")
Back to Journals » Cancer Management and Research » Volume 12
Development and Validation of a Prognostic Nomogram to Predict the Long-Time Prognosis in Non-B, Non-C Hepatocellular Carcinoma
Authors Lin K , Huang Q , Huo Y, Zeng J, Ding Z, Guo P, Chen Z, Zeng Y, Liu J
Received 5 April 2020
Accepted for publication 5 August 2020
Published 24 August 2020 Volume 2020:12 Pages 7771—7781
DOI https://doi.org/10.2147/CMAR.S257016
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Beicheng Sun
Kongying Lin,1,* Qizhen Huang,2,* Yuting Huo,3,* Jianxing Zeng,1 Zongren Ding,1 Pengfei Guo,4 Zhenwei Chen,4 Yongyi Zeng,1 Jingfeng Liu1,4
1Department of Hepatopancreatobiliary Surgery, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou 350025, People’s Republic of China; 2Department of Radiation Oncology, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou 350025, People’s Republic of China; 3Department of Otolaryngology, Fujian Medical Maternity and Child Care Hospital, Fuzhou 350014, People’s Republic of China; 4The Big Data Institute of Southeast Hepatobiliary Health Information, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou 350025, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingfeng Liu; Yongyi Zeng
Department of Hepatopancreatobiliary Surgery, Mengchao Hepatobiliary Hospital of Fujian Medical University, Xihong Road 312, Fuzhou 350025, People’s Republic of China
Tel/ Fax +86 591 8370 5927
Email [email protected]; [email protected]
Purpose: To develop and validate a nomogram for individualized prediction of the long-term prognosis of patients with non-B, non-C hepatocellular carcinoma (NBNC-HCC) who underwent hepatectomy.
Materials and Methods: Five hundred ninety-four patients who met the criteria were included in the research and randomly categorized into the training or validation cohort. The nomogram was constructed on the basis of the independent risk variables that were acquired via multivariate Cox proportional hazard regression analysis. Several complementary methods included the Harrell c-index, time-dependent areas under the receiver operating characteristic curve (tdAUC), and calibration plot, and the Kaplan–Meier curve with Log rank test were used to test predictive performance of the model. The clinical utility of the model was tested by the decision cure analysis (DCA).
Results: Tumor diameter, tumor number, elevated serum gamma-glutamyl transpeptidase (GGT) level, microvascular invasion (MVI), and macrovascular invasion were independent risk factors of prognosis of NBNC-HCC. C-indexes of the nomogram were 0.702 (95% confidence interval [CI], 0.662– 0.741) in the training cohort and 0.700 (95% CI, 0.643– 0.758) in the validation cohort, and median tdAUC values of the nomogram were 0.743 (range, 0.736– 0.775) in the training cohort and 0.751 (range, 0.686– 0.793) in the validation cohort, which were both higher than those in the conventionally used Barcelona Clinic Liver Cancer staging system, American Joint Committee on Cancer, and eighth edition and the model of Zhang et al. The calibration plot depicted a good consistency between prediction of the model and observed outcome. The Kaplan–Meier curve analysis showed that the model was able to separate patients into three distinct risk subgroups. The DCA analysis also demonstrated that the nomogram was clinically useful.
Conclusion: We developed and validated a nomogram that was accurate and clinically useful in patients with NBNC-HCC who underwent hepatectomy.
Keywords: non-B non-C hepatocellular carcinoma, resection, prognosis, nomogram, survival
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common malignant tumor and the fourth cause of cancer-associated deaths globally.1 Hepatitis B virus (HBV) and hepatitis C virus (HCV) infection are the main causes of HCC.2 However, with the change of lifestyle, popularity of hepatitis B vaccines, and clinical use of effective antiviral drugs, the incidence of virus-related HCC is decreasing gradually3,4 and accompanied with an increase of non-viral HCC, also known as non-B, non-C HCC (NBNC-HCC).5,6
As with viral-associated HCC, surgical resection remains the main treatment that can provide long-term prognosis in NBNC-HCC.7 Yet, the long-term outcome in NBNC-HCC postoperatively is still not satisfactory. In previous studies, the 5-year overall survival (OS) rate in NBNC-HCC has been reported as only 42.6%-48.8%.8,9 Because of the heterogeneous nature of HCC, accurate prediction of prognosis after treatment is of great significance. A good individualized prognostic prediction model may benefit some highly selected patients through well-selected therapeutic assignment.10,11
Currently, there are several widely used HCC staging systems such as the Barcelona Clinic Liver Cancer staging system (BCLC)12 and American Joint Committee on Cancer staging system, eight edition (AJCC8th),13 which have important guiding significance for prognosis. However, they fail to achieve individualized prognostic prediction, so even with the same treatment, patients within the same stage of HCC tend to have different outcomes. In addition, these staging systems were not specifically constructed for patients with NBNC-HCC. As an individualized predictive tool to predict the prognosis of patients, a nomogram has been used and validated in various tumors in recent years.14–16 The nomogram developed by Zhang et al17 was developed specifically for prognostic prediction in patients with NBNC-HCC who underwent hepatectomy, but the model was not validated in their study.
