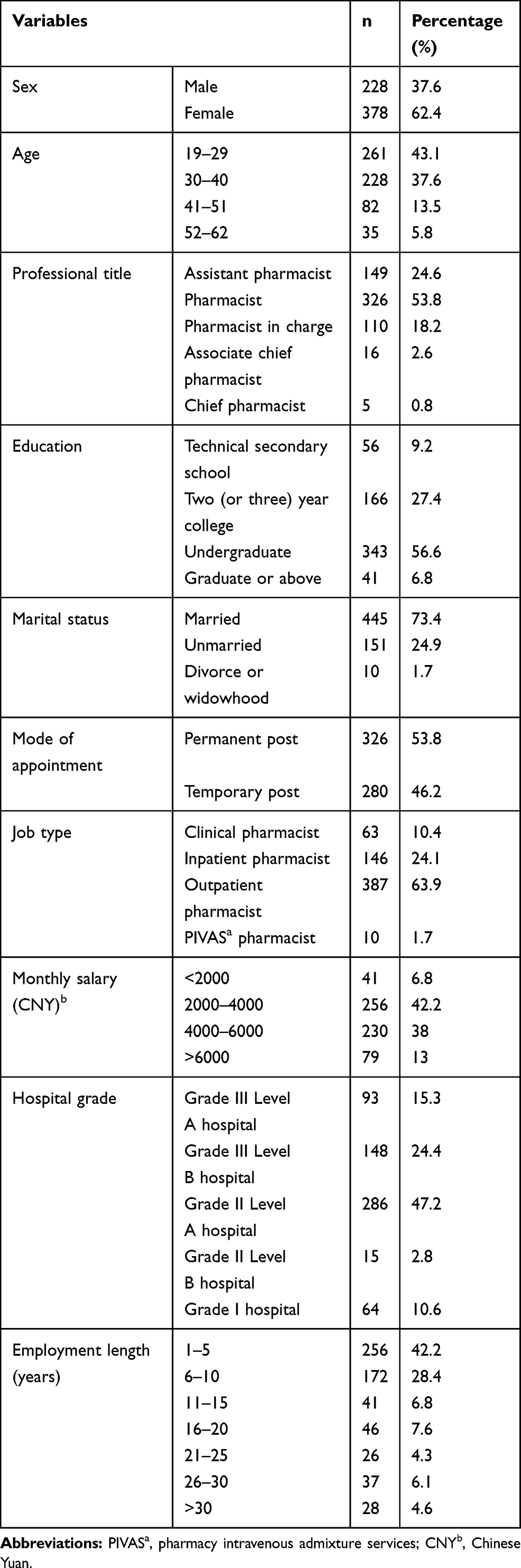 |
Table 1 Pharmacist Demographic Data |
Validity Analysis
Before the exploratory factor analysis, KMO measurement, and the Bartlett spherical test were conducted. The exploratory factor analysis showed that the KMO values of hospital responsibility, pharmacist responsibility, and government/society responsibility were 0.957, 0.930 and 0.917, respectively, all greater than 0.6. The significant probability of the Bartlett spherical test was 0.000, which indicated that factor analysis could be carried out. The explanatory rates of the cumulative variance of hospital responsibility, pharmacist responsibility, and government/society responsibility were 78.406% (Table 2), 73.451% (Table 2), and 75.779% (Table 2), respectively, all greater than 60%, indicating that the analysis results were reliable.
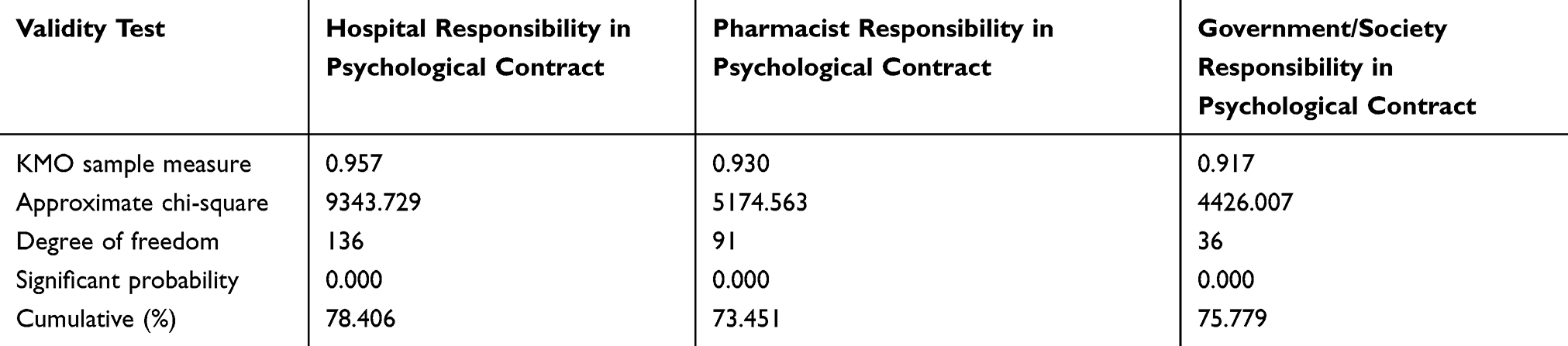 |
Table 2 KMO Measurement in Psychological Contract and Bartlett Spherical Test |
The factor load coefficients of a hospital, pharmacists, and government/society responsibility that pharmacists perceived were 0.515 to 0.839 (Table 3), 0.434 to 0.815 (Table 4) and 0.474 to 0.889 (Table 5), respectively, all greater than 0.4. The sub-scales of hospital and pharmacists’ responsibility both included four dimensions: transaction, development, cooperation, and concept responsibility. As shown in Table 3, items 1 to 4, items 5 to 9, items 10 to 12 and items 15 to 17 represent transaction, development, cooperation, and concept responsibility of the hospital perceived by pharmacists, respectively. Items 1 to 4, items 5 to 9, items 10 to 12 and items 15 to 17 in Table 4 represent transaction, development, cooperation, and concept responsibility of hospital pharmacists perceived by themselves, respectively. The sub-scale of government/society responsibility included two dimensions: government responsibility and society responsibility in pharmacists’ perception. Nomenclature and meaning of the factors are listed in Table 6.