Therefore, this study aimed to construct a nomogram for individualized prediction in patients with NBNC-HCC after resection and validate its predictive performance through several complementary methods in order to determine whether the model can predict prognosis more accurately than other models.
Materials and Methods
Ethical Statements
The study was conducted in accordance with the 1975 Declaration of Helsinki. Written informed consent was obtained from all study patients. The institutional research ethics committee of Mengchao Hepatobiliary Hospital of Fujian Medical University approved the study (approval number: 2019_049_01).
Patient Selection
Data of patients who underwent hepatectomy as their primary anti-cancer therapy for HCC between August 21, 2008 and December 31, 2014 were identified and collected through primary liver cancer big data. Patients who met all of the following criteria were included in the research for further statistical analysis: (1) patients with NBNC-HCC, defined as seronegative for the hepatitis B surface antigen, HBV-DNA, hepatitis C antibody, and HCV-RNA test;6 (2) those with liver function of Child-Pugh class A/B7; (3) those who underwent R0 resection (removal of all detectable tumor nodes and negative surgical margin in postoperative pathological examination); (4) those without extrahepatic metastasis; (5) those without a medical history of other malignancy; and (6) those with complete clinical and follow-up data. All data were verified by three independent researchers.
Diagnosis and Hepatectomy
Routine preoperative assessments of patients included liver, renal, and cardiopulmonary function tests, alpha fetoprotein (AFP) analysis, hepatitis B/C immunology, and imaging examination. Imaging examination included radiography or computed tomography (CT) scan of the chest, abdominal ultrasonography, contrast-enhanced CT, or magnetic resonance (MRI). The diagnosis of HCC was determined by the appearance of typical radiological features on contrast-enhanced MRI, CT, or abdominal ultrasonography and confirmed by postoperative pathological examination. The use of anatomical or partial hepatectomy depended on the tumor variables, such as the diameter, number, and location and patient’s liver function status. Intraoperative ultrasonography was routinely performed to ensure that all detectable tumor nodes were removed. The removal of three or more Couinaud segments intraoperatively was regarded as major liver resection.18
Follow-Up
All patients were followed up regularly in the outpatient department after discharge. The interval of follow-up was about every 2 months during the first 2 years and every 6 months thereafter. The routine follow-up assessments included abdominal ultrasonography and laboratory examination of variables, such as liver function and the serum AFP level. When recurrence was highly suspected in patients on the basis of findings, such as an abnormal ultrasonography result or continuously elevated AFP level, contrast-enhanced CT or MRI was routinely performed. When tumor recurrence was diagnosed, appropriate treatments, which were based on the basic condition, reserved liver function, and tumor recurrence pattern of each patient, were prescribed according to the advice of the multidisciplinary team.
Outcome Measure
The end-point in this research study was OS, which was defined as the interval between the date of resection and the date of either death or the last follow-up.
Statistical Analysis
Continuous variables are expressed as mean (standard deviation), and they were compared using the Student’s t-test or Mann–Whitney U-test. Categorical variables are expressed as number (percentage), and they were compared using the chi-square test or Fisher exact test. Univariate and multivariate Cox proportional hazard regression analyses of the training cohort were performed to acquire the independent risk factor for OS. The statistically significant (p<0.05) variables in the univariate Cox regression analysis were chosen for further multivariate Cox regression analysis via the stepwise backward selection method. The nomogram was constructed on the basis of the independent risk factors of OS using the R package “rms” (Institute for Statistics and Mathematics, Vienna, Austria).
Predictive performance of the nomogram model was verified through discrimination and calibration.19 The discriminative ability of the nomogram was analyzed by the Harrell c-index and time-dependent areas under the receiver operating characteristic curve (tdAUC).10 Calibration of the nomogram was analyzed by using the calibration plot. Clinical utility of the nomogram was tested via the decision cure analysis (DCA).20 Kaplan–Meier curves and the Log rank test for risk groups were further applied to measure the performance of the nomogram, and risk groups were generated by the previously reported cut-off values (50th and 85th percentiles) of the total points assessed using the nomogram.21
All the statistical tests were two-sided, and a p<0.05 was regarded as statistically significant. SPSS, version 20 (IBM Corp., Armonk, NY, USA) and R, version 3.5.2 (R packages “rms”, “CsChange”, “timeROC”, and “stdca”) were used to perform all statistical analyses in the study.
Results
Baseline Characteristics and Prognosis of Patients
According to the study’s inclusion criteria, 594 patients were enrolled and randomly categorized into the training cohort (n=396) or validation cohort (n=198) in a 2:1 ratio. The detailed flowchart for patient collection is shown in Figure S1. The baseline characteristics of the whole cohort and a comparison between the training and validation cohorts are shown in Table 1. Overall, non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD) were diagnosed in 6.9% and 9.4% of patients, respectively, and most patients (83.0%) were diagnosed with cryptogenic HCC. Most patients were male (87.2%); 26.8% of patients were diagnosed with hypertension, and 15.3% of patients had diabetes. Most patients had a solitary tumor node (83.8%), and the mean diameter of the tumor node was 7.39 ± 4.22 cm. According to the HCC staging system, 72.6% of patients remained BCLC A stage, and 56.4% of patients were classified as AJCC8th IB stage.
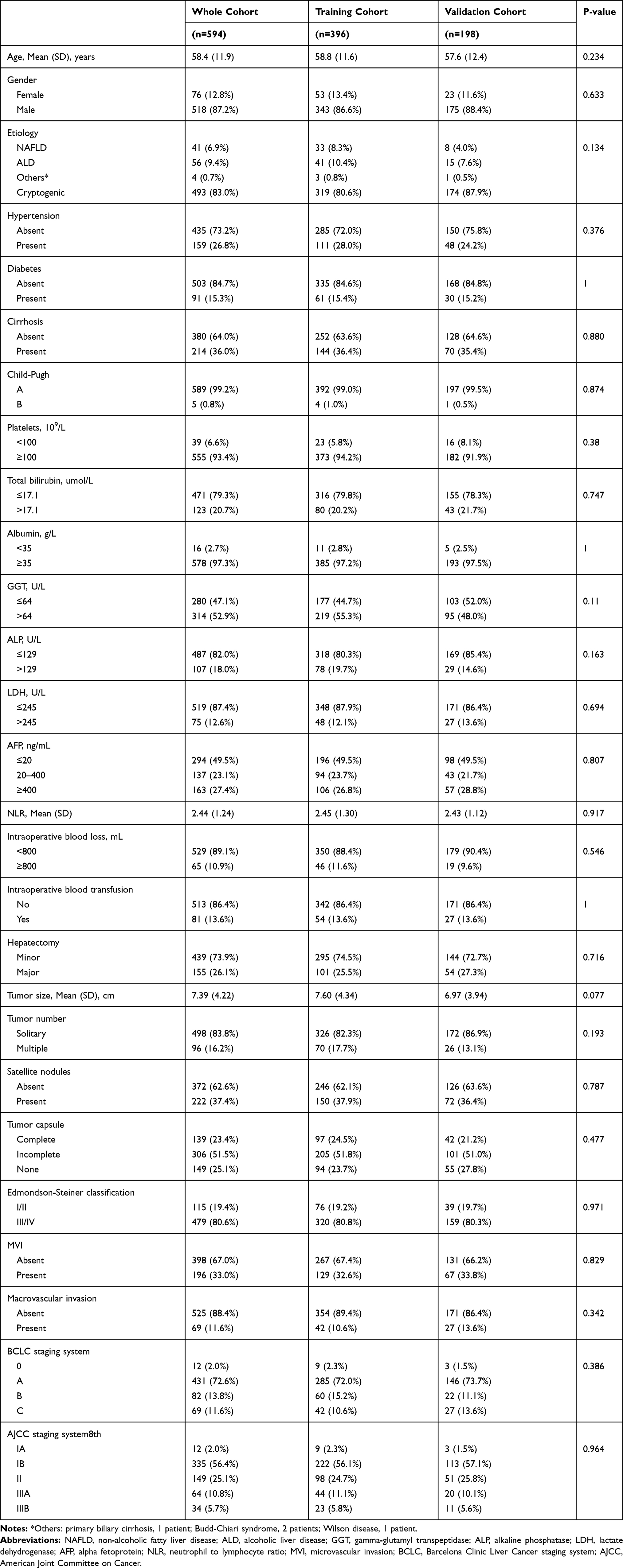 |
Table 1 Baseline Clinical Characteristics of Patients with NBNC-HCC |
The median follow-up times of patients were 59.2 months and 59.4 months in the training and validation cohorts, respectively. The 1-, 2-, 3-, 4-, and 5-year OS rates were 86.3%, 77.3%, 68.5%, 58.5%, and 50.8% in the training cohort and 84.0%, 76.3%, 69.3%, 61.2%, and 52.3% in the validation cohort, respectively.
Risk Factors for OS and Construction of the Nomogram
Results of the univariate and multivariate Cox proportional hazard regression analyses are shown in Tables 2 and 3. Multivariate analysis showed that five variables were independent risk factors of OS: large tumor diameter (p=0.015, hazard ratio [95% confidence interval]=1.042 [1.008–1.078]), multiple tumor nodes (p=0.003, 1.656 [1.184–2.315]), high preoperative serum GGT level (p=0.009, 1.517 [1.109–2.074]), presence of microvascular invasion (p=0.007, 1.593 [1.135–2.234]), and macrovascular invasion (p<0.001, 2.954 [1.937–4.505]) (Table 3). On the basis of these independent risk factors, a nomogram for predicting OS was constructed and verified in the training and validation cohorts (Figure 1).