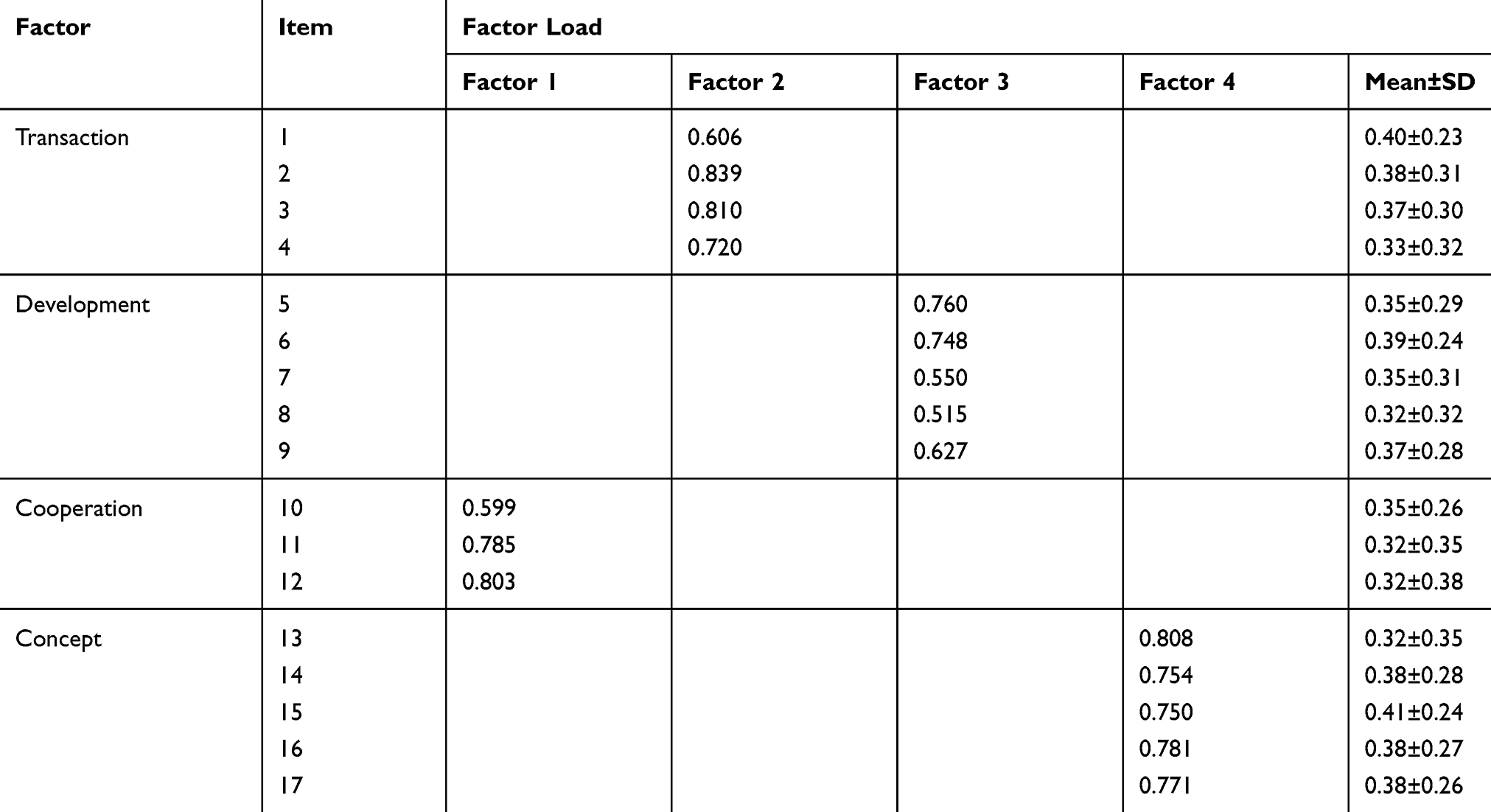 |
Table 3 Exploratory Factor Analysis of Hospital Responsibility in the Psychological Contract |
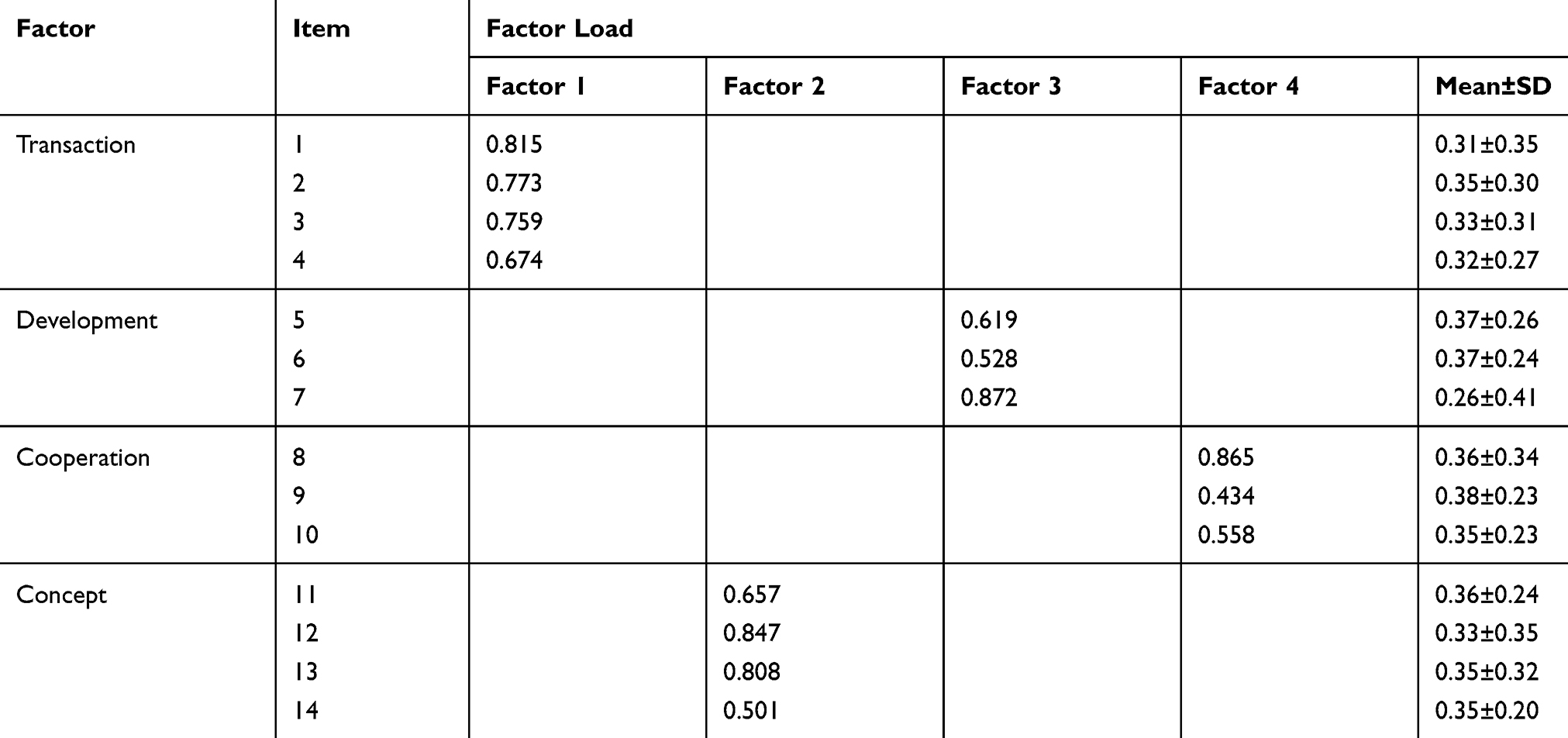 |
Table 4 Exploratory Factor Analysis of Pharmacists’ Responsibilities in the Psychological Contract |
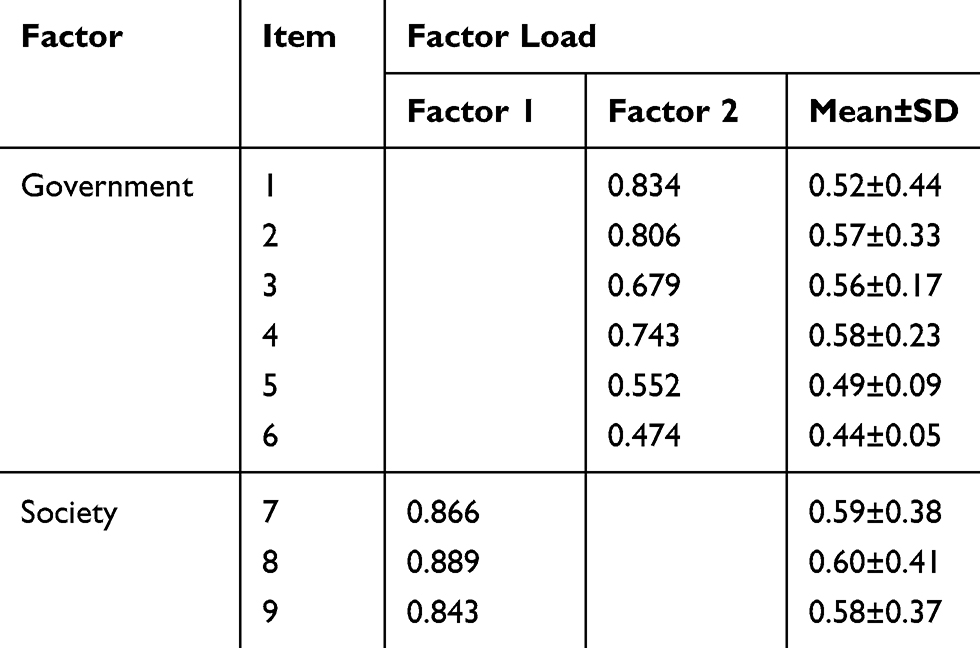 |
Table 5 Exploratory Factor Analysis of Government/Society Responsibilities in Psychological Contract |
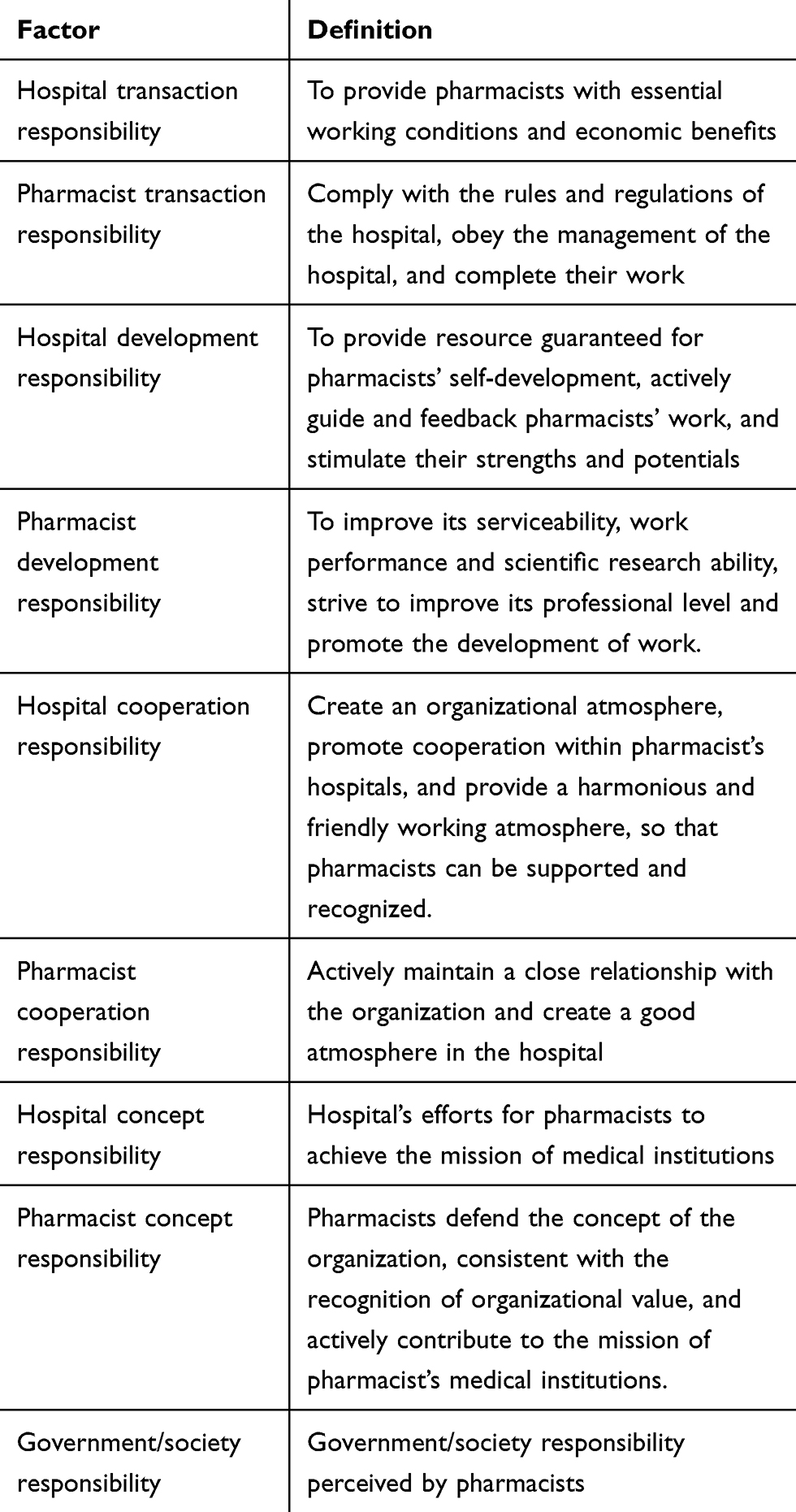 |
Table 6 Nomenclature and Meaning of Factors |
Taking the results mentioned above together, the contents of the questionnaire had good structural validity. This scale can be used to assess the psychological contract of hospital pharmacists.
Reliability Analysis
The results showed that the Cronbach’s alpha coefficient for hospital responsibility was 0.961, with half confidence of 0.924 and 0.951 (Table 7); the Cronbach’s alpha coefficient for pharmacists responsibility was 0.908, with half confidence of 0.823 and 0.882 (Table 8); and Cronbach’s alpha coefficient for government/society responsibility was 0.934, with half confidence of 0.879 and 0.932 (Table 9), indicating good internal consistency among items in the scale.
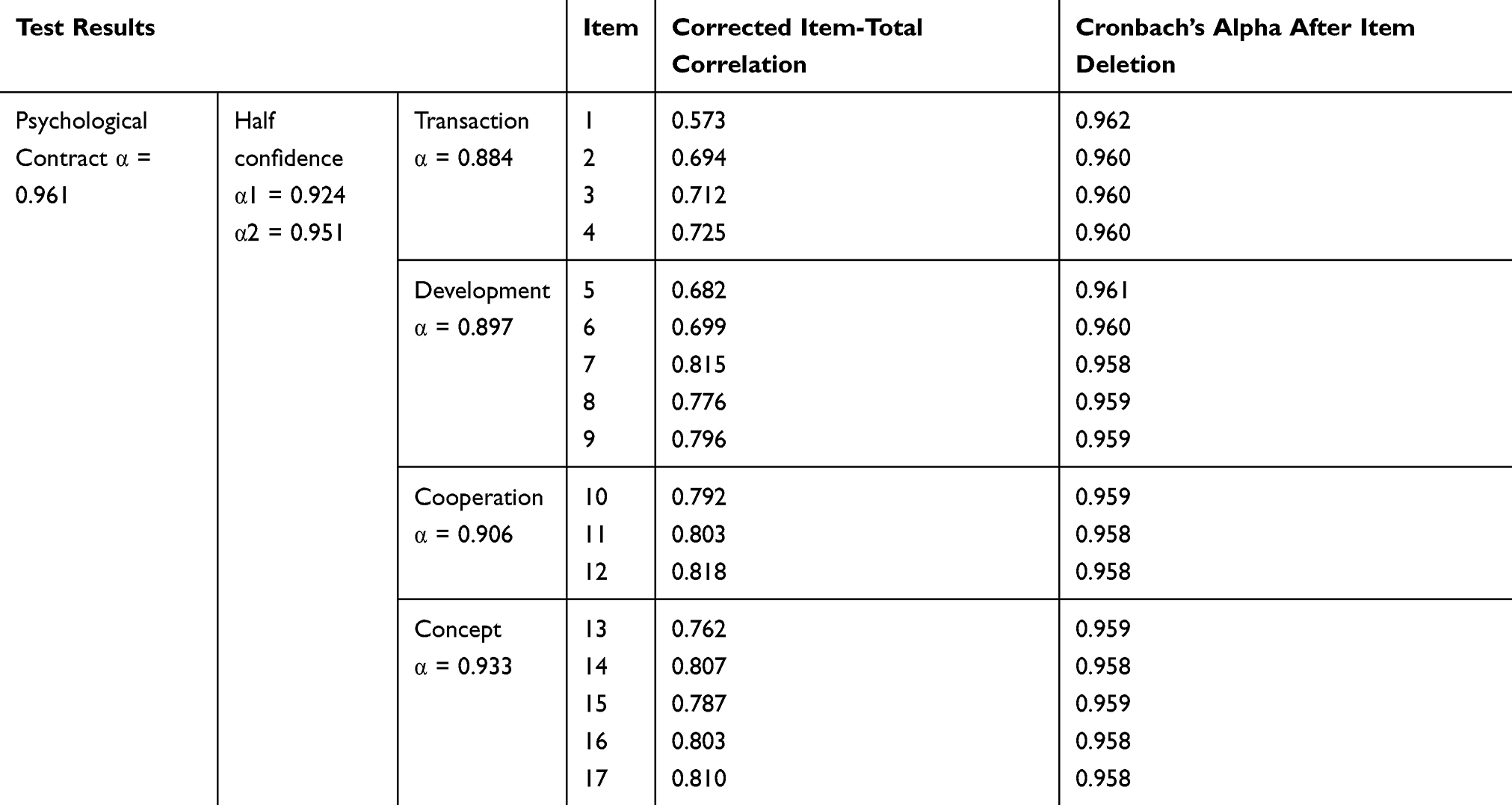 |
Table 7 Reliability Test for Hospital Responsibility in Psychological Contract |
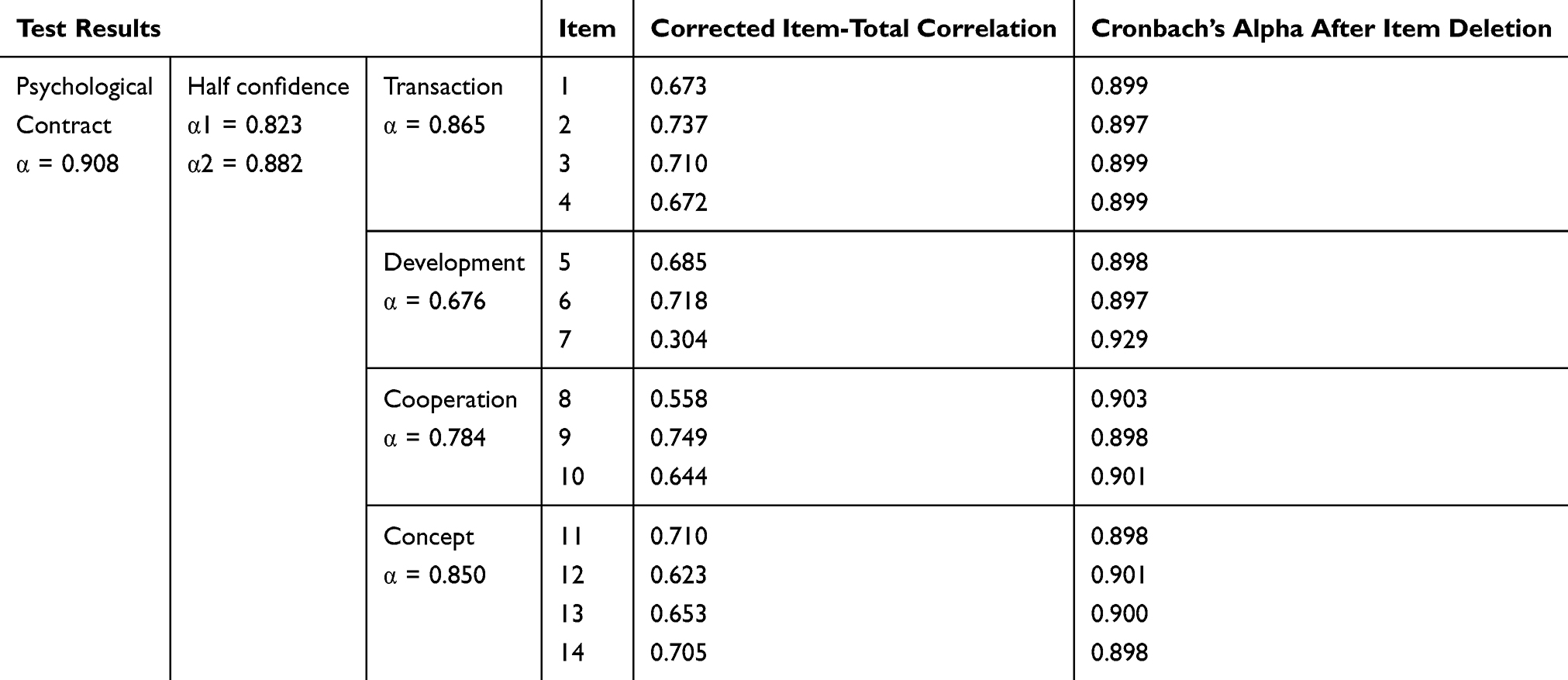 |
Table 8 Reliability Test for Pharmacists’ Responsibility in Psychological Contract |
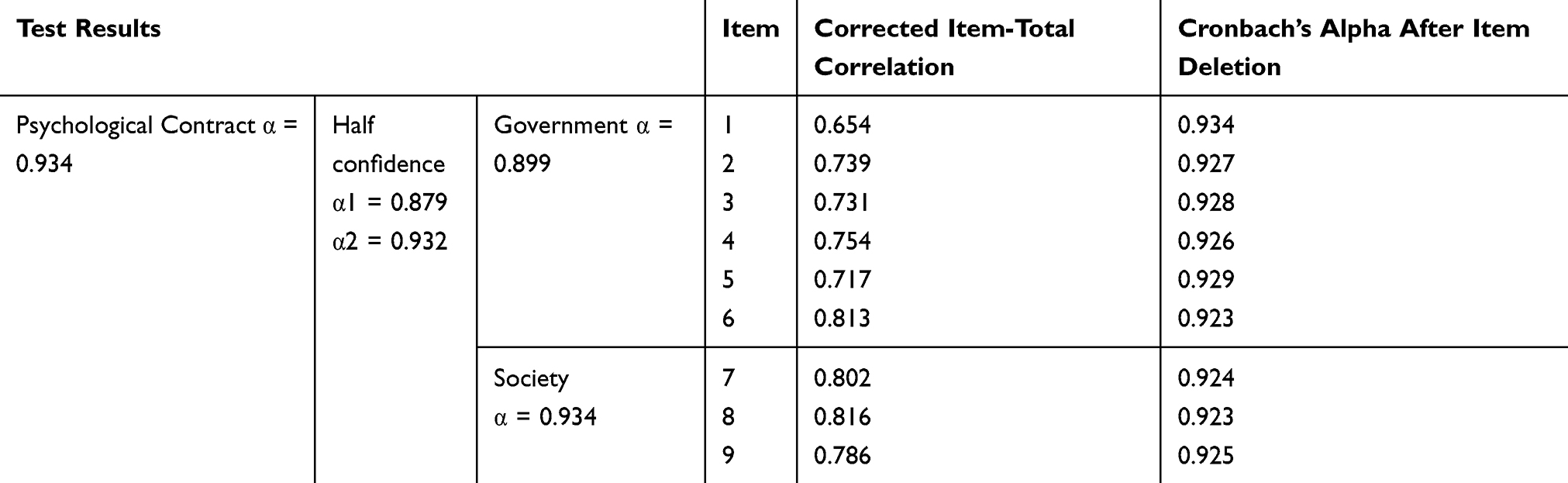 |
Table 9 Reliability Test for Government/Society Responsibility in Psychological Contract |
The Psychological Contract Scores of the Included Hospital Pharmacists