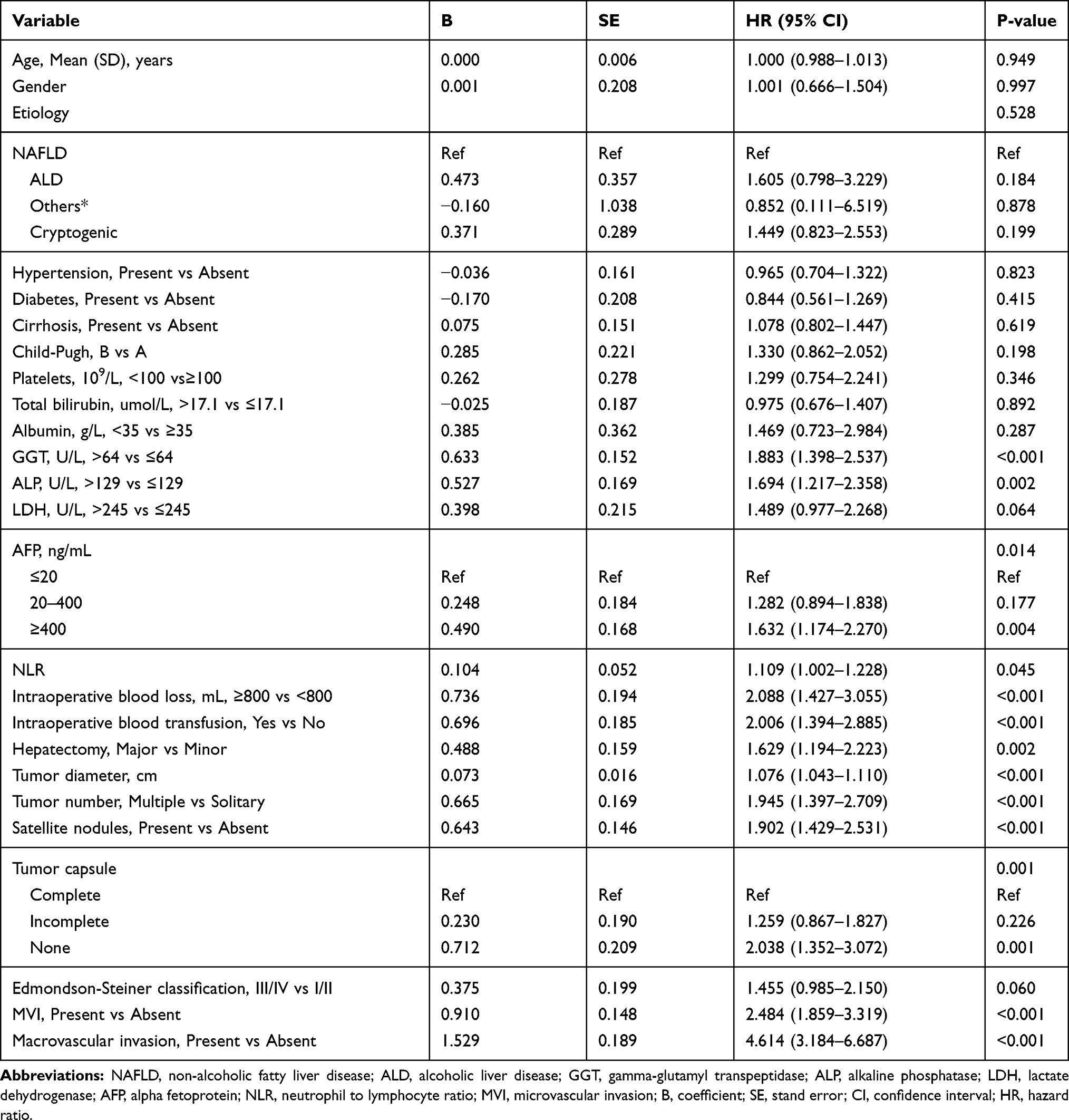 |
Table 2 Univariate Cox Regression Analysis of OS in the Training Cohort |
 |
Table 3 Multivariate Cox Regression Analysis of OS in the Training Cohort |
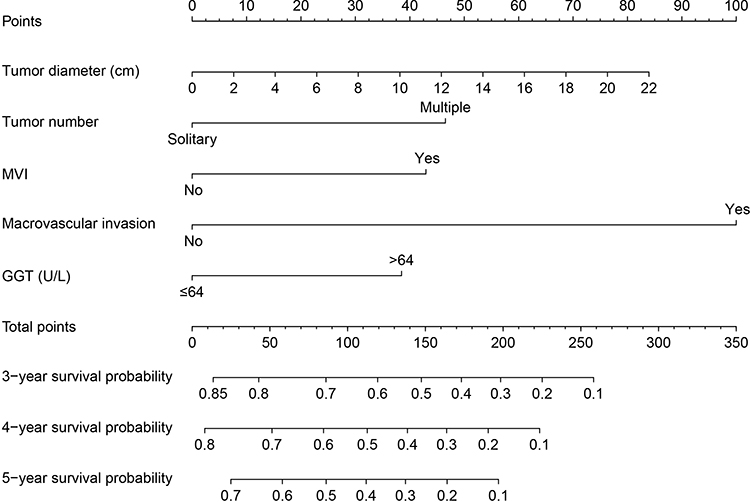 |
Figure 1 Nomogram for prognostic prediction in patients with non-B, non-C hepatocellular carcinoma who underwent hepatectomy. |
Predictive Performance of the Nomogram
C-indexes of the nomogram model reached 0.702 (95% confidence interval [CI], 0.662–0.741) in the training cohort and 0.700 (95% CI, 0.643–0.758) in the validation cohort, which were higher than those of the BCLC staging system (0.636, 95% CI 0.599–0.672, p<0.001; 0.626, 95% CI 0.572–0.680, p<0.001), AJCC8th staging system (0.658, 95% CI 0.620–0.695, p=0.002; 0.641, 95% CI 0.588–0.694, p=0.006), and Zhang et al’s model (0.658, 95% CI 0.618–0.698, p=0.003; 0.642, 95% CI 0.577–0.706, p=0.029).
The time-dependent AUC analysis also showed that the nomogram model had better discrimination than the other prognostic models (Figure 2A and B). Median tdAUC values of the nomogram were 0.743 (range, 0.736–0.775) in the training cohort and 0.751 (range, 0.686–0.793) in the validation cohort at various time points. Details of tdAUC values of the models are shown in Table S1.
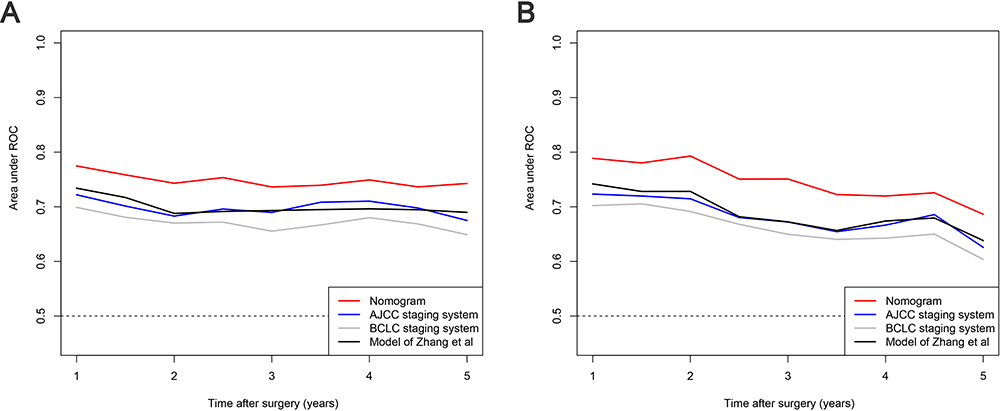 |
Figure 2 Comparisons of the time-dependent area under the curve between the nomogram and other models at various time points in the training (A) and validation (B) cohorts. |
For calibration of the nomogram, calibration plots depicted a good consistency between the predicted outcome of the nomogram and the observed outcome in terms of 3-, 4-, and 5-year OS in the training and validation cohorts (Figure 3A and B).
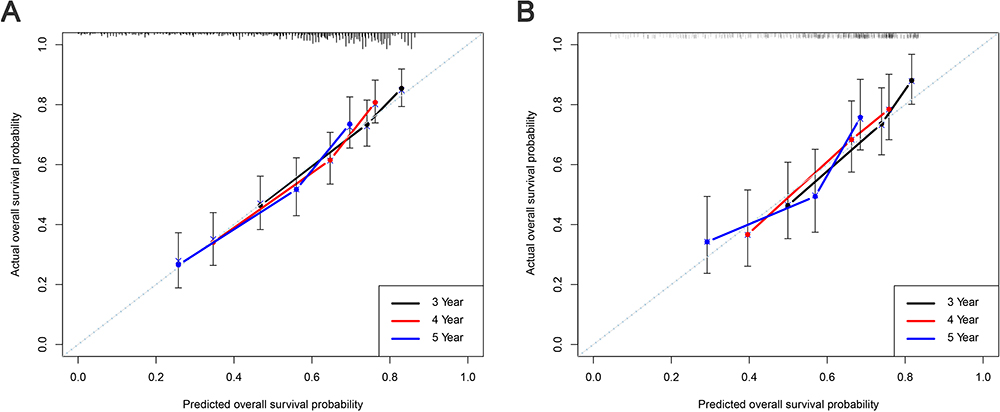 |
Figure 3 Calibration curves for predicting the 3-, 4-, and 5-year overall survival in the training (A) and validation cohorts (B). |
In addition, with the nomogram, each patient received a corresponding total point. Median total points were 66.0 (range, 3.8–311.4) in the training cohort and 61.2 (range, 6.1–258.7) in the validation cohort. Values of 66.0 and 146.4 points, which represent the 50th and 85th percentiles of the total points in the training cohort, were used to categorize the patients into three different risk subgroups (low, intermediate, and high risk). The Kaplan–Meier analysis showed that the three survival curves were widely separated in the training and validation cohorts (both p<0.001), which further indicated the good predictive performance of the nomogram model (Figure 4A and B).