According to the questionnaire survey results, the average total score of psychological contract of the included pharmacists was 4.85±0.785 with the average scores of the pharmacist responsibility, the hospital responsibility and the government/society responsibility in the pharmacists’ perception of 5.42±0.637, 4.64±1.069 and 4.49±1.134, respectively. The score of the pharmacist responsibility was higher than those of the hospital responsibility and the government/society responsibility and differences between them were both statistically significant (P<0.01). In each dimension, the average score of the hospitals’ transaction, development, cooperation and concept responsibility was 4.91±1.046, 4.53±1.200, 4.71±1.231 and 4.48±1.250, respectively; the average score of the pharmacists’ transaction, development, cooperation and concept responsibility was 5.58±0.722, 4.96±0.976, 5.62±0.608 and 5.44±1.134, respectively; and the differences between scores of a corresponding dimension were all statistically significant (P<0.01).
Discussion
In many parts of the world, the importance of pharmacists in providing patient care has been emphasized with the new roles and responsibility patterns. Pharmacists have become active participants in primary health care, providing medication and chronic disease management services.32–34 The hospital pharmacists’ medication intervention on patients has been proved effective in reducing the incidence of irrational medication and adverse drug reactions in hospitals, improving the utilization of medical resources, and exerting a positive impact on the health of patients.19,20,35 Many studies have focused on the transformation of pharmacists from traditional practices