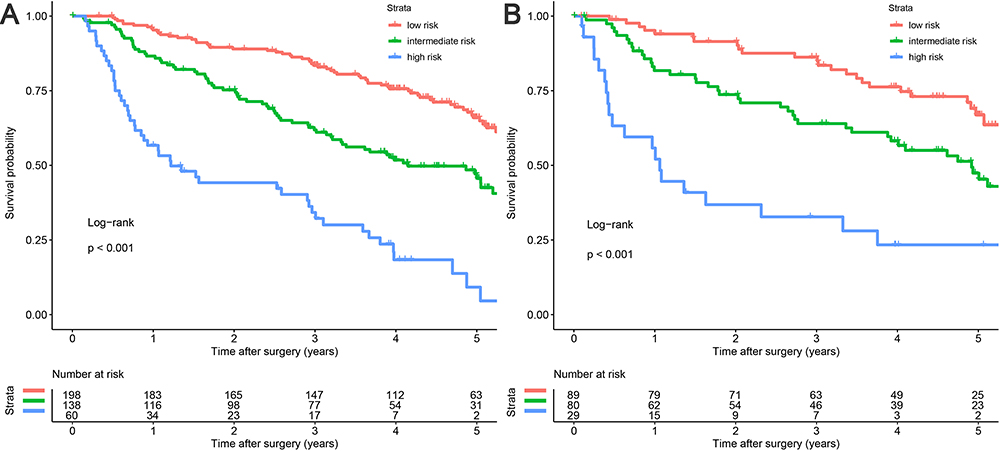 |
Figure 4 Kaplan–Meier plots for overall survival rates of risk groups defined by the nomogram model points. (A) Training cohort, (B) validation cohort. |
Clinical Utility of the Nomogram
DCA was performed to measure the clinical utility of the model. DCA consisted of the continuous risk of the probability threshold (x-axis) and the net benefit (y-axis), which graphically demonstrated the model’s clinical utility. As shown in Figure 5A and B, DCA revealed that the nomogram had better net benefits than the BCLC staging system, AJCC8th staging system, and Zhang et al’s model in the training and validation cohorts.
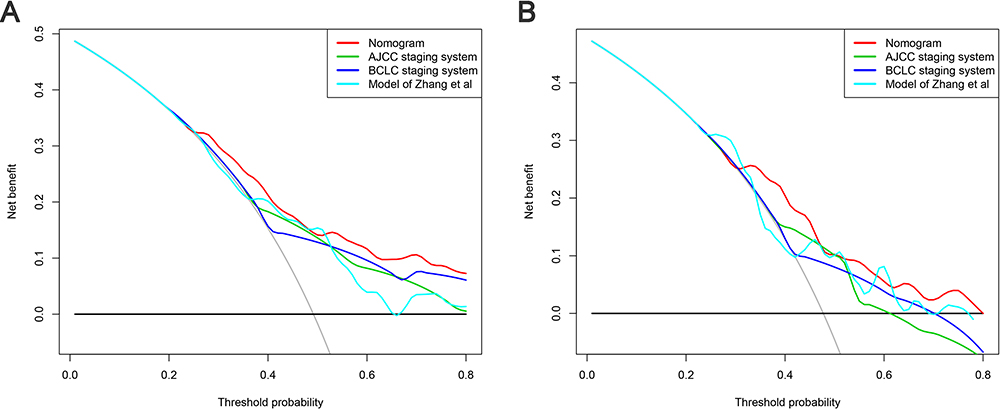 |
Figure 5 Decision curve analysis comparing the prognostic nomogram to other models in predicting 5-year overall survival. (A) Training cohort, (B) validation cohort. |
Discussion
Because of different pathogenic mechanisms of hepatocarcinogenesis between virus-associated HCC and NBNC-HCC, the clinicopathologic features, especially tumor characteristics, of patients are very different between the two cancers. For instance, compared to patients with virus-associated HCC, those with NBNC-HCC tend to have a larger tumor diameter, solitary tumor node, and fewer vascular invasion events.6,8 Although the conventionally used BCLC stage and AJCC8th staging systems integrate the tumor-associated variables, such as the number of tumor nodes, tumor diameter, and vascular invasion, they do not consider that these factors are very different in HCC with a different etiology; thus, for patients with NBNC-HCC, they cannot achieve good predictive performance. In addition, none of these models includes the clinical serum biomarker, and this may be one reason why their prediction efficiency is poor. Furthermore, these staging systems cannot achieve individualized prognostic prediction.
In the present study, we analyzed the independent risk factors for the prognosis of NBNC-HCC and constructed a prognostic nomogram model. The results showed that the predictive performance of the model was satisfactory, which was verified by various methodologies. Further, the tdAUC analysis confirmed the aforementioned results. In addition, the DCA curve analysis displayed the superior net benefit of the nomogram compared to the other models. Compared with the Zhang et al’s study, our study included patients from 2008 to 2014, which ensured that patients received a long enough follow-up for the observation of outcome at 4 and 5 years after resection. This factor may be the reason for the better accuracy of our model in the prediction of long-time prognosis in patients with NBNC-HCC.
According to each individualized total point given by the nomogram model, we were able to divide patients into three different risk subgroups (high, intermediate, and low risk). For the whole cohort, the high-risk subgroup consisted of 15.7% of patients, with only a 5-year OS rate of 14.3%, whereas the low and intermediate risk subgroups accounted for 51.9% and 32.5 of patients, with 5-year OS rates of 66.1% and 44.3%, respectively. This easy-to-apply graphical model can be an additional tool for clinicians to make individual predictions of patients’ prognosis and identify high-risk patients among those with NBNC-HCC, which may be valuable in guiding corresponding follow-up strategies and postoperative adjuvant therapy.
Tumor diameter, multiple tumor nodes, vascular invasion and elevated serum GGT level were identified as the independent unfavorable factors of NBNC-HCC in this study. The effects of tumor diameter, multiple tumor nodes, and vascular invasion, which are relevant to aggressive behavior of a tumor, on the prognosis of HCC have been reported in many previous literatures.6,9,22–25 In addition, several studies demonstrated the unfavorable effect of these factors in NBNC-HCC,9,22 which is consistent with our results. GGT, a cost-effective and easily accessible serum biomarker, has been reported to have diagnostic and prognostic effects in various malignancies.26,27 The possible mechanisms of GGT in HCC are as follows: (1) a high level GGT may induce DNA instability and result in tumor formation; and (2) the GGT level may be related to the aggressive behavior of HCC, such as poor differentiation, vascular invasion, or metastasis of tumor cells.28–30 Li et al8 also demonstrated the unfavorable association between the elevated GGT level and prognosis of NBNC-HCC. These studies may support our clinical findings. However, the exact mechanism of the association between GGT and survival of NBNC-HCC remains unclear and requires elucidation.
It is worth noting that 83% of the patients in the present cohort had cryptogenic HCC. The risk factors of NBNC-HCC include NAFLD/non-alcoholic steatohepatitis (NASH), ALD, aflatoxin infection, and aristolochic acid intake.2 Therefore, cryptogenic HCC in some of these patients may be caused by aflatoxin infection or aristolochic acid intake. Besides, NAFLD/NASH and ALD are mainly related to diet and lifestyle. The diet and lifestyle of Chinese individuals are different from those of western developed countries, which may be the reason why the proportion of NAFLD/NASH- and ALD-related HCC in our cohort differs from that in the western world.31 Currently, there are no data recording the contributions of ALD and NAFLD/NASH to HCC in China, although these entities will likely become leading causes of HCC in the future, and they deserve further exploration.32
There are several limitations to our study. Firstly, the nomogram model was constructed using retrospective data; therefore, the results need to be further validated in prospective studies. Secondly, the etiology of most patients included in the present study was cryptogenic; considering regional disparity of etiology of NBNC-HCC, multicenter cohorts are necessary to validate the predictive performance of the nomogram. Lastly, the present study included only the patients who underwent resection, so the nomogram may not be suitable for patients who underwent other treatments.
Conclusions
In summary, we developed and validated a prognostic nomogram for individualized prediction in patients with NBNC-HCC who underwent resection. This novel nomogram model may provide clinicians with useful guidance for postoperative follow-up and treatments.
Abbreviations
NBNC-HCC, non-B non-C hepatocellular carcinoma; NAFLD, non-alcoholic fatty liver disease; ALD, alcoholic liver disease; GGT, gamma-glutamyl transpeptidase; ALP, alkaline phosphatase; LDH, lactate dehydrogenase; AFP, alpha fetoprotein; NLR, neutrophil to lymphocyte ratio; MVI, microvascular invasion; BCLC, Barcelona Clinic Liver Cancer staging system; AJCC, American Joint Committee on Cancer; OS, overall survival.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Yang JD, Hainaut P, Gores GJ, et al. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–604. doi:10.1038/s41575-019-0186-y
3. Bosetti C, Levi F, Boffetta P, et al. Trends in mortality from hepatocellular carcinoma in Europe, 1980–2004. Hepatology. 2008;48(1):137–145. doi:10.1002/hep.22312
4. Goh GB, Chang PE, Tan CK. Changing epidemiology of hepatocellular carcinoma in Asia. Best Pract Res Clin Gastroenterol. 2015;29(6):919–928. doi:10.1016/j.bpg.2015.09.007
5. Nishikawa H, Osaki Y. Non-B, non-C hepatocellular carcinoma (Review). Int J Oncol. 2013;43(5):1333–1342. doi:10.3892/ijo.2013.2061
6. Utsunomiya T, Shimada M, Kudo M, et al. A comparison of the surgical outcomes among patients with HBV-positive, HCV-positive, and non-B non-C hepatocellular carcinoma: a nationwide study of 11,950 patients. Ann Surg. 2015;261(3):513–520. doi:10.1097/SLA.0000000000000821
7. Kim JM, Kwon CH, Joh JW, et al. Outcomes after curative hepatectomy in patients with non-B non-C hepatocellular carcinoma and hepatitis B virus hepatocellular carcinoma from non-cirrhotic liver. J Surg Oncol. 2014;110(8):976–981. doi:10.1002/jso.23772
8. Li T, Qin LX, Gong X, et al. Hepatitis B virus surface antigen-negative and hepatitis C virus antibody-negative hepatocellular carcinoma: clinical characteristics, outcome, and risk factors for early and late intrahepatic recurrence after resection. Cancer. 2013;119(1):126–135. doi:10.1002/cncr.27697
9. Tateishi R, Okanoue T, Fujiwara N, et al. Clinical characteristics, treatment, and prognosis of non-B, non-C hepatocellular carcinoma: a large retrospective multicenter cohort study. J Gastroenterol. 2015;50(3):350–360. doi:10.1007/s00535-014-0973-8
10. Zhang XP, Gao YZ, Chen ZH, et al. An Eastern hepatobiliary surgery hospital/portal vein tumor thrombus scoring system as an aid to decision making on hepatectomy for hepatocellular carcinoma patients with portal vein tumor thrombus: a multicenter study. Hepatology. 2019;69(5):2076–2090. doi:10.1002/hep.30490
11. Wang Q, Xia D, Bai W, et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: a multicentre observational study. J Hepatol. 2019;70(5):893–903. doi:10.1016/j.jhep.2019.01.013
12. Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(3):329–338. doi:10.1055/s-2007-1007122