to patient-centered care practices.36–38 However, despite these positive changes, many hospital pharmacists, especially in developing countries, are still ambiguous in their self-worth for the lack of clinical experience and recognition in their work.39 It has been shown that hospital pharmacists and their work were neglected because of the imperfection of hospital policy on pharmacist licensing, outdated management concepts, insufficient attention from hospital leaders, and lack of public awareness to hospital pharmacy.40 With the deepening of the medical system reform, the challenges facing hospital pharmacists are becoming increasingly complex. While we attach importance to the completion of work tasks and work quality, we need to understand the value of psychological fulfillment. Closer attention should be paid to the psychological needs of hospital pharmacists. Unfortunately, there has been no report on the professional management of hospital pharmacists based on the psychological contract within the scope of the literature we have reached. The current researches on the psychological contract of medical staff were almost all aimed at doctors or nurses.
Although not rigorous enough, our work is still a meaningful pioneering research attempt on the psychological contract of hospital pharmacists. The psychological contract scale for hospital pharmacists was designed according to the professional characteristics of hospital pharmacists in China by referring to the structure and some contents in similar scales used for doctors in public hospitals.27 The quality of the scale was improved through expert consultation and small sample investigation. The exploratory factor analysis and the internal consistency test showed that the psychological contract scale for hospital pharmacists had good reliability and validity. In addition, the factor load coefficients of the scale are all greater than 0.4; most of them greater than 0.7, indicating that the items can represent the related factors. The explanatory rates of the cumulative variance of the three sub-scales are all higher than 60%, indicating that the items of the scale were reliable. The selected hospitals involved multiple subtypes and levels of hospitals in Zunyi city, allowing a sufficient and representative sample size for Zunyi and similar cities. Based on empirical research, it is confirmed that the psychological contract scale for hospital pharmacists designed by this research has good reliability and validity. It provides a good tool for researchers and administrators in the hospital pharmacy area to conduct evaluation, maintenance and management of a hospital pharmacist psychological contract. Psychological contracts can provide a valid and reliable tool for hospital pharmacy management to understand the material and intangible needs of hospital pharmacists. Through these results, individualized management can be tailored to each hospital pharmacist for more effective management, improved occupational health and better performance.
From the comparison of scores the three subscales of the psychological contract scale of pharmacists at different levels of hospitals in Zunyi City included in this study, among the hospital responsibility, the pharmacist responsibility and government/society responsibility, the score of the pharmacist’s own responsibility was higher than the scores of hospital responsibility and the government/society responsibility. This indicates that the hospital pharmacists generally believe that they fulfill their responsibilities perceived by themselves to a high degree, and that hospitals and government/society have not fully fulfilled the responsibilities perceived by the hospital pharmacists compared to the contributions of the pharmacists. This result is basically consistent with the previous survey results for nurses and doctors.26,41,42 The persistence of this situation will lead to psychological contract problems and job burnout for the pharmacists. Among them, in terms of hospital responsibility, the score of conceptual responsibility is lower than those of other dimensions, indicating that the pharmacists are less satisfied with the hospital’s attention to the career planning and professional value of pharmacists. This may be related to the significant gap between hospital administrators and pharmacists in the understanding of the professional mission and philosophy of the hospital pharmacy; in terms of pharmacist’s responsibility, the scores of conceptual responsibility and development responsibility are lower than those of other dimensions, suggesting that the recognition and behavior of the hospital pharmacists on “defending the hospital mission and continuously improving their own abilities in scientific research and pharmaceutical service” need to be improved; in terms of government/society responsibility, the score of “giving pharmacists due social status and respect” is generally low, thus obtaining social recognition and enhancing self-worth are what pharmacists desire most.
Limitations and Considerations on Future Research
The content of psychological contract of hospital pharmacists in different regions may vary and change with time, thus, the scope of the sample should be expanded and more research may still be needed to improve the dimensions and/or items of the scale for future research. Since there is currently no research on scales related to pharmacist psychological contract, exploratory factor analysis is used to study the theory of internal structure first, and confirmatory structural analysis will be used for subsequent analysis in following research. In addition, because pharmacists working in hospitals of different levels may face different requirements and challenges, we will conduct separate studies for pharmacists working in hospitals of different levels and propose effective intervention plans for the hospital pharmacists’ psychological contract related issues.
Conclusion
The psychological contract scale for hospital pharmacists was developed and validated through literature research, expert consultation, small sample pre-investigation, repeated revisions and empirical research. With good reliability and validity, the scale can be used as a useful tool for researchers and administrators in the area related to hospital pharmacy management to objectively evaluate the quality of the psychological contract of hospital pharmacists. Hospital pharmacists generally believe that hospitals and government/society have not fully fulfilled the responsibilities perceived by the hospital pharmacists. The psychological contract of the hospital pharmacists needs certain timely maintenance and moderate intervention. Hospitals, governments, and relevant parties in society need to make effective efforts to enhance the social identity and professional value of hospital pharmacists.
Ethical Approval
The study was approved by the Medical Ethics Committee of Zunyi Medical University (ZMCER[2018]1-153). Through the explanation letter at the front of the questionnaire and the explanation work at the investigation site, all the pharmacists involved in the investigation clearly understood the purpose of the study. Participation in the study was voluntary and anonymous. Written informed consent was obtained.
Acknowledgments
The authors gratefully thank all hospital pharmacists who took part in the study. The authors would also like to acknowledge clinical pharmacist Jing Kong and Yan Yang at the First Hospital affiliated to Zunyi Medical University, China and Pharm. D, Specialized Residency in Geriatric Pharmacotherapy, clinical pharmacist Faith Mary Pranno at the Bergen Charity Hospital affiliated to Creighton University Medical Center, USA for their constructive comments helpful for improving the quality of the questionnaire and survey. The authors are especially grateful to Ph. D, associate professor Ping Zhou at Fudan University, China for her encouraging discussion with us and kind help in providing basic information about relevant research. The study was supported by Guizhou Provincial and Municipal Science and Technology Cooperation Special Project [No. 53, Provincial and Municipal Science and Technology Cooperation (2015)]; Funding for Key Discipline in Zunyi Medical University (4009403-0000014).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which the article will be submitted; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors have declared no potential conflicts of interest.
References
1. Rousseau DM. New hire perceptions of their own and their employer’s obligations: a study of psychological contracts. J Organ Behav. 1990;11(5):389–400. doi:10.1002/job.4030110506
2. Spies AR, Wilkin NE, Bentley JP, et al. Instrument to measure psychological contract violation in pharmacy students. Am J Pharm Educ. 2010;74(6):107. doi:10.5688/aj7406107
3. Scheine EH. Organizational Psychology. New Jersey: Prentice-Hall; 1980.
4. Farnese ML, Livi S, Barbieri B, et al. “You can see how things will end by the way they begin”: the contribution of early mutual obligations for the development of the psychological contract. Front Psychol. 2018;9:543. doi:10.3389/fpsyg.2018.00543
5. Griep Y, Vantilborgh T, Hansen SD, et al. Editorial: unraveling the role of time in psychological contract processes. Front Psychol. 2018;09:813. doi:10.3389/fpsyg.2018.00813
6. Trybou J, Maaike H, Elke H, et al. The mediating role of psychological contract violation between psychological contract breach and nurses’ organizational attitudes. Nurs Econ. 2016;34(6):296–302.
7. Trybou J, Gemmel P, Desmidt S, et al. Fulfillment of administrative and professional obligations of hospitals and mission motivation of physicians. BMC Health Serv Res. 2017;17(1):28. doi:10.1186/s12913-017-1990-0
8. Takase M, Teraoka S, Yabase K. Retaining the nursing workforce: factors contributing to the reduction of nurses’ turnover intention in Japan. J Nurs Manage. 2016;24(1):21–29. doi:10.1111/jonm.12266
9. Rodwell J, Ellershaw J. Fulfill promises and avoid breaches to retain satisfied, committed nurses. J Nurs Scholarship. 2016;48(4):406–413. doi:10.1111/jnu.12215
10. Jones SK, Griep Y. “I can only work so hard before I burn out.” a time sensitive conceptual integration of ideological psychological contract breach, work effort, and burnout. Front Psychol. 2018;9:131. doi:10.3389/fpsyg.2018.00131
11. Walker A. Outcomes associated with breach and fulfillment of the psychological contract of safety. J Safety Res. 2013;47:31–37. doi:10.1016/j.jsr.2013.08.008
12. Trybou J, De PK, Paeshuyse M, et al. The importance of social exchange to nurses and nurse assistants: impact on retention factors. J Nurs Manage. 2014;22(5):563–571. doi:10.1111/jonm.12039
13. Li S, Chen Y. The relationship between psychological contract breach and employees’ counterproductive work behaviors: the mediating effect of organizational cynicism and work alienation. Front Psychol. 2018;9:1273. doi:10.3389/fpsyg.2018.01273
14. Hofmans J. Modeling psychological contract violation using dual regime models: an event-based approach. Front Psychol. 2017;8:1948. doi:10.3389/fpsyg.2017.01948
15. Mccabe TJ, Sambrook S. Psychological contracts and commitment amongst nurses and nurse managers: A discourse analysis. Int J Nurs Stud. 2013;50(7):954–967. doi:10.1016/j.ijnurstu.2012.11.012
16. Gibbard K, Griep Y, Cooman RD, et al. One big happy family? Unraveling the relationship between shared perceptions of team psychological contracts, person-team fit and team performance. Front Psychol. 2017;8:1966. doi:10.3389/fpsyg.2017.01966
17. Corder E, Ronnie L. The role of the psychological contract in the motivation of nurses. Leadership in Health Ser. 2018;31(1):62–76. doi:10.1108/LHS-02-2017-0008
18. Guo H, Wu R, Yang H. Effect of rationally controlling the drug proportion under the intervention of clinical pharmacist. Chin J Hosp Pharm. 2019;39(1):84–86.