13. Amin MB, Gress DM. AJCC Cancer Staging Manual.
14. Chatellier G, Zapletal E, Lemaitre D, et al. The number needed to treat: a clinically useful nomogram in its proper context. BMJ. 1996;312(7028):426–429. doi:10.1136/bmj.312.7028.426
15. Iasonos A, Schrag D, Raj GV, et al. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
16. Wang Y, Li J, Xia Y, et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy. J Clin Oncol. 2013;31(9):1188–1195. doi:10.1200/JCO.2012.41.5984
17. Zhang W, Tan Y, Jiang L, et al. Prognostic nomogram for patients with non-B non-C hepatocellular carcinoma after curative liver resection. Int J Surg. 2017;44:160–165. doi:10.1016/j.ijsu.2017.06.041
18. Pol B, Campan P, Hardwigsen J, et al. Morbidity of major hepatic resections: a 100-case prospective study. Eur J Surg. 1999;165(5):446–453. doi:10.1080/110241599750006686
19. Royston P, Altman DG. External validation of a Cox prognostic model: principles and methods. BMC Med Res Methodol. 2013;13:33. doi:10.1186/1471-2288-13-33
20. Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making. 2006;26(6):565–574. doi:10.1177/0272989X06295361
21. Chan AWH, Zhong J, Berhane S, et al. Development of pre and post-operative models to predict early recurrence of hepatocellular carcinoma after surgical resection. J Hepatol. 2018;69(6):1284–1293. doi:10.1016/j.jhep.2018.08.027
22. Utsunomiya T, Shimada M, Kudo M, et al. Nationwide study of 4741 patients with non-B non-C hepatocellular carcinoma with special reference to the therapeutic impact. Ann Surg. 2014;259(2):336–345. doi:10.1097/SLA.0b013e31829291e9
23. Nishio T, Hatano E, Sakurai T, et al. Impact of hepatic steatosis on disease-free survival in patients with non-b non-c hepatocellular carcinoma undergoing hepatic resection. Ann Surg Oncol. 2015;22(7):2226–2234. doi:10.1245/s10434-014-4181-9
24. Wu ZF, Xu Z, Li WS, et al. Impact of occult hepatitis B virus infection on outcome after resection for non-B non-C hepatocellular carcinoma. J Surg Res. 2015;193(1):153–160. doi:10.1016/j.jss.2014.07.021
25. Kai K, Koga H, Aishima S, et al. Impact of smoking habit on surgical outcomes in non-B non-C patients with curative resection for hepatocellular carcinoma. World J Gastroenterol. 2017;23(8):1397–1405. doi:10.3748/wjg.v23.i8.1397
26. Zhang JB, Chen Y, Zhang B, et al. Prognostic significance of serum gamma-glutamyl transferase in patients with intermediate hepatocellular carcinoma treated with transcatheter arterial chemoembolization. Eur J Gastroenterol Hepatol. 2011;23(9):787–793. doi:10.1097/MEG.0b013e32834902dd
27. Fu S, Guo Z, Li S, et al. Prognostic value of preoperative serum gamma-glutamyltranspeptidase in patients with hepatocellular carcinoma after hepatectomy. Tumour Biol. 2016;37(3):3433–3440. doi:10.1007/s13277-015-4136-1
28. Song P, Inagaki Y, Wang Z, et al. High levels of gamma-glutamyl transferase and indocyanine green retention rate at 15 min as preoperative predictors of tumor recurrence in patients with hepatocellular carcinoma. Medicine. 2015;94(21):e810. doi:10.1097/MD.0000000000000810
29. Corti A, Duarte TL, Giommarelli C, et al. Membrane gamma-glutamyl transferase activity promotes iron-dependent oxidative DNA damage in melanoma cells. Mutat Res. 2009;669(1–2):112–121. doi:10.1016/j.mrfmmm.2009.05.010
30. Kunutsor SK. Gamma-glutamyltransferase-friend or foe within? Liver Int. 2016;36(12):1723–1734. doi:10.1111/liv.13221
31. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. 2011;34(3):274–285. doi:10.1111/j.1365-2036.2011.04724.x
32. Wang FS, Fan JG, Zhang Z, et al. The global burden of liver disease: the major impact of China. Hepatology. 2014;60(6):2099–2108. doi:10.1002/hep.27406
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.