19. Martin P, Tamblyn R, Benedetti A, et al. Effect of a pharmacist-led educational intervention on inappropriate medication prescriptions in older adults: the D-PRESCRIBE randomized clinical trial. JAMA. 2018;320(18):1889–1898. doi:10.1001/jama.2018.16131
20. Al-Hashar A, Al-Zakwani I, Eriksson T, et al. Impact of medication reconciliation and review and counselling, on adverse drug events and healthcare resource use. Int J Clin Pharm. 2018;40(5):1154–1164. doi:10.1007/s11096-018-0650-8
21. Abdulsalim S, Unnikrishnan MK, Manu MK, et al. Structured pharmacist-led intervention programme to improve medication adherence in COPD patients: A randomized controlled study. Res Social Adm Pharm. 2018;14(10):909–914. doi:10.1016/j.sapharm.2017.10.008
22. Zhang J, Yin CC, Li HF, et al. Application of once-monthly self-reported ACT questionnaire in management of adherence to Inhalers in outpatients with asthma. Patient Prefer Adher. 2020;14:1027–1036. doi:10.2147/PPA.S176683
23. Mu XR, Yin CC, He X, et al. Correlation between patients’ medication adherence and their psychological contract with hospital pharmacists. Patient Prefer Adher. 2020;14:1605–1613. doi:10.2147/PPA.S264026
24. Guo BM, Zhu AF. The relationship among psychological capital psychological contract and work engagement in nurses. Chin J Ind Hyg Occup Dis. 2018;36(8):614–617. doi:10.3760/cma.j.issn.1001-9391.2018.08.013
25. Bai F, Shi JW, Zhou P, et al. Analysis on the evaluation of public hospital physicians on fulfillment of their own responsibilities. Chin Hosp Manage. 2016;36(3):25–27.
26. Zhang Y, Zhou P, Shi JW, et al. Study on the evaluation of public hospital physicians on fulfillment of hospital responsibilities. Chin Hosp Manage. 2016;36(3):22–24.
27. Shi JW, Zhou P, Xue D, et al. Research on the scale for psychological contract of physicians in public hospitals. Chin Hosp Manage. 2016;36(3):19–21.
28. Guo X, Wu X, Guo A, et al. Reliability and validity of the Chinese CECA10 questionnaire for Chinese patients with condyloma acuminata. Medicine. 2018;97(9):e9917. doi:10.1097/MD.0000000000009917
29. Quach CW, Langer MM, Chen RC, et al. Reliability and validity of PROMIS measures administered by telephone interview in a longitudinal localized prostate cancer study. Qual Life Res. 2016;25(11):2811–2823. doi:10.1007/s11136-016-1325-3
30. Ark MV, Zwerver J, Diercks RL, et al. Cross-cultural adaptation and reliability and validity of the Dutch Patient-Rated Tennis Elbow Evaluation (PRTEE-D). BMC Musculoskel Dis. 2014;15(1):270. doi:10.1186/1471-2474-15-270
31. Wu SF. Rapid screening of psychological well-being of patients with chronic illness: reliability and validity test on WHO-5 and PHQ-9 scales. Depress Res Treat. 2014;2014:239490. doi:10.1155/2014/239490
32. Ramalho de Oliveira D, Brummel AR, Miller DB. Medication therapy management: 10 years of experience in a large integrated health care system. J Manage Care Pharm. 2010;16(3):185–195. doi:10.18553/jmcp.2010.16.3.185
33. Manolakis PG, Skelton JB. Pharmacists’ contributions to primary care in the United States collaborating to address unmet patient care needs: the emerging role for pharmacists to address the shortage of primary care providers. Am J Pharm Educ. 2010;74(10):S7. doi:10.5688/aj7410s7
34. Mossialos E, Courtin E, Naci H, et al. From “retailers” to health care providers: transforming the role of community pharmacists in chronic disease management. Health Policy (New York). 2015;119(5):628–639. doi:10.1016/j.healthpol.2015.02.007
35. Mekonnen AB, McLachlan AJ, Brien JA. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysis. BMJ Open. 2016;6(2):e010003. doi:10.1136/bmjopen-2015-010003
36. Grindrod KA, Marra CA, Colley L, et al. Pharmacists’ preferences for providing patient-centered services: a discrete choice experiment to guide health policy. Ann Pharmacother. 2010;44(10):1554–1564. doi:10.1345/aph.1P228
37. Scott A, Bond C, Inch J, et al. Preferences of community pharmacists for extended roles in primary care: a survey and discrete choice experiment. Pharmacoeconomics. 2007;25(9):783–792. doi:10.2165/00019053-200725090-00006
38. Kahan M, Wilson L, Wenghofer EF, et al. Pharmacists’ experiences with dispensing opioids: provincial survey. Can Fam Physician. 2011;57(11):e448–e454.
39. He Y, Yang F, Mu D, et al. Examination of psychosocial predictors of Chinese hospital pharmacists’ intention to provide clinical pharmacy services using the theory of planned behaviour: a cross-sectional questionnaire study. BMJ Open. 2016;6(10):e012775. doi:10.1136/bmjopen-2016-012775
40. Löffler C, Koudmani C, Böhmer F, et al. Perceptions of interprofessional collaboration of general practitioners and community pharmacists - a qualitative study. BMC Health Serv Res. 2017;17(1):224. doi:10.1186/s12913-017-2157-8
41. Xu Y, Wu XJ. Research status and application of nursing staff’s psychological contract. Chin J Nurs. 2012;47(5):476–478.
42. Zhang Y, Zhou P, Shi JW, et al. Study on the evaluation of public hospital physicians on fulfillment of government and social responsibilities. Chin Hosp Manage. 2016;36(3):28–30.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.